
Accuracy of Guided Endodontics in Posterior Teeth

 ,
,
Abstract
:1. Introduction
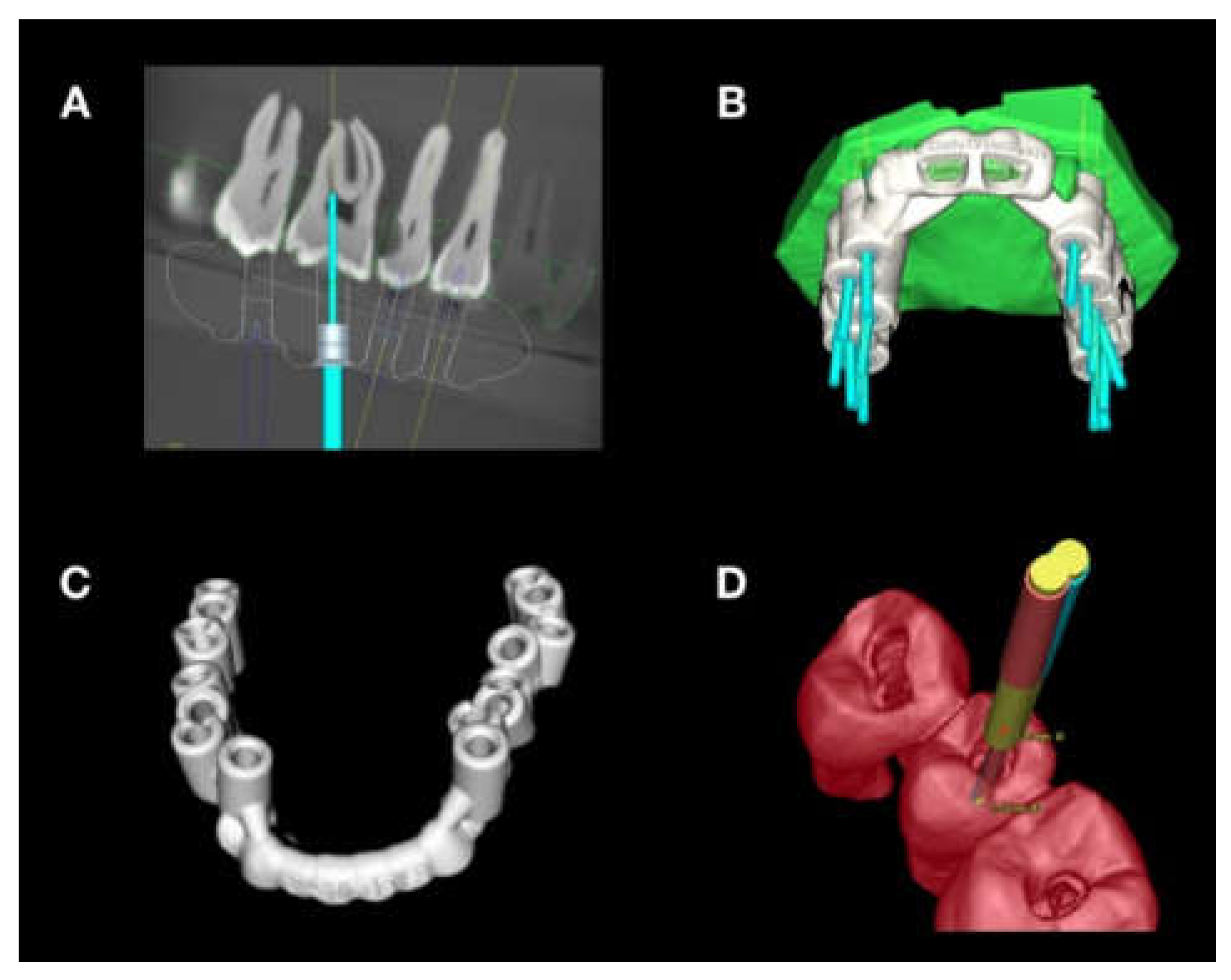
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- European Society of Endodontology. Quality guidelines for endodontic treatment: Consensus report of the European Society of Endodontology. Int. Endod. J. 2006, 39, 921–930. [Google Scholar] [CrossRef] [PubMed]
- Schilder, H. Cleaning and shaping the root canal. Dent. Clin. N. Am. 1974, 18, 269–296. [Google Scholar] [CrossRef] [PubMed]
- Kakehashi, S.; Stanley, R.; Fitzgerald, R.J. The effects of surgical exposures of dental pulps in germ-free and conventional laboratory rats. Oral. Surg. Oral. Med. Oral. Pathol. 1965, 20, 340–349. [Google Scholar] [CrossRef] [PubMed]
- Cvek M, G.L.; Lundberg, M. Failures and healing in endodontically treated non-vital anterior teeth with posttraumatically reduced pulpal lumen. Acta Odontol. Scand. 1982, 40, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Lang, H.; Korkmanz, Y.; Schneider, K.; Raab, W.H. Impact of Endodontic Treatments on the Rigidity of the Root. J. Dent. Res. 2006, 85, 364–368. [Google Scholar] [CrossRef] [PubMed]
- Kühl, S.; Payer, M.; Zitzmann, N.U.; Lambrecht, J.T.; Filippi, A. Technical accuracy of printed surgical templates for guided implant surgery with the coDiagnostiX software. Clin. Implant Dent. Relat. Res. 2015, 17, 177–182. [Google Scholar] [CrossRef]
- Connert, T.; Zehnder, M.S.; Weiger, R.; Kühl, S.; Krastl, G. Microguided Endodontics: Accuracy of a Miniaturized Technique for Apically Extended Access Cavity Preparation in Anterior Teeth. Int. Endod. J. 2017, 43, 787–790. [Google Scholar] [CrossRef] [PubMed]
- Krastl, G.; Zehnder, M.S.; Connert, T.; Weiger, R.; Kuhl, S. Guided Endodontics: A novel treatment approach for teeth with pulp canal calcification and apical pathology. Dent. Traumatol. 2015, 32, 240–246. [Google Scholar] [CrossRef]
- Connert, T.; Krug, R.; Eggmann, F.; Emsermann, I.; ElAyouti, A.; Weiger, R.; Kuhl, S.; Krastl, G. Guided Endodontics versus Conventional Access Cavity Preparation: A Comparative Study on Substance Loss Using 3-dimensional-printed Teeth. J. Endod. 2019, 45, 327–331. [Google Scholar] [CrossRef]
- Mozzo, P.; Procacci, C.; Tacconi, A.; Martini, P.T.; Andreis, I.A. A new volumetric CT machine for dental imaging based on the cone-beam technique: Preliminary results. Eur. Radiol. 1998, 8, 1558–1564. [Google Scholar] [CrossRef]
- Farman, A.G. ALARA still applies. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2005, 4, 395–397. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Brown, J.; Semper, M.; Abella, F.; Mannocci, F. European Society of Endodontology position statement: Use of cone beam computed tomography in Endodontics. Int. Endod. J. 2019, 52, 1675–1678. [Google Scholar] [CrossRef] [PubMed]
- van der Meer, W.J.; Vissink, A.; Ng, Y.L.; Gulabivala, K. 3D Computer aided treatment planning in endodontics. J. Dent. 2016, 45, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Lara-Mendes, S.T.O.; Barbosa, C.F.M.; Santa-Rosa, C.C.; Machado, V.C. Guided Endodontic Access in Maxillary Molars Using Cone-beam Computed Tomography and Computer-aided Design/Computer-aided Manufacturing System: A Case Report. J. Endod. 2018, 44, 875–879. [Google Scholar] [CrossRef]
- Lee, J.K.; Ha, B.H.; Choi, J.H.; Heo, S.M.; Perinpanayagam, H. Quantitative three-dimensional analysis of root canal curvature in maxillary first molars using micro-computed tomography. J. Endod. 2006, 32, 941–945. [Google Scholar] [CrossRef] [PubMed]
- Leontiev, W.; Bieri, O.; Madorin, P.; Dagassan-Berndt, D.; Kuhl, S.; Krastl, G.; Krug, R.; Weiger, R.; Connert, T. Suitability of Magnetic Resonance Imaging for Guided Endodontics: Proof of Principle. J. Endod. 2021, 47, 954–960. [Google Scholar] [CrossRef]
- Shi, X.; Zhao, S.; Wang, W.; Jiang, Q.; Yang, X. Novel navigation technique for the endodontic treatment of a molar with pulp canal calcification and apical pathology. Aust. Endod. J. 2018, 44, 66–70. [Google Scholar] [CrossRef]
- Zehnder, M.S.; Connert, T.; Weiger, R.; Krastl, G.; Kühl, S. Guided endodontics: Accuracy of a novel method for guided access cavity preparation and root canal location. Int. Endod. J. 2016, 49, 966–972. [Google Scholar] [CrossRef]
- Krug, R.; Reich, S.; Connert, T.; Kess, S.; Soliman, S.; Reymus, M.; Krastl, G. Guided endodontics: A comparative in vitro study on the accuracy and effort of two different planning workflows. Int. J. Comput. Dent. 2020, 23, 119–128. [Google Scholar]
- Connert, T.; Weiger, R.; Krastl, G. Present status and future directions—Guided endodontics. Int. Endod. J. 2022, 10, 995–1002. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Durack, C.; Abella, F.; Shemesh, H.; Roig, M.; Lemberg, K. Cone beam computed tomography in Endodontics—A review. Int. Endod. J. 2015, 48, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Endodontics, A.A.O. AAE and AAOMR Joint Position Statement—Use of Cone Beam Computed Tomography in Endodontics. Available online: https://www.aae.org/specialty/wp-content/uploads/sites/2/2017/06/conebeamstatement.pdf (accessed on 12 December 2022).
- Reymus, M.; Fabritius, R.; Keßler, A.; Hickel, R.; Edelhoff, D.; Stawarczyk, B. Fracture load of 3D-printed fixed dental prostheses compared with milled and conventionally fabricated ones: The impact of resin material, build direction, post-curing, and artificial aging-an in vitro study. Clin. Oral. Investig. 2020, 24, 701–710. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Deviation | Angle [Degrees] | Mesio-Distal, at Base of the Bur [mm] | Bucco-Oral, at Base of the Bur [mm] | Mesio-Distal, at Tip of the Bur [mm] | Bucco-Oral, at Tip of the Bur [mm] |
|---|---|---|---|---|---|
| Mean | 1.39 | 0.26 | 0.29 | 0.24 | 0.31 |
| Median | 1.10 | 0.20 | 0.21 | 0.18 | 0.21 |
| Minimum | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| Maximum | 7.8 | 1.19 | 1.96 | 1.61 | 1.36 |
| Deviation Type | Mean | |||||
|---|---|---|---|---|---|---|
| Maxilla | Mandible | p-Value | Premolar | Molar | p-Value | |
| Angle [°] | 1.70 | 1.04 | 0.03 | 1.52 | 1.34 | 0.89 |
| Mesiodistal, Base [mm] | 0.31 | 0.27 | 0.99 | 0.29 | 0.29 | 0.11 |
| Buccolingual, Base [mm] | 0.29 | 0.23 | 0.78 | 0.22 | 0.28 | 0.77 |
| Mesiodistal, Apex [mm] | 0.34 | 0.28 | 0.46 | 0.35 | 0.30 | 0.14 |
| Buccolingual, Apex [mm] | 0.26 | 0.21 | 0.97 | 0.16 | 0.27 | 0.77 |
| Angle Deviation [°] | |||
|---|---|---|---|
| Group 1 | Group 2 | Mean Difference: Group 1 vs. Group 2 [°] | p-Value |
| 1 CPT | 2 CPT | 1.12 | 0.006 |
| 3 CPT | 0.55 | 0.36 | |
| 2 CPT | 1 CPT | −1.12 | 0.006 |
| 3 CPT | −0.56 | 0.13 | |
| 3 CPT | 1 CPT | −0.55 | 0.36 |
| 2 CPT | 0.56 | 0.13 | |
| Bucco-Oral Deviation at Tip of the Bur [mm] | Mean Difference: Group 1 vs. Group 2 [mm] | p-Value | |
|---|---|---|---|
| Group 1 | Group 2 | ||
| 1 CPT | 2 CPT | 0.16 | 0.04 |
| 3 CPT | 0.12 | 0.21 | |
| 2 CPT | 1 CPT | −0.16 | 0.04 |
| 3 CPT | −0.04 | 1.00 | |
| 3 CPT | 1 CPT | −0.12 | 0.21 |
| 2 CPT | 0.04 | 1.00 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haarmann, B.; Leontiev, W.; Magni, E.; Kühl, S.; Dagassan-Berndt, D.; Weiger, R.; Connert, T. Accuracy of Guided Endodontics in Posterior Teeth. Appl. Sci. 2023, 13, 2321. https://doi.org/10.3390/app13042321
Haarmann B, Leontiev W, Magni E, Kühl S, Dagassan-Berndt D, Weiger R, Connert T. Accuracy of Guided Endodontics in Posterior Teeth. Applied Sciences. 2023; 13(4):2321. https://doi.org/10.3390/app13042321
Chicago/Turabian StyleHaarmann, Benjamin, Wadim Leontiev, Eva Magni, Sebastian Kühl, Dorothea Dagassan-Berndt, Roland Weiger, and Thomas Connert. 2023. "Accuracy of Guided Endodontics in Posterior Teeth" Applied Sciences 13, no. 4: 2321. https://doi.org/10.3390/app13042321