
Electromechanical and Robotic Devices for Gait and Balance Rehabilitation of Children with Neurological Disability: A Systematic Review

 ,
,  ,
,  , ,
, ,  , , , , ,
, , , , ,  , , ,
, , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources
2.3. Search Strategy
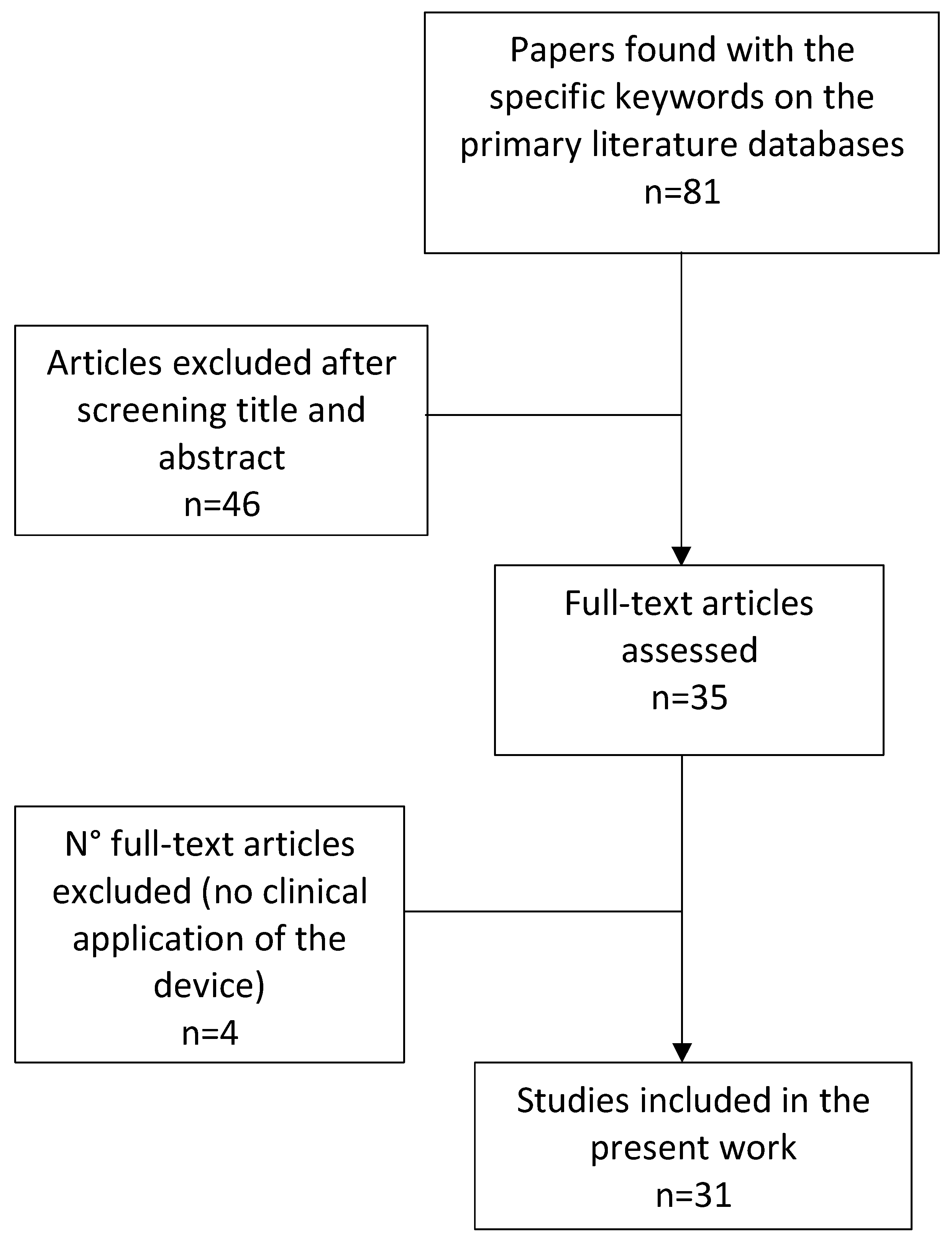
2.4. Selection Process
2.5. Data Collection
2.6. Study Quality Assessment
3. Results
3.1. Clinical Features
3.2. Robotic Devices
3.3. Rehabilitation Protocols Interventions

{kind=link}
| Study | Eligibility Criteria | Randomization | Allocation Concealment | Baseline Comparison | Blinding of All Subjects | Blinding of All Therapists | Blinding of All Assessors | Follow up Completeness | Intention to Treat | Between-Group Comparison | Point Estimates and Variability | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Beretta 2018 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 5 |
| Damiano 2017 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Druzbicki 2013 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 6 |
| Romei 2012 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 5 |
| Schroeder 2014 B | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 5 |
| Wallard 2017 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 8 |
| Wallard 2018 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Chen 2016 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 6 |
| Smania 2011 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 8 |
| Yazici 2019 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 4 |
| Device | Rehabilitation Aim | CE Class | CE MARK | CND | EE/Exo | Wearability | DoFs | Recorded Parameters | Control System | Device’s Main Features |
|---|---|---|---|---|---|---|---|---|---|---|
| Lokomat [27,28,30,32,33,34,37,49,50] | interactive | IIa | 1 | Z12069002 | Exo | no | (2 + 1) × 2 | kinematics, force | impedance, position | lower limbs gait orthosis with body weight support for treadmill walking |
| Lokomat + FreeD [41] | interactive | IIa | 1 | Z12069002 | Exo | no | (2 + 2) × 2 | ROM | impedance, position | lokomat + medio-lateral weight shifting support |
| MOTOMED [53] | interactive | IIa | 1 | Y034899 | EE | no | (2 + 1) × 2 | force | N/A | robotic cycling device |
| Hybrid Assistive Limb (HAL) [54] | interactive | IIb | 1 | N010299 | Exo | yes | (2 + 1) × 2 | - | force/kinematics, EMG | lower limbs wearable robot for overground walking |
| EksoGT [42] | interactive | IIa | 1 | Y99 | Exo | yes | (2 + 1) × 2 | kinematics | position | lower limbs wearable robot for overground walking |
| IntelliStretch [30,36,52,55,56,57] | interactive | - | - | - | EE | no | 1 + 0 | force, ROM | torque | device for ankle flexion-extension in sitting position with exergaming |
| Rutgers Ankle [43] | interactive | - | - | - | EE | no | 1 + 0 | ROM, force | position, force | device for ankle flexion-extension in sitting position with exergaming |
| PedBot [40] | interactive | - | - | - | EE | no | 2 + 0 | kinematics, force | force, torque | device for ankle assistive movement in sitting position with exergaming |
| ATLAS Exoskeleton [38] | interactive | - | - | - | Exo | yes | (3 + 0) ×2 | - | impedance | lower limbs wearable robot with weight support for overground walking |
| Exoskeleton for knee extension [47] | assistive | - | - | - | Exo | yes | 1 × 2 | kinematics, force | impedance | wearable robot for knee extension assistance during gait |
| Exoskeleton for ankle [45,46,51] | assistive | - | - | - | Exo | yes | 1 × 2 | torque, force | torque, force | wearable robot for ankle flexion-extension assistance during gait |
| pediAnklebot [39] | interactive | - | - | - | EE | no | 2 + 1 | kinematics, force | impedance | device for ankle assistive movement in sitting position with exergaming |
| FORTIS-102 [48] | interactive | - | - | - | EE | no | N/A | kinematics, force | N/A | device for simulation of horse riding |
| Gait Trainer GT1 [31] | assistive | - | - | - | EE | no | (1 + 2) × 2 | kinematics | position | gait assistive device with body weight support |
| Innowalk Pro [35] | interactive | - | - | - | Exo | yes | (1 + 2) × 2 | N/A | N/A | gait assistive device with body weight support |
| Trexo Home [44] | assistive | - | - | - | Exo | yes | (2 + 1) × 2 | N/A | N/A | lower limbs wearable robot for overground walking |
| Robot, Study | Study Design | nP, Mean Age (±SD), Diagnosis | Number of Sessions Session/Week | Sessions/ Day | Sessions’ Duration [min/ses] | Environment | Assistance Modality | Feedback | Difficulty Level | Study’s Main Results |
|---|---|---|---|---|---|---|---|---|---|---|
| Lokomat [27] | RCT | 26, 10.1y (2.2y) CP | 20 5/week | 1 | 45 | real | 0 | 2 | fixed | BG difference in the range of pelvic motion in the coronal plane on the right side No BG differences |
| Lokomat [28] | RCT | 14, 8.3y (1.2y) CP | 20 5/week | 1 | 40 | real | 0, 2 | 2 | adjustable | BG difference in balance in standing and walking (GMFM D-E) |
| Lokomat [29] | RCT | 14, 8.3y (1.2y) CP | 20 4 weeks | 1 | 40 | real | 0 | 2 | adjustable | BG difference in balance in standing and walking (GMFM D-E) |
| Lokomat [32] | RCT | 29, 11.2y (n.a) ABI | 20 5/week | 1 | 45 | real | 0 | 2 | adjustable | BG difference in balance in standing and walking (GMFM D-E) |
| Lokomat [34] | Uncontrolled trial | 18, 11.4y (4.9y) CP | 12 4/week | 1 | 30–60 | real | 0 | 2 | adjustable | WG improvement in balance in standing and walking (GMFM D-E) |
| Lokomat [37] | Uncontrolled trial | 14, 8.2y (5.4y) CP, SCI | 12 4/week | 1 | 50 | real | 0 | 2 | adjustable | WG improvement in balance in standing and walking (GMFM D-E) |
| Lokomat [49] | Uncontrolled trial | 22, 8.6y (2.1y) CP | 20 3–5/week | 1 | 45–60 | N/A | 0 | 2 | fixed | WG improvement in balance in standing (GMFM D) and walking speed |
| Lokomat [50] | Uncontrolled trial | 83, 10.8y (6.7y) CP | 12 4/week | 1 | 37 (±6) | real | 0 | 2 | adjustable | WG improvement in GMFM and COPM |
| Lokomat + FreeD [44] | Pilot comparative study | 15, 16y (2y) CP | 1 | 1 | 8 | real | 0, 6, 2 | 2 | adjustable | WG increase of proximal leg muscle activity when kinematic freedom of Lokomat was enlarged |
| MOTOMED [53] | RCT | 13, 9.2y (2.9y) CP | 60 5/week | 1 | 20 | real | 0, 2 | 2 | adjustable | BG difference in cadence while cycling—no differences in gait speed |
| HAL (Hybrid Assistive Limb) [54] | Uncontrolled trial | 6, 16.8y (3.5y) CP | 12 2–4/week | 1 | 20 | real | 3 | 2 | fixed | WG improvement of walking speed and spatiotemporal gait parameters |
| EksoGT [42] | Case study | 1, 17y CP | 12 3/week | 1 | 50 | real | 2 | 2, 3 | adjustable | WG improvement of speed and spatiotemporal gait parameters |
| IntelliStretch [30] | RCT | 18, 10.7y (6.0y) CP | 6 weeks 3/week | N/A | 40 | real | 0,2,7 | 1, 2 | adjustable | no BG differences (home vs lab robotic intervention) WG improvement in both groups for endurance, gait speed and balance (PBS) |
| IntelliStretch [52] | Uncontrolled trial | 28, 8.2y (3.6y) CP | 12 2/week | N/A | 75 | real | 0, 2, 7 | 1, 2 | adjustable | WG improvement in lower limb strength, spasticity (MAS), gait speed |
| IntelliStretch [55] | Uncontrolled trial | 23, 9yy (2.64) CP | 18 3/week | N/A | N/A | real | 0, 2, 7 | 1, 2 | adjustable | WG improvements in the ankle range of motion, muscle strength, spasticity (MAS) |
| IntelliStretch [36] | Uncontrolled trial | 10, 13.0y (3.9y) TBI | 15 3–5/week | N/A | 40 | real | 0, 2, 7 | 1, 2 | adjustable | WG improvements in the ankle range of motion, muscle strength, spasticity (MAS) |
| IntelliStretch [56] | Uncontrolled trial | 12, 8.6y (3.7y) CP | 18 3/week | N/A | 50 | real | 0, 2, 7 | 1, 2 | adjustable | WG improvements in the ankle range of motion, muscle strength, spasticity (MAS) |
| IntelliStretch [57] | Uncontrolled trial | 8, 13y (2.5y) CP | 18 3/week | N/A | 45–60 | real | 0, 3 | 1, 2, 3 | adjustable | WG improvement in spasticity (MAS) and balance (PBS) |
| Rutgers Ankle [43] | Uncontrolled trial | 1, 7y CP | 36 3/week | N/A | 40 | real | 1 | 1, 2 | adjustable | WG improvements in ankle strength and GMFM |
| PedBot [40] | Uncontrolled trial | 4, 13.7y (2.2y) CP | 20 N/A | N/A | 30 | virtual | 1, 3, 7 | 1, 2 | adjustable | WG improvement of ankle range of motion |
| ATLAS Exoskeleton [38] | Proof of concept | 2, 9y (12y) CP, Duchenne | N/A | N/A | N/A | real | 1, 3 | 2 | fixed | Not assessed |
| Exoskeleton for ankle [45] | Cohort study | 5, 5–30y CP | N/A | N/A | 25 | real | 2 | 2 | fixed | reducing of the metabolic cost of walking |
| Exoskeleton for ankle [46] | Uncontrolled trial | 5, 5–30y CP | N/A | N/A | N/A | real | 2 | 2 | fixed | WG increase of propulsive ankle joint power, reducing of plantar-flexor muscle iperactivity during walking |
| Exoskeleton for ankle [51] | Uncontrolled trial | 7, 14y (5y) CP | 1 | 1 | 8 | real | 2 | 2 | fixed | WG increasing in step length |
| pediAnklebot [39] | Uncontrolled trial | 3, 9y (n.a) CP, peroneal nerve lesion | N/A | N/A | N/A | real | 0, 3 | 1, 2 | adjustable | WG improvement device-assessed force parameters |
| Fortis-102 [48] | Case study | 1, 11y CP | 12 1/week | 1 | 45 | real | 0 | 2 | adjustable | increased abdominal muscle trophy and improve in static balance (stabilometry) |
| Gait trainer GT 1 [31] | RCT | 9, 13.9y (2.8y) CP | 10 5/week | N/A | 30 | real | 0 | 2 | adjustable | WG improvements in gait speed and endurance |
| Innowalk Pro [35] | CT | 12, 8.9y (n.a.) CP | 36 3/week | N/A | N/A | real | 1 | 2 | fixed | WG improvements in gait speed and endurance, no BG differences |
| Trexo Home [44] | Case study | 1, 7y CP | 36 3/week | N/A | 46 min/week | real | 0 | 2 | fixed | improved spasticity in knee flexion (MAS) |
4. Discussion
4.1. Population
4.2. Robotic Devices
4.3. Treatment Interventions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leonard, H.C. The Impact of Poor Motor Skills on Perceptual, Social and Cognitive Development: The Case of Developmental Coordination Disorder. Front. Psychol. 2016, 7, 311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreau, N.G.; Bodkin, A.W.; Bjornson, K.; Hobbs, A.; Soileau, M.; Lahasky, K. Effectiveness of Rehabilitation Interventions to Improve Gait Speed in Children with Cerebral Palsy: Systematic Review and Meta-analysis. Phys. Ther. 2016, 96, 1938–1954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucas, B.R.; Elliott, E.J.; Coggan, S.; Pinto, R.Z.; Jirikowic, T.; McCoy, S.W.; Latimer, J. Interventions to improve gross motor performance in children with neurodevelopmental disorders: A meta-analysis. BMC Pediatr. 2016, 16, 160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reid, L.; Rose, S.E.; Boyd, R.N. Rehabilitation and neuroplasticity in children with unilateral cerebral palsy. Nat. Rev. Neurol. 2015, 11, 390–400. [Google Scholar] [CrossRef]
- Langhorne, P.; Coupar, F.; Pollock, A. Motor recovery after stroke: A systematic review. Lancet Neurol. 2009, 8, 741–754. [Google Scholar] [CrossRef]
- Blank, R.; Smits-Engelsman, B.; Polatajko, H.; Wilson, P. European Academy for Childhood Dis-ability (EACD): Recommendations on the definition, diagnosis and intervention of developmental coordination disorder (long version). Dev. Med. Child Neurol. 2012, 54, 54. [Google Scholar] [CrossRef]
- YouRong, S.S.; Veeravagu, A.; Grant, G. Neuroplasticity after Traumatic Brain Injury in Translational Research in Traumatic Brain Injury; CRC Press/Taylor and Francis Group: Boca Raton, FL, USA, 2015. [Google Scholar]
- Siciliano, B.; Sciavicco, L.; Villani, L.; Oriolo, G. Robotics: Modelling, Planning and Control; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2010. [Google Scholar]
- Papaleo, E.; Zollo, L.; Garcia-Aracil, N.; Badesa, F.J.; Morales, R.; Mazzoleni, S.; Sterzi, S.; Guglielmelli, E. Upper-limb kinematic reconstruction during stroke robot-aided therapy. Med. Biol. Eng. Comput. 2015, 53, 815–828. [Google Scholar] [CrossRef]
- Gandolfi, M.; Formaggio, E.; Geroin, C.; Storti, S.F.; Boscolo Galazzo, I.; Bortolami, M.; Saltuari, L.; Picelli, A.; Waldner, A.; Manganotti, P.; et al. Quantification of Upper Limb Motor Recovery and EEG Power Changes after Robot-Assisted Bilateral Arm Training in Chronic Stroke Patients: A Prospective Pilot Study. Neural Plast. 2018, 2018, 8105480. [Google Scholar] [CrossRef] [Green Version]
- Gandolfi, M.; Formaggio, E.; Geroin, C.; Storti, S.F.; Galazzo, I.B.; Waldner, A.; Manganotti, P.; Smania, N. Electroencephalographic Changes of Brain Oscillatory Activity After Upper Limb Somatic Sensation Training in a Patient with Somatosensory Deficit After Stroke. Clin. EEG Neurosci. 2014, 46, 347–352. [Google Scholar] [CrossRef]
- Gandolfi, M.; Valè, N.; Posteraro, F.; Morone, G.; Dell’Orco, A.; Botticelli, A.; Dimitrova, E.; Gervasoni, E.; Goffredo, M.; Zenzeri, J.; et al. State of the art and challenges for the classification of studies on electromechanical and robotic devices in neurorehabilitation: A scoping review. Eur. J. Phys. Rehabil. Med. 2021, 57. [Google Scholar] [CrossRef]
- Turner, D.L.; Ramos-Murguialday, A.; Birbaumer, N.; Hoffmann, U.; Luft, A. Neurophysiology of robot-mediated training and therapy: A perspective for future use in clinical populations. Front. Neurol. 2013, 4, 184. [Google Scholar] [CrossRef] [Green Version]
- Rose, F.D.; Johnson, D.A.; Attree, E.A. Rehabilitation of the head-injured child: Basic research and new technology. Pediatric Rehabil. 1997, 1, 3–7. [Google Scholar] [CrossRef]
- Morone, G.; Cocchi, I.; Paolucci, S.; Iosa, M. Robot-assisted therapy for arm recovery for stroke patients: State of the art and clinical implication. Expert Rev. Med. Devices 2020, 17, 223–233. [Google Scholar] [CrossRef]
- Pisla, D.; Nadas, I.; Tucan, P.; Albert, S.; Carbone, G.; Antal, T.; Banica, A.; Gherman, B. Development of a Control System and Functional Validation of a Parallel Robot for Lower Limb Rehabilitation. Actuators 2021, 10, 277. [Google Scholar] [CrossRef]
- Vaida, C.; Birlescu, I.; Pisla, A.; Ulinici, I.-M.; Tarnita, D.; Carbone, G.; Pisla, D. Systematic Design of a Parallel Robotic System for Lower Limb Rehabilitation. IEEE Access 2020, 8, 34522–34537. [Google Scholar] [CrossRef]
- Shirota, C.; Jansa, J.; Diaz, J.; Balasubramanian, S.; Mazzoleni, S.; Borghese, N.A.; Melendez-Calderon, A. On the assessment of coordination between upper extremities: Towards a common language between rehabilitation engineers, clinicians and neuroscientists. J. Neuroeng. Rehabil. 2016, 13, 80. [Google Scholar] [CrossRef] [Green Version]
- Falzarano, V.; Marini, F.; Morasso, P.; Zenzeri, J. Devices and Protocols for Upper Limb Robot-Assisted Rehabilitation of Children with Neuromotor Disorders. Appl. Sci. 2019, 9, 2689. [Google Scholar] [CrossRef] [Green Version]
- Basteris, A.; Nijenhuis, S.M.; Stienen, A.H.A.; Buurke, J.H.; Prange, G.B.; Amirabdollahian, F. Training modalities in robot-mediated upper limb rehabilitation in stroke: A framework for classification based on a systematic review. J. Neuroeng. Rehabil. 2014, 11, 111. [Google Scholar] [CrossRef] [Green Version]
- Hariohm, K.; Prakash, V.; Saravankumar, J. Quantity and quality of randomized controlled trials published by Indian physiotherapists. Perspect. Clin. Res. 2015, 6, 91–97. [Google Scholar] [CrossRef]
- Krebs, H.I.; Rossi, S.; Kim, S.-J.; Artemiadis, P.; Williams, D.; Castelli, E.; Cappa, P. Pediatric anklebot. In Proceedings of the 2011 IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 27 June–1 July 2011; pp. 1–5. [Google Scholar]
- Herrero, P.; Asensio, A.; García, E.; Marco, A.; Oliván, B.; Ibarz, A.; Gómez-Trullén, E.M.; Casas, R. Study of the therapeutic effects of an advanced hippotherapy simulator in children with cerebral palsy: A randomized controlled trial. BMC Musculoskelet. Disord. 2010, 11, 71. [Google Scholar] [CrossRef] [Green Version]
- Gasparri, G.M.; Luque, J.; Lerner, Z.F. Proportional Joint-Moment Control for Instantaneously Adaptive Ankle Exoskeleton Assistance. IEEE Trans. Neural. Syst. Rehabil. Eng. 2019, 27, 751–759. [Google Scholar] [CrossRef]
- Borggraefe, I.; Klaiber, M.; Schuler, T.; Warken, B.; Schroeder, S.A.; Heinen, F.; Meyer-Heim, A. Safety of robotic-assisted treadmill therapy in children and adolescents with gait impairment: A bi-centre survey. Dev. Neurorehabilit. 2010, 13, 114–119. [Google Scholar] [CrossRef]
- Damiano, D.L. Activity, activity, activity: Rethinking our physical therapy approach to cerebral palsy. Phys. Ther. 2006, 86, 1534–1540. [Google Scholar] [CrossRef]
- Drużbicki, M.; Rusek, W.; Snela, S.; Dudek, J.; Szczepanik, M.; Zak, E.; Durmala, J.; Czernuszenko, A.; Bonikowski, M.; Sobota, G. Functional effects of robotic-assisted locomotor treadmill therapy in children with cerebral palsy. J. Rehabil. Med. 2013, 45, 358–363. [Google Scholar] [CrossRef] [Green Version]
- Wallard, L.; Dietrich, G.; Kerlirzin, Y.; Bredin, J. Robotic-assisted gait training improves walking abilities in diplegic children with cerebral palsy. Eur. J. Paediatr. Neurol. 2017, 21, 557–564. [Google Scholar] [CrossRef]
- Wallard, L.; Dietrich, G.; Kerlirzin, Y.; Bredin, J. Effect of robotic-assisted gait rehabilitation on dynamic equilibrium control in the gait of children with cerebral palsy. Gait Posture 2018, 60, 55–60. [Google Scholar] [CrossRef]
- Chen, K.; Wu, Y.-N.; Ren, Y.; Liu, L.; Gaebler-Spira, D.; Tankard, K.; Lee, J.; Song, W.; Wang, M.; Zhang, L.-Q. Home-Based Versus Laboratory-Based Robotic Ankle Training for Children with Cerebral Palsy: A Pilot Randomized Comparative Trial. Arch. Phys. Med. Rehabil. 2016, 97, 1237–1243. [Google Scholar] [CrossRef] [Green Version]
- Smania, N.; Bonetti, P.; Gandolfi, M.; Cosentino, A.; Waldner, A.; Hesse, S.; Werner, C.; Bisoffi, G.; Geroin, C.; Munari, D. Improved Gait After Repetitive Locomotor Training in Children with Cerebral Palsy. Am. J. Phys. Med. Rehabil. 2011, 90, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Beretta, E.; Molteni, E.; Biffi, E.; Morganti, R.; Avantaggiato, P.; Strazzer, S. Robotically-driven orthoses exert proximal-to-distal differential recovery on the lower limbs in children with hemiplegia, early after acquired brain injury. Eur. J. Paediatr. Neurol. 2018, 22, 652–661. [Google Scholar] [CrossRef] [PubMed]
- Romei, M.; Montinaro, A.; Piccinini, L.; Maghini, C.; Germiniasi, C.; Bo, I.; Turconi, A.C. Efficacy of robotic-assisted gait training compared with intensive task-oriented physiotherapy for children with Cerebral Palsy. In Proceedings of the 2012 4th IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics (BioRob), Rome, Italy, 24–27 June 2012; pp. 1890–1894. [Google Scholar]
- Schroeder, A.S.; Von Kries, R.; Riedel, C.; Homburg, M.; Auffermann, H.; Blaschek, A.; Jahn, K.; Heinen, F.; Borggraefe, I.; Berweck, S. Patient-specific determinants of responsiveness to robot-enhanced treadmill therapy in children and adolescents with cerebral palsy. Dev. Med. Child Neurol. 2014, 56, 1172–1179. [Google Scholar] [CrossRef] [PubMed]
- Yazıcı, M.; Livanelioğlu, A.; Gücüyener, K.; Tekin, L.; Sümer, E.; Yakut, Y. Effects of robotic rehabilitation on walking and balance in pediatric patients with hemiparetic cerebral palsy. Gait Posture 2019, 70, 397–402. [Google Scholar] [CrossRef]
- Chen, K.; Xiong, B.; Ren, Y.; Dvorkin, A.; Gaebler-Spira, D.; Sisung, C.; Zhang, L. Ankle passive and active movement training in children with acute brain injury using a wearable robot. J. Rehabil. Med. 2018, 50, 30–36. [Google Scholar] [CrossRef] [Green Version]
- Borggraefe, I.; Kiwull, L.; Schaefer, J.S.; Koerte, I.; Blaschek, A.; Meyer-Heim, A.; Heinen, F. Sustainability of motor performance after robotic-assisted treadmill therapy in children: An open, non-randomized baseline-treatment study. Eur. J. Phys. Rehabil. Med. 2010, 46, 125–131. [Google Scholar] [CrossRef]
- Garcia, E.; Cestari, M.; Sanz-Merodio, D. Wearable exoskeletons for the physical treatment of children with quad-riparesis. In Proceedings of the 2014 IEEE-RAS International Conference on Humanoid Robots, Madrid, Spain, 18–20 November 2014; pp. 425–430. [Google Scholar]
- Michmizos, K.P.; Rossi, S.; Castelli, E.; Cappa, P.; Krebs, H.I. Robot-Aided Neurorehabilitation: A Pediatric Robot for Ankle Rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 23, 1056–1067. [Google Scholar] [CrossRef] [Green Version]
- Cleary, K.; Monfaredi, R.; Salvador, T.; Talari, H.F.; Coley, C.; Kovelman, S.; Belschner, J.; Alyamani, S.; Schladen, M.; Evans, S.H. Pedbothome: Robotically-Assisted Ankle Rehabilitation System for Children with Cerebral Palsy. In Proceedings of the 2019 IEEE 16th International Conference on Rehabilitation Robotics (ICORR), Toronto, ON, Canada, 24–28 June 2019; Volume 2019, pp. 13–20. [Google Scholar]
- Aurich-Schuler, T.; Grob, F.; Van Hedel, H.J.; Labruyère, R. Can Lokomat therapy with children and adolescents be improved? An adaptive clinical pilot trial comparing Guidance force, Path control, and FreeD. J. Neuroeng. Rehabil. 2017, 14, 76. [Google Scholar] [CrossRef] [Green Version]
- Karunakaran, K.K.; Ehrenberg, N.; Cheng, J.; Nolan, K.J. Effects of Robotic Exoskeleton Gait Training on an Adolescent with Brain Injury. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; Volume 2019, pp. 4445–4448. [Google Scholar]
- Cioi, D.; Kale, A.; Burdea, G.; Engsberg, J.; Janes, W.; Ross, S. Ankle control and strength training for children with cerebral palsy using the Rutgers Ankle CP: A case study. In Proceedings of the IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 27 June–1 July 2011. [Google Scholar]
- Diot, C.M.; Thomas, R.L.; Raess, L.; Wrightson, J.G.; Condliffe, E.G. Robotic lower extremity exoskeleton use in a non-ambulatory child with cerebral palsy: A case study. Disabil. Rehabil. Assist. Technol. 2021, 1–5. [Google Scholar] [CrossRef]
- Lerner, Z.F.; Gasparri, G.M.; Bair, M.O.; Lawson, J.L.; Luque, J.; Harvey, T.A.; Lerner, A.T. An Untethered Ankle Exoskeleton Improves Walking Economy in a Pilot Study of Individuals with Cerebral Palsy. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 1985–1993. [Google Scholar] [CrossRef]
- Lerner, Z.F.; Harvey, T.A.; Lawson, J.L. A Battery-Powered Ankle Exoskeleton Improves Gait Mechanics in a Feasibility Study of Individuals with Cerebral Palsy. Ann. Biomed. Eng. 2019, 47, 1345–1356. [Google Scholar] [CrossRef]
- Lerner, Z.F.; Damiano, D.L.; Park, H.-S.; Gravunder, A.J.; Bulea, T.C. A Robotic Exoskeleton for Treatment of Crouch Gait in Children with Cerebral Palsy: Design and Initial Application. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 650–659. [Google Scholar] [CrossRef]
- Park, J.-H.; You, J.H. Innovative robotic hippotherapy improves postural muscle size and postural stability during the quiet stance and gait initiation in a child with cerebral palsy: A single case study. NeuroRehabilitation 2018, 42, 247–253. [Google Scholar] [CrossRef]
- Meyer-Heim, A.; Ammann-Reiffer, C.; Schmartz, A.; Schäfer, J.; Sennhauser, F.H.; Heinen, F.; Knecht, B.; Dabrowski, E.; Borggraefe, I. Improvement of walking abilities after robotic-assisted locomotion training in children with cerebral palsy. Arch. Dis. Child. 2009, 94, 615–620. [Google Scholar] [CrossRef] [Green Version]
- Schroeder, A.S.; Homburg, M.; Warken, B.; Auffermann, H.; Koerte, I.; Berweck, S.; Jahn, K.; Heinen, F.; Borggraefe, I. Prospective cohort study to evaluate changes of function, activity and participation in patients with bilateral spastic cerebral palsy after Robot-enhanced repetitive treadmill therapy. Eur. J. Paediatr. Neurol. Off. J. Eur. Paediatr. Neurol. Soc. 2014, 18, 502–510. [Google Scholar] [CrossRef]
- Fang, Y.; Lerner, Z.F. Feasibility of Augmenting Ankle Exoskeleton Walking Performance with Step Length Bio-feedback in Individuals with Cerebral Palsy. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 442–449. [Google Scholar] [CrossRef]
- Sukal-Moulton, T.; Clancy, T.; Zhang, L.Q.; Gaebler-Spira, D. Clinical application of a robotic ankle training pro-gram for cerebral palsy compared to the research laboratory application: Does it translate to practice? Arch. Phys. Med. Rehabil. 2014, 95, 1433–1440. [Google Scholar] [CrossRef] [Green Version]
- Damiano, D.L.; Stanley, C.J.; Ohlrich, L.; Alter, K.E. Task-Specific and Functional Effects of Speed-Focused El-liptical or Motor-Assisted Cycle Training in Children with Bilateral Cerebral Palsy: Randomized Clinical Trial. Neurorehabilit. Neural Repair 2017, 31, 736–745. [Google Scholar] [CrossRef]
- Matsuda, M.; Iwasaki, N.; Mataki, Y.; Mutsuzaki, H.; Yoshikawa, K.; Takahashi, K.; Enomoto, K.; Sano, K.; Kubota, A.; Nakayama, T.; et al. Robot-assisted training using Hybrid Assistive Limb® for cerebral palsy. Brain Dev. 2018, 40, 642–648. [Google Scholar] [CrossRef]
- Chen, K.; Ren, Y.; Gaebler-Spira, D.; Zhang, L.Q. Home-based tele-assisted robotic rehabilitation of joint impair-ments in children with cerebral palsy. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 5288–5291. [Google Scholar]
- Wu, Y.-N.; Hwang, M.; Ren, Y.; Gaebler-Spira, D.; Zhang, L.-Q. Combined Passive Stretching and Active Movement Rehabilitation of Lower-Limb Impairments in Children with Cerebral Palsy Using a Portable Robot. Neurorehabilit. Neural Repair 2011, 25, 378–385. [Google Scholar] [CrossRef]
- Lee, S.J.; Jin, D.; Kang, S.H.; Gaebler-Spira, D.; Zhang, L.Q. Combined ankle/knee stretching and pivoting stepping training for children with cerebral palsy. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 1743–1752. [Google Scholar] [CrossRef]
- Mehrholz, J.; Thomas, S.; Kugler, J.; Pohl, M.; Elsner, B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst. Rev. 2020, 10, CD006185. [Google Scholar]
- Morrissey, K.; Fairbrother, H. Severe Traumatic Brain Injury in Children: An Evidence-Based Review of Emergency Department Management. Pediatr. Emerg. Med. Pr. 2016, 13, 1–28. [Google Scholar]
- Iosa, M.; Morone, G.; Cherubini, A.; Paolucci, S. The three laws of neurorobotics: A review on what neurorehabilitation robots should do for patients and clinicians. J. Med. Biol. Eng. 2016, 36, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reyes, F.; Niedzwecki, C.; Gaebler-Spira, D. Technological Advancements in Cerebral Palsy Rehabilitation. Phys. Med. Rehabil. Clin. N. Am. 2020, 31, 117–129. [Google Scholar] [CrossRef] [PubMed]

| Section | Extracted data |
|---|---|
| Population | Study Authors |
| patients included (sample size, age, diagnosis) | |
| study design [observational, pilot multicentre, pilot, RCT, controlled prospective, case series, uncontrolled trial, feasibility study] | |
| Device | presence of CE mark |
| CE class [i, iia, iib] | |
| devices national classification according to the Italian regulatory system | |
| wearability | |
| EE/exo | |
| wearability [0, 1] | |
| environment [real, virtual] | |
| DoFs [nActive + nPassive] | |
| recorded parameters [ROM, force, kinematics] | |
| control system [force, ROM, impedance, EMG] | |
| Treatment | assistance modality |
| feedback modality | |
| difficulty level [fixed, adjustable] | |
| intensity (min/session) | |
| duration | |
| number of sessions per day | |
| rehabilitation aim |
| Total | ||
|---|---|---|
| Included studies | Total | 31 |
| RCT n° (%) | 10 (32%) | |
| other n° (%) | 21 (68%) | |
| Population * | ABI/TBI/SCI/PNI/CP/D | 1/1/1/1/29/1 |
| Devices | total (CE mark) | 16 (4) |
| EE/Exo | 8/8 | |
| Treatment | interactive | 12 |
| assistive | 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valè, N.; Gandolfi, M.; Vignoli, L.; Botticelli, A.; Posteraro, F.; Morone, G.; Dell’Orco, A.; Dimitrova, E.; Gervasoni, E.; Goffredo, M.; et al. Electromechanical and Robotic Devices for Gait and Balance Rehabilitation of Children with Neurological Disability: A Systematic Review. Appl. Sci. 2021, 11, 12061. https://doi.org/10.3390/app112412061
Valè N, Gandolfi M, Vignoli L, Botticelli A, Posteraro F, Morone G, Dell’Orco A, Dimitrova E, Gervasoni E, Goffredo M, et al. Electromechanical and Robotic Devices for Gait and Balance Rehabilitation of Children with Neurological Disability: A Systematic Review. Applied Sciences. 2021; 11(24):12061. https://doi.org/10.3390/app112412061
Chicago/Turabian StyleValè, Nicola, Marialuisa Gandolfi, Laura Vignoli, Anita Botticelli, Federico Posteraro, Giovanni Morone, Antonella Dell’Orco, Eleonora Dimitrova, Elisa Gervasoni, Michela Goffredo, and et al. 2021. "Electromechanical and Robotic Devices for Gait and Balance Rehabilitation of Children with Neurological Disability: A Systematic Review" Applied Sciences 11, no. 24: 12061. https://doi.org/10.3390/app112412061
APA StyleValè, N., Gandolfi, M., Vignoli, L., Botticelli, A., Posteraro, F., Morone, G., Dell’Orco, A., Dimitrova, E., Gervasoni, E., Goffredo, M., Zenzeri, J., Antonini, A., Daniele, C., Benanti, P., Boldrini, P., Bonaiuti, D., Castelli, E., Draicchio, F., Falabella, V., ... Italian Consensus Conference on Robotic in Neurorehabilitation CICERONE. (2021). Electromechanical and Robotic Devices for Gait and Balance Rehabilitation of Children with Neurological Disability: A Systematic Review. Applied Sciences, 11(24), 12061. https://doi.org/10.3390/app112412061