
Enhancing Inter-Patient Performance for Arrhythmia Classification with Adversarial Learning Using Beat-Score Maps



Abstract
:1. Introduction
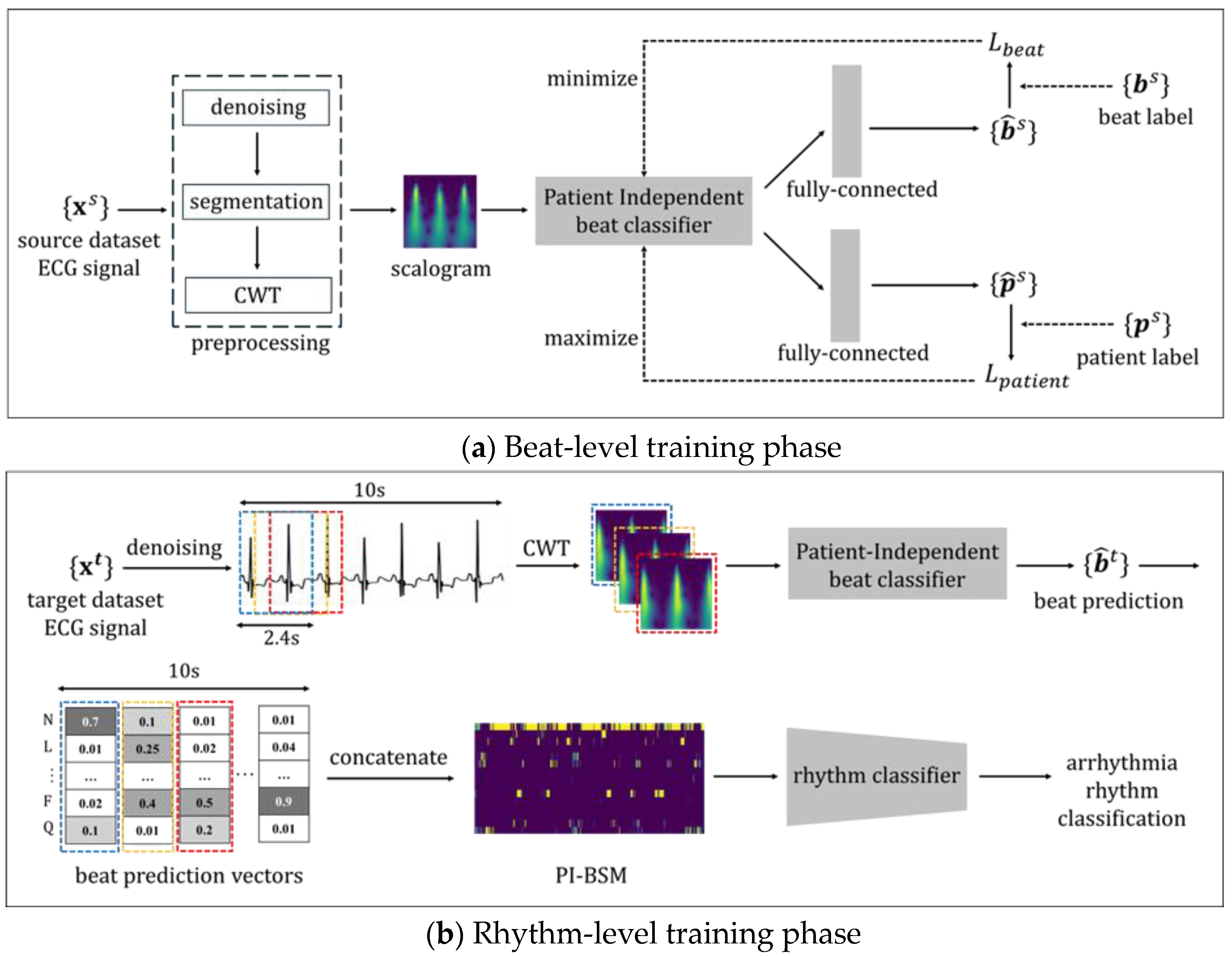
- The proposed method addresses inter-patient variability in ECG signals for the n-BSM-based arrhythmia classification by utilizing adversarial learning. Specifically, an adversarial framework is applied to the pre-training stage of the beat classifier used for PI-BSM generation. Consequently, PI-BSMs derived from ECG signals are able to effectively capture beat-related features while excluding patient-specific features;
- The proposed framework extends the applicability of the BSMs to cross databases by not mandating beat annotations. That is, a beat classifier can be pre-trained on any beat-annotated dataset (referred to as a source dataset), which is then used to derive PI-BSMs from other target datasets without beat annotations. This approach is suitable for real-world scenarios where beat annotations are lacking. Due to the enhanced generalization in the beat-level training phase, the PI-BSM can mitigate individual bias;
- The proposed method improves the performance of ECG arrhythmia classification in the inter-patient paradigm by using PI-BSMs as the input for a CNN-based rhythm classification model. Cross-validation within the MIT-BIH arrhythmia database (MIT-BIH dataset) showed a 14.27% improvement in the F1-score. When tested on the Chapman–Shaoxing 12-lead ECG database (SPH dataset) in a cross-database scenario, PI-BSM-based classification indicated a 4.97% improvement compared to our previous study;
- The proposed method achieves the most notable improvement in atrial fibrillation (AFib) rhythm, which exhibits the lowest performance in most other inter-patient studies. Utilizing this method demonstrated a 27.70% F1-score improvement in the MIT-BIH dataset cross-validation and a 16.22% increase in F1-score when tested with the SPH dataset. These findings confirm that there is significant variability among patients, particularly in AFib rhythms, and highlight the importance of taking this variability into account in AFib research.
2. Related Work
2.1. Subject-Specific Modeling Approach
2.2. Subject-Independent Modeling Approach
3. Materials and Methods
3.1. Data Preprocessing
3.2. Beat-Level Training Phase
- Beat Loss ()
- Patient Loss ()
- Total Loss ()
3.3. Rhythm-Level Training Phase
4. Results and Discussion
4.1. Experimental Setup
4.1.1. Dataset
4.1.2. Hyperparameter Setting
4.1.3. Evaluation Metrics
4.2. Experiment 1: Evaluation of the Proposed Method on a Single Database
4.3. Experiment 2: Evaluation of the Proposed Method on Cross-Database
4.3.1. Effect of Patient Loss () on PI-BSM Generation
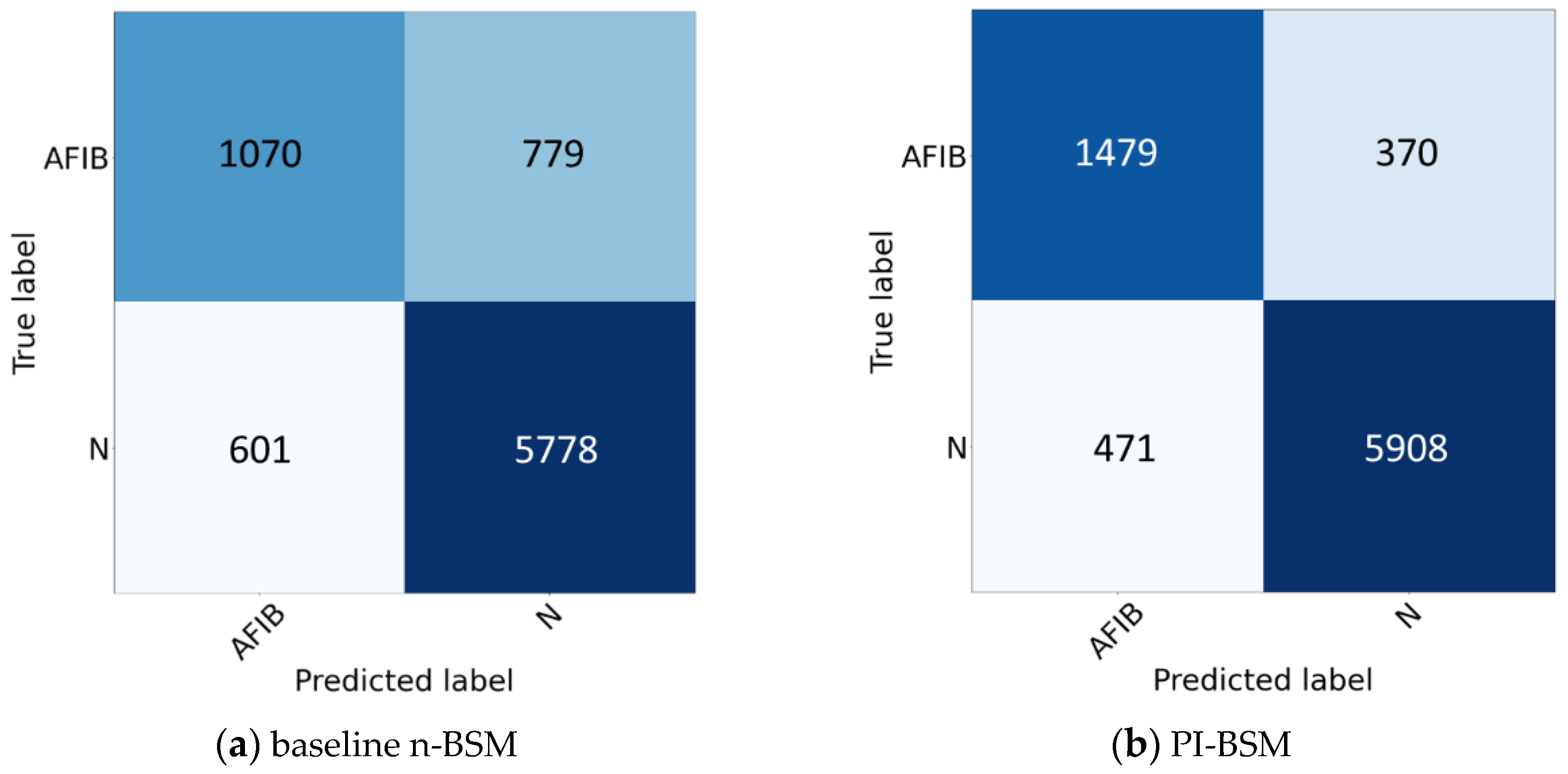
4.3.2. Characterization of PI-BSMs through Adversarial Learning
4.3.3. Comparison with State-of-the-Art Methods

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Database | No. of Classes | Method | Evaluation | Lead | F1-Score | Accuracy |
|---|---|---|---|---|---|---|---|
| Chandra et al. [35] (2017) | PhysioNet 2017 | 3 | CNN | Inter-patient | 1 | 71.0 | Unknown |
| Andreotti et al. [36] (2017) | PhysioNet 2017 | 3 | ResNet | Inter-patient | 1 | 83.0 | Unknown |
| Murat et al. [39] (2021) | SPH | 4 | Hybrid DNN | Intra-patient | 1 | 97.7 | 98.0 |
| Aziz et al. [37] (2021) | SPH | 4 | MLP | Unknown | 1 | 89.5 | 90.7 |
| Aziz et al. [37] (2021) | MIT-BIH, SPH | 3 | MLP | Unknown | 1 | 60.3 | 68.0 |
| Zhang et al. [38] (2023) | NFH, SPH | 4 | ST-ReGE | Inter-patient | 12 | 88.0 | 89.7 |
| Lee et al. [10] (2024) | MIT-BIH, SPH | 4 | SE-ResNet | Inter-patient | 1 | 83.2 | 86.3 |
| Proposed Method | MIT-BIH, SPH | 4 | SE-ResNet | Inter-patient | 1 | 87.4 | 88.7 |
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| N | normal beat |
| L | left bundle branch block beat |
| R | right bundle branch block beat |
| A | atrial premature beat |
| a | aberrated atrial premature beat |
| J | junctional premature beat |
| S | supraventricular premature beat |
| V | premature ventricular contraction |
| F | fusion of ventricular and normal beat |
| e | atrial escape beat |
| j | junctional escape beat |
| E | ventricular escape beat |
| / | paced beat |
| f | fusion of paced and normal beat |
| Q | unclassifiable beat |
| AFib | atrial fibrillation |
| GSVT | grouped supraventricular tachycardia |
| SR | sinus rhythm |
| SB | sinus bradycardia |
References
- Murat, F.; Yildirim, O.; Talo, M.; Baloglu, U.; Demir, Y.; Acharya, U. Application of deep learning techniques for heartbeats detection using ECG signals-analysis and review. Comput. Biol. Med. 2020, 120, 103726. [Google Scholar] [CrossRef] [PubMed]
- Haugaa, K.H.; Edvardsen, T.; Amlie, J.P. Prediction of life-threatening arrhythmias–still an unresolved problem. Cardiology 2011, 118, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Berger, F.A.; Sijs, H.; Gelder, T.; Kuijper, A.F.; Bemt, P.M.; Becker, M.L. Comparison of two algorithms to support medication surveillance for drug-drug interactions between QTc-prolonging drugs. Int. J. Med. Inform. 2021, 145, 104329. [Google Scholar] [CrossRef] [PubMed]
- Sinal, M.S.; Kamioka, E. Early abnormal heartbeat multistage classification by using decision tree and K-nearest neighbor. In Proceedings of the 2018 Artificial Intelligence and Cloud Computing Conference, New York, NY, USA, 21–23 December 2018; pp. 29–34. [Google Scholar] [CrossRef]
- Saber, M.; Abotaleb, M. Arrhythmia modern classification techniques: A review. J. Artif. Intell. Metaheuristics 2022, 1, 42–53. [Google Scholar] [CrossRef]
- Xiao, Q.; Lee, K.; Mokhtar, S.A.; Ismail, I.; Pauzi, A.L.b.M.; Zhang, Q.; Lim, P.Y. Deep learning-based ECG arrhythmia classification: A systematic review. Appl. Sci. 2023, 13, 4964. [Google Scholar] [CrossRef]
- Liu, W.; Huang, Q.; Chang, S.; Wang, H.; He, J. Multiple-feature-branch convolutional neural network for myocardial infarction diagnosis using electrocardiogram. Biomed. Signal Process. Control 2018, 45, 22–32. [Google Scholar] [CrossRef]
- Xu, S.S.; Mak, M.W.; Chang, C. Inter-patient ECG classification with i-vector based unsupervised patient adaptation. Expert Syst. Appl. 2022, 210, 118410. [Google Scholar] [CrossRef]
- Zahid, M.U.; Kiranyaz, S.; Gabbouj, M. Global ECG classification by self-operational neural networks with feature injection. IEEE Trans. Biomed. Eng. 2022, 70, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Shin, M. Using beat score maps with successive segmentation for ECG classification without R-peak detection. Biomed. Signal Process. Control 2024, 91, 105982. [Google Scholar] [CrossRef]
- Li, Y.; Pang, Y.; Wang, J.; Li, X. Patient-specific ECG classification by deeper CNN from generic to dedicated. Neurocomputing 2018, 314, 336–346. [Google Scholar] [CrossRef]
- Xu, S.S.; Mak, M.W.; Cheung, C.C. I-vector-based patient adaptation of deep neural networks for 22 automatic heartbeat classification. IEEE J. Biomed. Health Inform. 2019, 24, 717–727. [Google Scholar] [CrossRef] [PubMed]
- Kiranyaz, S.; Ince, T.; Gabbouj, M. Real-time patient-specific ECG classification by 1-D convolutional neural networks. IEEE Trans. Biomed. Eng. 2015, 63, 664–675. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Wang, G.; Zhao, J.; Gao, P.; Lin, J.; Yang, H. Patient-specific ECG classification based on recurrent neural networks and clustering technique. In Proceedings of the 2017 13th IASTED International Conference on Biomedical Engineering (BioMed), Innsbruck, Austria, 20–21 February 2017; pp. 63–67. [Google Scholar] [CrossRef]
- Xia, Y.; Zhang, H.; Xu, L.; Gao, Z.; Zhang, H.; Liu, H.; Li, S. An automatic cardiac arrhythmia classification system with wearable electrocardiogram. IEEE Access 2018, 6, 16529–16538. [Google Scholar] [CrossRef]
- Rahhal, M.M.; Bazi, Y.; AlHichri, H.; Alajlan, N.; Melgani, F.; Yager, R.R. Deep learning approach for active classification of electrocardiogram signals. Inf. Sci. 2016, 345, 340–354. [Google Scholar] [CrossRef]
- Golany, T.; Radinsky, K. Pgans: Personalized generative adversarial networks for ecg synthesis to improve patient-specific deep ecg classification. In Proceedings of the AAAI Conference on Artificial Intelligence, Honolulu, HI, USA, 27 January–1 February 2019; Volume 33, pp. 557–564. [Google Scholar] [CrossRef]
- Zhai, X.; Zhou, Z.; Tin, C. Semi-supervised learning for ECG classification without patient-specific labeled data. Expert Syst. Appl. 2020, 158, 113411. [Google Scholar] [CrossRef]
- Zhou, Z.; Zhai, X.; Tin, C. Fully automatic electrocardiogram classification system based on generative adversarial network with auxiliary classifier. Expert Syst. Appl. 2021, 174, 114809. [Google Scholar] [CrossRef]
- Ye, C.; Kumar, B.V.K.V.; Coimbra, M.T. An automatic subject-adaptable heartbeat classifier based on multiview learning. IEEE J. Biomed. Health Inform. 2015, 20, 1485–1492. [Google Scholar] [CrossRef] [PubMed]
- Niu, J.; Tang, Y.; Sun, Z.; Zhang, W. Inter-patient ECG classification with symbolic representations and multi-perspective convolutional neural networks. IEEE J. Biomed. Health Inform. 2019, 24, 1321–1332. [Google Scholar] [CrossRef] [PubMed]
- Xia, Y.; Xiong, Y.; Wang, K. A transformer model blended with CNN and denoising autoencoder for inter-patient ECG arrhythmia classification. Biomed. Signal Process. Control 2023, 86, 105271. [Google Scholar] [CrossRef]
- Zhou, F.; Sun, Y.; Wang, Y. Inter-patient ECG arrhythmia heartbeat classification network based on multiscale convolution and FCBA. Biomed. Signal Process. Control 2024, 90, 105789. [Google Scholar] [CrossRef]
- Guo, L.; Sim, G.; Matuszewski, B. Inter-patient ECG classification with convolutional and recurrent neural networks. Biocybern. Biomed. Eng. 2019, 39, 868–879. [Google Scholar] [CrossRef]
- He, Z.; Chen, Y.; Yuan, S.; Zhao, J.; Yuan, Z.; Polat, K.; Alhudhaif, A.; Alenezi, F.; Hamid, A. A novel unsupervised domain adaptation framework based on graph convolutional network and multi-level feature alignment for inter-subject ECG classification. Expert Syst. Appl. 2023, 221, 119711. [Google Scholar] [CrossRef]
- Rafi, T.H.; Ko, Y. SF-ECG: Source-free intersubject domain adaptation for electrocardiography-based arrhythmia classification. Appl. Sci. 2023, 13, 8551. [Google Scholar] [CrossRef]
- Yuan, L.; Siyal, M.Y. Target-oriented augmentation privacy-protection domain adaptation for imbalanced ECG beat classification. Biomed. Signal Process. Control 2023, 86, 105308. [Google Scholar] [CrossRef]
- Feng, P.; Fu, J.; Ge, Z.; Wang, H.; Zhou, Y.; Zhou, B.; Wang, Z. Unsupervised semantic-aware adaptive feature fusion network for arrhythmia detection. Inf. Sci. 2022, 582, 509–528. [Google Scholar] [CrossRef]
- Hu, J.; Shen, L.; Sun, G. Squeeze-and-excitation networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 7132–7141. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Wang, G.; Chen, M.; Ding, Z.; Li, J.; Yang, H.; Zhang, P. Inter-patient ECG arrhythmia heartbeat classification based on unsupervised domain adaptation. Neurocomputing 2021, 454, 339–349. [Google Scholar] [CrossRef]
- Moody, G.B.; Mark, R.G. The impact of the MIT-BIH arrhythmia database. IEEE Eng. Med. Biol. Mag. 2001, 20, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Zhang, J.; Danioko, S.; Yao, H.; Guo, H.; Rakovski, C. A 12-lead electrocardiogram database for arrhythmia research covering more than 10,000 patients. Sci. Data 2020, 7, 48. [Google Scholar] [CrossRef] [PubMed]
- Chazal, P.; O’Dwyer, M.; Reilly, R.B. Automatic classification of heartbeats using ECG morphology and heartbeat interval features. IEEE Trans. Biomed. Eng. 2004, 51, 1196–1206. [Google Scholar] [CrossRef] [PubMed]
- Chandra, B.S.; Sastry, C.S.; Jana, S.; Patidar, S. Atrial fibrillation detection using convolutional neural networks. In Proceedings of the 2017 Computing in Cardiology (CINC), Rennes, France, 24–27 September 2017. [Google Scholar] [CrossRef]
- Andreotti, F.; Carr, O.; Pimentel, M.A.; Mahdi, A.; De Vos, M. Comparing feature-based classifiers and convolutional neural networks to detect arrhythmia from short segments of ECG. In Proceedings of the 2017 Computing in Cardiology (CINC), Rennes, France, 24–27 September 2017. [Google Scholar] [CrossRef]
- Aziz, S.; Ahmed, S.; Alouini, M.S. ECG-based machine-learning algorithms for heartbeat classification. Sci. Rep. 2021, 11, 18738. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Liu, W.; Chang, S.; Wang, H.; He, J.; Huang, Q. ST-ReGE: A Novel Spatial-Temporal Residual Graph Convolutional Network for CVD. IEEE J. Biomed. Health Inform. 2023, 28, 216–227. [Google Scholar] [CrossRef]
- Murat, F.; Yildirim, O.; Talo, M.; Demir, Y.; Tan, R.S.; Ciaccio, E.J.; Acharya, U.R. Exploring deep features and ECG 23 attributes to detect cardiac rhythm classes. Knowl. Based Syst. 2021, 232, 107473. [Google Scholar] [CrossRef]







| Layer | Type | Output Size | Kernel Size | Strides |
|---|---|---|---|---|
| Layer 1 | Inputs | (150 × 360 × 1) | 7 × 7 | 2 × 2 |
| Layer 2 | 2D Convolution layer | (75 × 180 × 64) | 3 × 3 | 2 × 2 |
| Layer 3 | Max pooling | (37 × 89 × 64) | 3 × 3 | 2 × 2 |
| Layer 4 | SE-Identity Block | (37 × 89 × 64) | 3 × 3/5 × 5 | 1 × 1/1 × 1 |
| Layer 5 | SE-Identity Block | (37 × 89 × 64) | 3 × 3/5 × 5 | 1 × 1/1 × 1 |
| Layer 6 | SE-Convolution Block | (19 × 45 × 128) | 3 × 3/5 × 5/1 × 1 | 2 × 2/1 × 1/2 × 2 |
| Layer 7 | SE-Identity Block | (19 × 45 × 128) | 3 × 3/5 × 5 | 1 × 1/1 × 1 |
| Layer 8 | SE-Convolution Block | (10 × 23 × 256) | 3 × 3/5 × 5/1 × 1 | 2 × 2/1 × 1/2 × 2 |
| Layer 9 | SE-Identity Block | (10 × 23 × 256) | 3 × 3/5 × 5 | 1 × 1/1 × 1 |
| Layer 10 | SE-Convolution Block | (5 × 12 × 512) | 3 × 3/5 × 5/1 × 1 | 2 × 2/1 × 1/2 × 2 |
| Layer 11 | SE-Identity Block | (5 × 12 × 512) | 3 × 3/5 × 5 | 1 × 1/1 × 1 |
| Layer 12 | Global Average Pooling | (512) | - | - |
| N | L | R | V | A | a | J | F | |
|---|---|---|---|---|---|---|---|---|
| DS1 | 38041 | 3945 | 3776 | 3681 | 806 | 100 | 32 | 414 |
| DS2 | 36386 | 4119 | 3472 | 3217 | 1734 | 50 | 514 | 388 |
| j | E | Q | / | f | e | S | Record | |
| DS1 | 16 | 105 | 8 | 0 | 0 | 16 | 8 | 22 |
| DS2 | 213 | 1 | 7 | 0 | 0 | 0 | 0 | 22 |
| Normal Rhythm | AFib Rhythm | Overall | ||||||
|---|---|---|---|---|---|---|---|---|
| Pre | Sen | F1 | Pre | Sen | F1 | F1 | Acc | |
| Baseline | 87.7 | 90.3 | 89.0 | 64.0 | 57.9 | 61.0 | 75.0 | 83.2 |
| PI-BSM | 94.1 | 92.6 | 93.4 | 75.8 | 80.0 | 77.9 | 85.7 | 89.8 |
| Merged Rhythm | Rhythm | Number of Samples | |||
|---|---|---|---|---|---|
| Before Preprocessing | After Preprocessing | ||||
| AFIB | Atrial Flutter | 445 | 2225 | 438 | 2218 |
| Atrial Fibrillation | 1780 | 1780 | |||
| GSVT | Atrial Tachycardia | 121 | 2307 | 121 | 2260 |
| Atrioventricular Node Reentrant Tachycardia | 16 | 16 | |||
| Atrioventricular Reentrant Tachycardia | 8 | 8 | |||
| Sinus Atrium to Atrial Wandering Rhythm | 7 | 7 | |||
| Sinus Tachycardia | 1568 | 1564 | |||
| Supraventricular Tachycardia | 587 | 544 | |||
| SB | Sinus Bradycardia | 3889 | 3889 | 3888 | 3888 |
| SR | Sinus Rhythm | 1836 | 2225 | 1564 | 2222 |
| Sinus Irregularity | 399 | 397 | |||
| Total | 10,646 | 20,588 | |||
| (%) | (%) | (%) | (%) | (%) | Acc (%) | |
|---|---|---|---|---|---|---|
| baseline | 67.43 | 84.04 | 95.34 | 86.08 | 83.22 | 86.29 |
| = 0.01 | 73.86 | 85.09 | 96.01 | 88.10 | 85.77 | 87.56 |
| = 0.05 | 71.07 | 82.69 | 95.77 | 85.85 | 83.85 | 85.90 |
| = 0.075 | 78.37 | 86.87 | 95.88 | 88.32 | 87.36 | 88.73 |
| = 0.1 | 76.81 | 86.98 | 96.90 | 87.59 | 87.07 | 88.71 |
| = 0.25 | 75.45 | 86.24 | 94.57 | 86.52 | 85.69 | 87.24 |
| = 0.5 | 76.16 | 86.40 | 95.75 | 86.98 | 86.32 | 87.82 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeong, Y.; Lee, J.; Shin, M. Enhancing Inter-Patient Performance for Arrhythmia Classification with Adversarial Learning Using Beat-Score Maps. Appl. Sci. 2024, 14, 7227. https://doi.org/10.3390/app14167227
Jeong Y, Lee J, Shin M. Enhancing Inter-Patient Performance for Arrhythmia Classification with Adversarial Learning Using Beat-Score Maps. Applied Sciences. 2024; 14(16):7227. https://doi.org/10.3390/app14167227
Chicago/Turabian StyleJeong, Yeji, Jaewon Lee, and Miyoung Shin. 2024. "Enhancing Inter-Patient Performance for Arrhythmia Classification with Adversarial Learning Using Beat-Score Maps" Applied Sciences 14, no. 16: 7227. https://doi.org/10.3390/app14167227
APA StyleJeong, Y., Lee, J., & Shin, M. (2024). Enhancing Inter-Patient Performance for Arrhythmia Classification with Adversarial Learning Using Beat-Score Maps. Applied Sciences, 14(16), 7227. https://doi.org/10.3390/app14167227