
Soluble Receptor of Advanced Glycation End-Products (sRAGE) in Pediatric Asthma: A Prospective Study in 68 Children Aged 7 Years

 ,
,  , , , and
, , , and
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Collected Data
2.3.1. Clinical Data
2.3.2. Pulmonary Function Evaluation
2.3.3. Biological Assessment
2.4. Statistical Analysis
3. Results
3.1. Population
3.2. sRAGE Levels
3.2.1. Mean Levels
3.2.2. sRAGE in Asthma and Atopic Status
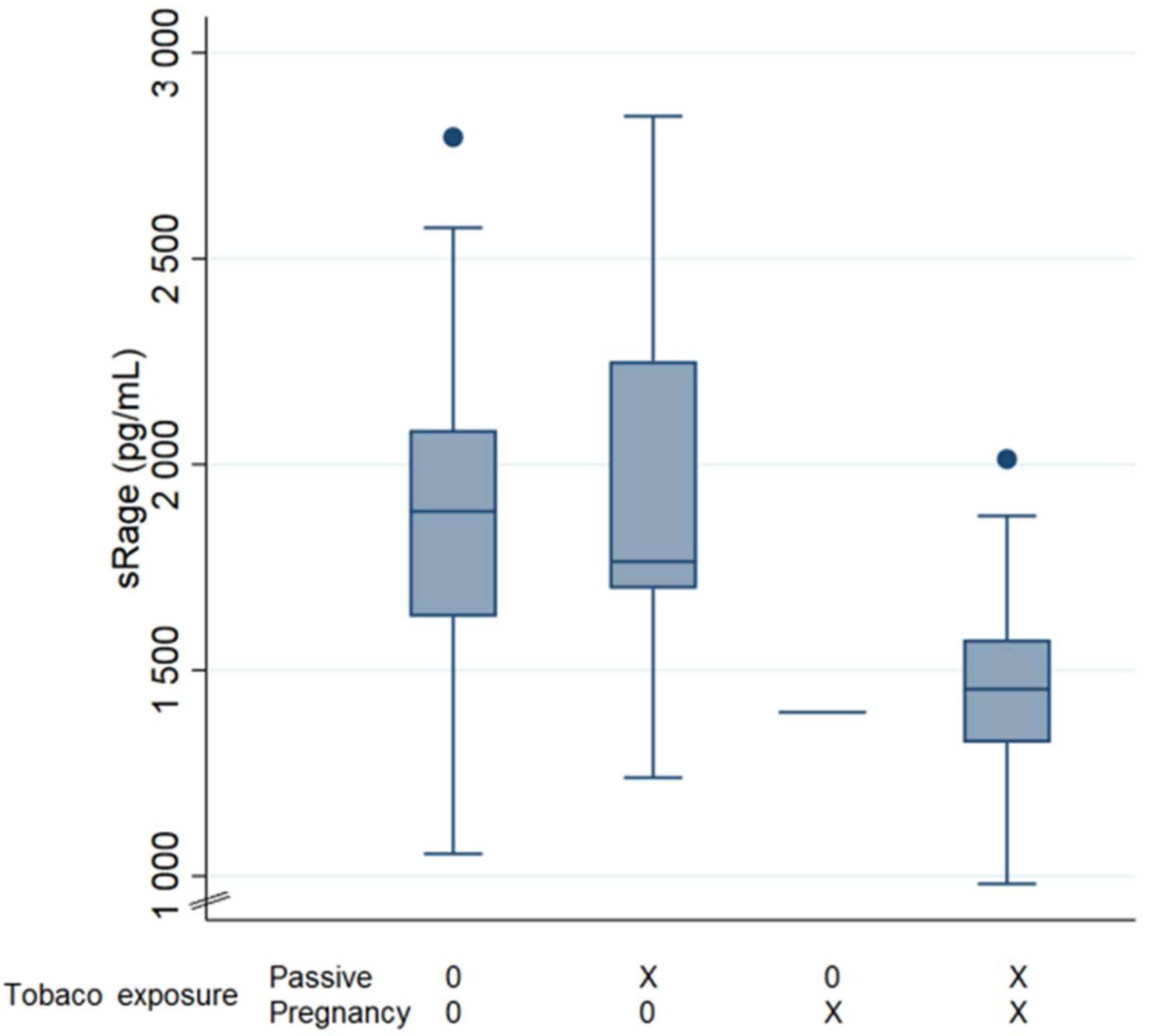
3.2.3. Environment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, Y.; Wu, R.; Tian, Y.; Bao, T.; Tian, Z. Fraction of Exhaled Nitric Oxide and Soluble Receptors for Advanced Glycation End Products Are Negatively Correlated in Children with Recurrent Wheezing. Asian Pac. J. Allergy Immunol. 2017, 35, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.; Khan, M.Y.; Rafi, Z.; Khan, H.; Siddiqui, Z.; Rehman, S.; Shahab, U.; Khan, M.S.; Saeed, M.; Alouffi, S.; et al. Oxidation, glycation and glycoxidation-The vicious cycle and lung cancer. Semin. Cancer Biol. 2018, 49, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.; Khan, H.; Siddiqui, Z.; Khan, M.Y.; Rehman, S.; Shahab, U.; Godovikova, T.; Silnikov, V.; Moinuddin. AGEs, RAGEs and s-RAGE; friend or foe for cancer. Semin. Cancer Biol. 2018, 4, 44–55. [Google Scholar] [CrossRef]
- Brandt, E.B.; Lewkowich, I.P. RAGE-Induced Asthma: A Role for the Receptor for Advanced Glycation End-Products in Promoting Allergic Airway Disease. J. Allergy Clin. Immunol. 2019, 144, 651–653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurtado Del Pozo, C.; Ruiz, H.H.; Arivazhagan, L.; Aranda, J.F.; Shim, C.; Daya, P.; Derk, J.; MacLean, M.; He, M.; Frye, L.; et al. A Receptor of the Immunoglobulin Superfamily Regulates Adaptive Thermogenesis. Cell Rep. 2019, 28, 773–791. [Google Scholar] [CrossRef]
- Yonekura, H.; Yamamoto, Y.; Sakurai, S.; Petrova, R.G.; Abedin, M.J.; Li, H.; Yasui, K.; Takeuchi, M.; Makita, Z.; Takasawa, S.; et al. Novel Splice Variants of the Receptor for Advanced Glycation End-Products Expressed in Human Vascular Endothelial Cells and Pericytes, and Their Putative Roles in Diabetes-Induced Vascular Injury. Biochem. J. 2003, 370, 1097–1109. [Google Scholar] [CrossRef]
- Shahab, U.; Ahmad, M.K.; Mahdi, A.A.; Waseem, M.; Arif, B.; Moinuddi; Ahmad, S. The receptor for advanced glycation end products: A fuel to pancreatic cancer. Semin. Cancer Biol. 2018, 49, 37–43. [Google Scholar] [CrossRef]
- Harashima, A.; Yamamoto, Y.; Cheng, C.; Tsuneyama, K.; Myint, K.M.; Takeuchi, A.; Yoshimura, K.; Li, H.; Watanabe, T.; Takasawa, S.; et al. Identification of Mouse Orthologue of Endogenous Secretory Receptor for Advanced Glycation End-Products: Structure, Function and Expression. Biochem. J. 2006, 396, 109–115. [Google Scholar] [CrossRef] [Green Version]
- Hanford, L.E.; Enghild, J.J.; Valnickova, Z.; Petersen, S.V.; Schaefer, L.M.; Schaefer, T.M.; Reinhart, T.A.; Oury, T.D. Purification and Characterization of Mouse Soluble Receptor for Advanced Glycation End Products (SRAGE). J. Biol. Chem. 2004, 279, 50019–50024. [Google Scholar] [CrossRef] [Green Version]
- Oczypok, E.A.; Perkins, T.N.; Oury, T.D. All the “RAGE” in Lung Disease: The Receptor for Advanced Glycation Endproducts (RAGE) Is a Major Mediator of Pulmonary Inflammatory Responses. Paediatr. Respir. Rev. 2017, 23, 40–49. [Google Scholar] [CrossRef]
- van der Zee, P.; Rietdijk, W.; Somhorst, P.; Endeman, H.; Gommers, D. A Systematic Review of Biomarkers Multivariately Associated with Acute Respiratory Distress Syndrome Development and Mortality. Crit. Care 2020, 24, 243. [Google Scholar] [CrossRef] [PubMed]
- Jabaudon, M.; Futier, E.; Roszyk, L.; Chalus, E.; Guerin, R.; Petit, A.; Mrozek, S.; Perbet, S.; Cayot-Constantin, S.; Chartier, C.; et al. Soluble Form of the Receptor for Advanced Glycation End Products Is a Marker of Acute Lung Injury but Not of Severe Sepsis in Critically Ill Patients. Crit. Care Med. 2011, 39, 480–488. [Google Scholar] [CrossRef] [PubMed]
- Mrozek, S.; Jabaudon, M.; Jaber, S.; Paugam-Burtz, C.; Lefrant, J.-Y.; Rouby, J.-J.; Asehnoune, K.; Allaouchiche, B.; Baldesi, O.; Leone, M.; et al. Elevated Plasma Levels of SRAGE Are Associated with Nonfocal CT-Based Lung Imaging in Patients with ARDS. Chest 2016, 150, 998–1007. [Google Scholar] [CrossRef] [PubMed]
- Jabaudon, M.; Blondonnet, R.; Pereira, B.; Cartin-Ceba, R.; Lichtenstern, C.; Mauri, T.; Determann, R.M.; Drabek, T.; Hubmayr, R.D.; Gajic, O.; et al. Plasma SRAGE Is Independently Associated with Increased Mortality in ARDS: A Meta-Analysis of Individual Patient Data. Intensive Care Med. 2018, 44, 1388–1399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yehya, N.; Thomas, N.J.; Meyer, N.J.; Christie, J.D.; Berg, R.A.; Margulies, S.S. Circulating Markers of Endothelial and Alveolar Epithelial Dysfunction Are Associated with Mortality in Pediatric Acute Respiratory Distress Syndrome. Intensive Care Med. 2016, 42, 1137–1145. [Google Scholar] [CrossRef] [PubMed]
- Yerkovich, S.T.; Chang, A.B.; Carroll, M.L.; Petsky, H.L.; Scrivener, G.; Upham, J.W. Soluble Receptor for Advanced Glycation End Products (SRAGE) Is Present at High Concentrations in the Lungs of Children and Varies with Age and the Pattern of Lung Inflammation. Respirology 2012, 17, 841–846. [Google Scholar] [CrossRef] [PubMed]
- Milutinovic, P.S.; Alcorn, J.F.; Englert, J.M.; Crum, L.T.; Oury, T.D. The Receptor for Advanced Glycation End Products Is a Central Mediator of Asthma Pathogenesis. Am. J. Pathol. 2012, 181, 1215–1225. [Google Scholar] [CrossRef] [Green Version]
- El-Seify, M.Y.H.; Fouda, E.M.; Nabih, E.S. Serum Level of Soluble Receptor for Advanced Glycation End Products in Asthmatic Children and Its Correlation to Severity and Pulmonary Functions. Clin. Lab. 2014, 60, 957–962. [Google Scholar] [CrossRef]
- Amat, F.; Plantard, C.; Mulliez, A.; Petit, I.; Rochette, E.; Verdan, M.; Henquell, C.; Labbé, G.; Heraud, M.C.; Evrard, B.; et al. RSV-HRV Co-Infection Is a Risk Factor for Recurrent Bronchial Obstruction and Early Sensitization 3 Years after Bronchiolitis. J. Med. Virol. 2018, 90, 867–872. [Google Scholar] [CrossRef]
- Sass, C.; Guéguen, R.; Moulin, J.-J.; Abric, L.; Dauphinot, V.; Dupré, C.; Giordanella, J.-P.; Girard, F.; Guenot, C.; Labbé, É.; et al. Comparaison du score individuel de précarité des Centres d’examens de santé, EPICES, à la définition socio-administrative de la précarité. Sante Publique 2006, 18, 513–522. [Google Scholar] [CrossRef]
- Hovland, V.; Riiser, A.; Mowinckel, P.; Carlsen, K.-H.; Carlsen, K.C.L. The Significance of Early Recurrent Wheeze for Asthma Outcomes in Late Childhood. Eur. Respir. J. 2013, 41, 838–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moral, L.; Vizmanos, G.; Torres-Borrego, J.; Praena-Crespo, M.; Tortajada-Girbés, M.; Pellegrini, F.J.; Asensio, Ó. Asthma Diagnosis in Infants and Preschool Children: A Systematic Review of Clinical Guidelines. Allergol. Immunopathol. 2019, 47, 107–121. [Google Scholar] [CrossRef] [PubMed]
- Standardisation of Spirometry|European Respiratory Society. Available online: https://erj.ersjournals.com/content/26/2/319.long (accessed on 26 April 2022).
- Beydon, N.; Matecki, S. L’exploration fonctionnelle respiratoire du jeune enfant. MISE AU POINT 5. Available online: https://www.edimark.fr/lettre-pneumologue/exploration-fonctionnelle-respiratoire-jeune-enfant (accessed on 26 April 2022).
- Ortega, H.G.; Liu, M.C.; Pavord, I.D.; Brusselle, G.G.; FitzGerald, J.M.; Chetta, A.; Humbert, M.; Katz, L.E.; Keene, O.N.; Yancey, S.W.; et al. Mepolizumab Treatment in Patients with Severe Eosinophilic Asthma. N. Engl. J. Med. 2014, 371, 1198–1207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egron, C.; Roszyk, L.; Rochette, E.; Jabaudon, M.; Sapin, V.; Mulliez, A.; Labbé, A.; Coste, K. Serum Soluble Receptor for Advanced Glycation End-Products during Acute Bronchiolitis in Infant: Prospective Study in 93 Cases. Pediatr. Pulmonol. 2018, 53, 1429–1435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyu, Y.; Zhao, H.; Ye, Y.; Liu, L.; Zhu, S.; Xia, Y.; Zou, F.; Cai, S. Decreased Soluble RAGE in Neutrophilic Asthma Is Correlated with Disease Severity and RAGE G82S Variants. Mol. Med. Rep. 2018, 17, 4131–4137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Salido, A.; Oñoro, G.; Melen, G.J.; Gómez-Piña, V.; Serrano-González, A.; Ramírez-Orellana, M.; Casado-Flores, J. Serum SRAGE as a Potential Biomarker for Pediatric Bronchiolitis: A Pilot Study. Lung 2015, 193, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Patregnani, J.T.; Brooks, B.A.; Chorvinsky, E.; Pillai, D.K. High BAL SRAGE Is Associated with Low Serum Eosinophils and IgE in Children with Asthma. Children 2020, 7, 110. [Google Scholar] [CrossRef]
- Iwamoto, H.; Gao, J.; Pulkkinen, V.; Toljamo, T.; Nieminen, P.; Mazur, W. Soluble Receptor for Advanced Glycation End-Products and Progression of Airway Disease. BMC Pulm. Med. 2014, 14, 68. [Google Scholar] [CrossRef] [Green Version]
- Sukkar, M.B.; Wood, L.G.; Tooze, M.; Simpson, J.L.; McDonald, V.M.; Gibson, P.G.; Wark, P.A.B. Soluble RAGE Is Deficient in Neutrophilic Asthma and COPD. Eur. Respir. J. 2012, 39, 721–729. [Google Scholar] [CrossRef]
- Reynolds, P.R.; Kasteler, S.D.; Cosio, M.G.; Sturrock, A.; Huecksteadt, T.; Hoidal, J.R. RAGE: Developmental Expression and Positive Feedback Regulation by Egr-1 during Cigarette Smoke Exposure in Pulmonary Epithelial Cells. Am J. Physiol. Lung Cell. Mol. Physiol. 2008, 294, L1094–L1101. [Google Scholar] [CrossRef] [Green Version]
- Prasad, K.; Dhar, I.; Caspar-Bell, G. Role of Advanced Glycation End Products and Its Receptors in the Pathogenesis of Cigarette Smoke-Induced Cardiovascular Disease. Int. J. Angiol. 2015, 24, 75–80. [Google Scholar] [CrossRef] [Green Version]
- Pouwels, S.D.; Klont, F.; Kwiatkowski, M.; Wiersma, V.R.; Faiz, A.; van den Berge, M.; Horvatovich, P.; Bischoff, R.; ten Hacken, N.H.T. Cigarette Smoking Acutely Decreases Serum Levels of the Chronic Obstructive Pulmonary Disease Biomarker SRAGE. Am. J. Respir. Crit. Care Med. 2018, 198, 1456–1458. [Google Scholar] [CrossRef] [PubMed]
- Thacher, J.D.; Gehring, U.; Gruzieva, O.; Standl, M.; Pershagen, G.; Bauer, C.-P.; Berdel, D.; Keller, T.; Koletzko, S.; Koppelman, G.H.; et al. Maternal Smoking during Pregnancy and Early Childhood and Development of Asthma and Rhinoconjunctivitis—A MeDALL Project. Environ. Health Perspect. 2018, 126, 047005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toppila-Salmi, S.; Luukkainen, A.T.; Xu, B.; Lampi, J.; Auvinen, J.; Dhaygude, K.; Järvelin, M.-R.; Pekkanen, J. Maternal Smoking during Pregnancy Affects Adult Onset of Asthma in Offspring: A Follow up from Birth to Age 46 Years. Eur. Respir. J. 2020, 55, 1901857. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Mean Plasma sRAGE (pg/mL) ± SD | |||||
|---|---|---|---|---|---|
| Yes | N | No | N | p | |
| Asthma 7 years | 1875 ± 472 | 15 | 1794 ± 418 | 53 | 0.525 |
| Patient with inhaled treatment | 1893 ± 453 | 23 | 1771 ± 414 | 45 | 0.271 |
| Personal atopic status | |||||
| Aeroallergen sensitization | 1908 ± 494 | 16 | 1783 ± 406 | 52 | 0.309 |
| Eosinophilia | 1821 ± 380 | 30 | 1819 ± 465 | 37 | 0.981 |
| Environmental exposures | |||||
| Tobacco smoking in utero | 1478 ± 296 | 10 | 1870 ± 422 | 58 | 0.007 * |
| Passive tobacco smoking | 1772 ± 479 | 26 | 1837 ± 397 | 42 | 0.547 |
| Apartment | 1557 ± 372 | 11 | 1863 ± 427 | 56 | 0.031 * |
| Cat | 1774 ± 311 | 25 | 1834 ± 485 | 43 | 0.579 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magnier, J.; Julian, V.; Sapin, V.; Mulliez, A.; Usclade, A.; Rochette, E.; Evrard, B.; Labbe, A.; Coste, K.; Egron, C. Soluble Receptor of Advanced Glycation End-Products (sRAGE) in Pediatric Asthma: A Prospective Study in 68 Children Aged 7 Years. Appl. Sci. 2022, 12, 5926. https://doi.org/10.3390/app12125926
Magnier J, Julian V, Sapin V, Mulliez A, Usclade A, Rochette E, Evrard B, Labbe A, Coste K, Egron C. Soluble Receptor of Advanced Glycation End-Products (sRAGE) in Pediatric Asthma: A Prospective Study in 68 Children Aged 7 Years. Applied Sciences. 2022; 12(12):5926. https://doi.org/10.3390/app12125926
Chicago/Turabian StyleMagnier, Julie, Valérie Julian, Vincent Sapin, Aurélien Mulliez, Alexandra Usclade, Emmanuelle Rochette, Bertrand Evrard, André Labbe, Karen Coste, and Carole Egron. 2022. "Soluble Receptor of Advanced Glycation End-Products (sRAGE) in Pediatric Asthma: A Prospective Study in 68 Children Aged 7 Years" Applied Sciences 12, no. 12: 5926. https://doi.org/10.3390/app12125926
APA StyleMagnier, J., Julian, V., Sapin, V., Mulliez, A., Usclade, A., Rochette, E., Evrard, B., Labbe, A., Coste, K., & Egron, C. (2022). Soluble Receptor of Advanced Glycation End-Products (sRAGE) in Pediatric Asthma: A Prospective Study in 68 Children Aged 7 Years. Applied Sciences, 12(12), 5926. https://doi.org/10.3390/app12125926