1. Introduction
One-sentence summary: We provide evidence that heart rate cannot be influenced by different tempi (bpm), regardless of age or whether a neurological disease (which can also cause cardiological changes) is present. Can heart rate be influenced by different music genres or modulated sounds? This was the question to be answered in the present study. For this purpose, the influence of different music genres and sounds on the heart rate is analyzed in three groups of subjects.
The question arises from the fact that musical influences on the cardiovascular system have been widely studied [
1,
2,
3,
4]. Basically, music activates several brain areas simultaneously, according to which timbre, rhythm and tones address the different brain areas [
5,
6,
7]. Depending on the perception of the sound, stimulating or relaxing effects can then be evoked [
8]. In this context, Bernardi et al. [
1] demonstrated that musical tracks with and without vocals elicited significant correlations between cardiovascular or respiratory signals and the music profile. Cardiovascular (especially skin vasomotion) and respiratory fluctuations were reflected in the music profile, especially when it contained a crescendo. Furthermore, they demonstrated that specific musical phrases (often in the rhythm of 6 cycles/min in famous arias by Verdi) can synchronize inherent cardiovascular rhythms and, thus, modulate cardiovascular control. These responses do not differ between musicians and non-musicians. Listening to pieces by Mozart and Strauss for 25 min each lowered blood pressure and heart rate when compared with music by ABBA, according to Trappe and Voit [
2]. They studied 120 cardiac healthy subjects aged 25–75 years as part of a randomized controlled trial. Similarly, the music of Mozart has been found to reduce systolic blood pressure compared to those subjects who listened to The Beatles or news on the radio [
4]. It has also been demonstrated that vocal and orchestral music produce significantly better correlations between cardiovascular or respiratory signals than music with a more uniform emphasis [
3].
Accordingly, both the heart rate and respiratory rate were found to be higher with “pleasant stimuli” than with “unpleasant stimuli” or silence [
9]. Listening to music compared with silence has also been studied several times and, similarly, cardiovascular parameters, such as heart rate, are lowest in silence and increase with music [
1,
9,
10,
11].
Three reviews of this topic on music and its physiological influences (i.e., the heart rate) [
2,
12,
13] conclude that, on the one hand listening to music which evokes higher emotional arousal is associated with a higher HR than that evoked by soothing music [
13]. Thus, exciting music is associated with a higher HR than soothing music [
14]. On the other hand, in terms of music genre, the greatest health benefits were evident with classical and meditation music, whereas listening to heavy metal or techno music were attributed as being not only ineffective but also possibly dangerous, because they could lead to stress and/or life-threatening arrhythmias [
3].
Consequently, Trappe and Voit [
2], Gruhlke et al. [
4] and Koelsch and Jäncke [
13] have found different responses to the different music styles on the heart rate and blood pressure, respectively. Demonstrable differences have also been found between vocal and orchestral music and music with a more uniform emphasis in this regard [
1]. According to Krabs et al. [
10], when arousal was counterbalanced by different music, no changes in HR were found with the time differences of the music (90 vs. 120 beats per minute [bpm]). Da Silva et al. [
15] confirmed this.
Therefore, uniform tones with equivalent beats per minute (bpm) were selected, in addition to different music styles with different bpm, to be investigated in the present study. In order to compare a neutral reference without tonal components, pink noise was also applied as a stimulus in the study. This is a sound in which all frequency ranges of the audible sound spectrum are perceived as being approximately of equal volume.
In the present study, the effect of music and sounds were to be measured and compared within and between three groups of subjects. This approach was taken due to the fact that both age and disease can influence the heart rate and younger adults have a higher HRV rest hear rate than older people [
16,
17]. In addition to the physiological ageing process, however, sociological aspects should also be taken into account when grouping. After all, musical preferences and the way people listen to music or their relationship to music changes with age. Since the reference values of various health parameters (e.g., blood pressure [
18], bone density [
19]) are either based on younger healthy adults, among others, up to 39 years of age or on age- and sex-specific reference values, this study was based on these values. Cardiac autonomic abnormalities have also been described in patients with Parkinson’s disease in particular, even at the early stages of the disease [
20,
21]. For example, Morris et al. [
22] found that the familiarity of music has a greater impact on listening pleasure in people with PD than in non-PD individuals. However, the PD patients perceived a lower self-evident association between the music and activity than healthy people. Thus, Morris et al. [
22] concluded that PD patients need more encouragement and empowerment to make familiar music choices in order to have better access to music-based interventions. Following this previous study, healthy adults were analyzed together with patients diagnosed with Parkinson’s disease (PD) in the present study.
Thus, the first aim of the present study was to analyze the influence of different music genres (classical, relaxation and heavy metal) with different speeds (given in beats per minute, bpm), three modulated noises equivalent to the three musical styles, a pink noise and silence on the heart rate. There were three conditions within the silence condition: without headphones (HP), with headphones without noise canceling (HP_w_NC) and with headphones with noise canceling (HP_NC).
Therefore, the secondary aim was the comparison of the heart rate between the three subject groups of young and elderly healthy people as well as patients with Parkinson’s disease. Since this study includes three groups of subjects, three different music genres, four tones, and three different silence conditions, it has a pilot character.
For the determination of the heart rate, the method of optical heart rate measurement was chosen in this study. This method has been shown to yield comparable data to that obtained by ECG measurement or heart rate recording via a chest strap and can, therefore, be used confidently under resting conditions [
23,
24]. Since the subjects were in a stationary stance only and, thus, no abrupt, violent or intensive movements occurred, (i.e., it was assumed that no displacement of the wristband nor varying heart rates due to physical activity had taken place), a continuous and reproducible measurement position could be assumed.
2. Material and Methods
2.1. Subjects
A total of 80 subjects (43 m/37 w) with a mean age of 50.7 ± 18.8 years participated in this study. The data of 3 subjects could not be analyzed for technical reasons, thus, 77 subjects were included in the study, divided into three groups:
Group YA: 29 (14 m/15 w) healthy adults aged 20–35 years with an average age of 29.9 ± 7.5 years. Inclusion criteria were as follows: subjectively reported to be cardiac healthy, free from musculoskeletal complaints, no musculoskeletal surgeries within the past 2 years, no hearing defects, no vertigo, no auditory system disorders, no current drug therapy and no neurological diseases.
Group EA: 28 (17 m/11 w) healthy adults aged 55–76 years with an average age of 64.0 ± 5.4 years. Inclusion criteria were as follows: subjectively reported to be cardiac healthy, free from musculoskeletal complaints, no musculoskeletal surgery within the past 2 years, no hearing defects, no vertigo, no auditory system disorders, no current drug therapy and no neurological diseases.
Group PD: 20 (10 m/10 w) adults diagnosed with Parkinson’s disease aged 42–76 with an average age of 64.1 ± 12.5 years. Inclusion criteria were as follows: a Yahr grade of disability of I–II, free from musculoskeletal complaints according to subjective data, no musculoskeletal surgeries within the past 2 years, no hearing defects, no vertigo, no auditory system disorders and a medically confirmed diagnosis of Parkinson’s disease. All patients with idiopathic Parkinson’s disease were diagnosed and treated according to guidelines and therefore they were likely to receive L-Dopa/Carbidopa [
25]. No influence of L-Dopa on cardiac frequency is mentioned in the drug information sheets although it might be possible that the basal heart rate may be marginally increased. The participants in the PD group were on medication when participating in the experiments.
Exclusion criteria for groups YA and EA were the presence of a neurological disease or, accordingly, the negation of the inclusion criteria. The same exclusions applied to group PD except that neurological complaints due to PD were an inclusion criterion. A medical hearing test was not performed.
Written informed consent was obtained from all patients prior to enrollment. Since this study was cross-sectional, there was no clinical trial that required a checklist. An approved ethics application from the Department of Psychology and Sports of the Goethe University Frankfurt is available for the study (processing number: 2016-63). The requirements of the ethics application are based on the ethical principles that apply to medical research on living subjects (humans). The principles are published in the latest edition of the Declaration of Helsinki, Finland (2013).
2.2. Heart Rate Monitor
The optical sensor “Polar OH1” (Polar Electro GmbH Germany, Büttelborn, Germany) was used to determine the heart rate as an optical pulse sensor. It was placed on the left forearm of each test person. In order to allow the light of the LEDs to penetrate deep enough into the tissue and also to capture the reflective light effectively, the wristband was worn approximately three finger widths above the wrist, according to the vendor’s recommendations. The display of the HR in beats per minute (bpm) was carried out via the compatible Polar Beat app. After selecting the corresponding activity, it was started and the HR was displayed simultaneously on the app.
Due to the high validity of this sensor, when compared to the electrocardiogram, the HR measurements taken during medium and high physical activities [
24], and also when compared to a Polar H/chest belt during different sports [
23] or 15-min sedentary activities, 10-min cycling on a bicycle ergometer, and an incremental exercise test to exhaustion on a motorized treadmill (18–42 min) [
26], it can be assumed that the data quality was good whilst the subject was standing.
2.3. Measurement Protocol
The measurements took place in a separate room without disturbing noises and other persons being present. This meant that apart from the person to be measured and the person who performed the measurement, no one else was present in the premises. The measurements were taken barefoot whilst standing in a habitual double-legged stance. To exclude any possible visual influencing factors, all subjects wore a blindfold. Measurements were taken in the standing position because the postural data were recorded on the same subjects during the course of this study. Everyone first stood for 15 min before the measurements commenced in order to counteract orthostatic hypertension with a compensatory heart rate increase.
Furthermore, all test persons used identical wireless headphones (Bose QC35; Friedrichsdorf, Germany), which have the option of switching off ambient noise via acoustic noise canceling (NC). The loudness of all acoustic stimuli were adjusted to equal level. To do this, the RMS (Root Mean Square) level over the entire length of the digital audio signal of the respective sounds was calculated and adjusted, respectively, to equal. The playback level was set to 70 dB(A).
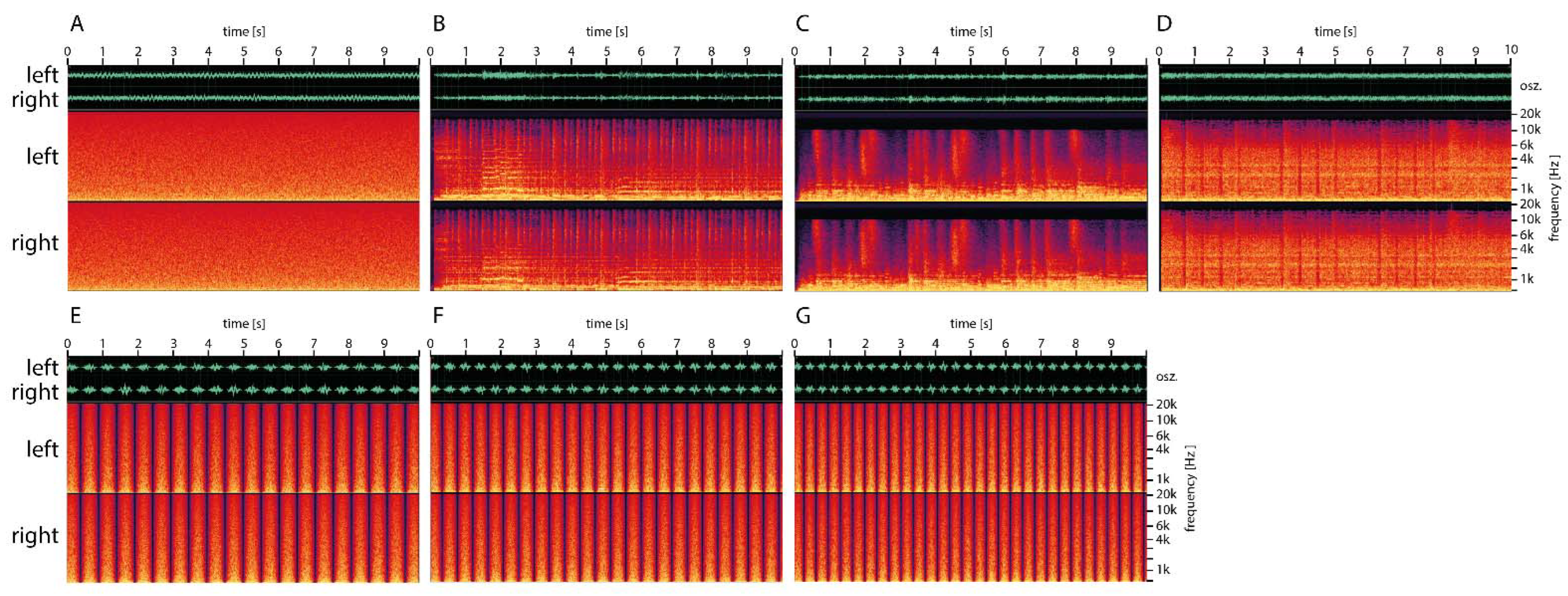
Pink noise was used as the noise signal. Pink noise decreases in amplitude with increasing frequency at 1/f. This is perceived as a noise in which the average person perceives all frequency ranges of the audible sound spectrum as being approximately equal volume [
27]. A graphical representation of the first 10 s of the acoustic stimuli in the time and frequency domains is shown in
Figure 1.
This HR display was launched on the app after the appropriate activity level was selected. The HR was measured continuously throughout the performance, with documentation of the HR occurring within the three trials, each after 25 s of the 30 s measurement interval. Subsequently, the three values of HR were statistically averaged. Due to the precarious stance of the selected PD patients, a longer measurement sequence was not possible based on pilot measurements. The following measurement conditions were recorded at constant volume, in a randomized order:
- -
(A) without headphones (wHP)
- -
(B) with headphones without ambient noise canceling (Bose) (HP without noise canceling; HP_w_NC)
- -
(C) headphones with noise cancelation (HP_NC).
- -
(D) genre relaxation (Drifting Clouds—Florenc Hegedus; 117 bpm, 800–1300 Hz) with NC
- -
(E) genre classical music (Carmina Burana- Carl Orff; 139 bpm, 1400–1800 Hz) with NC
- -
(F) genre heavy metal (Stricken—Disturbed; 174 bpm, 6000–8000 Hz) with NC
- -
(G) modulated pink noise at 117 bpm with NC
- -
(H) modulated pink noise at 139 bpm with NC
- -
(I) modulated pink noise at 174 bpm with NC
2.4. Statistical Analysis Procedures
Statistical analysis was conducted by using BIAS (Epsilon Verlag, Darmstadt, Germany). After testing the data of each group for normal distribution using the Kolmogorov-Smirnov test, it was found that the data of group 3 were not normally distributed and, therefore, non-parametric tests were used. To test for group differences per measurement condition, the Kruskal-Wallis test was used, while to compare measurement conditions per group, the Friedman test was used. For the following multiple pair comparison, the Conover-Iman test or Wilcoxon matched pairs test were used accordingly. All p-values were subsequently subjected to a Bonferroni-Holm correction. The significance level was set at 5%.
3. Results
In this case, 50% of the heart rates were found between the 1st (25%) and 3rd quartile (75% The comparisons of the measurement conditions (Friedman test) without noise among each other, i.e., (a) without headphones, (b) headphones with noise canceling and (c) headphones without noise canceling, showed no significant differences in any of the groups (
Table 1).
Table 1 also presents the comparisons of the effects of the measured sound conditions on HR per group (within-group differences). Group 1 (
p ≤ 0.001) presented the most significant group differences (
p ≤ 0.05–0.001) between the measurement conditions. Most frequently, the 117 bpm measurement condition differed significantly from the other measurement conditions (
p ≤ 0.05–0.001; HP without NC, HP with NC, classical music, relaxation music, heavy metal music, 139 bpm and 174 bpm). In addition, the measurement condition “pink noise” was often significantly different from the other conditions (
p ≤ 0.05–0.001; without HP, HP without NC, classical music, heavy metal music, 139 bpm). The median difference (
Table 1) of all the significant HR differences was a maximum of 6 bpm and a minimum of 1 bpm.
In group 2 (p ≤ 0.001), significant pairwise comparisons (p ≤ 0.05–0.001) were present only in the following comparisons: without HP vs. 117 bpm, HP without noise canceling vs. 117 bpm and relaxation music vs. 117 bpm, with the median HR differing between 4.5–3 bpm between these significant differences.
In group 3, the Friedman test was not significant (p ≤ 0.64) and, consequently, there were no group differences observed.
The interaction effect between group and gender was F = 0.11 (p = 0.74). In conclusion the different gender ratio did not have an effect.
Between-Group Differences
Table 2 contains the group-specific median values as well as the data of the 1st and 3rd quartiles. This table also contains the
p-values of the group comparisons of the Kruskal-Wallis test for each sound condition as well as the corrected
p-values of the pair comparisons after Bonferroni-Holm correction (between-group differences). Furthermore, the
p-values of the Friedman test and the subsequent multiple pairwise comparisons, according to Conover-Iman including Bonferroni-Holm correction, across all measurement conditions per group are shown in this table.
When the three subject groups were compared for each measurement condition, group differences were evident (
p ≤ 0.05–0.001). The subsequent pairwise comparison illustrates a significant group difference (
p ≤ 0.05–0.001) in each parameter between the first and second group, i.e., between the young and older healthy adults. Only in the case of the continuous noise at 117 bpm did the heart rate additionally differ between groups YA and PD with
p ≤ 0.04. In each comparison, the HR of the subjects from group YA was at least 8 bpm above the median of the subjects from group EA and group PD, respectively. The average HR of each subject in their group is shown in
Figure 2, where the divergent heart rates between the three groups can be seen. While the median HR in group YA ranged 86–92 bpm for all measurement conditions, it ranged 75.5–80 bpm in group EA and 80–84 bpm in group PD.
4. Discussion
The objective of the present study was to analyze the influence of music genres (classical, relaxation and heavy metal), the speed and frequency of three modulated sounds (117 bpm, 139 bpm and 174 bpm) as well as a pink noise on the HR of three different subject groups: (a) young adults, (b) older adults and (c) Parkinson’s disease patients.
For this purpose, the HR in silence was also compared in advance under three different conditions (without headphones, with headphones without ambient noise canceling and with headphones with ambient noise canceling) for each group. Statistical analysis revealed no significant differences between these three conditions in each group. Thus, wearing headphones either alone or with noise canceling does not affect the heart rate, regardless of whether one is neurologically and cardiologically healthy or has a medical diagnosis of Parkinson’s neurological disease.
4.1. Within-Group Analysis
Different responses when listening to the different music sequences in the younger adults were more frequent than in the older adults, while the HR of the PD patients did not change significantly. In the YA, listening to a “pink noise” and a modulated pink noise at 117 bpm proved to be the conditions in which the mean heart rate was significantly higher than in the other conditions. However, these responses were observed for modulated noises only and not for songs. A similar pattern was seen in the older adult group with respect to a modulated pink noise at 117 bpm.
Other studies [
16,
17] have shown that younger people have a higher heart rate variability than older individuals, while people with chronic diseases have been shown to have a lower heart rate variability (HRV) than healthy individuals [
17]. Based on these findings, it can be hypothesized that the HRs of the younger people were correspondingly more sensitive to the measurement conditions than the older individuals. In group PD, which comprised of the chronically ill, the lowest responses to the different conditions were found. Older people often show an age-related hearing loss that increases with age [
28]. The playback level of 70 dB in this study was selected so that all relevant frequencies were sufficiently audible even in this group of people.
However, emotional reactions may change the HR, although these changes are not due to the tempi underlying the music/sound in question. Insofar as the demonstrable differences between the measurement conditions (music and sounds) were predominantly found in the younger subjects [
14], this may be because younger people have a higher HRV than older people and, thus, were correspondingly more sensitive to the conditions studied [
16,
17]. Furthermore, with regard to emotional reactions, it must also be taken into account that both music and speech can determine physiological indices of semantic processing [
29]. In this context, Salimpoor et al. [
30] investigated the high social value of music and were able to show that intense pleasure in reaction to music leads to a dopamine release in the striatal system. Specifically, the anticipation of an abstract reward can result in dopamine release in an anatomical pathway distinct from that associated with the actual high pleasure.
In addition, the people with PD barely responded at all to music in terms of the effects on HR which may be due to a reduced HRV in chronically ill people. The higher average HR of the elderly subjects, when compared with those having PD can be explained by the age range within the groups when taking into account the age-related pathophysiological mechanisms: group PD included participants aged 42 years and older, while in group EA, the participants were aged 55 years or more.
4.2. Between-Group Analysis
Examination of the significant differences of the HR among the groups in each measurement condition shows that the median HR in each measurement condition and also at rest without headphones, was on average about 10 bpm higher in young adults than in older adults (without PD). The median HR of the PD adults was an intermediate between these two groups, but was also below the HR of the younger adults (
Figure 1). The significant difference between the older adults and the PD patients for the modulated noise, 117 bpm, is rather negligible on the basis of identical medians. Therefore, young adults tend to have a slightly higher HR than older people (groups EA and PD) and, thus, the differences found cannot be associated with listening to music or sounds.
The finding that exciting music, such as heavy metal music, is associated with a higher HR than soothing music [
13], cannot be confirmed in the context of this study for any of the groups. In addition, we could not demonstrate evidence for a coupling of the heart rate to the musical beats. However, Krab’s statement [
10] can be confirmed by our study, i.e., that when arousal is balanced by different music, there are no changes in the HR with the time differences of the music (90 vs. 120 bpm). Likewise, there was no integration of the HR with the musical beats, confirming the finding of Ellis and Thayer [
31]. Contrary to the results of Orini et al. [
9], there was no evidence of increased heart rate with “unpleasant stimuli” (such as pink noise or continuous noise at 117, 139 or 174 bpm) or with “silence” versus “pleasant stimuli” (musical songs).
The correlation between resting pulse rate, age and sex of 92,457 adults [
32] showed that the resting pulse rate increases until about the age of 50 years and then decreases regardless of sex. Thus, the present differences observed in our study, between group YA and groups EA and PD, cannot be explained by the present age differences alone. However, EA did include an increased proportion of men. However, the difference in the number of sexes has not been shown to have any significant interaction effect.
The potential reason for the decreasing heart rate with increasing age might be on the basis of a reduced left ventricular compliance due to an increase in the collagen content and the associated decrease in water content leading to fibrosis [
20,
33]. Changes in the conduction system itself may also play a role [
20,
33]. With decreasing pacemaker cells and increasing fatty infiltration a loss of specialized fibers results and, thus, an intrinsic decrease in sinus automatism. In addition, dynamic histochemical and immunohistochemical changes during the aging process appear to have an impact on the autonomic responses associated with the decrease in heart rate in the elderly [
34,
35]. Furthermore, it should be taken into account that possible effects due to medication (e.g., L-dopa) in PD patients could have biased the results.
4.3. Limitations
We did not perform the measurements in a soundproof room, but in a quiet office room, thus, randomly occurring noises could not be excluded during the measurements. However, we always made sure that no external noise disturbed the measurements. As the intra- and inter-day reliabilities of heart rate variability had previously been demonstrated [
36], all the measurements should have been performed in the same time window. Most measurements in our study were performed in the morning. However, a uniform measurement time was not possible because of the scheduling discrepancies of the subjects.
Furthermore, the measurement durations were longer in other studies. Ellis et al. [
31] measured for at least 2.5 min for each condition, while for Trappe [
3] this was >30 min. In our study, the individual measurement periods of 3 × 30 s (statistically averaged) were shorter, but we conducted more measurement conditions and all our subjects were blindfolded for the entire measurement time. This represented an enormous challenge for the PD patients whose temporal extension of a measurement condition would have been to the detriment of the standing quality.
In future studies, it would be desirable to investigate further PD patients with a Yahr grade of disability of III or IV with regard to the present research question, whereby the medication should also be evaluated and its possible influence on the measurement result analyzed.
In addition, future studies could analyze whether a different starting position (e.g., sitting), a different measurement duration (e.g., 5 min per condition), or medication affects HR.
Thus, based on these results of this pilot study, it can be concluded that, in general, listening to different music genres or sounds of different tempi barely affects the HR. However, due to the technology used, we do not have time dependent data to calculate heart rate variability in a validated manner. The capture of heart rate variability would be worth setting up future measurement.
Nevertheless, the between-group comparison and the within-group comparison of the significant measurement conditions 50% of the heart rates were found between the 1st (25%) and 3rd quartile (75%) and that, in this range, there was predominantly a range of approximately 20 bpm. Therefore, the medians of the heart rate differences should be considered rather as trends with low clinical relevance.



 ,
, 




{kind=link}
{kind=link}