
The Relationship between Skinfold and Ultrasound Measures of Subcutaneous Fat in Untrained Healthy Males



Abstract
:1. Introduction
2. Materials and Methods
3. Results
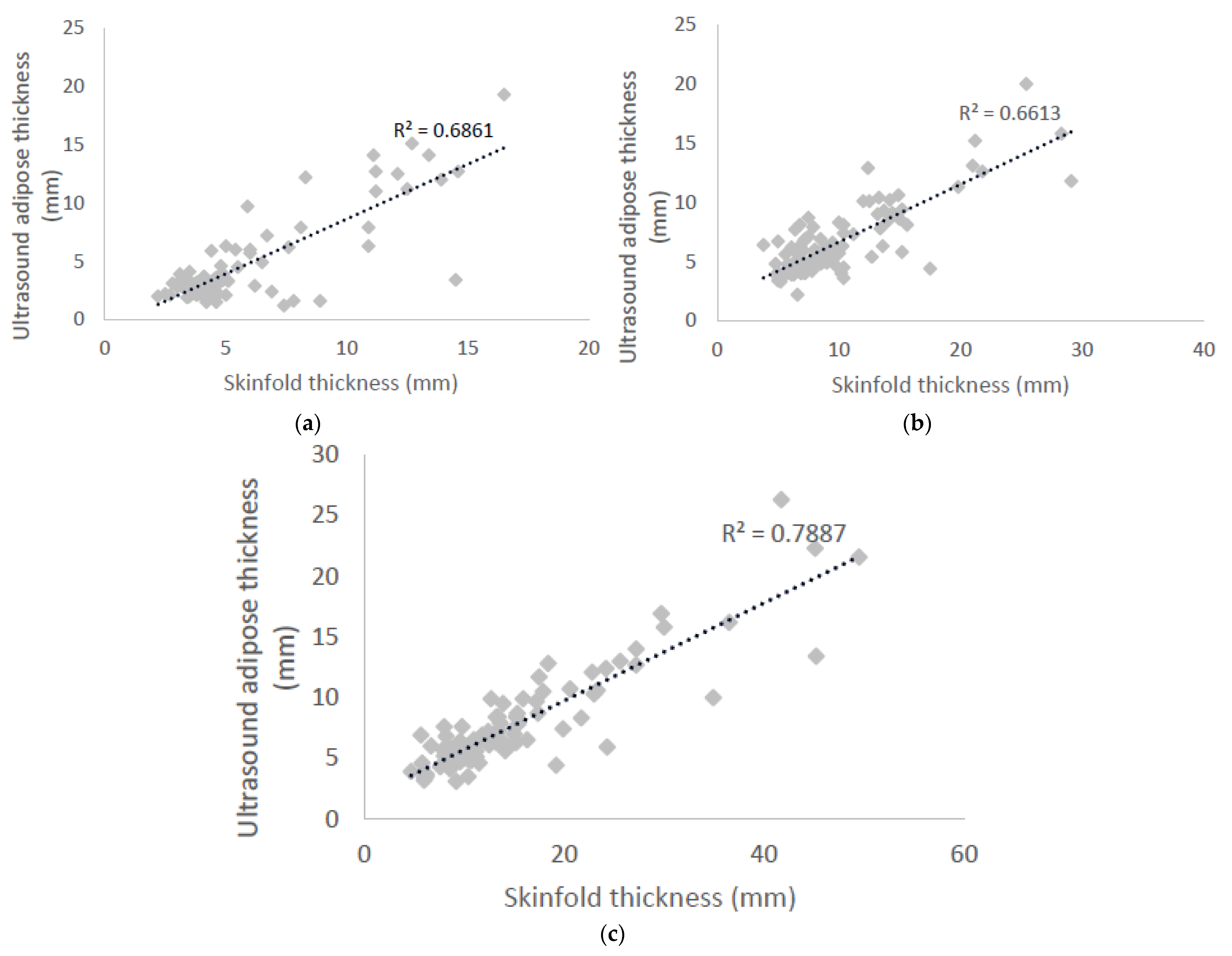
3.1. Pearson’s Correlation
3.2. Variance of Techniques
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Norton, K.; Olds, T. Anthropometrica: A Textbook of Body Measurement for Sports and Health Courses; UNSW Press: Kennington, Australia, 1996. [Google Scholar]
- Fosbøl, M.Ø.; Zerahn, B. Contemporary methods of body composition measurement. Clin. Physiol. Funct. Imaging 2015, 35, 81–97. [Google Scholar] [CrossRef] [PubMed]
- Ackland, T.R.; Lohman, T.G.; Sundgot-Borgen, J.; Maughan, R.J.; Meyer, N.L.; Stewart, A.D.; Müller, W. Current status of body composition assessment in sport. Sports Med. 2012, 42, 227–249. [Google Scholar] [CrossRef] [PubMed]
- Lemos, T.; Gallagher, D. Current body composition measurement techniques. Curr. Opin. Endocrinol. Diabetes Obes. 2017, 24, 310. [Google Scholar] [CrossRef] [PubMed]
- Kuriyan, R. Body composition techniques. Indian J. Med. Res. 2018, 148, 648. [Google Scholar] [CrossRef]
- Buchheit, M.; Mendez-Villanueva, A. Reliability and stability of anthropometric and performance measures in highly-trained young soccer players: Effect of age and maturation. J. Sports Sci. 2013, 31, 1332–1343. [Google Scholar] [CrossRef] [PubMed]
- Wagner, D.R. Ultrasound as a tool to assess body fat. J. Obes. 2013, 2013, 280713. [Google Scholar] [CrossRef]
- Duck, F.A.; Baker, A.C.; Starritt, H.C. Ultrasound in Medicine; CRC Press: Boca Raton, FL, USA, 2020. [Google Scholar]
- McArdle, W.D.; Katch, F.I.; Katch, V.L. Exercise Physiology: Nutrition, Energy and Human Performance; Wolters Kluwer Health: Baltimore, MD, USA, 2015. [Google Scholar]
- Pineau, J.C.; Lalys, L.; Bocquet, M.; Guihard-Costa, A.M.; Polak, M.; Frelut, M.L.; Peres, G.; Dabbas-Tyan, M. Ultrasound measurement of total body fat in obese adolescents. Ann. Nutr. Metab. 2010, 56, 36–44. [Google Scholar] [CrossRef]
- Ismail, C.; Zabal, J.; Hernandez, H.J.; Woletz, P.; Manning, H.; Teixeira, C.; DiPietro, L.; Blackman, M.R.; Harris-Love, M.O. Diagnostic ultrasound estimates of muscle mass and muscle quality discriminate between women with and without sarcopenia. Front. Physiol. 2015, 6, 302. [Google Scholar] [CrossRef] [Green Version]
- Takai, Y.; Ohta, M.; Akagi, R.; Kato, E.; Wakahara, T.; Kawakami, Y.; Fukunaga, T.; Kanehisa, H. Applicability of ultrasound muscle thickness measurements for predicting fat-free mass in elderly population. J. Nutr. Health Aging 2014, 18, 579–585. [Google Scholar] [CrossRef]
- Pereira, A.Z.; Marchini, J.S.; Carneiro, G.; Arasaki, C.H.; Zanella, M.T. Lean and fat mass loss in obese patients before and after Roux-en-Y gastric bypass: A new application for ultrasound technique. Obes. Surg. 2012, 22, 597–601. [Google Scholar] [CrossRef]
- Andreoli, A.; Garaci, F.; Cafarelli, F.P.; Guglielmi, G. Body composition in clinical practice. Eur. J. Radiol. 2016, 85, 1461–1468. [Google Scholar] [CrossRef] [Green Version]
- Bazzocchi, A.; Filonzi, G.; Ponti, F.; Albisinni, U.; Guglielmi, G.; Battista, G. Ultrasound: Which role in body composition? Eur. J. Radiol. 2016, 85, 1469–1480. [Google Scholar] [CrossRef]
- Madden, A.M.; Smith, S. Body composition and morphological assessment of nutritional status in adults: A review of anthropometric variables. J. Hum. Nutr. Diet. 2016, 29, 7–25. [Google Scholar] [CrossRef]
- Esparza-Ros, F.; Vaquero-Cristobal, R.; Marfell-Jones, M. International Standards for Anthropometric Assessment; The International Society for the Advancement of Kinanthropomety: Murcia, Spain, 2019. [Google Scholar]
- Hume, P.; Marfell-Jones, M. The importance of accurate site location for skinfold measurement. J. Sports Sci. 2008, 26, 1333–1340. [Google Scholar] [CrossRef] [PubMed]
- Bray, G.A.; Greenway, F.L.; Molitch, M.E.; Dahms, W.T.; Atkinson, R.L.; Hamilton, K. Use of anthropometric measures to assess weight loss. Am. J. Clin. Nutr. 1978, 31, 769–773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Himes, J.H.; Roche, A.F.; Siervogel, R.M. Compressibility of skinfolds and the measurement of subcutaneous fatness. Am. J. Clin. Nutr. 1979, 32, 1734–1740. [Google Scholar] [CrossRef] [Green Version]
- Selkow, N.M.; Pietrosimone, B.G.; Saliba, S.A. Subcutaneous thigh fat assessment: A comparison of skinfold calipers and ultrasound imaging. J. Athl. Train. 2011, 46, 50–54. [Google Scholar] [CrossRef] [Green Version]
- Müller, W.; Horn, M.; Fürhapter-Rieger, A.; Kainz, P.; Kröpfl, J.M.; Maughan, R.J.; Ahammer, H. Body composition in sport: A comparison of a novel ultrasound imaging technique to measure subcutaneous fat tissue compared with skinfold measurement. Br. J. Sports Med. 2013, 47, 1028–1035. [Google Scholar] [CrossRef]
- McRae, M.P. Male and female differences in variability with estimating body fat composition using skinfold calipers. J. Chiropr. Med. 2010, 9, 157–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thoirs, K.; English, C. Ultrasound measures of muscle thickness: Intra-examiner reliability and influence of body position. Clin. Physiol. Funct. Imaging 2009, 29, 440–446. [Google Scholar] [CrossRef]
- Müller, W.; Maughan, R.J. The need for a novel approach to measure body composition: Is ultrasound an answer? Br. J. Sports Med. 2013, 47, 1001–1002. [Google Scholar] [CrossRef] [PubMed]
- Müller, W.; Lohman, T.G.; Stewart, A.D.; Maughan, R.J.; Meyer, N.L.; Sardinha, L.B.; Kirihennedige, N.; Reguant-Closa, A.; Risoul-Salas, V.; Sundgot-Borgen, J.; et al. Subcutaneous fat patterning in athletes: Selection of appropriate sites and standardisation of a novel ultrasound measurement technique: Ad hoc working group on body composition, health and performance, under the auspices of the IOC Medical Commission. Br. J. Sports Med. 2016, 50, 45–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. Set correlation and contingency tables. Appl. Psychol. Meas. 1988, 12, 425–434. [Google Scholar] [CrossRef]
- Kelso, A.; Trájer, E.; Machus, K.; Treff, G.; Müller, W.; Steinacker, J.M. Assessment of subcutaneous adipose tissue using ultrasound in highly trained junior rowers. Eur. J. Sport Sci. 2017, 17, 576–585. [Google Scholar] [CrossRef] [PubMed]
- Ulbricht, L.; Neves, E.B.; Ripka, W.L.; Romaneli, E.F. Comparison between body fat measurements obtained by portable ultrasound and caliper in young adults. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 1952–1955. [Google Scholar]
- Ng, J.; Rohling, R.; Lawrence, P.D. Automatic measurement of human subcutaneous fat with ultrasound. IEEE Trans. Ultrason. Ferroelectr. Freq. Control. 2009, 56, 1642–1653. [Google Scholar] [CrossRef] [Green Version]
- Vatier, C.; Poitou, C.; Clément, K. Evaluation of Visceral Fat. In Nutrition in the Prevention and Treatment of Abdominal Obesity; Watson, R.R., Ed.; Elseiver: London, UK, 2014; pp. 68–73. [Google Scholar]
- Kuczmarski, R.J.; Fanelli, M.T.; Koch, G.G. Ultrasonic assessment of body composition in obese adults: Overcoming the limitations of the skinfold caliper. Am. J. Clin. Nutr. 1987, 45, 717–724. [Google Scholar] [CrossRef] [Green Version]
- Spinner, D.A.; Kirschner, J.S.; Herrera, J.E. Atlas of Ultrasound Guided Musculoskeletal Injections; Springer: New York, NY, USA, 2014. [Google Scholar]
- Saranteas, T. Limitations in ultrasound imaging techniques in anesthesia: Obesity and muscle atrophy? Anesth. Analg. 2009, 109, 993–994. [Google Scholar] [CrossRef]
- Gomes, A.C.; Landers, G.J.; Binnie, M.J.; Goods, P.S.; Fulton, S.K.; Ackland, T.R. Body composition assessment in athletes: Comparison of a novel ultrasound technique to traditional skinfold measures and criterion DXA measure. J. Sci. Med. Sport 2020, 23, 1006–1010. [Google Scholar] [CrossRef]


{kind=link}
| Measurement Site | Skinfold (mm) | Ultrasound (mm) | Difference (mm) |
|---|---|---|---|
| Biceps | 5.5 ± 3.1 | 4.4 ± 3.6 | 1.1 ± 2.0 * |
| Triceps | 9.9 ± 5.0 | 6.6 ± 3.0 | 3.3 ± 3.1 * |
| Front Thigh | 14.8 ± 9.0 | 7.6 ± 4.1 | 7.1 ± 5.7 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ryan-Stewart, H.; O’Leary, A.; Paine, E.; Faulkner, J.; Jobson, S. The Relationship between Skinfold and Ultrasound Measures of Subcutaneous Fat in Untrained Healthy Males. Appl. Sci. 2021, 11, 10561. https://doi.org/10.3390/app112210561
Ryan-Stewart H, O’Leary A, Paine E, Faulkner J, Jobson S. The Relationship between Skinfold and Ultrasound Measures of Subcutaneous Fat in Untrained Healthy Males. Applied Sciences. 2021; 11(22):10561. https://doi.org/10.3390/app112210561
Chicago/Turabian StyleRyan-Stewart, Helen, Abigail O’Leary, Eloise Paine, James Faulkner, and Simon Jobson. 2021. "The Relationship between Skinfold and Ultrasound Measures of Subcutaneous Fat in Untrained Healthy Males" Applied Sciences 11, no. 22: 10561. https://doi.org/10.3390/app112210561
APA StyleRyan-Stewart, H., O’Leary, A., Paine, E., Faulkner, J., & Jobson, S. (2021). The Relationship between Skinfold and Ultrasound Measures of Subcutaneous Fat in Untrained Healthy Males. Applied Sciences, 11(22), 10561. https://doi.org/10.3390/app112210561