
The Application of a 3-Dimensional Printing Technique in Refining the Orthodontic Trans-Palatal Arch


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Acquisition of Digitized Dental Models
- (1)
- Impressions of the patient’s dentition are taken using routine impression materials; plaster casts are made and scanned with a SHINING 3D scanner (SHINING 3D, Hangzhou, China).
- (2)
- Impressions of the patient’s dentition are taken with polyvinyl siloxane (PVS) materials; the PVS impressions are scanned with a SHINING 3D scanner (SHINING 3D, China).
- (3)
- The dentitions are scanned directly using oral scanners.
2.2. Computer-Aided Design and 3D Printing
- (1)
- The undercut areas are analyzed to determine the appropriate path of insertion of the 3D TPAs.
- (2)
- To the greatest extent possible, the metal plate should be designed over the undercut line.
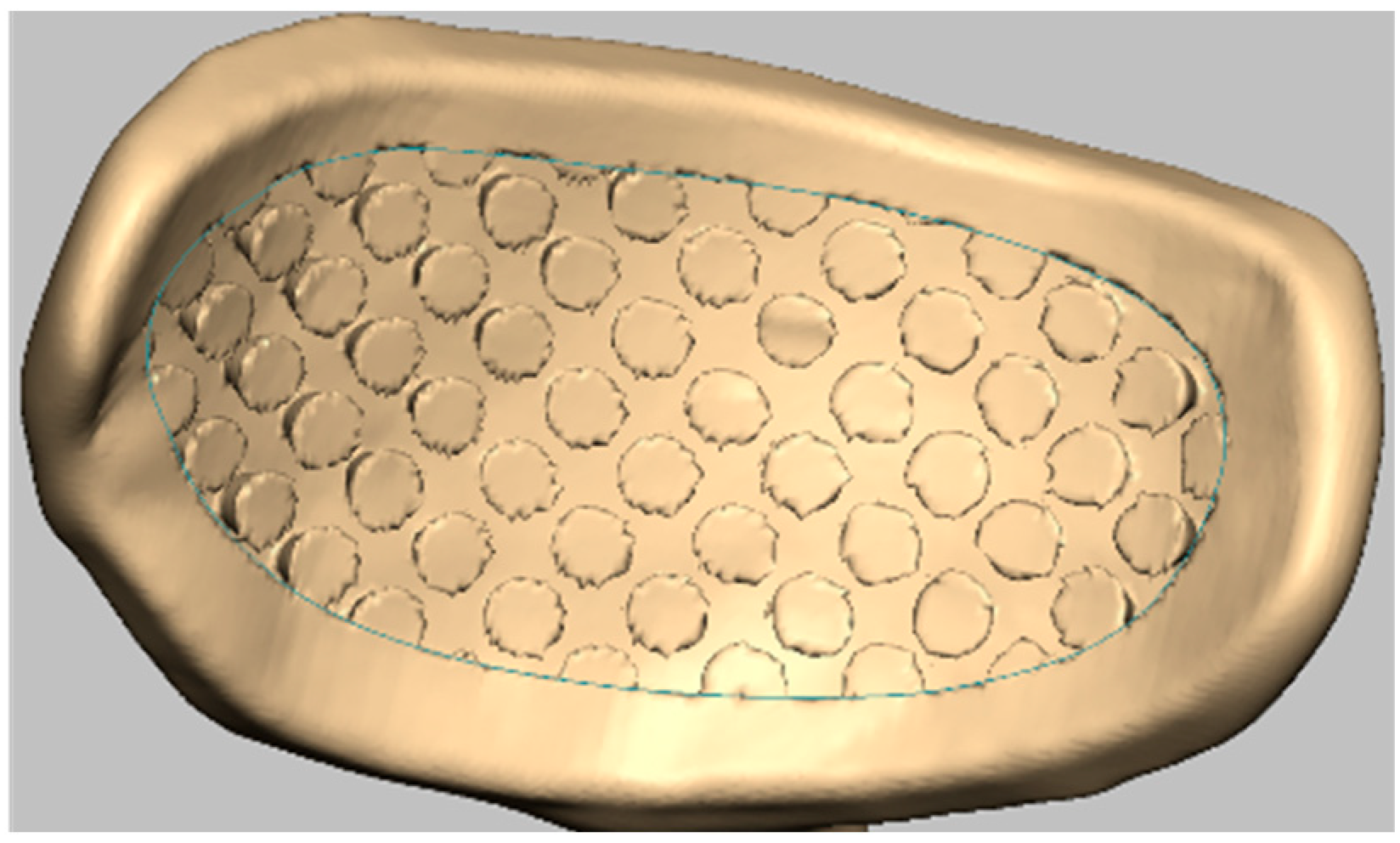
- (3)
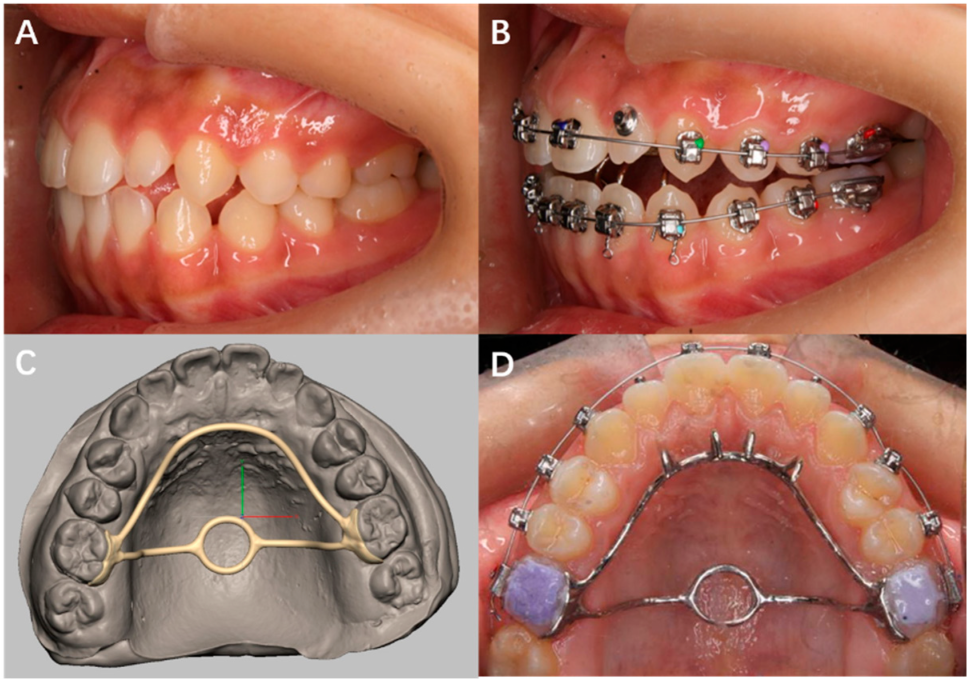
- The adhesive surface was modified with the undercut (Figure 1). The adhesive surface was an orthodontic bracket data provided by Jing Mei dental center (Chongqing, China).
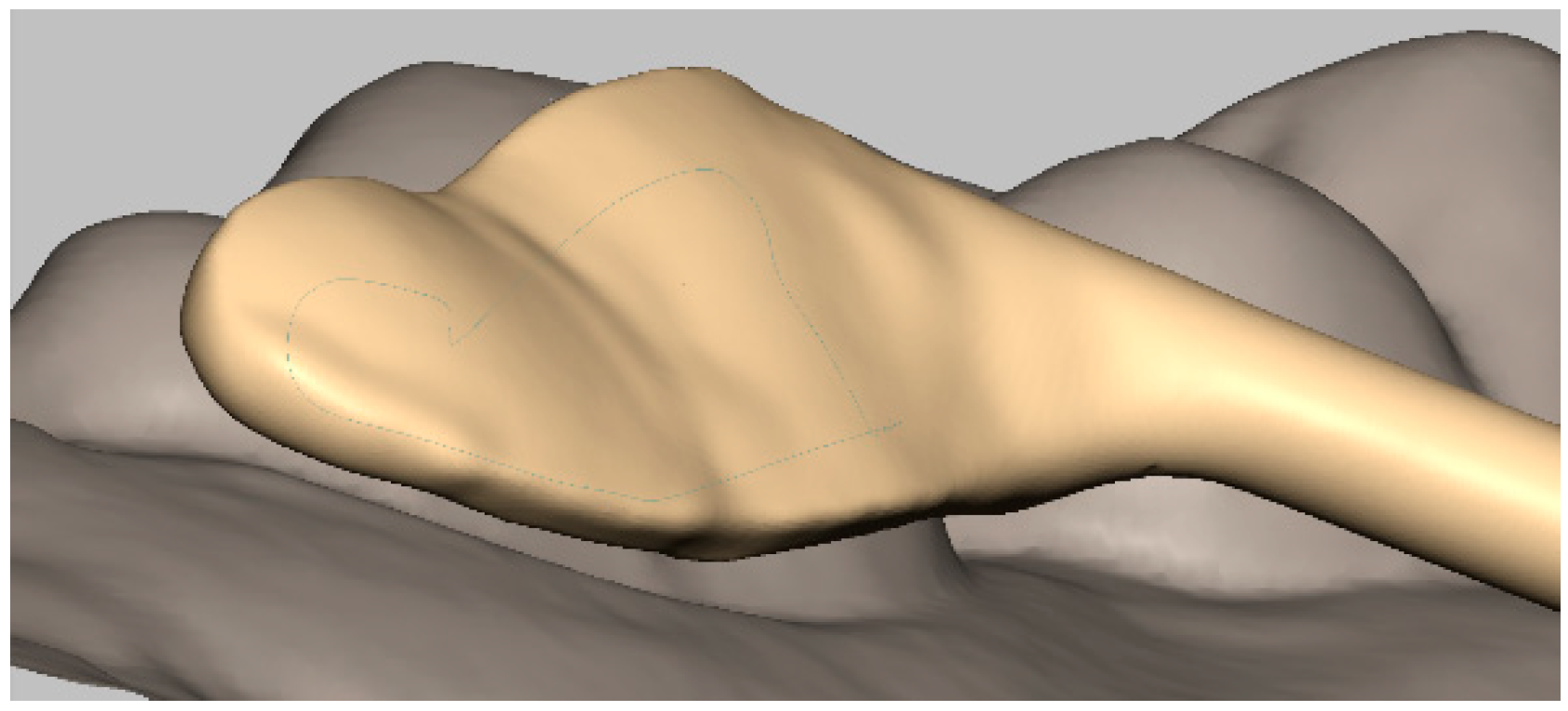
- (4)
- The distance from the gingival margin to the plate margin should measure more than 1.5 mm to maintain a suitable and healthy gingival condition (Figure 2).
- (5)
- Care should be taken to avoid occlusal interferences.
- (6)
- The shape of the metal bar, the distance from the bar to the palatal mucosa and the affiliated apparatus are designed according to both the clinician’s preference and the nature of the malocclusion.
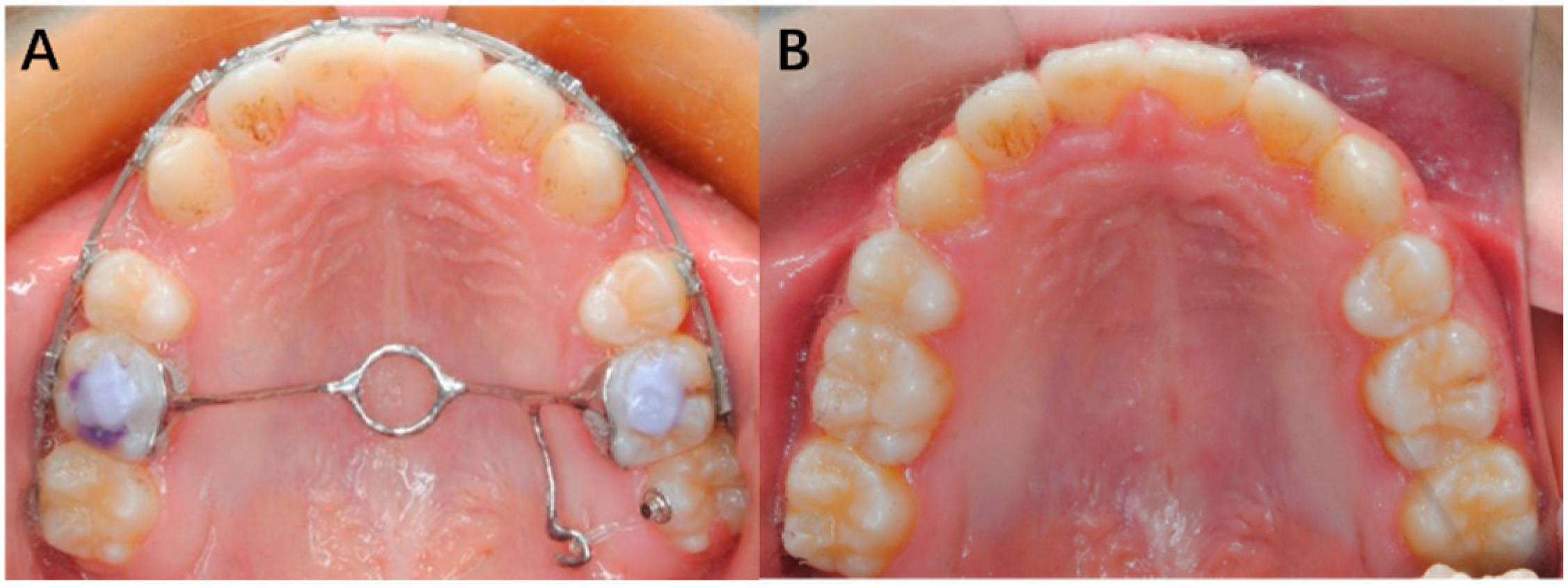
2.3. Bonding of 3D TPAs
3. Clinical Application
3.1. Case 1
3.2. Case 2
3.3. Case 3
3.4. Case 4
3.5. Case 5
3.6. Case 6
3.7. Case 7
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Miyazaki, T.; Hotta, Y.; Kunii, J.; Kuriyama, S.; Tamaki, Y. A review of dental CAD/CAM: Current status and future perspectives from 20 years of experience. Dent. Mater. J. 2009, 28, 44–56. [Google Scholar] [CrossRef] [Green Version]
- Feuerstein, P. CAD/CAM: Enhancing productivity through automation. Compend. Contin. Educ. Dent. 2011, 32, 42–43. [Google Scholar]
- Peltola, S.M.; Melchels, F.P.W.; Grijpma, D.W.; Kellomäki, M. A review of rapid prototyping techniques for tissue engineering purposes. Ann. Med. 2008, 40, 268–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mankovich, N.J.; Cheeseman, A.M.; Stoker, N.G. The display of three-dimensional anatomy with stereolithographic models. J. Digit. Imaging 1990, 3, 200–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hems, E.; Knott, N.J. 3D printing in prosthodontics. Fac. Dent. J. 2014, 5, 152–157. [Google Scholar] [CrossRef]
- Seres, L.; Varga, J.E.; Kocsis, A.; Rasko, Z.; Bago, B.; Piffko, J. Correction of a severe facial asymmetry with computerized planning and with the use of a rapid prototyped surgical template: A case report/technique article. Head Face Med. 2014, 10, 27. [Google Scholar] [CrossRef] [Green Version]
- Tunchel, S.; Blay, A.; Kolerman, R.; Mijiritsky, E.; Shibli, J.A. 3D Printing/Additive Manufacturing Single Titanium Dental Implants: A Prospective Multicenter Study with 3 Years of Follow-Up. Int. J. Dent. 2016, 2016, 859097. [Google Scholar] [CrossRef] [Green Version]
- Wiechmann, D.; Rummel, V.; Thalheim, A.; Simon, J.S.; Wiechmann, L. Customized brackets and archwires for lingual orthodontic treatment. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 593. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Sheng, Y.; Zhang, G. Design and Finite Element Analysis of the Personalized Labial Self-Ligating Bracket. Mach. Des. Manuf. 2018, 3, 71–74. [Google Scholar] [CrossRef]
- Retrouvey, J.M.; Kader, E.; Caron, E.; Tamimi, F.; Light, N. Printing Orthodontic Retainers Using CAD/CAM Technology. 2013. Available online: https://www.researchgate.net/profile/Jean-Marc-Retrouvey/publication/258699129_Printing_Orthodontic_Retainers_Using_CADCAM_Technology/links/0c960528d6a0be23fb000000/Printing-Orthodontic-Retainers-Using-CAD-CAM-Technology.pdf (accessed on 2 March 2022).
- Nasef, A.A.; El-Beialy, A.R.; Mostafa, Y.A. Virtual techniques for designing and fabricating a retainer. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 394–398. [Google Scholar] [CrossRef] [PubMed]
- Hong, K.J. Transparent Aligner and Method for Manufacturing Same. U.S. Patent 10,258,431, 16 April 2019. [Google Scholar]
- Farronato, G.; Santamaria, G.; Cressoni, P.; Falzone, D.; Colombo, M. The digital-titanium Herbst. J. Clin. Orthod. 2011, 45, 263. [Google Scholar]
- Graf, S.; Cornelis, M.A.; Hauber, G.G.; Cattaneo, P.M. Computer-aided design and manufacture of hyrax devices: Can we really go digital? Am. J. Orthod. Dentofac. Orthop. 2017, 152, 870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yañez-Vico, R.M.; Perula, M.; Solano-Reina, E. Vertical and Transverse Management with Transpalatal Arches in an Adult with Class III Malocclusion. Case Rep. Dent. 2017, 2017, 4062105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wise, J.B.; Magness, W.B.; Powers, J.M. Maxillary molar vertical control with the use of transpalatal arches. Am. J. Orthod. Dentofac. Orthop. 1994, 106, 403. [Google Scholar] [CrossRef]
- Raucci, G.; Elyasi, M.; Pachêcopereira, C.; Grassia, V.; d’Apuzzo, F.; Flores-Mir, C.; Perillo, L. Predictors of long-term stability of maxillary dental arch dimensions in patients treated with a transpalatal arch followed by fixed appliances. Prog. Orthod. 2015, 16, 24. [Google Scholar] [CrossRef] [Green Version]
- Patel, D.R.; Mehta, D.F.; Mehta, D.S.; Khonde, D.S. Case report: Intra-arch non-compliant mechanics for maxillary 2nd molar buccal crossbite: A transpalatal arch with L-Loop. India J. Basic Appl. Med. Res. 2015, 4, 497–501. [Google Scholar]
- Ingervall, B.; Göllner, P.; Gebauer, U.; Fröhlich, K. A clinical investigation of the correction of unilateral first molar crossbite with a transpalatal arch. Am. J. Orthod. Dentofac. Orthop. 1995, 107, 418–425. [Google Scholar] [CrossRef]
- Sonawane, M.S.; Karandikar, G.R.; Pawar, P.A.; Shah, S.S. Reinstating Buccally Flared Molars using a Modified Transpalatal Arch. J. Contemp. Dent. 2013, 3, 98–101. [Google Scholar] [CrossRef]
- Mehta, D.F.; Patel, D.R.; Kharadi, D.L.; Mehta, S. A Modified Transpalatal Arch for Correction of Bucally Placed Maxillary 2nd Molars: Non-Compliant Mechanics. Iosr J. Dent. Med. Sci. 2014, 13, 24–26. [Google Scholar] [CrossRef]
- Durgekar, S.; Nagaraj, K. Modified transpalatal arch for molar intrusion. Int. J. Orthod. 2012, 23, 59. [Google Scholar]
- Gupta, G.; Rozario, J.E.; Patil, A.K.; Singh, R.K. Maxillary Molar Intrusion Evaluation using Mini-implants along with Transpalatal Arch Bar. J. Contemp. Dent. 2015, 5, 158–164. [Google Scholar] [CrossRef]
- Eyüboǧlu, S.; Bengi, A.O.; Gürton, A.U.; Akin, E. Asymmetric Maxillary First Molar Distalization with the Transpalatal Arch. Turk. J. Med. Sci. 2004, 34, 59–66. [Google Scholar]
- Miresmaeili, A.; Sajedi, A.; Moghimbeigi, A.; Farhadian, N. Three-dimensional analysis of the distal movement of maxillary 1st molars in patients fitted with mini-implant-aided trans-palatal arches. Korean J. Orthod. 2015, 45, 236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raucci, G.; Pachêcopereira, C.; Grassia, V.; d’Apuzzo, F.; Flores-Mir, C.; Perillo, L. Maxillary arch changes with transpalatal arch treatment followed by full fixed appliances. Angle Orthod. 2015, 85, 683–689. [Google Scholar] [CrossRef] [Green Version]
- Tsetsilas, M.; Konermann, A.C.; Keilig, L.; Reimann, S.; Jäger, A.; Bourauel, C. Symmetric and asymmetric expansion of molars using a Burstone-type transpalatal arch: Biomechanical and clinical analysis. J. Orofac. Orthop. 2015, 76, 377–390. [Google Scholar] [CrossRef]
- Kuang, Y.; Wang, C.; Hu, B.; Feng, G.; Wang, C.; Song, J. Biomechanical analysis of reinstating buccally flared maxillary 2nd molars using 3D printing anchorage supports: A 3D finite element study. Comput. Methods Biomech. Biomed. Eng. 2021, 24, 1085–1096. [Google Scholar] [CrossRef]









Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuang, Y.; Hu, B.; Feng, G.; Huang, L.; Song, J. The Application of a 3-Dimensional Printing Technique in Refining the Orthodontic Trans-Palatal Arch. Appl. Sci. 2022, 12, 7497. https://doi.org/10.3390/app12157497
Kuang Y, Hu B, Feng G, Huang L, Song J. The Application of a 3-Dimensional Printing Technique in Refining the Orthodontic Trans-Palatal Arch. Applied Sciences. 2022; 12(15):7497. https://doi.org/10.3390/app12157497
Chicago/Turabian StyleKuang, Yunchun, Bo Hu, Ge Feng, Lan Huang, and Jinlin Song. 2022. "The Application of a 3-Dimensional Printing Technique in Refining the Orthodontic Trans-Palatal Arch" Applied Sciences 12, no. 15: 7497. https://doi.org/10.3390/app12157497
APA StyleKuang, Y., Hu, B., Feng, G., Huang, L., & Song, J. (2022). The Application of a 3-Dimensional Printing Technique in Refining the Orthodontic Trans-Palatal Arch. Applied Sciences, 12(15), 7497. https://doi.org/10.3390/app12157497