Abstract
Objective: The purpose of this retrospective preliminary study was to analyze the skeletal and dentoalveolar effects of a new clear functional appliance in a sample of patients close to growth spurt with class II malocclusion attributable to mandibular retrusion. Materials and methods: A sample of growing patients underwent functional Class II correction using F22® (Sweden and Martina, Due Carrare (PD), Italy) Young, realized combining the aesthetic characteristics of the F22® clear aligner with the structural features of a functional appliance. For each patient, a digital setup was performed by a single operator to plan a mandibular advancement to the therapeutic position. Cephalometric analysis before and after treatment was performed. The purpose of the statistical analysis was to evaluate dental and skeletal changes associated with F22® Young device, and whether there were statistically significant differences in anatomical measurements between the beginning and end of treatment. Results: 15 patients, 7 females and 8 males of average age 10.3, were treated with the F22® Young appliance for an average period of 10 months ± 0.5 (maximum 11.5 months, minimum 10.5 months). The data showed that the SNB angle increase was statistically significant from T0 to T1, leading to a reduction in the ANB angle. Values for the mandible length, both total (Co-Gn) and at the base (Go-Pg), significantly increased. Conclusions: According to this preliminary study, F22® Young appliance is effective in promoting mandibular advancement when used near the pubertal growth peak. The device is comfortable and aesthetic, which certainly promoted patient compliance, a key factor for treatment success.
1. Introduction
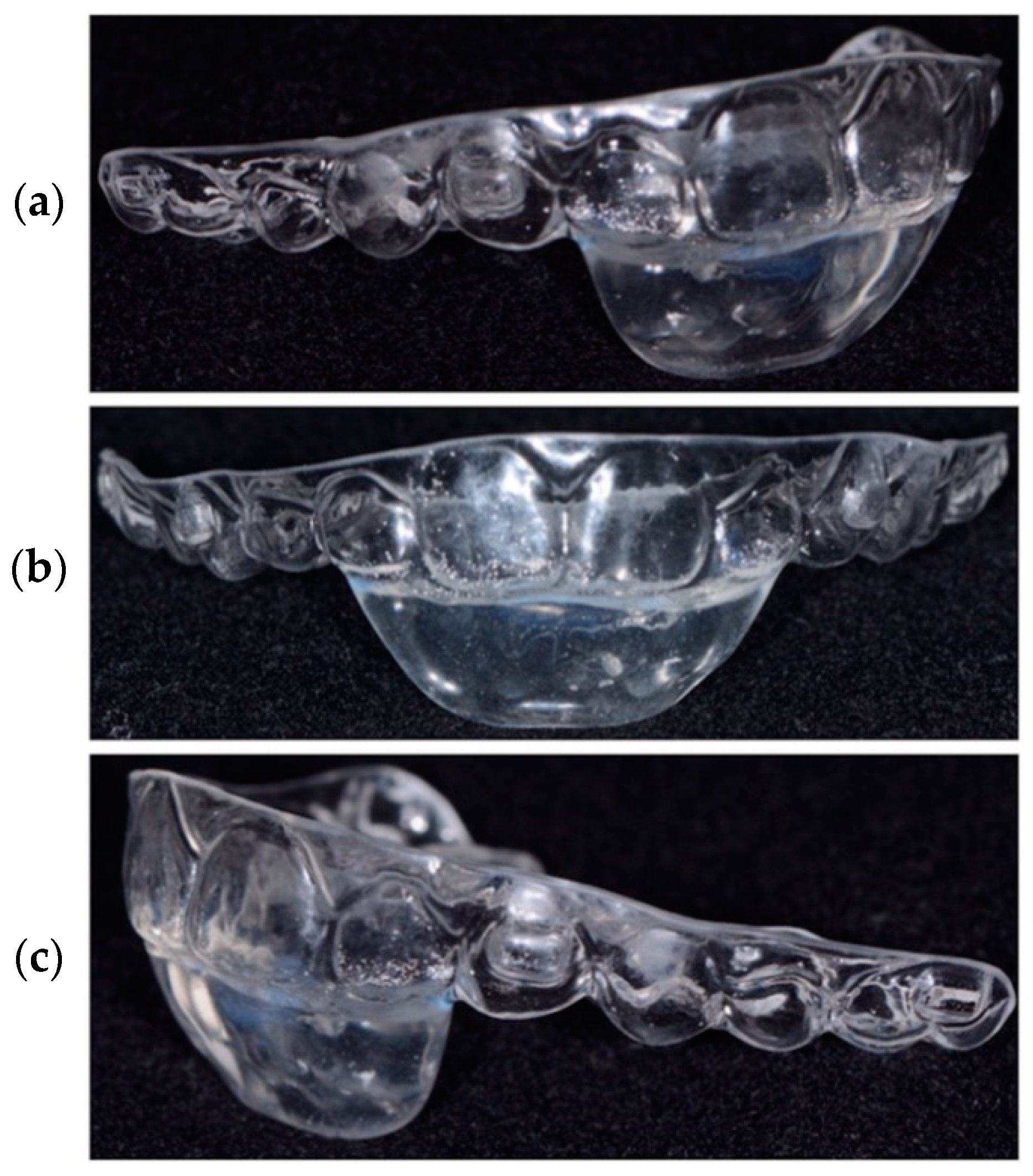
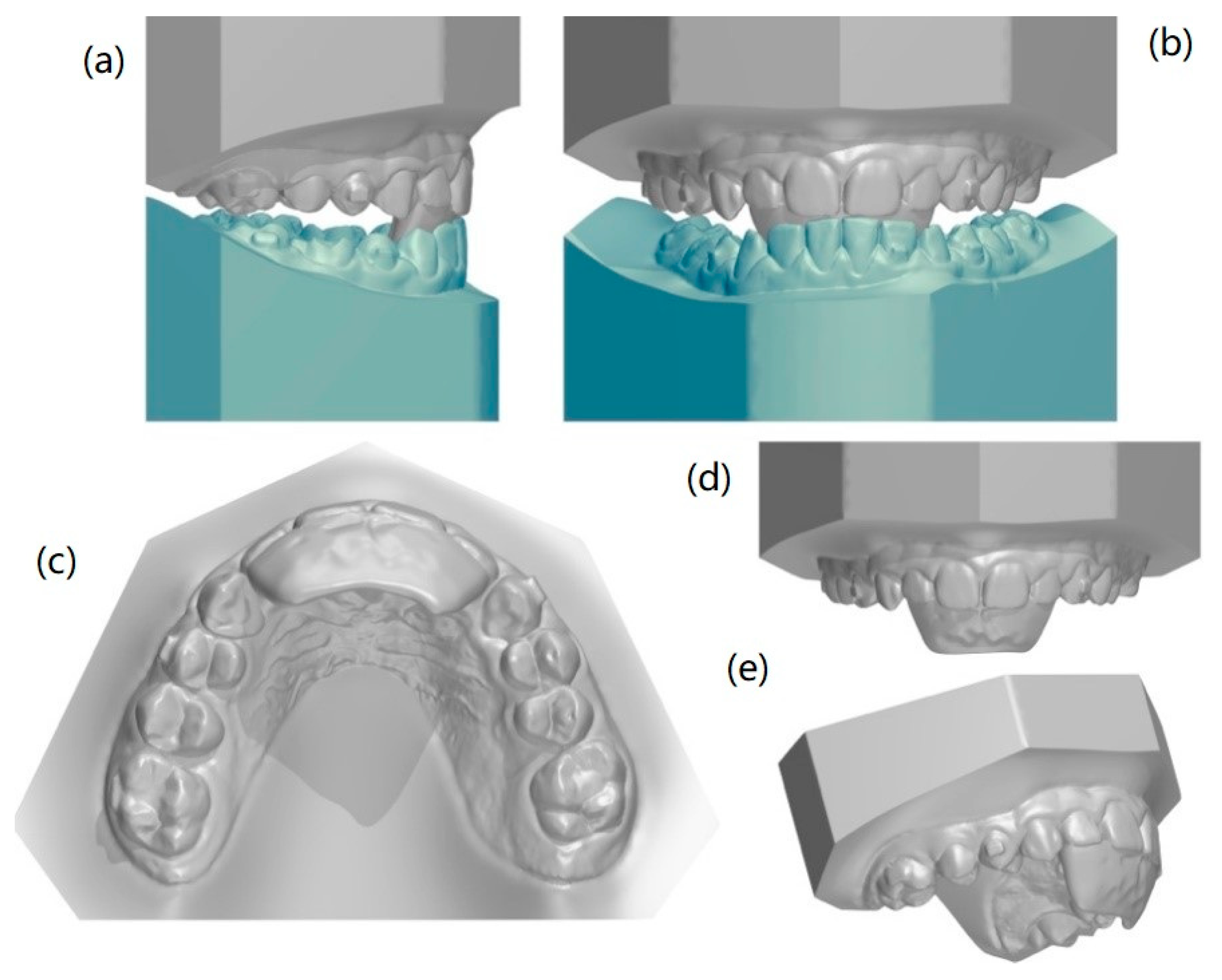
Skeletal class II is a widespread malocclusion in the population, and it can appear with a wide variety of dental and skeletal configurations. A 1981 study by McNamara [1] with a sample of 277 children of both sexes aged 8–10 showed that mandibular retrusion is the most common finding in such class II malocclusion patients. The development of a class II malocclusion may be associated with a deficit of the maxillary transversal dimension, as demonstrated by Tollaro et al. [2]. In subjects with class II, mandibular growth is slower and limited compared to controls, and dentoskeletal disharmony unlikely self-correct with age. Rapid expansion can improve the parameters of a class II malocclusion reducing the interference factor preventing the lower jaw from growing forward. For this reason, functional equipment, removable or fixed, is widely used in growing patients, with the aim of stimulating and guiding growth towards a proper jaw relationship [3,4]. The Twin Block device is one of the most studied functional appliances, and its dental, skeletal and soft tissue effects are amply described in the literature [5]. It was designed by Clark in 1982, and its widespread use is favoured by its high acceptability and ability to be effective rapidly over time [6]. However, the aesthetic demands of pre-teen and adolescent patients have increased exponentially in recent years. As early as 5 years of age, children are able to distinguish between different types of smiles, and from the age of 8 the adults aesthetic canons are already largely consolidated [7]. To increase greater patient compliance with removable equipment, efforts have been made to improve the comfort and aesthetics of removable devices. This has led to the development of F22® Young, a device, designed and manufactured at the Postgraduate School of Orthodontics, University of Ferrara (Figure 1a–c) which has the advantage of the aesthetic characteristics of clear aligners but at the same time overcomes their limits in providing orthopaedic effects [8,9]. This upper advancement aligner is realized using repeatable methods and based on careful planning (Figure 2a–e).
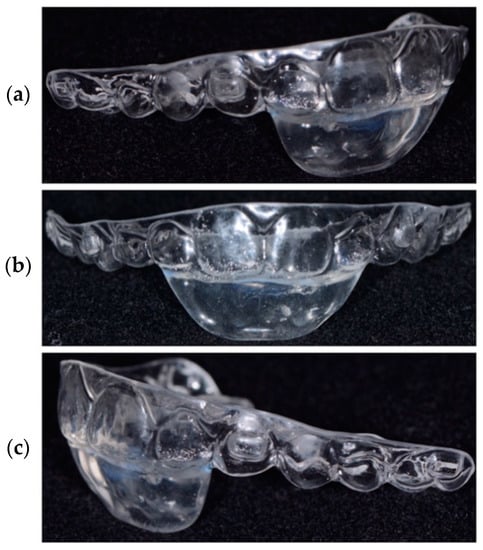
Figure 1.
(a–c) F22 Young.
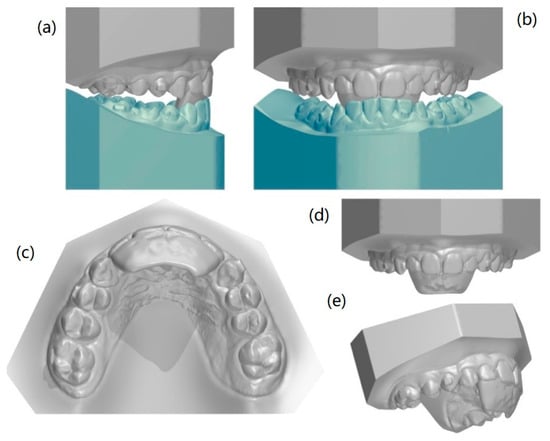
Figure 2.
(a–e) Digital planning of F22 Young treatment.
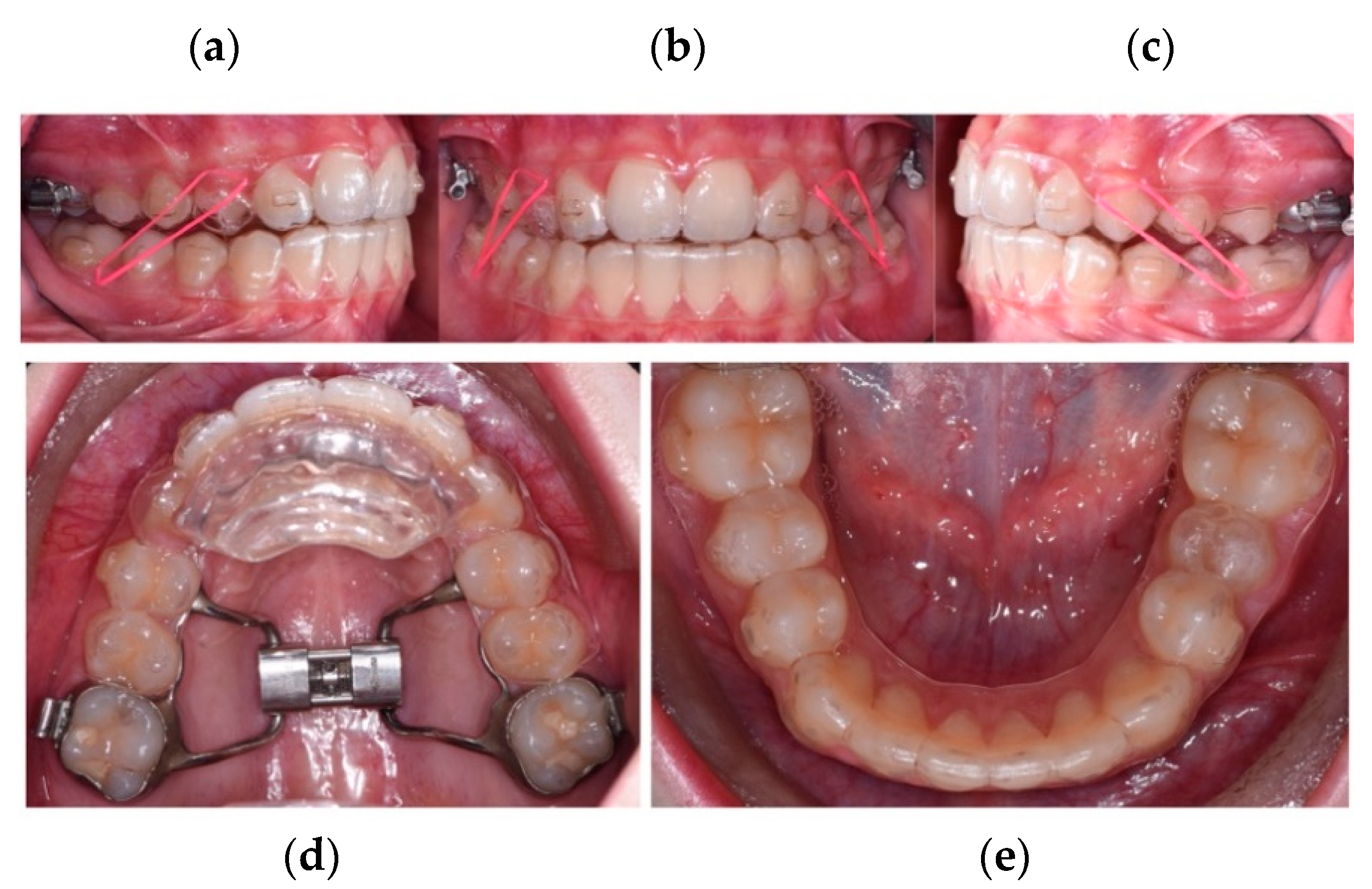
Its main feature is a customizable “block” behind the upper incisors designed to fit behind the lower aligner, push the mandible forward and consequently drive its advancement. The appliance is highly versatile, and can be used in conjunction with auxiliaries such as class II elastics, rapid palatal expansion or extraoral traction (Figure 3a–e). The purpose of this retrospective preliminary study was to analyze the skeletal and dentoalveolar effects of F22® Young in a sample of patients close to growth spurt with class II malocclusion ascribable to mandibular retrusion.
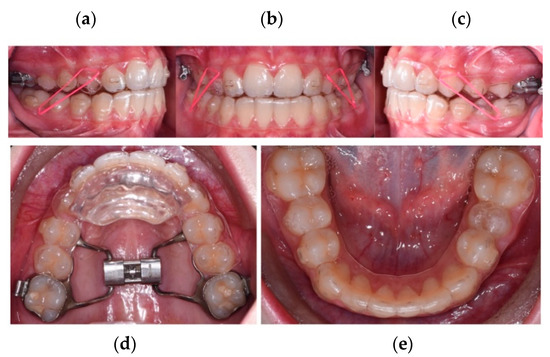
Figure 3.
(a–e) Rapid palatal expander (RPE) and class II elastics used simultaneously with F22 Young.
2. Materials and Methods
A sample of patients underwent functional class II correction using F22® (Sweden and Martina, Due Carrare (PD), Italy) Young [10]. They all met the following inclusion criteria: mixed dentition; CSV3-CSV4 cervical vertebral stage maturation according to Baccetti et al. [1]; Class II skeletal malocclusion characterized by mandibular retrusion (SNB < 78° and ANB > 4°), full class II or head-to-head sagittal molar relationship, with OJ < 10 mm, normo- or hypodivergent growth pattern (FMA < 27°). All patients underwent a rapid palatal expansion to have a normalization of transversal diameters before starting the mandibular advancement.
The following records were collected for each patient at T0 (at the start of mandibular advancement, at the RPE removal) and T1 (at the end of the active functional treatment): intra- and extraoral photographs, panoramic radiographs, laterolateral radiography and digital models.
For each patient, a digital setup was elaborated by a single operator (F.Cr.) to plan both the first phase, alignment of the incisor group, and the second phase, mandibular advancement to the desired position, i.e., hypercorrection of the molar class and normalization of the overjet. For each patient, all the advancement was planned in a single step, thanks to a customized anterior block, with different height and inclination, depending on individual occlusal characteristics and different need of posterior disclusion.
All patients were given the same instructions for active functional therapy, namely the use of the upper advancement aligner associated with a lower prescription aligner for 15 h/day, and 6-oz Impala Class II elastics (Ormco Corporation, Orange, CA, USA) to be used on special notches made on the aligners and worn at night. Elastics were worn also by night to ensure a correct positioning all day long, and to counteract the potential detrimental effects of habits such as mouth breathing. Laterolateral radiography before and after treatment were performed using a Carestream® digital machine (Carestream Health Inc., New York, NY, USA), with an effective dose in a range of 2,2–3,4 uSv.
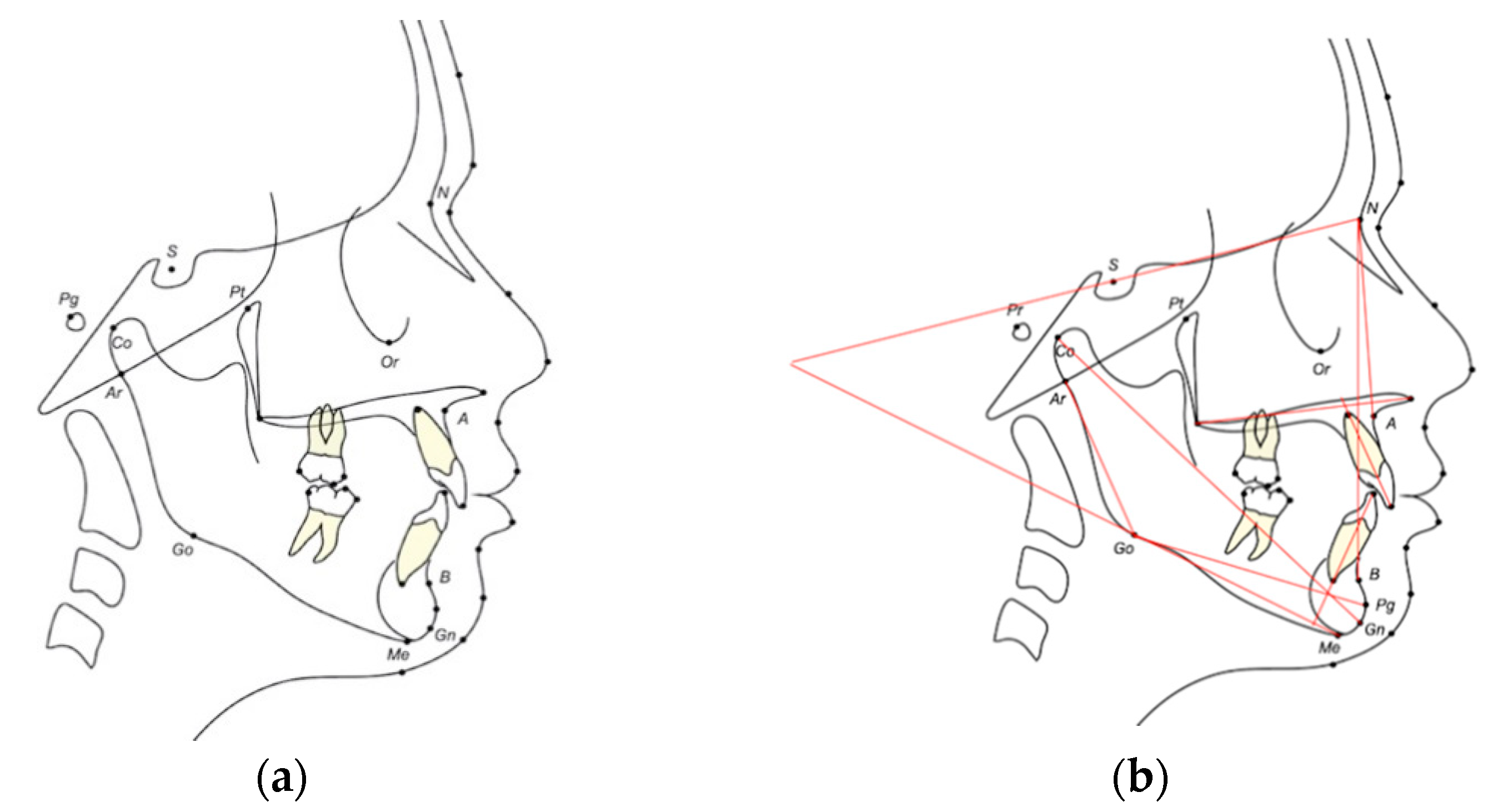
Cephalometric analysis of T0 and T1 teleradiographs were performed three times by the same operator using Dolphin Imaging Software (Dolphin Imaging and Management Solutions, Chatsworth, CA, USA), maintaining a standard magnification of 1:1. The three cephalometric tracings performed on each x-ray were made seven days apart, in order to prevent the influence of memory of the previous tracing. The same procedure was used to measure the digital models using 3Shape Ortho Analyzer ™ software (3Shape A/S, Copenhagen, Denmark). Data for the twelve angular and three linear measurements made on the cephalometric tracings (Figure 4a,b), in addition to three linear measurements made on the digital models (Figure 5), are presented in Table 1, Table 2 and Table 3. The three sets of repeated measures made by the same operator were entered into an Excel spreadsheet and analysed statistically.
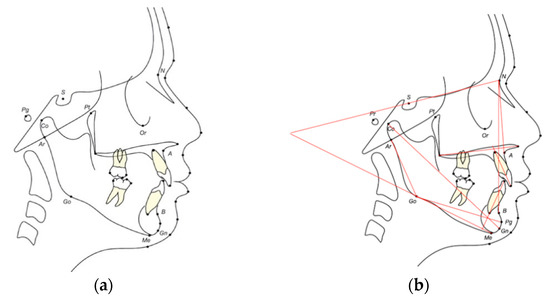
Figure 4.
(a) Reference points for the cephalometric analysis; (b) Angular and linear measurements in the cephalometric analysis.
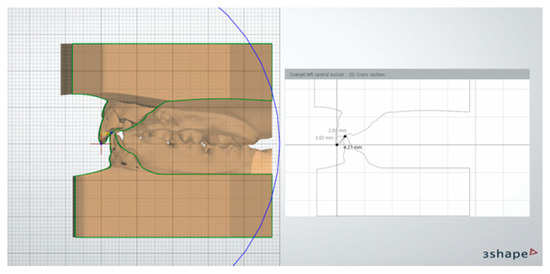
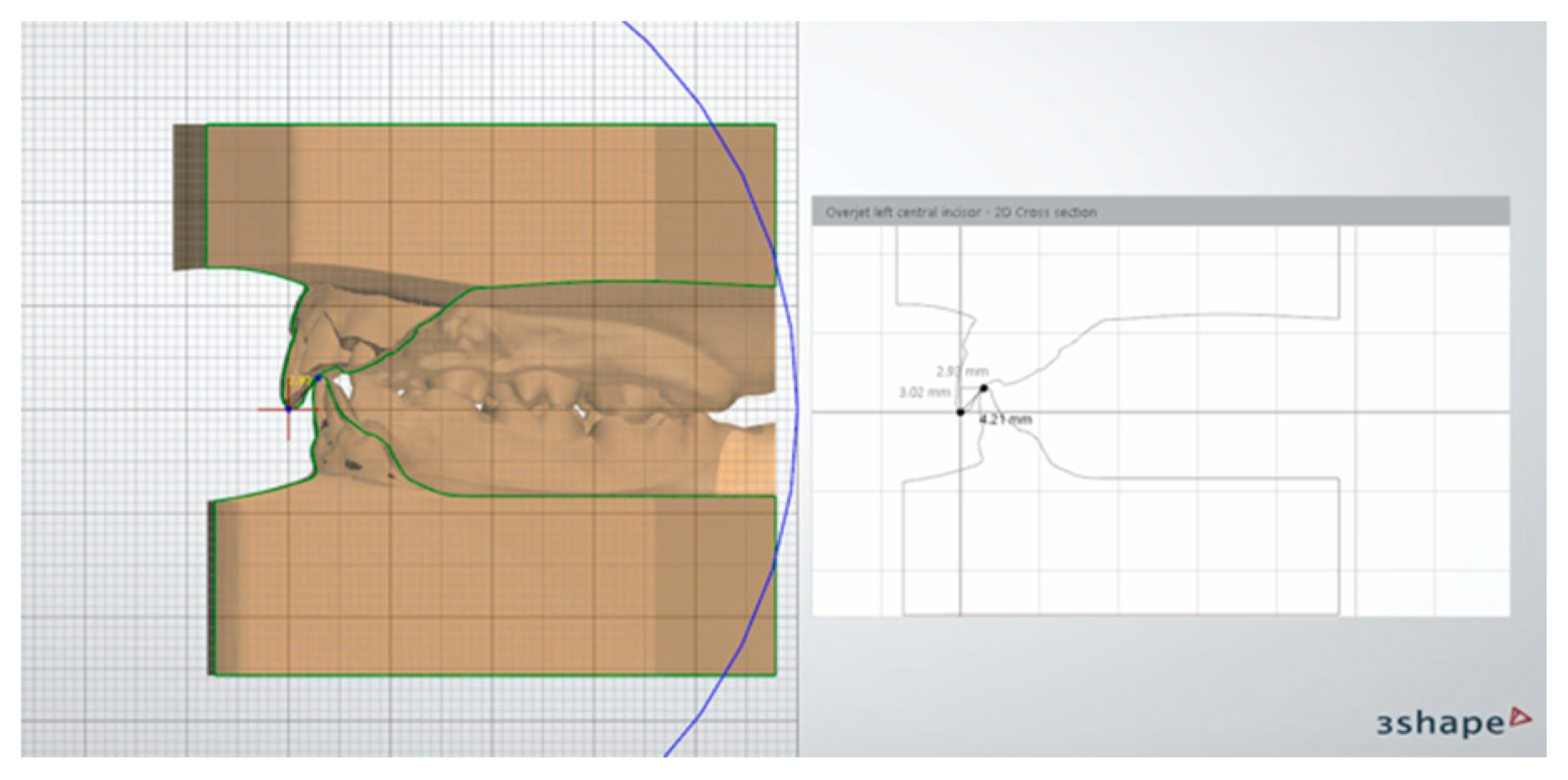
Figure 5.
Linear measurements (for example, overjet and overbite) were made on digital models using 3Shape Ortho Analyzer ™ software (3Shape A/S • Holmens Kanal 7, 4. 1060 Copenhagen, Denmark).

Table 1.
Angular cephalometric values measured on the teleradiography of the skull in a lateral-lateral projection.
Table 2.
Linear cephalometric values measured on the teleradiography of the skull in a lateral-lateral projection.
Table 3.
Linear values measured on digital models.
The study design was approved by the Ethics Committee of the Ferrara University Postgraduate School of Orthodontics (Via Luigi Borsari 46, Ferrara, Italy; approval number 6/2019).
3. Statistical Analysis
The purpose of the statistical analysis carried out was to evaluate the dental and skeletal changes associated with use of the F22®. Young device, and whether there were statistically significant differences in anatomical measurements between the beginning and end of treatment. Each measurement was repeated three times to ensure that the results were repeatable, making a total of 45 T0 measurements and 45 T1 measurements.
The statistical analysis was carried out using a t-test for paired data, via R Statistical software (R Core Team 2018), to highlight differences between T0 and T1 values. Given the sample size, a significance level of was set, at which the analysis should be able to identify an effect size of dz = 0.675 between average and large thresholds (0.5–0.8) according to Sawiloski.
The measurement error, in terms of repeatability, was estimated using the intra-class correlation (ICC) index.
4. Results
15 patients, 7 females and 8 males of average age 10.3 ± 1.8, were treated with the F22® Young appliance by the same operator (F.Cr.) at the Postgraduate School of Orthodontics, University of Ferrara, for an average period of 10 months ± 0.5 (maximum 11.5 months, minimum 10.5 months). According to Baccetti et al. [8] CSV3 stage was valued in 10 patients (5 F, 5 M) and CS4 stage in 5 patients (2 F, 3 M). All measurements taken (18 in total) were repeated three times in order to calculate the intra-class correlation (ICC) index, and then estimate the average measurement error. As shown in Table 4, all outcomes had an ICC index > 0.94, indicative of excellent sample repeatability.
Table 4.
Statistical repeatability analysis. ICC index report for each outcome.
Table 5 shows all the synthesized values, with the pre- and post-treatment averages found, along with the standard deviation and significant statistics according to the t-test applied. The statistical analysis was carried out and revealed significant differences between some pre- and post-treatment values but not for others. For each outcome, a bivariate graph was constructed according to the formula:
Table 5.
Descriptive information (mean/standard deviation for each value) at T0 and T1, and relative statistical significance (p < 0.05 *).
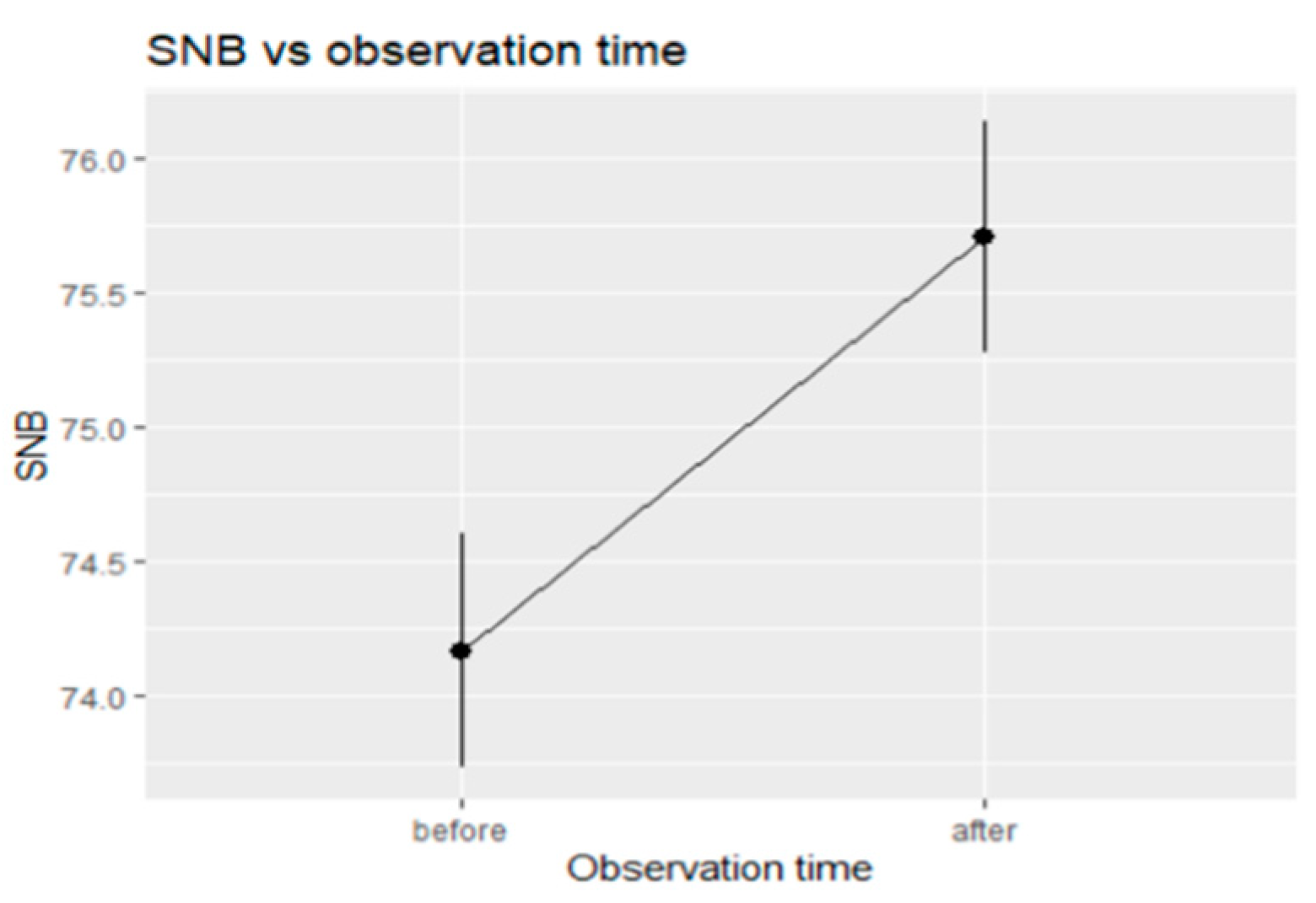
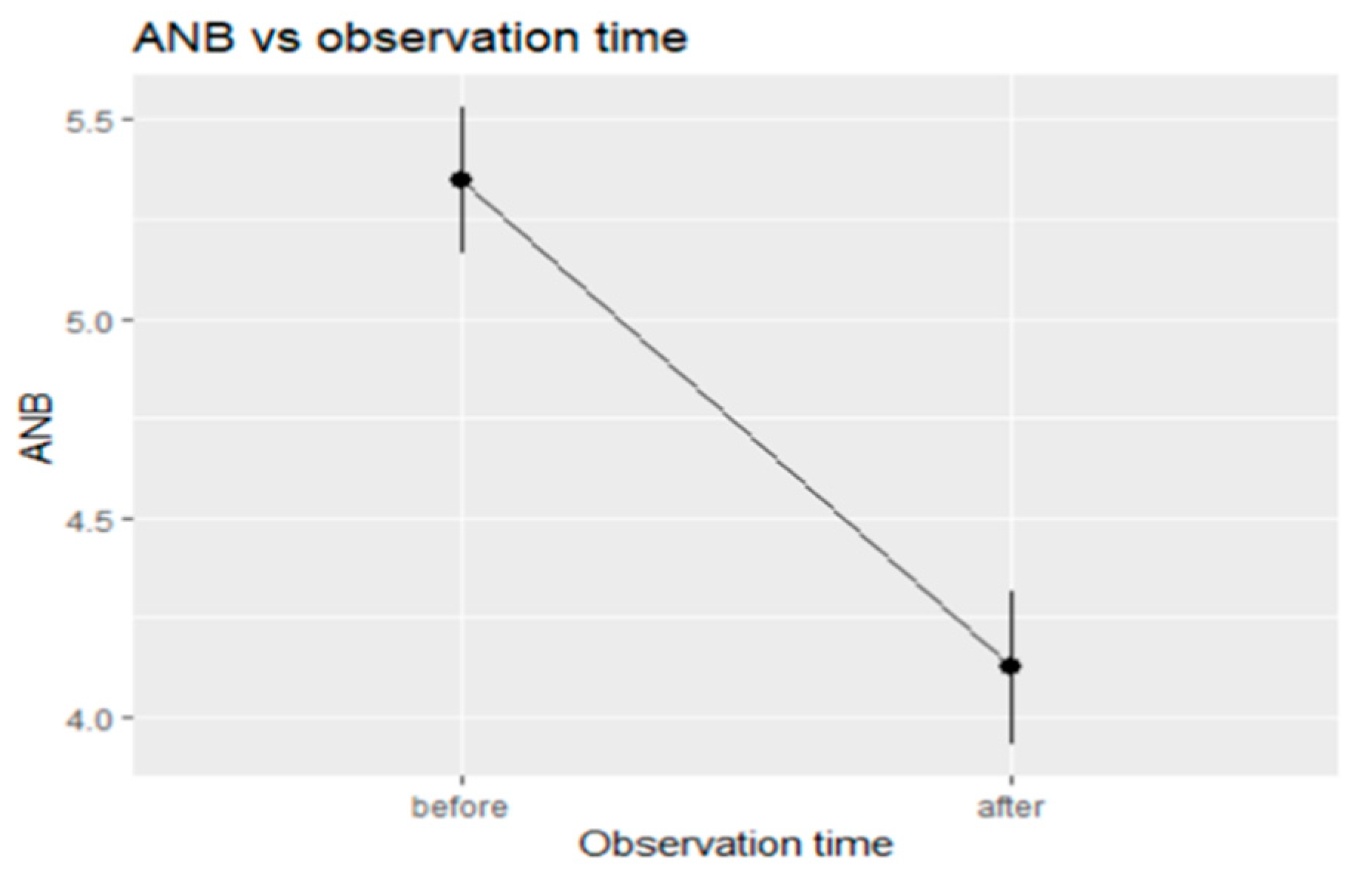
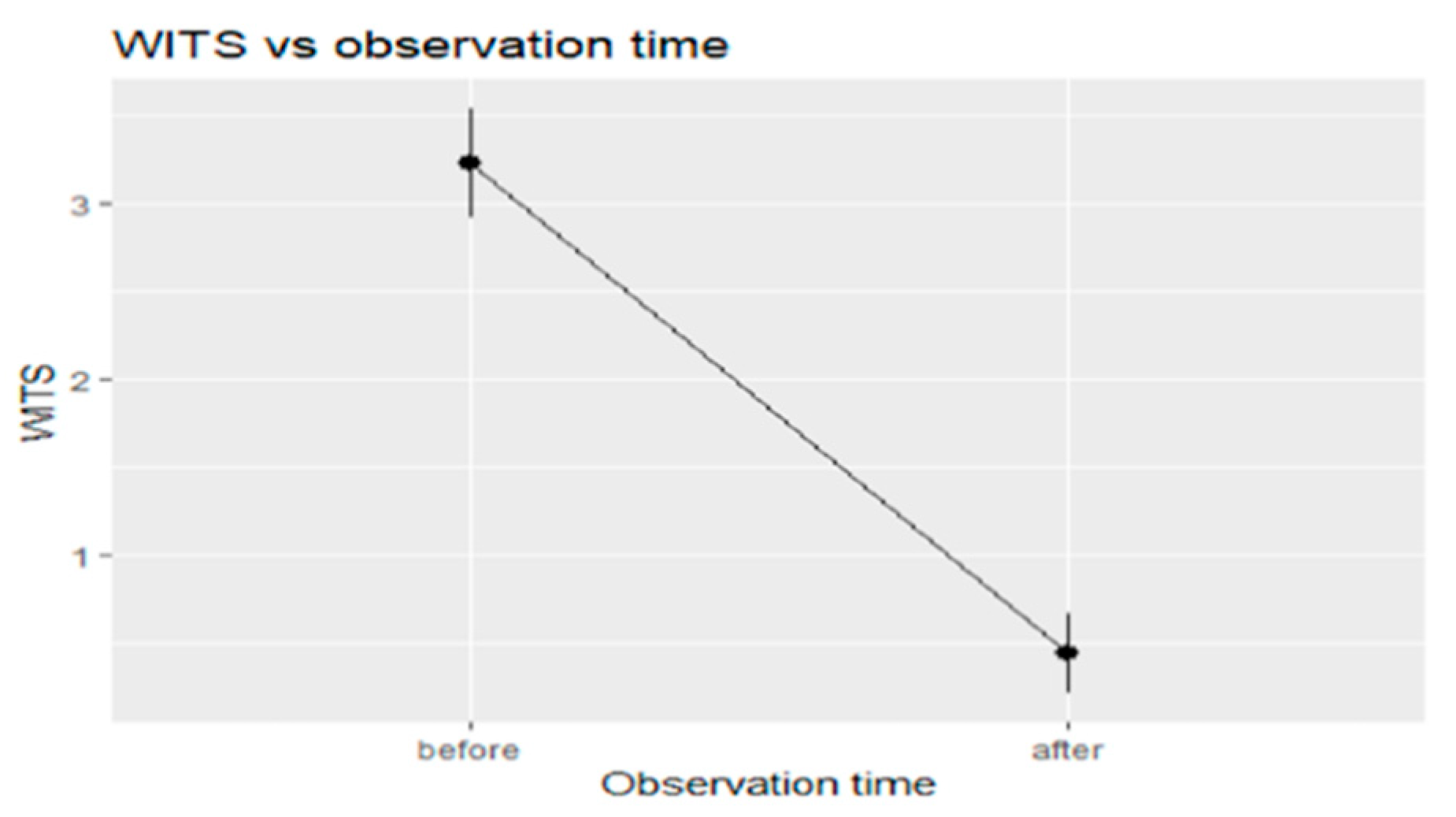
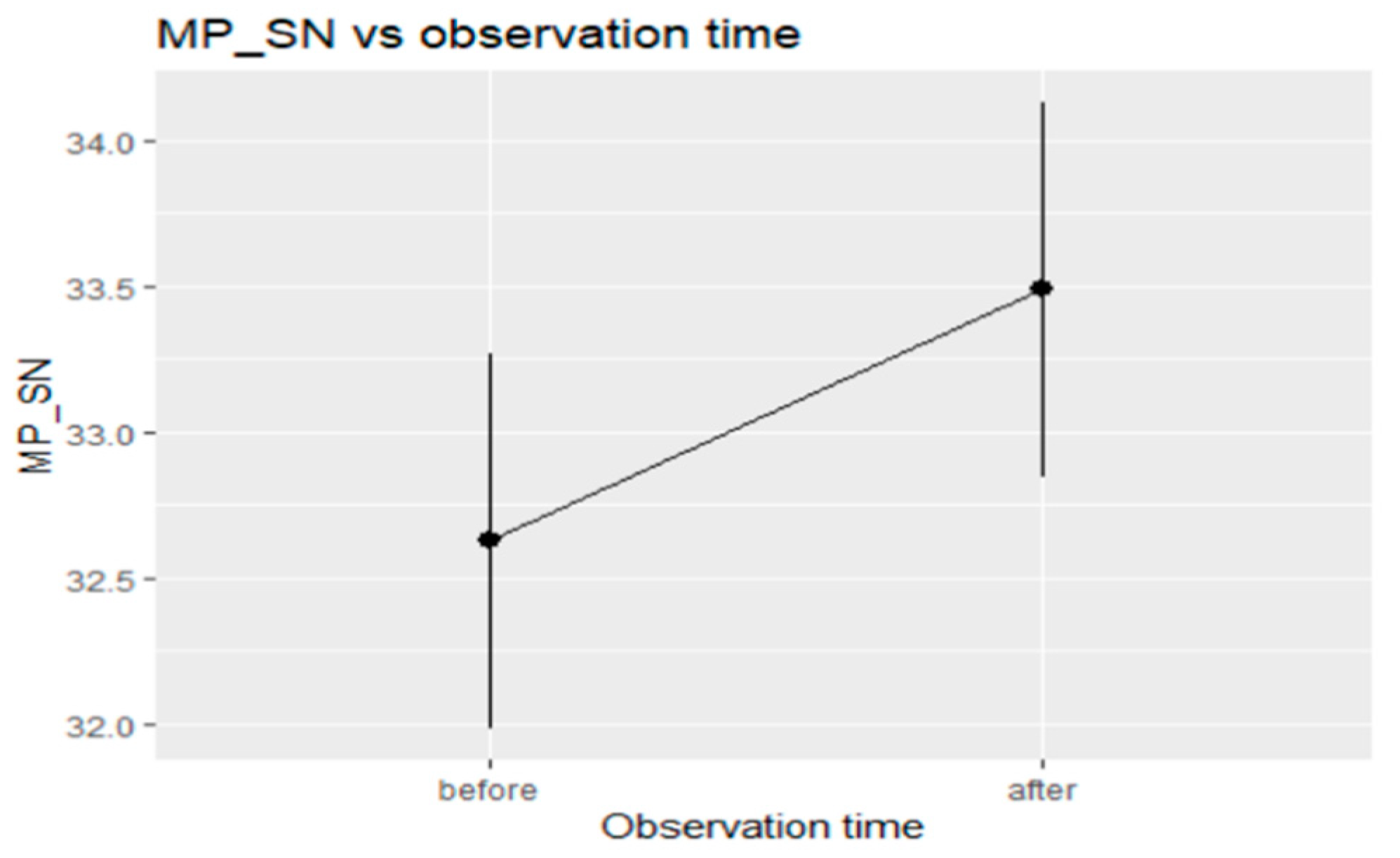
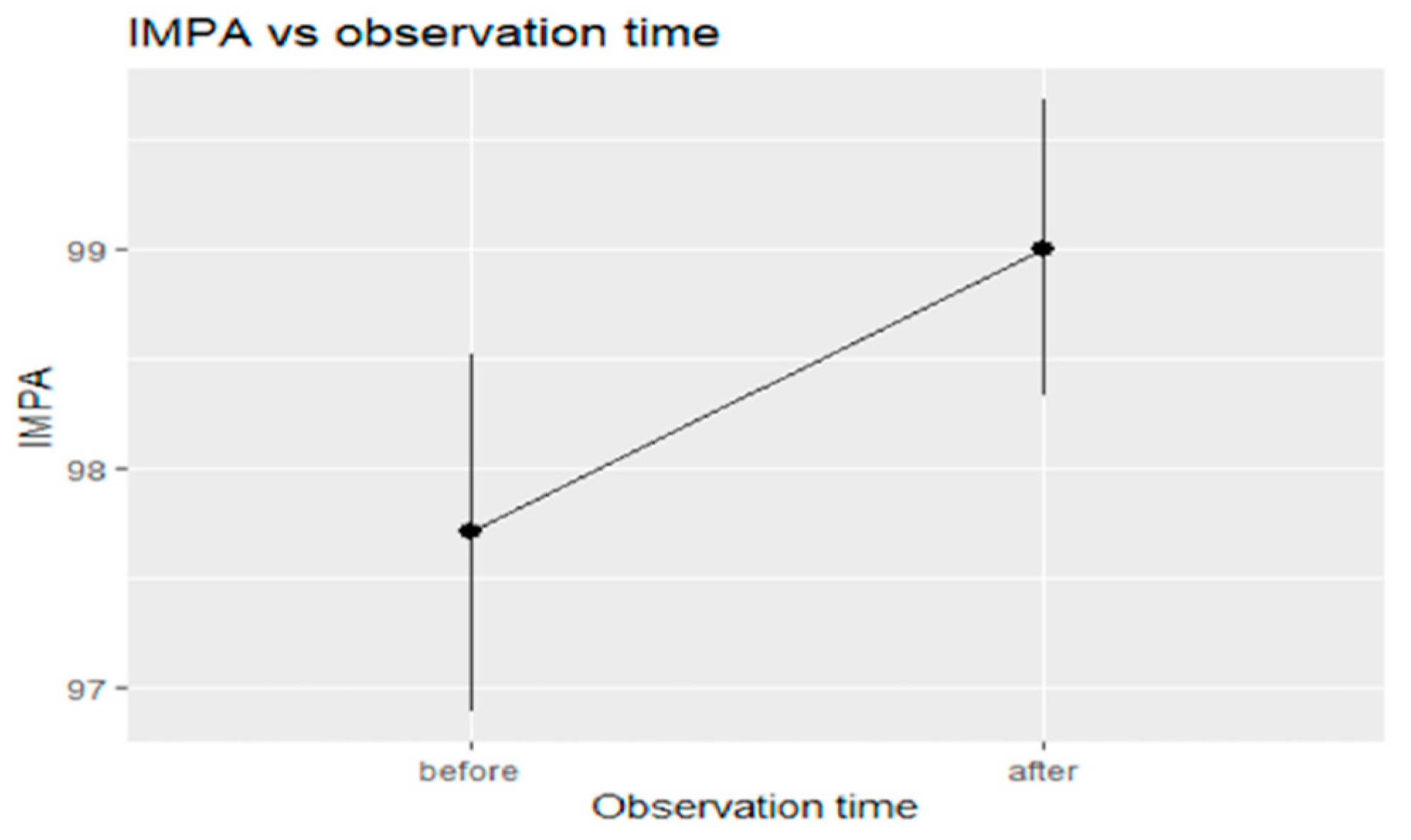
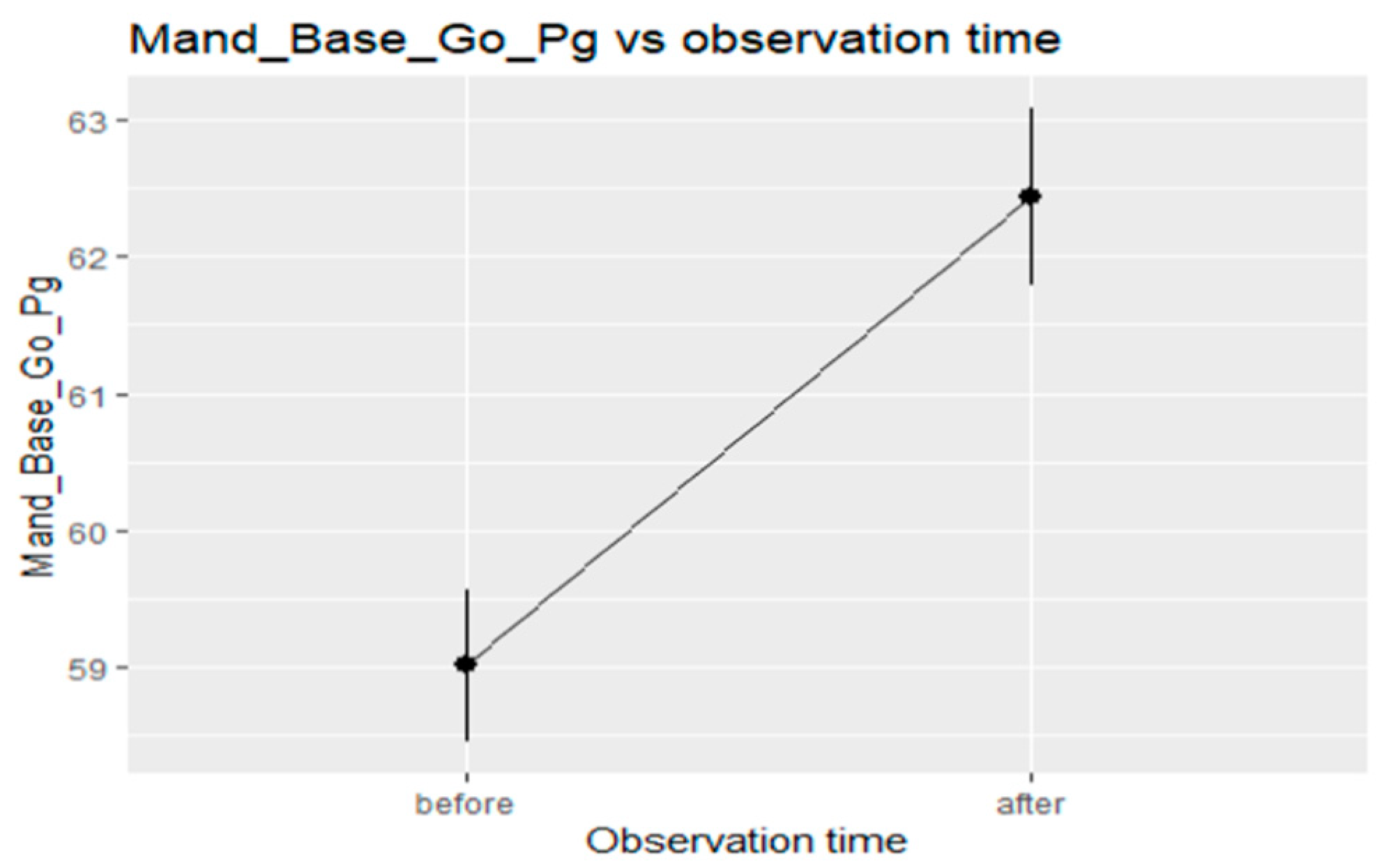
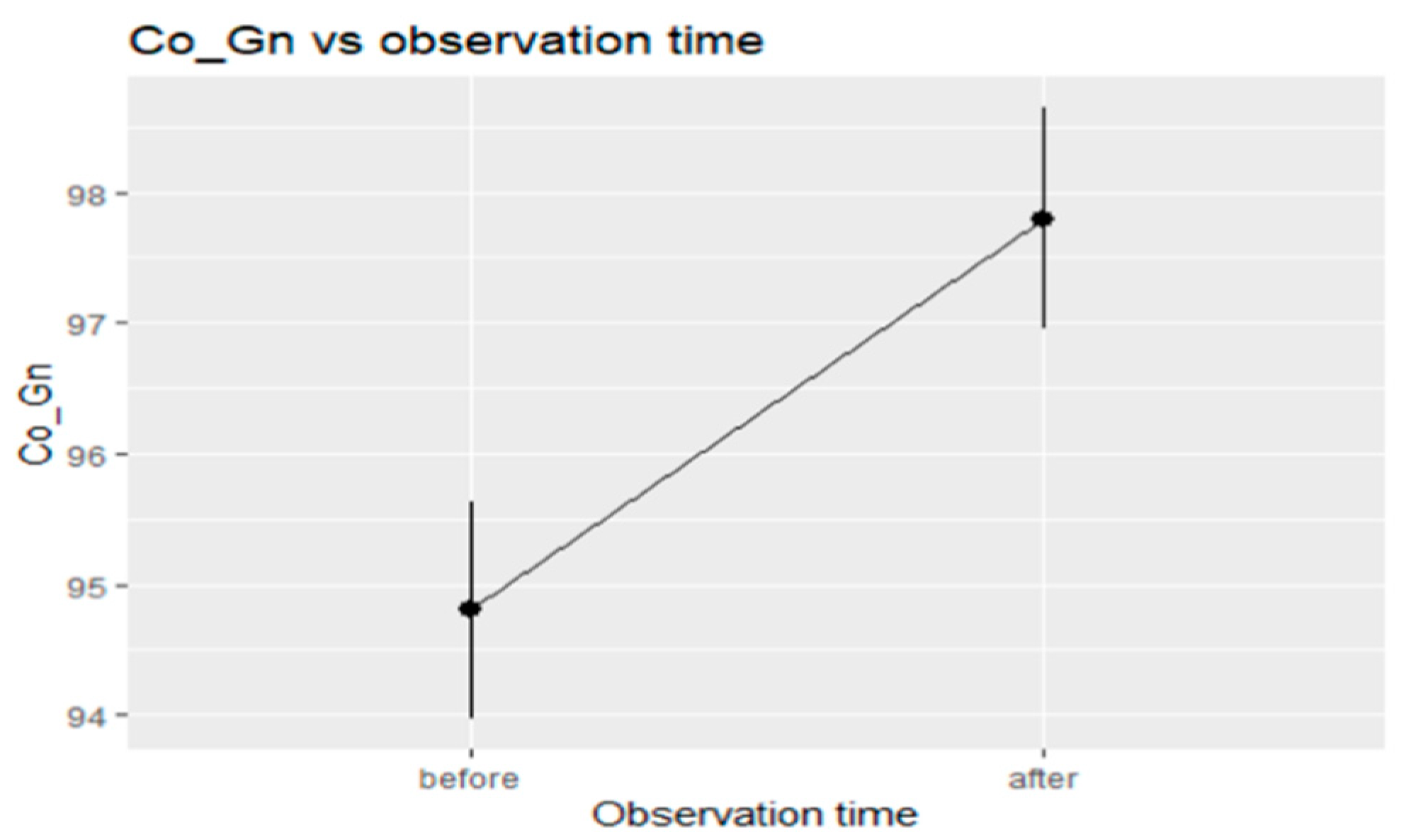
The data showed that SNB angle increased statistically significantly from T0 to T1 (Figure 6), leading to a reduction in the ANB angle (Figure 7). Point B advanced significantly, resulting in a reduction in the sagittal skeletal discrepancy between the upper and lower jaws. The distance on the occlusal plane between points A and B also decreased significantly (Figure 8), and there was a weakly statistically significant increase in the MP-SN angle as a result of F22® Young treatment (Figure 9). The FMA angle, on the other hand, remained almost unchanged. As for the inclination of the incisors with respect to their skeletal base, there was a significant increase in the angle formed by the long axis through the lower incisor and the mandibular plane (IMPA) (Figure 10), but not of the angle formed by the upper incisor long axis and the bispinal plane, which was reduced by less than 1° as compared to the beginning of treatment (U1-PP). Finally, values for the mandible length, both total (Co-Gn) and at the base (Go-Pg), significantly increased as a result of treatment with the F22® Young appliance (Figure 11 and Figure 12). With regard to the linear measurements obtained from analysis of the digital models, both the overjet and the overbite were significantly reduced, falling within normal ranges at T1. The molar class, measured as the distance between an axis passing through the vestibular groove on the lower first molar and the axis passing through the top of the mesiovestibular cusp on the upper first molar, also considerably decreased from T0 to T1, reaching values closer to 0 on both sides.
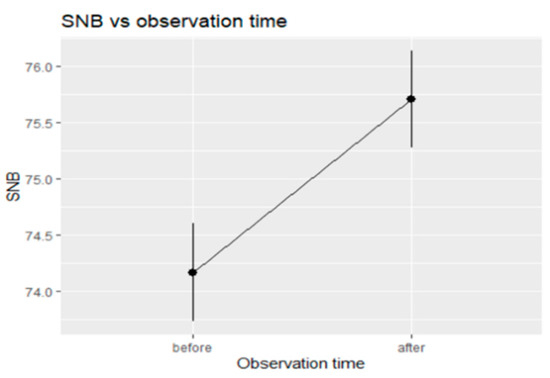
Figure 6.
Trend in SNB over time from T0 to T1.
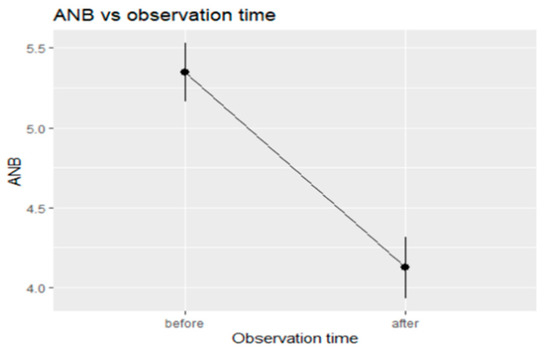
Figure 7.
Trend in ANB over time from T0 to T1.
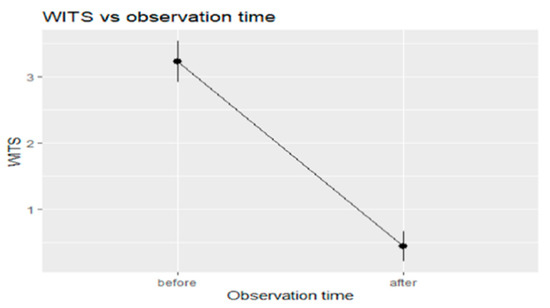
Figure 8.
Trend in Wits appraisal over time from T0 to T1.
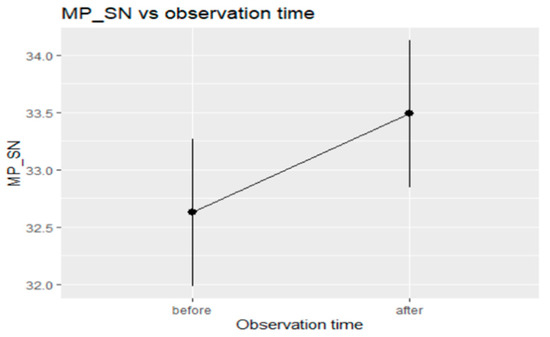
Figure 9.
Trend in MP-SN over time from T0 to T1.
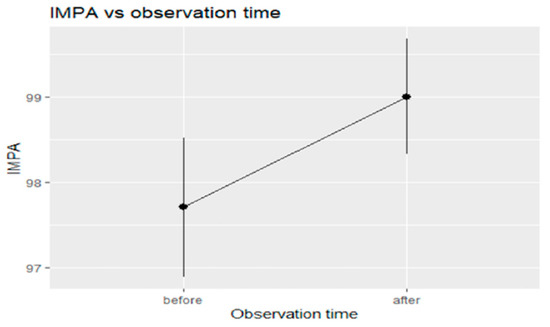
Figure 10.
Trend in IMPA over time from T0 to T1.
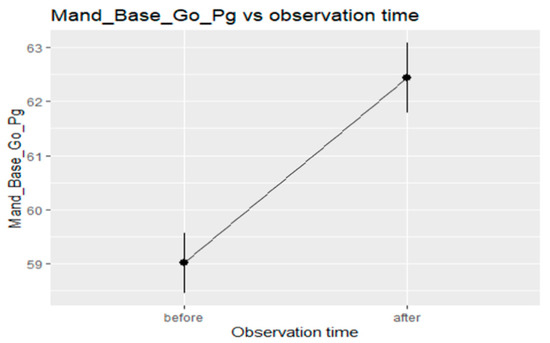
Figure 11.
Trend in Go-Pg over time from T0 to T1.
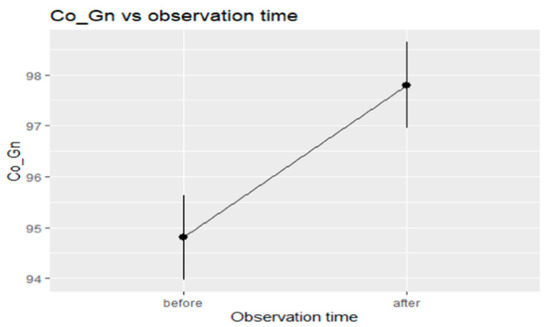
Figure 12.
Trend in Co-Gn over time from T0 to T1.
5. Discussion
Functional treatment of growing patients with class II malocclusion can lead to significant skeletal and dentoalveolar changes when carried out near the peak of growth. This study shows the results of treatment with F22®. Young for the correction of class II malocclusion in a group of patients at stage CSV3–CSV4. Before treatment, the 15 patients had an average age of 10.3 years, but were highly compliant, wearing the device for 15/20 h per day for an average total period of 10 months ± 0.5 (maximum 11.5 months, minimum 10.5 months). Even if it’s possible to start the mandibular advancement with RPE still bonded, T0 records were collected after its removal, in order to analyze just the mandibular advancement benefits with normalized transversal diameters. The resulting improvements in overjet and overbite, and the correction of the molar class on both the right and left sides, are indicators of how effective the device is in resolving class II malocclusion, providing significant normalization of dental parameters.
At the level of the upper jaw there were no significant changes; the position of point A remained unchanged, without any alteration in the SNA angle. On this point the literature is controversial. O’Brien et al. [11] found minimal effects of constriction of upper jaw growth after the use of the Twin Block, which is about 13% of the total skeletal changes. Similarly, Illing et al. [12] showed a small reduction in the SNA angle. The stretching of the surrounding muscles and soft tissues following mandibular advancement could in fact lead to a headgear-type effect, blocking or constricting the upper jaw. However, similar to many studies in the literature, [13] our data do not confirm this outcome, with no significant reduction in the SNA angle.
As for the dental effects, i.e., the inclination of the incisors with respect to their bony base, we found that the U1-PP angle was not reduced, while the IMPA increased by about 1.3° on average. This is an indication that, despite using a lower aligner for anchorage, it was not possible to completely counteract the vestibularisation related to the use of a mandibular advancement device. Considering that the initial position values of the lower incisors were generally increased with respect to the normal range (average at T0: 97.7 ± 5.493), the limited gain linked to the functional treatment was not a study group exclusion factor. Since a significant proclination of mandibular incisors is generally found when functional appliances are used during CSV1, CSV2, CSV5, the cervical vertebral stage maturation (CSV3, CSV4) represented an important inclusion criteria [14].
A large difference with respect to other studies in the literature is the non-significant variation in the upper incisor position, which remained largely unchanged. In other studies, the upper incisors were affected by a clinically and statistically significant degree of lingualisation, contributing to the reduction of the overjet [13,15]. A recent study comparing the dento-alveolar effects correlated to mandibular advancement performed with Twin-Block Appliance (TB) and Invisalign Mandibular Advancement (MA) confirms that clear aligners better control the incisors inclination. The biomechanical action of clear aligners is very useful in avoiding this great limit of class II functional appliances, since reduction of upper incisors’ inclination reduce the potential skeletal mandibular advancement [16].
Another effect that is inevitably linked to this type of treatment is an increase in divergence due to extrusion of the molars, and therefore backwards rotation of the mandibular plane. This was also seen in our patients, but only in part, as the FMA did not change in a statistically significant manner, while the change in MP-SN angle was significant, but probably not clinically appreciable (Δ average: +0.86).
When planning mandibular advancement, the correct timing is vital to achieve the maximum skeletal effects. The randomized clinical trials reviewed by Cozza et al. [17] in 2006 all agree that the amount of additional mandibular growth recorded after the use of functional appliances appears to be significantly higher when applied at the peak growth stage. A measure of the efficacy of functional appliances can be obtained by dividing the total mandibular length gained by the total number of months of treatment performed (efficacy coefficient). For the Herbst appliance it has been reported as 0.28 mm/month, the Twin Block 0.23 mm/month, the Bionator 0.17 mm/month, the Activator 0.12 mm/month, and the Frankel 0.09 mm/month. As expected, the most effective device turns out to be the only fixed, and therefore compliance-independent, one. Among the removable appliances, the Twin Block has the highest efficacy coefficient, and is very commonly used due to its high acceptability and ability to produce results rapidly over time [6]. In our sample the average treatment time with F22® Young was 10 months. Dividing this by the total mandibular elongation (+3.016 mm) we acquire a value of 0.3 mm/month. This is even higher than that of the Herbst appliance, which, coupled with the high acceptability of removable appliances, makes the F22®. Young a promising option, at least in the short term. Indeed, the device was highly accepted by all patients treated: nobody reported any particular pain, discomfort or tooth sensitivity for all treatment time [18].
The maintenance of the therapeutic position was ensured by the use of class II elastics directly applied to specific cuts performed on the aligners. The mandibular advancement can also lead to an improvement of sleep quality, with a contemporary tongue reposition, increasing the airway space and facilitating the superior respiratory system [19,20].
Recent studies have been conducted with the aim of investigating and quantitatively comparing the skeletal and dental effects obtained after a period of treatment with functional orthodontics on laterolateral radiographs. For example, Khojia et al. [13] compared changes in skeletal, dentoalveolar and soft tissue levels measured via cephalometry on radiographs taken before and after treatment with Twin Block, and confirmed an increase in the overall mandible length (Co-Gn) of 3.21 mm over a period of 12 months of treatment. Our results are just as good, if not better, revealing an increase of 3 mm over 10 months of observation. As for the SNB angle, Khojia et al. [13] found an improvement of 1.56° from the start of treatment, alongside a 1.82° reduction in the ANB. Similarly, Toth and McNamara [21] found a 1.8° reduction in the ANB angle in a group of patients treated via Twin Block. Our data are in line with those findings.
However, in order to interpret the results obtained in a meaningful fashion, it is important to be aware of the limitations of this study, one of which being the influence of natural growth, which may have differed to a greater or lesser extent in the patients analysed. Nonetheless, the changes seen in our group of patients, treated around the growth spurt, would have not normally be observed with natural growth. In fact, a longitudinal study comparing untreated class II (study group) and class I (control group) malocclusion patients during the stages of growth CSV3-CSV4 showed that the Co-Gn tends to vary significantly, less in the former than in the latter (a difference of about 2 mm). This means that in Class II subjects, the initial deficit remains constant during growth, without self-correcting, and the mandibular size discrepancy with respect to class I subjects therefore increases [22].
It is, however, important to note that we did not have a control or comparison class II group to compare the outcomes of our device with no treatment or those associated with another device, respectively. Of course, the present study is a first retrospective case series which evaluate for the first time a new clear functional appliance design. To confirm the results, further case-control studies are requested. Another limitation of our study is the lack of follow-up after the end of active treatment, which means that we cannot make any claims about the stability of the results achieved. Nonetheless, Baccetti [23] in 2009 compared the craniofacial changes in a sample of untreated class II and class I subjects occurring from late puberty to young adulthood. All anatomical landmarks near CS6 remained stable, with no significant variations over time or differences between the two groups. Again, long term stability skeletal corrections achieved with functional appliances was recently confirmed, with no specific intermaxillary retention approach needed [24]. This information is clinically very important, and confirms the high stability of orthopaedic changes brought by functional treatment implemented during the pubertal growth spurt.
6. Conclusions
According to this preliminary study, F22® Young appliance is effective in favouring mandibular advancement when used near the pubertal growth peak. Cephalometric analysis showed that it provided a significant increase in the total mandible length, and a consequent forward shift of point B, with normalization of the sagittal relationship between the jaws. A dental compensation has to be taken into consideration, because a proclination of lower incisor and extrusion of molars always represents a risk in a mandibular advancement treatment. Further studies are requested to validate these results.
Concerning the device design, it is comfortable, not bulky and “invisible”, which certainly promoted patient compliance—key factor for treatment success when using removable functional appliances.
Author Contributions
Conceptualization, G.S. and L.L.; methodology, F.C. (Francesca Cervinara) and L.L.; validation, G.S.; investigation, F.C. (Francesca Cremonini); data curation, F.C. (Francesca Cremonini) and F.C. (Francesca Cervinara); writing, F.C. (Francesca Cremonini). Supervision, L.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
All procedures performed in the study were in accordance with the ethical standards of the institutional and national research committee and with the 1975 Helsinki declaration and its later amendments or comparable ethical standards. The study design was reviewed and approved by the Ethics Committee of Postgraduated School of Orthodontics of Ferrara University, via Borsari 46, Ferrara, Italy (approval number 6/B/2019).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors certify that they have NO affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
References
- McNamara, J.A., Jr. Components of Class II malocclusion in children 8–10 years of age. Angle Orthod. 1981, 51, 177–202. [Google Scholar] [PubMed]
- Tollaro, I.; Baccetti, T.; Franchi, L.; Tanasescu, C.D. Role of posterior transverse interarch discrepancy in Class II, Division 1 malocclusion during the mixed dentition phase. Am. J. Orthod. Dentofac. Orhop. 1996, 110, 417–422. [Google Scholar] [CrossRef]
- Frankel, R.; Frankel, C. Orthodontics in orofacial region with help of function regulators. Inf. Orthod. Kieferorthop. 1988, 20, 277–309. [Google Scholar]
- Perinetti, G.; Primožič, J.; Franchi, L.; Contardo, L. Treatment effects of removable functional appliances in prepubertal and pubertal Class II patients: A systematic review and meta-analysis of controlled studies. PLoS ONE 2015, 10, e0141198. [Google Scholar] [CrossRef]
- Baysal, A.; Uysal, T. Soft tissue effects of Twin Block and Herbst appliances in patients with Class II division 1 mandibular retrognathy. Eur. J. Orthod. 2013, 35, 71–81. [Google Scholar] [CrossRef] [Green Version]
- Gill, D.; Sharma, A.; Naini, F.; Jones, S. The Twin Block appliance for the correction of Class II malocclusion. Dent. Update 2005, 32, 158–168. [Google Scholar] [CrossRef]
- Walton, D.K.; Fields, H.W.; Johnston, W.M.; Rosenstiel, S.F.; Firestone, A.R.; Christensen, J.C. Orthodontic appliance preferences of children and adolescents. Am. J. Orthod. Dentofac. Orthop. 2010, 138, 698.e1–698.e12. [Google Scholar] [CrossRef]
- Lombardo, L.; Arreghini, A.; Ramina, F.; Huanca Ghislanzoni, L.T.; Siciliani, G. Predictability of orthodontic movement with orthodontic aligners: A retrospective study. Prog. Orthod. 2017, 18, 35. [Google Scholar] [CrossRef] [Green Version]
- Rossini, G.; Parrini, S.; Castroflorio, T.; Deregibus, A.; Debernardi, C.L. Efficacy of clear aligners in controlling orthodontic tooth movement: A systematic review. Angle Orthod. 2014, 85, 881–889. [Google Scholar] [CrossRef] [Green Version]
- Baccetti, T.; Franchi, L.; McNamara, J.A., Jr. The cervical vertebral maturation (CVM) method for the assessment of optimal treatment timing in dentofacial orthopedics. Semin. Orthod. 2005, 11, 119. [Google Scholar] [CrossRef]
- O’Brien, K.; Wright, J.; Conboy, F.; Sanjie, Y.; Mandall, N.; Chadwick, S.; Connolly, I.; Cook, P.; Birnie, D.; Hammond, M.; et al. Effectiveness of early orthodontic treatment with the Twin-Block appliance: A multicenter, randomized, controlled trial. Part 1: Dental and skeletal effects. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 234–243. [Google Scholar] [CrossRef]
- Illing, H.M.; Morris, D.O.; Lee, R.T. A prospective evaluation of Bass, Bionator and Twin block appliances. Part I—The hard tissues. Eur. J. Orthod. 1998, 20, 501–516. [Google Scholar] [CrossRef] [PubMed]
- Khojia, A.; Fida, M.; Shaikh, A. Cephalometric evaluation of the effects of Twin Block appliance in subjects with Class II, Division I malocclusion among different cervical vertebral maturation stages. Dent. Press J. Orthod. 2016, 21, 73–84. [Google Scholar] [CrossRef] [Green Version]
- Guinot, F.; Ferrer, M.; Diaz-Gonzalez, L.; Garcia, C.; Maura, I. Effects of Orthodontic Functional Appliances in Relation to Skeletal Maturation of Cervical Vertebrae in Class II Malocclusion. J. Clin. Pediatr. Dent. 2021, 145, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Di Fazio, D.; Lombardo, L.; Gracco, A.; D’Amico, P.; Siciliani, G. Lip Pressure at rest and during function in 2 groups of patients with different occlusions. Am. J. Orthod. Dentofac. Orthop. 2011, 139, e1–e6. [Google Scholar] [CrossRef] [PubMed]
- Caruso, S.; Nota, A.; Caruso, S.; Severino, M.; Gatto, R.; Meuli, S.; Mattei, A.; Tecco, S. Mandibular advancement with clear aligners in the treatment of skeletal class II. A retrospective controlled study. Eur. J. Paediatr. Dent. 2021, 22, 26–30. [Google Scholar]
- Cozza, P.; Baccetti, T.; Franchi, L.; De Toffol, L.; McNamara, J.A., Jr. Mandibular canges produced by functional appliances in Class II malocclusion: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 599.e1–599.e12. [Google Scholar] [CrossRef] [Green Version]
- Scribante, A.; Gallo, S.; Celmare, R.L.; D’Antò, V.; Grippaudo, C.; Gandini, P.; Sfondrini, M.F. Orthodontic debonding and tooth sensitivity of anterior and posterior teeth. A Prospective clinical trial. Angle Orthod. 2020, 90, 766–773. [Google Scholar] [CrossRef]
- Modesti-Vedolin, G.; Chies, C.; Chaves-Fagondes, S.; Piza-Pelizzer, E.; Lima-Grossi, M. Efficacy of a mandibular advancement intraoral appliance (MOA) for the treatment of obstructive sleep apnea syndrome (OSAS) in pediatric patients: A pilot-study. Med. Oral Patol. Oral Cir. Bucal. 2018, 23, e656–e663. [Google Scholar] [CrossRef]
- Neagos, A.; Vrinceanu, D.; Dumitru, M.; Costache, A.; Cergan, R. Demographic, anthropometric, and metabolic characteristics of obstructive sleep apnea patients from Romania before the COVID-19 pandemic. Exp. Ther. Med. 2021, 22, 1487. [Google Scholar] [CrossRef]
- ToTh, L.R.; McNamara, J.A., Jr. Treatment effects produced by the twin block appliance and the FR-2 appliance of Frankel compared with an untreated Class II sample. Am. J. Orthod. Dentofac. Orthop. 1999, 116, 597–609. [Google Scholar] [CrossRef]
- Stahl, F.; Baccetti, T.; Franchi, L.; McNamara, J.A., Jr. Longitudinal growth changes in untreated subjects with Class II Division 1 malocclusion. Am. J. Orthod. Dentofac. Orthop. 2008, 134, 125–137. [Google Scholar] [CrossRef] [PubMed]
- Baccetti, T.; Stahl, F.; McNamara, J.A., Jr. Dentofacial growth changes in subjects with untreated Class II malocclusion from late puberty through young adulthood. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Moro, A.; Mattos, C.; Borges, S.; Flores-Mir, C.; Topolski, F. Stability of class II corrections with removable and fixed functional appliances: A literature review. J. World Fed. Orthod. 2020, 9, 56–67. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).