1. Introduction
The coronavirus family has hundreds of virus types; although only seven are harmful to humans [
1]. Mammals such as bats transfer these viruses into the human body [
2]. The virus can transfer from one animal (or person) to another through the air and by physical interaction with a COVID-19 positive patient, i.e., handshaking [
3]. The COVID-19 virus causes an acute respiratory infection in people, and it has now become the world’s greatest pandemic. At first, the virus contaminated residents of Wuhan, China, in December of 2019 [
4]. The COVID-19 virus is lethal to humans due to its rapid propagation. The World Health Organization (WHO) has officially declared that COVID-19 is a pandemic [
5,
6]. COVID-19 indicators are high temperature, exhaustion, coughing, loss of taste, breathing difficulty, etc. [
7]. The virus usually affects the lungs in humans, producing pneumonia in extreme situations. As a result, the oxygen level in the body plummets. COVID-19 takes 3 to 13 days to grow, but symptoms in the patient’s body take 6 to 7 days to appear. So far, the WHO has documented 396,558,014 COVID-19 cases globally, with 5,745,032 losses [
8]. According to the Pakistani government, 1,531,242 cases of COVID-19 have been reported in Pakistan, with 30,381 fatalities and 1,498,017 recoveries [
9]. As a response to the unpredicted COVID-19 outbreak, numerous research centers’ research and innovation groups are working hard to create an accurate detection method and treatment vaccine [
10]. Researchers from various fields, such as machine learning, computer science, and artificial intelligence, collaborate to control and mitigate the epidemic by sharing their technical insights and alternative solutions [
11,
12,
13,
14,
15].
Moreover, existing COVID-19 detection tests are inefficient and require several hours to produce results. The antibody and polymerase chain reaction (PCR) test is usually used to identify COVID-19 around the globe. The antibody test, which is an indirect method of testing, can determine if the immune system has come into contact with the virus. Antibodies can take up to 9 to 28 days to form after an infection has taken hold, which is a long time. If the diseased person is not kept separate, the infection can spread. In most cases, PCR tests are used in medical research [
16,
17]. However, the number of patients continues to rise, and performing enough PCR testing has become difficult due to time constraints, a lack of medical resources, and the associated costs [
18,
19,
20]. A fundamental constraint of PCR tests is the high expense of importing the required chemicals and other ingredients necessary in the kits. One PCR test costs almost up to USD 30 (compared to Pakistani rupees), and the price varies depending on availability in different regions of the world. That takes us to the following constraint: availability; not every country has the exact needs and resources. Some states have a larger population and fewer kits available, while others have more kits than are needed. As a result of COVID-19, clinical laboratories have developed, tested, and implemented various virus detection approaches. It has been crucial in identifying patients, making isolation recommendations, and assisting with disease control. As the need for COVID-19 testing has expanded, laboratory professionals have run across a growing number of barriers, doubts, and, in some cases, disagreements. As a result, there is an urgent need to develop alternative testing (automated COVID-19 diagnosis) techniques that can reliably detect the virus in a short period and low cost, allowing patients to be identified and quarantined or isolated quickly. One of the alternative solutions is to use chest radiographs for COVID-19 detection. One radiograph costs approximately USD 3; therefore, we can obtain a large number of image samples to efficiently and correctly identify COVID-19 using chest radiograph images. Furthermore, the time required to conduct a chest radiograph is approximately 15 min compared to the PCR test.
An important aspect of home tests for COVID-19, which are relatively simple to perform and interpret, is the immediacy of test results, between 10 and 30 min. Previously, patients had to wait several days or more for results from commercial reference laboratories. There are several important issues regarding using and interpreting home COVID-19 tests. Foremost among these are obtaining a quality specimen and the performance of the test. The process for the consumer has been simplified by the manufacturer-provided visual aids, videos, or online guidance to assist in specimen collection and understanding test performance. For home emergency use, authorization from the Food and Drug Administration (FDA) required feasibility data showing that people in the authorized age ranges can safely and accurately perform these tests. Individuals performing these tests must read and follow the manufacturer’s instructions. Regardless of the test type, whether performed at home or in the laboratory, an inferior quality specimen often translates into inferior test results. Furthermore, positive results in asymptomatic individuals are less accurate and should be confirmed by more accurate tests. Additionally, home-based COVID-19 testing is not common globally, especially in underdeveloped countries. For example, currently, there is not a home-based COVID-19 testing facility in Pakistan. In contrast, the PCR-based COVID-19 facility is frequently available globally but is time-consuming compared to the proposed approach.
Furthermore, COVID-19 has been reliably detected in its initial stages using a variety of medical imaging modalities, including chest radiography, electrocardiogram trace images, and computed tomography (CT) scan. Medical practitioners place a higher value on chest radiograph images since they are easily accessible through radiology departments. According to radiologists, chest radiograph images aid in the precise knowledge of chest pathology. As a result, the X-ray modality [
21] is the first low-cost and low-risk approach for the COVID-19 analysis. The X-ray approach is an extensively utilized, most effective and accessible tool to identify and diagnose pneumonia [
22]. Pneumonia is an infection that inflames the lungs’ air sacs. X-ray serves an important role in clinical care and epidemiological studies. Detecting pneumonia in chest X-rays, on the other hand, is a difficult task that requires the presence of professional radiologists. We offer a model that can detect pneumonia from chest X-rays more accurately than experienced radiologists in this paper. X-rays are simpler, quicker, inexpensive, less harmful, and expose individuals to less radiation than CT and magnetic resonance imaging (MRI) [
23].
Recent research has shown that Artificial Intelligence (AI) methods employing deep learning (DL) methodologies can identify numerous disorders on chest radiographs with accuracy comparable to expert radiologists [
24,
25,
26,
27]. When experienced radiologists are unavailable, these computer-aided detection (CADs) systems can help with imaging-based patient classification in resource-constrained situations and increase practitioner’s chest radiograph interpretation accuracy and inter-reader variability [
28,
29]. Deep learning-based CAD has been shown in several recent studies to detect and identify COVID-19 on chest radiographs with high (radiologist-level) accuracy and to use it in medical practice [
30,
31]. DL approaches employ unstructured data, extract more significant features automatically [
32], and generate more accurate results than classic ML techniques. Several investigations were started at the beginning of 2020 to build automated DL models for reliable COVID-19 detection [
33]. Convolutional neural networks (CNNs) were employed in most of this research to classify and assess COVID-19-infected or normal chest X-ray pictures. To detect and identify brain tumors from magnetic resonance images (MRI) data, specialists can use CAD based on classical DL [
34]. CNNs are commonly used in image classification and identification applications such as MRI brain cancer image classification [
35] and others.
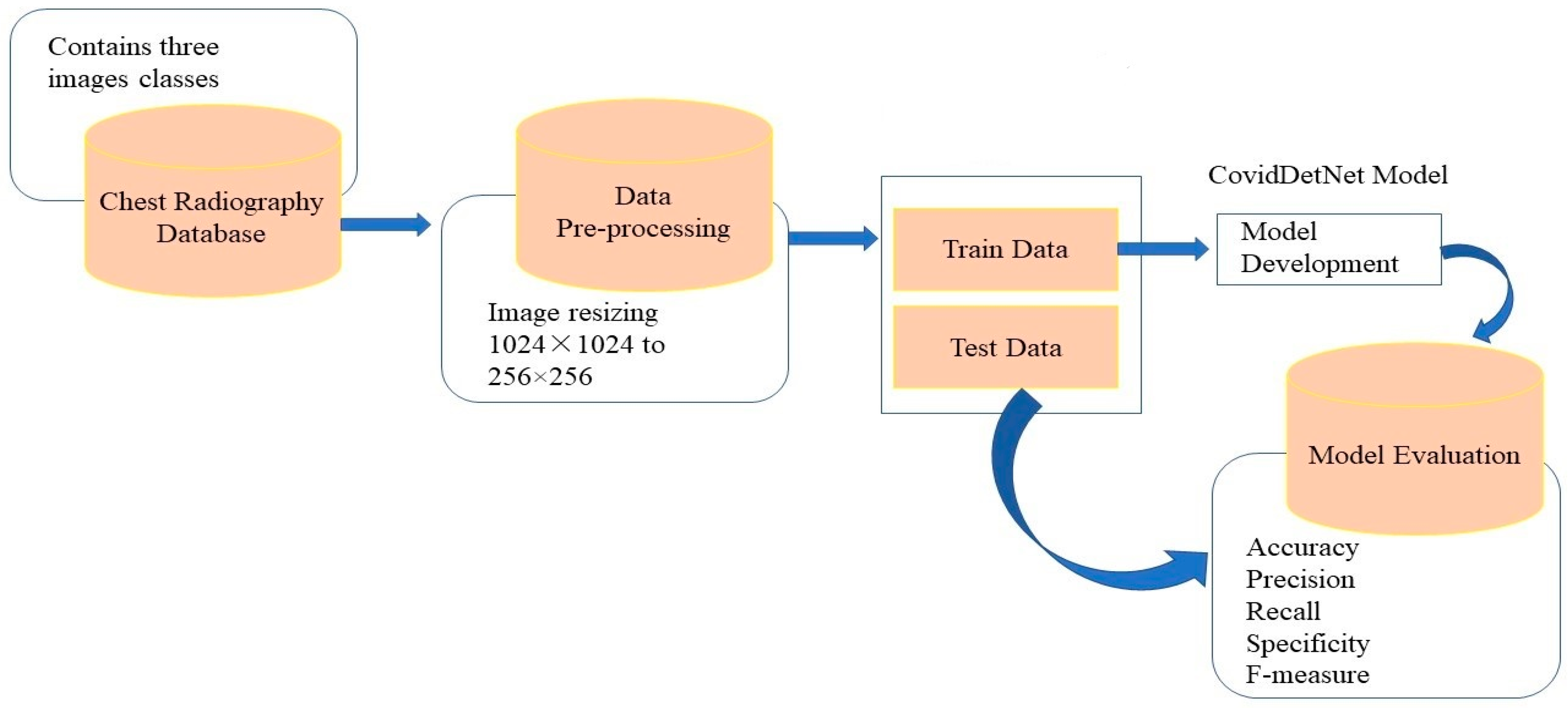
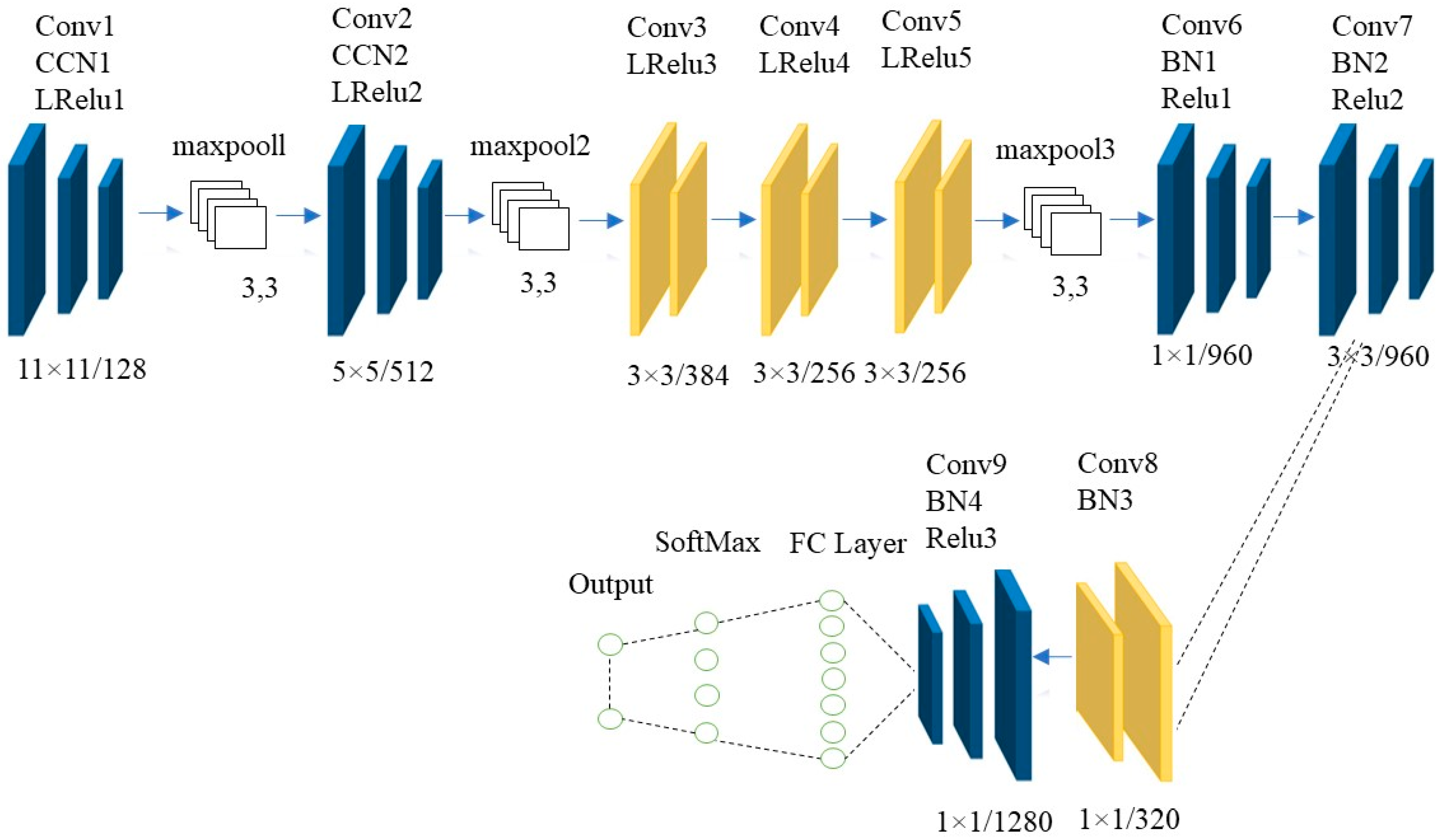
According to our knowledge, when it comes to AI-driven tools that use imaging techniques, COVID-19 does not have a lot of state-of-the-art literature. Existing COVID-19 detection research has certain limitations, i.e., low accuracy of COVID-19 detection. Most studies relied on datasets with fewer images (small datasets). There are fewer training data, the model is not perfectly generalized, and the training samples may have been overfitted. Most studies use classic ML and transfer learning algorithms to detect and assess COVID-19. Still, the most concerning limitation of traditional ML (such as support vector machine (SVM)) is the long training time for large datasets. In contrast, the most concerning limitations in transfer learning systems are negative transfer and overfitting. One of the drawbacks of using pre-trained classification approaches is that they are frequently trained on the ImageNet database, which contains images that are unrelated to medical images. As a result, putting in place effective CADS to reliably and quickly identify COVID-19 from chest radiographs remains a difficult task. To address these limitations, the CovidDetNet DL model is proposed. It utilizes filter-based feature extraction, which can help achieve high classification performance. The proposed model has been created with a convolutional layer and both ReLu and Leaky ReLu activation functions, which extract the most detailed and important features from the chest radiograph images. The architecture can minimize many weight parameters by using a max-pooling operation. We implemented both Relu and leaky ReLu activation functions and batch and cross channel normalization operations in the proposed model, making it a novel COVID-19 detection and classification method. The proposed approach also tackles the issue of PCR kit scarcity by requiring only an X-ray machine, which is currently found in most hospitals across the world. As a result, people will not have to wait longer for colossal PCR kit shipments. The proposed approach would efficiently enable the contact and isolation of COVID-19 individuals and limit community transmission with the rapid detection of COVID-19. Therefore, as chest radiographs are low-cost and time-efficient, and available in practically every clinic, chest radiograph images were utilized as a sample dataset in this study. The suggested architecture was validated using a standard Kaggle (publicly available) dataset. According to the results, the proposed structure performs satisfactorily in COVID-19 detection in test accuracy. The main contributions of this research are:
A CovidDetNet DL model is proposed to detect COVID-19 positive cases using chest radiograph images.
Chest radiographs are favored over CT scans since X-ray machines are readily available in most hospitals and CT scans emit less ionizing radiation.
To evaluate the efficacy of the proposed model, we compared the proposed CovidDetNet model performance with hybrid approaches on the same dataset and experimental configuration. For this purpose, we utilized various classification metrics, i.e., accuracy, precision, recall, and f1-score.
We evaluated the performance of the proposed novel CovidDetNet DL model on a standard COVID-19 radiography database.
The remainder of this paper is arranged as follows.
Section 2 presents the related work about COVID-19 detection methods. The motivation and description of the proposed work are discussed in
Section 3.
Section 4 explains the datasets, evaluation measures, and experimental results.
Section 5 discusses the proposed approach and explains the future directions and
Section 6 concludes the paper.
2. Related Work
Although COVID-19 has only just begun to spread, researchers have created a substantial number of research approaches in such a short time. To detect and classify COVID-19 images, which is still under research and needs further improvements, many ML, hybrid, and DL approaches have been presented in the literature. To highlight the critical literature work in COVID-19 detection and classification, below we discuss and analyze several related works on COVID-19.
Mahdy et al. [
36] used multi-level thresholding and an SVM approach to identify and detect COVID-19. They used a median filter to increase the input image contrast after analyzing the patient’s lung radiograph image. The Otsu objective function is then utilized to create a multi-level picture segmentation threshold. Next, the SVM was employed to distinguish between diseased and uninfected lungs. Using the proposed model, the authors achieved high average accuracy for classifying lung radiograph images than the existing approaches. Singh et al. [
37] introduced a research method based on the least-squares SVM (LS-SVM) and autoregressive integrated moving average (ARIMA) to detect and identify COVID-19. The study’s research data were obtained from the US, UK, Italy, France, and Spain, where most confirmed coronavirus cases occurred. The authors used different feature extraction methods to increase the performance of the proposed approach. The dataset is then fed into the algorithm that predicts the disease’s spread one month ahead of time. LS-SVM outperformed ARIMA in terms of accuracy. Based on the locality-weighted learning and self-organization map (LWL-SOM), Osman et al. [
38] proposed a novel COVID-19 detection method. They employed the SOM approach to group pictures from the chest radiographs dataset based on similar features in distinct clusters to distinguish between COVID-19 and normal patients. The LWL approach is then used to create a model for detecting COVID-19. The proposed model improved the correlation coefficient performance outcomes between COVID-19, normal, and pneumonia cases; pneumonia and normal cases; COVID-19 and pneumonia cases; and COVID-19 and normal cases. The proposed model improved the correlation coefficient performance outcomes. Current ML-based methods that use AI evaluation measures to distinguish COVID-19 and normal patients outperformed the proposed model. In [
39], the authors present a fusion scheme based on an ML system using three significant texture features, namely, local binary pattern (LBP), fractal dimension (FD), and grey level co-occurrence matrices (GLCM). In experimental results, to demonstrate the efficiency of the proposed scheme, we have collected 300 CT scan images from a publicly available database.
Furthermore, traditional ML approaches perform poorly compared to DL techniques because they rely heavily on manual feature extraction and adequate feature selection. In contrast, DL approaches use unstructured data, extract more robust deep features, and produce more accurate results than traditional ML algorithms. Recently, DL algorithms have been frequently employed to extract classification features automatically. Classifiers based on DL can be utilized to develop fully automated classifiers that can detect COVID-19 using chest radiograph images. Recently, Ozturk et al. [
40] proposed a binary classifier that recognizes COVID-19 and normal chest radiograph pictures and a multi-class classifier that detects COVID-19, pneumonia, and normal images using the DarkNet transfer learning (TL) architecture. Similarly, the Xception TL approach was utilized as a pre-trained network by Khan et al. [
41]. The tests were carried out on publicly available datasets. Apostolopoulos et al. [
42] used the MobileNet DL algorithm, trained the model from scratch, and extracted various classification features for COVID-19 classification. On the COVID-19 diagnostic, Ucar et al. [
43] used the Bayesian optimization method to optimize the SqueezeNet network. The COVID-19 images dataset has also been improved to improve its performance. Additionally, Okolo et al. [
44] employed eleven CNN models to classify chest radiograph images as belonging to healthy persons, people with COVID-19, or people with viral pneumonia. They analyzed three distinct improvements to modify the frameworks for the COVID-19 detection by expanding them with extra layers. All of the investigated networks are established frameworks that have been demonstrated to be effective in image detection and classification tasks. The proposed techniques were tested on a COVID-19 radiography database for all of the studied designs, with the EfficientNetB4 and Xception-based models providing the best classification results. Uddin et al. [
45] suggested a CNN-based model for detecting COVID-19 from chest radiograph images, making the test more effective and trustworthy. The proposed model used a TL technique and a bespoke model to improve accuracy. The pre-trained CNN models, such as InceptionV3, MobileNetV2, ResNet50, and VGG16, were utilized to extract deep features. The categorization and classification accuracy were utilized as a criterion for gauging performance in this study. According to the results of this study, DL can detect SARS-CoV-2 from CXR images. Out of all of these TL models, InceptionV3 has achieved the highest accuracy.
Aside from ML approaches and DL models, previous research has also used hybrid models that combine both classic ML and DL-based methodologies. Sethy et al. [
46] employed chest radiograph images to detect COVID-19 infected patients (deep feature and SVM-based approach) using a hybrid approach. For classification, SVM is used rather than a DL-based classifier because the latter requires a large training dataset. Deep features from the DL models’ fully connected (FC) layers are obtained and fed into the SVM for COVID-19 categorization and classification. The distant chest radiograph data sources used in the technique are pneumonia, normal, and COVID-19. The method aids medical practitioners in distinguishing between healthy people, COVID-19, and pneumonia patients. The SVM algorithm is evaluated for COVID-19 detection using the attributes of 13 DL frameworks. The best results were from ResNet50 and SVM algorithms. Based on chest radiograph image data, Novitasari et al. [
47] employed CNN architectures as feature extractors and the SVM as a classification tool to determine if the participants were normal, COVID-19 positive, or had pneumonia. The tests contrasted the kernel used, feature selection strategies, feature extraction frameworks, and different classes. The authors used resnet50, resnet18, resnet101, and googlenet TL approaches to separate three classes: normal, pneumonia, and COVID-19. They attained the maximum average accuracy using resnet50, resnet18, resnet101, and googlenet.
The studies mentioned above could be increased even further. Both the images sent to the model and the network’s architecture are beneficial in diagnosing COVID-19 infection. As seen above, traditional ML, CNN, transfer learning, and hybrid algorithms have all been employed to detect COVID-19. The primary goal of this study is to obtain satisfactory results in detecting COVID-19 instances while avoiding false positives. When the findings are analyzed, it is clear that the proposed method is effective and simple for COVID-19 detection.
5. Discussion and Future Research Direction
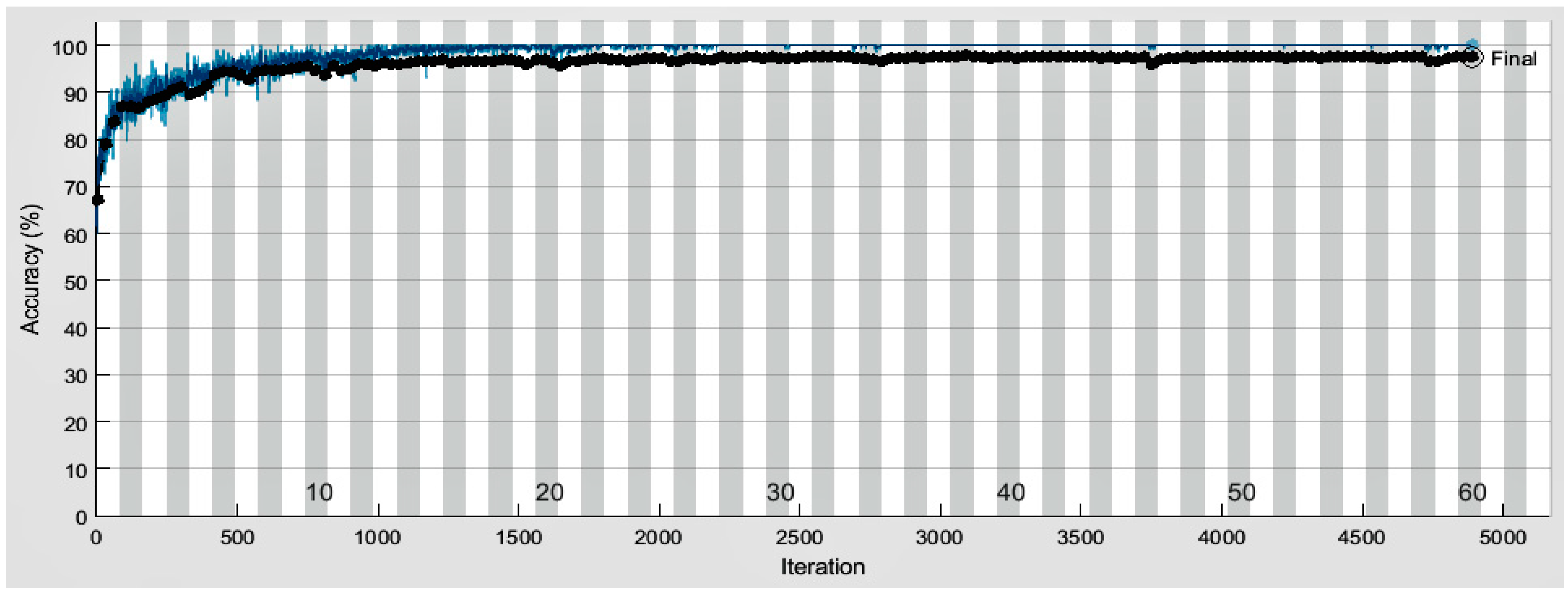
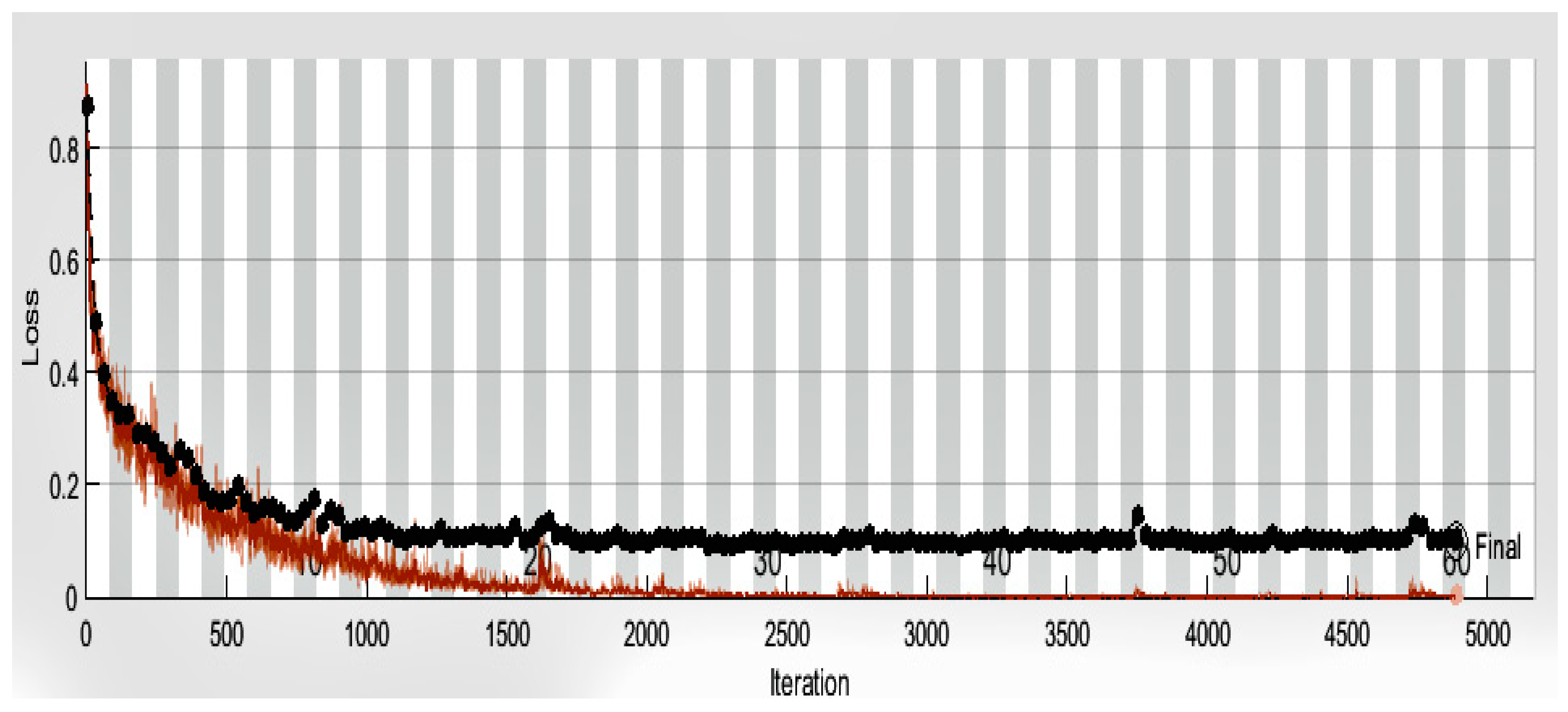
In this research, we have adopted a model with higher accuracy (98.40) than competing models in detecting COVID-19 from chest radiography. The training and testing accuracy of the model proliferates after each epoch, as shown in
Figure 4, and the training and testing loss decrease gradually, as depicted in
Figure 5. Although the prop approach yielded promising results, we recognized several limitations and made some recommendations for future research. Due to the unavailability of the research datasets that could be used as a baseline to investigate the severity level of COVID-19 infection, the proposed approach was unable to categorize the various stages of COVID-19 infection, such as pre-symptomatic, asymptomatic, moderate, and severe. The proposed method does not reveal how well the system detects COVID-19 using other imaging modalities such as computerized tomography (CT scans) and electrocardiogram (ECG) trace images. We continuously split image data into a 70% training set and a 30% test set in the proposed approach. Alternative splits, on the other hand, may produce different results. In the future, we plan to conduct experiments using comparable large-scale datasets of chest radiographs, CT scans, and ECG trace images to assess the models’ generalization ability by testing them on a range of large-scale datasets from diverse sources and images obtained by several machines. We want to use the same method to categorize the various stages of COVID-19 infection, such as pre-symptomatic, asymptomatic, mild, severe, and so on. According to the experimental results, the proposed CovidDetNet method is more accurate than PCR because PCR results rely heavily on sample collection timing, type, storage, handling, and processing. A false-negative result is possible if the sample is not properly obtained or if an individual is tested too early after exposure to the virus or too late in their infection. Therefore, in the future, we intend to provide further experimental evidence to compare the performance of the proposed system (CovidDetNet approach) with PCR and other manual COVID-19 testing methods to identify its performance in identifying COVID-19. The proposed CovidDetNet approach estimated accuracy might be biased or inflated because we used a dataset containing images with only three classes (normal, pneumonia, covid) for training and testing the proposed model. Therefore, in the future, we intend to use the proposed method in other COVID-19 datasets or other medical datasets with CT scans or chest radiographs to test the generalization ability of the proposed CovidDetNet model so that it can be used in practice to detect different diseases such as tuberculosis, breast cancer, and lung opacity, etc. Furthermore, the challenge faced by the machine and deep learning experts these days is the unavailability of relevant data. Currently, the dataset adopted for the proposed approach contains only three types of images such as normal, COVID-19, and pneumonia. Therefore, to generalize the proposed CovidDetNet approach, we need to evaluate it with other types of chest radiograph disease images. For this purpose, in the future, we need to explore the existing benchmark dataset of chest radiographs containing breast cancer, tuberculosis, and lungs opacity together with the COVID-19 detection. This paper only focuses on the approaches that use deep learning to detect and identify COVID-19 from chest radiograph images. In the future, we are interested in conducting an experiment with expert radiologists and identifying the proposed approach’s efficacy in identifying COVID-19. It is currently difficult to identify radiologist experts in the area where most of the authors reside. We claim that the proposed CovidDetNet approach can be used as a replacement for expert radiologists to timely identify COVID-19 and help stop the spread of the virus. Furthermore, to perfectly know the time gained comparing chest radiography with the proposed CovidDetNet approach, we need to experiment with the domain experts diagnosing COVID-19 from X-rays and compare the results and time taken with the proposed CovidDetNet approach. Additionally, to generalize the proposed CovidDetNet approach, we aim to test and validate the proposed approach with the emerging new variants of COVID-19 and record its performance and accuracy to identify the new types of COVID-19 virus. Additionally, we are interested to identify the performance of proposed approach on detecting & removing mask [
70] and heart disease predication [
71,
72].
Furthermore, healthcare institutions in many countries are incorporating a large number of smart devices for combating the disease and obtaining information about its growth. In addition, blockchain and IoT are also assisting medical professionals in gaining valuable insights about behavior and symptoms. At the same time, physicians are using various IoT-enabled devices for remote monitoring of patients, considering that COVID-19 spreads faster than the average communicable disease. In particular, the Internet of Medical Things (IoMT) applications involve tracking medication orders, monitoring COVID-19 patients remotely, and incorporating wearables for transmitting healthcare information to the respective healthcare professionals. The healthcare sector is banking on the potential of IoMT technologies to collect, evaluate, and transmit healthcare information efficiently. IoT devices can pacify the diagnosis process of infectious diseases, which is essential in the case of COVID-19. IoT-enabled devices can capture body temperatures, collect samples from possible cases, and eliminate human intervention. Even during the quarantine period, IoT devices can remotely monitor patients, preventing further infection. Even IoT-based drones are being used for thermal imaging, disinfecting, medical purposes, surveillance, and announcements to draw the line of defense against COVID-19. Therefore, there is a rising demand to develop deep learning models based on IoT and blockchain technologies—since both have significantly leveraged the global healthcare industry—to detect COVID-19 infection early from the data gathered from IoT-enabled devices.



 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}