
Impact of Physiotherapy on Patients Suffering from COVID-19: An Observational Study

 ,
,  ,
, 
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Participants and Tools
- -
- (BA1) basic vital signs: blood oxygen saturation, respiratory rate, heart rate, blood pressure, and temperature;
- -
- (BA2) range of motion (passive and active);
- -
- (BA3) the degree of dyspnea.
- -
- CRP was selected for being measured, as it represents a valuable indicator of inflammation. Literature has associated mild COVID-19 with CRP values < 22 mg/L, while severe forms of COVID-19 have been associated with CRP > 80 mg/L [32];
- -
- IL-6 is a cytokine representing an early indicator of acute inflammation, with very high values of this parameter being associated with more severe forms of COVID-19 [33]. It has been observed that the decrease in IL-6 levels is closely related to the effectiveness of the treatment, while the increase in IL-6 levels indicates the worsening of the disease. For this reason, elevated serum IL-6 levels may be an ideal marker for disease monitoring [34];
- -
- Ferritin was monitored for a similar reason (its concentrations have also been associated with the severity of the disease and it may also serve as a predictive biomarker, as well as in the triage of COVID-19 patients) [35].
2.3. Ethical Considerations
2.4. Intervention
- -
- (PT1) Patients were advised to change their body positions every two hours during the day, going through prone, semi-dorsal, and lateral decubitus. Changing the patient’s position reduces the development of bedsores and can reduce the degree of dyspnea. Prone position ventilation: patients with severe COVID-19 with PaO2/FiO2 less than 150 mmHg at 16 h per day;
- -
- (PT2) Lying on the bed (supine position) with head on the pillow at a 45-degree position of the bed, the patient slowly performs the clenching of the fist and fingers and relaxes, and the planar-dorsal flexion of the ankles (10 times slowly);
- -
- (PT3) From the supine position with head on the pillow at a 45-degree position of the bed, the patient slowly performs the flexion-extension of the elbows (10 times slowly);
- -
- (PT4) From the supine position with head on the pillow at a 45-degree position of the bed, the patient slowly performs the flexion-extension of the knees, without lifting the sole of the floor (10 times, slowly);
- -
- (PT5) From the supine position, with head on the pillow at a 45-degree position of the bed, the patient slowly performs lifting and lowering the shoulders, abduction, and adduction of the scapula (5 times);
- -
- (PT6) Belly Breathing (Diaphragmic Breathing): the patient is in a supine position, with a pillow under his head or with his bed at a 45-degree position and bent knees. The patient puts one of his hands on the chest and the other one on the abdomen, just below the rib cage, inhaling slowly through the nose, letting the air go deep into the lower abdomen. The hand on the chest should remain still, while the hand on the belly should rise. The patient contracts the abdominal muscles and lets them fall inward, exhaling through tight lips. The hand on the abdomen should move back to the starting position. The exercise is performed with a progressive increase of the duration time from 1 to 5 min, considering the distress and the fatigue that can appear;
- -
- (PT7) Pursed Lip Breathing: the patient is in a sitting position, with the muscles of the shoulders and neck relaxed. The patient inhales slowly through the nose for two seconds, keeping the mouth closed, but breathing normally. They are advised that it may be helpful to count for themselves: inspire, one, two. After this, they have to wrinkle or “squeeze” their lips, as if they are whistling or lightly flickering the flame of a candle, then exhale slowly through their tight lips as they count to four. It may be helpful to count: exhale, one, two, three, four. The exercise is performed with a progressive increase of the duration time, from 1 to 5 min, considering the distress and fatigue that can appear;
- -
- (PT8) General exercises. The patients are advised to: squeeze their shoulder blade (8 to 12 times); strengthen the lower legs (10–20 times); raise the heels (20 times); lift the knees, hold for 10 s (3–5 times); shift weight, hold for 10 s (3–5 times); get a single leg balance.
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mocanu, G.D.; Murariu, G.; Iordan, D.A.; Sandu, I.; Munteanu, M.O.A. The Perception of the Online Teaching Process during the COVID-19 Pandemic for the Students of the Physical Education and Sports Domain. Appl. Sci. 2021, 11, 5558. [Google Scholar] [CrossRef]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.T.; Leung, K.; Leung, G.M. Nowcasting and forecasting the potential domestic and international spread of the 2019-nCoV outbreak originating in Wuhan, China: A modelling study. Lancet 2020, 395, 689–697. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Li, J. Rehabilitation management of patients with COVID-19: Lessons learned from the first experience in China. Eur. J. Phys. Rehabil. Med. 2020, 56, 335–338. [Google Scholar] [CrossRef]
- Oltenacu, R.C.; Ciubara, A.B.; Nechifor, A.; Burlea, S.L.; Ciubara, A. The Evolution of Mental Health in Patients with Psoriasis during the COVID-19 Pandemic. BRAIN Broad Res. Artif. Intell. Neurosci. 2021, 12, 342–348. [Google Scholar] [CrossRef]
- Munteanu, C.; Păun, D.L.; Șuță, A.F.; Florescu, S.A.; Onose, G. Diabetes mellitus and COVID-19 in the post-acute phase patients—possible links with physical and rehabilitation medicine and balneotherapy. Balneo Res. J. 2020, 11, 350–367. [Google Scholar] [CrossRef]
- Elena, R.O.; Adrian, C.D.R.; Cristina, V.; Magdalena, Ț.A.; Carmen, T.A.; Ioana, B. Challenges in the diagnosis, treatment and management of asthma during COVID-19 pandemic. Pneumologia 2020, 69, 73–80. [Google Scholar] [CrossRef]
- Oxley, T.J.; Mocco, J.; Majidi, S.; Kellner, C.P.; Shoirah, H.; Singh, I.P.; De Leacy, R.A.; Shigematsu, T.; Ladner, T.R.; Yaeger, K.A.; et al. Large-vessel stroke as a presenting feature of Covid-19 in the young. N. Engl. J. Med. 2020, 382, e60. [Google Scholar] [CrossRef] [PubMed]
- Williamson, E.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. OpenSAFELY: Factors associated with COVID-19-related hospital death in the linked electronic health records of 17 million adult NHS patients. MedRxiv 2020, 584, 430–436. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease (COVID-2019) Situation Reports. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/ (accessed on 15 January 2022).
- Sharma, A.; Ahmad Farouk, I.; Lal, S.K. COVID-19: A Review on the Novel Coronavirus Disease Evolution, Transmission, Detection, Control and Prevention. Viruses 2021, 13, 202. [Google Scholar] [CrossRef]
- Yüce, M.; Filiztekin, E.; Özkaya, K.G. COVID-19 diagnosis—A review of current methods. Biosens. Bioelectron. 2021, 172, 112752. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 21 April 2022).
- Therapeutics and COVID-19: Living Guideline. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-therapeutics-2022.3 (accessed on 15 January 2022).
- Bai, C.; Chotirmall, S.-H.; Rello, J.; Alba, G.-A.; Ginns, L.-C.; Krishnan, J.A.; Rogers, R.; Bendstrup, E.; Burgel, P.-R.; Chalmers, J.D.; et al. Updated guidance on the management of COVID-19: From an American Thoracic Society/European Respiratory Society coordinated International Task Force. Eur. Respir. Rev. 2020, 29, 200287. [Google Scholar] [CrossRef]
- Yang, L.-L.; Yang, T. Pulmonary rehabilitation for patients with coronavirus disease 2019 (COVID-19). Chronic Dis. Transl. Med. 2020, 6, 79–86. [Google Scholar] [CrossRef]
- Halpin, D.M.G.; Criner, G.J.; Papi, A.; Singh, D.; Anzueto, A.; Martinez, F.J.; Agusti, A.A.; Vogelmeier, C.F. Global Initiative for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease. The 2020 GOLD Science Committee Report on COVID-19 and Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2021, 203, 24–36. [Google Scholar] [CrossRef]
- Hsieh, M.J.; Lee, W.C.; Cho, H.Y.; Wu, M.-F.; Hu, H.-C.; Kao, K.-C.; Chen, N.-H.; Tsai, Y.-H.; Huang, C.-C. Recovery of pulmonary functions, exercise capacity, and quality of life after pulmonary rehabilitation in survivors of ARDS due to severe influenza A (H1N1) pneumonitis. Influenza Other Respir. Viruses 2018, 12, 643–648. [Google Scholar] [CrossRef]
- Rokach, A.; Romem, A.; Arish, N.; Azulai, H.; Chen, C.; Bertisch, M.; Izbicki, G. The effect of pulmonary rehabilitation on non-chronic obstructive pulmonary disease patients. Isr. Med. Assoc. J. 2009, 5, 326–329. [Google Scholar]
- Lindenauer, P.K.; Stefan, M.S.; Pekow, P.S.; Mazor, K.M.; Priya, A.; Spitzer, K.A.; Lagu, T.C.; Pack, Q.R.; Pinto-Plata, V.M.; ZuWallack, R. Association between initiation of pulmonary rehabilitation after hospitalization for COPD and 1-year survival among Medicare beneficiaries. JAMA 2020, 232, 1813. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Santiago, V.; Diez-Vega, I.; Santana-Sosa, E.; Lopez Nuevo, C.; Iturriaga Ramirez, T.; Vendrusculo, F.M.; Donadio, M.-V.F.; Villa Asensi, J.R.; Pérez-Ruiz, M. Effect of a combined exercise program on physical fitness, lung function, and quality of life in patients with controlled asthma and exercise symptoms: A randomized controlled trial. Pediatr. Pulmonol. 2020, 55, 1608–1616. [Google Scholar] [CrossRef]
- Yuetong, Z.; Wang, Z.; Zhou, Y.; Onoda, K.; Maruyama, H.; Hu, C.; Liu, Z. Summary of respiratory rehabilitation and physical therapy guidelines for patients with COVID-19 based on recommendations of World Confederation for Physical Therapy and National Association of Physical Therapy. J. Phys. Ther. Sci. 2020, 32, 545–549. [Google Scholar] [CrossRef]
- Ohtake, P.J.; Lee, A.C.; Scott, J.C.; Hinman, R.S.; Ali, N.; Hinkson, C.R.; Needham, D.M.; Shutter, L.; Smith-Gabai, H.; Spires, M.C.; et al. Physical Impairments Associated with Post-Intensive Care Syndrome: Systematic Review Based on the World Health Organization’s International Classification of Functioning, Disability and Health Framework. Phys. Ther. 2018, 98, 631–645. [Google Scholar] [CrossRef] [Green Version]
- Popa-Velea, O.; Pristavu, C.; Ionescu, C.; Mihăilescu, A.; Diaconescu, L. Teaching Style, Coping Strategies, Stress and Social Support: Associations to the Medical Students’ Perception of Learning during the SARS-CoV-2 Pandemic. Educ. Sci. 2021, 11, 414. [Google Scholar] [CrossRef]
- Cieloszczyk, A.; Lewko, A.; Śliwka, A.; Włoch, T.; Pyszora, A. Recommendations for physiotherapy of adult patients with COVID-19. Available online: https://world.physio/sites/default/files/2020-06/Polish-Respiratory-Physiotherapy-Expert-Group-adult-patients-English.pdf (accessed on 15 January 2022).
- Boldrini, P.; Bernetti, A.; Fiore, P. SIMFER Executive Committee and SIMFER Committee for international affairs. Impact of COVID-19 outbreak on rehabilitation services and Physical and Rehabilitation Medicine (PRM) physicians’ activities in Italy. An official document of the Italian PRM Society (SIMFER). Eur. J. Phys. Rehabil. Med. 2020, 56, 316–318. [Google Scholar] [CrossRef]
- Agostini, F.; Mangone, M.; Ruiu, P.; Paolucci, T.; Santilli, V.; Bernetti, A. Rehabilitation settings during and after covid-19: An overview of recommendations. J. Rehabil. Med. 2021, 53, jrm00141. [Google Scholar] [CrossRef]
- Liu, K.; Zhang, W.; Yang, Y.; Zhang, J.; Li, Y.; Chen, Y. Respiratory rehabilitation in elderly patients with COVID-19: A randomized controlled study. Complement. Ther. Clin. Pract. 2020, 39, 101166. [Google Scholar] [CrossRef]
- Battaglini, D.; Robba, C.; Caiffa, S.; Ball, L.; Brunetti, I.; Loconte, M.; Giacobbe, D.R.; Vena, A.; Patroniti, N.; Bassetti, M.; et al. Chest physiotherapy: An important adjuvant in critically ill mechanically ventilated patients with COVID-19. Respir. Physiol. Neurobiol. 2020, 282, 103529. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, M.; Clerckx, B.; Janssen, K.; Segers, J.; Demeyere, I.; Frickx, B.; Merckx, E.; Hermans, G.; Van der Meulen, I.; Van Lancker, T.; et al. Early mobilization in clinical practice: The reliability and feasibility of the ‘Start To Move’ Protocol. Physiother. Theory Pract. 2022, 38, 908–918. [Google Scholar] [CrossRef]
- Tordjman, M.; Mekki, A.; Mali, R.D.; Monnier, H.; Neveu, S.; Chassagnon, G.; Mihoubi, F.; Carlier, N.; Marey, J.; Fournier, L.; et al. Determining extent of COVID-19 pneumonia on CT based on biological variables. Respir. Med. 2020, 175, 106206. [Google Scholar] [CrossRef]
- Thakur, A.K.; Yerra, A.; Shaikh, F.; Dekate, P.; Sachane, K.; Chirla, D.; Desai, U.; Narayanan, K. Role of serum il-6 and ferritin levels as marker of severity and outcome predictor in children with multiorgan dysfunction syndrome. Indian J. Crit. Care Medicin. 2021, 25, S99–S100. [Google Scholar] [CrossRef]
- Sabaka, P.; Koščálová, A.; Straka, I.; Hodosy, J.; Lipták, R.; Kmotorková, B.; Kachlíková, M.; Kušnírová, A. Role of interleukin 6 as a predictive factor for a severe course of Covid-19: Retrospective data analysis of patients from a long-term care facility during Covid-19 outbreak. BMC Infect. Dis. 2021, 21, 308. [Google Scholar] [CrossRef]
- Kaushal, K.; Kaur, H.; Sarma, P.; Bhattacharyya, A.; Sharma, D.J.; Prajapat, M.; Pathak, M.; Kothari, A.; Kumar, S.; Rana, S.; et al. Serum ferritin as a predictive biomarker in COVID-19. A systematic review, meta-analysis and meta-regression analysis. J. Crit. Care 2022, 67, 172–181. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Jiandani, M.P.; Salagre, S.B.; Kazi, S.; Iyer, S.; Patil, P.; Khot, W.Y.; Patil, E.; Sopariwala, M. Preliminary Observations and Experiences of Physiotherapy Practice in Acute Care Setup of COVID 19: A Retrospective Observational Study. J. Assoc. Physicians India 2020, 68, 18–24. [Google Scholar] [PubMed]
- Nandasena, H.M.R.K.G.; Pathirathna, M.L.; Atapattu, A.M.M.P.; Prasanga, P.T.S. Quality of life of COVID 19 patients after discharge: Systematic review. PLoS ONE 2022, 17, e0263941. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Patients (N = 45) | Mild Physiotherapy | Active Physiotherapy (%) | No Physiotherapy (%) | p |
|---|---|---|---|---|---|
| Male | 28 | 49 | 24 | 27 | 0.13 |
| Female | 17 | 35 | 28 | 37 | 0.14 |
| Median age (years) | 65 | 66 | 68 | 58 | 0.54 |
| Dry cough at admission | 25 | 40 | 28 | 32 | 0.50 |
| Dry cough at discharge | 6 | 0 | 0 | 100 | - |
| Dyspnea at admission | 30 | 42 | 31 | 27 | 0.10 |
| Dyspnea at discharge | 5 | 4 | 0 | 96 | - |
| Gastric ulcer | 14 | 22 | 15 | 63 | 0.62 |
| Duodenal ulcer | 18 | 33 | 26 | 41 | 0.23 |
| Cirrhosis | 10 | 22 | 8 | 70 | 0.03 |
| Parameter | Phase of Treatment | Mean | Median | Standard Deviation | Min. | Max. |
|---|---|---|---|---|---|---|
| Ferritin (ng/mL) | hospitalization | 1933.88 | 856.00 | 2420.94 | 45.00 | 9801.00 |
| discharge | 85.97 | 69.50 | 73.21 | 12.30 | 475.00 | |
| IL-6 (pg/mL) | hospitalization | 181.68 | 78.50 | 322.77 | 4.56 | 1491.00 |
| discharge | 19.57 | 12.50 | 21.31 | 5.09 | 89.54 | |
| CRP (mg/L) | hospitalization | 104.60 | 95.58 | 79.01 | 12.30 | 486.00 |
| discharge | 16.60 | 8.90 | 17.18 | 1.06 | 73.37 | |
| Pulse | hospitalization | 100.37 | 96.00 | 19.04 | 69.00 | 145.00 |
| discharge | 74.50 | 72.00 | 10.70 | 56.00 | 100.00 | |
| Oxygen saturation | hospitalization | 94.19 | 95.00 | 3.73 | 85.00 | 98.00 |
| discharge | 97.77 | 98.00 | 1.11 | 94.00 | 99.00 |
| Biological Parameters | Wilks’–Lambda | Partial–Lambda | F | p | Tolerance | 1-Tolerance (R-Square) |
|---|---|---|---|---|---|---|
| Ferritin at admission | 0.019 | 0.998 | 0.034 | 0.966 | 0.294 | 0.706 |
| Ferritin at discharge | 0.021 | 0.920 | 1.259 | 0.299 | 0.543 | 0.457 |
| IL-6 at admisson | 0.050 | 0.380 | 23.615 | 0.001 | 0.313 | 0.687 |
| IL-6 at dischcarge | 0.021 | 0.899 | 1.632 | 0.213 | 0.500 | 0.500 |
| CRP at admission | 0.021 | 0.929 | 1.113 | 0.342 | 0.416 | 0.584 |
| CRP at discharge | 0.028 | 0.668 | 7.195 | 0.003 | 0.320 | 0.680 |
| Dyspnea at admission | 0.019 | 1.000 | 0.004 | 0.996 | 0.870 | 0.130 |
| Dyspnea at discharge | 0.023 | 0.831 | 5.954 | 0.051 | 0.450 | 0.550 |
| Pulse at admission | 0.022 | 0.878 | 2.020 | 0.151 | 0.357 | 0.643 |
| Pulse at discharge | 0.020 | 0.958 | 0.635 | 0.537 | 0.380 | 0.620 |
| Oxygen saturation on admission | 0.023 | 0.842 | 2.720 | 0.083 | 0.237 | 0.763 |
| Oxygen saturation on discharge | 0.021 | 0.900 | 1.607 | 0.218 | 0.589 | 0.411 |
| Dry cough at admission | 0.022 | 0.883 | 1.916 | 0.165 | 0.549 | 0.451 |
| Dry cough at discharge | 0.140 | 0.136 | 92.277 | 0.001 | 0.296 | 0.704 |
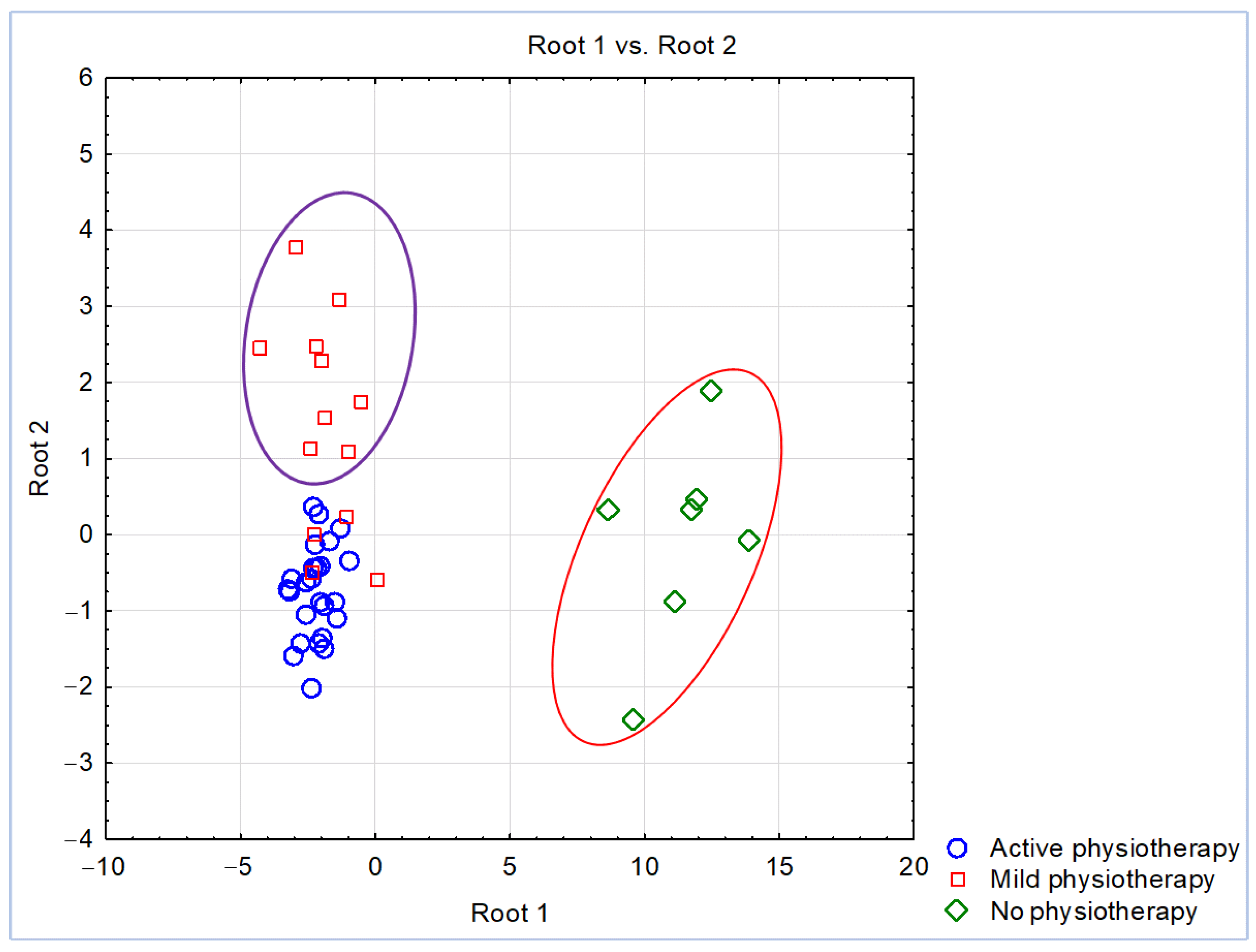
| Variables | Standardized Coefficients for Canonical Variables | |
|---|---|---|
| Function 1 (Root 1) | Function 2 (Root 2) | |
| IL-6 at admission | −0.550 | 0.918 |
| Ferritin at discharge | −0.526 | 0.731 |
| Dyspnea at discharge | −0.983 | −0.320 |
| CRP at discharge | −0.680 | −1.071 |
| Oxygen saturation at admission | 0.935 | 0.457 |
| CRP at admission | 0.741 | 0.064 |
| Ferritin at admission | 0.564 | −0.266 |
| Pulse at discharge | −0.336 | 0.290 |
| IL-6 at discharge | −0.365 | −0.147 |
| Variables | Rank Sum Mild PT | Rank Sum Active PT | U | Z | p | Z Adjusted | p Adjusted |
|---|---|---|---|---|---|---|---|
| Ferritin at admission | 502.500 | 532.500 | 177.500 | −1.645 | 0.100 | −1.645 | 0.100 |
| Ferritin at discharge | 544.000 | 491.000 | 219.000 | −0.697 | 0.486 | −0.697 | 0.486 |
| IL-6 at admisson | 459.500 | 575.500 | 134.500 | −2.627 | 0.009 | −2.627 | 0.009 |
| IL-6 at dischcarge | 471.500 | 563.500 | 146.500 | −2.353 | 0.019 | −2.354 | 0.019 |
| CRP at admission | 496.500 | 538.500 | 171.500 | −1.782 | 0.075 | −1.782 | 0.075 |
| CRP at discharge | 488.500 | 546.500 | 163.500 | −1.964 | 0.049 | −1.964 | 0.049 |
| Dyspnea at admission | 517.000 | 518.000 | 192.000 | −1.313 | 0.189 | −1.600 | 0.110 |
| Dyspnea at discharge | 512.500 | 522.500 | 187.500 | −1.416 | 0.157 | −2.601 | 0.009 |
| Pulse at admission | 476.000 | 559.000 | 151.000 | −2.250 | 0.024 | −2.253 | 0.024 |
| Pulse at discharge | 554.000 | 481.000 | 229.000 | −0.468 | 0.640 | −0.470 | 0.639 |
| Oxygen saturation on admission | 666.000 | 369.000 | 159.000 | 2.067 | 0.039 | 2.093 | 0.036 |
| Oxygen saturation on discharge | 655.500 | 379.500 | 169.500 | 1.827 | 0.068 | 1.905 | 0.057 |
| Dry cough at admission | 549.000 | 486.000 | 224.000 | −0.582 | 0.560 | −0.668 | 0.504 |
| Dry cough at discharge | 500.000 | 535.000 | 175.000 | −1.702 | 0.089 | −2.889 | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Onu, I.; Iordan, D.-A.; Matei, D.; Hrisca-Eva, O.-D.; Buculei, I.; Galaction, A.-I.; Serban, I.L.; Dobrin, M.-E.; Popa-Velea, O.; Costin, D.E.; et al. Impact of Physiotherapy on Patients Suffering from COVID-19: An Observational Study. Appl. Sci. 2022, 12, 5795. https://doi.org/10.3390/app12125795
Onu I, Iordan D-A, Matei D, Hrisca-Eva O-D, Buculei I, Galaction A-I, Serban IL, Dobrin M-E, Popa-Velea O, Costin DE, et al. Impact of Physiotherapy on Patients Suffering from COVID-19: An Observational Study. Applied Sciences. 2022; 12(12):5795. https://doi.org/10.3390/app12125795
Chicago/Turabian StyleOnu, Ilie, Daniel-Andrei Iordan, Daniela Matei, Oana-Diana Hrisca-Eva, Ioana Buculei, Anca-Irina Galaction, Ionela Lăcrămioara Serban, Mona-Elisabeta Dobrin, Ovidiu Popa-Velea, Dan Eugen Costin, and et al. 2022. "Impact of Physiotherapy on Patients Suffering from COVID-19: An Observational Study" Applied Sciences 12, no. 12: 5795. https://doi.org/10.3390/app12125795
APA StyleOnu, I., Iordan, D.-A., Matei, D., Hrisca-Eva, O.-D., Buculei, I., Galaction, A.-I., Serban, I. L., Dobrin, M.-E., Popa-Velea, O., Costin, D. E., Mocanu, G. D., Dobre, A.-G., & Gherghel, R. (2022). Impact of Physiotherapy on Patients Suffering from COVID-19: An Observational Study. Applied Sciences, 12(12), 5795. https://doi.org/10.3390/app12125795