Abstract
Patients with upper limb disorders are limited in their activities of daily living and impose an important healthcare burden due to the repetitive rehabilitation they require. A way to reduce this burden is through home-based therapy using virtual reality solutions, since they are readily available, provide immersion, and enable accurate motion tracking, and custom applications can be developed for them. However, there is lack of guidelines for the design of effective VR rehabilitation applications in the literature, particularly for bimanual training. This work introduces a VR telerehabilitation system that uses off-the-shelf hardware, a real-time remote setup, and a bimanual training application that aims to improve upper extremity motor function. It is made of six activities and was evaluated by five physiotherapists specialised in (2) neuromotor disorders and (3) functional rehabilitation and occupational therapy. A descriptive analysis of the results obtained from the System Usability Scale test of the application and a collection of qualitative assessments of each game have been carried out. The application obtained a mean score of 86.25 (±8.96 SD) in the System Usability Scale, and the experts concluded that it accurately reproduces activities of daily living movements except for wrist and finger movements. They also offer a set of design guidelines.
1. Introduction
1.1. Rehabilitation of Upper Limb Disorders
Upper limb disorders (ULD) represent a major concern for healthcare systems because of the considerable economic burden they generate [1]. Most patients with ULD are limited in their activities of daily living (ADL) and require a continuous rehabilitation process [2], whose aim is to restore the lost capabilities and range of motion. Due to the complex nature of this type of injury [3], there are discrepancies about the most effective intervention therapies for ailment. However, most physical intervention methodologies agree that the patient must perform strength and repetition tasks [4,5,6]. Such tasks enable the patient to work on various parts of the body in a structured and separate manner. However, strength and repetition tasks, by their own nature, do not train the patient in the complications inherent in the organization of whole limb movements. This fact hinders functional improvement in ADL and delays the eventual return of the patient to a productive and fulfilling life.
One of the major concerns involved in this type of rehabilitation is that the patients need to experience enough repetitions to induce the underlying neuroplastic adaptations necessary for their improvement [6]. For many patients, such a volume of therapy is economically unfeasible when it must be done in specialised centers and under the supervision of trained physicians. This is why conventional home-based therapy has become an alternative to extend the practice hours outside the clinic sessions and helps to establish a steady regime. However, most home-based therapy programs are monotonous and repetitive, resulting in a lack of motivation and reduced commitment from the patients [7]. This causes low adherence to treatment, which is crucial for achieving patient recovery. On top of that, such programs also lack the supervision of a therapist that can properly ensure that the exercises are correctly performed. Put together, these two facts are the reason that most home-based programs fail to influence the rehabilitation results in a noticeable way [8].
To try to mitigate this problem, several telerehabilitation solutions have been proposed. However, most are limited to offline monitoring by the therapist, telephone calls, or in some cases, videoconferencing [9,10,11]. There are more elaborate approaches that involve the installation of equipment in the patient’s home [12], designed and custom built specifically for this purpose, and they are therefore, expensive. To avoid this high cost, some authors have tried to use off-the-shelf products, such as video game consoles and peripherals. These solutions, due to their origin in gaming, were expected to increase the patient’s engagement. However, they are less than ideal for rehabilitation tasks, since commercial games and their peripherals have not been initially designed for the specific movements that the patient must perform [13,14] and are not yet sufficiently engaging for all patients [13,15]. In some cases, this gap cannot be bridged, due to the inability to develop custom software solutions or modify already available games for proprietary systems, such as game consoles. On top of that, these games are difficult to operate for patients [16].
On the other hand, the use of virtual reality (VR) systems used as complementing tools for rehabilitation and motor retraining have proven successful in promoting patient adherence to therapy and optimising therapeutic gains [17]. Indeed, virtual reality promotes adherence to physical activity (PA), whether commercial or customisable games are used. One study [18] pointed out that the adoption of home-based virtual rehabilitation at home for patients with neuromotor disabilities could be enhanced by using commercial games, but only if these detect compensatory movements, integrate social platforms, provide kinematic reports, and track the patient’s progress. However, the development of purpose-built VR games allows one to provide task-oriented exercises, and visual and auditory feedback regarding the performance of the patient’s PA [19], which could lead to neuromuscular reeducation and functional improvement [20]. The studies of Wu et al. (2019) [21] and Tarakci, E. et al. (2019) [22] evaluated the effectiveness and feasibility of their VR solutions for hand and upper extremity rehabilitation, respectively, using Leap Motion, a commercial device that enables hand recognition. Their findings pointed out that movements learned in VR environments can be transferred to real-world equivalent tasks in most cases, and that VR engages the player to increase the rehabilitation intensity.
Taking all these facts into account, the benefits that VR telerehabilitation solutions can provide are usually dampened by the use of expensive equipment and/or the need to rely on commercial games. Therefore, it is necessary to build solutions that (a) use off-the-self low-cost hardware VR devices instead of costly and custom equipment, and (b) employ software applications specifically designed for the rehabilitation tasks instead of commercial games.
The main novelty of this work is that it objectively defines the actions and ranges of movement that must be achieved in each VR game for upper limb rehabilitation of bimanual ADL movements. This clarity in the design represents a guideline not found to date in the literature for the construction of virtual environments (VEs) for functional rehabilitation. Additionally, of course, this VR application is supported by a real-time remote system using a novel feasible methodology for video compression.
1.2. Hardware Selection Considerations
Concerning the hardware, most existing game-based therapies focus on two fundamental features: to induce as much immersion as possible and to accurately track the movements of the patient. The former improves the user’s engagement in a task that is eminently physical (increases the adherence to treatment), whereas the latter is necessary for assessing if the movements have been properly performed (reduces the need for supervision by a therapist).
To accurately capture the movements of the patient during the rehabilitation session, it is desirable to use sensors with six degrees of freedom (movement and rotation in the three axes). This is why the Kinect™ device is one of the most widely-used systems for motion capture in the field of physiological therapy [23,24].
Virtual reality devices, by their own nature, are capable of very accurate motion capture, since precise tracking of the user’s head and hand movements is required for an immersive simulation, which is precisely the other criterion listed before. Therefore, VR provides reliable and precise data about the hands and head motions, and at the same time, produces an immersive simulation. On top of that, unlike other commercial closed solutions, such as video game consoles, it is easy to develop and distribute custom software for most VR devices.
Although VR headsets have their drawbacks (for instance, they may be challenging to use for some stroke survivors and cerebral palsy patients [25]), rehabilitation solutions based on immersive environments are more effective than traditional [26] because they:
- Improve the engagement of the patient: Exergames increase the energy expenditure of the patient and involve both cognitive and physiologicaly rewarding tasks [27], improving the adherence to treatment.
- Provide physical fidelity to real movements: The patient performs motions similar to those needed for analogous daily life situations.
- Provide cognitive fidelity to a real situation: The patient completes activities inside an environment designed to be similar to the real world.
Therefore, it is expected that an immersive VR solution for telerehabilitation will increase the patient’s adherence to treatment and improve the fidelity of the movements performed. However, such a solution requires not only the use of a VR head-mounted display (HMD), but also a high-performance computer that renders the virtual experience and sends the movement and session information to the therapist. Such a computer could be a considerable expense—an economic barrier to access that limits this solution.
1.3. Designing Gamified Virtual Reality Content For Rehabilitation
Despite there being currently no standardised criteria for the selection of commercial games for rehabilitation, some literature reviews have succeeded in establishing general guidelines to support the selection of systems [28] and games based on therapist and patient needs [5,18]. These guidelines are designed to evaluate how well existing VR commercial games can be adapted to a rehabilitation scenario; these frameworks focus on characterising the degree to which software and task parameters can be controlled so the therapeutic goals are achieved. As such, they do not aim to guide the design of newly developed VR applications for rehabilitation. However, the aspects they focus on offer valuable lessons that must be taken into account. This is especially important when we consider that clear strategies for the development of home-based rehabilitation therapies based on VR technologies have yet to be determined.
Taking these lessons into account, we can see that VR scenarios must implement motivational strategies based on self-determination and task-oriented challenges [19,29]. Such strategies stimulate the self-improvement of the individual and increase the patient’s autonomy [30,31] during the practice. Game mechanics based on them have shown that increasing the user’s engagement leads to more practice and also to higher quality practice [18].
Concrete guidelines for the design of effective rehabilitation games that go further than that are still not present in the literature. This lack of guidelines in the design of VR and augmented reality (AR) content has also been pointed out in the field of physical exercise for the older population [32]. Moreover, many rehabilitation solutions present in the literature that use the term “VR” are non-immersive applications in which the user sees a representation of their own body on a computer monitor [26,27,33,34,35]. This terminology problem is exacerbated when looking for design guidelines for what is now being called "fully-immersive VR" in the literature, since these solutions are not thoroughly explored in the field of functional rehabilitation.
On top of that, the VR-based solutions present in the literature are not focused on bimanual training. This is especially important for this work, since most ADL tasks typically involve asymmetrical bimanual movement [36]. There was an study [37] that focused on bimanual training, but again, not with a VR solution. Game design approaches for bimanual rehabilitation systems in VR are still unexplored, and there is a lack of guidelines that can guide their development.
This work introduces a VR telerehabilitation system that uses off-the-shelf hardware and a newly developed application: FarmDay. This application aims to enhance the bimanual upper extremity motor function of patients with ULD. Its design, due to the aforementioned gap in the literature, was guided by the expert opinions of practicioners and evaluated by them. This way, a set of design principles for the development of VR-based rehabilitation solutions and a collection of valuable lessons learned can begin to form.
2. Material and Methods
The solution developed for this work (named FarmDay) addresses the need to integrate VR exercises with a functional component inside an existing rehabilitation programme, currently performed in a clinic by therapists. It is hoped that these VR exercises will enable a telerehabilitation setup that the patients can use to increase their volumes of work without needing to leave their houses. This rehabilitation programme focuses on patients that have suffered a stroke or other neurological damage.
Various research studies have confirmed that exercises aimed at improving ADL have greater acceptance among adults, increase motivation, and improve adherence to the treatment [38,39,40]. Therefore, the exercises developed must have an intentional goal that makes the user perform one or more of the functional movements present in ADL.
2.1. VR Real-Time Remote System
As previously stated, one the main drawbacks of a VR solution is the need for an expensive high-performance computer that renders the VE and relays the session’s information to the therapist. To avoid this problem, the FarmDay application was designed to run on top of a real-time, remote VR system.
The details of this system are out of the scope of this document, but its architecture can be explained briefly. In this real-time, remote VR system, the VR application runs on a remote high-powered cloud computer (the server), from which the rendered environment is encoded and streamed to a less powerful computer at the patient’s home (the client), which in turn is connected to the VR HMD and controllers. This is possible through the use of an elastic down-sampling video compression codec [41]. This architecture relies on the continuous transmission of HMD and controller positions and interaction events from the client to the server. This way, the results of the interactions can be computed on the server and the video image relayed to the client. Figure 1 shows the architecture of this real-time, remote VR system. The FarmDay application is, therefore, run in the cloud server but used by the patient at their home. This way, the cost of running this setup for the user is greatly reduced.
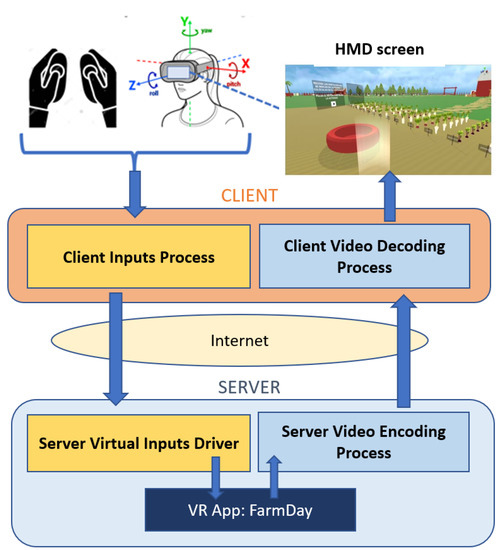
Figure 1.
Diagram of the the real-time, remote VR system architecture.
Every VR application designed to use this system must use the OpenVR libraries, since it must use four custom components developed for it:
- A client inputs process that captures the HMD and controllers inputs and sends them to the server.
- A server virtual inputs driver that receives the input data from the client and feeds them to the actual VR application running in the server (in this case, FarmDay).
- A server video encoding driver that captures the rendered VE product of these interactions, encodes it, and sends it to the client.
- A client video decoding process that receives the encoded video, decodes it, and shows it in the client’s HMD.
2.2. VR Application
The FarmDay application was developed using the Unity3D game engine v.2019.2.13f, mainly using the collection of scripts and predefined elements of the Virtual Reality ToolKit (VRTK) v.3.3.0 framework. This open source toolkit was used to implement the virtual space locomotion, object grasping interactions, object interaction via pointers, 3D button interactions, and 3D body physics within the virtual space.
- (i)
- VR framework and platform
As stated before, and due to the custom real-time remoting system developed in OpenVR, it was consequently determined that the VR application should be built for systems compatible with the OpenVR platform. Then, FarmDay was designed for the OpenVR SDK (Software Development Kit), so the real-time remote system can be used. The VR application was developed entirely as a single Unity scenario. In this 3D scenario, six activities are distributed through specific areas of the environment. For interactive actions and locomotion control, the VRTK prefab module was used. The VR solution generated supports the HTC Vive™ and Oculus Rift™ platforms’ controllers, which are used for the interactions.
- (ii)
- Gamification elements
The gamification strategy of the activities included in the FarmDay experience is based on goal achievement. Thus, each activity is composed of a sequence of actions that the user must perform to complete the task. The achievement of these objectives implies that the motions of the different body segments involved in the ADL functional movements were properly performed.
- (iii)
- Design of activities
Of the six activities offered by the application, three are based on real-life situations and were designed following the guidelines and advice of five physiotherapists specialised in neuromotor disorders from the Spinal Cord Injury Foundation (Fundación de Lesionado Medular, FLM) and CEU San Pablo University (Universidad San Pablo CEU, USPCEU). They are hand-washing, pouring a drink, and playing the piano.
The three remaining activities were themed around farm life and designed to involve movements similar to ADL. They are animal caring, picking apples from trees, and picking vegetables up off the ground. This way, the user can perform a bigger variety of exercises, hopefully increasing their adherence, reducing the feeling of boredom, and allowing them to work on similar movements in different ways.
- (iv)
- User Interaction
The FarmDay application begins by placing the user at the entrance of the farm, allowing them to explore the environment by moving around the delimited physical space, either by directly walking or by using a teleport functionality that can be activated with any of the two controllers. Additionally, game selection panels have been distributed throughout the environment. Through them, the user can teleport from one activity to another without having to physically traverse the VE.
These game selection panels consist of six interactive buttons that react when pressed with the controller, moving the user to the zone of the selected activity. The zone for each activity has a floating transparent panel which shows the objective of the activity and contains a play button. When the user presses the play button (by moving their hand), this game panel fades out and the activity starts. Once the activity is completed, the game panel fades in again, allowing the user to repeat the activity as many times as desired, restoring all the environment elements to their initial positions.
Design of Activities
Since each of the six activities aims to make the user perform movements specific to a particular ADL, it was essential to identify such movements. It was also necessary to determine the range of motion (ROM) for each joint (neck, shoulder, elbow, and wrist) and action, to make the tasks’ movements as faithful as possible to what the user would do in a real-world ADL. A recent state-of-the art review of devices for performing physical therapy at home or assisting with ADLs identified at least 15 systems that employ VR feedback, and in most of these cases, wrist support (ROM assessment), and in a few cases grip function, was considered [42]. No further information on finger movements is given. Therefore, the definition of the virtual scenarios and the placement of the interactive virtual objects were done in such a way so the user must reach a certain ROM for each joint to actually perform the tasks. All six virtual scenarios are depicted in Figure 2.
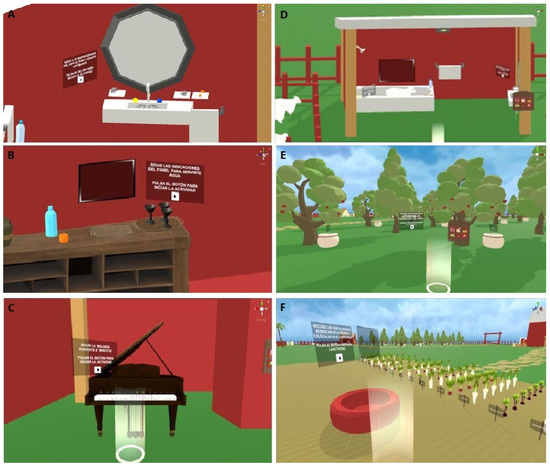
Figure 2.
Virtual environments for the activities. (A) The cabin area for the hand-washing activity, consisting of a faucet, a mirror, and the interactive objects: gloves and soap. (B) The barn dinning area for the pouring a drink activity. (C) The interactive keyboard for the playing the piano activity. (D) The toilet cabin area for the animal caring activity. (E) The forest area for the picking apples from trees activity. (F) The orchard field area for the picking vegetables up off the ground activity.
By applying inverse kinematics to the controllers’ positional and rotational data, the ROMs in the sagittal and horizontal planes of these body joints were evaluated. Table 1, Table 2, Table 3, Table 4, Table 5 and Table 6 detail the sequence of actions to be performed in each activity, the movements of the upper limb, and the ROMs involved for each joint. Each activity is further described in detail.

Table 1.
Sequence of actions and the upper limb movements involved in the hand-washing activity.
Table 2.
Sequence of actions and the upper limb movements involved in the pouring a drink activity.
Table 3.
Sequence of actions and the upper limb movements involved in the playing piano activity.
Table 4.
Sequence of actions and the upper limb movements involved in the animal caring activity.
Table 5.
Sequence of actions and the upper limb movements involved in the picking apples from trees activity.
Table 6.
Sequence of actions and the upper limb movements involved in the picking vegetables up off the ground activity.
Hand-washing activity: In this task, the user must follow the instructions shown in the mirror, step by step, to complete the action of washing their hands. The user is located in front of the toilet cabin and must move to stand in front of the sink, whose tap can be opened and closed by interacting with the yellow and blue buttons. Small shelves are placed to the left and right of the tap. On top of those shelves there are objects that must be reached: gloves and soap (see Figure 2A). The height and distance of these shelves and the buttons on the faucet are configured according to user’s position to ensure the proper shoulder extension, elbow movements, and wrist rotations (see Table 1).
Pouring a drink activity: In this task, the user must follow the instructions shown on the board, step by step, to complete the actions of pouring water into a glass and drinking from it. Initially, the user is placed in front of the bar where the interactive objects (bottle, glass and wooden board) are placed (see Figure 2B). They are arranged at a comfortable height and a distance appropriate to perform the flexion movements at the elbow, shoulder, and wrist to reach the objects; and elbow pronation and wrist movements to grab the objects (see Table 2).
Playing the piano activity: In this task, the user stands in front of the piano keyboard. The height of the piano is set to allow the subject to perform the elbow, shoulder, and slight wrist flexing movements (see Figure 2C). To complete the activity, the user must follow the melody for 2 min. This involves pressing the keys shown on the score panel (see Table 3).
Animal caring activity: In this task, the user must follow the instructions on the board, step by step, to complete the action of showering a sheep. Initially, the user is located in front of the bathtub (see Figure 2D). The interactive objects (buttons to activate the bathtub tap, soap bottle, and brush) are placed on the shelf of the shower or the floor, allowing the movements of flexion of the shoulder, the elbow, and the wrist, and internal rotation of the shoulder and elbow pronation to pour the soap on the sheep. Additionally, the brushing action induces elbow abduction (ABD) and adduction (ADD) movements and wrist radial-ulnar rotation movements (see Table 4).
Picking apples from trees activity: This task asks the user to pick as many apples from the trees as possible in 2 min and place them in the baskets next to each tree (see Figure 2E). To do this, the user must move to each tree. The collection of the apples from the tree and the placement of these in the baskets involves movements of flexion and extension of the elbow, shoulder, and wrist. Additionally, this action induces shoulder ABD/ADD movements. On top of that, the task forces the user incline their neck tilt, for gaze redirection (see Table 5).
Picking vegetables up off the ground activity: This task asks the user to collect the vegetables indicated on the board and place them in a red basket. Once the correct vegetable is picked and placed, the new vegetable to be picked is shown on the board. There is no time limit for the picking action for each vegetable, so this activity lasts as long as the user needs to pick all the vegetables listed. This list varies randomly (5 to 10 elements) each time the task is started. Thus, the user will have to move to a particular row of vegetables inside a zone defined prior to the start of the VR application. The reach to the vegetables on the ground and the placement of these in the red basket induce elbow and shoulder extension movements, wrist flexion, and raldial-ulnar deviation movements to grab the objects, along with the flexion of the neck for gaze redirection (see Figure 2F).
2.3. Usability and Design Evaluation
Five experts from FLM and USPCEU were asked to test the VR application. These experts were all physiotherapists specialised in neuromotor disorders. For these tests, a SteamVR room was set up to delimit a 3 × 2 m2 free movement physical area. The HTC Vive™ HMD and controllers were used. Before starting, they were instructed on how to use the controllers to teleport, grab objects, and interact with them. Then, they were asked to perform all six activities of FarmDay in an order of their choosing.
To evaluate the ability of the activities to achieve rehabilitation for specific actions, a customised, open-ended, non-scaled qualitative response survey was developed based on human–computer interface acceptability standards [43]. After performing their test, for each activity, the experts were asked “Does the activity allow for the movements required for the rehabilitation of this action? If the answer is negative, please indicate the aspects that need to be improved.” This way, in the case of a negative answer, the expert was asked whether the movement/interaction could be performed in another way and which modifications could be made to improve the activity.
To evaluate the ease of use of the VR experience, a Standard Usability Scale (SUS) questionnaire was also included [44,45].
3. Results
Table 7 and Table 8 show the experts’ answers to the qualitative response survey’s questions. In those cases in which the experts confirmed that the activity permitted the performance of the functional ROMs identified for each action, the answer was “The activity is adequate”.
Table 7.
Results of activities’ evaluation by FLM experts.
Table 8.
Results of activities’ evaluation by USPCEU experts.
To interpret the SUS score, it must be converted to a percentile rank. The outcomes from the experts’ evaluations are shown in Table 9. Based on the distribution of all scores, a raw SUS score of 86.25 converts to a percentile rank of 86.25%, which objectively means that the evaluated system has a higher perceived usability than 86.25% of all products tested.
Table 9.
Results of the System Usability Scale.
4. Discussion
4.1. Game Design Evaluation
As can be seen in Table 7 and Table 8, the consulted experts tended to agree on several points. On the positive side, all experts (5/5) concurred that the three activities designed around the farm life theme are adequate for the corresponding ADL movements. As explained in Section 2.2, these were not initially proposed by the experts. Instead, they were explicitly designed to involve ADL movements, their representativeness of real-life situations being only a secondary concern. This shows that having the ability to decide on the movements first and then planning an activity around them afterwards helped the designers to achieve higher movement accuracy. Therefore, if possible, this should be the approach followed by designers of future VR scenarios. Moreover, the positive response of the experts precisely to the activities that were not suggested by them showed that they welcome such an approach.
Looking at the answers to the these activities, three of the experts were not concerned that the tasks involve movements in addition to those specifically targeted: USPCEU2 favoured the crouching exercise in the picking vegetables activity, USPCEU3 liked the shoulder ABD/ADD movements in the animal caring activity, and USPCEU2 indicated that the raising of the arms above the head in the picking apples activity is desirable. This shows that the designers of tasks focused on inducing ADL movements should not be concerned about expanding them to also cover other movements.
The three initially proposed activities were not perceived as totally adequate for the real movements: 5/5 experts found one inaccuracy with the playing the piano activity, 4/5 experts with the hand-washing activity, and 3/5 experts with the pouring a drink activity. For these activities, the experts were concerned about certain limitations on the wrist and finger movements, with the former being present in the hand-washing and the pouring a drink activities, and the latter in the pouring a drink and playing the piano activities.
In particular, the hand-washing activity was implemented with the strategy of grabbing a pair of gloves instead of offering a realistic simulation for the hands of the user. This means that the movements of rinsing the hands under the tap induce slightly forced wrist rotations with respect to the natural movements. To solve this problem, it would be ideal to replace the controllers with a hand tracking controlerless setup for this specific exercise.
A similar problem was observed in the simulation of bringing the glass of water to the mouth. Although the hand and controller are assessed as being close to the user’s headset, the need to perform the wrist rotation movement involved in tilting the glass to empty the water is not evident. This is mainly attributed to the following facts: First, the application simulates emptying the glass at a horizontal distance of 6 cm from eye level to prevent the user from bumping the controller against their HMD. Second, the grabbing of the glass involves an object snap, so that the position of the object is consistent with the movement. Therefore, the user does not feel the need to rotate the wrist any further.
Concerning the finger movements, the experts specially miss them in the playing the piano activity. This indicates that this activity is not suitable for VR controllers, and as with the hand-washing movement, it would be ideal to replace the controller with a hand tracking setup. Two experts also indicated the inaccuracy of the finger movements in the glass grabbing part of the pouring a drink activity. The VR application expects the user to press the trigger button to grab the glass, since this act induces flexion–extension movements in the index finger, but they considered that this was not suitable enough. However, one expert stated positively that in the playing the piano activity, each musical note was represented by three keys in the keyboard (see Figure 2). This has the potential to allow the physiotherapist to evaluate whether the precision of the movement of tapping a single key was accurate or not without interrupting the task. This design could be exploited from the point of view of motion analysis.
Therefore, it can be seen that the tested setup (HTC Vive™ controllers) is not particularly adequate for wrist and finger movements. According to the expert’s opinion, for such tasks, a designer should take into account that a hand tracking setup would be probably better suited. With that said, a study of telerehabilitation using HTC Vive™ devices [37] has shown that the handling of these controllers improved finger extension, so further testing is needed in this regard.
4.2. Bimanual Interaction and Hand Movement
A central principle to the design of the six activities was the bimanual interaction, since this approach provides greater freedom of movement to the user and offers a context particularly faithful to that found in the ADLs. Therefore, this work combines a task-oriented strategy [29] with bimanual coordination. In the future, it would be interesting to explore if this approach offers an improvement in the effectiveness of functional training in comparison to the more commonly used approach of movement restrictions. One study [37] showed significant evidence of improvement in bilateral movements derived from intervention with bimanual interaction, but more studies are needed. This is a gap in the literature that was identified in Section 1.3. However, future work should consider dissociated finger movements using hand tracking and gesture detection systems to enable this improvement. In fact, the integration of systems such as Leap Motion could solve the analysis of finger movements. Although the studies reviewed by Pererira et al. (2020) [19] implemented hand movement tracking, none took advantage of this feature, with the exception of Wu et al.’s [21] work, which used Leap Motion for validation of wrist flexion and extension and radial and ulnar deviation. Therefore, although the current study has not been able to contribute to this aspect, we identify that further work is needed in this area.
4.3. Usability Outcomes
According to the results of the System Usability Scale questionnaire for the application, where the average value was 86.25 (SD = 8.96) and the minimum SUS score obtained was 75.00/100.00, FarmDay was accepted by the experts, and its ease of use can be rated as excellent [45], as shown in Figure 3. From this assessment, it can be inferred that the design of the VE; the distribution of the activities; and the intuitive way of interacting and the gamification strategy in each activity are adequate for this purpose. The design of the experience is focused on being easy to handle and on making it simple for the user to quickly learn the mechanics of each activity. This is relevant, since the existing literature has stated the need to incorporate patient-centred methodologies and ADL-enhancing games in telerehabilitation approaches [35]. Therefore, when designing activities similar to those presented in this work, it is important to focus not only on the generation of ADL-enhancing games themselves [46,47], but also on their ease of use for patients with ULD, an aspect that can be evaluated with the rating provided by the System Usability Scale.
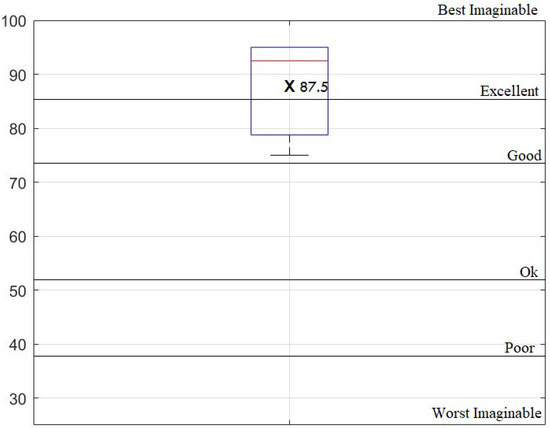
Figure 3.
Boxplot of System Usability Scale outcomes, overlapped with the 7-point adjective SUS scale interpretation [45].
4.4. Limitations
Finally, several methodological considerations have to be made. Although the work presented here was a study of the usability and feasibility of the application, only professional input was considered. In this area, clinicians’ expertise is considered to be more important than users’ perspectives [48], since in the neurorehabilitation field, the physiotherapist has better knowledge about how to implement an effective rehabilitation programme. On top of that, they are involved in the direct delivery of the rehabilitation process. Nevertheless, future studies with patients with ULD are needed to corroborate that the proposed VR application contributes to the physical improvement of the upper extremity and manages to motivate and maintain adherence to the rehabilitation treatment. Such a study could be made possible by the real-time, remote VR setup presented, which reduces the cost of deploying such a solution at the patients’ homes. This is aligned with the literature’s suggestion [46] to provide feasible solutions for telerehabilitation, allowing the patients to benefit from social care and home-based rehabilitation [35].
5. Conclusions
This work introduced a VR telerehabilitation system that uses off-the-shelf hardware, a real-time remote setup, and a bimanual training application that aims to improve the upper extremity’s motor function. It is made of six activities and was evaluated by five physiotherapists. Two of them specialised in neuromotor disorders at Fundación de Lesionado Medular and three of them specialised in functional rehabilitation and occupational therapy at CEU University. The definition of the sequences of actions and the range of movement for each joint and action for all six VR games for bimanual ADL exercises have been established. From the evaluation of this solution, it can be concluded that all six activities could be used for upper limb functional rehabilitation, with the exception of wrist and finger movements. Except for these caveats, the experts agree that the activities enable the user to perform suitable upper limb ADL-exercises in a realistic and immersive context. On top of that, the authors believe that this discussion offers a set of valuable lessons that can be applied to any future design of a VR application for rehabilitation of patients with ULD, particularly for bimanual interaction. Finally, the high usability score of the application reflects the reliability of the virtual reality tool for patients with UDL.
Author Contributions
A.R.: conceptualisation (equal); study implementation; software (lead); formal analysis (lead); writing—original draft (lead). J.Á.S.-P.: writing—review and editing (equal). Á.S.-P.: writing—review and editing (equal). R.R.: writing—review and editing (equal). R.G.-C.: conceptualisation (lead); writing—original draft (supporting); writing—review and editing (lead). All authors were accountable for the final version of the article. All authors have read and agreed to the published version of the manuscript.
Funding
The study was funded by the Spanish Ministry of Science, Innovation and University, under the grant European Regional Development Fund (ERDF) with project reference IDI-20191120, and also by the SPANISH GOVERNMENT (FEDER/Ministry of Science and Innovation/AEI), grant number RTI2018-097122-A-I00.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We want to thank our collaborators at Nokia Spain S.A. and Fundación Lesionado Medular for their help during the development of the JIRAFA research project.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ABD | Abduction |
| ADD | Adduction |
| ADL | Activities of Daily Living |
| FLM | Fundación Lesionado Medular (Spinal Cord Injury Foundation) |
| HMD | Head-Mounted Display |
| ROM | Range of motion |
| SDK | Software Development Toolkit |
| SUS | System Usability Scale |
| ULD | Upper Limb Disorders |
| USPCEU | Universidad San Pablo CEU |
| VE | Virtual environment |
| VR | Virtual Reality |
| VRTK | Virtual Reality ToolKit |
References
- Huisstede, B.; Bierma-Zeinstra, S.; Koes, B.; Verhaar, J. Incidence and Prevalence of Upper-Extremity Musculoskeletal Disorders. A Systematic Appraisal of the Literature. BMC Musculoskelet. Disord. 2006, 7, 7. [Google Scholar] [CrossRef] [PubMed]
- Cha, R.; Kim, J.Y.; Gu, W.H.; Lee, S.A.; Jung, B.K. Towards the Development of telerehabilitation System Based on Virtual RealityEnvironment and Cloud Service. Adv. Sci. Lett. 2017, 23, 12807–12811. [Google Scholar] [CrossRef]
- Raghavan, P. Upper Limb Motor Impairment After Stroke. Phys. Med. Rehabil. Clin. N. Am. 2015, 26, 599–610. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.S.; Park, M.J.; Yoon, I.J.; Park, S.H. Effects of virtual reality on upperextremity function and activities of daily living performance in acute stroke: A double-blind randomized clinical trial. NeuroRehabilitation 2011, 31, 379–385. [Google Scholar] [CrossRef]
- Howard, M.C. A Meta-Analysis and Systematic Literature Review of Virtual Reality Rehabilitation Programs. Comput. Hum. Behav. 2017, 70, 317–327. [Google Scholar] [CrossRef]
- Cheung, K.L.; Tunik, E.; Adamovich, S.V.; Boyd, L.A. Neuroplasticity and virtual reality. In Virtual Reality for Physical and Motor Rehabilitation; Weiss, P., Keshner, E., Levin, M., Eds.; Springer: New York, NY, USA, 2014; pp. 5–24. [Google Scholar]
- Burdea, G. Keynote address: Virtual rehabilitation-benefits and challenges. In Proceedings of the 1st International Workshop on Virtual Reality Rehabilitation (Mental Health, Neurological, Physical, Vocational) VRMHR, Lausanne, Switzerland, 7–8 November 2002; pp. 1–11. [Google Scholar]
- Syed, U.E.; Kamal, A. Video game-based and conventional therapies in patients of neurological deficits: An experimental study. Disabil. Rehabil. Assist. Technol. 2021, 16, 332–339. [Google Scholar] [CrossRef]
- de Araújo, A.V.L.; Neiva, J.F.D.O.; Monteiro, C.B.D.M.; Magalhães, F.H. Efficacy of virtual reality rehabilitation after spinal cord injury: A systematic review. BioMed Res. 2019, 2019, 7106951. [Google Scholar] [CrossRef]
- Kizony, R.; Raz, L.; Katz, N.; Weingarden, H.; Weiss, P.L.T. Video-capture virtual reality system for patients with paraplegic spinal cord injury. J. Rehabil. Res. Dev. 2005, 42, 595–608. [Google Scholar] [CrossRef]
- Trincado-Alonso, F.; Dimbwadyo-Terrer, I.; de los Reyes-Guzmán, A.; López-Monteagudo, P.; Bernal-Sahún, A.; Gil-Agudo, Á. Kinematic metrics based on the virtual reality system toyra as an assessment of the upper limb rehabilitation in people with spinal cord injury. BioMed Res. Int. 2014, 2014, 904985. [Google Scholar] [CrossRef][Green Version]
- Cano de la Cuerda, R.; Munoz-Hellin, E.; Alguacil-Diego, I.; Molina-Rueda, F. Telerrehabilitación y Neurología. Revista de Neurología 2010, 51, 49–56. [Google Scholar] [CrossRef]
- Saposnik, G.; Levin, M. Virtual reality in stroke rehabilitation: A meta-analysis and implications for clinicians. Stroke 2011, 42, 1380–1386. [Google Scholar] [CrossRef] [PubMed]
- Cheok, G.; Tan, D.; Low, A.; Hewitt, J. Is Nintendo Wii an effective intervention for individuals with stroke? A systematic review and meta-analysis. J. Am. Med. Dir. Assoc. 2015, 16, 923–932. [Google Scholar] [CrossRef] [PubMed]
- Laver, K.; George, S.; Thomas, S.; Deutsch, J.; Crotty, M. Virtual reality for stroke rehabilitation. Cochrane Database Syst Rev. 2015, 2, CD008349. [Google Scholar] [CrossRef] [PubMed]
- Wall, T.; Feinn, R.; Chui, K.; Cheng, M.S. The effects of the Nintendo™ Wii Fit on gait, balance, and quality of life in individuals with incomplete. spinal cord injury. J. Spinal Cord Med. 2015, 38, 777–789. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lopes, S.; Magalhães, P.; Pereira, A.; Martins, J.; Magalhães, C.; Chaleta, E.; Rosário, P. Games Used With Serious Purposes: A Systematic Review of Interventions in Patients With Cerebral Palsy. Front. Psychol. 2018, 9, 1712. [Google Scholar] [CrossRef]
- Valdés, B.A.; Glegg, S.M.; Lambert-Shirzad, N.; Schneider, A.N.; Marr, J.; Bernard, R.; Van der Loos, H.M. Application of commercial games for home-based rehabilitation for people with hemiparesis: Challenges and lessons learned. Games Health J. 2018, 7, 197–207. [Google Scholar] [CrossRef]
- Pereira, M.F.; Prahm, C.; Kolbenschlag, J.; Oliveira, E.; Rodrigues, N.F. Application of AR and VR in hand rehabilitation: A systematic review. J. Biomed. Inform. 2020, 111, 103584. [Google Scholar] [CrossRef]
- Gorsic, M.; Cikajlo, I.; Goljar, N.; Novak, D. A multisession evaluation of an adaptive competitive arm rehabilitation game. J. Neuroeng. Rehabil. 2017, 14, 1–15. [Google Scholar] [CrossRef]
- Wu, Y.-T.; Chen, K.-H.; Ban, S.-L.; Tung, K.-Y.; Chen, L.-R. Evaluation of leap motion control for hand rehabilitation in burn patients: An experience in the dust explosion disaster in Formosa Fun Coast. Burns 2019, 45, 157–164. [Google Scholar] [CrossRef]
- Tarakci, E.; Arman, N.; Tarakci, D.; Kasapcopur, O. Leap Motion Controller–based training for upper extremity rehabilitation in children and adolescents with physical disabilities: A randomized controlled trial. J. Hand Ther. 2020, 33, 220–228. [Google Scholar] [CrossRef]
- Dimbwadyo-Terrer, I.; Trincado-Alonso, F.; de los Reyes-Guzmán, A.; Aznar, M.A.; Alcubilla, C.; Pérez-Nombela, S.; Gil-Agudo, A. Upper limb rehabilitation after spinal cord injury: A treatment based on a data glove and an immersive virtual reality environment. Disabil. Rehabil. Assist. Technol. 2016, 11, 462–467. [Google Scholar] [CrossRef] [PubMed]
- Bayón, M.; Martínez, J. Rehabilitación del ictus mediante realidad virtual. Rehabilitación 2010, 44, 256–260. [Google Scholar] [CrossRef]
- Lee, K. Virtual Reality Gait Training to Promote Balance and Gait Among Older People: A Randomized Clinical Trial. Geriatrics 2021, 6, 1. [Google Scholar] [CrossRef] [PubMed]
- Viñas-Diaz, S.; Sobrido-Prieto, M. Realidad virtual con fines terapéuticos en pacientes con ictus: Revisión sistemática. Neurología 2016, 34, 255–277. [Google Scholar] [CrossRef] [PubMed]
- Maillot, P.; Perrot, A.; Hartley, A. Effects of Interactive Physical-Activity Video-Game Training on Physical and cognitive Function in Older Adults. Psychol. Aging 2012, 27, 589. [Google Scholar] [CrossRef]
- Beckers, L.W.M.E.; Geijen, M.M.E.; Kleijnen, J.; Rameckers, E.A.; Schnackers, M.L.; Smeets, R.J.; Janssen-Potten, Y.J. Feasibility and effectiveness of home-based therapy programmes for children with cerebral palsy: A systematic review. BMJ Open 2020, 10, e035454. [Google Scholar] [CrossRef]
- Sakzewski, L.; Ziviani, J.; Boyd, R.N. Efficacy of upper limb therapies for unilateral cerebral palsy: A meta-analysis. Pediatrics 2014, 133, e175–e204. [Google Scholar] [CrossRef]
- Keetch, K.M.; Lee, T.D. The effect of self-regulated and experimenter-imposed practice schedules on motor learning for tasks of varying difficulty. Res. Q. Exerc. Sport 2007, 78, 476–486. [Google Scholar] [CrossRef]
- Leike, A.M.; Bruzi, A.T.; Miller, M.W.; Nelson, M.; Wegman, R.; Lohse, K.R. The effects of autonomous difficulty selection on engagement, motivation, and learning in a motion-controlled video game task. Hum. Mov. Sci. 2016, 49, 326–335. [Google Scholar] [CrossRef]
- Lee, L.N.; Kim, M.J.; Hwang, W.J. Potential of Augmented Reality and Virtual Reality Technologies to Promote Wellbeing in Older Adults. Appl. Sci. 2019, 9, 3556. [Google Scholar] [CrossRef]
- Sveistrup, H.; McComas, J.; Thornton, M.; Marshall, S.; Finestone, H.; McCormick, A.; Babulic, K.; Mayhew, A. Experimental studies of virtual reality-delivered compared to conventional exercise programs for rehabilitation. CyberPsychol. Behav. 2003, 6, 245–249. [Google Scholar] [CrossRef]
- Gutiérrez, Á.; Sepúlveda-Muñoz, D.; Gil-Agudo, Á.; de los Reyes Guzmán, A. Serious Game Platform with Haptic Feedback and EMG Monitoring for Upper Limb Rehabilitation and Smoothness Quantification on Spinal Cord Injury Patients. Appl. Sci. 2020, 10, 963. [Google Scholar] [CrossRef]
- O’Neil, O.; Fernandez, M.M.; Herzog, J.; Beorchia, M.; Gower, V.; Gramatica, F.; Starrost, K.; Kiwull, L. Virtual reality for neurorehabilitation: Insights from 3 European Clinics. PM & R 2018, 10, 198–206. [Google Scholar]
- Charles, J.; Gordon, A.M. Development of hand–arm bimanual intensive training (HABIT) for improving bimanual coordination in children with hemiplegic cerebral palsy. Dev. Med. Child Neurol. 2006, 48, 931–936. [Google Scholar] [CrossRef] [PubMed]
- Burdea, G.C.; Grampurohit, N.; Kim, N.; Polistico, K.; Kadaru, A.; Pollack, S.; Oh-Park, M.; Barrett, A.M.; Kaplan, E.; Masmela, J.; et al. Feasibility of integrative games and novel therapeutic game controller for telerehabilitation of individuals chronic post-stroke living in the community. Top. Stroke Rehabil. 2020, 27, 321–336. [Google Scholar] [CrossRef] [PubMed]
- Garcia Garcia, E.; Sánchez-Herrera Baeza, P.; Cuesta Gómez, A. Efectividad de la realidad virtual en la rehabilitación del miembro superior en la lesión de la médula espinal. Revisión sistemática. Revista de Neurología 2019, 69, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Albiol Pérez, S. Rehabilitación Virtual Motora: Una Evaluación al tratamiento de pacientes con Daño Cerebral Adquirido. Ph.D. Thesis, Universitat Politècnica de València, Valencia, Spain, 2014. [Google Scholar]
- Sveistrup, H. Motor rehabilitation using virtual reality. J. Neuroeng. Rehabil. 2004, 1, 1–8. [Google Scholar] [CrossRef]
- García Aranda, J.J.; Alarcón Granero, M.; Juan Quintanilla, F.J.; Caffarena, G.; García-Carmona, R. Elastic Downsampling: An Adaptive Downsampling Technique to Preserve Image Quality. Electronics 2021, 10, 400. [Google Scholar] [CrossRef]
- Bos, R.A.; Haarman, C.J.; Stortelder, T.; Nizamis, K.; Herder, J.L.; Stienen, A.H.; Plettenburg, D.H. A structured overview of trends and technologies used in dynamic hand orthoses. J. Neuroeng. Rehabil. 2016, 13, 62. [Google Scholar] [CrossRef]
- Ozok, A.A. Survey design and implementation in HCI. In The Human–Computer Interaction Handbook; CRC Press: Boca Raton, FL, USA, 2012; pp. 1259–1277. [Google Scholar]
- Brooke, J. SUS: A Quick and Dirty Usability Scale. Usability Evaluation in Industry; Taylor & Francis: London, UK, 1996; pp. 189–194. [Google Scholar]
- Sauro, J. 5 Ways to Interpret SUS Score. MeasuringU. 19 September 2018. Available online: https://measuringu.com/interpret-sus-score/ (accessed on 30 May 2022).
- Rizzo, A.; Strickl, D.; Bouchard, S. The challenge of using virtual reality in telerehabilitation. Telemed J. e-Health 2004, 10, 184–195. [Google Scholar] [CrossRef]
- August, K.; Bleichenbacher, D.; Adamovich, S. Virtual reality physical therapy: A telerehabilitation tool for hand and finger movement exercise monitoring and motor skills analysis. In Proceedings of the IEEE 31st Annual Northeast Bioengineering Conference, Hoboken, NJ, USA, 2–3 April 2005; Volume 2. [Google Scholar]
- Lewis, G.N.; Rosie, J.A. Virtual reality games for movement rehabilitation in neurological conditions: How do we meet the needs and expectations of the users? Disabil. Rehabil. 2012, 34, 1880–1886. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).