1. Introduction
Adjustments in body balance mainly integrate information from three sensory inputs—vestibular sense, visual sense, and somatosensory input—in the central nervous system and output it as muscle movements of the eyes, neck, trunk, and limbs for postural control [
1,
2,
3]. Even when postural changes are made voluntarily, hierarchical reflexes or unconscious control processes are activated. Therefore, environmental and internal factors that affect vestibular sensation, visual sensation, and somatosensory sensation influence the postural control function. In particular, factors, such as occlusion [
4,
5,
6], age and sex [
7,
8], and height and weight [
9] clearly affect postural control.
The postural control function is often measured by center of gravity (COG) sway testing, which is based on the analysis of movement of foot center of pressure (COP) [
3,
4,
5,
6,
10,
11,
12]. Such testing is used to diagnose balance disorders in otorhinolaryngology, neurology, and ophthalmology; examine occupational aptitude; and measure fatigue. The COP, which is the fulcrum of the force applied to the body, moves synchronously with the body’s COG, and the usefulness and validity of the COP as an index of the COG have been established [
13], with a gravity center fluctuation meter widely used in research to analyze the role of postural control in maintaining a static standing posture [
14].
Occlusion is the state of contact between the teeth of the maxilla (upper jaw) and mandible (lower jaw) [
15]. The maxilla is part of the lower skull, whereas the mandible is attached to the skull via the temporomandibular joint and suspended by several muscles in the head and neck. The contraction and relaxation of these muscles cause the mandible to move, with the temporomandibular joint acting as a fulcrum. Therefore, the teeth, muscles, temporomandibular joints, and the central nervous system are all involved in occlusion, and a problem with any one of these can affect occlusion.
Because occlusion is involved in somatosensory input from the stomatognathic region and in vestibular input, many studies have been conducted on its relationship with postural control [
4,
5,
6]. It has been shown experimentally that imparting occlusal interference increases COG sway [
5] and that equalization of occlusal contact by use of an intraoral appliance suppresses COP displacement [
6]. In addition, in the postural control of athletes, the weighting of sensory inputs has been reported to differ according to the characteristics and level of the sport, with the differences evident only under conditions that match the training environment [
11]. It is expected that such information about postural control will be applicable to training and rehabilitation [
11,
16,
17,
18,
19].
The aim of this study was to clarify the effect on the postural control function of equalizing the occlusal contact state by wearing a mouthguard. Therefore, the difference in COP displacement among athletes and non-athletes was examined with and without a mouthguard. The null hypothesis was that COP displacement would not be affected by wearing a mouthguard, regardless of whether the wearer is an athlete or non-athlete.
2. Materials and Methods
This study was approved by the Ethics Committee of The Nippon Dental University School of Life Dentistry at Niigata (ECNG-R-375). The details of the study were described in full to all participants, and their written informed consent was obtained.
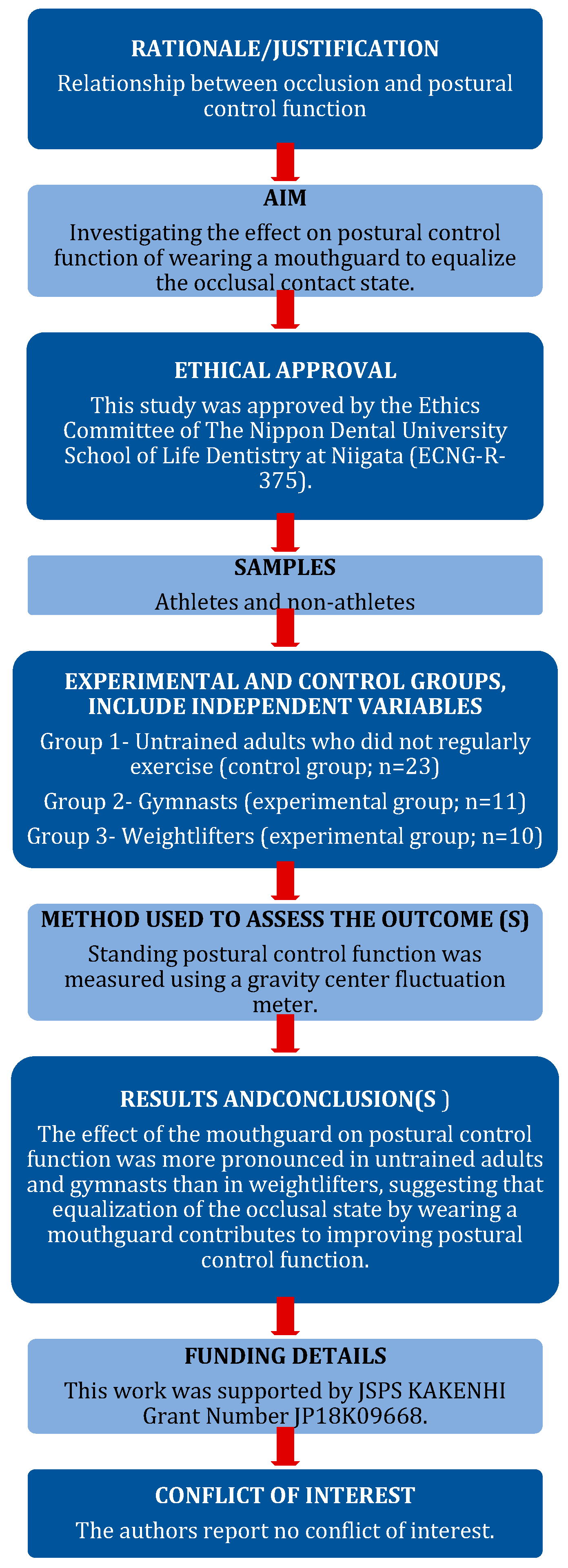
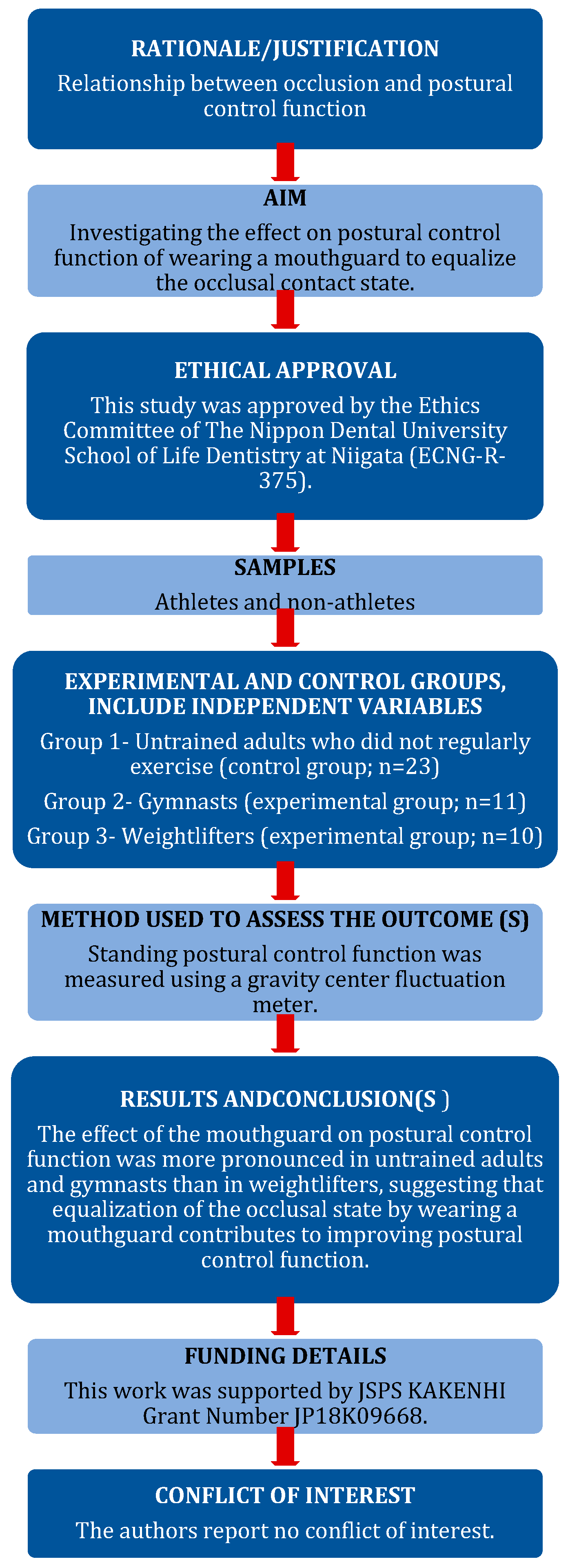
This study was conducted in accordance with the PRILE 2021 guidelines (
Figure 1) [
20].
2.1. Participants
Participants included 23 untrained adults (20.5 ± 1.1 years) who did not regularly exercise, 11 gymnasts (19.7 ± 1.4 years), and 10 weightlifters (20.0 ± 1.2 years). All participants were male, and the difference in the occlusal force between the left and right sides was less than 15%. All of the untrained adult participants had a body mass index from 18.5 to less than 25.
The occlusal state was measured using a pressure-sensitive film (Dental Prescale, 50H-R type; Fujifilm Co., Ltd., Tokyo, Japan) and evaluated using an Occluzer (FPD-707; Fujifilm Co., Ltd.) [
21,
22]. Participants inserted the Dental Prescale into the mouth and then clenched with a maximum force for 3 s in the intercuspal position. The Dental Prescale was removed, and the occlusal contact area and occlusal force were analyzed with an Occluzer. All measurements were made by a single dentist skilled in occlusal measurement. The occlusal force was calculated as the product of the occlusal contact area and occlusal pressure, and the distribution of the occlusal force on the left and right sides was displayed by the Occluzer. In this study, participants with a <15% difference in the left-and-right occlusal force against the total occlusal force were selected. For each participant, measurements were performed three times.
2.2. Mouthguard Fabrication
For each participant, a custom mouthguard was fabricated using a 2.0-mm-thick thermoplastic sheet (Sports Mouthguard, Keystone Industries, Cherry Hill, NJ, USA) and a pressure molding machine (Model Capture, Shofu, Kyoto, Japan). The amount of occlusal elevation was within the freeway space and was adjusted so that all teeth were in even contact with light clenching (
Figure 2).
2.3. Measurement of Standing Postural Control Function
A gravity center fluctuation meter (GRAVICORDER, GS-7, Anima, Tokyo, Japan) was used to measure the standing postural control function [
3,
4,
6,
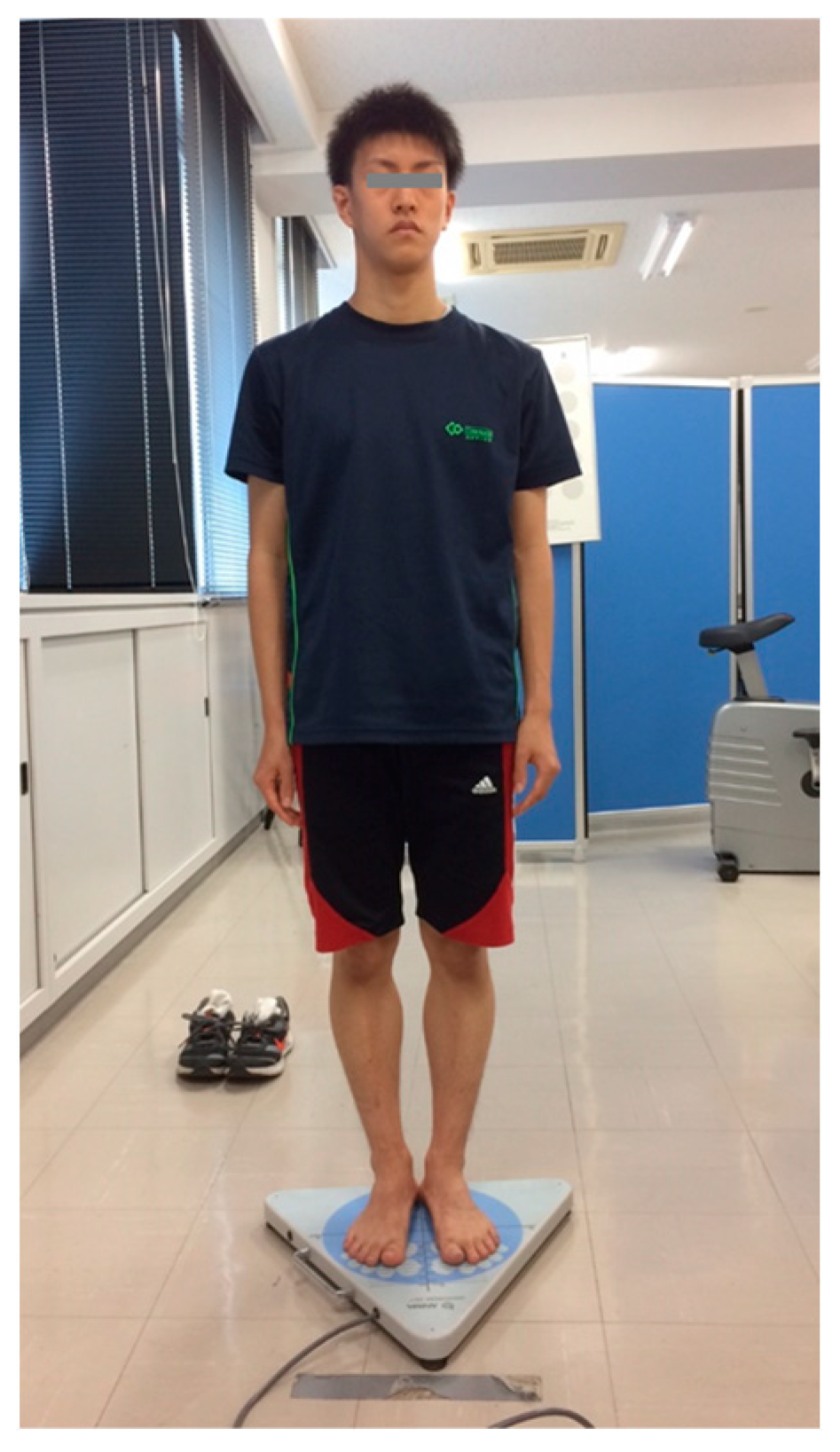
12] according to the manufacturer’s recommendations. To prevent body deviation due to visual and auditory stimuli, the participants stood upright in a quiet and evenly lit environment in a closed position with both legs in contact so that the center of the sole coincided with the reference point of the measurement table. The participants were instructed to gaze at a target 2 m away at eye level. Next, the participants were instructed to clench their teeth lightly and, after stabilization of the standing posture, to close their eyes. Measurements were taken for 30 s about 20 s after the eyes were closed (
Figure 3).
Next, measurements were taken using the same procedure under the “with mouthguard” condition. To avoid the influence of discomfort immediately after the mouthguard was inserted, participants were instructed to wear the mouthguard in advance. If discomfort was present, the mouthguard was adjusted; after the absence of discomfort was confirmed, the measurements were started.
The evaluation indices included COP displacement in the front-and-back direction (COP-FB), COP displacement in the left-and-right direction (COP-LR), and the area enclosed by the trajectory of the COP fluctuation (COP-Area). COP-FB and COP-LR were recorded as positive values for frontward and rightward displacements and negative values for backward and leftward displacements, respectively. Therefore, the absolute value was used as the displacement of COP in the analysis. Each measurement was taken three times.
2.4. Statistical Analysis
Statistical analysis software (IBM SPSS 24.0, SPSS Japan Inc., Tokyo, Japan) was used for statistical processing. For all measured values, the Shapiro–Wilk test was used to test normality, and Levene’s test was used to test homoscedasticity. Because normality and homoscedasticity were observed at each level for each factor of the participant and mouthguard, the differences in COP displacement among participants and between mouthguard conditions (i.e., with and without a mouthguard) were analyzed using a split-plot design. Next, the difference in the reduction rate of COP displacement when wearing a mouthguard was compared among participant groups. A one-way analysis of variance with Welch’s test was performed because there were levels showing unequal variances. Significance was set at p < 0.05.
3. Results
Table 1,
Table 2 and
Table 3 show the results of statistical analysis with a split-plot design for each evaluation index. In the COP-FB, COP-LR, and COP-Area evaluation indices, the participant and the mouthguard were significant factors, and their interaction was not significant. Therefore, multiple comparison tests were performed using the Bonferroni method to examine the differences in COP displacement among participants. In addition, the difference in COP displacement between mouthguard conditions was analyzed using a paired
t-test.
Figure 4 shows the difference in COP-FB among participants and between mouthguard conditions. COP-FB significantly decreased in the order from untrained adults to weightlifters to gymnasts (
p < 0.01,
p < 0.05), irrespective of the mouthguard factor. Differences due to the mouthguard factor were observed in all participants, with COP-FB being significantly lower with a mouthguard than without a mouthguard (gymnasts:
p < 0.01; untrained adults and weightlifters:
p < 0.05).
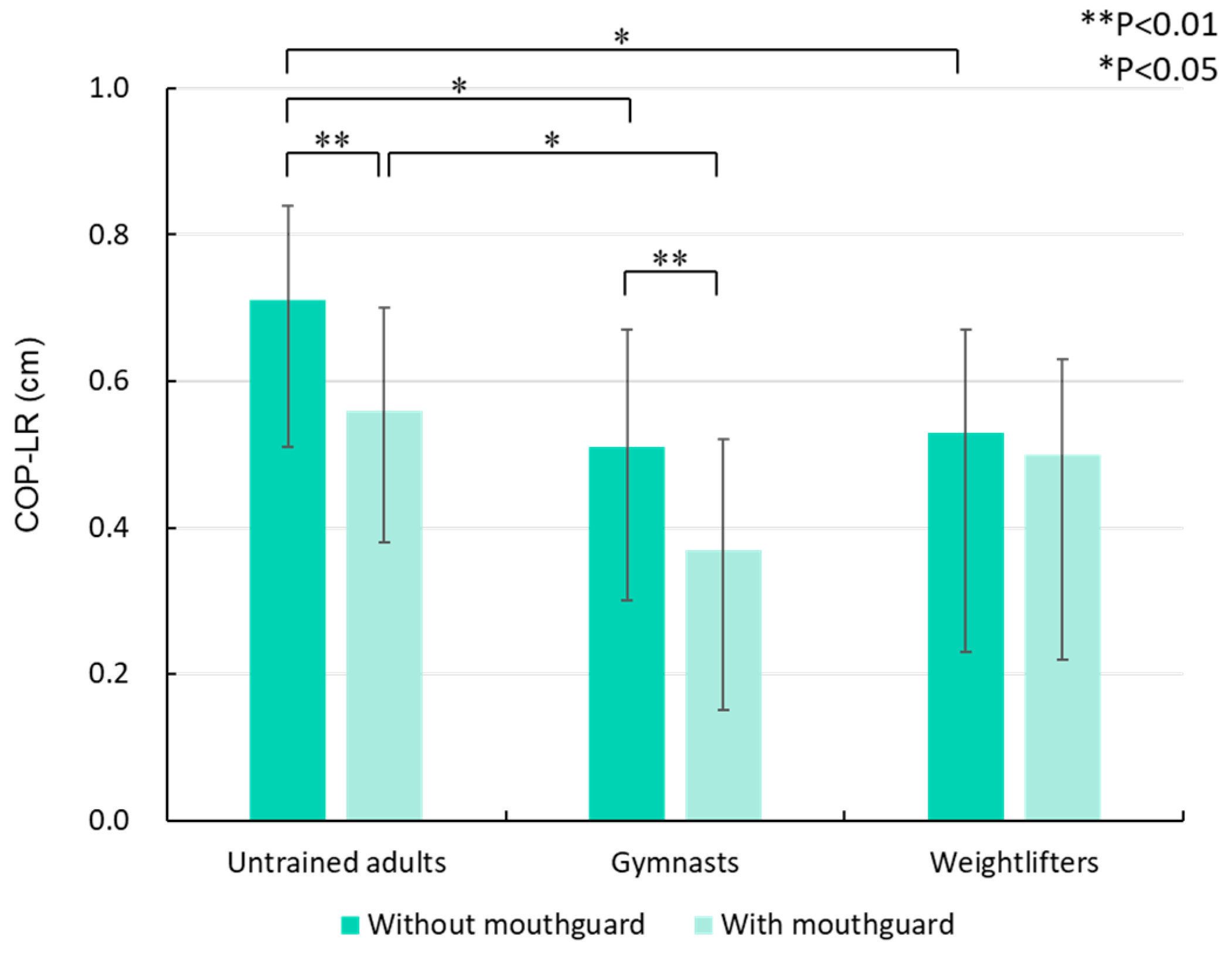
Figure 5 shows the difference in COP-LR among participants and between mouthguard conditions. Significant differences were observed between untrained adults and gymnasts and between untrained adults and weightlifters without a mouthguard, and the COP-LR values of gymnasts and weightlifters were lower than those of untrained adults (
p < 0.05). With a mouthguard, gymnasts showed significantly lower values than untrained adults (
p < 0.05). Differences due to the mouthguard factor were observed in untrained adults and gymnasts, with COP-LR values significantly lower with a mouthguard than without a mouthguard (
p < 0.01).
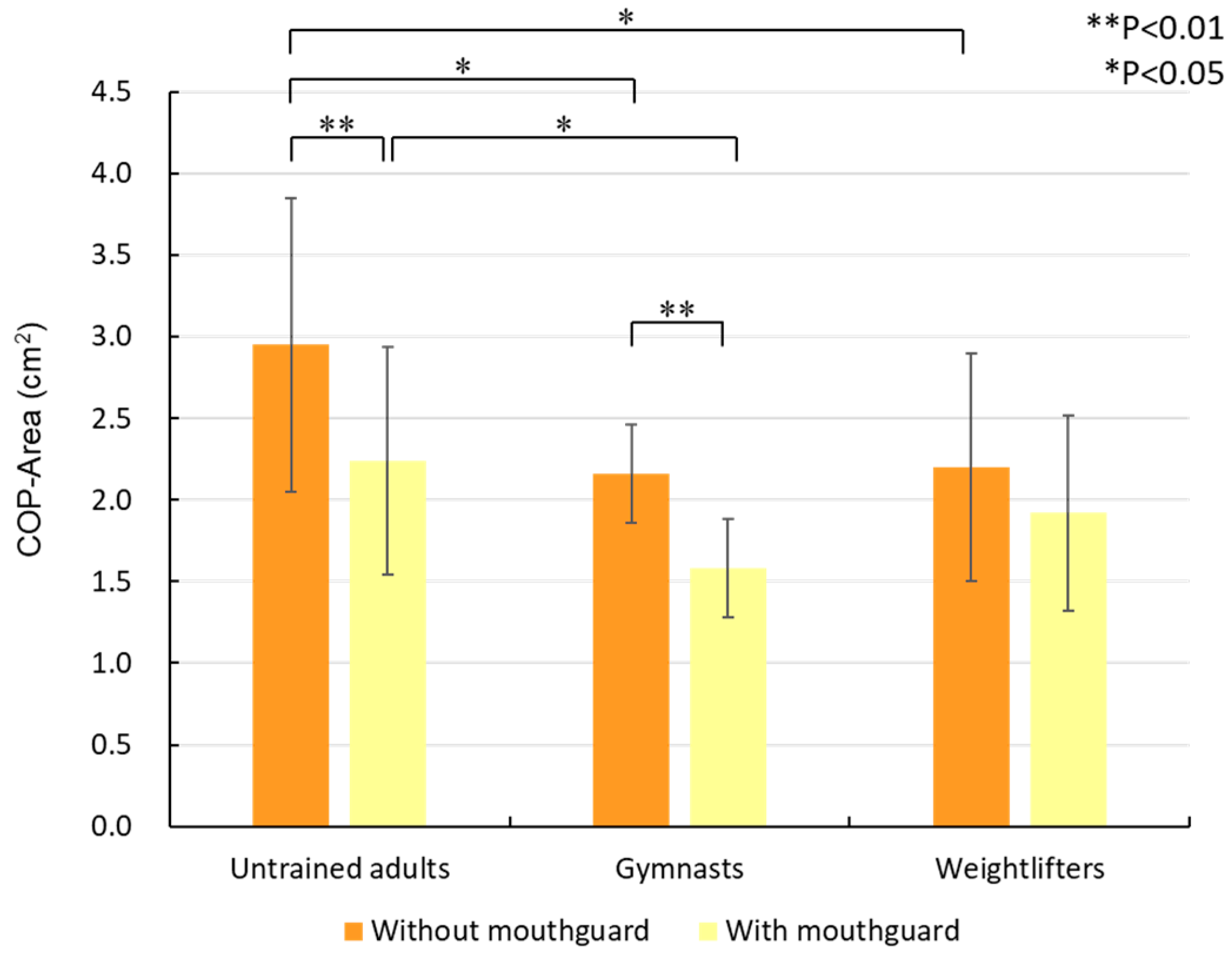
Figure 6 shows the difference in COP-Area among participants and between mouthguard conditions. Significant differences were observed between untrained adults and gymnasts and between untrained adults and weightlifters without a mouthguard, and the COP-Area values of gymnasts and weightlifters were lower than those of untrained adults (
p < 0.05). With a mouthguard, gymnasts showed significantly lower values than untrained adults (
p < 0.05). Differences due to the mouthguard factor were observed in untrained adults and gymnasts, with COP-Area values significantly lower with a mouthguard than without a mouthguard (
p < 0.01).
The results of the one-way analysis of variance using Welch’s test were as follows: COP-FB, p = 0.025; COP-LR, p = 0.040; and COP-Area, p = 0.186. Therefore, the differences in the reduction rate of COP-FB and COP-LR among participant groups were analyzed using the Games–Howell multiple comparison test.
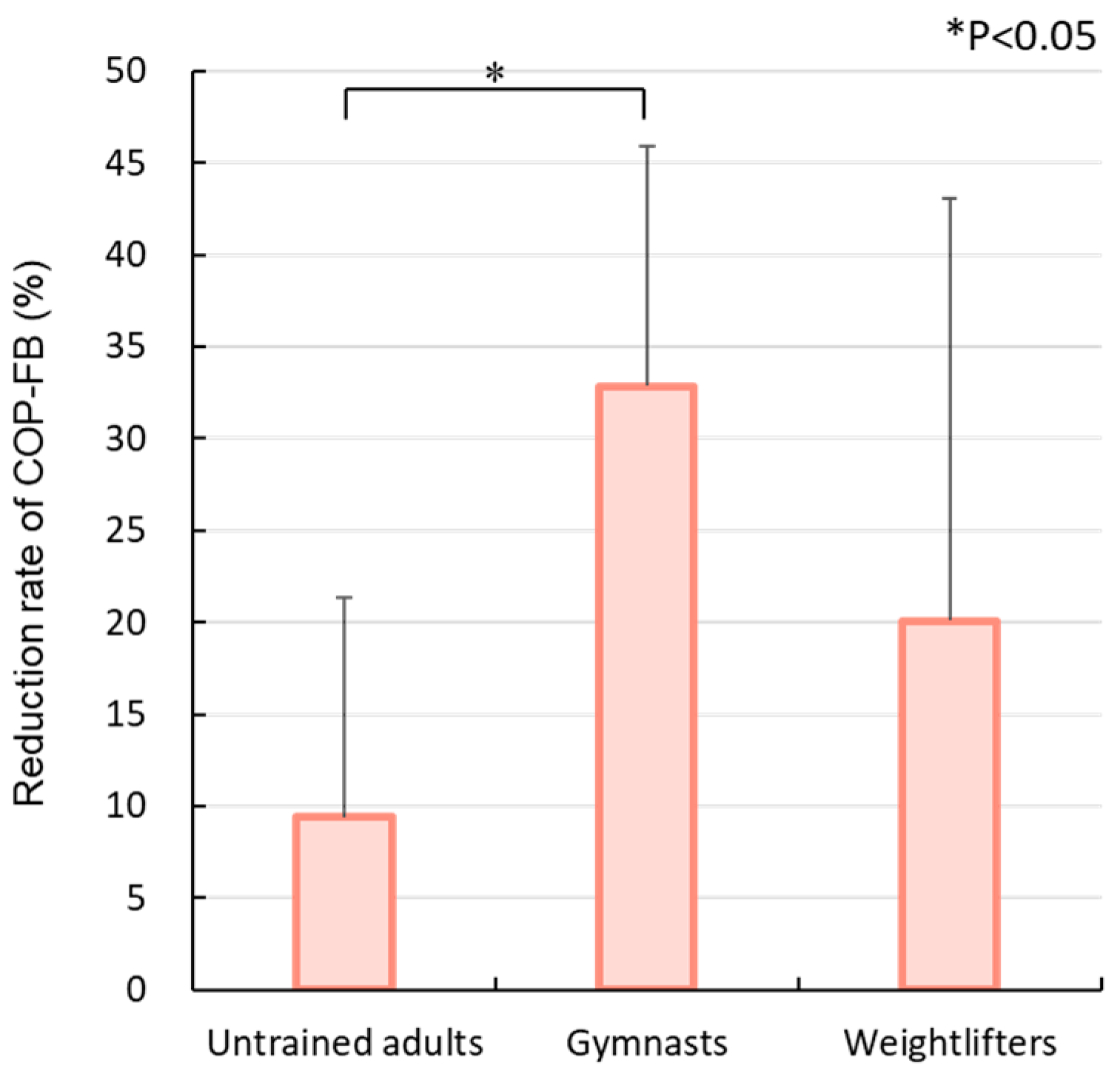
With a mouthguard, the reduction rate of COP-FB decreased in the order of gymnasts, weightlifters, and untrained adults (
Figure 7), and a significant difference was observed between gymnasts and untrained adults (
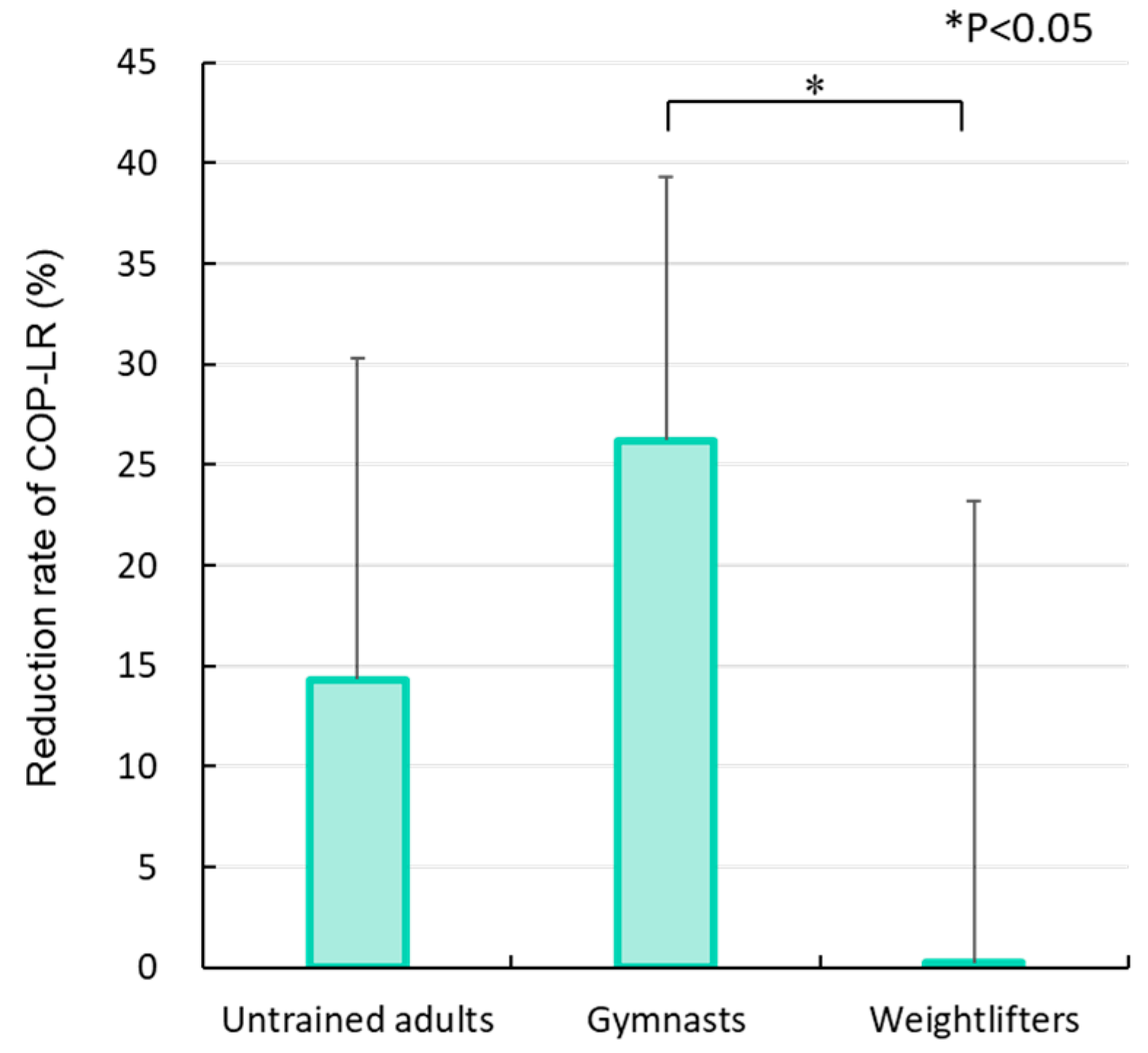
p < 0.05). For COP-LR, the reduction rate when wearing a mouthguard decreased in the order of gymnasts, untrained adults, and weightlifters (
Figure 8), and the difference between gymnasts and weightlifters was significant (
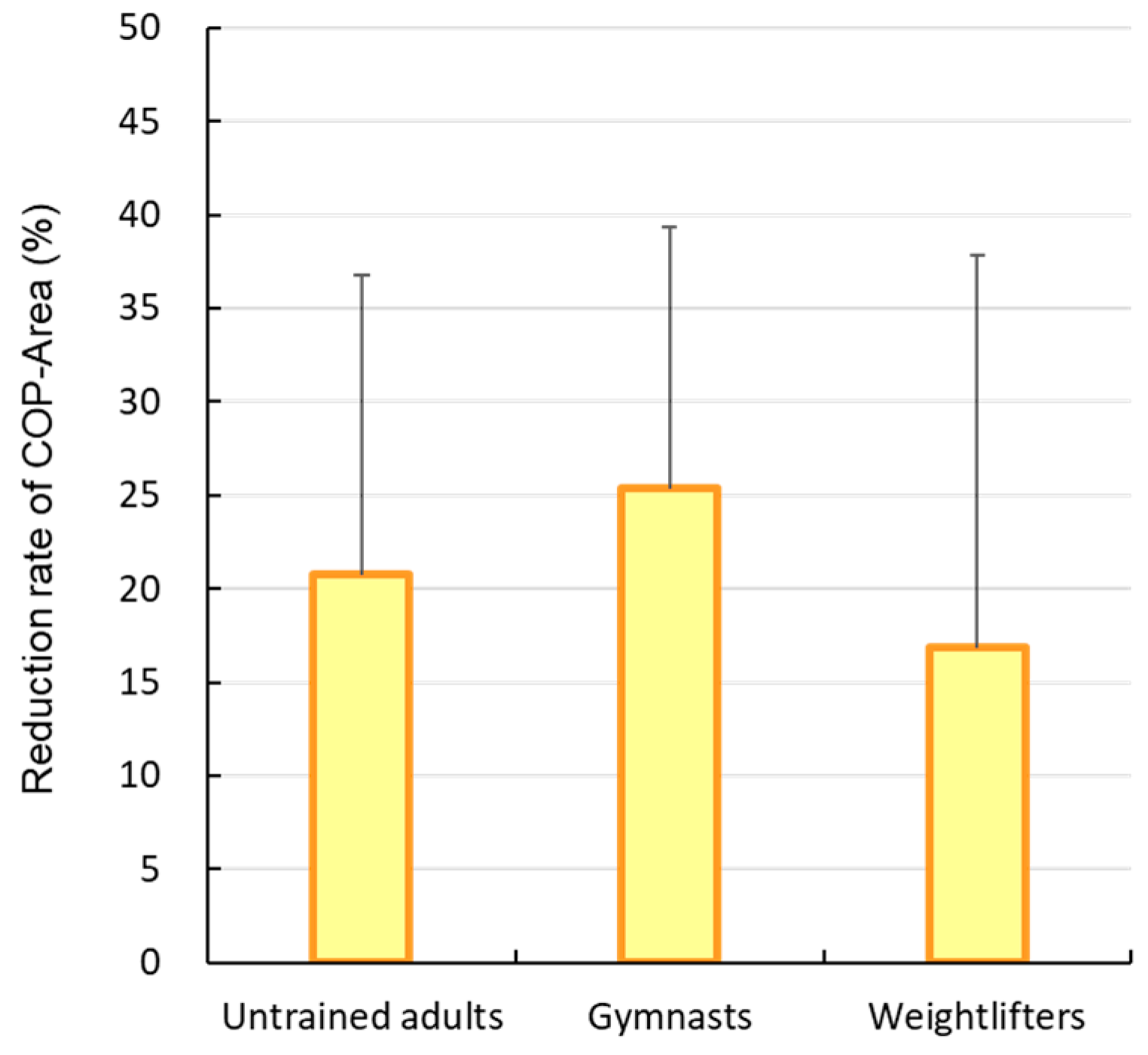
p < 0.05). The reduction rate of COP-Area when wearing a mouthguard decreased in the order of gymnasts, untrained adults, and weightlifters (
Figure 9), but no significant difference was observed.
4. Discussion
This study investigated the effects on the postural control function of wearing a mouthguard to equalize the occlusal contact state by examining differences in COP displacement among gymnasts, weightlifters, and non-athletes with and without a mouthguard. Our results indicated that COP displacement differed among participant groups and was reduced by wearing a mouthguard. In particular, the postural control function of gymnasts was higher than that of untrained adults and weightlifters. The gymnasts had a high baseline, and the reduction rate of COP displacement when wearing a mouthguard was higher in this group compared with the other groups. Therefore, the null hypothesis was rejected.
For measurement of the COG sway, the COP displacement was analyzed separately in the front-and-back and left-and-right directions because both are managed based on different control systems [
14,
23]. Front-and-back COP displacement is affected by the stiffness of the ankle joint. Left-and-right COP displacement, on the other hand, is influenced by ankle varus/valgus and hip joint varus/abduction, and there is a tendency for less sway compared with the front-to-back direction [
24,
25]. In addition, postural muscles are responsible for standing control against forward-leaning posture and are increased by the sensitivity of the somatosensory input in postural control [
25,
26]. Postural stability is affected by the fascial chain; the masseter muscle, which maintains clenching, belongs to the deep front line, and the sternocleidomastoid muscle belongs to the lateral line, superficial front line, and superficial back line, with both contributing to body stabilization [
27]. Although visual input is the most important factor in posture localization [
28], it is less important for maintaining standing posture [
3]. Therefore, the visual condition in this study was set as closed eyes.
The threshold of sensory input due to postural sway depends on the sway speed; sensory thresholds at static or slow sway have the lowest proprioception [
26], and the importance of sensory input differs according to the characteristics of the sport [
3,
11,
16,
17,
18,
19,
29,
30]. Based on the above, the present study targeted untrained adults who do not exercise regularly, gymnasts who emphasize balance training, and weightlifters who mainly do strength training. Then, the difference in COP displacement due to the difference in the occlusal contact state (i.e., somatosensory input) was investigated. Participants with a difference of 15% or more in the occlusal force between the left and right sides were excluded to avoid the possible difficulty in comparison among participants or between mouthguard conditions due to a large bias in COP displacement under the “without mouthguard” condition.
Differences in COP displacement among participants were observed in all evaluation indices, with the COP displacement of gymnasts tending to be smaller than that of untrained adults and weightlifters. It has been reported that gymnasts, for whom postural training is emphasized, have a superior postural control function compared with other athletes and that this function is particularly evident under conditions that match the training environment [
11]. The gymnasts targeted in this study had trained to maintain a posture in which the shoulders, hip joints, knees, and lateral malleolus were in a straight line and the COG was distributed over the entire sole. The results of this study support the training effect and are consistent with previous research [
11]. On the other hand, the COP displacement of weightlifters was significantly smaller than that of untrained adults, but the difference for gymnasts was not as large, except for COP-FB. The difference between untrained adults and weightlifters in this study may be due to the fact that body sway tends to be smaller with a greater body weight [
9]. In addition, because the sway of the COG might be greater in more muscular or stronger athletes than in athletes who focus on balance, there was a tendency for COP displacement to be greater in the weightlifters than in the gymnasts. Furthermore, there may be an effect of foot position during measurement. The foot position during the gravity center fluctuation test significantly affects the measured values, and the closed foot position is able to detect minute changes in the COG [
31]. In this study, measurements were taken in the closed foot position; however, this position did not match the practice environment for weightlifters, and the COP displacement may have been increased. It is thus necessary to verify the effect of foot position on the COP displacement of weightlifters. The most significant between-participant differences were detected in COP-FB because the COP displacement is greater in the front-and-back direction than in the left-and-right direction [
24,
25].
Differences in COP displacement from wearing a mouthguard were significant under all conditions, except for COP-LR and COP-Area in weightlifters, and COP displacement was smaller when wearing a mouthguard. These results demonstrated that equalization of the occlusal contact state by wearing a mouthguard reduces the COP displacement and that the effect on the postural control function depends on the participating groups. It has been clarified that people with a good occlusal contact state have less COG sway and that equalization of occlusal contact with an oral appliance reduces the sway [
5,
6,
12]; the present results also showed similar findings. Weightlifters’ occlusal contact area may have influenced the lack of a significant difference in COP-LR and COP-Area due to wearing a mouthguard. The participants in this study were selected based on the difference in the occlusal force between the left and right sides, but weightlifters included those with significant tooth wear due to the characteristics of their sport. Because participants with significant tooth wear and large occlusal contact areas tended to have a small difference in occlusal contact areas between the left and right sides, it is possible that there was not much difference in their occlusal contact state when wearing a mouthguard. In future work, it will be necessary to focus on the distribution of the occlusal contact area and to refine the selection of participants.
Furthermore, gymnasts showed the greatest reduction in COP displacement when wearing mouthguards. They showed significantly higher reduction rates in COP-FB compared with untrained adults and in COP-LR compared with weightlifters. This study revealed that gymnasts, the group with the best postural control without a mouthguard, showed the greatest reduction in COP displacement when wearing a mouthguard. In other words, it was suggested that ensuring a well-balanced occlusal contact state in gymnasts with excellent postural control function could lead to further improvement. Furthermore, the stabilization of occlusion by wearing a mouthguard also contributed to the improvement of postural control function in weightlifters, who mainly engage in strength training, as well as in non-athletes.
The results of this study indicate that equalization of occlusal contact contributes to the improvement of postural control function, suggesting that oral health management, including the wearing of mouthguards, may lead to the prevention and reduction of sports injuries as well as the improvement of athletic performance. This is because posture frequently changes while engaged in sports activities, and smooth movements are achieved through hierarchical reflexes and postural control [
3]. If these reactions are not timed correctly and balance is lost, it can lead to serious sports injuries [
6]. Meanwhile, it has been reported that a higher number of missing teeth is associated with a higher risk of falling in the elderly [
32]. Therefore, the impact of occlusal contact on postural stability is important even in daily life, and this study supports the idea that oral health management contributes to the improvement of quality of life.




 ,
, 









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}