On the Optimal Synthesis of a Finger Rehabilitation Slider-Crank-Based Device with a Prescribed Real Trajectory: Motion Specifications and Design Process




Abstract
:
1. Introduction
2. Materials and Methods
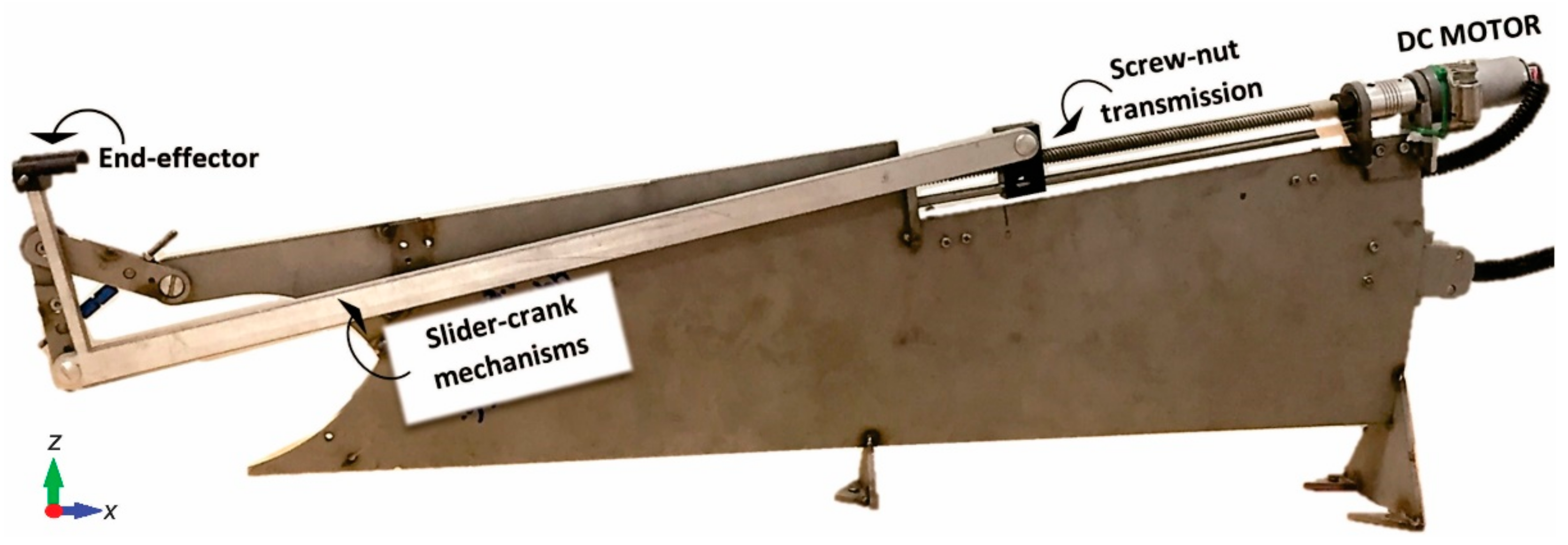
2.1. Finger Rehabilitation Device
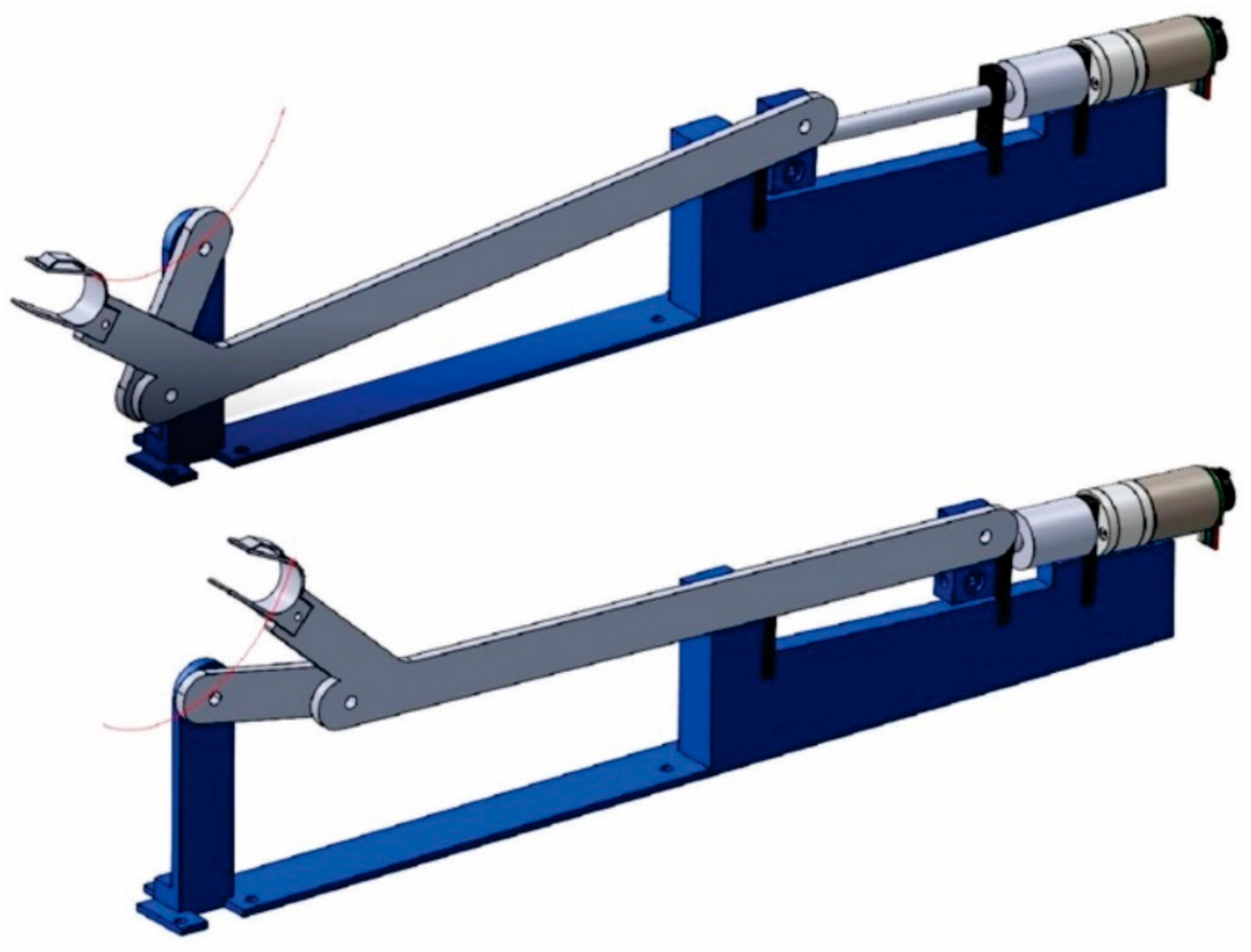
2.1.1. Existing Prototype
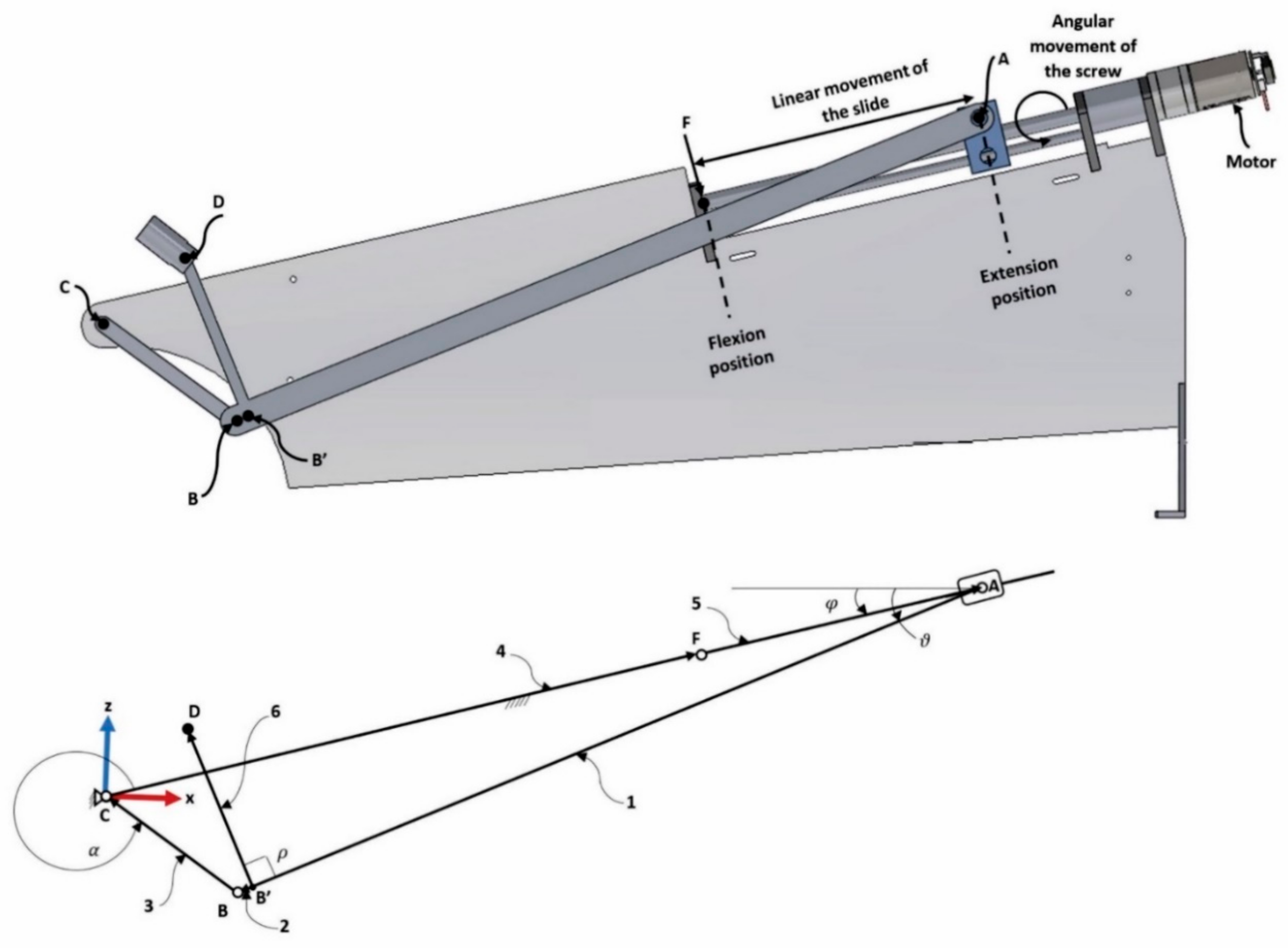
2.1.2. Architecture and Kinematic Model
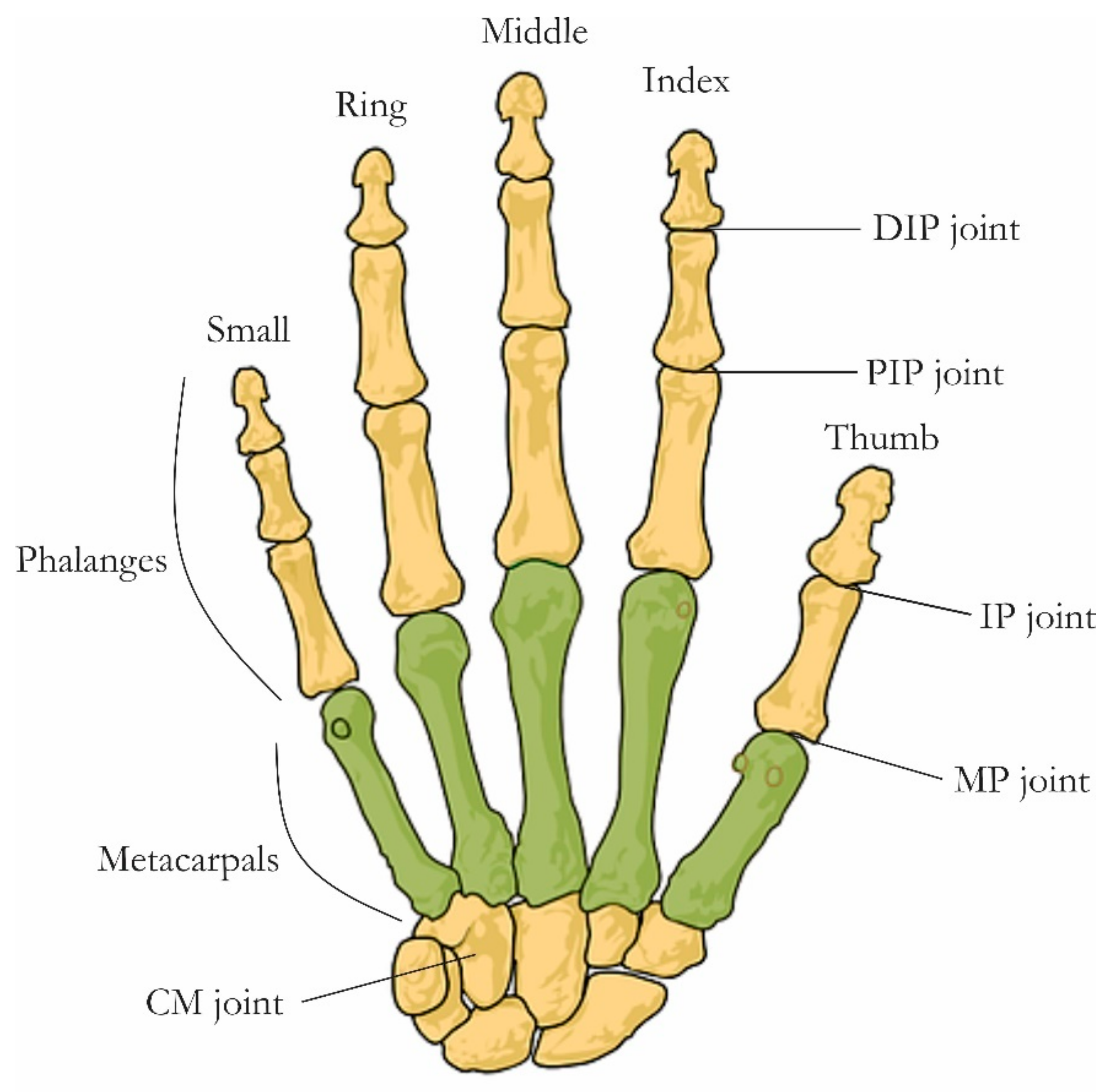
2.2. Finger Real Motion
2.2.1. Experimental Setup
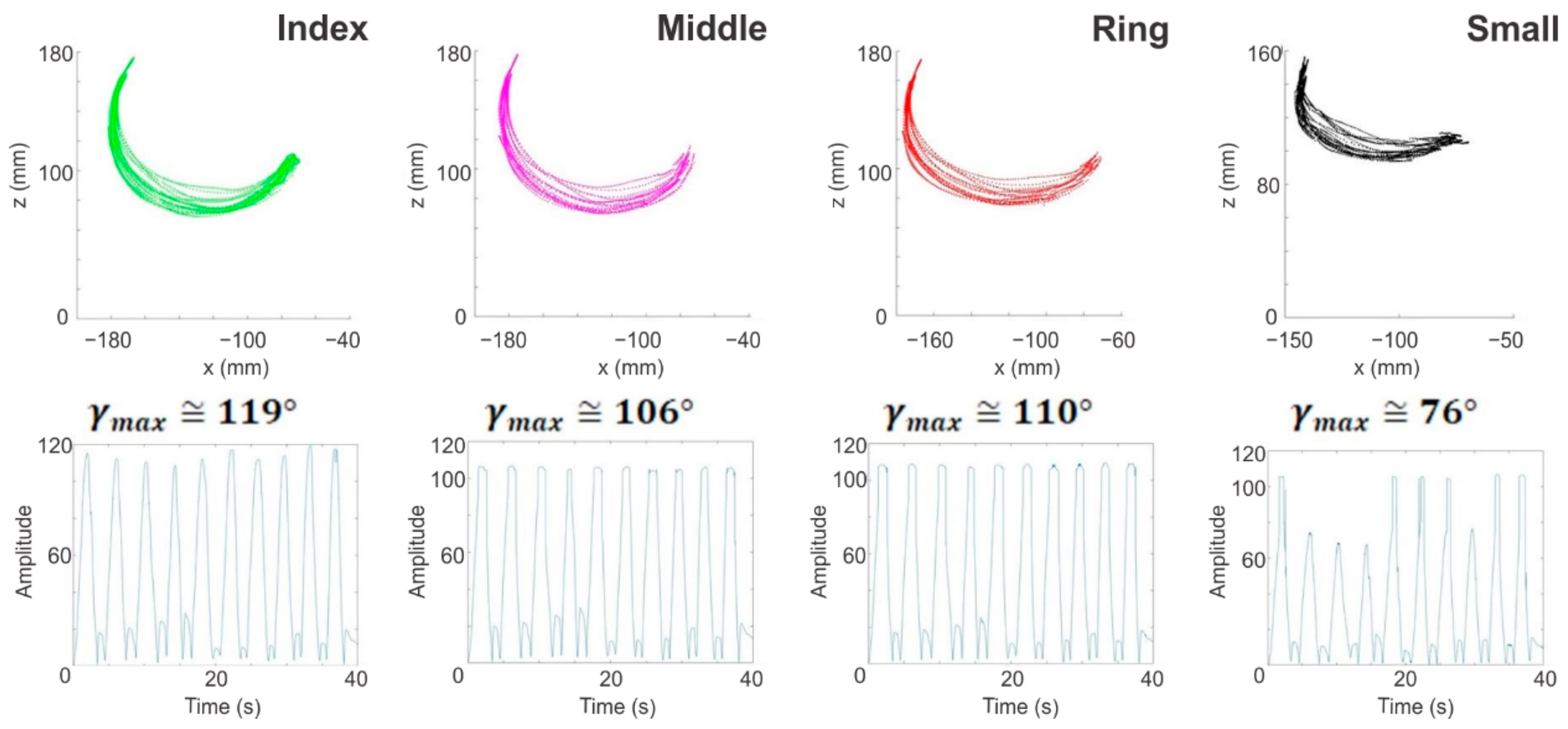
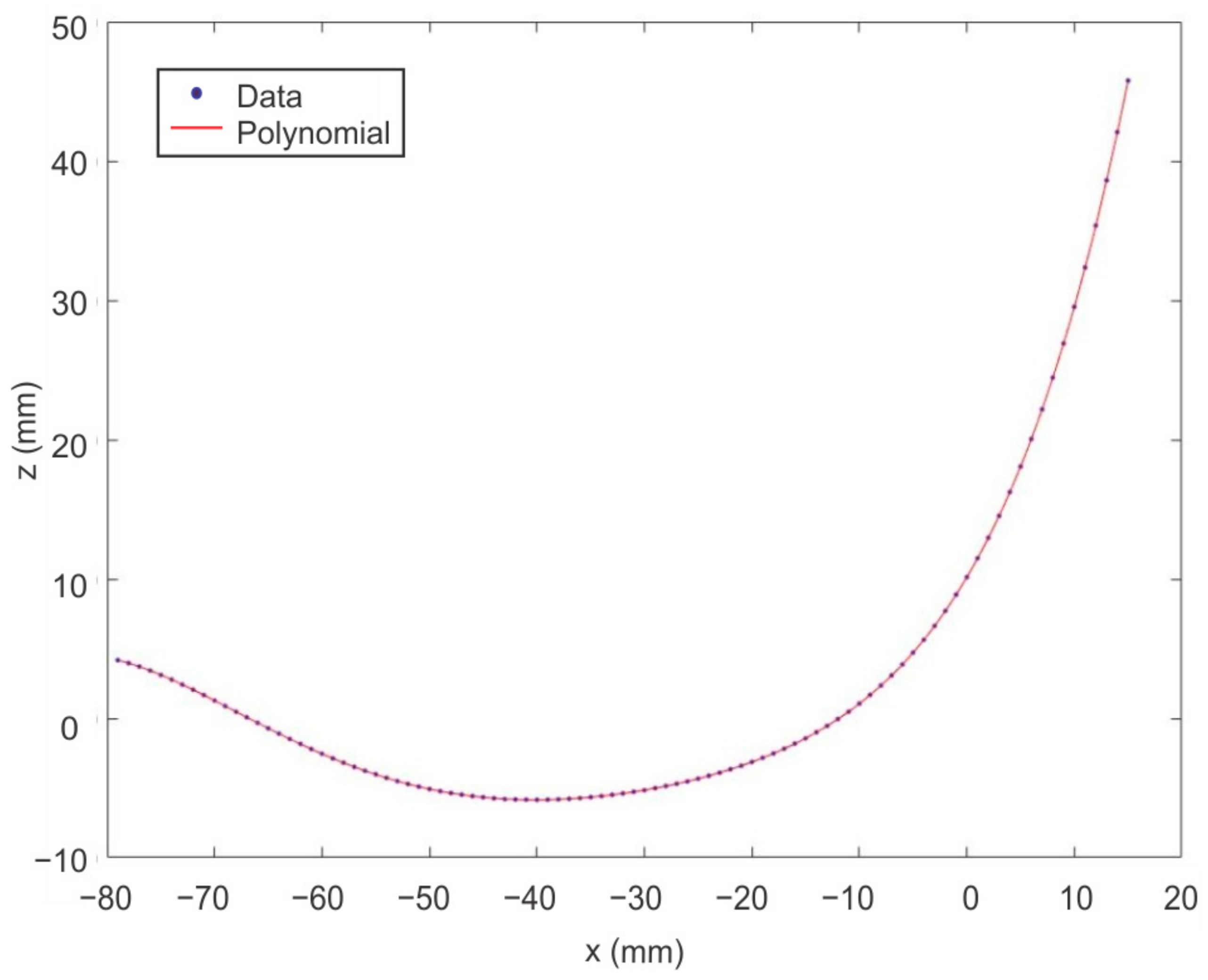
2.2.2. Results of the Analysis of the Fingers Real Motion
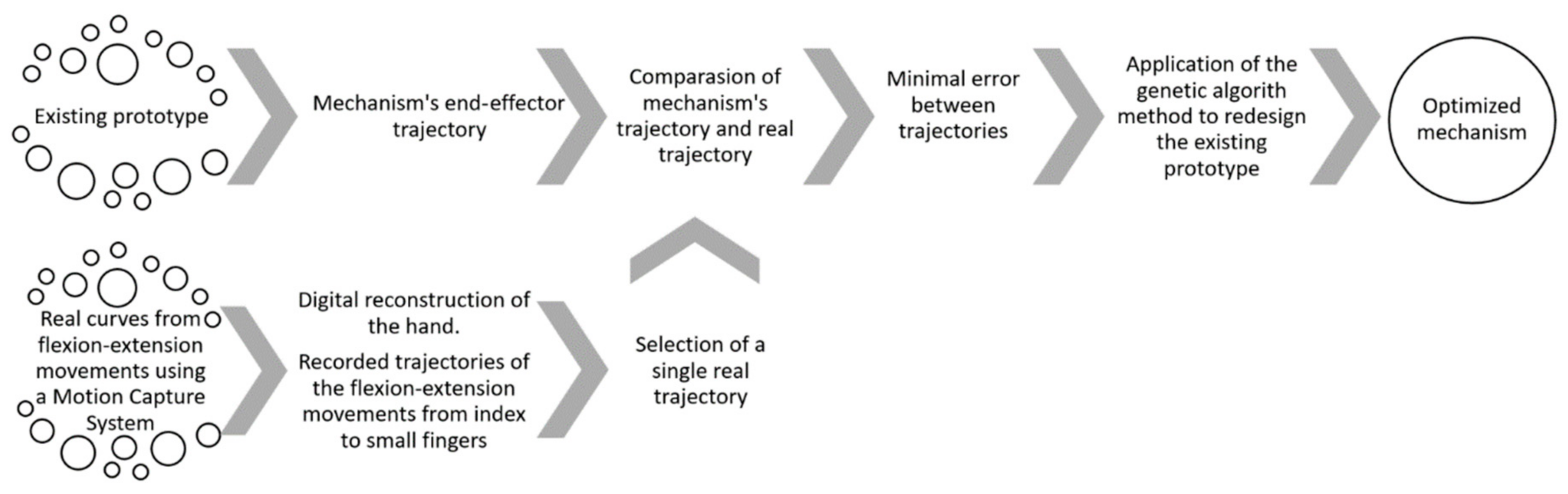
2.3. Synthesis Problem
2.3.1. Formulation of the Problem
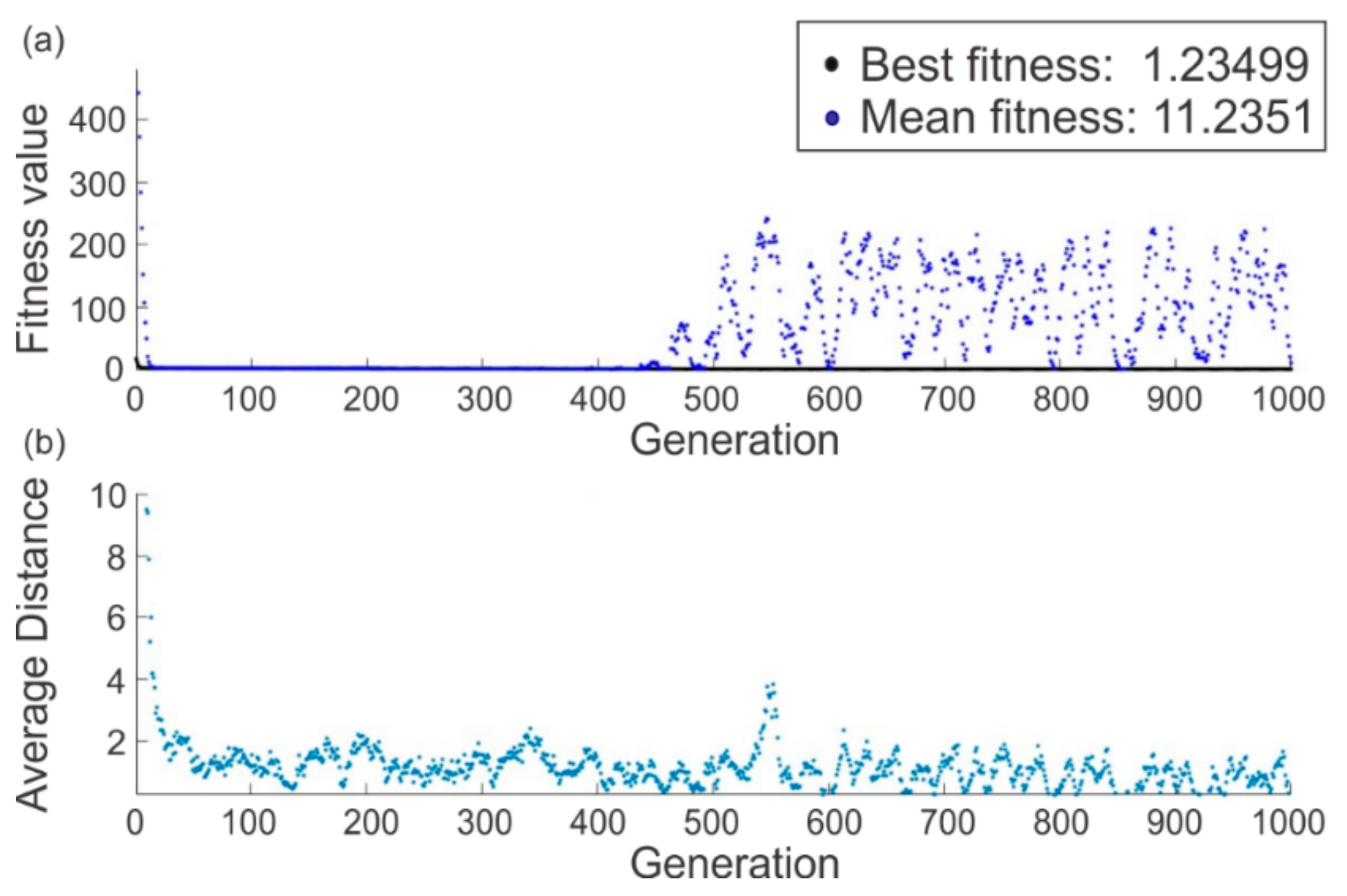
2.3.2. Genetic Algorithm Method Implementation and Curves Enhancement
3. Improvement of the Existing Mechanism and Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cooper, R.A.; Dicianno, B.E.; Brewer, B.; LoPresti, E.; Ding, D.; Simpson, R.; Grindle, G.; Wang, H. A Perspective on Intelligent Devices and Environments in Medical Rehabilitation. Med. Eng. Phys. 2008, 30, 1387–1398. [Google Scholar] [CrossRef] [PubMed]
- Freis, N.E. La Rehabilitación En Ortopedia y Traumatología Parte, I. Rev. Asoc. Argentina Ortop. Traumatol. 2006, 71, 272–277. (In Spanish) [Google Scholar] [CrossRef]
- Freis, N.E.; Heinrichs, K. La Rehabilitación En Ortopedia y Traumatología Parte II. Rev. Asoc. Argentina Ortop. Traumatol. 2006, 71, 362–368. (In Spanish) [Google Scholar]
- Dutton, M. Range of Motion. In Introduction to Physical Therapy and Patient Skills; McGraw-Hill Education: New York, NY, USA, 2014. [Google Scholar]
- Physical Rehabilitation. Available online: https://www.martinpetkov.com/your-opportunity/physical-rehabilitation (accessed on 9 December 2020).
- Borobia, C. Valoración Del Daño Corporal. Medicina de Los Seguros. Miembro Superior; Valoración del Daño Corporal; Masson Elsevier: Barcelona, Spain, 2006; Available online: https://books.google.com.mx/books?id=OClwWvys-ysC (accessed on 19 April 2020).
- Kim, Y.H.; Choi, J.H.; Chung, Y.K.; Kim, S.W.; Kim, J. Epidemiologic Study of Hand and Upper Extremity Injuries by Power Tools. Arch. Plast. Surg. 2019, 46, 63–68. [Google Scholar] [CrossRef] [Green Version]
- Krebs, H.I.; Edwards, D.; Hogan, N. Forging Mens et Manus: The MIT Robotic Therapy; Reinkensmeyer, D.J., Dietz, V., Eds.; Springer International Publishing: Berlin, Germany, 2016; pp. 333–350. [Google Scholar] [CrossRef]
- Burgar, C.G.; Lum, P.S.; Shor, P.C.; Machiel Van der Loos, H.F. Development of Robots for Rehabilitation Therapy: The Palo Alto VA/Stanford Experience. J. Rehabil. Res. Dev. 2000, 37, 663–673. [Google Scholar]
- Fasoli, S.E.; Krebs, H.I.; Stein, J.; Frontera, W.R.; Hogan, N. Effects of Robotic Therapy on Motor Impairment and Recovery in Chronic Stroke. Arch. Phys. Med. Rehabil. 2003, 84, 477–482. [Google Scholar] [CrossRef] [Green Version]
- Krebs, H.I.; Volpe, B.T.; Williams, D.; Celestino, J.; Charles, S.K.; Lynch, D.; Hogan, N. Robot-Aided Neurorehabilitation: A Robot for Wrist Rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2007, 15, 327–335. [Google Scholar] [CrossRef] [Green Version]
- Volpe, B.T.; Ferraro, M.; Krebs, H.I.; Hogan, N. Robotics in the Rehabilitation Treatment of Patients with Stroke. Curr. Atheroscler. Rep. 2002, 4, 270–276. [Google Scholar] [CrossRef]
- Fasoli, S.E.; Adans-Dester, C.P. A Paradigm Shift: Rehabilitation Robotics, Cognitive Skills Training, and Function after Stroke. Front. Neurol. 2019, 10, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Prunotto, L.; Cano-De La Cuerda, R.; Cuesta-Gómez, A.; Alguacil-Diego, I.M.; Molina-Rueda, F. Terapia Robótica Para La Rehabilitación Del Miembro Superior En Patología Neurológica. Rehabilitacion 2014, 48, 104–128. [Google Scholar] [CrossRef]
- Aggogeri, F.; Mikolajczyk, T.; Kane, J.O. Robotics for Rehabilitation of Hand Movement in Stroke Survivors. Adv. Mech. Eng. 2019, 11, 1–14. [Google Scholar] [CrossRef]
- Maciejasz, P.; Eschweiler, J.; Gerlach-hahn, K.; Jansen-troy, A.; Leonhardt, S. A Survey on Robotic Devices for Upper Limb Rehabilitation. J. Neuroeng. Rehabil. 2014, 11, 1–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yue, Z.; Zhang, X.; Wang, J. Hand Rehabilitation Robotics on Poststroke Motor Recovery. Behav. Neurol. 2017, 2017, 3908135. [Google Scholar] [CrossRef] [PubMed]
- Wege, A.; Zimmermann, A. Electromyography Sensor Based Control for a Hand Exoskeleton. In Proceedings of the 2007 IEEE International Conference on Robotics and Biomimetics, ROBIO, Sanya, China, 15–18 December 2007; pp. 1470–1475. [Google Scholar] [CrossRef]
- Bhandari, V.B. Design of Machine Elements; Tata McGraw-Hill Education: New Delhi, Delhi, India, 2007; Available online: https://books.google.com.mx/books?id=d-eNe-VRc1oC (accessed on 31 March 2020).
- Chiri, A.; Vitiello, N.; Giovacchini, F.; Roccella, S.; Vecchi, F.; Carrozza, M.C. Mechatronic Design and Characterization of the Index Finger Module of a Hand Exoskeleton for Post-Stroke Rehabilitation. IEEE/ASME Trans. Mechatron. 2012, 17, 884–894. [Google Scholar] [CrossRef]
- Pierce, R.M.; Fedalei, E.A.; Kuchenbecker, K.J. A Wearable Device for Controlling a Robot Gripper with Fingertip Contact, Pressure, Vibrotactile, and Grip Force Feedback. IEEE Haptics Symp. HAPTICS 2014, 19–25. [Google Scholar] [CrossRef]
- Amadeo®: The Hand Therapy World Champion. Available online: https://tyromotion.com/en/produkte/amadeo/ (accessed on 25 August 2019).
- Amar, J.; Nagase, K. Design Optimization of Tree-Type Robotic Systems Using Exponential Coordinates and Genetic Algorithms. In Proceedings of the 2020 6th International Conference on Control, Automation and Robotics (ICCAR), Singapore, 20–23 April 2020; pp. 67–73. [Google Scholar] [CrossRef]
- Premachandra, H.A.G.C.; Herath, H.M.A.; Suriyage, M.P.; Thathsarana, K.M.; Amarasinghe, Y.W.; Gopura, R.A.R.; Nanayakkara, S.A. Genetic Algorithm Based Pick and Place Sequence Optimization for a Color and Size Sorting Delta Robot. In Proceedings of the 2020 6th International Conference on Control, Automation and Robotics, ICCAR 2020, Singapore, 20–23 April 2020; pp. 209–213. [Google Scholar]
- Jamwal, P.K.; Kapsalyamov, A.; Hussain, S.; Ghayesh, M.H. Performance Based Design Optimization of an Intrinsically Compliant 6-Dof Parallel Robot. Mech. Based Des. Struct. Mach. 2020, 1–16. [Google Scholar] [CrossRef]
- Zeiaee, A.; Soltani-Zarrin, R.; Langari, R.; Tafreshi, R. Kinematic Design Optimization of an Eight Degree-of-Freedom Upper-Limb Exoskeleton. Robotica 2019, 37, 2073–2086. [Google Scholar] [CrossRef]
- Zhou, L.; Li, Y.; Bai, S. A Human-Centered Design Optimization Approach for Robotic Exoskeletons through Biomechanical Simulation. Rob. Auton. Syst. 2017, 91, 337–347. [Google Scholar] [CrossRef]
- Moosavian, S.A.A.; Nabipour, M.; Absalan, F.; Akbari, V. RoboWalk: Explicit Augmented Human-Robot Dynamics Modeling for Design Optimization. arXiv 2019, arXiv:1907.04114. [Google Scholar]
- Hernandez, E.; Valdez, S.I.; Carbone, G.; Ceccarelli, M. Design Optimization of a Cable-Driven Parallel Robot in Upper Arm Training-Rehabilitation Processes. Mech. Mach. Sci. 2018, 54, 413–423. [Google Scholar] [CrossRef]
- Dong, H.; Asadi, E.; Qiu, C.; Dai, J.; Chen, I.M. Geometric Design Optimization of an Under-Actuated Tendon-Driven Robotic Gripper. Robot. Comput. Integr. Manuf. 2018, 50, 80–89. [Google Scholar] [CrossRef]
- Bhupender, B.; Rahul, R. Study and Analysis of Design Optimization and Synthesis of Robotic ARM. Int. J. Adv. Eng. Manag. Sci. 2016, 2, 239459. [Google Scholar]
- Dutton, M. Improving Mobility. In Dutton’s Orthopaedic Examination, Evaluation, and Intervention; McGraw-Hill Education: New York, NY, USA, 2020. [Google Scholar]
- Edgerton, V.R.; Roy, R.R. Robotic Training and Spinal Cord Plasticity. Brain Res. Bull. 2009, 78, 4–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aguilar-Pereyra, J.F.; Castillo-Castaneda, E. Design of a Reconfigurable Robotic System for Flexoextension Fitted to Hand Fingers Size. Appl. Bionics Biomech. 2016, 1712831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, Y.; Iwashita, H.; Kawahira, K.; Hayashi, R. Development of Rehabilitation Device for Hemiplegic Fingers by Finger-Expansion Facilitation Exercise with Stretch Reflex. In Proceedings of the 2013 IEEE International Conference on Robotics and Biomimetics, ROBIO 2013, Shenzhen, China, 12–14 December 2013; pp. 1317–1323. [Google Scholar] [CrossRef]
- Castillo-Castaneda, E.; Bemardo-Vasquez, A. Personalized Design of a Hand Prosthesis Considering Anthropometry of a Real Hand Extracted from Radiography. In Proceedings of the 2017 IEEE International Conference on Rehabilitation Robotics (ICORR), London, UK, 17–20 July 2017; pp. 1215–1220. [Google Scholar] [CrossRef]
- Kamper, D.G. Stereotypical Fingertip Trajectories During Grasp. J. Neurophysiol. 2003, 90, 3702–3710. [Google Scholar] [CrossRef]
- Bishop, L.; Gordon, A.M.; Kim, H. Hand Robotic Therapy in Children with Hemiparesis: A Pilot Study. Am. J. Phys. Med. Rehabil. 2017, 96, 1–7. [Google Scholar] [CrossRef]
- Stein, J.; Bishop, L.; Gillen, G.; Helbok, R. Robot-Assisted Exercise for Hand Weakness After Stroke. Am. J. Phys. Med. Rehabil. 2011, 90, 887–894. [Google Scholar] [CrossRef]
- Treatment Technology. Available online: http://synergicpro.com/en/treatment-en/ (accessed on 9 December 2019).
- Zapatero-Gutiérrez, A.; Castillo-Castañeda, E. Control Design for a Fingers Rehabilitation Device. In Proceedings of the 2017 IEEE 3rd Colombian Conference on Automatic Control, CCAC 2017, Cartagena, Colombia, 18–20 October 2018; pp. 1–6. [Google Scholar] [CrossRef]
- Jolliffe, I.T. Principal Component Analysis; Springer Series in Statistics; Springer: New York, NY, USA, 2013; Available online: https://books.google.com.mx/books?id=-ongBwAAQBAJ (accessed on 19 April 2020).
- Ringnér, M. What Is Principal Component Analysis? Nat. Biotechnol. 2008, 26, 303–304. [Google Scholar] [CrossRef]
- Practical Guide to Principal Component Methods in R. Available online: http://www.sthda.com (accessed on 8 October 2019).
- Erdman, A.G. Computer-Aided Mechanism Design: Now and the Future. J. Mech. Des. Trans. ASME 1995, 117, 93–100. [Google Scholar] [CrossRef]
- Laribi, M.A.; Mlika, A.; Romdhane, L.; Zeghloul, S. A Combined Genetic Algorithm-Fuzzy Logic Method (GA-FL) in Mechanisms Synthesis. Mech. Mach. Theory 2004, 39, 717–735. [Google Scholar] [CrossRef]
- What Is the Genetic Algorithm? Available online: https://la.mathworks.com/help/gads/what-is-the-genetic-algorithm.html (accessed on 15 April 2019).
- Ortenzi, D.; Scarcia, U.; Meattini, R.; Palli, G.; Melchiorri, C. Synergy-Based Control of Anthropomorphic Robotic Hands with Contact Force Sensors. IFAC-PapersOnLine 2019, 52, 340–345. [Google Scholar] [CrossRef]
- Ficuciello, F.; Palli, G.; Melchiorri, C.; Siciliano, B. Postural Synergies of the UB Hand IV for Human-like Grasping. Robot. Auton. Syst. 2014, 62, 515–527. [Google Scholar] [CrossRef]
- Palli, G.; Ficuciello, F.; Scarcia, U.; Melchiorri, C.; Siciliano, B. Experimental Evaluation of Synergy-Based in-Hand Manipulation; IFAC: Cape Town, South Africa, 2014; Volume 19. [Google Scholar] [CrossRef] [Green Version]
- Santello, M.; Flanders, M.; Soechting, J.F. Postural Hand Synergies for Tool Use. J. Neurosci. 1998, 18, 10105–10115. [Google Scholar] [CrossRef] [PubMed]
- Amadeo® in Practice. Available online: https://irp-cdn.multiscreensite.com/91b5b819/files/uploaded/Factsheet_Amadeo_V1_en_screen.pdf (accessed on 13 December 2019).
- Digitrainer. Available online: https://www.ostracon.gr/wp-content/uploads/2020/12/DigiTrainer_Flyer_english_2019-20_web.pdf (accessed on 13 December 2019).

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Vector | 1 From A to B | 2 From B’ to B | 3 From B to C | 4 From C to F | 5 From C to A | 6 From B’ to D |
|---|---|---|---|---|---|---|
| Tag |
| Finger | Marker | Articulation |
|---|---|---|
| Thumb | T1 | Tip |
| T2 | IP | |
| T3 | MCP | |
| Index | I1 | Tip |
| I2 | DIJ | |
| I3 | PIJ | |
| I4 | MCP | |
| Middle | M1 | Tip |
| M2 | DIJ | |
| M3 | PIJ | |
| M4 | MCP | |
| Ring | R1 | Tip |
| R2 | DIJ | |
| R3 | PIJ | |
| R4 | MCP | |
| Small | S1 | Tip |
| S2 | DIJ | |
| S3 | PIJ | |
| S4 | MCP | |
| Wrist | W1 | Carpal bones |
| W2 | Carpal bones |
| New Set of Variables | Eigenvalues | % of the Total Variance | % of the Cumulative Variance |
|---|---|---|---|
| PC1 | 2444.9 | 82.0531 | 82.05 |
| PC2 | 516.5 | 17.3345 | 99.39 |
| PC3 | 18.2 | 0.6125 | 100.00 |
| Finger | ||||||
|---|---|---|---|---|---|---|
| Index | ||||||
| Middle | ||||||
| Ring | ||||||
| Small |
| Fitting Parameter | Error |
|---|---|
| 100 | 20 | 5 | 10 | −10 | −20 | 0 | −100 | −10 | −10 | |
| 1000 | 600 | 70 | 200 | 120 | 200 | 900 | 4 | 4 | 10 | |
| Prototype | 411.19 | 83.77 | 7.63 | 87.17 | 10 | 90 | 344 | 0 | 0 | 125 |
| GA | 295.11 | 54.29 | 21.11 | 69.88 | −3.56 | 139.71 | 246.11 | 3.99 | −6.51 | 9.99 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zapatero-Gutiérrez, A.; Castillo-Castañeda, E.; Laribi, M.A. On the Optimal Synthesis of a Finger Rehabilitation Slider-Crank-Based Device with a Prescribed Real Trajectory: Motion Specifications and Design Process. Appl. Sci. 2021, 11, 708. https://doi.org/10.3390/app11020708
Zapatero-Gutiérrez A, Castillo-Castañeda E, Laribi MA. On the Optimal Synthesis of a Finger Rehabilitation Slider-Crank-Based Device with a Prescribed Real Trajectory: Motion Specifications and Design Process. Applied Sciences. 2021; 11(2):708. https://doi.org/10.3390/app11020708
Chicago/Turabian StyleZapatero-Gutiérrez, Araceli, Eduardo Castillo-Castañeda, and Med Amine Laribi. 2021. "On the Optimal Synthesis of a Finger Rehabilitation Slider-Crank-Based Device with a Prescribed Real Trajectory: Motion Specifications and Design Process" Applied Sciences 11, no. 2: 708. https://doi.org/10.3390/app11020708