
Towards an Extensive Thumb Assist: A Comparison between Whole-Finger and Modular Types of Soft Pneumatic Actuators


Abstract
:1. Introduction
2. Actuator Structure and Fabrication
2.1. RoM Requirements of Actuators
2.2. Consideration of Actuator Design Parameters
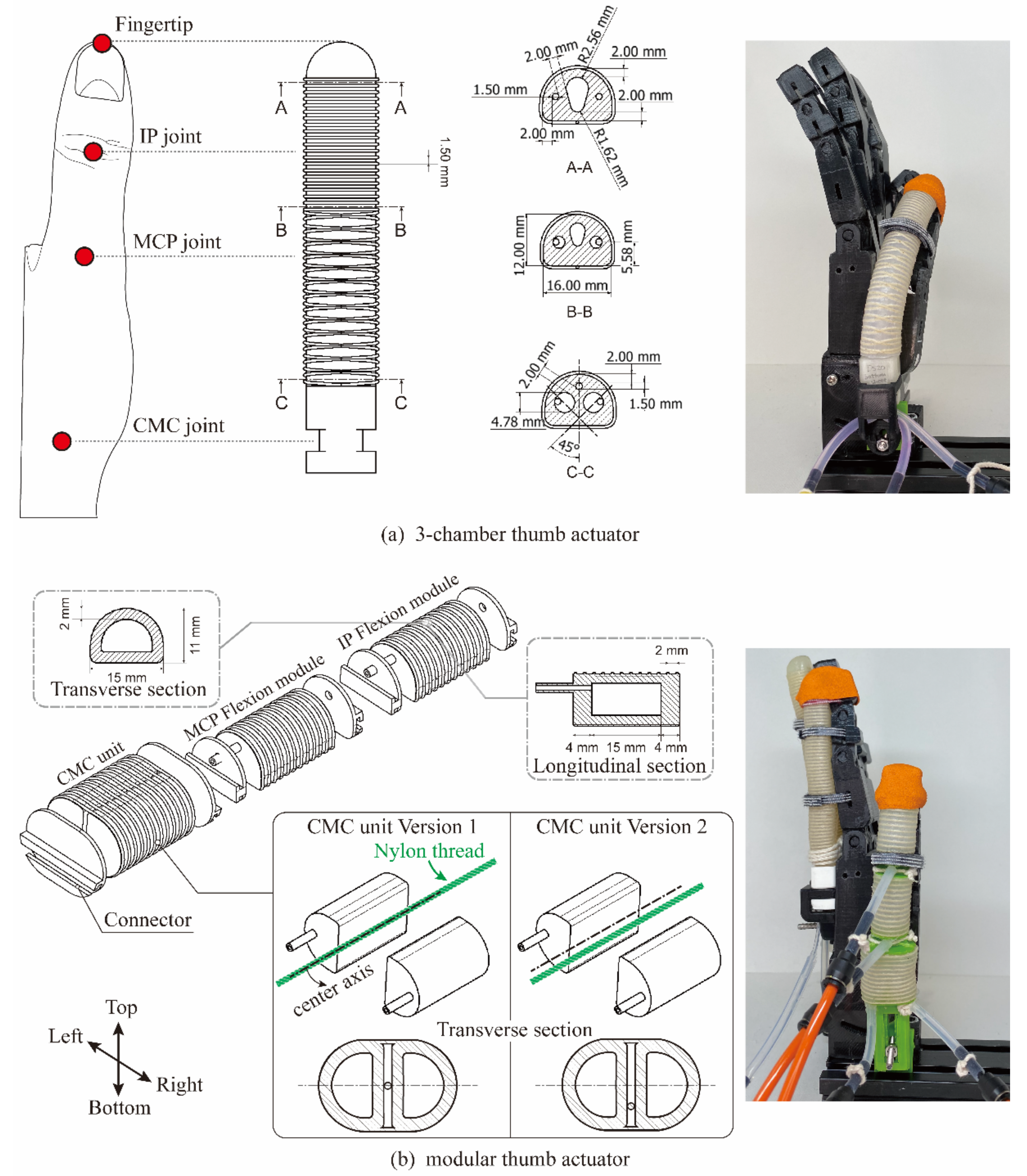
2.2.1. Whole-Finger Thumb Actuator: Three-Chamber Actuator
2.2.2. Modular Thumb Actuator
2.3. Actuator Manufacture
3. Evaluations
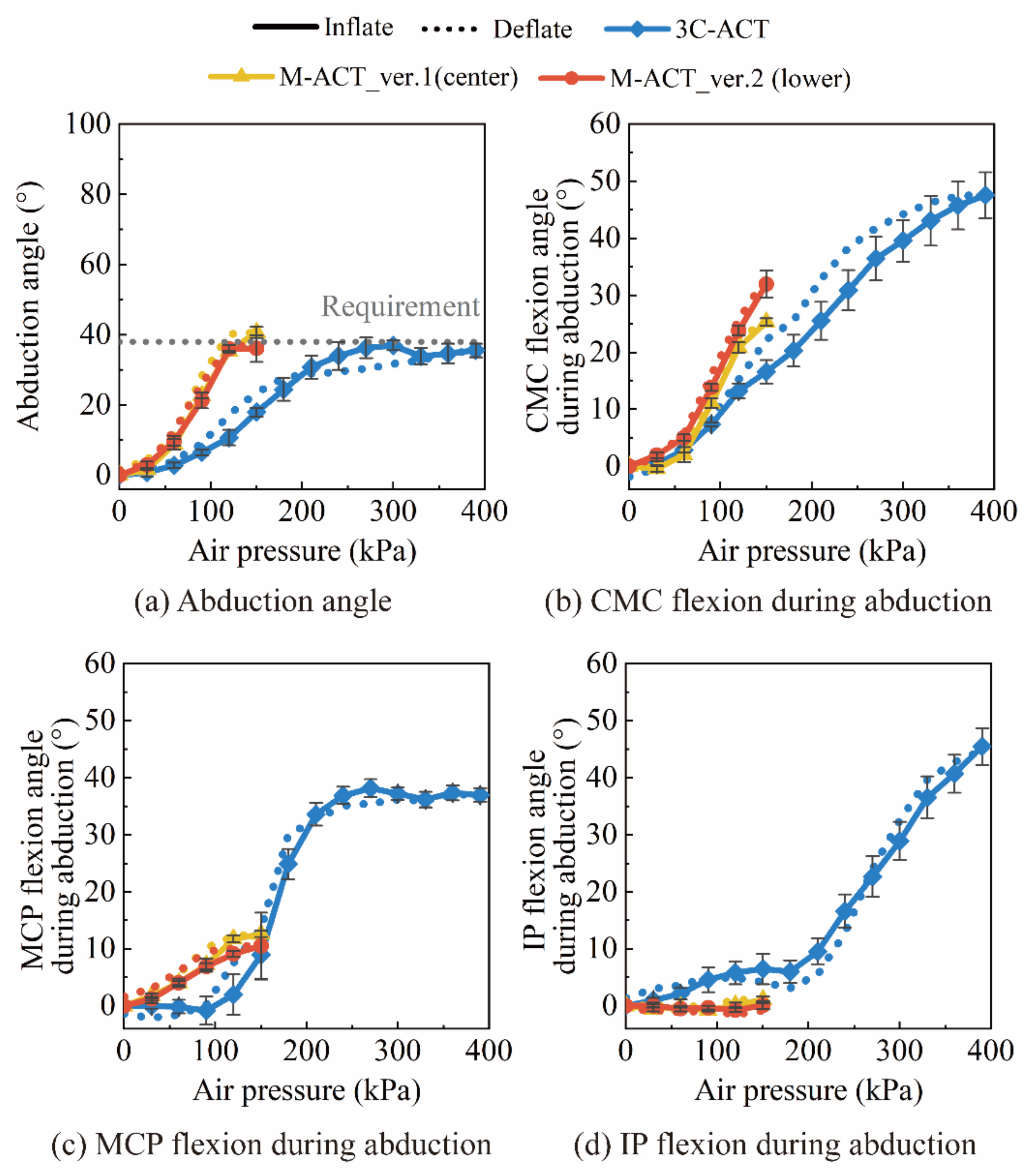
3.1. RoM Measurement
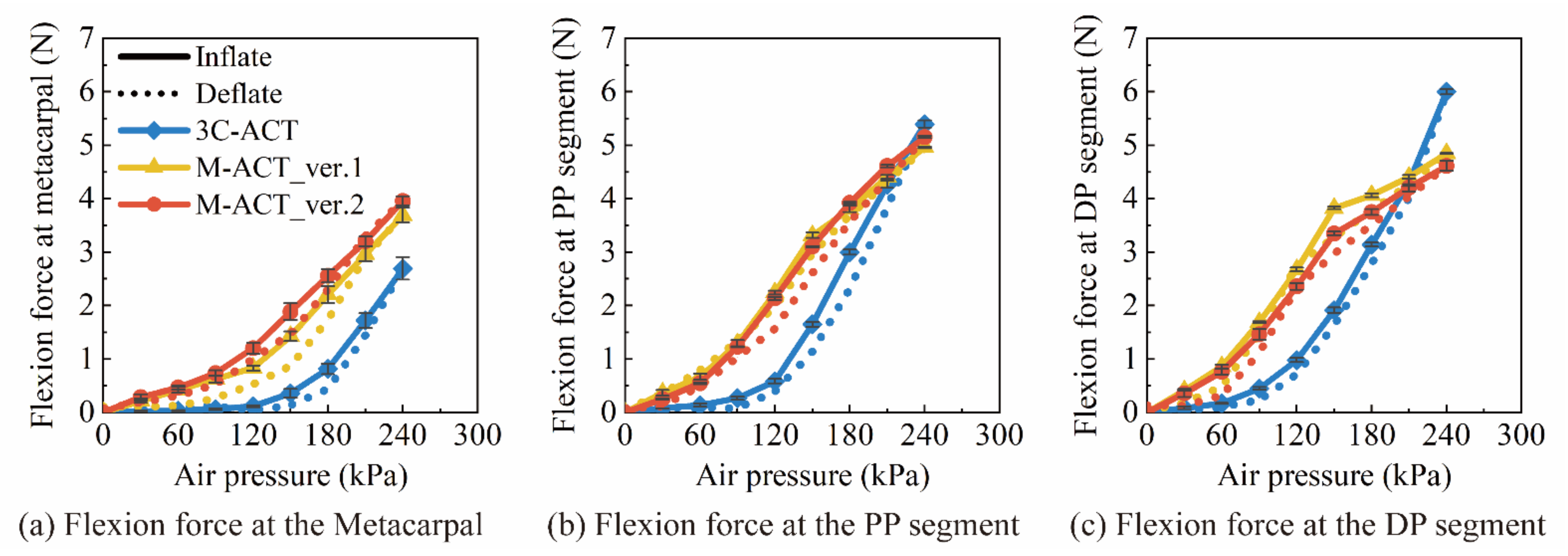
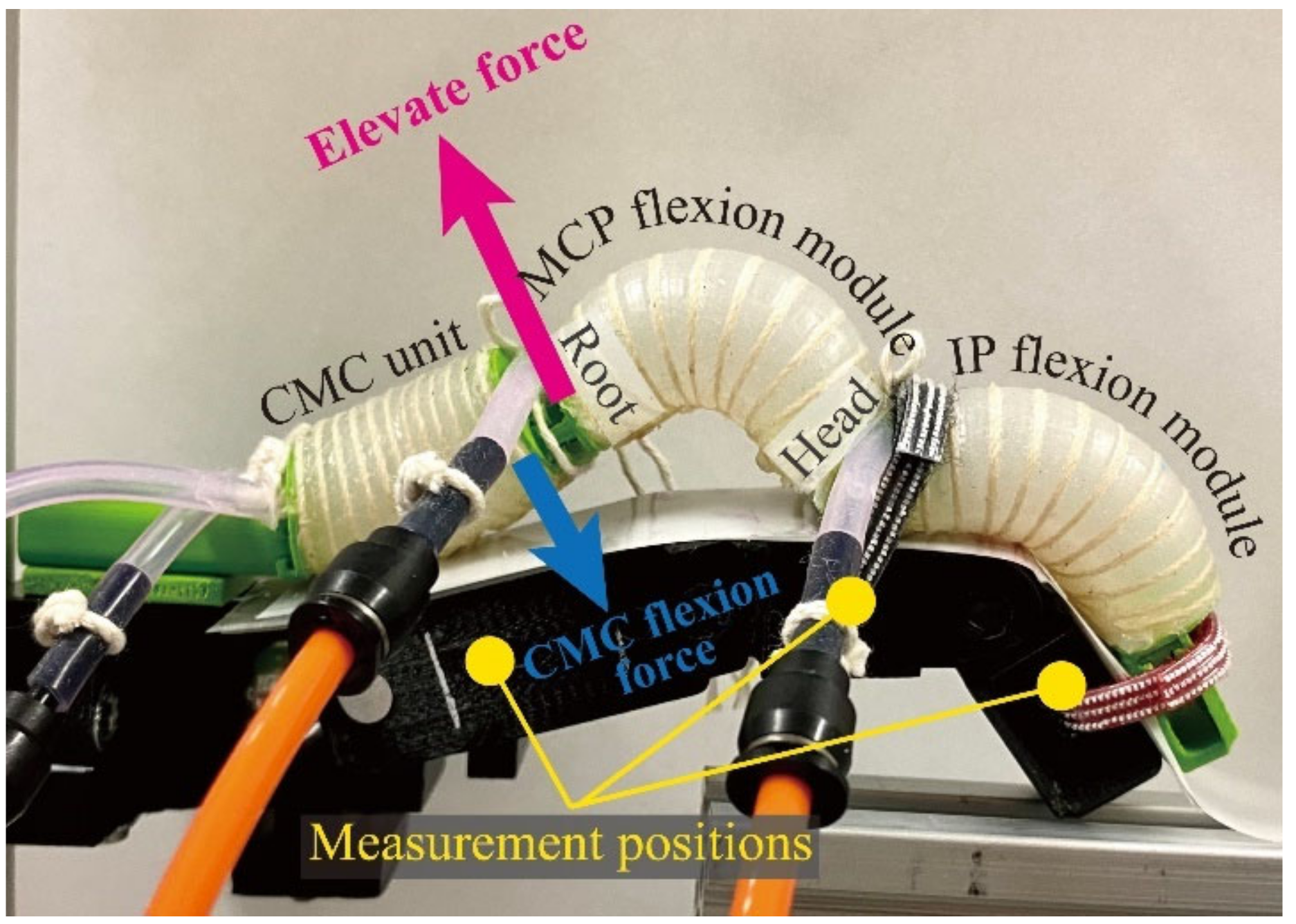
3.2. Force Output Measurement
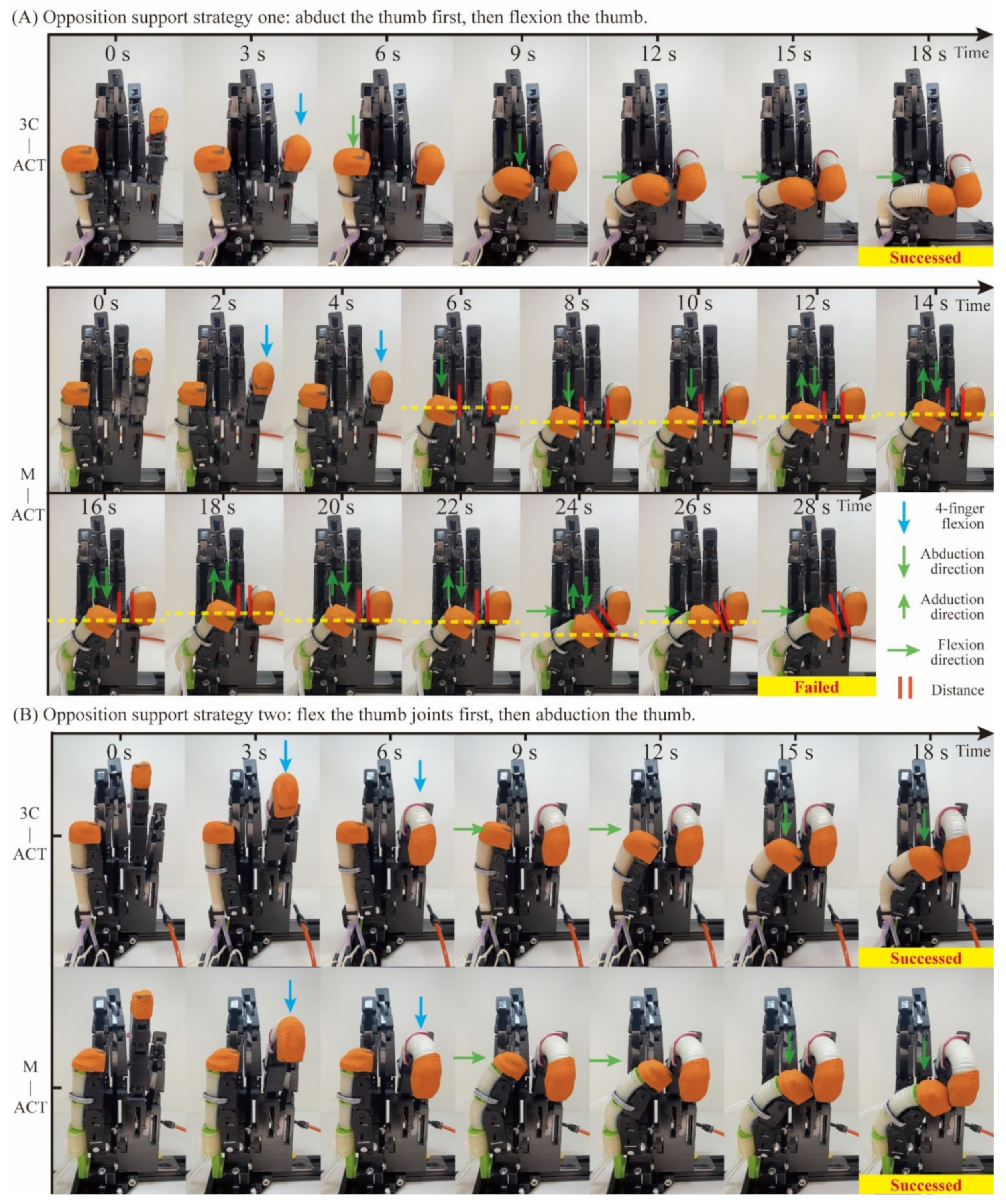
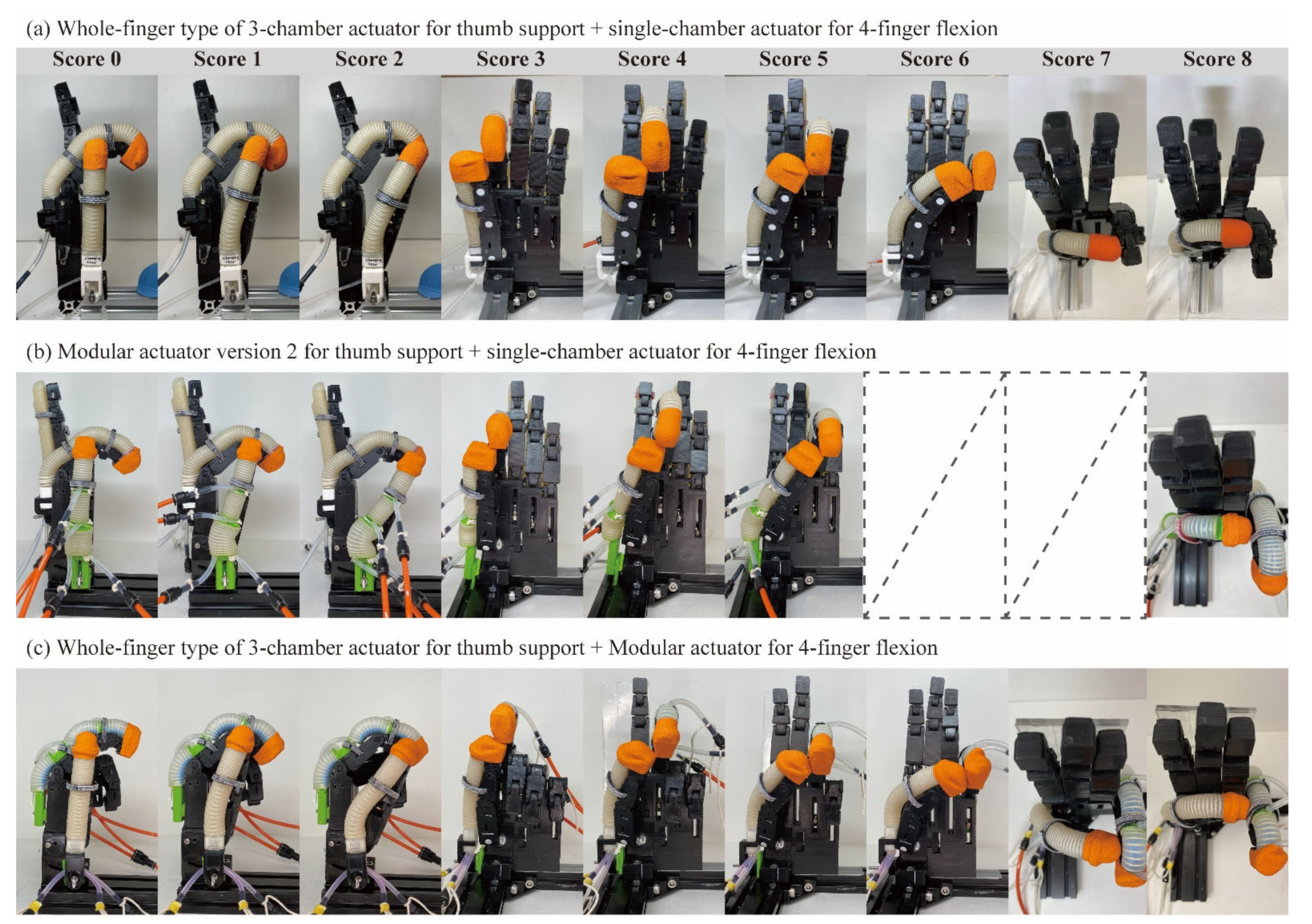
3.3. The Measurement of the Enhanced Kapndji Test
- A 3C-ACT for thumb assistance and a conventional single-chamber actuator for four-finger assistance.
- An M-ACT for thumb assistance and a single-chamber actuator for four-finger assistance.
- A 3C-ACT for thumb assistance and an M-ACT with three flexion modules connected in series for four-finger assistance.
4. Results
4.1. RoM Results
4.1.1. Flexion RoM
4.1.2. Abduction RoM
4.2. Force Output Results
4.2.1. Flexion Force
4.2.2. Abduction Torque/Force
4.3. The Enhanced Kapandji Test Results
4.3.1. Kapandji Score
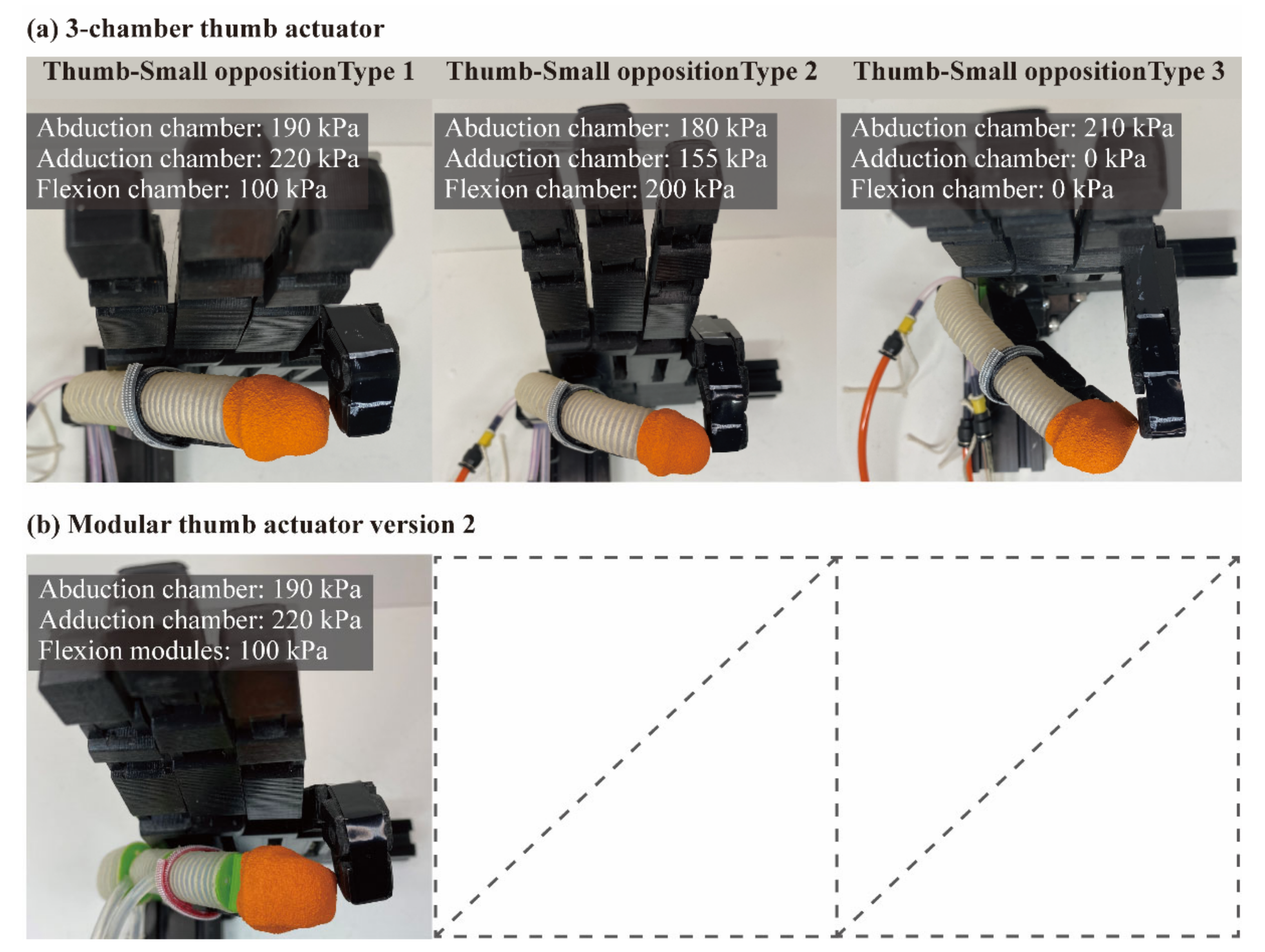
4.3.2. Thumb–Small Opposition
4.3.3. Thumb-Tip Pinch Force
5. Discussion
5.1. Comparison between the Two Versions of Modular Thumb Actuator
5.2. Comparison between the Modular Actuator and the Three-Chamber Actuator
5.2.1. Single-DoF Support Performance
5.2.2. Multi-DoF Support Performance
6. Contribution and Future Work
- The superior single-DoF support capability of the modular thumb actuator.
- The superior multi-DoF support capability of the whole-finger thumb actuator.
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| WPI | whole-person impairment |
| RoM | range of motion |
| DoF | degree of freedom |
| MCP | metacarpophalangeal (thumb middle joint) |
| CMC | carpometacarpal (thumb root joint) |
| IP | interphalangeal (thumb tip joint) |
| DP | distal phalanx (thumb tip segment) |
| PP | proximal phalanx (thumb middle segment) |
| M-ACT | modular finger actuator |
| 3C-ACT | three-chamber actuator |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Actuator combination | Thumb–Index | Thumb–Middle | Thumb–Ring | Thumb–Small | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Chamber for Thumb Abduction | Chamber for Thumb Flexion | Chamber for 4-Finger Flexion | Chamber for Thumb Abduction | Chamber for Thumb Flexion | Chamber for 4-Finger Flexion | Chamber for Thumb Abduction | Chamber for Thumb Flexion | Chamber for 4-Finger Flexion | Chamber for Thumb Abduction | Chamber for Thumb Flexion | Chamber for 4-Finger Flexion | |
| 3C-ACT + single-chamber ACT | 150 | 0–240 | 90–150 | 180 | 0–240 | 160–240 | 195 | 0–240 | 160–240 | 210 | 0–240 | 150–240 |
| M-ACT + single-chamber ACT | 100 | 0–240 | 90–150 | 100 | 0–240 | 160–240 | 90 | 90–240 | 130–240 | - | - | - |
| 3C-ACT + M-ACT | 90 | 0–240 | 230–300 | 150 | 0–240 | 280–300 | 170 | 120–240 | 300 (max) | 190 | 150–240 | 260–300 |
References
- Raghavan, P. The nature of hand motor impairment after stroke and its treatment. Curr. Treat. Options Cardiovasc. Med. 2007, 9, 221–228. [Google Scholar] [CrossRef]
- Australia Government. Commission for the Safety Rehabilitation and Compensation of Commonwealth Employee; Guide to the Assessment of the Degree of Permanent Impairment (Edition 2.1). 2009. Available online: https://www.comcare.gov.au/__data/assets/pdf_file/0015/100905/Guide_to_the_assessment_of_the_degree_of_permanent_impairment_the_Guide_Edition_2.1_of_the_Guide_PDF,_1.84_MB.pdf (accessed on 25 February 2022).
- Fischer, H.C.; Triandafilou, K.M.; Thielbar, K.O.; Ochoa, J.M.; Lazzaro, E.D.; Pacholski, K.A.; Kamper, D.G. Use of a Portable Assistive Glove to Facilitate Rehabilitation in Stroke Survivors With Severe Hand Impairment. IEEE Trans. Neural Syst. Rehabil. Eng. 2016, 24, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Proulx, C.E.; Beaulac, M.; David, M.; Deguire, C.; Haché, C.; Klug, F.; Kupnik, M.; Higgins, J.; Gagnon, D.H. Review of the effects of soft robotic gloves for activity-based rehabilitation in individuals with reduced hand function and manual dexterity following a neurological event. J. Rehabil. Assist. Technol. Eng. 2020, 7, 2055668320918130. [Google Scholar] [CrossRef] [PubMed]
- Radder, B.; Prange-Lasonder, G.B.; Kottink, A.I.R.; Melendez-Calderon, A.; Buurke, J.H.; Rietman, J.S. Feasibility of a wearable soft-robotic glove to support impaired hand function in stroke patients. J. Rehabil. Med. 2018, 50, 598–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiloyannis, M.; Cappello, L.; Khanh, D.B.; Yen, S.C.; Masia, L. Modelling and Design of a Synergy-Based Actuator for a Tendon-Driven Soft Robotic Glove. In Proceedings of the 2016 6th IEEE International Conference on Biomedical Robotics and Biomechatronics (BioRob), Singapore, 26–29 July 2016; pp. 1213–1219. [Google Scholar] [CrossRef]
- Chirinos, S.C.; Vela, E.A. A Modular Soft Robotic Exoskeleton for Active Hand Rehabilitation after Stroke. In Proceedings of the 2021 IEEE Engineering International Research Conference (EIRCON), Lima, Peru, 27–29 October 2021; pp. 1–4. [Google Scholar] [CrossRef]
- Yoon, J.G.; Lee, M.C. Design of tendon mechanism for soft wearable robotic hand and its fuzzy control using electromyogram sensor. Intell. Serv. Robot. 2021, 14, 119–128. [Google Scholar] [CrossRef]
- Jo, I.; Bae, J. Design and control of a wearable and force-controllable hand exoskeleton system. Mechatronics 2017, 41, 90–101. [Google Scholar] [CrossRef]
- Connolly, F.; Walsh, C.J.; Bertoldi, K. Automatic design of fiber-reinforced soft actuators for trajectory matching. Proc. Natl. Acad. Sci. USA 2017, 114, 51–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polygerinos, P.; Galloway, K.C.; Savage, E.; Herman, M.; Donnell, K.O.; Walsh, C.J. Soft Robotic Glove for Hand Rehabilitation and task Specific Training. In Proceedings of the IEEE International Conference on Robotics and Automation, Seattle, WA, USA, 25–30 May 2015; pp. 2913–2919. [Google Scholar] [CrossRef]
- Polygerinos, P.; Wang, Z.; Galloway, K.C.; Wood, R.J.; Walsh, C.J. Soft robotic glove for combined assistance and at-home rehabilitation. Robot. Auton. Syst. 2015, 73, 135–143. [Google Scholar] [CrossRef] [Green Version]
- Yap, H.K.; Ang, B.W.K.; Lim, J.H.; Goh, J.C.H.; Yeow, C.-H. A Fabric-Regulated Soft Robotic Glove with User Intent Detection Using EMG and RFID for Hand Assistive Application. In Proceedings of the 2016 IEEE International Conference on Robotics and Automation (ICRA), Stockholm, Sweden, 16–21 May 2016; pp. 3537–3542. [Google Scholar] [CrossRef]
- Polygerinos, P.; Lyne, S.; Wang, Z.; Nicolini, L.F.; Mosadegh, B.; Whitesides, G.M.; Walsh, C.J. Towards a Soft Pneumatic Glove for Hand Rehabilitation. In Proceedings of the IEEE/RSJ International Conference on Intelligent Robots and Systems, Tokyo, Japan, 3–7 November 2013; pp. 1512–1517. [Google Scholar] [CrossRef]
- Gu, G.; Wang, D.; Ge, L.; Zhu, X. Analytical Modeling and Design of Generalized Pneu-Net Soft Actuators with Three-Dimensional Deformations. Soft Robot. 2021, 8, 462–477. [Google Scholar] [CrossRef]
- Wang, J.; Fei, Y.; Pang, W. Design, Modeling, and Testing of a Soft Pneumatic Glove With Segmented PneuNets Bending Actuators. IEEE/ASME Trans. Mechatron. 2019, 24, 990–1001. [Google Scholar] [CrossRef]
- Yap, H.K.; Lim, J.H.; Nasrallah, F.; Goh, J.C.H.; Yeow, R.C.H. A Soft Exoskeleton for Hand Assistive and Rehabilitation Application Using Pneumatic Actuators with Variable Stiffness. In Proceedings of the 2015 IEEE International Conference on Robotics and Automation (ICRA), Seattle, WA, USA, 26–30 May 2015; pp. 4967–4972. [Google Scholar] [CrossRef]
- Li, M.; Wang, T.; Zhuo, Y.; He, B.; Tao, T.; Xie, J.; Xu, G. A Soft Robotic Glove for Hand Rehabilitation Training Controlled by Movements of the Healthy Hand. In Proceedings of the 7th International Conference on Ubiquitous Robots (UR), Kyoto, Japan, 22–26 June 2020; pp. 62–67. [Google Scholar] [CrossRef]
- Shiota, K.; Kokubu, S.; Tarvainen, T.V.; Sekine, M.; Kita, K.; Huang, S.Y.; Yu, W. Enhanced Kapandji test evaluation of a soft robotic thumb rehabilitation device by developing a fiber-reinforced elastomer-actuator based 5-digit assist system. Robot. Auton. Syst. 2018, 111, 20–30. [Google Scholar] [CrossRef]
- Heung, K.H.L.; Tong, R.K.Y.; Lau, A.T.H.; Li, Z. Robotic Glove with Soft-Elastic Composite Actuators for Assisting Activities of Daily Living. Soft Robot. 2019, 6, 289–304. [Google Scholar] [CrossRef]
- Heung, H.L.; Tang, Z.Q.; Shi, X.Q.; Tong, K.Y.; Li, Z. Soft Rehabilitation Actuator With Integrated Post-stroke Finger Spasticity Evaluation. Front. Bioeng. Biotechnol. 2020, 8, 111. [Google Scholar] [CrossRef] [Green Version]
- Guo, N.; Sun, Z.; Wang, X.; Yeung, E.H.K.; To, M.K.T.; Li, X.; Hu, Y. Simulation analysis for optimal design of pneumatic bellow actuators for soft-robotic glove. Biocybern. Biomed. Eng. 2020, 40, 1359–1368. [Google Scholar] [CrossRef]
- Hu, D.; Zhang, J.; Yang, Y.; Li, Q.; Li, D.; Hong, J. A Novel Soft Robotic Glove with Positive-Negative Pneumatic Actuator for Hand Rehabilitation. In Proceedings of the IEEE/ASME International Conference on Advanced Intelligent Mechatronics, Virtual event, 6–10 July 2020; pp. 1840–1847. [Google Scholar] [CrossRef]
- Jones, L.A.; Lederman, S.J. Human Hand Function; Oxford University Press: New York, NY, USA, 2007; pp. 141–143. [Google Scholar] [CrossRef]
- Barakat, M.J.; Field, J.; Taylor, J. The Range of Movement of the Thumb. Hand 2013, 8, 179–182. [Google Scholar] [CrossRef] [Green Version]
- Holzbauer, M.; Hopfner, M.; Haslhofer, D.; Kwasny, O.; Duscher, D.; Froschauer, S.M. Radial and palmar active range of motion measurement: Reliability of six methods in healthy adults. J. Plast. Surg. Hand Surg. 2020, 55, 41–47. [Google Scholar] [CrossRef]
- Wang, Y.; Kokubu, S.; Zhou, Z.; Guo, X.; Hsueh, Y.-H.; Yu, W. Designing Soft Pneumatic Actuators for Thumb Movements. IEEE Robot. Autom. Lett. 2021, 6, 8450–8457. [Google Scholar] [CrossRef]
- Kokubu, S.; Wang, Y.; Tortós Vinocour, P.E.; Lu, Y.; Huang, S.; Nishimura, R.; Hsueh, Y.-H.; Yu, W. Evaluation of Fiber-Reinforced Modular Soft Actuators for Individualized Soft Rehabilitation Gloves. Actuators 2022, 11, 84. [Google Scholar] [CrossRef]
- Kapandji, A.I. Clinical evaluation of the thumb’s opposition. J. Hand Ther. 1992, 5, 102–106. [Google Scholar] [CrossRef]
- De Kraker, M.; Selles, R.W.; Schreuders, T.A.R.; Stam, H.J.; Hovius, S.E.R. Palmar Abduction: Reliability of 6 Measurement Methods in Healthy Adults. J. Hand Surg. 2009, 34, 523–530. [Google Scholar] [CrossRef]
- Schuind, F.; Garcia-Elias, M.; Cooney, W.P.; An, K.-N. Flexor tendon forces: In vivo measurements. J. Hand Surg. 1992, 17, 291–298. [Google Scholar] [CrossRef]
- Ellegaard, K.; von Bülow, C.; Ropke, A.; Bartholdy, C.; Hansen, I.S.; Rifbjerg-Madsen, S.; Henriksen, M.; Wæhrens, E.E. Hand exercise for women with rheumatoid arthritis and decreased hand function: An exploratory randomized controlled trial. Arthritis Res. Ther. 2019, 21, 158. [Google Scholar] [CrossRef] [PubMed] [Green Version]



| Thumb Motion | Real Thumb RoM [°] | Actuator RoM Requirement [°] | |
|---|---|---|---|
| Goniometer Value | OpenCV Value | ||
| IP joint flexion | 90 | 89 | 89 |
| MCP joint flexion | 37 | 32 | 32 |
| CMC joint flexion | 15 | 13 | 13 |
| CMC joint abduction | 43 | 38 | 38 |
| Actuator Combination | Thumb–Index | Thumb–Middle | Thumb–Ring | Thumb–Small |
|---|---|---|---|---|
| 3C-ACT (thumb) + single-chamber ACT (4-finger) | 5.7 | 4.1 | 3.7 | 4 |
| M-ACT (thumb) + single-chamber ACT (4-finger) | 5.8 | 4.3 | 3.2 | - |
| 3C-ACT (thumb) + M-ACT (4-finger) | 6.2 | 5.0 | 3.5 | 3.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Kokubu, S.; Huang, S.; Hsueh, Y.-H.; Yu, W. Towards an Extensive Thumb Assist: A Comparison between Whole-Finger and Modular Types of Soft Pneumatic Actuators. Appl. Sci. 2022, 12, 3735. https://doi.org/10.3390/app12083735
Wang Y, Kokubu S, Huang S, Hsueh Y-H, Yu W. Towards an Extensive Thumb Assist: A Comparison between Whole-Finger and Modular Types of Soft Pneumatic Actuators. Applied Sciences. 2022; 12(8):3735. https://doi.org/10.3390/app12083735
Chicago/Turabian StyleWang, Yuanyuan, Shota Kokubu, Shaoying Huang, Ya-Hsin Hsueh, and Wenwei Yu. 2022. "Towards an Extensive Thumb Assist: A Comparison between Whole-Finger and Modular Types of Soft Pneumatic Actuators" Applied Sciences 12, no. 8: 3735. https://doi.org/10.3390/app12083735