
Epidemiology of Injury Complaints in Elite Sprinting Athletes in Athletics (Track and Field)

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Overall Procedure
2.2. Population
2.3. Primary Outcome
2.4. Data Collection
2.5. Statistical Analyses
3. Results
3.1. Population
3.2. Injury Number and Prevalence
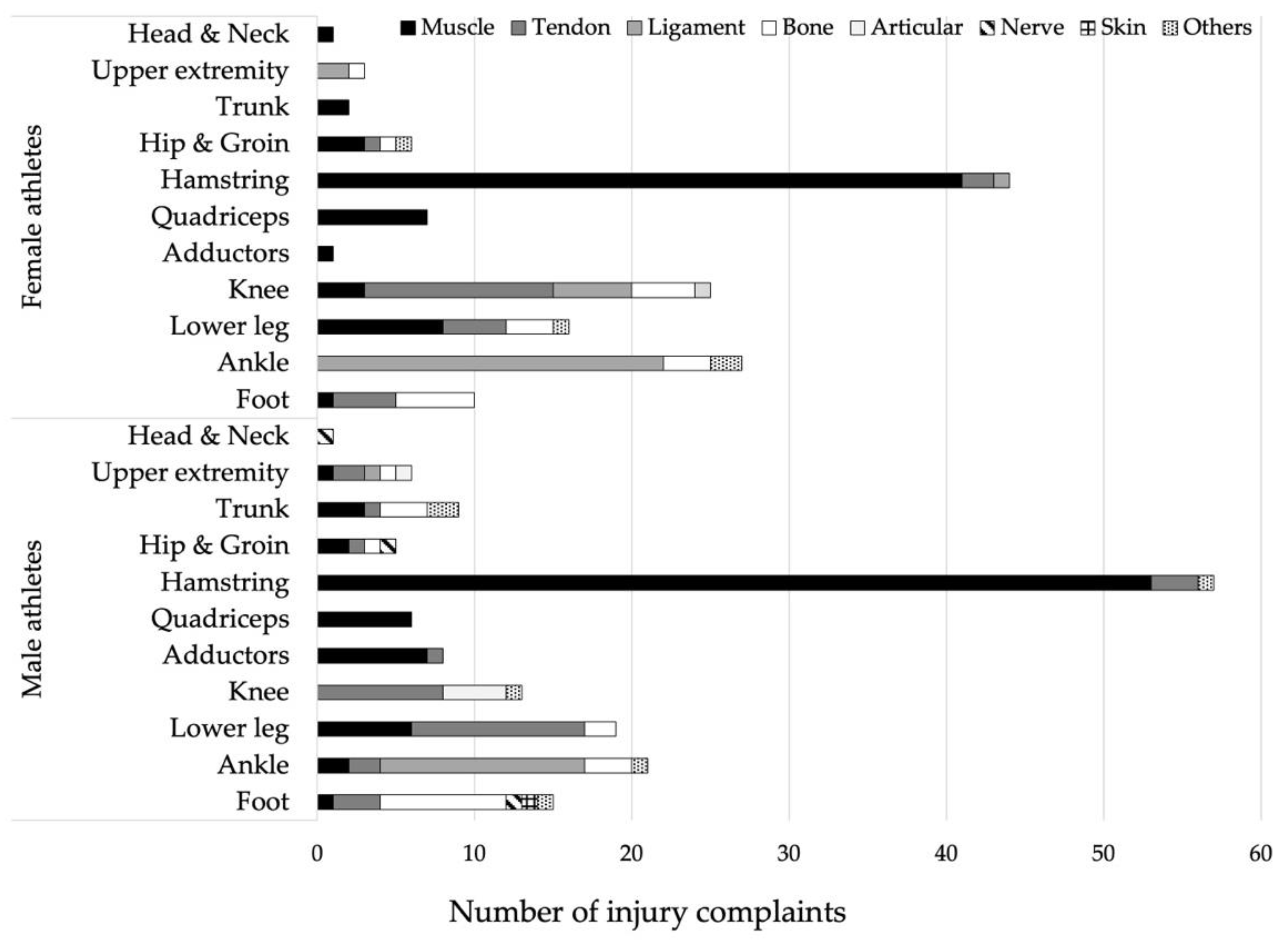
3.3. Injury Characteristics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Edouard, P.; Morel, N.; Serra, J.M.; Pruvost, J.; Oullion, R.; Depiesse, F. Prévention des lésions de l’appareil locomoteur liées à la pratique de l’athlétisme sur piste. Revue des données épidémiologiques. Sci. Sport. 2011, 26, 307–315. [Google Scholar] [CrossRef]
- van Mechelen, W.; Hlobil, H.; Kemper, H.C.G. Incidence, severity, aetiology and prevention of sports injuries. Sport. Med. 1992, 14, 82–99. [Google Scholar] [CrossRef] [PubMed]
- Yeung, S.S.; Suen, A.M.Y.; Yeung, E.W. A prospective cohort study of hamstring injuries in competitive sprinters: Preseason muscle imbalance as a possible risk factor. Br. J. Sports Med. 2009, 43, 589–594. [Google Scholar] [CrossRef] [PubMed]
- Edouard, P.; Pollock, N.; Guex, K.; Kelly, S.; Prince, C.; Navarro, L.; Branco, P.; Depiesse, F.; Gremeaux, V.; Hollander, K. Hamstring Muscle Injuries and Hamstring Specific Training in Elite Athletics (Track and Field) Athletes. Int. J. Environ. Res. Public Health 2022, 19, 10992. [Google Scholar] [CrossRef] [PubMed]
- Eckard, T.G.; Padua, D.A.; Hearn, D.W.; Pexa, B.S.; Frank, B.S. The Relationship Between Training Load and Injury in Athletes: A Systematic Review; Springer International Publishing: Berlin/Heidelberg, Germany, 2018; Volume 48, ISBN 0123456789. [Google Scholar]
- Edouard, P.; Navarro, L.; Branco, P.; Gremeaux, V.; Timpka, T.; Junge, A. Injury frequency and characteristics (location, type, cause and severity) differed significantly among athletics (‘track and field’) disciplines during 14 international championships (2007–2018): Implications for medical service planning. Br. J. Sports Med. 2020, 54, 159–167. [Google Scholar] [CrossRef]
- Edouard, P.; Hollander, K.; Navarro, L.; Lacourpaille, L.; Morales-Artacho, A.J.; Hanon, C.; Morin, J.B.; Le Garrec, S.; Branco, P.; Junge, A.; et al. Lower limb muscle injury location shift from posterior lower leg to hamstring muscles with increasing discipline-related running velocity in international athletics championships. J. Sci. Med. Sport 2021, 24, 653–659. [Google Scholar] [CrossRef]
- Ahuja, A.; Ghosh, A.K. Pre-Asiad ’82 injuries in elite Indian athletes. Br. J. Sports Med. 1985, 19, 24–26. [Google Scholar] [CrossRef] [Green Version]
- D’Souza, D. Track and Field athletics injuries—A one-year survey*. Br. J. Sports Med. 1994, 28, 197–202. [Google Scholar] [CrossRef] [Green Version]
- Bennell, K.L.; Crossley, K. Musculoskeletal injuries in track and field: Incidence, distribution and risk factors. Aust. J. Sci. Med. Sport 1996, 28, 69–75. [Google Scholar]
- Jacobsson, J.; Timpka, T.; Kowalski, J.; Nilsson, S.; Ekberg, J.; Renström, P. Prevalence of musculoskeletal injuries in Swedish elite track and field athletes. Am. J. Sports Med. 2012, 40, 163–169. [Google Scholar] [CrossRef]
- Jacobsson, J.; Timpka, T.; Kowalski, J.; Nilsson, S.; Ekberg, J.; Dahlström, Ö.; Renström, P.A. Injury patterns in Swedish elite athletics: Annual incidence, injury types and risk factors. Br. J. Sports Med. 2013, 47, 986–991. [Google Scholar] [CrossRef]
- Carragher, P.; Rankin, A.; Edouard, P. A One-Season Prospective Study of Illnesses, Acute, and Overuse Injuries in Elite Youth and Junior Track and Field Athletes. Front. Sport. Act. Living 2019, 1, 13. [Google Scholar] [CrossRef]
- Martínez-Silván, D.; Wik, E.H.; Alonso, J.M.; Jeanguyot, E.; Salcinovic, B.; Johnson, A.; Cardinale, M. Injury characteristics in male youth athletics: A five-season prospective study in a full-time sports academy. Br. J. Sports Med. 2021, 55, 954–960. [Google Scholar] [CrossRef] [PubMed]
- Edouard, P.; Steffen, K.; Peuriere, M.; Gardet, P.; Navarro, L.; Blanco, D. Effect of an unsupervised exercises-based athletics injury prevention programme on injury complaints leading to participation restriction in athletics: A cluster-randomised controlled trial. Int. J. Environ. Res. Public Health 2021, 18, 11334. [Google Scholar] [CrossRef] [PubMed]
- Bahr, R.; Clarsen, B.; Derman, W.; Dvorak, J.; Emery, C.A.; Finch, C.F.; Hägglund, M.; Junge, A.; Kemp, S.; Khan, K.M.; et al. International Olympic Committee consensus statement: Methods for recording and reporting of epidemiological data on injury and illness in sport 2020 (including STROBE Extension for Sport Injury and Illness Surveillance (STROBE-SIIS)). Br. J. Sports Med. 2020, 54, 372–389. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, R.O.; Debes-Kristensen, K.; Hulme, A.; Bertelsen, M.L.; Møller, M.; Parner, E.T.; Mansournia, M.A. Are prevalence measures better than incidence measures in sports injury research? Br. J. Sports Med. 2019, 53, 396–397. [Google Scholar] [CrossRef] [PubMed]
- Edouard, P.; Ruffault, A.; Bolling, C.; Navarro, L.; Martin, S.; Depiesse, F.; Oestergaard Nielsen, R.; Verhagen, E. French Athletics Stakeholders’ Perceptions of Relevance and Expectations on Injury Prevention. Int. J. Sports Med. 2021, 43, 1052–1060. [Google Scholar] [CrossRef]
- Ruffault, A.; Sorg, M.; Martin, S.; Hanon, C.; Jacquet, L.; Verhagen, E.; Edouard, P. Determinants of the adoption of injury risk reduction programmes in athletics (track and field): An online survey of 7715 French athletes. Br. J. Sports Med. 2022, 56, 499–505. [Google Scholar] [CrossRef]
- Edouard, P.; Richardson, A.; Murray, A.; Duncan, J.; Glover, D.; Kiss, M.; Depiesse, F.; Branco, P. Ten Tips to Hurdle the Injuries and Illnesses During Major Athletics Championships: Practical Recommendations and Resources. Front. Sport. Act. Living 2019, 1, 12. [Google Scholar] [CrossRef] [Green Version]
- Sugiura, Y.; Saito, T.; Sakuraba, K.; Sakuma, K.; Suzuki, E. Strength deficits identified with concentric action of the hip extensors and eccentric action of the hamstrings predispose to hamstring injury in elite sprinters. J. Orthop. Sports Phys. Ther. 2008, 38, 457–464. [Google Scholar] [CrossRef] [Green Version]
- Pollock, N.; Patel, A.; Chakraverty, J.; Suokas, A.; James, S.L.J.; Chakraverty, R. Time to return to full training is delayed and recurrence rate is higher in intratendinous (‘c’) acute hamstring injury in elite track and field athletes: Clinical application of the British Athletics Muscle Injury Classification. Br. J. Sports Med. 2016, 50, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Pollock, N.; Kelly, S.; Lee, J.; Stone, B.; Giakoumis, M.; Polglass, G.; Brown, J.; Macdonald, B. A 4-year study of hamstring injury outcomes in elite track and field using the British Athletics rehabilitation approach. Br. J. Sports Med. 2022, 56, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Dorn, T.W.; Schache, A.G.; Pandy, M.G. Muscular strategy shift in human running: Dependence of running speed on hip and ankle muscle performance. J. Exp. Biol. 2012, 215, 1944–1956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pandy, M.G.; Lai, A.K.M.; Schache, A.G.; Lin, Y.C. How muscles maximize performance in accelerated sprinting. Scand. J. Med. Sci. Sport. 2021, 31, 1882–1896. [Google Scholar] [CrossRef] [PubMed]
- Edouard, P.; Mendiguchia, J.; Guex, K.; Lahti, J.; Prince, C.; Samozino, P.; Morin, J.B. Sprinting: A key piece of the hamstring injury risk management puzzle. Br. J. Sports Med. 2022, 57, 4–6. [Google Scholar] [CrossRef] [PubMed]
- Green, B.; Bourne, M.N.; Van Dyk, N.; Pizzari, T. Recalibrating the risk of hamstring strain injury (HSI): A 2020 systematic review and meta-Analysis of risk factors for index and recurrent hamstring strain injury in sport. Br. J. Sports Med. 2020, 54, 1081–1088. [Google Scholar] [CrossRef]
- Guex, K.; Millet, G.P. Conceptual framework for strengthening exercises to prevent hamstring strains. Sport. Med. 2013, 43, 1207–1215. [Google Scholar] [CrossRef]
- MacDonald, B.; McAleer, S.; Kelly, S.; Chakraverty, R.; Johnston, M.; Pollock, N. Hamstring rehabilitation in elite track and field athletes: Applying the British Athletics Muscle Injury Classification in clinical practice. Br. J. Sports Med. 2019, 53, 1464–1473. [Google Scholar] [CrossRef]
- Sugiura, Y.; Sakuma, K.; Fujita, S.; Aoki, K.; Takazawa, Y. Effects of Various Numbers of Runs on the Success of Hamstring Injury Prevention Program in Sprinters. Int. J. Environ. Res. Public Health 2022, 19, 9375. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Total | Female Athletes | Male Athletes | ||||
|---|---|---|---|---|---|---|
| Number of athletes (n (%)) | 68 | (100.0%) | 34 | (50.0%) | 34 | (50.0%) |
| Anthropometrics | ||||||
| Age (years) (mean ± SD) | 23.3 | ±3.8 | 23.1 | ±4.3 | 23.6 | ±3.3 |
| Body mass (kg) (mean ± SD) | 68.5 | ±10.7 | 60.7 | ±5.9 | 76.3 | ±8.7 |
| Height (cm) (mean ± SD) | 175.4 | ±8.5 | 169.3 | ±5.2 | 181.5 | ±6.5 |
| Athletics activity | ||||||
| Disciplines of athletics (n (%)): | ||||||
| Sprints | 37 | (54.4%) | 18 | (52.9%) | 19 | (52.8%) |
| Hurdles | 23 | (33.8%) | 10 | (29.4%) | 13 | (36.1%) |
| Jumps | 2 | (2.9%) | 2 | (5.9%) | 0 | (0.0%) |
| Combined events | 6 | (8.8%) | 4 | (11.8%) | 2 | (5.9%) |
| Level of athletics activity (n (%)): | ||||||
| International | 28 | (41.2%) | 18 | (52.9%) | 10 | (29.4%) |
| National | 40 | (58.8%) | 16 | (47.1%) | 24 | (70.6%) |
| Number of years of athletics activity (mean ± SD) | 7.8 | ±4.1 | 7.1 | ±4.5 | 8.4 | ±3.7 |
| Mean number of athletics sessions per week (mean ± SD) | 6.8 | ±1.7 | 6.9 | ±1.8 | 6.6 | ±1.5 |
| Mean hours of athletics per week (mean ± SD) | 13.9 | ±4.7 | 14.3 | ±4.2 | 13.5 | ±5.3 |
| Mean hours of sports outside athletics per week (mean ± SD) | 2.2 | ±5.1 | 1.9 | ±5.6 | 2.5 | ±4.7 |
| History of injury complaints related to athletics activity | ||||||
| Lifetime injury complaints (n (%)) | 65 | (95.6%) | 33 | (97.1%) | 32 | (94.1%) |
| Lifetime prevalence proportion (% (95% CI)) | 95.6 | (90.7 to 100.5) | 97.1 | (91.4 to 102.7) | 94.1 | (86.2 to 102.0) |
| Injury complaints during the one-year period (n (%)) | 42 | (61.8%) | 19 | (55.9%) | 23 | (67.6%) |
| 1-year prevalence proportion (% (95% CI)) | 61.8 | (50.2 to 73.3) | 55.9 | (39.2 to 72.6) | 67.6 | (51.9 to 83.4) |
| Injury complaints at the time of the survey (n (%)) | 11 | (16.2%) | 6 | (17.6%) | 5 | (14.7%) |
| Point prevalence proportion (% (95% CI)) | 16.2 | (7.4 to 24.9) | 17.6 | (4.8 to 30.5) | 14.7 | (2.8 to 26.6) |
| Lifetime Injury Complaints | Injury Complaints during the One-Year Period before the Survey | Injury Complaints at the Time of the Survey | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | Female Athletes | Male Athletes | Total | Female Athletes | Male Athletes | Total | Female Athletes | Male Athletes | ||||||||||
| Total (n (%)) | 302 | (100.0) | 142 | (100.0) | 160 | (100.0) | 84 | (100.0) | 37 | (100.0) | 47 | (100.0) | 17 | (100.0) | 11 | (100.0) | 6 | (100.0) |
| Location | ||||||||||||||||||
| Head and neck | 2 | (0.6) | 1 | (0.7) | 1 | (0.6) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Upper extremity | 9 | (3.0) | 3 | (2.1) | 6 | (3.8) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Trunk | 11 | (3.6) | 2 | (1.4) | 9 | (5.6) | 5 | (6.0) | 2 | (5.4) | 3 | (6.4) | 1 | (5.9) | 1 | (9.1) | 0 | (0.0) |
| Hip and groin | 11 | (3.6) | 6 | (4.2) | 5 | (3.1) | 4 | (4.8) | 3 | (8.1) | 1 | (2.1) | 1 | (5.9) | 1 | (9.1) | 0 | (0.0) |
| Hamstrings | 101 | (33.4) | 44 | (31.0) | 57 | (35.6) | 31 | (36.9) | 17 | (45.9) | 14 | (29.8) | 7 | (41.2) | 5 | (45.5) | 2 | (33.3) |
| Quadriceps | 13 | (4.3) | 7 | (4.9) | 6 | (3.8) | 1 | (1.2) | 0 | (0.0) | 1 | (2.1) | 1 | (5.9) | 0 | (0.0) | 1 | (16.7) |
| Adductors | 9 | (3.0) | 1 | (0.7) | 8 | (5.0) | 2 | (2.4) | 0 | (0.0) | 2 | (4.3) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Knee | 38 | (12.6) | 25 | (17.6) | 13 | (8.1) | 8 | (9.5) | 5 | (13.5) | 3 | (6.4) | 1 | (5.9) | 1 | (9.1) | 0 | (0.0) |
| Lower leg | 35 | (11.6) | 16 | (11.3) | 19 | (11.9) | 14 | (16.7) | 3 | (8.1) | 11 | (23.4) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Ankle | 48 | (15.9) | 27 | (19.0) | 21 | (13.1) | 14 | (16.7) | 6 | (16.2) | 8 | (17.0) | 4 | (23.5) | 2 | (18.2) | 2 | (33.3) |
| Foot | 25 | (8.3) | 10 | (7.0) | 15 | (9.4) | 5 | (6.0) | 1 | (2.7) | 4 | (8.5) | 2 | (11.8) | 1 | (9.1) | 1 | (16.7) |
| Type | ||||||||||||||||||
| Muscle | 148 | (49.0) | 67 | (47.2) | 81 | (50.6) | 42 | (50.0) | 21 | (56.8) | 21 | (44.7) | 7 | (41.2) | 5 | (45.5) | 2 | (33.3) |
| Tendon | 55 | (18.2) | 23 | (16.2) | 32 | (20.0) | 16 | (19.0) | 5 | (13.5) | 11 | (23.4) | 3 | (17.6) | 2 | (18.2) | 1 | (16.7) |
| Ligament | 44 | (14.6) | 30 | (21.1) | 14 | (8.8) | 14 | (16.7) | 6 | (16.2) | 8 | (17.0) | 4 | (23.5) | 2 | (18.2) | 2 | (33.3) |
| Bone | 35 | (11.6) | 17 | (12.0) | 18 | (11.3) | 6 | (7.1) | 4 | (10.8) | 2 | (4.3) | 2 | (11.8) | 2 | (18.2) | 0 | (0.0) |
| Articular | 6 | (2.0) | 1 | (0.7) | 5 | (3.1) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Nerve | 3 | (1.0) | 0 | (0.0) | 3 | (1.9) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Skin | 1 | (0.3) | 0 | (0.0) | 1 | (0.6) | 1 | (1.2) | 0 | (0.0) | 1 | (2.1) | 1 | (5.9) | 0 | (0.0) | 1 | (16.7) |
| Others | 10 | (3.3) | 4 | (2.8) | 6 | (3.8) | 5 | (6.0) | 1 | (2.7) | 4 | (8.5) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Circumstances | ||||||||||||||||||
| Training | 210 | (69.5) | 106 | (74.6) | 104 | (65.0) | 65 | (77.4) | 26 | (70.3) | 39 | (83.0) | 11 | (64.7) | 6 | (54.5) | 5 | (83.3) |
| Competition | 92 | (30.5) | 36 | (25.4) | 56 | (35.0) | 19 | (22.6) | 11 | (29.7) | 8 | (17.0) | 6 | (35.3) | 5 | (45.5) | 1 | (16.7) |
| Mode of onset | ||||||||||||||||||
| Sudden | 203 | (67.2) | 93 | (65.5) | 110 | (68.8) | 51 | (60.7) | 27 | (73.0) | 24 | (51.1) | 13 | (76.5) | 9 | (81.8) | 4 | (66.7) |
| Gradual | 98 | (32.5) | 49 | (34.5) | 49 | (30.6) | 33 | (39.3) | 10 | (27.0) | 23 | (48.9) | 4 | (23.5) | 2 | (18.2) | 2 | (33.3) |
| Missing | 1 | (0.3) | 0 | (0.0) | 1 | (0.6) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Mechanism | ||||||||||||||||||
| Mode of onset clearly identifiable with contact | 32 | (10.6) | 17 | (12.0) | 15 | (9.4) | 10 | (11.9) | 5 | (13.5) | 5 | (10.6) | 3 | (17.6) | 1 | (9.1) | 2 | (33.3) |
| Mode of onset clearly identifiable without contact | 89 | (29.5) | 44 | (31.0) | 45 | (28.1) | 21 | (25.0) | 12 | (32.4) | 9 | (19.1) | 7 | (41.2) | 7 | (63.6) | (0.0) | |
| Mode of onset not clearly identifiable | 152 | (50.3) | 67 | (47.2) | 85 | (53.1) | 45 | (53.6) | 17 | (45.9) | 28 | (59.6) | 7 | (41.2) | 3 | (27.3) | 4 | (66.7) |
| Missing | 29 | (9.6) | 14 | (9.9) | 15 | (9.4) | 8 | (9.5) | 3 | (8.1) | 5 | (10.6) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Severity | ||||||||||||||||||
| No time loss in sport | 48 | (15.9) | 26 | (18.3) | 22 | (13.8) | 21 | (25.0) | 8 | (21.6) | 13 | (27.7) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Time loss < 7 days | 42 | (13.9) | 19 | (13.4) | 23 | (14.4) | 18 | (21.4) | 6 | (16.2) | 12 | (25.5) | 3 | (17.6) | 2 | (18.2) | 1 | (16.7) |
| Time loss between 7 and 28 days | 112 | (37.1) | 53 | (37.3) | 59 | (36.9) | 22 | (26.2) | 10 | (27.0) | 12 | (25.5) | 7 | (41.2) | 3 | (27.3) | 4 | (66.7) |
| Time loss > 28 days | 100 | (33.1) | 44 | (31.0) | 56 | (35.0) | 23 | (27.4) | 13 | (35.1) | 10 | (21.3) | 7 | (41.2) | 6 | (54.5) | 1 | (16.7) |
| Total Lifetime Injuries | Muscle | Tendon | Ligament | Bone | Articular | Nerve | Skin | Others | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | ||||||||||||||||||
| Total lifetime injuries | 302 | (100.0) | 148 | (49.0) | 55 | (18.2) | 44 | (14.6) | 35 | (11.6) | 6 | (2.0) | 3 | (1.0) | 1 | (0.3) | 10 | (3.3) |
| Head and neck | 2 | (0.7) | 1 | (0.3) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 1 | (0.3) | 0 | (0.0) | 0 | (0.0) |
| Upper extremity | 9 | (3.0) | 1 | (0.3) | 2 | (0.7) | 3 | (1.0) | 2 | (0.7) | 1 | (0.3) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Trunk | 11 | (3.6) | 5 | (1.7) | 1 | (0.3) | 0 | (0.0) | 3 | (1.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 2 | (0.7) |
| Hip and groin | 11 | (3.6) | 5 | (1.7) | 2 | (0.7) | 0 | (0.0) | 2 | (0.7) | 0 | (0.0) | 1 | (0.3) | 0 | (0.0) | 1 | (0.3) |
| Hamstrings | 101 | (33.4) | 94 | (31.1) | 5 | (1.7) | 1 | (0.3) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 1 | (0.3) |
| Quadriceps | 13 | (4.3) | 13 | (4.3) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Adductors | 9 | (3.0) | 8 | (2.6) | 1 | (0.3) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Knee | 38 | (12.6) | 3 | (1.0) | 20 | (6.6) | 5 | (1.7) | 4 | (1.3) | 5 | (1.7) | 0 | (0.0) | 0 | (0.0) | 1 | (0.3) |
| Lower leg | 35 | (11.6) | 14 | (4.6) | 15 | (5.0) | 0 | (0.0) | 5 | (1.7) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 1 | (0.3) |
| Ankle | 48 | (15.9) | 2 | (0.7) | 2 | (0.7) | 35 | (11.6) | 6 | (2.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 3 | (1.0) |
| Foot | 25 | (8.3) | 2 | (0.7) | 7 | (2.3) | 0 | (0.0) | 13 | (4.3) | 0 | (0.0) | 1 | (0.3) | 1 | (0.3) | 1 | (0.3) |
| Female athletes | ||||||||||||||||||
| Total lifetime injuries | 142 | (100.0) | 67 | (47.2) | 23 | (16.2) | 30 | (21.1) | 17 | (12.0) | 1 | (0.7) | 0 | (0.0) | 0 | (0.0) | 4 | (2.8) |
| Head and neck | 1 | (0.7) | 1 | (0.7) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Upper extremity | 3 | (2.1) | 0 | (0.0) | 0 | (0.0) | 2 | (1.4) | 1 | (0.7) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Trunk | 2 | (1.4) | 2 | (1.4) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Hip and groin | 6 | (4.2) | 3 | (2.1) | 1 | (0.7) | 0 | (0.0) | 1 | (0.7) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 1 | (0.7) |
| Hamstrings | 44 | (31.0) | 41 | (28.9) | 2 | (1.4) | 1 | (0.7) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Quadriceps | 7 | (4.9) | 7 | (4.9) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Adductors | 1 | (0.7) | 1 | (0.7) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Knee | 25 | (17.6) | 3 | (2.1) | 12 | (8.5) | 5 | (3.5) | 4 | (2.8) | 1 | (0.7) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Lower leg | 16 | (11.3) | 8 | (5.6) | 4 | (2.8) | 0 | (0.0) | 3 | (2.1) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 1 | (0.7) |
| Ankle | 27 | (19.0) | 0 | (0.0) | 0 | (0.0) | 22 | (15.5) | 3 | (2.1) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 2 | (1.4) |
| Foot | 10 | (7.0) | 1 | (0.7) | 4 | (2.8) | 0 | (0.0) | 5 | (3.5) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Male athletes | ||||||||||||||||||
| Total lifetime injuries | 160 | (100.0) | 81 | (50.6) | 32 | (20.0) | 14 | (8.8) | 18 | (11.3) | 5 | (3.1) | 3 | (1.9) | 1 | (0.6) | 6 | (3.8) |
| Head and neck | 1 | (0.6) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 1 | (0.6) | 0 | (0.0) | 0 | (0.0) |
| Upper extremity | 6 | (3.8) | 1 | (0.6) | 2 | (1.3) | 1 | (0.6) | 1 | (0.6) | 1 | (0.6) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Trunk | 9 | (5.6) | 3 | (1.9) | 1 | (0.6) | 0 | (0.0) | 3 | (1.9) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 2 | (1.3) |
| Hip and groin | 5 | (3.1) | 2 | (1.3) | 1 | (0.6) | 0 | (0.0) | 1 | (0.6) | 0 | (0.0) | 1 | (0.6) | 0 | (0.0) | 0 | (0.0) |
| Hamstrings | 57 | (35.6) | 53 | (33.1) | 3 | (1.9) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 1 | (0.6) |
| Quadriceps | 6 | (3.8) | 6 | (3.8) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Adductors | 8 | (5.0) | 7 | (4.4) | 1 | (0.6) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Knee | 13 | (8.1) | 0 | (0.0) | 8 | (5.0) | 0 | (0.0) | 0 | (0.0) | 4 | (2.5) | 0 | (0.0) | 0 | (0.0) | 1 | (0.6) |
| Lower leg | 19 | (11.9) | 6 | (3.8) | 11 | (6.9) | 0 | (0.0) | 2 | (1.3) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Ankle | 21 | (13.1) | 2 | (1.3) | 2 | (1.3) | 13 | (8.1) | 3 | (1.9) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 1 | (0.6) |
| Foot | 15 | (9.4) | 1 | (0.6) | 3 | (1.9) | 0 | (0.0) | 8 | (5.0) | 0 | (0.0) | 1 | (0.6) | 1 | (0.6) | 1 | (0.6) |
| Total One-Year Period Injuries | Muscle | Tendon | Ligament | Bone | Articular | Nerve | Skin | Others | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | ||||||||||||||||||
| Total one-year period injuries | 84 | (100.0) | 42 | (50.0) | 16 | (19.0) | 14 | (16.7) | 6 | (7.1) | 0 | (0.0) | 0 | (0.0) | 1 | (1.2) | 5 | (6.0) |
| Head and neck | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Upper extremity | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Trunk | 5 | (6.0) | 3 | (3.6) | 1 | (1.2) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 1 | (1.2) |
| Hip and groin | 4 | (4.8) | 3 | (3.6) | 0 | (0.0) | 0 | (0.0) | 1 | (1.2) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Hamstring | 31 | (36.9) | 25 | (29.8) | 4 | (4.8) | 1 | (1.2) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 1 | (1.2) |
| Quadriceps | 1 | (1.2) | 1 | (1.2) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Adductors | 2 | (2.4) | 2 | (2.4) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Knee | 8 | (9.5) | 1 | (1.2) | 5 | (6.0) | 1 | (1.2) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 1 | (1.2) |
| Lower leg | 14 | (16.7) | 7 | (8.3) | 5 | (6.0) | 0 | (0.0) | 1 | (1.2) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 1 | (1.2) |
| Ankle | 14 | (16.7) | 0 | (0.0) | 0 | (0.0) | 12 | (14.3) | 2 | (2.4) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Foot | 5 | (6.0) | 0 | (0.0) | 1 | (1.2) | 0 | (0.0) | 2 | (2.4) | 0 | (0.0) | 0 | (0.0) | 1 | (1.2) | 1 | (1.2) |
| Female athletes | ||||||||||||||||||
| Total one-year period injuries | 37 | (100.0) | 21 | (56.8) | 5 | (13.5) | 6 | (16.2) | 4 | (10.8) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 1 | (2.7) |
| Head and neck | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Upper extremity | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Trunk | 2 | (5.4) | 2 | (5.4) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Hip and groin | 3 | (8.1) | 2 | (5.4) | 0 | (0.0) | 0 | (0.0) | 1 | (2.7) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Hamstring | 17 | (45.9) | 15 | (40.5) | 1 | (2.7) | 1 | (2.7) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Quadriceps | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Adductors | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Knee | 5 | (13.5) | 1 | (2.7) | 3 | (8.1) | 1 | (2.7) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Lower leg | 3 | (8.1) | 1 | (2.7) | 0 | (0.0) | 0 | (0.0) | 1 | (2.7) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 1 | (2.7) |
| Ankle | 6 | (16.2) | 0 | (0.0) | 0 | (0.0) | 4 | (10.8) | 2 | (5.4) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Foot | 1 | (2.7) | 0 | (0.0) | 1 | (2.7) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Male athletes | ||||||||||||||||||
| Total one-year period injuries | 47 | (100.0) | 21 | (44.7) | 11 | (23.4) | 8 | (17.0) | 2 | (4.3) | 0 | (0.0) | 0 | (0.0) | 1 | (2.1) | 4 | (8.5) |
| Head and neck | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Upper extremity | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Trunk | 3 | (6.4) | 1 | (2.1) | 1 | (2.1) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 1 | (2.1) |
| Hip and groin | 1 | (2.1) | 1 | (2.1) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Hamstring | 14 | (29.8) | 10 | (21.3) | 3 | (6.4) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 1 | (2.1) |
| Quadriceps | 1 | (2.1) | 1 | (2.1) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Adductors | 2 | (4.3) | 2 | (4.3) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Knee | 3 | (6.4) | 0 | (0.0) | 2 | (4.3) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 1 | (2.1) |
| Lower leg | 11 | (23.4) | 6 | (12.8) | 5 | (10.6) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Ankle | 8 | (17.0) | 0 | (0.0) | 0 | (0.0) | 8 | (17.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) |
| Foot | 4 | (8.5) | 0 | (0.0) | 0 | (0.0) | 0 | (0.0) | 2 | (4.3) | 0 | (0.0) | 0 | (0.0) | 1 | (2.1) | 1 | (2.1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Edouard, P.; Caumeil, B.; Giroux, C.; Bruneau, A.; Tondut, J.; Navarro, L.; Hanon, C.; Guilhem, G.; Ruffault, A. Epidemiology of Injury Complaints in Elite Sprinting Athletes in Athletics (Track and Field). Appl. Sci. 2023, 13, 8105. https://doi.org/10.3390/app13148105
Edouard P, Caumeil B, Giroux C, Bruneau A, Tondut J, Navarro L, Hanon C, Guilhem G, Ruffault A. Epidemiology of Injury Complaints in Elite Sprinting Athletes in Athletics (Track and Field). Applied Sciences. 2023; 13(14):8105. https://doi.org/10.3390/app13148105
Chicago/Turabian StyleEdouard, Pascal, Benjamin Caumeil, Caroline Giroux, Antoine Bruneau, Jeanne Tondut, Laurent Navarro, Christine Hanon, Gaël Guilhem, and Alexis Ruffault. 2023. "Epidemiology of Injury Complaints in Elite Sprinting Athletes in Athletics (Track and Field)" Applied Sciences 13, no. 14: 8105. https://doi.org/10.3390/app13148105
APA StyleEdouard, P., Caumeil, B., Giroux, C., Bruneau, A., Tondut, J., Navarro, L., Hanon, C., Guilhem, G., & Ruffault, A. (2023). Epidemiology of Injury Complaints in Elite Sprinting Athletes in Athletics (Track and Field). Applied Sciences, 13(14), 8105. https://doi.org/10.3390/app13148105