
Evaluation of the Differences in the Stability of Alveolar Bone around Dental Implant and Implant Failure between Platform Matching and Platform Switching: A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Eligibility Criteria
2.2. Information Sources and Search Strategy
2.3. Study Selection and Data Extraction
2.4. Risk-of-Bias Assessment
2.5. Data Synthesis and Analysis
3. Results
3.1. Study Selection and Data Extraction
3.2. Risk of Bias Assessment
3.3. Meta-Analysis
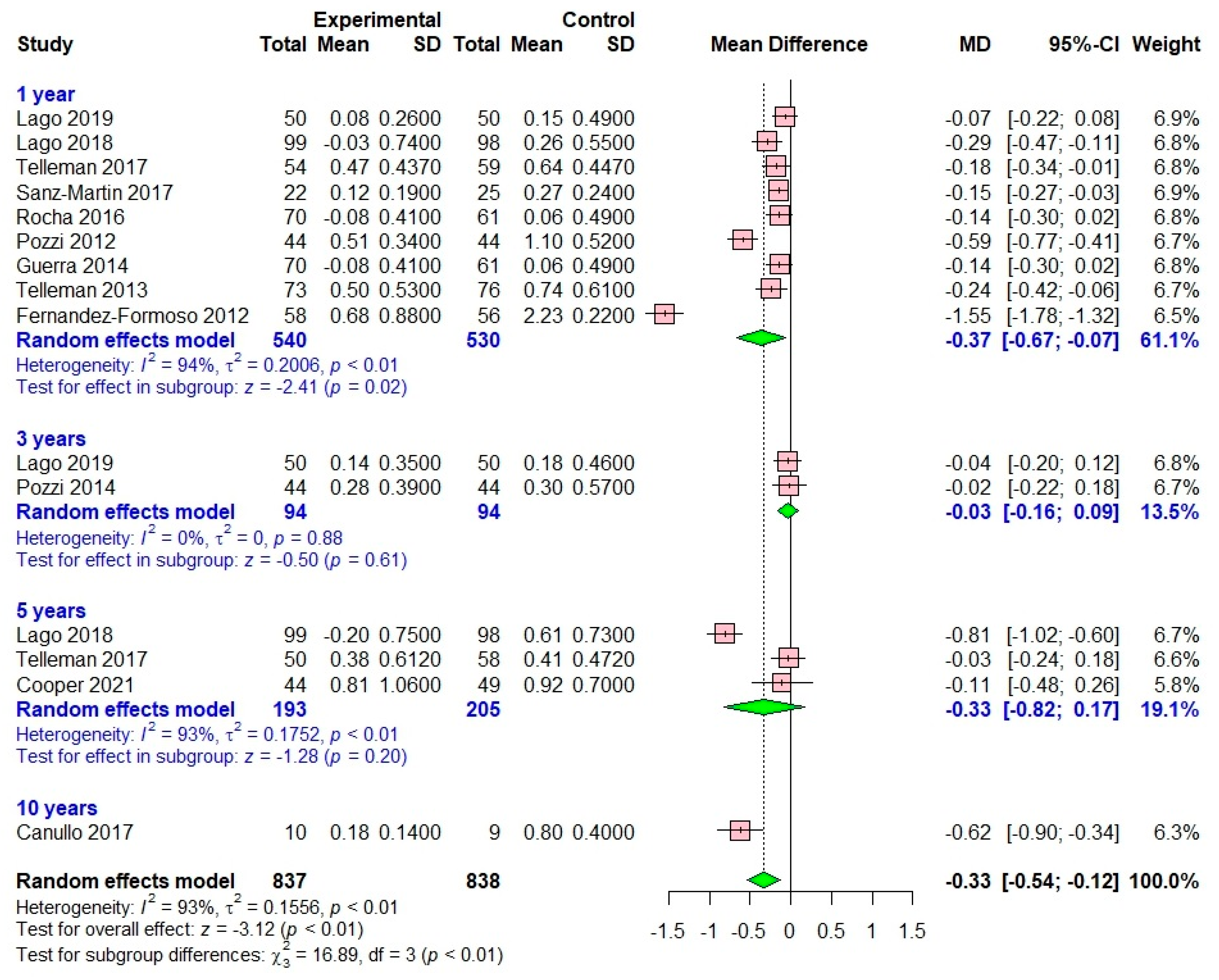
3.3.1. Marginal Bone Loss
One Year after Loading
Three Years after Loading
Five Years after Loading
Ten Years after Loading
3.3.2. Implant Failure
3.3.3. Sensitivity Meta-Analysis
3.3.4. Publication Bias Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lazzara, R.J.; Porter, S.S. Platform switching: A new concept in implant dentistry for controlling postrestorative crestal bone levels. Int. J. Periodontics Restor. Dent. 2006, 26, 9–17. [Google Scholar]
- Nayak, R.; Devanna, R.; Dharamsi, A.M.; Shetty, J.; Mokashi, R.; Malhotra, S. Crestal Bone Loss around Dental Implants: Platform Switching vs Platform Matching—A Retrospective Study. J. Contemp. Dent. Pract. 2018, 19, 574–578. [Google Scholar] [PubMed]
- Romanos, G.E. The implant-abutment connection and its impact on prevention of peri-implant diseases and crestal bone stability—An academic and clinical evaluation of the literature. Front. Oral Maxillofac. Med. 2021, 5. [Google Scholar] [CrossRef]
- Macedo, J.P.; Pereira, J.; Vahey, B.R.; Henriques, B.; Benfatti, C.A.M.; Magini, R.S.; López-López, J.; Souza, J.C.M. Morse taper dental implants and platform switching: The new paradigm in oral implantology. Eur. J. Dent. 2016, 10, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Khorshidi, H.; Raoofi, S.; Moattari, A.; Bagheri, A.; Kalantari, M.H. In Vitro Evaluation of Bacterial Leakage at Implant-Abutment Connection: An 11-Degree Morse Taper Compared to a Butt Joint Connection. Int. J. Biomater. 2016, 2016, 8527849. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.C.; Kan, J.Y.; Rungcharassaeng, K.; Roe, P.; Lozada, J.L. Marginal bone response of implants with platform switching and non-platform switching abutments in posterior healed sites: A 1-year prospective study. Clin. Oral Implant. Res. 2015, 26, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Uraz, A.; Isler, S.C.; Cula, S.; Tunc, S.; Yalim, M.; Cetiner, D. Platform-switched implants vs platform-matched implants placed in different implant-abutment interface positions: A prospective randomized clinical and microbiological study. Clin. Implant. Dent. Relat. Res. 2020, 22, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Stacchi, C.; Lamazza, L.; Rapani, A.; Troiano, G.; Messina, M.; Antonelli, A.; Giudice, A.; Lombardi, T. Marginal bone changes around platform-switched conical connection implants placed 1 or 2 mm subcrestally: A multicenter crossover randomized controlled trial. Clin. Implant. Dent. Relat. Res. 2023, 25, 398–408. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Yang, J.; Chen, K.; Li, Z.; Chen, Z.; Huang, B. Clinical and radiographic results of crestal vs. subcrestal placement of implants in posterior areas: A split-mouth randomized controlled clinical trial. Clin. Implant. Dent. Relat. Res. 2023, 25, 948–959. [Google Scholar] [CrossRef]
- Aimetti, M.; Ferrarotti, F.; Mariani, G.M.; Ghelardoni, C.; Romano, F. Soft tissue and crestal bone changes around implants with platform-switched abutments placed nonsubmerged at subcrestal position: A 2-year clinical and radiographic evaluation. Int. J. Oral Maxillofac. Implant. 2015, 30, 1369–1377. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.F.; Reside, G.; DeKok, I.; Stanford, C.; Barwacz, C.; Feine, J.; Nader, S.; Scheyer, T.; McGuire, M. A 5-Year Esthetic RCT Assessment of Anterior Maxillary Single-Tooth Implants with Different Abutment Interfaces. Int. J. Oral Maxillofac. Implant. 2021, 36, 165–176. [Google Scholar] [CrossRef] [PubMed]
- Lago, L.; da Silva, L.; Martinez-Silva, I.; Rilo, B. Radiographic Assessment of Crestal Bone Loss in Tissue-Level Implants Restored by Platform Matching Compared with Bone-Level Implants Restored by Platform Switching: A Randomized, Controlled, Split-Mouth Trial with 3-Year Follow-Up. Int. J. Oral Maxillofac. Implant. 2019, 34, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Lago, L.; da Silva, L.; Martinez-Silva, I.; Rilo, B. Crestal Bone Level Around Tissue-Level Implants Restored with Platform Matching and Bone-Level Implants Restored with Platform Switching: A 5-Year Randomized Controlled Trial. Int. J. Oral Maxillofac. Implant. 2018, 33, 448–456. [Google Scholar] [CrossRef]
- Telleman, G.; Raghoebar, G.M.; Vissink, A.; Meijer, H.J. Impact of platform switching on inter-proximal bone levels around 8.5 mm implants in the posterior region; 5-year results from a randomized clinical trial. J. Clin. Periodontol. 2017, 44, 326–336. [Google Scholar] [CrossRef]
- Sanz-Martín, I.; Sanz-Sánchez, I.; Noguerol, F.; Cok, S.; Ortiz-Vigón, A.; Sanz, M. Randomized controlled clinical trial comparing two dental implants with different neck configurations. Clin. Implant. Dent. Relat. Res. 2017, 19, 512–522. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Caneva, M.; Tallarico, M. Ten-year hard and soft tissue results of a pilot double-blinded randomized controlled trial on immediately loaded post-extractive implants using platform-switching concept. Clin. Oral Implant. Res. 2017, 28, 1195–1203. [Google Scholar] [CrossRef] [PubMed]
- Rocha, S.; Wagner, W.; Wiltfang, J.; Nicolau, P.; Moergel, M.; Messias, A.; Behrens, E.; Guerra, F. Effect of platform switching on crestal bone levels around implants in the posterior mandible: 3 years results from a multicentre randomized clinical trial. J. Clin. Periodontol. 2016, 43, 374–382. [Google Scholar] [CrossRef]
- Pozzi, A.; Tallarico, M.; Moy, P.K. Three-year post-loading results of a randomised, controlled, split-mouth trial comparing implants with different prosthetic interfaces and design in partially posterior edentulous mandibles. Eur. J. Oral Implantol. 2014, 7, 47–61. [Google Scholar]
- Guerra, F.; Wagner, W.; Wiltfang, J.; Rocha, S.; Moergel, M.; Behrens, E.; Nicolau, P. Platform switch versus platform match in the posterior mandible–1-year results of a multicentre randomized clinical trial. J. Clin. Periodontol. 2014, 41, 521–529. [Google Scholar] [CrossRef]
- Telleman, G.; Meijer, H.J.; Vissink, A.; Raghoebar, G.M. Short implants with a nanometer-sized CaP surface provided with either a platform-switched or platform-matched abutment connection in the posterior region: A randomized clinical trial. Clin. Oral Implant. Res. 2013, 24, 1316–1324. [Google Scholar] [CrossRef] [PubMed]
- Pozzi, A.; Agliardi, E.; Tallarico, M.; Barlattani, A. Clinical and radiological outcomes of two implants with different prosthetic interfaces and neck configurations: Randomized, controlled, split-mouth clinical trial. Clin. Implant. Dent. Relat. Res. 2012, 16, 96–106. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Formoso, N.; Rilo, B.; Mora, M.J.; Martínez-Silva, I.; Díaz-Afonso, A.M. Radiographic evaluation of marginal bone maintenance around tissue level implant and bone level implant: A randomised controlled trial. A 1-year follow-up. J. Oral Rehabil. 2012, 39, 830–837. [Google Scholar] [CrossRef] [PubMed]
- Vinhas, A.S.; Aroso, C.; Salazar, F.; López-Jarana, P.; Ríos-Santos, J.V.; Herrero-Climent, M. Review of the Mechanical Behavior of Different Implant-Abutment Connections. Int. J. Environ. Res. Public Health 2020, 17, 8685. [Google Scholar] [CrossRef] [PubMed]
- Vigolo, P.; Fonzi, F.; Majzoub, Z.; Cordioli, G. Evaluation of gold-machined UCLA-type abutments and CAD/CAM titanium abutments with hexagonal external connection and with internal connection. Int. J. Oral Maxillofac. Implant. 2008, 23, 247–252. [Google Scholar]
- Ceruso, F.M.; Barnaba, P.; Mazzoleni, S.; Ottria, L.; Gargari, M.; Zuccon, A.; Di Fiore, A. Implant-abutment connections on single crowns: A systematic review. ORAL Implantol. 2017, 10, 349–353. [Google Scholar] [CrossRef] [PubMed]
- Weng, D.; Nagata, M.J.; Leite, C.M.; de Melo, L.G.; Bosco, A.F. Influence of microgap location and configuration on radiographic bone loss in nonsubmerged implants: An experimental study in dogs. Int. J. Prosthodont. 2011, 24, 445–452. [Google Scholar] [PubMed]
- Broggini, N.; McManus, L.M.; Hermann, J.S.; Medina, R.; Schenk, R.K.; Buser, D.; Cochran, D. Peri-implant inflammation defined by the implant-abutment interface. J. Dent. Res. 2006, 85, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Vigolo, P.; Mutinelli, S.; Stellini, E.; Di Fiore, A. Influence of Platform-Switched Restoration on Bone Resorption in Patients Treated with Wide-Diameter, External-Hex-Connection Dental Implants: A 10-Year Follow-up Study. Int. J. Oral Maxillofac. Implant. 2023, 38, 46–52. [Google Scholar] [CrossRef]
- Afazal, M.; Gupta, S.; Tevatia, A.; Afreen, S.; Chanda, A. Computational Investigation of Dental Implant Restoration Using Platform-Switched and -Matched Configurations. Computation 2023, 11, 79. [Google Scholar] [CrossRef]
- Liu, S.; Tang, C.; Yu, J.; Dai, W.; Bao, Y.; Hu, D. The effect of platform switching on stress distribution in implants and periimplant bone studied by nonlinear finite element analysis. J. Prosthet. Dent. 2014, 112, 1111–1118. [Google Scholar] [CrossRef]
- Salama, A.A.; Katamish, H.A.; Halim, C.H.; Farid, K.A. The mechanical complications of platform switching connection on implant supported restorations: A systematic review and meta-analysis. J. Osseointegr. 2019, 11, 3. [Google Scholar]
- Hsu, Y.T.; Chan, H.L.; Rudek, I.; Bashutski, J.; Oh, W.S.; Wang, H.L.; Oh, T.-J. Comparison of Clinical and Radiographic Outcomes of Platform-Switched Implants with a Rough Collar and Platform-Matched Implants with a Smooth Collar: A 1-Year Randomized Clinical Trial. Int. J. Oral Maxillofac. Implant. 2016, 31, 382–390. [Google Scholar] [CrossRef]
- Enkling, N.; Jöhren, P.; Katsoulis, J.; Bayer, S.; Jervøe-Storm, P.M.; Mericske-Stern, R.; Jepsen, S. Influence of platform switching on bone-level alterations: A three-year randomized clinical trial. J. Dent. Res. 2013, 92, 139s–145s. [Google Scholar] [CrossRef] [PubMed]
- Pieri, F.; Aldini, N.N.; Marchetti, C.; Corinaldesi, G. Influence of implant-abutment interface design on bone and soft tissue levels around immediately placed and restored single-tooth implants: A randomized controlled clinical trial. Int. J. Oral Maxillofac. Implant. 2011, 26, 169–178. [Google Scholar]
- Mangalvedhekar, M.; Manas, A.; Jyothirmayee, K.; Tenglikar, P.; Das, A.C. Assessment of Clinical and Radiological Outcome of Implant with Two Different Connections Con iguration: A Controlled Trial. J. Pharm. Bioallied Sci. 2022, 14, S974–S976. [Google Scholar]
- Messias, A.; Rocha, S.; Wagner, W.; Wiltfang, J.; Moergel, M.; Behrens, E.; Nicolau, P.; Guerra, F. Peri-implant marginal bone loss reduction with platform-switching components: 5-Year post-loading results of an equivalence randomized clinical trial. J. Clin. Periodontol. 2019, 46, 678–687. [Google Scholar] [CrossRef]
- Cooper, L.F.; Reside, G.; Stanford, C.; Barwacz, C.; Feine, J.; Nader, S.A.; Scheyer, T.; McGuire, M. Three-Year Prospective Randomized Comparative Assessment of Anterior Maxillary Single Implants with Different Abutment Interfaces. Int. J. Oral Maxillofac. Implant. 2019, 34, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Vandeweghe, S.; De Bruyn, H. A within-implant comparison to evaluate the concept of platform switching: A randomised controlled trial. Eur. J. Oral Implantol. 2012, 5, 253–262. [Google Scholar]
- Cooper, L.F.; Reside, G.; Stanford, C.; Barwacz, C.; Feine, J.; Abi Nader, S.; Scheyer, E.; McGuire, M. A multicenter randomized comparative trial of implants with different abutment interfaces to replace anterior maxillary single teeth. Int. J. Oral Maxillofac. Implant. 2015, 30, 622–632. [Google Scholar] [CrossRef]
- Enkling, N.; Jöhren, P.; Klimberg, V.; Bayer, S.; Mericske-Stern, R.; Jepsen, S. Effect of platform switching on peri-implant bone levels: A randomized clinical trial. Clin. Oral Implant. Res. 2011, 22, 1185–1192. [Google Scholar] [CrossRef] [PubMed]
- Lowy, J.; Kwon, H.S.; Patel, A.; Greenwell, H.; Hill, M.; Katwal, D.; Rademacher, A.; Mendoza, J. The Effect of Platform-Switching Plus Laser Grooving on Peri-implant Hard and Soft Tissue Level: A Randomized, Controlled, Blinded Clinical Trial. Int. J. Periodontics Restor. Dent. 2019, 39, 669–674. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Maghaireh, H.; Pistilli, R.; Grusovin, M.G.; Lee, S.T.; Trullenque-Eriksson, A.; Gualini, F. Dental implants with internal versus external connections: 5-year post-loading results from a pragmatic multicenter randomised controlled trial. Eur. J. Oral Implantol. 2016, 9 (Suppl. S1), 129–141. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Maghaireh, H.; Pistilli, R.; Grusovin, M.G.; Lee, S.T.; Gualini, F.; Yoo, J.; Buti, J. Dental implants with internal versus external connections: 1-year post-loading results from a pragmatic multicenter randomised controlled trial. Eur. J. Oral Implantol. 2015, 8, 331–344. [Google Scholar] [CrossRef] [PubMed]
- Meloni, S.M.; Jovanovic, S.A.; Lolli, F.M.; Pisano, M.; De Riu, G.; De Riu, N.; Lugliè, P.F.; Tullio, A. Platform switching vs regular platform implants: Nine-month post-loading results from a randomised controlled trial. Eur. J. Oral Implantol. 2014, 7, 257–265. [Google Scholar] [PubMed]
- Crespi, R.; Capparè, P.; Gherlone, E. Radiographic evaluation of marginal bone levels around platform-switched and non-platform-switched implants used in an immediate loading protocol. Int. J. Oral Maxillofac. Implant. 2009, 24, 920–926. [Google Scholar]
- Canullo, L.; Goglia, G.; Iurlaro, G.; Iannello, G. Short-term bone level observations associated with platform switching in immediately placed and restored single maxillary implants: A preliminary report. Int. J. Prosthodont. 2009, 22, 277–282. [Google Scholar] [PubMed]
- Díaz-Sánchez, R.M.; Delgado-Muñoz, J.M.; Serrera-Figallo, M.A.; González-Martín, M.I.; Torres-Lagares, D.; Gutiérrez-Pérez, J.L. Analysis of marginal bone loss and implant stability quotient by resonance frequency analysis in different osteointegrated implant systems. Randomized prospective clinical trial. Med. Oral Patol. Oral Cir. Bucal 2019, 24, e260–e264. [Google Scholar] [CrossRef] [PubMed]
- Spies, B.C.; Bateli, M.; Ben Rahal, G.; Christmann, M.; Vach, K.; Kohal, R.J. Does Oral Implant Design Affect Marginal Bone Loss? Results of a Parallel-Group Randomized Controlled Equivalence Trial. BioMed Res. Int. 2018, 2018, 8436437. [Google Scholar] [CrossRef]
- Glibert, M.; Vervaeke, S.; Jacquet, W.; Vermeersch, K.; Östman, P.O.; De Bruyn, H. A randomized controlled clinical trial to assess crestal bone remodeling of four different implant designs. Clin. Implant. Dent. Relat. Res. 2018, 20, 455–462. [Google Scholar] [CrossRef]
- Flores-Guillen, J.; Álvarez-Novoa, C.; Barbieri, G.; Martín, C.; Sanz, M. Five-year outcomes of a randomized clinical trial comparing bone-level implants with either submerged or transmucosal healing. J. Clin. Periodontol. 2018, 45, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Pessoa, R.S.; Sousa, R.M.; Pereira, L.M.; Neves, F.D.; Bezerra, F.J.; Jaecques, S.V.; Spin-Neto, R. Bone Remodeling Around Implants with External Hexagon and Morse-Taper Connections: A Randomized, Controlled, Split-Mouth, Clinical Trial. Clin. Implant. Dent. Relat. Res. 2017, 19, 97–110. [Google Scholar] [CrossRef] [PubMed]
- Palaska, I.; Tsaousoglou, P.; Vouros, I.; Konstantinidis, A.; Menexes, G. Influence of placement depth and abutment connection pattern on bone remodeling around 1-stage implants: A prospective randomized controlled clinical trial. Clin. Oral Implant. Res. 2016, 27, e47–e56. [Google Scholar] [CrossRef] [PubMed]
- Van Nimwegen, W.G.; Raghoebar, G.M.; Stellingsma, K.; Tymstra, N.; Vissink, A.; Meijer, H.J. Treatment Outcome of Two Adjacent Implant-Supported Restorations with Different Implant Platform Designs in the Esthetic Region: A Five-Year Randomized Clinical Trial. Int. J. Prosthodont. 2015, 28, 490–498. [Google Scholar] [CrossRef] [PubMed]
- De Angelis, N.; Nevins, M.L.; Camelo, M.C.; Ono, Y.; Campailla, M.; Benedicenti, S. Platform switching versus conventional technique: A randomized controlled clinical trial. Int. J. Periodontics Restor. Dent. 2014, 34 (Suppl. S3), s75–s79. [Google Scholar]
- Telleman, G.; Raghoebar, G.M.; Vissink, A.; Meijer, H.J. Impact of platform switching on inter-proximal bone levels around short implants in the posterior region; 1-year results from a randomized clinical trial. J. Clin. Periodontol. 2012, 39, 688–697. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Rosa, J.C.; Pinto, V.S.; Francischone, C.E.; Götz, W. Inward-inclined implant platform for the amplified platform-switching concept: 18-month follow-up report of a prospective randomized matched-pair controlled trial. Int. J. Oral Maxillofac. Implant. 2012, 27, 927–934. [Google Scholar]
- Tymstra, N.; Raghoebar, G.M.; Vissink, A.; Den Hartog, L.; Stellingsma, K.; Meijer, H.J. Treatment outcome of two adjacent implant crowns with different implant platform designs in the aesthetic zone: A 1-year randomized clinical trial. J. Clin. Periodontol. 2011, 38, 74–85. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Iannello, G.; Götz, W. The influence of individual bone patterns on peri-implant bone loss: Preliminary report from a 3-year randomized clinical and histologic trial in patients treated with implants restored with matching-diameter abutments or the platform-switching concept. Int. J. Oral Maxillofac. Implant. 2011, 26, 618–630. [Google Scholar]
- Canullo, L.; Fedele, G.R.; Iannello, G.; Jepsen, S. Platform switching and marginal bone-level alterations: The results of a randomized-controlled trial. Clin. Oral Implant. Res. 2010, 21, 115–121. [Google Scholar] [CrossRef]
- Prosper, L.; Redaelli, S.; Pasi, M.; Zarone, F.; Radaelli, G.; Gherlone, E.F. A randomized prospective multicenter trial evaluating the platform-switching technique for the prevention of postrestorative crestal bone loss. Int. J. Oral Maxillofac. Implant. 2009, 24, 299–308. [Google Scholar]
- Fickl, S.; Zuhr, O.; Stein, J.M.; Hürzeler, M.B. Peri-implant bone level around implants with platform-switched abutments. Int. J. Oral Maxillofac. Implant. 2010, 25, 577–581. [Google Scholar]
- Vigolo, P.; Givani, A. Platform-switched restorations on wide-diameter implants: A 5-year clinical prospective study. Int. J. Oral Maxillofac. Implant. 2009, 24, 103–109. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Year/Nationality | No. of Patients/Total No. of Implants | Follow-Up Time (Range) | History of Periodontal Disease | Smoking Habit | Implant System | ITI Classification | Bone Grafting | Healing Period/Loading | Implant Diameter/Implant Length | Implant Connection Type | Implant Sites | Implant Failure | Success Rate (%) | Marginal Bone Loss (Mean ± SD, mm) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cooper 2021/USA [12] | 141/141 | 5 yrs | Not explicitly mentioned | None | OsseoSpeed TX (conical interface), NobelSpeedy (flat-to-flat interface), and NanoTite Certain PREVAIL (PS interface) | delayed | None | Immediate provisionalization | Not explicitly mentioned | Conical (Internal hex), flat-to-flat (external hex), and PS (internal hex) interfaces | Mx | 0 conical, 8 flat-to-flat, 6 PS | Conical: 100%; Flat-to-flat: 83.7%; PS: 86.4% | Conical: −0.16 ± 0.45; Flat-to-flat: −0.92 ± 0.70; PS: −0.81 ± 1.06 |
| Lago 2019/Spain [13] | 35/100 | 3 yrs | Not explicitly mentioned | ≤10 cigarettes/day | Straumann | delayed | None | ≥2 months post-placement | Not explicitly mentioned | Control: Tissue-level (internal hex) vs. Test: Bone-level (internal hex) | Mx/Mn | 0 | 100% | Control: 0.18 ± 0.46, Test: 0.14 ± 0.35 |
| Lago 2018/Spain [14] | 100/202 | 5 yrs | Not explicitly mentioned | None | Straumann | delayed | None | ≥2 months post-placement | Diameter | Control: Tissue-level (internal hex) vs. Test: Bone-level (external hex) | Mx/Mn | 2 in control, 3 in test | Implied as 98% for control and 96.1% for test | Control: 0.61 ± 0.73, Test: −0.20 ± 0.75 |
| PM: 4.1, 4.8 | ||||||||||||||
| PS: 3.3, 4.1, 4.8 | ||||||||||||||
| Length | ||||||||||||||
| 8, 10, 12 | ||||||||||||||
| Telleman 2017/Netherlands [15] | 80/113 | 5 yrs | Not explicitly mentioned | None | Biomet 3i, 8.5 mm length, 58 in control (PM) and 55 in test (PS) | delayed | Performed if dehiscence or fenestrations are <3 mm | Not explicitly mentioned, but assessments at 1 month, 1 year, and 5 years | Diameter | Control: PM (internal hex) vs. Test: PS (internal hex) | Mx/Mn | 2 PS implants, 0 PM implant | 96.3% survival for PS, 100% for PM | Control group 0.41 ± 0.47 mm, Test group 0.38 ± 0.61 mm |
| 4.0, 5.0 | ||||||||||||||
| Length | ||||||||||||||
| 8.5 | ||||||||||||||
| Sanz-Martin 2017/Spain [16] | 47/61 | 24 mo | Not explicitly mentioned | ≤10 cigarettes/day | Sweden & Martina Premium, TG (Transgingival) and SP (PS) implants | delayed | Performed if dehiscence or fenestrations are <3 mm | Prostheses delivered after 12 months | Diameter | Transgingival (internal hex) vs. PS (internal hex) | Mx/Mn | 4 PS implants, 2 PM implant | 92.8% survival for PS, 93.9% for PM | TG group: Loading to 12 months: −0.27 ± 0.24 mm; SP group: Loading to 12 months: −0.12 ± 0.19 mm |
| 3.8, 4.25, 5.0 | ||||||||||||||
| Length | ||||||||||||||
| 7, 8.5, 10, 11.5, 13 | ||||||||||||||
| Canullo 2017/Italy [17] | 19/19 | 10 yrs | Not explicitly mentioned | ≤10 cigarettes/day | Global Implant, Sweden & Martina, 13 mm length, 5.5 mm platform | delayed | Performed if dehiscence or fenestrations are <3 mm | Immediate loading | Diameter | PS (internal hex) vs. PM (internal hex) | Mx | 0 | 100% | Test: 0.18 ± 0.14; Control: 0.80 ± 0.40 |
| 5.5 | ||||||||||||||
| Length | ||||||||||||||
| 13 | ||||||||||||||
| Rocha 2016/Multicenter (Germany, Portugal) [18] | 63/135 | 3 yrs | Not explicitly mentioned | ≤10 cigarettes/day | CAMLOG SCREW-LINE implants, Promote plus surface | delayed | None | Conventional loading, 6–14 weeks post-placement | Diameter | PS (internal hex) vs. PM (internal hex) | Mn | 2 PS implants, 1 PM implant | 97.3% survival for PS, 97.1% for PM | PS: 0.28 ± 0.56 mm, PM: 0.68 ± 0.64 mm over 3 years |
| 3.8, 4.3, 5.0 | ||||||||||||||
| Length | ||||||||||||||
| 9, 11, 13 | ||||||||||||||
| Pozzi 2014/Multicenter (Italy, USA) [19] | 34/88 | 3 yrs | Not explicitly mentioned | ≤10 cigarettes/day | NobelActive (NA) and NobelSpeedy Groovy (NSG), Nobel Biocare | delayed | None | Not explicitly mentioned | Diameter | Internal conical connection (NA) vs. External hexagon flat-to-flat (NSG) | Mn | 0 | 100% | NA implants: 0.66 mm; NSG implants: 1.25 mm vertical bone resorption |
| PM: 4.1 | ||||||||||||||
| PS: 3.9 | ||||||||||||||
| Length | ||||||||||||||
| 8.5, 10, 11.5, 13 | ||||||||||||||
| Guerra 2014/Multicenter (Portugal, Germany) [20] | 68/146 | 1 yr | Not explicitly mentioned | ≤10 cigarettes/day | CAMLOG SCREW-LINE Implants, Promote plus surface | delayed | None | Minimum of 8 weeks transgingival healing period before definitive restorations | Diameter | PS (internal hex) vs. PM (external hex) | Mx/Mn | 2 implants lost in PS group before loading | 97.3% for PS, 100% for PM | PS: −0.69 ± 0.68 mm, PM: −0.40 ± 0.46 mm |
| 3.8, 4.3, 5.0 | ||||||||||||||
| Length | ||||||||||||||
| 9, 11, 13 | ||||||||||||||
| Telleman 2013/Netherlands [21] | 92/149 | 1 yr | Not explicitly mentioned | None | NanoTite Certain Prevail (PS) and NanoTite XP Certain (PM), Biomet 3i | delayed | None | Not explicitly mentioned | Diameter | PS (internal hex) vs. PM (external hex) | Mx/Mn | 6 in control group, 3 in test group | Control group: 92.1%, Test group: 95.9% | Control (PM) 0.74 ± 0.61 mm, Test (PS) 0.50 ± 0.53 mm |
| 4.0, 5.0 | ||||||||||||||
| Length | ||||||||||||||
| 8.5 | ||||||||||||||
| Pozzi 2012/Multicenter (Italy, USA) [22] | 34/88 | 1 yr | Not explicitly mentioned | ≤10 cigarettes/day | NobelActive (NA, internal conical connection with PS) vs. NobelSpeedy Groovy (NSG, external hexagon with flat-to-flat interface), Nobel Biocare | delayed | None | Immediate loading | Diameter | Internal conical (NA) vs. External hexagon (NSG) | Mn | 0 | 100% | PS (NA): −0.37 ± 0.48 mm, PM (NSG): −0.80 ± 0.50 mm |
| PM: 4.0 | ||||||||||||||
| PS: 4.3 | ||||||||||||||
| Length | ||||||||||||||
| 10 to 13 | ||||||||||||||
| Fernandez-Formoso 2012/Spain [23] | 51/114 | 1 yr | Not explicitly mentioned | None | Straumann implants; Standard Plus Type for control (tissue level) and Bone Level Type for test (bone level with PS) | delayed | None | Immediate loading | Diameter | Control: Tissue-level (internal hex), | Mx/Mn | 0 | 100% | Control group: 0.42 mm, Test group (PS): −0.01 mm |
| 3.3, 4.1, 4.8 | Test: Bone-level (internal hex) | |||||||||||||
| Length | ||||||||||||||
| 8 to 14 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, S.-H.; Kim, N.J.; Park, W.-J.; Park, J.-B. Evaluation of the Differences in the Stability of Alveolar Bone around Dental Implant and Implant Failure between Platform Matching and Platform Switching: A Systematic Review and Meta-Analysis. Appl. Sci. 2024, 14, 4975. https://doi.org/10.3390/app14124975
Han S-H, Kim NJ, Park W-J, Park J-B. Evaluation of the Differences in the Stability of Alveolar Bone around Dental Implant and Implant Failure between Platform Matching and Platform Switching: A Systematic Review and Meta-Analysis. Applied Sciences. 2024; 14(12):4975. https://doi.org/10.3390/app14124975
Chicago/Turabian StyleHan, Sung-Hoon, Na Jin Kim, Won-Jong Park, and Jun-Beom Park. 2024. "Evaluation of the Differences in the Stability of Alveolar Bone around Dental Implant and Implant Failure between Platform Matching and Platform Switching: A Systematic Review and Meta-Analysis" Applied Sciences 14, no. 12: 4975. https://doi.org/10.3390/app14124975
APA StyleHan, S.-H., Kim, N. J., Park, W.-J., & Park, J.-B. (2024). Evaluation of the Differences in the Stability of Alveolar Bone around Dental Implant and Implant Failure between Platform Matching and Platform Switching: A Systematic Review and Meta-Analysis. Applied Sciences, 14(12), 4975. https://doi.org/10.3390/app14124975