Abstract
In forensics, the positive identification of decomposed or skeletonized bodies is a fundamental task, with the age-at-death estimation of adult individuals as one of the main objectives. Among different dental methods, root dentin translucency (RDT) is often applied since it is easy to perform and non-destructive. However, this method has some biases, and several equations have been proposed in the literature. This study aimed to test the performance of the previously published equations in an Italian sample with known age and sex, and to develop an equation specific to the Italian population. In total, we examined a sample of 155 single and multi-rooted teeth from male and female individuals aged 18-85 years. The regression equation developed for Italians was tested on a holdout sample drawn from the same population. Intra- and inter-observer errors were calculated using ICC analysis. Both root length and RDT showed excellent repeatability and reproducibility regardless of tooth type. Two of the seven published equations tested performed better in our sample, but the newly proposed equation performed better than those on the Italian population. In conclusion, RDT has proven to be a reliable indicator for age estimation, and the proposed new formula may be effective in such estimation, especially in individuals aged <40.
1. Introduction
In the forensic field, the reconstruction of an individual biological profile (generic identification) from human remains in varying degrees of decomposition or completely skeletonized involves considerable difficulty, especially in estimating the age at death [1]. Age assessment is particularly difficult in adults because of the variability of morphological characters (e.g., sternal rib morphology or auricular surface changes) generally used as indicators of the age of death. Because of this, Ubelaker [2] recommends using several age indicators to assess age at death in adults.
The use of teeth in the assessment of age at death is always of great importance but becomes essential when other skeletal indicators are weakly preserved. While in immature individuals, one of the most accurate indicators of age is the degree of dental development [2], in adults, other indicators are required. Regarding dental methodologies, an age-at-death estimation can be performed on adult skeletons by invasive or noninvasive techniques. Specifically, among the different dental age estimation methods that can be employed are the Lamendin method, tooth cementum thickness, dental cementum annulation, and aspartic acid racemization [3,4,5,6,7]. Some of these dental methods require histological analysis that will lead to the destruction of the tooth. Wanting to apply a noninvasive method, root dentin translucency (RDT) and gingival regression (periodontosis) can be employed following Lamendin et al. [6]. Previous studies conducted on samples from different populations have shown a good performance of this method which is based on the increasing level of RDT with age [8,9,10]. However, validation studies of RDT have shown a tendency for overestimation of age in young individuals and underestimation in older individuals [8,11]. More generally, the inaccuracy of all skeletal and dental indicators increases above 60 years of age [12]. In this regard, Martrille et al. [12] showed that the RDT method was the most effective in the 41–60 age group among four different age assessment methods (pubic symphysis, auricular surface, fourth ribs, RDT). Contrasting findings on the effect of sex on age estimation by RDT resulted from the literature, with the sex being significant [8,13] or non-significant factor [6,14] depending on the studies. Another particularly important issue that emerged from the literature concerns the differences among populations [8,15,16]. In addition to possible genetic differences, environmental factors (hygiene and dental care) may affect RDT [8,16]. Moreover, the majority of the equations proposed to estimate the age are based on single-rooted teeth, and few attempts have been made to test their efficacy on multi-rooted teeth [17,18].
The apparent ease of the technique, its noninvasiveness, and the feasibility of the application, which requires only the use of a caliper and an appropriate light system for the RDT recording, contribute to its particular interest. However, its reliability should be ascertained before its application in forensics, taking into account sex and population. Moreover, the influence of tooth type should be analyzed more deeply. Therefore, this study aims to: (i) test the inter- and intra-operator variability considering tooth age and type; (ii) test the reliability of previously proposed age estimation formulas [6,8,10,17,19,20,21] on a sample of Italians, considering age classes and tooth type; and (iii) test and develop new specific formulae for deriving the most reliable estimate of age in modern Italians.
2. Materials and Methods
2.1. Sample
In this study, we investigated a sample of 155 permanent teeth which were extracted for therapeutic needs (in 2015–2019). The teeth have been stored in the refrigerator and were not modified or processed in any way after the extraction. The initial sample size was 174 teeth, but 19 of them were excluded from the sample for the impossibility of measuring Root Height (RH) and/or Root Height Translucency (RHT). The sample, in the age range 18–84 years, included both males (n = 63) and females (n = 92). While respecting anonymity, data on the person’s sex and age were collected at the time of dental extraction. In addition, we provided a numerical code for each tooth specimen. Having decided not to give any preference regarding tooth type, we used both multi-rooted and single-rooted teeth for this study [1,19]. As single-rooted, we considered: incisors, canines, inferior premolars, and the second superior premolars. As multi-rooted, we considered: all the molars and the first superior premolars. Teeth with root caries or with any alteration in the cervical apex (ankylosis or reabsorption) were excluded.
2.2. Procedure
According to Lamendin et al. method [6], we recorded translucency height (the maximum distance of the translucency region of the tooth root from the root apex, RHT), periodontal retraction (maximum distance between the cement enamel junction and the line of soft tissues attachment, PH), and maximum root height (the maximum straight-line distance between apex and amelocemental junction, RH) on lingual and labial surfaces directly on the root of un-sectioned teeth (Supplementary Figure S1). Each tooth was examined intact, dry, and cleaned. Tooth sizes were taken using a digital Vernier sliding caliper with a calibration of 0.01 mm (SUNROM, Ahmedabad, Gujarat, India). The translucency measurement was obtained in a dark room, exposing the tooth to a LED light table positioned behind the tooth with an intensity set at 1600 lumen.
2.3. Statistical Analysis
An a priori power analysis was conducted to ensure that the number of participants was representative for the purposes of this study using the program G*Power (3.1.9.2, Universität Kiel, Kiel, Germany). A two-independent Pearson correlation was selected, imputing an α error probability =0.05 and a (1 − β) = 0.95; the effect size was q =0.6. The outcomes parameters thus calculated detected a total sample size of 128 teeth. Moreover, to calculate the a priori sample size required for the regression analysis, we used Green’s rule of thumb (medium effect), which indicated a required total sample size of 105 teeth. Additional subjects were included to ensure the availability of data.
Descriptive statistics were performed through mean and standard deviation for the continuous variables and percentage for the categorical variables. For statistical comparisons, we divided the sample into three age classes (<40; between 40 and 59; ≥60 years) [22]. Comparisons between sexes were performed through independent sample t-tests, whereas comparisons between the three age classes were through analysis of variance (ANOVA). A Tukey post hoc test was also performed.
All the teeth were independently measured by the same operator (A) in two independent measurement sessions one month apart (A1 and A2) and independently by a second operator (B). The first operator was an expert in the field of biological anthropology, whereas the second operator was a master’s student. Intra-operator and inter-operator reliability was assessed by Intraclass Correlation Coefficient (ICC) by comparing the results obtained by the same operator (A1 vs. A2) and the two independent operators (A1 and B), respectively. ICC is based on a two-way model considering single measures and the same rater for all subjects. To prevent bias, both operators were blind to the other’s result and the chronological age (CA) of the subject. Values of ICC below 0.5 indicate poor reliability, between 0.5 and 0.75 moderate reliability, between 0.75 and 0.9 good reliability, and any value above 0.9 indicates excellent reliability [23]. Pearson correlation was performed between CA and the three dental measures (RH, PH, and RHT). We then proceeded to test the different equations of the literature estimating the age of each tooth by applying the formulas of Bang and Ramm [19], Lamendin et al. [6], Prince and Ubelaker [8], Gonzales-Colmenares et al. [17], Ubelaker and Parra [20], Singhal et al. [11], and Bhardwaj et al. [21] (Table 1). Each equation has been applied only on teeth with RHT > 0 and for Bhardawaj’s formula only on RHT ≥ 3. For each equation, we calculated the Bias (mean error: [Ʃ(estimated age − chronological age)]/n), the precision (standard deviation of the mean error), and the inaccuracy (mean absolute error: [Ʃ(ǀestimated age − chronological ageǀ)]/n) [22]. In addition, the number (and percentage) of estimates with errors ≤±5, ≤±10 years, and ≥±15 years was also calculated. Solheim and Sundnes [24] have categorized the former as “acceptable” and designated the latter as “unsatisfactory” in forensic age estimation.

Table 1.
Equations to estimate age-at-death (A) based on dentin translucency from the literature reported separately for indeterminate sexes, male sex and female sex.
The second step was to create a specific regression equation based on the Italian sample. For comparison purposes, we selected randomly from the whole sample (N = 155) a holdout sample of 20 individuals (10 males and 10 females). Data from this subsample were excluded from the database used to develop new formulas for age estimation. Thus, the study sample used consisted of 135 teeth (M = 53; F = 82). To minimize the bias, every holdout group for each sex comprises 3 single-rooted teeth (1 with an age < 40; 1 with an age comprised between 40 and 59 years; 1 with an age > 60 years); 3 multi-rooted teeth (1 with an age < 40; 1 with an age comprised between 40 and 59 years; 1 with an age > 60 years); 4 teeth randomly selected among all the teeth typology and age. In addition, subjects with a translucency value of 0 were excluded from the holdout samples. The final equation was performed using a final dataset of 133 teeth.
The CA of the holdout sample was compared with the age estimated from the equation developed in this study and the equations from the literature that performed better in the previous analysis. Statistical comparisons between CA and estimated age were performed by Wilcoxon paired test. Moreover, Bias, Precision, and Inaccuracy were also calculated.
All data were analyzed using Statistica software version 11.0 (StatSoft Srl, Tulsa, OK, USA) and MedCalc Statistical Software version 14.8.1 (MedCalc Software bvba, Ostend, Belgium).
The level of significance used in all statistical analyses was p < 0.05.
3. Results
The characteristics of the sample are reported in Table S2 of the Supplementary Materials. The sample is mainly composed of females (59.4% of the total sample). Dividing the sample into three age groups, the majority of males were 60 years of age or more, whilst, in females, the youngest and the oldest group are numerically equally represented (p = 0.041). As regards the tooth type, the most represented are the multi-rooted teeth in both sexes (more than two-thirds of the sample).
Table 2 reports the mean and standard deviation of the three considered tooth measures (RH, PH, and RHT). Females’ teeth have significantly lower RH and RHT. Comparing the two sexes, no differences emerged in the PH, whereas RH and RHT resulted in significantly higher in males in the oldest group and the total sample. On the other hand, all three measures are always significantly different between age classes, with an increasing trend with increasing age, both in the total sample and in each sex separately. The youngest group always has significantly lower measures than the other groups.
Table 2.
Mean and standard deviation of the considered tooth measures (RH, PH, and RHT) in the total sample and for each sex separately, divided by age classes.
Table 3 presents the results of the intra- and inter-operator variability for the three considered tooth measures, and Table S3 reports the ICC values for the sample divided by age class. Again, the results indicate excellent reliability for all the measures in the total sample and for the majority of the measures dividing the sample by age class and by tooth type. The only exceptions are RHT for the youngest and the oldest group and PH for the oldest group, which reported good reliability.
Table 3.
ICC intra-operator (first part) e inter-operator (second part) variability for the total sample by tooth type.
Less reliability, in general, resulted in inter-operator variability. ICC for RH indicates excellent reliability in the oldest group and single-rooted teeth, good reliability in the 40–59 years old group and multi-rooted teeth, and moderate in the youngest group. In general, the reliability of the total sample was good. The inter-operator reliability for the PH measures was generally lower, with moderate reliability in the total sample and a decreased reliability with increasing age. The reliability was good for both tooth types, with higher values for multi-rooted teeth. As regard RHT, the reliability was excellent for the total sample and good in the three age groups considered separately (Table S3). Dividing for tooth type, the reliability was excellent for multi-rooted and good for single-rooted teeth.
The correlations between tooth measures and CA are reported in Table 4. The two sexes performed similarly for RH and RHT, but a higher coefficient of correlation is found in females for PH. As expected, RH correlated poorly with age; the strongest correlations were found between CA and RHT. Dividing age groups, RH did not result in significant correlations and PH only for the youngest age group. RHT was strongly correlated with CA in the youngest group, but no correlation resulted in the oldest one. As regards the differences between tooth types, for all three variables, the strongest correlations are found in the multi-rooted teeth.
Table 4.
Pearson correlation between variables and chronological age by sex, age classes, and tooth type.
In Table 5, we have reported the prediction performance of the selected seven equations from the literature tested in our sample, and in Table S4, the results by age group. Considering the total sample, all the equations tend to underestimate age, with less bias found in the equations of Bang and Ramm [19], Prince and Ubelaker [8], and Singhal et al. [11]. The precision is low in all the formulas and ranges between 10.5 and 18 years, with the highest values in Bhardwaj et al. [21] and the lowest in Gonzales-Colmenares et al. [17] and Lamendin et al. [6]. The inaccuracy is similar for all the equations, with values around 12 years; also, in this case, the equations of Bhardwaj et al. [21] had the highest value. Dividing the sample into three age classes, heterogeneous results were obtained by the different formulas, but the equations that performed better seem those of Bang and Ramm [19], Lamendin et al. [6], Gonzales-Colmenares et al. [17], and Singhal et al. [11]. Also, in this case, Bhardwaj’s formula had the worst performance. All equations gave similar results for the 40–59 age group with a bias that never exceeds ±5.5 years, except for Bhardwaj’s formula. In general, all the equations performed poorly in the oldest age group, with Bang and Ramm [19], Prince and Ubelaker [8], and Singhal et al. [11] that had the best performance. As regard tooth type, the results from different formulas are heterogeneous, but generally, the application of the equations on multi-rooted teeth gave the best results, with lower bias, inaccuracy, and higher precision. Even if the results are quite different based on tooth type and age class, it can be concluded that, in general, the best formulas for our sample were those of Bang and Ramm [19] and Singhal et al. [11].
Table 5.
Bias, precision, and inaccuracy of the selected formula divided for the total sample and tooth type.
Subsequently, we randomly excluded from the total sample a holdout sample of 20 teeth (10 from each sex). From the remaining sample of 135 teeth, the regression analysis was performed. The non-linear quadratic regression gave the best fitting with the following equation:
where x is RHT, the R2 was 0.72, and the SEE was 10.9 years. The graphical representation is reported in Figure 1.
Age = 23.2239 + 9.9108x + (−0.5366x2)
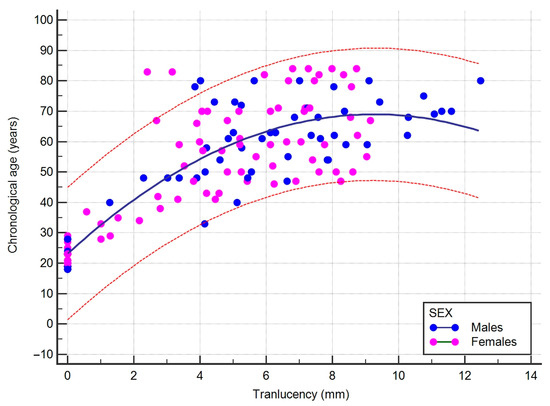
Figure 1.
Scatterplot showing the quadratic correlation and the 95% prediction (red line) between root height translucency (RHT) and chronological age (CA). The blue line represents the regression line. Blue dots represent males, and pink dots females.
The newly created formula was applied to the holdout sample, together with the two equations from the literature that showed the best performance in the total sample, for comparison purposes. No statistical differences between the CA and the estimated age were detected using our formula (p = 0.202) or Singhal’s formula (p = 0.597); instead, the difference between CA and the age estimated with the Bang and Ramm’s formula resulted in almost significant value (p = 0.0532). Bias, precision, and inaccuracy are reported in Table 6. Our equation performed better both in the total sample and separately by sexes, with values of bias, precision, and inaccuracy slightly lower than those resulting from the application of Singhal’s equations. Bang and Ramm’s equation had higher values, especially in accuracy and precision. Two individuals exceed 15 years of difference between CA and the estimated age calculated with our equations, nine with Bang and Ramm’s equation, and six with Singhal’s equation.
Table 6.
Bias, precision, and inaccuracy were calculated by applying the equation proposed in this study, Bang and Ramm’s and Singhal’s equations on the holdout sample.
4. Discussion
Age estimation constitutes a fundamental goal of Forensic Anthropology in the process of identifying unknown human skeletal remains. Using teeth for age estimation overcomes some of the difficulties that arise from using other anthropological methods based on degenerative changes in bone [17,25]. An additional factor in favor of the application of dental methods is the greater probability of tooth preservation compared to other skeletal elements, even in adverse environments, such as in post-conflict or natural disaster grave sites [26]. Moreover, fieldwork under these difficult conditions makes the RDT method particularly advantageous because it does not need specific instrumentation [26]. Other dental methods used in age estimation include Tooth Cementum Annulations (TCA) and total cementum thickness measurement, both involving histological techniques, while aspartic acid racemization requires a mass spectrometric analysis. Unlike the above methods, the RDT is a non-destructive, simple method and requires no special technical equipment [27].
The method of RDT for age-at-death estimation is based on a specific characteristic of the dentin that becomes translucent with increasing age. The translucency of dentin is a result of increased intratubular mineralization and is first observed in the apical part of the tooth due to the smaller diameter of the dentinal tubules in the root dentin than in the coronal part [11]. In this study, our purpose was to validate this French technique in a sample of Italian adults allowing the method to be extended to a different population than the one in which it was developed [6] or validated (among others: [8,15,16,17]).
Current research gives support for the application of the dental translucency method in adult age estimation. We found good/excellent inter- and intra-operator reliability for all dental measurements taken. In particular, RHT reliability was excellent for multi-rooted teeth.
Previous studies had shown a greater association of CA with RDT than with other techniques, reporting correlation coefficients between 0.65 and 0.87 [11,19,28,29]. Our results, with values of the r coefficient being within this range for the total sample, confirm the strong association between RHT and CA. However, this association decreases with age since there would be slower development of translucency in old age because of a possible delay in this process in the root’s coronal part [11,19]. The increase of RDT with increasing age is generally deemed a physiological change with aging [30]. Moreover, errors in estimating the age of older people may result from the fact that root shortening may mask the concomitant increase in root translucency [16]. As a result of this, we found a more precise and accurate age estimation in individuals aged < 40 years and an underestimation of age in older people according to a pattern observable from age 40 and beyond consistently with the literature [11,17,31]. Unlike the age factor, sex does not seem to influence the age estimate obtained with RTD significantly. This result generally finds confirmation in other previous studies (among others: [10,14,31]).
Other studies previously developed and applied regression equations to estimate age from dental translucency in different populations (as detailed in Table 1). Because none of these equations has been developed specifically for the Italian population, we checked the reliability of the estimates obtained by applying these formulas to our sample. The results obtained applying these literature equations on the overall Italian sample indicated a better performance with the equations developed by Bang and Ramm [19] and Singhal et al. [11] regardless of population (in the first case, they were Norwegians and in the second Indians) or tooth type (in the first case any type, in the second lower central incisors). Although it is generally believed that biological profiles should be drawn taking into account the population of origin, the results obtained seem to indicate a reduced influence of population affinity on RDT, as also noted by Doria Martinez [32] in contrast to Gonzales-Colmenares et al. [17]. On the other hand, Prince and Ubelaker [8] recognized that ancestry is not a significant factor but suggested considering both ancestry and sex to reduce the mean error. As for tooth type, the use of only single-rooted teeth for RDT purposes is prevalent in the literature, with a few exceptions (among those applied: [19,21]). Confirming previous research [18], our study had the merit of showing that multi-rooted teeth can be used for age estimation, performing even better than mono-rooted teeth. This finding will have an important implication in forensics since age estimation can be conducted anyway, whatever type of tooth is available.
In this study, we developed a new formula to estimate the age of unidentified individuals based on RTD. In particular, this regression equation employs only one variable, as RHT was found to be the most significant age predictor of the three indicators considered. Moreover, PH had lower reliability and reproducibility in comparison to RHT. An analogous choice was made by Bang and Ramm [19] and Bhardwaj et al. [21]. The new equation applied to the holdout sample resulted in a better age estimate than that obtained from the formulas of Bang and Ramm [19] and Singhal et al. [11]. This new equation, therefore, can be considered a relevant addition to the estimation of adult age-at-death in forensics, but its application should be supported by the use of other skeletal indicators of age. Moreover, further studies are needed to validate our new formula on other population samples.
Strengths of this study include the application of a dental method of age estimation that does not require specific and costly laboratory instruments. In addition, we used different types of teeth (mono and multi-rooted), proving the applicability of RDT. Being concerned with forensically unknown human remains, one appreciable element of RHT is that it appears to be little influenced by sex and population affinity. Unlike several other studies that have examined RTD in osteological collections -the remains’ antiquity and the postmortem environment would affect the RTD according to Megyesi et al. [33], we examined a current population sample with known age and sex, thus providing results that can be applied with greater confidence in the forensic field on contemporary human remains. The main limitations of this study relate to the use of extracted teeth for therapeutic purposes. However, according to findings from previous studies [15,34], periodontal disease does not necessarily affect translucency. Lastly, the sample size examined is small when compared with specimens collected from osteological collections [8,10,16] but is numerically similar to or larger than those generally employed in translucency studies in current populations [14,17,26].
5. Conclusions
The relative easiness and accuracy of RTD display its potential in tooth-based age estimation. The results we obtained by examining a sample of mono and multi-rooted teeth from an Italian population confirm that RTD is a precise and accurate method for estimating CA. In addition to the formulas proposed by Bang and Ramm [19] and Singhal et al. [11], the new RTH-based regression equation developed in this study provides acceptable estimates of age at death, especially in individuals aged < 40 years. This regression equation can be relevant in estimating age during the identification process. In any case, to support the estimation provided by the RTD method, multiple anthropological methods or indicators need to be applied in the identification process, especially in forensic cases and in older adults. Future investigations should explore the reliability of this equation in estimating age on other samples of European and non-European populations.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/app13106289/s1, Figure S1: Picture representing the measurement of root length (RH), periodontal retraction (PH), and root height translucency (RHT). RHT has been measured on the labial or buccal surface, exposing the tooth to a light source. Table S1: Bang and Ramm’s coefficient for unsanctioned teeth based on tooth type and RHT > or < than 9 mm (modified by Bang and Ramm [19]); Table S2: Total Italian sample characteristics and distribution by sex, chronological age, and tooth type; Table S3: ICC intra-operator (first part) e inter-operator (second part) variability for the total sample, age groups, and tooth type; Table S4: Bias, precision, and inaccuracy of the selected formula divided for the total sample, age classes, and tooth type. Absolute and relative frequencies of the tooth with less than 5 and 10 years of bias and more than 15 years of bias between actual and estimated age.
Author Contributions
Conceptualization, N.R., M.N. and E.G.-R.; Data curation, N.R., I.S. and F.D.L.; Formal analysis, N.R. and F.D.L.; Investigation, I.S. and P.F.; Methodology, N.R., I.S. and P.F.; Project administration, M.N. and E.G.-R.; Resources, N.R., M.N. and E.G.-R.; Supervision, N.R. and E.G.-R.; Writing—original draft, N.R. and E.G.-R.; Writing—review & editing, N.R., I.S., F.D.L., M.N., P.F. and E.G.-R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to the REASON that data processing complies with the general authorization for scientific research purposes granted by the Italian Data Protection Authority (1 March 2012 as published in Italy’s Official Journal no. 72 dated 26 March 2012) since the data do not entail any significant personalized impact on data subjects. Approval by an institutional and/or licensing committee is not required since experimental protocols are not applied in this study. The patients’ data were completely anonymized, according to Regulation (EU) 2016/679 of the European Parliament and the Council: “The data protection principles should therefore not apply to anonymous information, i.e., information that does not relate to an identified or identifiable natural person or to personal data made sufficiently anonymous to prevent or no longer allow the identification of the data subject. Therefore, this regulation does not apply to the processing of such anonymous information, including for statistical or research purposes.”
Informed Consent Statement
Patient consent was waived due to the REASON listed above, which makes specific Informed Consent unnecessary. As this is a retrospective study using anonymized dental material, it was impossible to contact patients to obtain specific consent for this study.
Data Availability Statement
The databases used and/or analyzed during this study are available from the corresponding authors upon reasonable request.
Acknowledgments
We thank the dentists of the Centro Odontoiatrico Sforza and Studio Odontoiatrico Placanica (Bologna, Italy) for providing the materials used in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Gualdi-Russo, E.; Belcastro, M.G.; Sineo, L.; Capasso, L.; Pilli, E.; Martinez-Labarga, C.; Viciano, J.; Toselli, S. Antropologia forense. In Manuale di Antropologia. Evoluzione e Biodiversità Umana; Sineo, L., Moggi-Cecchi, J., Eds.; UTET: Torino, Italy, 2022; pp. 557–574. [Google Scholar]
- Ubelaker, D.H. Forensic Anthropology: Methodology and applications. In Biological Anthropology of the Human Skeleton, 3rd ed.; Katzenberg, M.A., Grauer, A.L., Eds.; John Wiley & Sons, Inc.: Oxford, UK, 2019; pp. 43–71. [Google Scholar]
- Gualdi-Russo, E.; Saguto, I.; Frisoni, P.; Neri, M.; Mongillo, J.; Rinaldo, N. Age estimation using tooth cementum annulations: Bias and sources of inaccuracy. Front. Biosci.-Landmark 2022, 27, 141. [Google Scholar] [CrossRef]
- Gualdi-Russo, E.; Saguto, I.; Frisoni, P.; Neri, M.; Rinaldo, N. Tooth Cementum Thickness as a Method of Age Estimation in the Forensic Context. Biology 2022, 11, 784. [Google Scholar] [CrossRef]
- Wittwer-Backofen, U.; Gampe, J.; Vaupel, J.W. Tooth cementum annulation for age estimation: Results from a large known-age validation study. Am. J. Phys. Anthr. 2003, 123, 119–129. [Google Scholar] [CrossRef]
- Lamendin, H.; Baccino, E.; Humbert, J.F.; Tavernier, J.C.; Nossintchouk, R.M.; Zerilli, A. A simple technique for age estimation in adult corpses: The two criteria dental method. J. Forensic Sci. 1992, 37, 1373–1379. [Google Scholar] [CrossRef] [PubMed]
- Arany, S.; Ohtani, S. Age estimation by racemization method in teeth: Application of aspartic acid, glutamate, and alanine. J. Forensic Sci. 2010, 55, 701–705. [Google Scholar] [CrossRef] [PubMed]
- Prince, D.A.; Ubelaker, D.H. Application of Lamendin’s adult dental aging technique to a diverse skeletal sample. J. Forensic Sci. 2002, 47, 107–116. [Google Scholar] [CrossRef]
- Ribeiro Lopes, J.; Borges Braga dos Santos Queiroz, S.; Marques Fernandez, M.; Saavedra de Paiva, L.A.; Nogueira de Oliveira, R. Age estimation by teeth periodontosis and transparency: Accuracy of Lamendin’s method on a Brazilian sample. Braz. J. Oral Sci. 2014, 13, 17–21. [Google Scholar] [CrossRef]
- Garizoain, G.; Petrone, S.; Plischuk, M.; Inda, A.M.; Garcia, M.N. Evaluation of Lamendin’s age-at-death estimation method in a documented osteological collection (La Plata, Argentina). Forensic Sci. Int. Rep. 2020, 2, 100060. [Google Scholar] [CrossRef]
- Singhal, A.; Ramesh, V.; Balamurali, P. A comparative analysis of root dentin transparency with known age. J. Forensic Dent. Sci. 2010, 2, 18–21. [Google Scholar] [CrossRef]
- Martrille, L.; Ubelaker, D.H.; Cattaneo, C.; Seguret, F.; Trembla, M.; Baccino, E. Comparison of four skeletal methods for the estimation of age at death on white and black adults. J. Forensic Sci. 2007, 52, 302–307. [Google Scholar] [CrossRef]
- Lorentsen, M.; Solheim, T. Age assessment based on translucent dentine. J. Forensic Odontostomatol. 1989, 7, 3–9. [Google Scholar] [PubMed]
- Foti, B.; Adalian, P.; Signoli, M.; Ardagna, Y.; Dutour, O.; Leonetti, G. Limits of the Lamendin method in age determination. Forensic Sci. Int. 2001, 122, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Zorba, E.; Goutas, N.; Spiliopoulou, C.; Moraitis, K. An evaluation of dental methods by Lamendin and Prince and Ubelaker for estimation of adult age in a sample of modern Greeks. Homo 2018, 69, 17–28. [Google Scholar] [CrossRef]
- Ackermann, A.; Steyn, M. A test of the Lamendin method of age estimation in South African canines. Forensic Sci. Int. 2014, 236, 192.e1–192.e6. [Google Scholar] [CrossRef]
- González-Colmenares, G.; Botella-López, M.C.; Moreno-Rueda, G.; Fernández-Cardenete, J.R. Age estimation by a dental method: A comparison of Lamendin’s and Prince & Ubelaker’s technique. J. Forensic Sci. 2007, 52, 1156–1160. [Google Scholar] [CrossRef] [PubMed]
- Puneeth, K.H.; Nandini, D.B.; Praveen, S.B.; Selvamani, M.; Mandana, D. A comparative study of efficacy of single rooted and double rooted teeth in age estimation using dentin translucency. J. Forensic Odontostomatol. 2016, 34, 1–10. [Google Scholar]
- Bang, G.; Ramm, E. Determination of age in humans from root dentin transparency. Acta Odontol. Scand. 1970, 28, 3–35. [Google Scholar] [CrossRef]
- Ubelaker, D.H.; Parra, R.C. Application of three dental methods of adult age estimation from intact single rooted teeth to a Peruvian sample. J. Forensic Sci. 2008, 53, 608–611. [Google Scholar] [CrossRef] [PubMed]
- Bhardwaj, N.; Puri, A.; Nangia, R.; Bhat, N.; Bhatt, S.; Shakil, S. Assessment of root dentin translucency for age estimation: The first comparative study of conventional, stereomicroscopic & digital methods. Ann. Int. Med. Den. Res. 2019, 5, 7. [Google Scholar]
- Meinl, A.; Huber, C.D.; Tang, S.; Gruber, G.M.; Teschler-Nicola, M.; Watze, G. Comparison of the validity of three dental methods for the estimation of age at death. Forensic Sci. Int. 2008, 178, 96–105. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Solheim, T.; Sundnes, P.K. Dental age estimation of Norwegian adults—A comparison of different methods. Forensic Sci. Int. 1980, 16, 7–17. [Google Scholar] [CrossRef]
- Lucy, D.; Pollard, A.M.; Roberts, C.A. A comparison of three dental techniques for estimating age at death in humans. J. Archaeol. Sci. 1995, 22, 417–428. [Google Scholar] [CrossRef]
- Soomer, H.; Ranta, H.; Lincoln, M.J.; Penttilä, A.; Leibur, E. Reliability and validity of eight dental age estimation methods for adults. J. Forensic Sci. 2003, 48, 149–152. [Google Scholar] [CrossRef]
- Phulari, R.G.S.; Dave, E.J. Evolution of dental age estimation methods in adults over the years from occlusal wear to more sophisticated recent techniques. Egypt. J. Forensic Sci. 2021, 11, 36. [Google Scholar] [CrossRef]
- Johanson, G. Age determinations from human teeth. Odontol Rev. 1971, 22 (Suppl. 21), 1–126. [Google Scholar]
- Vasiliadis, L.; Darling, A.I.; Levers, B.G. The amount and distribution of sclerotic human root dentine. Arch. Oral Biol. 1983, 28, 645–649. [Google Scholar] [CrossRef]
- Azaz, B.; Michaeli, Y.; Nitzan, D. Aging tissues of the roots of nonfunctional human teeth (impacted canines). Oral Surg. Oral Med. Oral Pathol. 1977, 43, 572–578. [Google Scholar] [CrossRef] [PubMed]
- Garizoain, G.; Parra, R.C.; Escalante-Flórez, K.J.; Aranda, C.M.; Luna, L.H.; Condori, L.A.; Valderrama-Leal, C.I.; Retana-Milán, F. Age-at-death estimation in adults using three forensic methodologies: A Lamendin’s technique approach for Latin American context and the extension of a forensic international dental database. J. Forensic Sci. 2021, 66, 2456–2468. [Google Scholar] [CrossRef] [PubMed]
- Doria Martínez, A.M.; Vásquez Escobar, R.B.; Guzmán López, Z. Comparison of Two Methods, Lamendin and González-Colmenares, to Estimate Age in Adults. Univ. Odontológica 2022, 41. [Google Scholar] [CrossRef]
- Megyesi, M.S.; Ubelaker, D.H.; Sauer, N.J. Test of the Lamendin aging method on two historic skeletal samples. Am. J. Phys. Anthropol. 2006, 131, 363–367. [Google Scholar] [CrossRef] [PubMed]
- Solheim, T. Dental root translucency as an indicator of age. Scand. J. Dent. Res. 1989, 97, 189–197. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).