
Is Stretching Effective for Reducing Glenohumeral Internal Rotation Deficit? A Systematic Review and Meta-Analysis
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Search Strategy
2.3. Eligibility Criteria
2.4. Data Extraction
2.5. Methodological Quality
2.6. Data Synthesis and Analysis
2.7. Certainty of Evidence
3. Results
3.1. Characteristics of the Included Studies
3.2. Methodological Quality
3.3. Synthesis of the Results
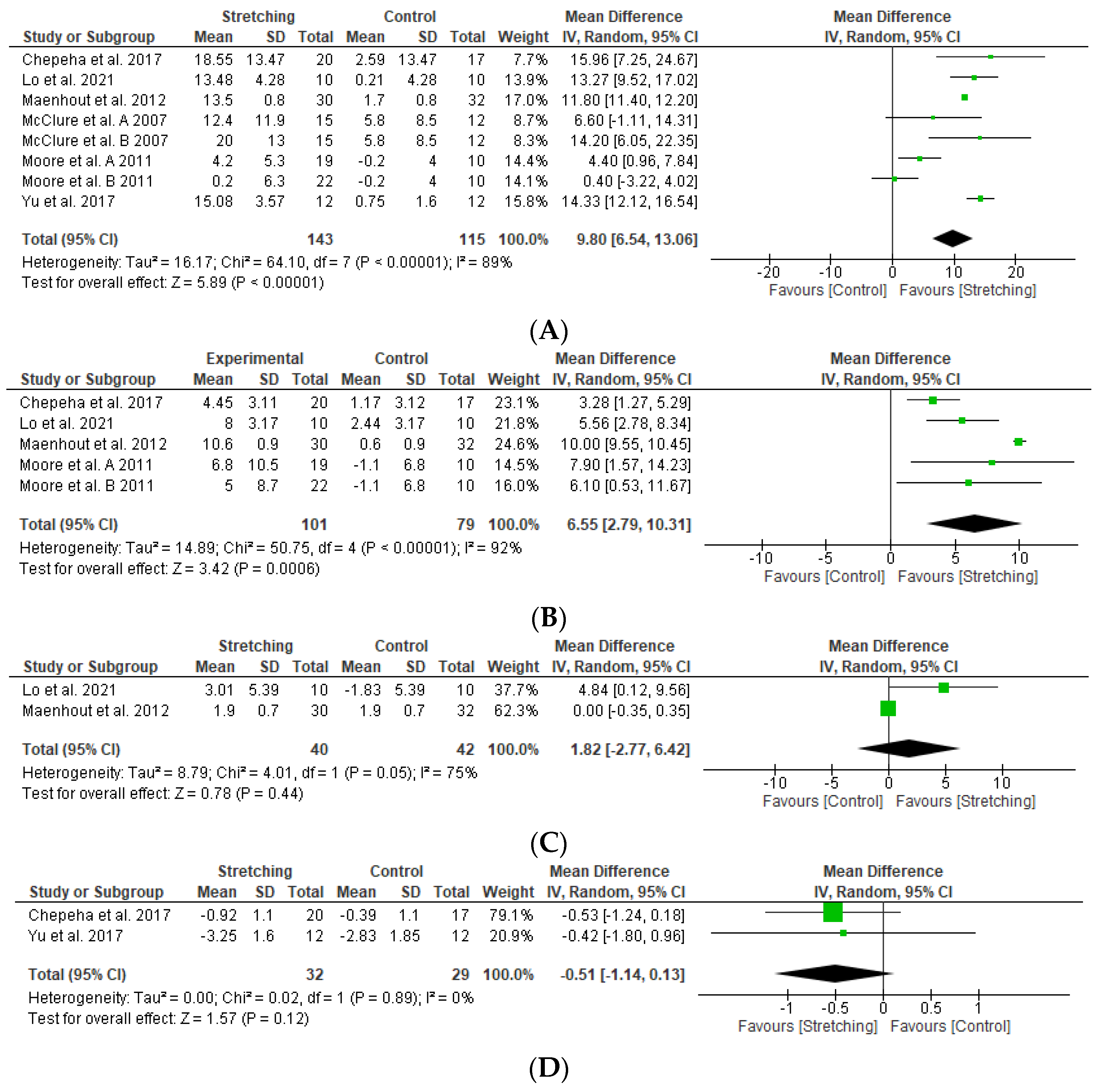
3.3.1. Stretching versus Control
3.3.2. Stretching Plus Manual Therapy versus Stretching in Isolation
3.3.3. Stretching versus Stretching
4. Discussion
4.1. Stretching versus Control
4.2. Stretching Plus Manual Therapy versus Stretching in Isolation
4.3. Stretching versus Stretching
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Search Strategy Used in Each Database
- MEDLINE
- (Athletes [MeSH] OR “Upper extremity” OR “young adult” OR handball OR volleyball OR baseball OR waterpolo OR swimmer OR overhead) AND (“rotator cuff tendinopathy” OR “rotator cuff related pain” OR “impingement syndrome” OR “shoulder impingement” OR “non-specific shoulder pain” OR “joint instability” OR “athletic injuries” OR “shoulder injuries” OR “shoulder pain” OR “GIRD” OR “glenohumeral internal rotation deficit”) AND (physical therapy modalities [MeSH] OR exercise [MeSH] OR stretching OR sleeper OR “cross-body stretch” OR “manual therapy” OR “physical therapy” OR physiotherapy) AND (pain [MeSH] OR range of motion [MeSH] OR internal rotation OR “posterior stiffness”)
- Date: 01-02-2024
- Studies retrieved: 244
- PEDro
- Athletes AND overhead
- Date: 1 February 2024
- Studies retrieved: 32
- Glenohumeral internal rotation deficit
- Date: 1 February 2024
- Studies retrieved: 12 (all duplicates)
- Cochrane Library
- (Athletes OR “Upper extremity” OR “young adult” OR handball OR volleyball OR baseball OR waterpolo OR swimmer OR overhead) AND (“rotator cuff tendinopathy” OR “rotator cuff related pain” OR “impingement syndrome” OR “shoulder impingement” OR “non-specific shoulder pain” OR “joint instability” OR “athletic injuries” OR “shoulder injuries” OR “shoulder pain” OR “GIRD” OR “glenohumeral internal rotation deficit”) AND (physical therapy modalities OR exercise OR stretching OR sleeper OR “cross-body stretch” OR “manual therapy” OR “physical therapy” OR physiotherapy) AND (pain OR range of motion OR internal rotation OR “posterior stiffness”)
- Date: 1 February 2024
- Studies retrieved: 624
- Web of Science
- ((((TS = (athletes OR handball OR volleyball OR baseball OR waterpolo OR swimmer OR overhead)) AND TS = (rotator cuff tendinopathy OR rotator cuff related pain OR impingement syndrome OR shoulder impingement OR non-specific shoulder pain OR joint instability OR athletic injuries OR shoulder injuries OR shoulder pain OR GIRD OR glenohumeral internal rotation deficit)) AND TS = (stretching OR sleeper OR cross-body stretch OR manual therapy OR physical therapy OR physiotherapy)) AND TS = (pain OR range of motion OR internal rotation OR posterior stiffness)) AND TS = (clinical trial OR randomized controlled trial OR randomized controlled clinical trial OR randomised controlled trial OR randomised controlled clinical trial)
- Date: 1 February 2024
- Studies retrieved: 268
References
- Hudson, V.J. Evaluation, Diagnosis, and Treatment of Shoulder Injuries in Athletes. Clin. Sports Med. 2010, 29, 19–32. [Google Scholar] [CrossRef]
- Seil, R.; Rupp, S.; Tempelhof, S.; Kohn, D. Sport Injuries in Team Handball. A One-Year Prospective Study of Sixteen Men’s Senior Teams of a Superior Nonprofessional Level. Am. J. Sports Med. 1998, 26, 681–687. [Google Scholar] [CrossRef]
- Ben Kibler, W.; Kuhn, J.E.; Wilk, K.; Sciascia, A.; Moore, S.; Laudner, K.; Ellenbecker, T.; Thigpen, C.; Uhl, T. The Disabled Throwing Shoulder: Spectrum of Pathology—10-Year Update. Arthrosc. J. Arthrosc. Relat. Surg. 2013, 29, 141–161. [Google Scholar] [CrossRef]
- Karcher, C.; Buchheit, M. On-Court Demands of Elite Handball, with Special Reference to Playing Positions. Sports Med. 2014, 44, 797–814. [Google Scholar] [CrossRef] [PubMed]
- Tooth, C.; Gofflot, A.; Schwartz, C.; Croisier, J.L.; Beaudart, C.; Bruyère, O.; Forthomme, B. Risk Factors of Overuse Shoulder Injuries in Overhead Athletes: A Review. Sports Health 2020, 12, 478. [Google Scholar] [CrossRef]
- Clarsen, B.; Bahr, R.; Andersson, S.H.; Munk, R.; Myklebust, G. Reduced Glenohumeral Rotation, External Rotation Weakness and Scapular Dyskinesis Are Risk Factors for Shoulder Injuries among Elite Male Handball Players: A Prospective Cohort Study. Br. J. Sports Med. 2014, 48, 1327–1333. [Google Scholar] [CrossRef]
- Wilk, K.E.; MacRina, L.C.; Fleisig, G.S.; Porterfield, R.; Simpson, C.D.; Harker, P.; Paparesta, N.; Andrews, J.R. Correlation of Glenohumeral Internal Rotation Deficit and Total Rotational Motion to Shoulder Injuries in Professional Baseball Pitchers. Am. J. Sports Med. 2011, 39, 329–335. [Google Scholar] [CrossRef]
- Almeida, G.P.L.; Silveira, P.F.; Rosseto, N.P.; Barbosa, G.; Ejnisman, B.; Cohen, M. Glenohumeral Range of Motion in Handball Players with and without Throwing-Related Shoulder Pain. J. Should. Elb. Surg. 2013, 22, 602–607. [Google Scholar] [CrossRef] [PubMed]
- Edouard, P.; Degache, F.; Oullion, R.; Plessis, J.-Y.; Gleizes-Cervera, S.; Calmels, P. Shoulder Strength Imbalances as Injury Risk in Handball. Int. J. Sports Med. 2013, 34, 654–660. [Google Scholar] [CrossRef] [PubMed]
- Edouard, P.; Degache, F.; Beguin, L.; Samozino, P.; Gresta, G.; Fayolle-Minon, I.; Farizon, F.; Calmels, P. Rotator Cuff Strength in Recurrent Anterior Shoulder Instability. J. Bone Jt. Surg. 2011, 93, 759–765. [Google Scholar] [CrossRef]
- Burkhart, S.S.; Morgan, C.D.; Kibler, W.B. The Disabled Throwing Shoulder: Spectrum of Pathology Part I: Pathoanatomy and Biomechanics. Arthrosc. J. Arthrosc. Relat. Surg. 2003, 19, 404–420. [Google Scholar] [CrossRef] [PubMed]
- Burkhart, S.S.; Morgan, C.D.; Kibler, W.B. The Disabled Throwing Shoulder: Spectrum of Pathology Part II: Evaluation and Treatment of SLAP Lesions in Throwers. Arthrosc. J. Arthrosc. Relat. Surg. 2003, 19, 531–539. [Google Scholar] [CrossRef]
- Thomas, S.J.; Swanik, C.B.; Higginson, J.S.; Kaminski, T.W.; Swanik, K.A.; Bartolozzi, A.R.; Abboud, J.A.; Nazarian, L.N. A Bilateral Comparison of Posterior Capsule Thickness and Its Correlation with Glenohumeral Range of Motion and Scapular Upward Rotation in Collegiate Baseball Players. J. Should. Elb. Surg. 2011, 20, 708–716. [Google Scholar] [CrossRef]
- Thomas, S.J.; Swanik, C.B.; Kaminski, T.W.; Higginson, J.S.; Swanik, K.A.; Bartolozzi, A.R.; Nazarian, L.N. Humeral Retroversion and Its Association with Posterior Capsule Thickness in Collegiate Baseball Players. J. Should. Elb. Surg. 2012, 21, 910–916. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-del-Barrio, S.; Jiménez-Rejano, J.J.; Rebollo-Salas, M.; Mingo-Gómez, M.T.; Lorenzo-Muñoz, A.; Ceballos-Laita, L. Increased Tone and Stiffness of the Teres Major Muscle in Elite Handball Athletes: A Cross-Sectional Study. Appl. Sci. 2023, 13, 8457. [Google Scholar] [CrossRef]
- Kamali, F.; Ghasempour, N.; Dehno, N.S. Immediate Effect of Combining Glenohumeral and Scapulothoracic Mobilization with Stretching on Improving Shoulder Internal Rotation in Overhead Throwing Athletes with Glenohumeral Internal Rotation Deficit: A Randomized Clinical Trial Study. Physiother. Pract. Res. 2021, 42, 119–126. [Google Scholar] [CrossRef]
- Kang, M.H.; Oh, J.S. Effects of Self-Stretching with Mobilization on Shoulder Range of Motion in Individuals with Glenohumeral Internal Rotation Deficits: A Randomized Controlled Trial. J. Should. Elb. Surg. 2020, 29, 36–43. [Google Scholar] [CrossRef]
- Manske, R.C.; Meschke, M.; Porter, A.; Smith, B.; Reiman, M. A Randomized Controlled Single-Blinded Comparison of Stretching versus Stretching and Joint Mobilization for Posterior Shoulder Tightness Measured by Internal Rotation Motion Loss. Sports Health 2010, 2, 94–100. [Google Scholar] [CrossRef]
- Ceballos-Laita, L.; Medrano-De-la-fuente, R.; Estébanez-De-miguel, E.; Moreno-Cerviño, J.; Mingo-Gómez, M.T.; Hernando-Garijo, I.; Jiménez-Del-barrio, S. Effects of Dry Needling in Teres Major Muscle in Elite Handball Athletes. A Randomised Controlled Trial. J. Clin. Med. 2021, 10, 4260. [Google Scholar] [CrossRef]
- Ceballos-Laita, L.; Jiménez-Rejano, J.J.; Rebollo-Salas, M.; Mingo-Gómez, M.T.; Hernández-Lázaro, H.; Jiménez-del-Barrio, S. Dry Needling versus Diacutaneous Fibrolysis for the Treatment of the Mechanical Properties of the Teres Major Muscle: A Randomized Clinical Trial. Appl. Sci. 2023, 13, 10995. [Google Scholar] [CrossRef]
- Fairall, R.R.; Cabell, L.; Boergers, R.J.; Battaglia, F. Acute Effects of Self-Myofascial Release and Stretching in Overhead Athletes with GIRD. J. Bodyw. Mov. Ther. 2017, 21, 648–652. [Google Scholar] [CrossRef] [PubMed]
- Bailey, L.B.; Thigpen, C.A.; Hawkins, R.J.; Beattie, P.F.; Shanley, E. Effectiveness of Manual Therapy and Stretching for Baseball Players with Shoulder Range of Motion Deficits. Sports Health 2017, 9, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Nichols, J.; Calver, S.; Chester, R. Are Stretches Effective in the Prevention and Treatment of Glenohumeral Internal Rotation Deficit? Phys. Ther. Rev. 2012, 17, 261–270. [Google Scholar] [CrossRef]
- Mine, K.; Nakayama, T.; Milanese, S.; Grimmer, K. Effectiveness of Stretching on Posterior Shoulder Tightness and Glenohumeral Internal-Rotation Deficit: A Systematic Review of Randomized Controlled Trials. J. Sport Rehabil. 2017, 26, 294–305. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Verhagen, A.P.; de Vet, H.C.; de Bie, R.A.; Kessels, A.G.; Boers, M.; Bouter, L.M.; Knipschild, P.G. The Delphi List: A Criteria List for Quality Assessment of Randomized Clinical Trials for Conducting Systematic Reviews Developed by Delphi Consensus. J. Clin. Epidemiol. 1998, 51, 1235–1241. [Google Scholar] [CrossRef]
- Higgins, J.; Deeks, J. Chapter 6: Choosing Effect Measures and Computing Estimates of Effect. In Cochrane Handbook for Systematic Reviews of Interventions, version 6.4; Updated August 2023; The Cochrane Collaboration: London, UK, 2023. [Google Scholar]
- Higgins, J.; Deeks, J.; Altman, D. Chapter 16: Special Topics in Statistics. In Cochrane Handbook for Systematic Reviews of Interventions, version 5.1.0; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; The Cochrane Collaboration: London, UK, 2019; pp. 1–694. [Google Scholar] [CrossRef]
- Schünemann, H.J.; Higgins, J.P.T.; Vist, G.E.; Glasziou, P.; Akl, E.A.; Skoetz, N.; Guyatt, G.H. Chapter 14: Completing ‘Summary of Findings’ Tables and Grading the Certainty of the Evidence. In Cochrane Handbook for Systematic Reviews of Interventions, version 6.4; Updated August 2023; The Cochrane Collaboration: London, UK, 2023. [Google Scholar]
- Guyatt, G.; Zhao, Y.; Mayer, M.; Briel, M.; Mustafa, R.; Izcovich, A.; Hultcrantz, M.; Iorio, A.; Alba, A.C.; Foroutan, F.; et al. GRADE Guidance 36: Updates to GRADE’s Approach to Addressing Inconsistency. J. Clin. Epidemiol. 2023, 158, 70–83. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Glasziou, P.; Jaeschke, R.; Akl, E.A.; et al. GRADE Guidelines: 7. Rating the Quality of Evidence—Inconsistency. J. Clin. Epidemiol. 2011, 64, 1294–1302. [Google Scholar] [CrossRef] [PubMed]
- Dantas, L.O.; Osani, M.C.; Bannuru, R.R. Therapeutic Ultrasound for Knee Osteoarthritis: A Systematic Review and Meta-Analysis with Grade Quality Assessment. Braz. J. Phys. Ther. 2021, 25, 688–697. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Rind, D.; Devereaux, P.J.; Montori, V.M.; Freyschuss, B.; Vist, G.; et al. GRADE Guidelines 6. Rating the Quality of Evidence—Imprecision. J. Clin. Epidemiol. 2011, 64, 1283–1293. [Google Scholar] [CrossRef]
- Dal Farra, F.; Risio, R.G.; Vismara, L.; Bergna, A. Effectiveness of Osteopathic Interventions in Chronic Non-Specific Low Back Pain: A Systematic Review and Meta-Analysis. Complement. Ther. Med. 2021, 56, 102616. [Google Scholar] [CrossRef] [PubMed]
- Curcio, J.E.; Grana, M.J.; England, S.; Banyas, P.M.; Palmer, B.D.; Placke, A.E.; Rieck, W.A.; Eade, A.M. Use of the Spencer Technique on Collegiate Baseball Players: Effect on Physical Performance and Self-Report Measures. J. Am. Osteopath. Assoc. 2017, 117, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Mathew, N.P.; Prabu Raja, G.; Davis, F. Effect of Fascial Manipulation on Glenohumeral Internal Rotation Deficit in Overhead Athletes—A Randomized Controlled Trial. Muscles Ligaments Tendons J. 2020, 10, 17–23. [Google Scholar] [CrossRef]
- Lo, C.-L.; Hsueh, Y.-H.; Wang, C.-H.; Chang, H.-Y. Comparison of the Acute Effects of Kinesio Taping and Sleeper Stretching on the Shoulder Rotation Range of Motion, Manual Muscle Strength, and Sub-Acromial Space in Pitchers with Glenohumeral Internal Rotation Deficit. Medicina 2021, 57, 102. [Google Scholar] [CrossRef]
- Chepeha, J.C.; Magee, D.J.; Bouliane, M.; Sheps, D.; Beaupre, L. Effectiveness of a Posterior Shoulder Stretching Program on University-Level Overhead Athletes: Randomized Controlled Trial. Clin. J. Sport Med. 2018, 28, 146–152. [Google Scholar] [CrossRef]
- Ilyoung, Y.; Minhyeok, K.; Jaeseop, O. The Effects of Posterior Shoulder Stretch on Rotator Cuff Strength Ratio in Adolescent Baseball Players with Scapular Dyskinesis: A Randomized Controlled Trial. Isokinet. Exerc. Sci. 2018, 26, 63–71. [Google Scholar] [CrossRef]
- Moore, S.D.; Laudner, K.G.; Mcloda, T.A.; Shaffer, M.A. The Immediate Effects of Muscle Energy Technique on Posterior Shoulder Tightness: A Randomized Controlled Trial. J. Orthop. Sports Phys. Ther. 2011, 41, 400–407. [Google Scholar] [CrossRef]
- Maenhout, A.; Van Eessel, V.; Van Dyck, L.; Vanraes, A.; Cools, A. Quantifying Acromiohumeral Distance in Overhead Athletes with Glenohumeral Internal Rotation Loss and the Influence of a Stretching Program. Am. J. Sports Med. 2012, 40, 2105–2112. [Google Scholar] [CrossRef]
- Park, K.; Kwon, O.-Y.; Weon, J.; Choung, S.; Kim, S.-H. Comparison of the Effects of Local Cryotherapy and Passive Cross-Body Stretch on Extensibility in Subjects with Posterior Shoulder Tightness. Artic. J. Sports Sci. Med. 2014, 13, 84–90. [Google Scholar]
- McClure, P.; Balaicuis, J.; Heiland, D.; Broersma, M.E.; Thorndike, C.K.; Wood, A. A Randomized Controlled Comparison of Stretching Procedures for Posterior Shoulder Tightness. J. Orthop. Sports Phys. Ther. 2007, 37, 108–114. [Google Scholar] [CrossRef]
- Cools, A.M.; Johansson, F.R.; Cagnie, B.; Cambier, D.C.; Witvrouw, E.E. Stretching the Posterior Shoulder Structures in Subjects with Internal Rotation Deficit: Comparison of Two Stretching Techniques. Should. Elb. 2012, 4, 56–63. [Google Scholar] [CrossRef]
- Salamh, P.A.; Kolber, M.J.; Hanney, W.J. Effect of Scapular Stabilization during Horizontal Adduction Stretching on Passive Internal Rotation and Posterior Shoulder Tightness in Young Women Volleyball Athletes: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2015, 96, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Guney, H.; Karabicak, G.O.; Pekyavas, N.O. Which Stretching Technique Is Effective in Decreasing Glenohumeral Internal Rotation Deficit? Med. Dello Sport 2015, 68, 291–302. [Google Scholar]
- Gharisia, O.; Lohman, E.; Daher, N.; Eldridge, A.; Shallan, A.; Jaber, H. Effect of a Novel Stretching Technique on Shoulder Range of Motion in Overhead Athletes with Glenohumeral Internal Rotation Deficits: A Randomized Controlled Trial. BMC Musculoskelet. Disord. 2021, 22, 402. [Google Scholar] [CrossRef]
- Kamper, S.J. Blinding: Linking Evidence to Practice. J. Orthop. Sports Phys. Ther. 2018, 48, 825–826. [Google Scholar] [CrossRef]
- Tyler, T.F.; Nicholas, S.J.; Lee, S.J.; Mullaney, M.; McHugh, M.P. Correction of Posterior Shoulder Tightness Is Associated with Symptom Resolution in Patients with Internal Impingement. Am. J. Sports Med. 2010, 38, 114–119. [Google Scholar] [CrossRef]
- Seabra, P.; Van Eck, C.F.; Sá, M.; Torres, J. Are Professional Handball Players at Risk for Developing a Glenohumeral Internal Rotation Deficit in Their Dominant Arm? Physician Sports Med. 2017, 45, 77–81. [Google Scholar] [CrossRef]
- Lintner, D.; Mayol, M.; Uzodinma, O.; Jones, R.; Labossiere, D. Glenohumeral Internal Rotation Deficits in Professional Pitchers Enrolled in an Internal Rotation Stretching Program. Am. J. Sports Med. 2007, 35, 617–621. [Google Scholar] [CrossRef] [PubMed]
- Kubuk, B.S.; Carrasco-Uribarren, A.; Cabanillas-Barea, S.; Ceballos-Laita, L.; Jimenéz-del-Barrio, S.; Pérez-Guillén, S. The Effects of End-Range Interventions in the Management of Primary Adhesive Capsulitis of the Shoulder: A Systematic Review and Meta-Analysis. Disabil. Rehabil. 2024, 46, 3206–3220. [Google Scholar] [CrossRef]
- López-de-Celis, C.; Caudevilla-Polo, S.; Pérez-Bellmunt, A.; González-Rueda, V.; Bueno-Gracia, E.; Estébanez-de-Miguel, E. Effect of Scapular Fixation on Lateral Movement and Scapular Rotation during Glenohumeral Lateral Distraction Mobilisation. Healthcare 2023, 11, 1829. [Google Scholar] [CrossRef]
- Talbott, N.R.; Witt, D.W. In Vivo Measurements of Humeral Movement during Posterior Glenohumeral Mobilizations. J. Man. Manip. Ther. 2016, 24, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Wilk, K.E.; Hooks, T.R.; Macrina, L.C. The Modified Sleeper Stretch and Modified Cross-Body Stretch to Increase Shoulder Internal Rotation Range of Motion in the Overhead Throwing Athlete. J. Orthop. Sports Phys. Ther. 2013, 43, 891–894. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Age | Sport | GIRD | EG | CG | Session Duration | Sessions/Week | Total n° of Sessions | Outcome Variables (Tool) | Main Results |
|---|---|---|---|---|---|---|---|---|---|---|
| Stretching vs. control | ||||||||||
| Lo et al., 2021 [38] | EG: 20.51 (1.18) CG: 20.90 (1.45) | Baseball | 10% decrease in total ROM | Sleeper stretch (n = 10) | Control (n = 10) | 5 reps. 30 s each | 1 | 1 | ROM
| ↑ ND ↑ |
| Chepeha et al., 2017 [39] | 20.51 (1.18) | Volleyball Tennis Swimming | >15° | Sleeper stretch (n = 20) | Control (n = 17) | 5 reps. 2 min each | 7 | 56 8 sem | ROM
| ↑ ↑ ND |
| Yu et al., 2017 [40] | EG: 17.25 (1.35) CG: 16.90 (1.52) | baseball | >15° | Sleeper stretch + standard care (n = 12) | Standard care (n = 12) | 3 reps. 30 s each | 3 | 18 6 sem | ROM
| ↑ ↑ ND |
| Park et al., 2014 [43] | EG: 23.3 (2.0) CG: 23.3 (2.0) | No data | >10° | Cross-body stretch (n = 29) | Control (n = 29) | 6 reps. 30 s each | 1 | 1 | ROM
| ↑ ↑ |
| Maenhout et al., 2012 [42] | EG: 21.4 (2.5) CG: 21.1 (2.2) | Volleyball Tennis Waterpolo Squash badminton | >15° | Sleeper stretch (n = 30) | Control (n = 32) | 3 reps. 30 s each | 7 | 42 6 weeks | ROM
| ↑ ND ↑ |
| Moore et al., 2011 A [41] | EG: 19.5 (1.0) CG: 19.8 (1.1) | Baseball | <8° in total ROM | Cross-body stretch (n = 19) | Control (n = 20) | 3 reps. 2 min in total | 1 | 1 | ROM
| ↑ ↑ |
| Moore et al., 2011 B [41] | EG: 20.4 (1.1) CG: 19.8 (1.1) | Baseball | <8° in total ROM | Sleeper stretch (n = 22) | Control (n = 20) | 3 reps. 2 min in total | 1 | 1 | ROM
| ND ND |
| McClure et al., 2007 A [44] | EG: 23.5 (1.7) CG: 23.5 (1.8) | No data | >10° | Sleeper stretch (n = 15) | Control (n = 24) | 5 reps. 30 s each. | 1 | 28 4 weeks | ROM
| ↑ ND |
| McClure et al., 2007 B [44] | EG: 22.9 (1.5) CG: 23.5 (1.8) | No data | >10° | Cross-body stretch (n = 15) | Control (n = 24) | 5 reps. 30 s each. | 1 | 28 4 weeks | ROM
| ↑ ND |
| Stretching plus manual therapy vs. stretching in isolation | ||||||||||
| Manske et al., 2010 [18] | No data | No data | >10° | GH dorsal glide + cross-body stretch (n = 19) | Cross-body stretch (n = 20) | Stretching: 5 reps. 30 s each Dorsal glide: 10 min | Stretching 3–4 Manual therapy 2–3 | 4 weeks | ROM
| ND ND |
| Fairall et al., 2017 [21] | 36.9 (11.1) | Softball | >20° | Myofascial release + sleeper and cross-body stretch (n = 4) | sleeper and cross-body stretch (n = 4) | Stretching: 3 reps. 30 s each Myofascial release: 2 reps. 60 s each | 1 | 1 | ROM
| ND |
| Bailey et al., 2017 [22] | EG: 18.8 (2.6) CG: 18.6 (2.1) | Baseball | >15° | Manual therapy + stretching (sleeper and cross-body stretch) (n = 30) | Stretching (sleeper and cross-body stretch) (n = 30) | Stretching: 2 reps. 1 min each Manual therapy: friction in teres minor and infraspinatus | 1 | 1 | ROM
| ↑ ↑ ↑ |
| Kang et al., 2020 [17] | EG: 22.2 (2.7) CG: 22.4 (2.3) | No data | >10° | GH dorsal glide + cross-body stretch (n = 20) | Cross-body stretch (n = 20) | 2 reps. 30 s each | 1 | 1 | ROM
| ↑ ↑ |
| Kamali et al., 2021 [16] | EG: 21.26 (2.98) CG: 23.40 (4.79) | Volleyball | >15° | GH dorsal glide + stretching (sleeper and cross-body stretch) (n = 15) | Stretching (sleeper and cross-body stretch) (n = 15) | Stretching: 5 reps. 30 s each Mobilization: 3 sets of 10 reps | 3 | 3 | ROM
| ND ND |
| Stretching vs. stretching | ||||||||||
| Mcclure et al., 2007 [44] | EG: 23.5 (1.7) CG: 22.9 (1.5) | No data | >10° | Sleeper stretch (n = 15) | Cross-body stretch (n = 15) | 5 reps. 30 s each | 7 | 28 4 weeks | ROM
| ND |
| Cools et al., 2011 A [45] | 24.5 (7.8) | Volleyball Tennis Squash Badminton | 20° | Sleeper and cross-body stretch (n = 15) | Dorsal and caudal gliding (n = 15) | 15 m | 3 | 9 3 weeks | ROM
| ND |
| Cools et al., 2011 B [45] | 25.4 (6.7) | Volleyball Tennis Squash Badminton | 20° | Sleeper and cross-body stretch (n = 15) | Dorsal and caudal gliding (n = 15) | 15 m | 3 | 9 3 weeks | ROM
| ND |
| Salamh et al., 2014 [46] | EG: 16.1 (1.2) CG: 16.5 (1.5) | Volleyball | >10° | Cross-body stretch with manual stabilization (n = 30) | Cross-body stretch (n = 30) | 2 reps. 30 s each | 1 | 1 | ROM
| ↑ ↑ |
| Guney et al., 2015 A [47] | EG: 23.8 (1.7) CG: 24.1 (4.1) | No data | >18° | Sleeper stretch (n = 24) | Cross-body stretch (n = 23) | 3 reps. 30 s each | 7 | 1 | ROM
| ND ND ND |
| Guney et al., 2015 B [47] | EG: 23.9 (1.5) CG: 24.1 (4.1) | No data | >18° | Cross-body stretch with manual stabilization (n = 24) | Cross-body stretch (n = 23) | 3 reps. 30 s each | 7 | 1 | ROM
| ↑ ↑ ↑ |
| Gharisia et al., 2021 [48] | EG: 26.0 (2.5) CG: 25.9 (2.6) | Volleyball Tennis Waterpolo Squash Baseball Swimming | 15.6 (5.5) | Sleeper stretch (n = 20) | Passive Internal rotation with clam shell bridging (n = 20) | 3 reps. 30 s each | 3 | 12 4 weeks | ROM
| ND ↑ CG vs. EG |
| Author | Items | Total | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | ||
| Stretching vs. control | ||||||||||||
| Lo et al., 2021 [38] | Y | Y | N | Y | N | N | N | Y | Y | Y | Y | 6/10 |
| Chepeha et al., 2018 [39] | Y | Y | N | Y | N | N | Y | Y | N | Y | Y | 6/10 |
| Yu et al., 2017 [40] | N | Y | Y | Y | N | N | N | Y | Y | Y | Y | 7/10 |
| Park et al., 2014 [43] | Y | Y | N | N | N | N | Y | N | N | Y | N | 3/10 |
| Maenhout et al., 2012 [42] | N | Y | N | Y | N | N | N | N | N | Y | Y | 4/10 |
| Moore et al., 2011 [41] | Y | Y | N | Y | N | N | Y | Y | N | Y | Y | 6/10 |
| Stretching plus manual therapy vs. stretching in isolation | ||||||||||||
| Manske et al., 2010 [18] | N | Y | N | Y | N | N | Y | Y | N | Y | Y | 6/10 |
| Fairall et al., 2017 [21] | Y | N | N | Y | N | N | N | Y | Y | N | Y | 4/10 |
| Baley et al., 2017 [22] | N | Y | N | Y | N | N | N | Y | N | Y | Y | 5/10 |
| Kang et al., 2020 [17] | Y | Y | Y | Y | N | N | N | Y | Y | Y | Y | 7/10 |
| Kamali et al., 2021 [16] | Y | Y | Y | N | N | Y | Y | Y | Y | Y | Y | 8/10 |
| Stretching vs. stretching | ||||||||||||
| Mcclure et al., 2007 [44] | Y | Y | N | Y | N | N | Y | Y | N | Y | Y | 6/10 |
| Cools et al., 2011 [45] | Y | Y | N | Y | N | N | N | N | N | Y | Y | 4/10 |
| Salamh et al., 2014 [46] | Y | Y | N | Y | N | N | Y | N | N | Y | Y | 5/10 |
| Guney et al., 2015 [47] | Y | Y | Y | Y | N | N | Y | Y | Y | Y | Y | 8/10 |
| Gharisia et al., 2021 [48] | Y | Y | Y | Y | N | N | Y | Y | Y | Y | Y | 8/10 |
| Outcome | No. of Studies (Participants) | Risk of Bias | Inconsistency | Indirectness | Imprecision | Certainty of Evidence |
|---|---|---|---|---|---|---|
| Stretching vs. control | ||||||
| IR ROM | 6 (258) | Very serious a | Very serious c | Serious e | None | Very low |
| HA ROM | 4 (180) | Very serious a | Very serious c | Serious e | Serious f | Very low |
| ER ROM | 2 (82) | Very serious a | Very serious c | Serious e | Serious f | Very low |
| Pain | 2 (61) | serious b | None | Serious e | Serious f | Very low |
| Dorsal gliding + stretching vs. stretching | ||||||
| IR ROM | 3 (109) | serious b | None | Serious e | Serious f | Very low |
| ER ROM | 2 (69) | serious b | None | Serious e | Serious f | Very low |
| Soft-tissue therapy + stretching vs. stretching | ||||||
| IR ROM | 2 (68) | Very serious a | Very serious c | Serious e | Serious f | Very low |
| Cross-body stretch + stabilization vs. cross-body stretch | ||||||
| IR ROM | 2 (107) | serious b | serious d | None | Serious f | Very low |
| Sleeper stretch vs. cross-body stretch | ||||||
| IR ROM | 2 (77) | serious b | Very serious c | None | Serious f | Very low |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ceballos-Laita, L.; Robles-Pérez, R.; Carrasco-Uribarren, A.; Cabanillas-Barea, S.; Pérez-Guillén, S.; Greidane, E.; Jiménez-del-Barrio, S. Is Stretching Effective for Reducing Glenohumeral Internal Rotation Deficit? A Systematic Review and Meta-Analysis. Appl. Sci. 2024, 14, 7166. https://doi.org/10.3390/app14167166
Ceballos-Laita L, Robles-Pérez R, Carrasco-Uribarren A, Cabanillas-Barea S, Pérez-Guillén S, Greidane E, Jiménez-del-Barrio S. Is Stretching Effective for Reducing Glenohumeral Internal Rotation Deficit? A Systematic Review and Meta-Analysis. Applied Sciences. 2024; 14(16):7166. https://doi.org/10.3390/app14167166
Chicago/Turabian StyleCeballos-Laita, Luis, Román Robles-Pérez, Andoni Carrasco-Uribarren, Sara Cabanillas-Barea, Silvia Pérez-Guillén, Evita Greidane, and Sandra Jiménez-del-Barrio. 2024. "Is Stretching Effective for Reducing Glenohumeral Internal Rotation Deficit? A Systematic Review and Meta-Analysis" Applied Sciences 14, no. 16: 7166. https://doi.org/10.3390/app14167166