
Mandibular Molar Distalization in Class III Malocclusion: A Systematic Review

 ,
,  ,
,  ,
,  , , , ,
, , , ,  , ,
, ,  and
and 
Abstract
:1. Introduction
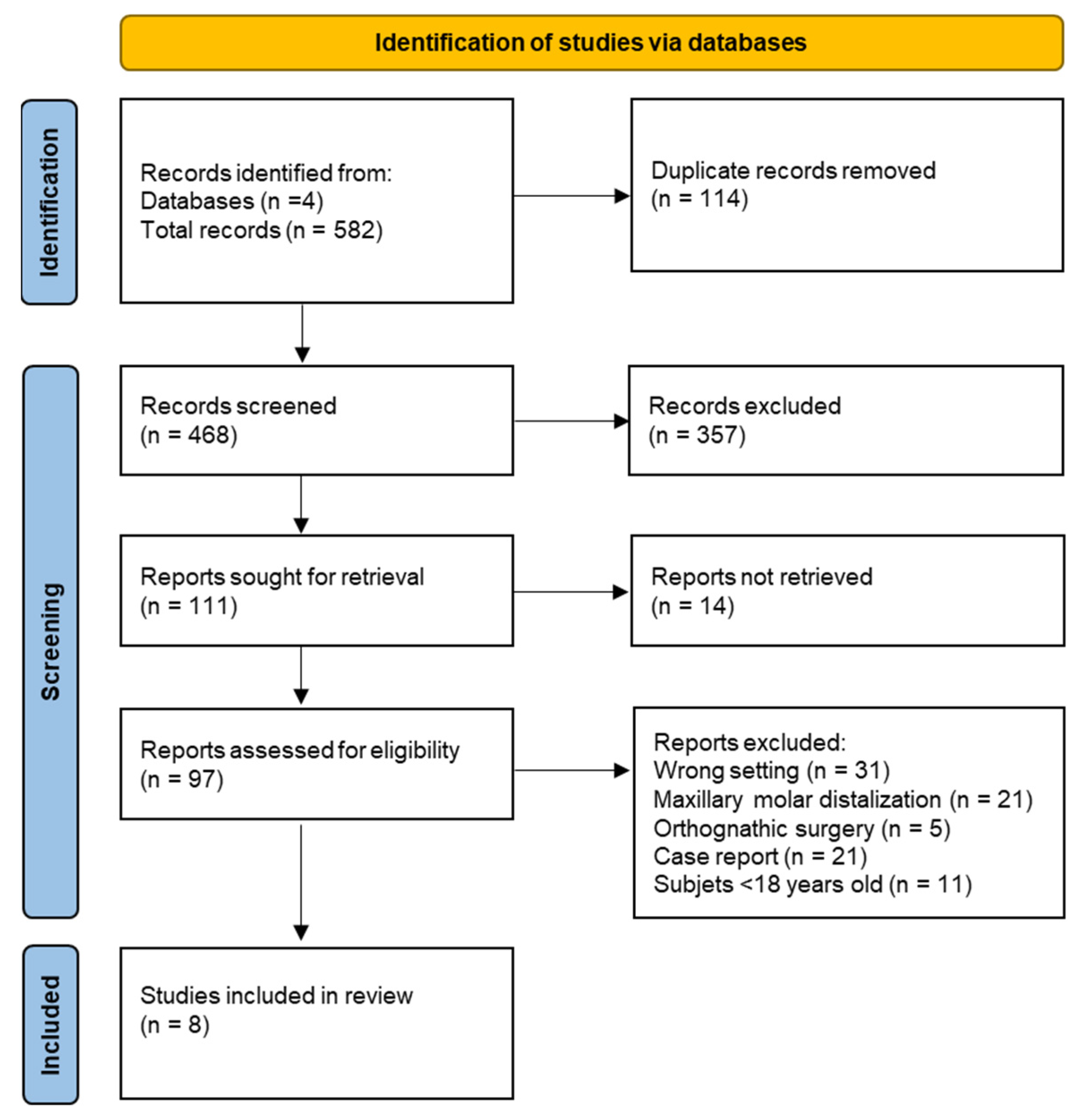
2. Materials and Methods
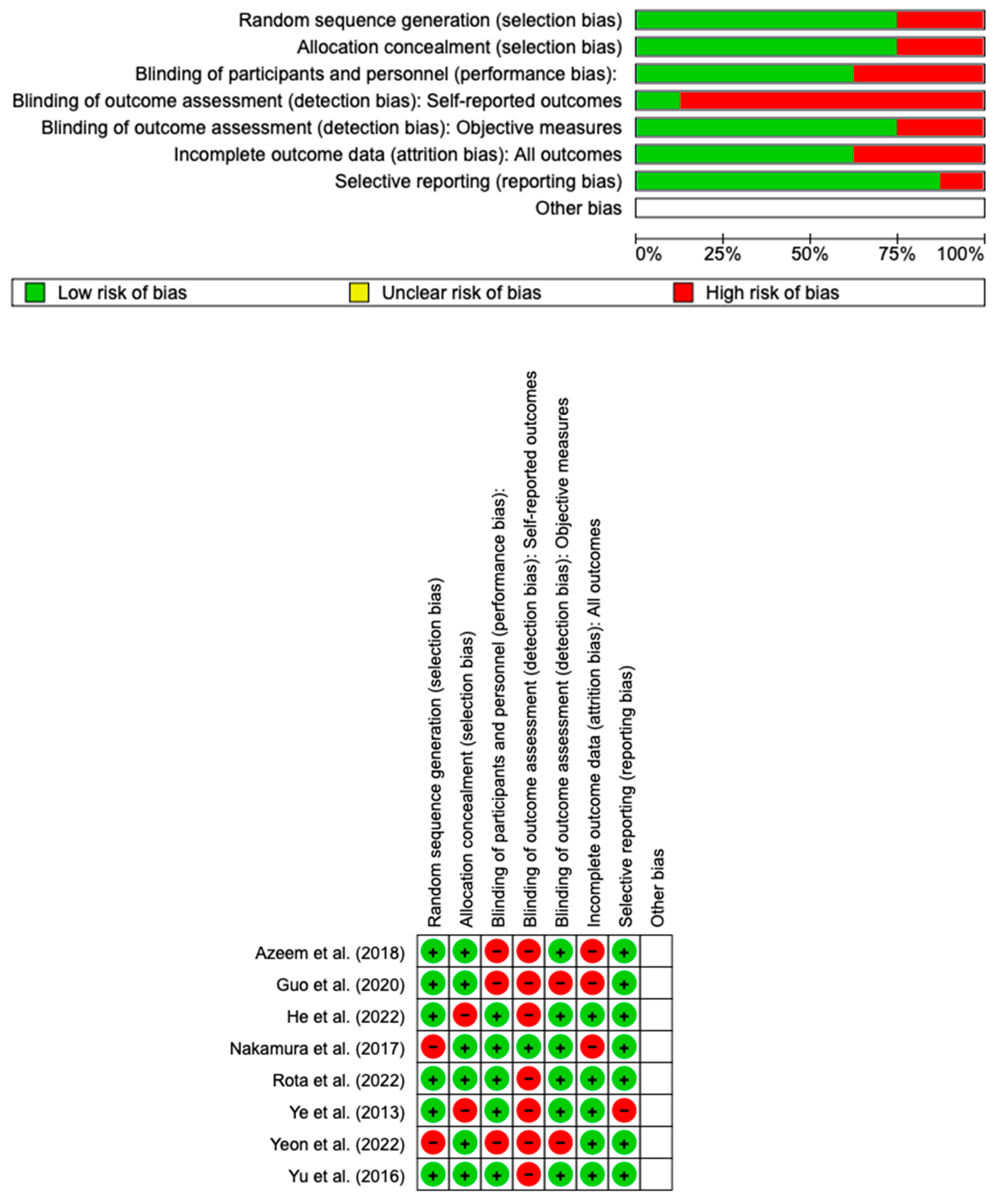
Quality Assessment
3. Results
Quality Assessment and Risk of Bias
4. Discussion
4.1. MMD via a Fixed Appliance
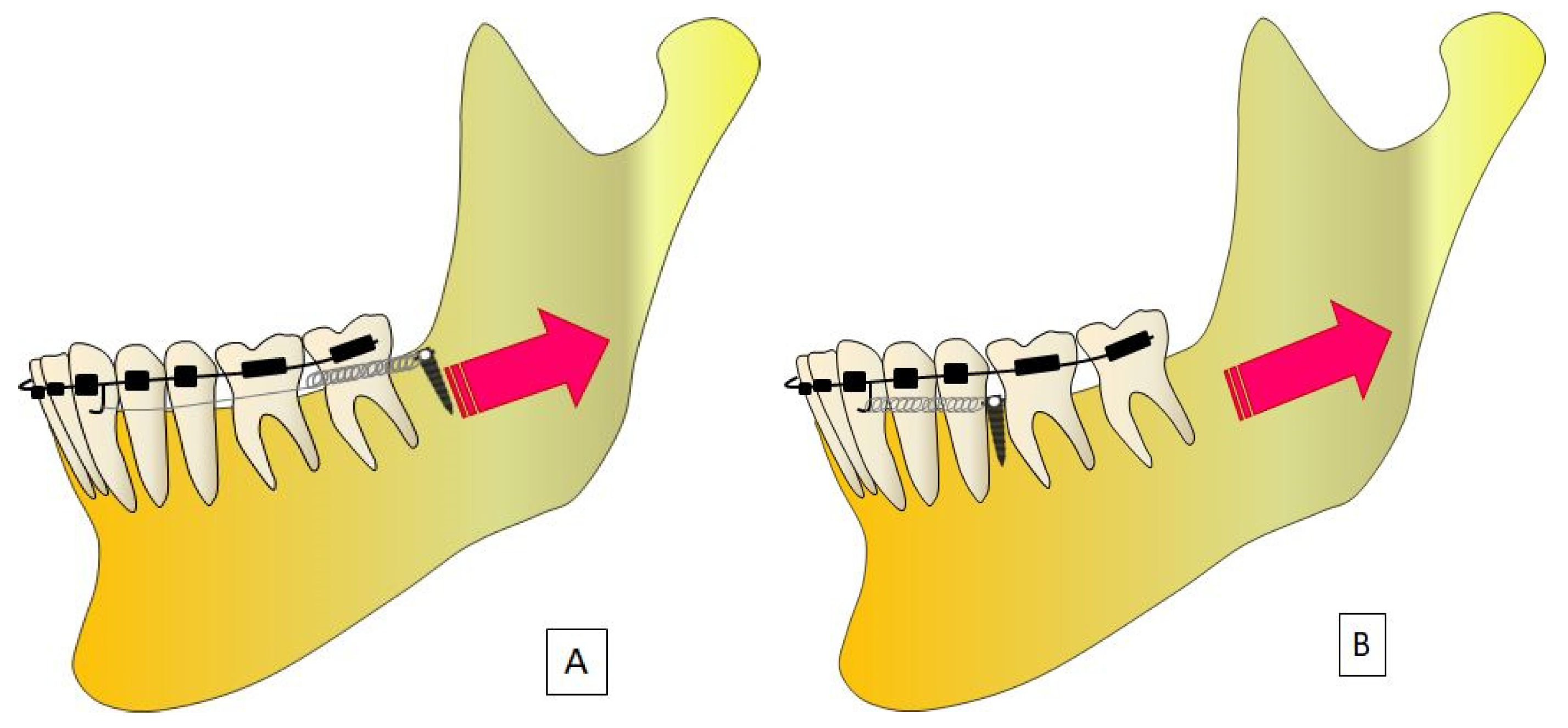
4.2. MMD with Skeletal Anchorage
4.2.1. TADs
4.2.2. Mini-Plates
4.2.3. Ramal Plates
4.3. MMD with Clear Aligners
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| MEAW | Multiloop Edgewise Arch Wire |
| MMD | Mandibular Molar Distalization |
| P RISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| SJ | Sliding Jigs |
| TADs | Temporary Anchorage Devices |
| TCM | Third Class Malocclusion |
| TMJ | Temporomandibular Joint |
References
- Ghodasra, R.; Brizuela, M. Orthodontics, Malocclusion. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Di Pede, C.; Garibaldi, M.; Ciocia, A.M.; et al. Treatment of Class III Malocclusion and Anterior Crossbite with Aligners: A Case Report. Medicina 2022, 58, 603. [Google Scholar] [CrossRef]
- Dehesa-Santos, A.; Iber-Diaz, P.; Iglesias-Linares, A. Genetic Factors Contributing to Skeletal Class III Malocclusion: A Systematic Review and Meta-Analysis. Clin. Oral. Investig. 2021, 25, 1587–1612. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, G.; Vena, F.; Negri, P.; Pagano, S.; Barilotti, C.; Paglia, L.; Colombo, S.; Orso, M.; Cianetti, S. Worldwide Prevalence of Malocclusion in the Different Stages of Dentition: A Systematic Review and Meta-Analysis. Eur. J. Paediatr. Dent. 2020, 21, 115–122. [Google Scholar] [CrossRef]
- Ngan, P.; Moon, W. Evolution of Class III Treatment in Orthodontics. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 22–36. [Google Scholar] [CrossRef] [PubMed]
- Quinzi, V.; Scibetta, E.T.; Marchetti, E.; Mummolo, S.; Giannì, A.B.; Romano, M.; Beltramini, G.; Marzo, G. Analyze My Face. J. Biol. Regul. Homeost. Agents 2018, 32, 149–158. [Google Scholar] [PubMed]
- Mummolo, S.; Nota, A.; Marchetti, E.; Padricelli, G.; Marzo, G. The 3D Tele Motion Tracking for the Orthodontic Facial Analysis. Biomed. Res. Int. 2016, 2016, 4932136. [Google Scholar] [CrossRef]
- Byloff, F.; Darendeliler, M.A.; Stoff, F. Mandibular Molar Distalization with the Franzulum Appliance. J. Clin. Orthod. 2000, 34, 518–523. [Google Scholar] [PubMed]
- Quinzi, V.; Saccomanno, S.; Manenti, R.J.; Giancaspro, S.; Coceani Paskay, L.; Marzo, G. Efficacy of Rapid Maxillary Expansion with or without Previous Adenotonsillectomy for Pediatric Obstructive Sleep Apnea Syndrome Based on Polysomnographic Data: A Systematic Review and Meta-Analysis. Appl. Sci. 2020, 10, 6485. [Google Scholar] [CrossRef]
- D’Apuzzo, F.; Grassia, V.; Quinzi, V.; Vitale, M.; Marzo, G.; Perillo, L. Paediatric Orthodontics. Part 4: SEC III Protocol in Class III Malocclusion. Eur. J. Paediatr. Dent. 2019, 20, 330–334. [Google Scholar] [CrossRef]
- Kanas, R.J.; Carapezza, L.; Kanas, S.J. Treatment Classification of Class III Malocclusion. J. Clin. Pediatr. Dent. 2008, 33, 175–185. [Google Scholar] [CrossRef]
- Eslami, S.; Faber, J.; Fateh, A.; Sheikholaemmeh, F.; Grassia, V.; Jamilian, A. Treatment Decision in Adult Patients with Class III Malocclusion: Surgery versus Orthodontics. Prog. Orthod. 2018, 19, 28. [Google Scholar] [CrossRef] [PubMed]
- Alhammadi, M.S.; Almashraqi, A.A.; Khadhi, A.H.; Arishi, K.A.; Alamir, A.A.; Beleges, E.M.; Halboub, E. Orthodontic Camouflage versus Orthodontic-Orthognathic Surgical Treatment in Borderline Class III Malocclusion: A Systematic Review. Clin. Oral. Investig. 2022, 26, 6443–6455. [Google Scholar] [CrossRef] [PubMed]
- Bezerra, G.D.C.; Gaschler, J.A.M.; Lourenço, V.S.; Patel, M.P.; Nahás-Scocate, A.C.R.; Maltagliati, L.Á. Compensatory Treatment of a Complex Class III Malocclusion Using Contemporary Mechanics. J. Clin. Orthod. 2022, 56, 201–209. [Google Scholar] [PubMed]
- Rongo, R.; D’Antò, V.; Bucci, R.; Polito, I.; Martina, R.; Michelotti, A. Skeletal and Dental Effects of Class III Orthopaedic Treatment: A Systematic Review and Meta-Analysis. J. Oral. Rehabil. 2017, 44, 545–562. [Google Scholar] [CrossRef] [PubMed]
- Sugawara, J.; Daimaruya, T.; Umemori, M.; Nagasaka, H.; Takahashi, I.; Kawamura, H.; Mitani, H. Distal Movement of Mandibular Molars in Adult Patients with the Skeletal Anchorage System. Am. J. Orthod. Dentofacial Orthop. 2004, 125, 130–138. [Google Scholar] [CrossRef]
- Alogaibi, Y.A.; Al-Fraidi, A.A.; Alhajrasi, M.K.; Alkhathami, S.S.; Hatrom, A.; Afify, A.R. Distalization in Orthodontics: A Review and Case Series. Case Rep. Dent. 2021, 2021, 8843959. [Google Scholar] [CrossRef]
- Özden, S.; Uslu, F.; Dedeoğlu, N. Evaluation of Bone Area in the Posterior Region for Mandibular Molar Distalization in Class I and Class III Patients. Clin. Oral. Investig. 2023, 27, 2041–2048. [Google Scholar] [CrossRef]
- Quinzi, V.; Marchetti, E.; Guerriero, L.; Bosco, F.; Marzo, G.; Mummolo, S. Dentoskeletal Class II Malocclusion: Maxillary Molar Distalization with No-Compliance Fixed Orthodontic Equipment. Dent. J. 2020, 8, 26. [Google Scholar] [CrossRef]
- Kim, H.-J.; Jang, W.-S.; Park, H.-S. Anatomical Limits for Distalization of Lower Posterior Molars with Micro-Implant Anchorage. J. Clin. Orthod. 2019, 53, 305–313. [Google Scholar]
- Wang, Y.; Sun, J.; Shi, Y.; Li, X.; Wang, Z. Buccal Bone Thickness of Posterior Mandible for Microscrews Implantation in Molar Distalization. Ann. Anat. 2022, 244, 151993. [Google Scholar] [CrossRef]
- Nucera, R.; Lo Giudice, A.; Bellocchio, A.M.; Spinuzza, P.; Caprioglio, A.; Perillo, L.; Matarese, G.; Cordasco, G. Bone and Cortical Bone Thickness of Mandibular Buccal Shelf for Mini-Screw Insertion in Adults. Angle Orthod. 2017, 87, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Wu, X.; Tan, J.; Li, X. Safe Regions of Miniscrew Implantation for Distalization of Mandibular Dentition with CBCT. Prog. Orthod. 2019, 20, 45. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.T.; Kim, Y.-J.; Yang, K.-S.; Lee, D.-Y. Bone Availability for Mandibular Molar Distalization in Adults with Mandibular Prognathism. Angle Orthod. 2018, 88, 52–57. [Google Scholar] [CrossRef]
- Leo, M.; Cerroni, L.; Pasquantonio, G.; Condò, S.G.; Condò, R. Temporary Anchorage Devices (TADs) in Orthodontics: Review of the Factors That Influence the Clinical Success Rate of the Mini-Implants. Clin. Ter. 2016, 167, e70–e77. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ 2009, 62, e1–e34. [Google Scholar] [CrossRef]
- He, Y.; Wang, Y.; Wang, X.; Wang, J.; Bai, D.; Guo, Y. Nonsurgical Treatment of a Hyperdivergent Skeletal Class III Patient with Mini-Screw–Assisted Mandibular Dentition Distalization and Flattening of the Occlusal Plane. Angle Orthod. 2022, 92, 287–293. [Google Scholar] [CrossRef]
- Guo, Y.; Qiao, X.; Yao, S.; Li, T.; Jiang, N.; Peng, C. CBCT Analysis of Changes in Dental Occlusion and Temporomandibular Joints before and after MEAW Orthotherapy in Patients with Nonlow Angle of Skeletal Class III. BioMed Res. Int. 2020, 2020, 7238263. [Google Scholar] [CrossRef]
- Nakamura, M.; Kawanabe, N.; Kataoka, T.; Murakami, T.; Yamashiro, T.; Kamioka, H. Comparative Evaluation of Treatment Outcomes between Temporary Anchorage Devices and Class III Elastics in Class III Malocclusions. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 1116–1124. [Google Scholar] [CrossRef]
- Yeon, B.M.; Lee, N.-K.; Park, J.H.; Kim, J.M.; Kim, S.-H.; Kook, Y.-A. Comparison of Treatment Effects after Total Mandibular Arch Distalization with Miniscrews vs Ramal Plates in Patients with Class III Malocclusion. Am. J. Orthod. Dentofac. Orthop. 2022, 161, 529–536. [Google Scholar] [CrossRef]
- Azeem, M.; Ul Haq, A.; Ul Hamid, W.; Hayat, M.B.; Khan, D.I.; Ahmed, A.; Khan, M.T. Efficiency of Class III Malocclusion Treatment with 2-Premolar Extraction and Molar Distalization Protocols. Int. Orthod. 2018, 16, 665–675. [Google Scholar] [CrossRef]
- Rota, E.; Parrini, S.; Malekian, K.; Cugliari, G.; Mampieri, G.; Deregibus, A.; Castroflorio, T. Lower Molar Distalization Using Clear Aligners: Bodily Movement or Uprighting? A Preliminary Study. Appl. Sci. 2022, 12, 7123. [Google Scholar] [CrossRef]
- Yu, J.; Park, J.H.; Bayome, M.; Kim, S.; Kook, Y.-A.; Kim, Y.; Kim, C.-H. Treatment Effects of Mandibular Total Arch Distalization Using a Ramal Plate. Korean J. Orthod. 2016, 46, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Ye, C.; Zhihe, Z.; Zhao, Q.; Ye, J. Treatment Effects of Distal Movement of Lower Arch With Miniscrews in the Retromolar Area Compared With Miniscrews in the Posterior Area of the Maxillary. J. Craniofacial Surg. 2013, 24, 1974–1979. [Google Scholar] [CrossRef] [PubMed]
- Quinzi, V.; Ferro, R.; Rizzo, F.A.; Marranzini, E.M.; Federici Canova, F.; Mummolo, S.; Mattei, A.; Marzo, G. The Two by Four Appliance: A Nationwide Cross-Sectional Survey. Eur. J. Paediatr. Dent. 2018, 19, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Chen, J.; Guo, J.; Li, F.; Liu, Z.; He, S.; Zou, S. Distalization of the Mandibular Dentition of an Adult with a Skeletal Class III Malocclusion. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 854–862. [Google Scholar] [CrossRef]
- Hisano, M.; Chung, C.J.; Soma, K. Nonsurgical Correction of Skeletal Class III Malocclusion with Lateral Shift in an Adult. Am. J. Orthod. Dentofac. Orthop. 2007, 131, 797–804. [Google Scholar] [CrossRef]
- Successful and Stable Orthodontic Camouflage of a Mandibular Asymmetry with Sliding Jigs. Available online: https://journals.sagepub.com/doi/epdf/10.1080/14653125.2018.1444539 (accessed on 21 June 2023).
- Inchingolo, A.M.; Malcangi, G.; Costa, S.; Fatone, M.C.; Avantario, P.; Campanelli, M.; Piras, F.; Patano, A.; Ferrara, I.; Di Pede, C.; et al. Tooth Complications after Orthodontic Miniscrews Insertion. Int. J. Environ. Res. Public Health 2023, 20, 1562. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Ferrara, I.; Viapiano, F.; Netti, A.; Campanelli, M.; Buongiorno, S.; Latini, G.; Carpentiere, V.; Ciocia, A.M.; Ceci, S.; et al. Rapid Maxillary Expansion on the Adolescent Patient: Systematic Review and Case Report. Children 2022, 9, 1046. [Google Scholar] [CrossRef]
- Kim, D.; Sung, S. Nonsurgical Correction of a Class III Skeletal Anterior Open-Bite Malocclusion Using Multiple Microscrew Implants and Digital Profile Prediction. Am. J. Orthod. Dentofac. Orthop. 2018, 154, 283–293. [Google Scholar] [CrossRef]
- Rosa, M.; Quinzi, V.; Marzo, G. Paediatric Orthodontics Part 1: Anterior Open Bite in the Mixed Dentition. Eur. J. Paediatr. Dent. 2019, 20, 80–82. [Google Scholar] [CrossRef]
- Aslan, B.I.; Küçükkaraca, E. Nonextraction Treatment of a Class III Malocclusion Case Using Mini-Screw-Assisted Lower Molar Distalization. Turk. J. Orthod. 2019, 32, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Lima, C.E.O.; Lima, M.T.O. Directional Force Treatment for an Adult with Class III Malocclusion and Open Bite. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 817–824. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Heo, S.; Tai, K.; Kojima, Y.; Kook, Y.-A.; Chae, J.-M. Biomechanical Considerations for Total Distalization of the Mandibular Dentition in the Treatment of Class III Malocclusion. Semin. Orthod. 2020, 26, 148–156. [Google Scholar] [CrossRef]
- Tai, K.; Park, J.H.; Tatamiya, M.; Kojima, Y. Distal Movement of the Mandibular Dentition with Temporary Skeletal Anchorage Devices to Correct a Class III Malocclusion. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 715–725. [Google Scholar] [CrossRef] [PubMed]
- Ma, Q.L.; Conley, R.S.; Wu, T.; Li, H. Asymmetric Molar Distalization with Miniscrews to Correct a Severe Unilateral Class III Malocclusion. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 729–739. [Google Scholar] [CrossRef]
- Patano, A.; Inchingolo, A.M.; Laudadio, C.; Azzollini, D.; Marinelli, G.; Ceci, S.; Latini, G.; Rapone, B.; Inchingolo, A.D.; Mancini, A.; et al. Therapeutic Strategies of Primary Molar Infraocclusion: A Systematic Review. Children 2023, 10, 582. [Google Scholar] [CrossRef] [PubMed]
- Patano, A.; Malcangi, G.; Inchingolo, A.D.; Garofoli, G.; De Leonardis, N.; Azzollini, D.; Latini, G.; Mancini, A.; Carpentiere, V.; Laudadio, C.; et al. Mandibular Crowding: Diagnosis and Management—A Scoping Review. J. Pers. Med. 2023, 13, 774. [Google Scholar] [CrossRef]
- Seo, Y.-J.; Park, J.H.; Chang, N.-Y.; Chae, J.-M. Non-Surgical Camouflage Treatment of a Skeletal Class III Patient with Anterior Open Bite and Asymmetry Using Orthodontic Miniscrews and Intermaxillary Elastics. Appl. Sci. 2023, 13, 4535. [Google Scholar] [CrossRef]
- Jing, Y.; Han, X.; Guo, Y.; Li, J.; Bai, D. Nonsurgical Correction of a Class III Malocclusion in an Adult by Miniscrew-Assisted Mandibular Dentition Distalization. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 877–887. [Google Scholar] [CrossRef]
- Laudadio, C.; Inchingolo, A.D.; Malcangi, G.; Limongelli, L.; Marinelli, G.; Coloccia, G.; Montenegro, V.; Patano, A.; Inchingolo, F.; Bordea, I.R.; et al. Management of Anterior Open-Bite in the Deciduous, Mixed and Permanent Dentition Stage: A Descriptive Review. J. Biol. Regul. Homeost. Agents 2021, 35, 271–281. [Google Scholar] [CrossRef]
- Sha, H.N.; Lim, S.Y.; Kwon, S.M.; Cha, J.-Y. Camouflage Treatment for Skeletal Class III Patient with Facial Asymmetry Using Customized Bracket Based on CAD/CAM Virtual Orthodontic System. Angle Orthod. 2020, 90, 607–618. [Google Scholar] [CrossRef]
- Schätzle, M.; Männchen, R.; Zwahlen, M.; Lang, N.P. Survival and Failure Rates of Orthodontic Temporary Anchorage Devices: A Systematic Review. Clin. Oral. Implant. Res. 2009, 20, 1351–1359. [Google Scholar] [CrossRef] [PubMed]
- Sugawara, Y.; Kuroda, S.; Tamamura, N.; Takano-Yamamoto, T. Adult Patient with Mandibular Protrusion and Unstable Occlusion Treated with Titanium Screw Anchorage. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 102–111. [Google Scholar] [CrossRef]
- Hakami, Z.; Chen, P.J.; Ahmida, A.; Janakiraman, N.; Uribe, F. Miniplate-Aided Mandibular Dentition Distalization as a Camouflage Treatment of a Class III Malocclusion in an Adult. Case Rep. Dent. 2018, 2018, 3542792. [Google Scholar] [CrossRef] [PubMed]
- Kook, Y.-A.; Park, J.H.; Bayome, M.; Kim, S.; Han, E.; Kim, C.H. Distalization of the Mandibular Dentition with a Ramal Plate for Skeletal Class III Malocclusion Correction. Am. J. Orthod. Dentofac. Orthop. 2016, 150, 364–377. [Google Scholar] [CrossRef] [PubMed]
- Patano, A.; Cardarelli, F.; Montenegro, V.; Ceci, S.; Inchingolo, A.D.; Semjonova, A.; Palmieri, G.; Pede, C.D.; Mancini, A.; Maggiore, M.E.; et al. Early Functional Orthodontic Treatment of Bad Oral Habits with AMCOP® Bio-Activators. J. Biol. Regul. Homeost. Agents 2022, 36, 91–110. [Google Scholar] [CrossRef]
- Suh, H.-Y.; Lee, S.-J.; Park, H.S. Use of Mini-Implants to Avoid Maxillary Surgery for Class III Mandibular Prognathic Patient: A Long-Term Post-Retention Case. Korean J. Orthod. 2014, 44, 342–349. [Google Scholar] [CrossRef]
- Simon, M.; Keilig, L.; Schwarze, J.; Jung, B.A.; Bourauel, C. Forces and Moments Generated by Removable Thermoplastic Aligners: Incisor Torque, Premolar Derotation, and Molar Distalization. Am. J. Orthod. Dentofac. Orthop. 2014, 145, 728–736. [Google Scholar] [CrossRef]
- Bowman, S.J. Upper-Molar Distalization and the Distal Jet. J. Clin. Orthod. 2016, 50, 159–169. [Google Scholar]
- Pasciuti, E.; Coloccia, G.; Inchingolo, A.D.; Patano, A.; Ceci, S.; Bordea, I.R.; Cardarelli, F.; Di Venere, D.; Inchingolo, F.; Dipalma, G. Deep Bite Treatment with Aligners: A New Protocol. Appl. Sci. 2022, 12, 6709. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Laudadio, C.; Di Pede, C.; et al. The Efficacy of a New AMCOP(R) Elastodontic Protocol for Orthodontic Interceptive Treatment: A Case Series and Literature Overview. Int. J. Environ. Res. Public. Health 2022, 19, 988. [Google Scholar] [CrossRef] [PubMed]
- Auladell, A.; De La Iglesia, F.; Quevedo, O.; Walter, A.; Puigdollers, A. The Efficiency of Molar Distalization Using Clear Aligners and Mini-Implants: Two Clinical Cases. Int. Orthod. 2022, 20, 100604. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Articles screening strategy | Keywords: (“distalization”) AND (“Class III”) |
| Timespan: from January 2013 up to 11 May 2023 | |
| Electronic Databases: PubMed, Scopus, Cochrane, and Web of Science. |
| Author (Year) | Study Design | Patient (Age) | Distalization Method |
|---|---|---|---|
| He et al. (2022) [27] | Retrospective Study | 44 patients (mean age 21 yrs) | Comparison with TADs and fixed appliance |
| Guo et al. (2020) [28] | Retrospective Study | 22 patients (mean age 21 yrs) | Fixed appliance |
| Nakamura et al. (2017) [29] | Retrospective Study | 23 patients (mean age 25 yrs) | Comparison with TADs and fixed appliance |
| Yeon et al. (2022) [30] | Retrospective Study | 40 patients (mean age 26 yrs) | Comparison with TADs and Ramal plates |
| Azeem et al. (2018) [31] | Retrospective Study | 60 patients (mean age 18 yrs) | Comparison with TADs and extraction |
| Rota et al. (2022) [32] | Retrospective study | 16 patients (mean age 25 yrs) | Clear aligners |
| Yu et al. (2016) [33] | Retrospective study | 22 patients (mean age 23 yrs) | Ramal plate and fixed appliance |
| Ye et al. (2013) [34] | Observational study | 19 patients (mean age 20 yrs) | TADs and fixed appliance |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inchingolo, A.M.; Patano, A.; Malcangi, G.; Azzollini, D.; Laudadio, C.; Ciocia, A.M.; Sardano, R.; Ferrante, L.; Campanelli, M.; Dipalma, G.; et al. Mandibular Molar Distalization in Class III Malocclusion: A Systematic Review. Appl. Sci. 2023, 13, 9337. https://doi.org/10.3390/app13169337
Inchingolo AM, Patano A, Malcangi G, Azzollini D, Laudadio C, Ciocia AM, Sardano R, Ferrante L, Campanelli M, Dipalma G, et al. Mandibular Molar Distalization in Class III Malocclusion: A Systematic Review. Applied Sciences. 2023; 13(16):9337. https://doi.org/10.3390/app13169337
Chicago/Turabian StyleInchingolo, Angelo Michele, Assunta Patano, Giuseppina Malcangi, Daniela Azzollini, Claudia Laudadio, Anna Maria Ciocia, Roberta Sardano, Laura Ferrante, Merigrazia Campanelli, Gianna Dipalma, and et al. 2023. "Mandibular Molar Distalization in Class III Malocclusion: A Systematic Review" Applied Sciences 13, no. 16: 9337. https://doi.org/10.3390/app13169337
APA StyleInchingolo, A. M., Patano, A., Malcangi, G., Azzollini, D., Laudadio, C., Ciocia, A. M., Sardano, R., Ferrante, L., Campanelli, M., Dipalma, G., Di Venere, D., Inchingolo, A. D., & Inchingolo, F. (2023). Mandibular Molar Distalization in Class III Malocclusion: A Systematic Review. Applied Sciences, 13(16), 9337. https://doi.org/10.3390/app13169337