Abstract
The present research aimed to reveal the in vitro effects of different endodontic file systems utilizing different endodontic access cavity designs on the elimination of Enterococcus faecalis from root canal systems. One hundred and fifty mandibular molar teeth were separated into three groups with respect to the access cavity design: traditional endodontic cavity (TEC), conservative endodontic cavity (CEC), and truss access cavity (TAC) (n = 50). After access cavity preparation, inolulation of teeth with E. faecalis was undertaken for 21 days. Following the first sampling (S1), further division of the groups into five subgroups (n = 10) was performed: ProTaper Gold, 2Shape, TruNatomy, Reciproc Blue, and WaveOne Gold. After instrumentation, bacterial sampling (S2) was performed. Bacterial reduction was evaluated in colony-forming units/mL, and statistical analysis was carried out. The E. faecalis count decreased significantly in all groups (p < 0.05). The range of mean values for a decrease in E. faecalis in log numbers was lowest in the TAC and Reciproc Blue groups, while the highest values of bacterial reduction were detected in the TEC and ProTaper Gold groups. The highest level of antibacterial action was obtained with the use of ProTaper Gold compared to the other file systems tested.
1. Introduction
The elimination of the bacterial population from the root canal system represents the most essential phase of endodontic treatment [1,2]. The presence of persistent bacteria within the root canals after chemomechanical procedures is a key reason for endodontic failure [3,4]. Enterococcus faecalis is a Gram-positive, facultative anaerobic bacterium, commonly isolated from persistent root canal infections [5,6]. The prevalence of E. faecalis is usually high in cases of unsuccessful root canal treatment owing to the different virulence factors expressed by the bacterium. E. faecalis can penetrate into dentinal tubules at different levels using these virulence factors and resist removal even after preparation [7]. Due to its highly virulent nature, the elimination of the bacterial population during root canal treatment is accomplished mostly via a combination of mechanical instrumentation, irrigation procedures, and intracanal medicaments [8].
Various improved nickel–titanium instrumentation systems with different characteristics have been developed to improve the procedure of intracanal bacterial reduction [9,10]. The ProTaper Gold (Dentsply Maillefer, Ballaigues, Switzerland) file system is produced using M-Wire technology and employs a continuous rotational movement. Each file has a progressive taper shape and a convex triangular cross-sectional design that has been claimed to enhance its cutting efficiency [11].
Following this evolution, the TruNatomy (TRN; Dentsply Maillefer, Ballaigues, Switzerland) multi-file system was designed, featuring a small taper size for conservative preparations. This system has different taper sizes to protect the structural dentin in narrow endodontic access cavities. The manufacturer has suggested that TruNatomy files are more flexible and fatigue-resistant due to their unique design, which is provided by a special heat treatment [12,13].
In 2017, the new 2Shape file system was introduced by Micro-Mega using a Ni–Ti alloy named T-wire. The manufacturers produced this system with a unique cross-sectional design comprising a modified triple helix equipped with two main cutting edges for cutting efficiency, and an offset blade to enhance debris removal and increase the effectiveness of efficient selective cleaning [13].
In recent years, single file systems have also been developed. In these systems, the files perform a reciprocation motion, which requires special motors. Such systems include WaveOne Gold (Dentsply Maillefer, Ballagigues, Switzerland) and Reciproc Blue (RCP; VDW GmbH, Munich, Germany). The WaveOne Gold has been produced using a heat-treated gold metal alloy. It has a unique off-centered parallelogram cross-sectional shape with two cutting edges [9,14], whilst the Reciproc Blue system has an S-shaped horizontal cross-sectional design, also with two cutting edges [15].
Selection of the appropriate access cavity preparation is important for efficient instrumentation and irrigation, and has an impact on the success of endodontic treatment [1]. The aim of the traditional endodontic access cavity (TEC) preparation is to achieve complete unroofing of the pulp chamber, to ensure that all the pulp horns are exposed, and to provide straight-line access to the root canals without undercuts. This cavity design can enable visualization of the pulp chamber and all of the root canal orifices, prevent errors during preparation, and increase the efficiency of irrigation. However, it also decreases the fracture resistance of the tooth due to the removal of a large amount of dentin tissue [16].
A minimally invasive endodontic access concept has been presented to preserve the roof of the pulp chamber and pericervical dentin as much as possible, and to decrease the fracture risk of teeth that have undergone endodontic treatment (1, 17). The mentioned concept has two types of access cavity design. The aim of the conservative endodontic access cavity (CEC) is to partially deroof the pulp chamber and preserve the pulp horns. On the other hand, the truss access cavity (TAC) comprises two separated individual cavities in molar teeth. In mandibular molar teeth, one cavity is usually opened above the mesial cavity, and the other one above the distal cavity to increase dentin preservation between the cavities [1,17,18]. Despite mechanical advantages, minimally invasive endodontic access cavities have some risks related to irrigation, preparation, and obturation of the root canal system [19].
The current research aimed to examine different endodontic file systems in mandibular molar teeth utilizing different endodontic access cavity concepts and to assess the impact of these different file systems and cavity concepts in reducing E. faecalis levels in root canal systems. According to the null hypothesis, various access cavity designs and instrument systems will provide similar reductions in E. faecalis.
2. Materials and Methods
2.1. Selection of Specimens
G*Power 3.1 software (Heinrich Heine University, Dusseldorf, Germany) was used to estimate the sample size. Accordingly, to ensure an alpha-type error of 0.05 and 80% power, a sample size of 10 teeth was determined for each group in the analysis.
Approval for this research was obtained from the Institutional Review Board at Near East University (YDU/2020/85-1207). A total of 183 mature mandibular molar teeth extracted for orthodontic or periodontal reasons were selected. All teeth were examined under an operating microscope at x16 magnification to eliminate any teeth with fractures, cracks, or fusion. Preoperative radiographs in the buccolingual and mesiodistal directions were taken, and 28 teeth which had undergone previous root canal treatment, restoration, or resorption were excluded. The remaining 155 teeth were selected to be examined in this study. These study teeth each had 3 separate root canals and a degree of root canal curvature ranging between 100 and 200 [20]. To ensure standardization, teeth lengths were measured from the crown to the apical region by means of a digital caliper (Digimess Instrumentos de Precisao Ltda., Sao Paulo, Brazil, SP, Brazil) and teeth with similar lengths (21 ± 1 mm) were selected. All remaining hard and soft tissues on the teeth surface were removed mechanically and kept in 0.1% thymol solution at a temperature of 4 °C until use.
2.2. Access Cavity Preparation
The teeth were separated into three different groups (n = 50) according to the access cavity design: TEC, CEC, and TAC. Access cavity preparation was performed by the same operator for all teeth. The preparation of access cavities was performed using an 856-diameter diamond bur (Komet Italia S.R.L, Milan, Italy) with a high-speed handpiece under water cooling. In the TEC group, the pulp chamber’s roof and all the pulp horns were completely removed, and a direct access to the root canals was created ensuring coronally divergent axial walls with no undercut. In the CEC group, teeth were prepared by undertaking partial unroofing of the pulp chamber and preserving the pulp horns. Access cavity walls were created with a slight convergence toward the occlusal surface until the canal orifices could be detected. In the TAC group, a single access to the mesial canals was formed in the buccal–lingual direction, and another access was created in order to reach the distal canal orifice. The roof of the pulp chamber between the mesial and distal cavities was preserved.
After access cavity preparation, apical patency was determined using #10 K-file (Dentsply Maillefer). The #10 K-file was inserted into the canal until it could be observed from the apical foramen. Root canals which were wider than a size #20 K-file at the apical foramen were excluded. The working length was calculated as 1 mm shorter in comparison to the length in question, and the canals were instrumented up to a #20 K-file. Between each file, 2 mL of 5.25% sodium hypochlorite (NaOCl) was used for the irrigation of the root canals. The root canals were then filled with 17% ethylenediaminetetraacetic acid (EDTA) for one minute and were rinsed with 5.25% NaOCl, followed by sterile distilled water to remove the smear layer.
The apical part of each root was sealed with composite resin, and the radicular surface was varnished with nail polish for the purpose of preventing bacterial leakage. Cotton pellets were placed into the canal orifice and subsequently sealed with a temporary filling. To facilitate both handling and identification, each tooth was placed vertically into an Eppendorf tube (Jencons Scientific Ltd., England) with acrylic resin. After the acrylic resin was set, the removal of the temporary filling and pellet was carried out. The tubes were placed in autoclave sachets, and their sterilization in an autoclave was conducted at a temperature of 121 °C for a period of 15 min. Sterilization was ensured using an indicator (4A Medical, Emulating Indicator, Class 6, Turkey) present in the sachets.
2.3. Root Canal Contamination with E. faecalis
The E. faecalis strain ATCC 29,212 (American Type Culture Collection, Manassas, VA) was used to inoculate the root canals. E. faecalis was grown on brain heart infusion agar (BHI; Difco Laboratories Inc., Detroit, MI, USA) mixed with 5% sheep blood at a temperature of 37 °C for a period of 48 h. Colonies were inoculated into sterile BHI broth to acquire a 1-McFarland bacterial suspension, which was diluted to obtain 1 × 108 colony-forming units (CFU) per milliliter. The Eppendorf tubes with the sterilized samples were opened under a laminar flow hood, and each root canal was inoculated with the bacterial suspension using a sterile pipette. A #15 K-file (Dentsply Maillefer) was inserted into the canal within 1 mm of the working length, and the canal was filed circumferentially for a period of 10 s. The incubation of the specimens was performed at 37 °C for 21 days. Fresh BHI was added to the root canals every other day. Five teeth were randomly selected as a control group and were submerged in BHI broth for 1 day to ensure the effectiveness of sterilization.
2.4. Instrumentation of Root Canals
The access cavity groups were separated into the subgroups described in Table 1 below (5 subgroups each) (n = 10):

Table 1.
Overview of sample size of each experimental group.
ProTaper Gold Sx (#19, 0.04v), S1 (#18, 0.02v), S2 (#20, 0.04v), F1 (#20, 0.07v), and F2 (#25, 0.08v) files were used one by one with an X-Smart Plus rotary endodontic motor (X-Smart; Dentsply Maillefer) operating with rotational motion. Files were utilized with in-and-out movements according to the instructions of the manufacturer.
The TruNatomy files orifice modifier (#20, 08v), glider (#17, 02v), small (#20, 0.04v), and prime (#26, 0.04v), were used sequentially. The files were utilized with 2–3 small amplitudes about 2–5 mm in and out of the root canal. When the working length was reached, file removal was performed with the aim of avoiding the over-enlargement of the apical foramen.
2Shape files were used in sequence as TS1 (25/04) and TS2 (25/06) with two or three steps until the working length had been reached, in line with the instructions of the manufacturer. A single downward motion in a free progression was performed until resistance was met, then two brushing strokes were performed to free the file before it proceeded in an apical direction.
A WaveOne Gold primary file (#25, 0.07) was used with a reciprocating motion in the WaveOne ALL program on an X-Smart Plus rotary endodontic motor (X-Smart; Dentsply Maillefer). The file was used with a slight apical pressure and brushing motion, following the instructions of the manufacturer.
A Reciproc Blue R25 file (VDW, Munich, Germany) was utilized in the Reciproc ALL program on an X-Smart Plus rotary endodontic motor (X-Smart; Dentsply Maillefer). The file was inserted with an up-and-down pecking motion with a slight apical pressure and an amplitude of 3 mm. This procedure was repeated three times.
Instrumentation was performed three times with in-and-out motions and gentle apical pressure. The same procedure was repeated for three cycles, and files were cleaned with sterile gauze between each cycle. The same operator performed all the instrumentation procedures for the elimination of any bias. In the course of preparation procedures, every sample was rinsed with 10 mL of distilled water between each file. Distilled water was delivered into the canals using a 30-gauge needle coupled to a 5 mL plastic syringe (NaviTip, Ultradent Products, Inc., South Jordan, UT, USA) up to 1 mm short of the working length. Each procedure was applied to the different access cavity groups.
2.5. Quantification of the Bacterial Load
Bacterial samples were taken prior to (S1) and following instrumentation (S2) from the root canals. Each root canal was initially rinsed using 1 mL of 0.85% sterile saline solution. Subsequently, a sterile #20 K-file was inserted into the canals and the canal walls were slightly touched with an in-and-out motion circumferentially to remove intact bacterial cells. Initial samples (S1) were obtained from the root canals by inserting three pieces of #15 sterile paper point for one minute. The paper points were transferred to an Eppendorf tube with 1 mL of 0.85% phosphate-buffered solution and were vortexed for one minute. For quantitative bacterial assessment, 10-fold serial dilutions were prepared, and every dilution was plated on a BHI agar medium and incubated at 37 °C for 24 h. CFU counting was performed, and counts were converted into CFU/mL based on the dilution factor.
Second samples (S2) were obtained from the root canals using three pieces of #25 sterile paper points. The same culturing procedures were applied as for S1 (Figure 1).
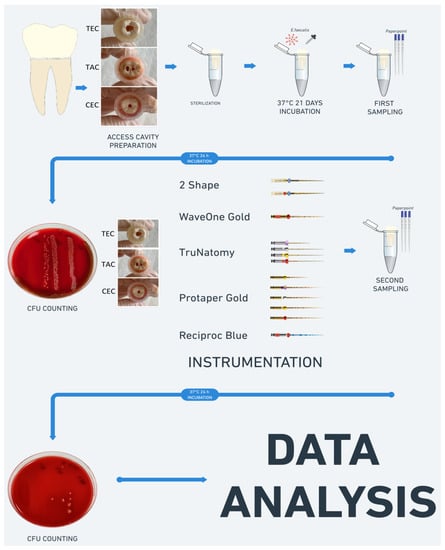
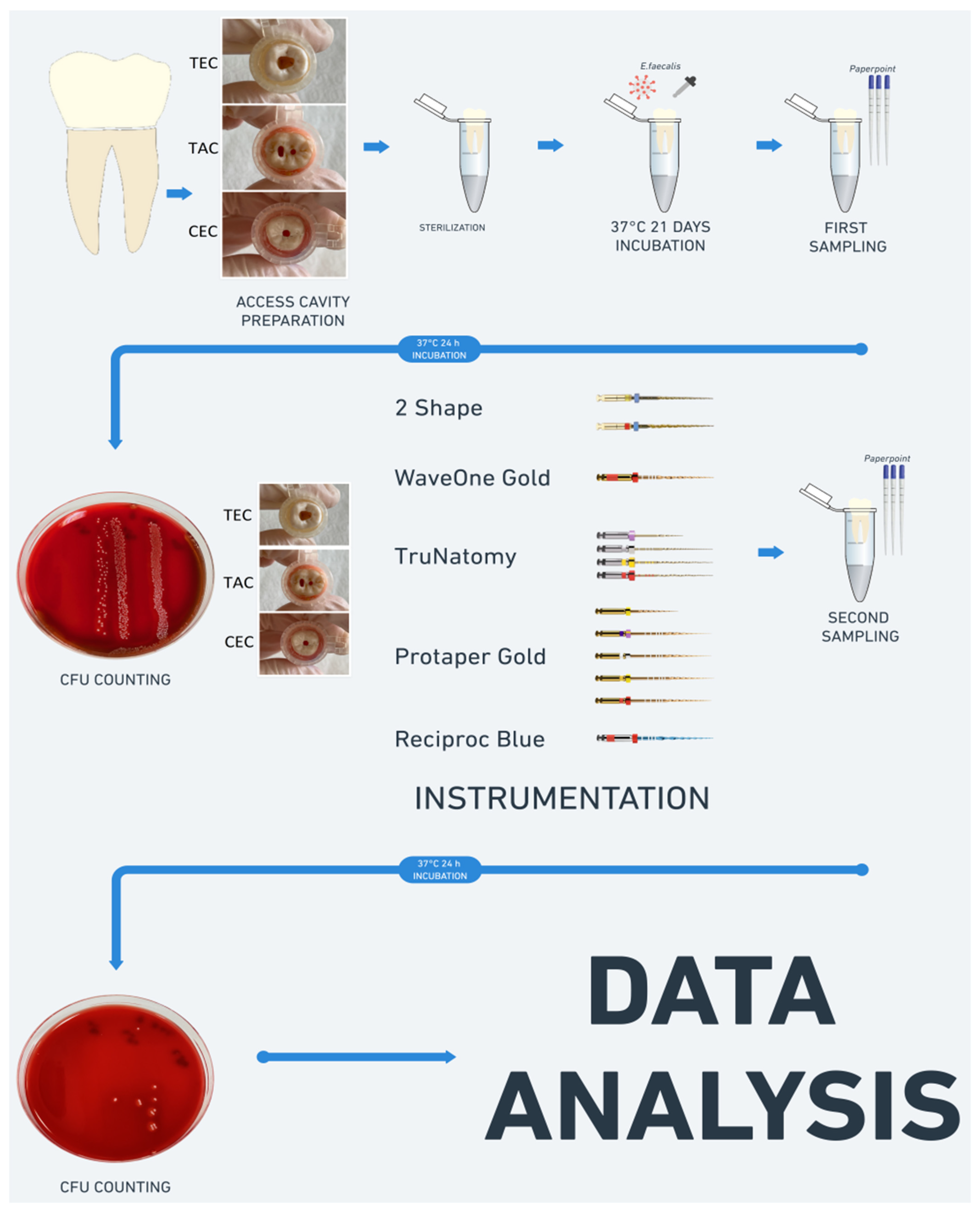
Figure 1.
The schematic diagram of the methods used in this study.
2.6. Statistical Analysis
A Kolmogorov–Smirnov test was conducted to analyze the normality of the log-transformed variables. Statistical analysis of the data acquired from samples prior to and following instrumentation was performed to determine any differences among the groups in terms of microbial reduction using two-way ANOVA, while Tukey’s test was carried out for multiple comparisons. A paired sample t-test was conducted to evaluate differences within every group between bacterial counts prior to and following instrumentation. A p-value < 0.05 was accepted as statistically significant.
3. Results
The initial bacterial counts taken before chemomechanical preparation produced similar values for all groups. This result indicates the homogeneity of the initial bacterial count in the experimental groups. The multiple variance analysis of the data revealed a statistically significant decrease in E. faecalis in all groups after instrumentation utilizing various cavity designs (p < 0.05) (Table 2).
Table 2.
Mean values of bacterial counts (in log colony-forming units/mL) in the root canals before and after mechanical instrumentation using different endodontic cavities.
When the effectiveness of the mechanical preparations in reducing bacterial load in the TEC groups was evaluated, a significantly greater bacterial reduction was observed in the TEC-ProTaper Gold group than in the TEC-Reciproc Blue, TEC-WaveOne Gold, and TEC-TruNatomy groups. In addition, the TEC-2Shape group exhibited greater bacterial reduction compared to the TEC-Reciproc Blue (p ˂ 0.05) group. In the CEC groups, differences between the tested file systems were not significant (p > 0.05). In the TAC groups, bacterial reduction was significantly greater in the TAC-ProTaper Gold group in comparison to the TAC-WaveOne Gold and TAC-Reciproc Blue groups.
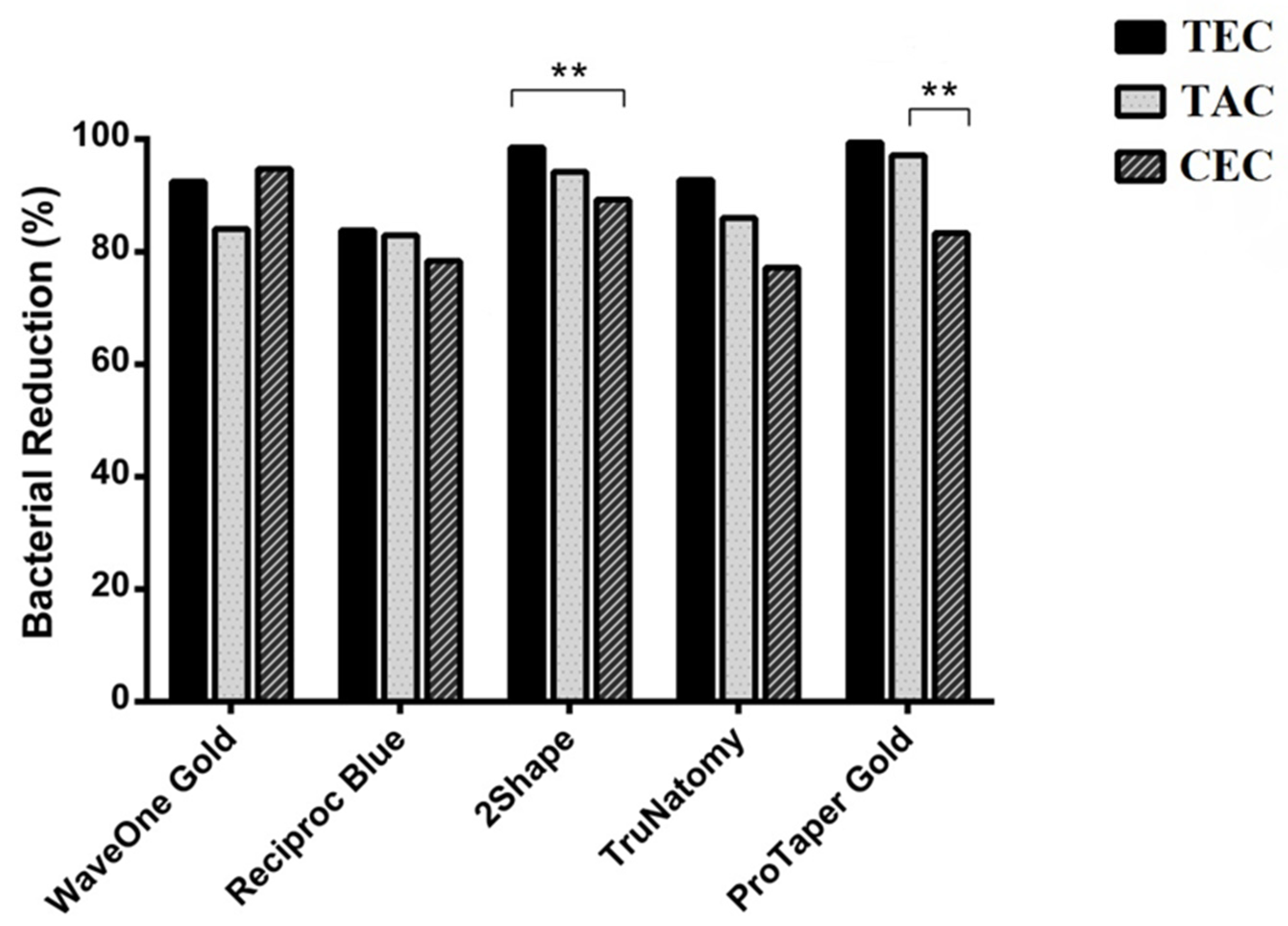
When the efficacy of the access cavity design in reducing the E. faecalis count was assessed, the CEC design was less effective in bacterial reduction than the TEC and TAC designs in the ProTaper Gold and 2Shape groups. No statistically significant differences were observed among other groups with respect to the access cavity design (p > 0.05) (Figure 2).
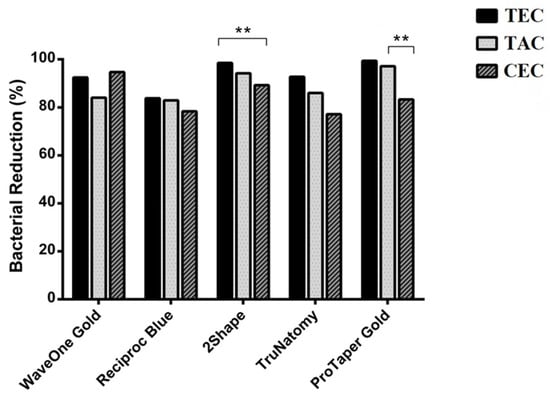
Figure 2.
Percentage differences in bacterial reduction in root canals utilizing WaveOne Gold, Reciproc Blue, 2Shape, TruNatomy, and ProTaper Gold between different access cavity designs, ** p < 0.05.
4. Discussion
E. faecalis is a Gram-positive, facultatively anaerobic bacterium with considerable clinical significance. It is commonly isolated in endodontic infections and can cause periradicular inflammation. The bacterium has the capacity to penetrate deep into dentinal tubules to establish communities that are organized in biofilms. It can survive as a monoinfection of the root canal under unusual environmental stress and is resistant to chemomechanical preparation [17,21]. Therefore, it serves as a model microorganism for studies utilizing a bacteriological assessment method and was selected as a bacteriological marker in this study.
In previous studies, E. faecalis has been incubated in root canals for variable time periods ranging from 24 h to 30 days [21,22,23]. The incubation period selected for in vitro research may have an effect on the elimination of microorganisms from root canals. A longer incubation period allows the bacteria to penetrate deeper into dentinal tubules. In light of the data available in the literature, in this study, specimens were infected for 21 days in order to ensure the effective penetration of E. faecalis into the dentinal tubules [5,6,24].
The most common technique for bacteriological assessment is CFU quantification employing culturing techniques, which is followed by molecular methods utilizing DNA detection. Molecular methods have higher sensitivity. However, they may also detect non-viable microorganisms in the root canal, which may be problematic when examining samples obtained right after treatment procedures. In this study, the CFU counting method was preferred due to its effectiveness and simplicity [1,25,26].
The primary cause of a failure of a root canal treatment is the presence of bacteria. Therefore, microbiological elimination is of utmost importance during treatment procedures. Several methods have been used to evaluate this concept. There are numerous studies in the literature evaluating the effectiveness of mechanical instrumentation with various types of file systems in microbial reduction [15,26]. However, only a few studies have compared both endodontic access cavities and file systems [1,2,18]. Our research aimed to assess the impact of different endodontic access cavities and file systems on bacterial reduction in infected root canals [1,2,27].
Bacteriological sampling was performed with a sterile paper point. Sampling using paper points has the advantage of being usable during both in vitro and in vivo experimentation. On the other hand, it has certain limitations, such as providing the opportunity for sampling microorganisms only within the root canal, not those inside dentin tubules [8]. In the current research, prior to sampling, the hand file was inserted into the root canals with an in-and-out motion to allow for enhanced collection of microorganisms from all regions of the possible sampling areas. It has previously been demonstrated that sterile distilled water used as a root canal irrigant during mechanical preparation does not eradicate microorganisms within infected root canals [8]. Since the present study focused on the comparison between the mechanical effects of different file systems on E. faecalis reduction, an antimicrobial irrigation solution was not used [14,24].
Bacterial counts indicated a significant reduction in microbial load following all instrumentation methods in each sample. The null hypothesis was rejected. The use of the WaveOne Gold and Reciproc Blue file systems resulted in a smaller percentage reduction in E. faecalis compared to the ProTaper Gold in the TEC and TAC design groups. In accordance with this study, the ProTaper file system has been previously demonstrated to be significantly more effective in bacterial reduction than other systems [8,28,29]. Otero et al. [30] also found that ProTaper Gold showed superior bacterial reduction compared to WaveOne Gold. Moreover, Nascimento et al. [10] reported that the Reciproc Blue file system exhibited lower antibacterial action when compared to the ProTaper Next file system. These results can be attributed to the fact that the ProTaper file system removes the dentin surface more aggressively therefore leading to lower bacterial counts in samples after instrumentation [8]. In contrast with these results, other previous studies have indicated no significant differences in the efficacy of bacterial removal between WaveOne and ProTaper Gold rotary files [6,24].
In the current study, 2Shape instrumentation led to significantly greater bacterial reduction within root canals compared with Reciproc Blue in the TEC design group. Moreover, significant differences were revealed in E. faecalis counts between TruNatomy and ProTaper Gold file systems in the TEC design group. There is no previous research in the literature on the levels of bacterial reduction in root canals after mechanical instrumentation applied to teeth using the 2Shape and TruNatomy file systems.
The results of this study highlighted significantly lower bacterial reductions in the CEC group than in the TAC and TEC groups following instrumentation with the ProTaper Gold and 2Shape file systems. In contrast with our results, Tüfenkçi and Yılmaz [1] determined the impact of root canal instrumentation on the amount of E. faecalis reduction within the root canal system by utilizing various file systems in teeth with the TEC and CEC access cavity designs, finding no significant differences between the cavities. Similarly, in their study, Barbosa et al. [17] examined the efficacy of canal instrumentation in microbial reduction in mandibular molar teeth, revealing no significant differences in microbial reduction. The authors also obtained similar results for unprepared areas between three access cavities. These results are in accordance with the findings obtained by Rover et al. [31], which indicated similar results for unprepared areas. According to the results of our study, mechanical instrumentation might be affected by the access cavity design. In particular, there may have been more unprepared areas in the root canals utilizing a CEC design due to the absence of straight-line access.
This study has specific limitations. One of the limitations was that only sterile saline was used as an irrigation solution. This allowed examination of the mechanical action of endodontic instruments; however, it did not reflect the real-world clinical conditions of endodontic treatment. In addition, this was an in vitro study that could not exactly mimic in vivo conditions. Further studies should be performed utilizing different irrigation solutions in vitro and in vivo to evaluate the effectiveness of the instrument systems used in this study.
5. Conclusions
In conclusion, bacterial reduction was lower in the CEC design compared to the TAC and TEC designs when the preparation was performed using the ProTaper Gold and 2Shape file systems. The use of the ProTaper Gold file system ensured a higher level of antibacterial action in comparison with the WaveOne Gold and Reciproc Blue in the TEC and TAC groups.
Author Contributions
Conceptualization, G.A., A.K. and F.B.; Methodology, G.A., F.B. and B.B.; Software, G.A. and B.B.; Validation. G.A., A.K. and F.B.; Formal Analysis, G.A. and B.B.; Investigation, G.A.; Resources, B.B.; Data Curation, G.A. and A.K.; Writing—Original Draft Preparation, G.A., F.B. and B.B.; Writing—Review & Editing, G.A., F.B. and A.K.; Visualization, G.A.; Supervision, G.A. and F.B.; Project Administration, G.A. and A.K.; Funding Acquisition, G.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of Near East University (YDU/2020/85-1207 and 26 November 2020).
Informed Consent Statement
Not applicable.
Data Availability Statement
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Acknowledgments
We thank Ozgur Irmak for his help with the statistical analysis.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Tüfenkçi, P.; Yılmaz, K. The effects of different endodontic access cavity design and using XP-endo finisher on the reduction of Enterococcus faecalis in the root canal system. J. Endod. 2020, 46, 419–424. [Google Scholar] [CrossRef]
- Vieira, G.C.; Pérez, A.R.; Alves, F.R.; Provenzano, J.C.; Mdala, I.; Siqueira, J.F.; Roças, I.N. Impact of contracted endodontic cavities on root canal disinfection and shaping. J. Endod. 2020, 46, 655–661. [Google Scholar] [CrossRef]
- Prada, I.; Micó-Muñoz, P.; Giner-Lluesma, T.; Mico-Martinez, P.; Colla-do-Castellano, N.; Manzano-Saiz, A. Influence of microbiology on endodontic failure. Literature review. Med. Oral Patol. Oral Cir. Bucal 2019, 24, e364. [Google Scholar] [CrossRef] [PubMed]
- Neelakantan, P.; Khan, K.; Ng, G.P.H.; Yip, C.Y.; Zhang, C.; Cheung, G.S.P. Does the orifice-directed dentin conservation access design debride pulp chamber and mesial root canal systems of mandibular molars similar to a traditional access design? J. Endod. 2018, 44, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, K.G.C.; da Silva, B.B.; Boer, N.C.; Mandarini, D.R.; Moreti, L.C.T.; Kato, A.S.; Bueno, C.E.S.; Limoeiro, A.G.S.; Pinheiro, S.L.; Martin, A.S.; et al. The effectiveness of three irrigation systems in the Enterococcus faecalis reduction after instrumentation with a reciprocating instrument. Eur. J. Dent. 2020, 14, 539. [Google Scholar] [CrossRef] [PubMed]
- Guillén, R.E.; Nabeshima, C.K.; Caballero-Flores, H.; Cayon, M.R.; Mercade, M.; Cai, S.; Machado, M.E.L. Evaluation of the WaveOne Gold and One Shape New Generation in reducing Enterococcus faecalis from root canal. Braz. Dent. J. 2018, 29, 249–253. [Google Scholar] [CrossRef]
- Francisco, P.A.; da Graça Fagundes, P.I.; Lemes-Junior, J.C.; Lima, A.R.; Passini, M.R.Z.; Gomes, B.P.F.A. Pathogenic potential of Enterococcus faecalis strains isolated from root canals after unsuccessful endodontic treatment. Clin. Oral Investig. 2021, 25, 1–9. [Google Scholar] [CrossRef]
- Gorduysus, M.; Nagas, E.; Torun, O.Y.; Gorduysus, O. A comparison of three rotary systems and hand instrumentation technique for the elimination of Enterococcus faecalis from the root canal. Aust. Endod. J. 2011, 37, 128–133. [Google Scholar] [CrossRef]
- Üreyen Kaya, B.; Erik, C.E.; Sesli Çetin, E.; Köle, M.; Maden, M. Mechanical reduction in intracanal Enterococcus faecalis when using three different single-file systems: An ex vivo comparative study. Int. Endod. J. 2019, 52, 77–85. [Google Scholar] [CrossRef] [Green Version]
- Nascimento, W.M.; da Silva Limoeiro, A.G.; Moraes, M.M.; Campos, D.D.L.; Drumond, J.P.; Maeda, W.; Soares, A.J.; Prado, M.C.; Frozoni, M. Reduction in Enteroccocus faecalis counts produced by three file systems in severely curved canals. Res. Soc. Dev. 2021, 10, 1–9. [Google Scholar]
- Singh, S. Shaping ability of two-shape and ProTaper gold files by using cone-beam computed tomography. J. Contemp. Dent. Pract. 2019, 20, 330–334. [Google Scholar]
- Gündoğar, M.; Uslu, G.; Özyürek, T.; Plotino, G. Comparison of the cyclic fatigue resistance of VDW Rotate, TruNatomy, 2Shape, and HyFlex CM nickel-titanium rotary files at body temperature. Restor. Dent. Endod. 2020, 45, e37. [Google Scholar] [CrossRef] [PubMed]
- Çırakoglu, N.Y.; Özbay, Y. Apically extruded debris associated with ProTaper Next, ProTaper Gold, and TruNatomy systems: An in vitro study. J. Dent. Res. Dent. Clin. Dent. Prospect. 2021, 15, 35. [Google Scholar] [CrossRef] [PubMed]
- Özyürek, T.; Yılmaz, K.; Uslu, G. Shaping ability of Reciproc, WaveOne GOLD, and HyFlex EDM single-file systems in simulated S-shaped canals. J. Endod. 2017, 43, 805–809. [Google Scholar] [CrossRef] [PubMed]
- Generali, L.; Puddu, P.; Borghi, A.; Brancolini, S.; Lusvarghi, L.; Bolelli, G.; Consolo, U.; Pedulla, E. Mechanical properties and metallurgical features of new and ex vivo used Reciproc Blue and Reciproc. Int. Endod. J. 2020, 53, 250–264. [Google Scholar] [CrossRef]
- Jiang, Q.; Huang, Y.; Tu, X.; Li, Z.; He, Y.; Yang, X. Biomechanical properties of first maxillary molars with different endodontic cavities: A finite element analysis. J. Endod 2018, 44, 1283–1288. [Google Scholar] [CrossRef]
- Barbosa, A.F.A.; Silva, E.J.N.L.; Coelho, B.P.; Ferreira, C.M.A.; Lima, C.O.; Sassone, L.M. The influence of endodontic access cavity design on the efficacy of canal instrumentation, microbial reduction, root canal filling and fracture resistance in mandibular molars. Int. Endod. J. 2020, 53, 1666–1679. [Google Scholar] [CrossRef] [PubMed]
- Isufi, A.; Plotino, G.; Grande, N.M.; Testarelli, L.; Gambarini, G. Standardization of endodontic access cavities based on 3-dimensional quantitative analysis of dentin and enamel removed. J. Endod. 2020, 46, 1495–1500. [Google Scholar] [CrossRef]
- Shabbir, J.; Zehra, T.; Najmi, N.; Hasan, A.; Naz, M.; Piasecki, L.; Azim, A.A. Access cavity preparations: Classification and literature review of traditional and minimally invasive endodontic access cavity designs. J. Endod. 2021, 47, 1229–1244. [Google Scholar] [CrossRef]
- Schneider, S.W. A comparison of canal preparations in straight and curved root canals. Oral Surg. Oral Med. Oral Pathol. 1971, 32, 271–275. [Google Scholar] [CrossRef]
- Moshari, A.A.; Akhlaghi, N.M.; Rahimifard, N.; Darmiani, S. Reduction of Enteroccocus faecalis in curved root canals after various sizes and tapers of canal preparation. J. Conserv. Dent. 2015, 18, 306–309. [Google Scholar] [PubMed] [Green Version]
- Schlafer, S.; Garcia, J.; Meyer, R.L.; Vaeth, M.; Neuhaus, K.W. Effect of DNase treatment on adhesion and early biofilm formation of Enteroccocus faecalis. Eur. Endod. J. 2018, 3, 82–86. [Google Scholar]
- Basmaci, F.; Öztan, M.D.; Kiyan, M. Ex vivo evaluation of various instrumentation techniques and irrigants in reducing E. faecalis within root canals. Int. Endod. J. 2013, 46, 823–830. [Google Scholar] [CrossRef] [PubMed]
- Machado, M.E.L.; Nabeshima, C.K.; Leonardo, M.F.P.; Reis, F.A.S.; Britto, M.L.B.; Cai, S. Influence of reciprocating single-file and rotary instrumentation on bacterial reduction on infected root canals. Int. Endod. J. 2013, 46, 1083–1087. [Google Scholar] [CrossRef] [PubMed]
- Chuste-Guillot, M.P.; Badet, C.; Peli, J.F.; Perez, F. Effect of three nickel-titanium rotary file techniques on infected root dentin reduction. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 102, 254–258. [Google Scholar] [CrossRef] [PubMed]
- Küçükkaya, E.S.; Uzunoğlu-Özyürek, E.; Karahan, S. Influence of reciprocating and rotary instrumentation on microbial reduction: A systematic review and meta-analysis of in vitro studies. Restor. Dent. Endod. 2021, 46, e19. [Google Scholar] [CrossRef]
- Tewari, R.K.; Ali, S.; Mishra, S.K.; Kumar, A.; Andrabi, S.M.U.N.; Zoya, A.; Alam, S. Mechanical reduction of the intracanal Enterococcus faecalis population by Hyflex CM, K3 XF, ProTaper Next, and two manual instrument systems: An in vitro comparative study. J. Investig. Clin. Dent. 2016, 7, 168–173. [Google Scholar] [CrossRef]
- Halkai, R.; Hegde, M.N.; Halkai, K. Enteroccocus faecalis can survive extreme challenges-overview. Nitte. Univ. J. Health Sci. 2012, 2, 49–53. [Google Scholar]
- Portenier, I.; Waltimo, T.; Ørstavik, D.; Haapasalo, M. The susceptibility of starved, stationary phase, and growing cells of Enteroccocus faecalis to endodontic medicaments. J. Endod. 2005, 31, 380–386. [Google Scholar] [CrossRef]
- Otero, D.; Selvaraju, S.B.; Kathpalia, A.; Elmallah, W.; Elbatouty, K.; Nagy, M.M. Evaluation of bacterial reduction after root canal shaping using ProTaper Gold and WaveOne Gold rotary systems. Eur. J. Gen. Dent. 2021, 10, 73–77. [Google Scholar] [CrossRef]
- Rover, G.; Belladonna, F.G.; Bortoluzzi, E.A.; De-Deus, G.; Silva, E.J.N.L.; Teixeira, C.S. Influence of access cavity design on root canal detection, instrumentation efficacy, and fracture resistance assessed in maxillary molars. J. Endod. 2017, 43, 1657–1662. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).