
Comparative Electromyographic Analysis in Leg Press of Traditional Fitness Equipment, Traditional Outdoor Fitness Equipment, and a New Model of Outdoor Fitness Equipment in Trained Young Men
 ,
,  , , ,
, , ,  , and
, and 
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Experimental Approach to the Problem
2.2. Subjects
2.3. Measurements
2.3.1. Questionnaire
2.3.2. Anthropometric Characteristics
2.3.3. Determination of 1RM
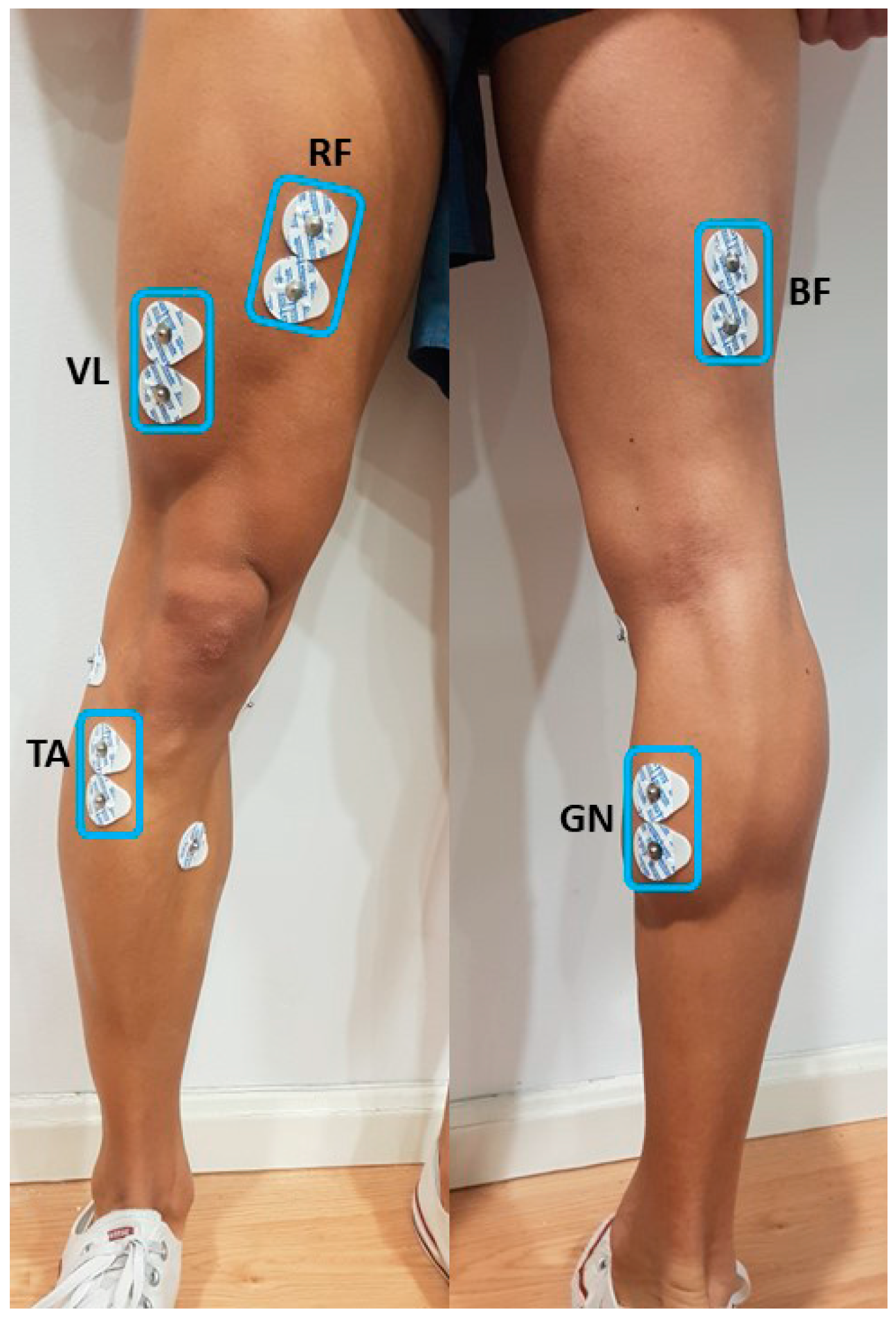
2.3.4. Electromyographic (EMG) Analysis
2.3.5. Determination of Concentric and Eccentric Phases
2.4. Randomization and Blinding
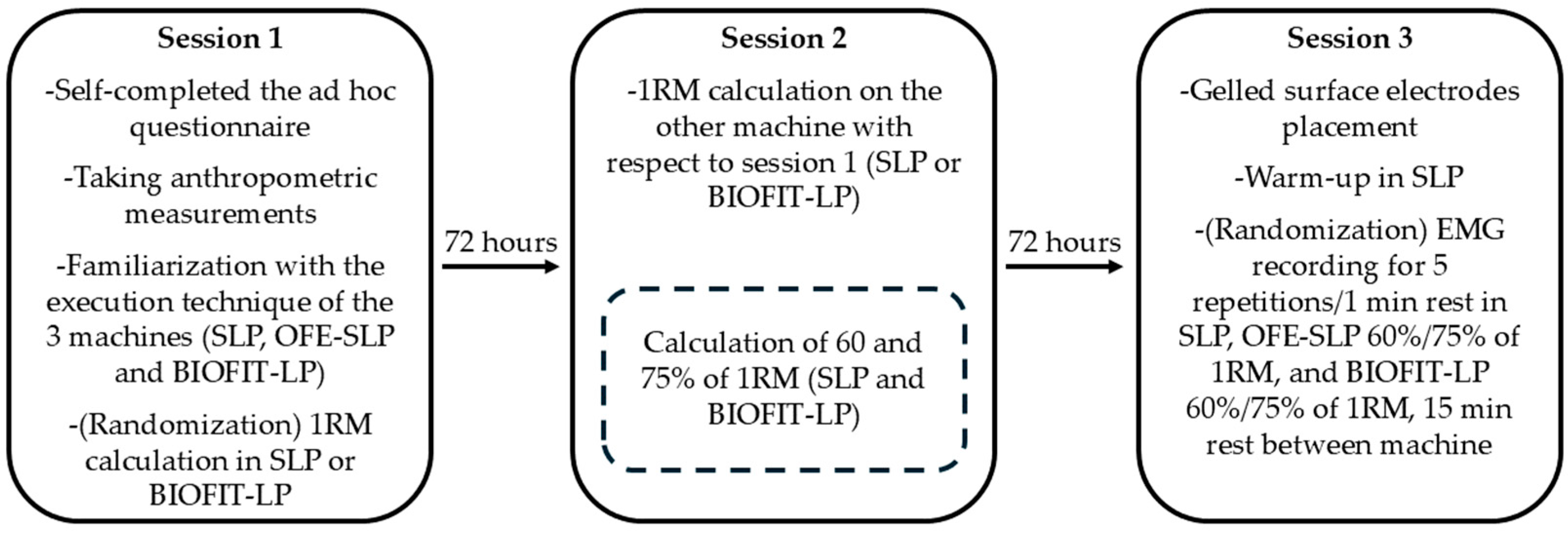
2.5. Procedure
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Armstrong, R.; Baltzopoulos, V.; Langan-Evans, C.; Clark, D.; Jarvis, J.; Stewart, C.; O’Brien, T. An Investigation of Movement Dynamics and Muscle Activity during Traditional and Accentuated-Eccentric Squatting. PLoS ONE 2022, 17, e0276096. [Google Scholar] [CrossRef]
- Fragala, M.S.; Cadore, E.L.; Dorgo, S.; Izquierdo, M.; Kraemer, W.J.; Peterson, M.D.; Ryan, E.D. Resistance Training for Older Adults: Position Statement From the National Strength and Conditioning Association. J. Strength Cond. Res. 2019, 33, 2019–2052. [Google Scholar] [CrossRef]
- Martín-Fuentes, I.; Oliva-Lozano, J.M.; Muyor, J.M. Electromyographic Activity in Deadlift Exercise and Its Variants. A Systematic Review. PLoS ONE 2020, 15, e0229507. [Google Scholar] [CrossRef] [PubMed]
- Escamilla, R.F.; Fleisig, G.S.; Zheng, N.; Lander, J.E.; Barrentine, S.W.; Andrews, J.R.; Bergemann, B.W.; Moorman, C.T. Effects of Technique Variations on Knee Biomechanics during the Squat and Leg Press. Med. Sci. Sports Exerc. 2001, 33, 1552–1566. [Google Scholar] [CrossRef] [PubMed]
- Sarto, F.; Franchi, M.V.; Rigon, P.A.; Grigoletto, D.; Zoffoli, L.; Zanuso, S.; Narici, M.V. Muscle Activation during Leg-Press Exercise with or without Eccentric Overload. Eur. J. Appl. Physiol. 2020, 120, 1651–1656. [Google Scholar] [CrossRef] [PubMed]
- Schwanbeck, S.R.; Cornish, S.M.; Barss, T.; Chilibeck, P.D. Effects of Training with Free Weights Versus Machines on Muscle Mass, Strength, Free Testosterone, and Free Cortisol Levels. J. Strength Cond. Res. 2020, 34, 1851–1859. [Google Scholar] [CrossRef]
- Abelleira-Lamela, T.; Vaquero-Cristóbal, R.; González-Gálvez, N.; Esparza-Ros, F.; Espeso-García, A.; Marcos-Pardo, P.J. Sagittal Spine Disposition and Pelvic Tilt during Outdoor Fitness Equipment Use and Their Associations with Kinanthropometry Proportions in Middle-Aged and Older Adults. PeerJ 2021, 9, e12657. [Google Scholar] [CrossRef]
- Chow, H.; Wu, D.-R. Outdoor Fitness Equipment Usage Behaviors in Natural Settings. Int. J. Environ. Res. Public Health 2019, 16, 391. [Google Scholar] [CrossRef]
- Marcos-Pardo, P.J.; Espeso-García, A.; Vaquero-Cristóbal, R.; Abelleira-Lamela, T.; González-Gálvez, N. The Effect of Resistance Training with Outdoor Fitness Equipment on the Body Composition, Physical Fitness, and Physical Health of Middle-Aged and Older Adults: A Randomized Controlled Trial. Healthcare 2024, 12, 726. [Google Scholar] [CrossRef]
- Handsfield, G.G.; Meyer, C.H.; Hart, J.M.; Abel, M.F.; Blemker, S.S. Relationships of 35 Lower Limb Muscles to Height and Body Mass Quantified Using MRI. J. Biomech. 2014, 47, 631–638. [Google Scholar] [CrossRef]
- Da Silva, E.M.; Brentano, M.A.; Cadore, E.L.; De Almeida, A.P.V.; Kruel, L.F.M. Analysis of Muscle Activation During Different Leg Press Exercises at Submaximum Effort Levels. J. Strength Cond. Res. 2008, 22, 1059–1065. [Google Scholar] [CrossRef] [PubMed]
- van den Tillaar, R.; Kristiansen, E.L.; Larsen, S. Is the Occurrence of the Sticking Region in Maximum Smith Machine Squats the Result of Diminishing Potentiation and Co-Contraction of the Prime Movers among Recreationally Resistance Trained Males? Int. J. Environ. Res. Public Health 2021, 18, 1366. [Google Scholar] [CrossRef] [PubMed]
- Alizadeh, S.; Rayner, M.; Mamdouh, M.; Mahmoud, I.; Behm, D.G.; John’, S.; Labrador, C. Push-Ups vs. Bench Press Differences in Repetitions and Muscle Activation between Sexes. J. Sports Sci. Med. 2020, 19, 289–297. [Google Scholar]
- van den Tillaar, R.; Andersen, V.; Saeterbakken, A.H. Comparison of Muscle Activation and Kinematics during Free-Weight Back Squats with Different Loads. PLoS ONE 2019, 14, e0217044. [Google Scholar] [CrossRef] [PubMed]
- Miyajima, T.; Ishida, K.; Sato, M.; Yamagata, Z. Pilot Study to Test the Safety of an Exercise Machine on Healthy Adult Females. Jpn. J. Nurs. Sci. 2010, 7, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Krause Neto, W.; Vieira, L.; Gama, E.F. Barbell Hip Thrust, Muscular Activation and Performance: A Systematic Review. J. Sports Sci. Med. 2019, 18, 198–206. [Google Scholar]
- Llurda-Almuzara, L.; Labata-Lezaun, N.; López-de-Celis, C.; Aiguadé-Aiguadé, R.; Romaní-Sánchez, S.; Rodríguez-Sanz, J.; Fernández-de-las-Peñas, C.; Pérez-Bellmunt, A. Biceps Femoris Activation during Hamstring Strength Exercises: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 8733. [Google Scholar] [CrossRef] [PubMed]
- Zambrano, H.; Torres, X.; Coleman, M.; Franchi, M.V.; Fisher, J.P.; Oberlin, D.; Van Hooren, B.; Swinton, P.A.; Schoenfeld, B.J. Myoelectric Activity during Electromagnetic Resistance Alone and in Combination with Variable Resistance or Eccentric Overload. Sci. Rep. 2023, 13, 8212. [Google Scholar] [CrossRef]
- Martín-Fuentes, I.; Oliva-Lozano, J.M.; Muyor, J.M. Evaluation of the Lower Limb Muscles’ Electromyographic Activity during the Leg Press Exercise and Its Variants: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 4626. [Google Scholar] [CrossRef]
- Trebs, A.A.; Brandenburg, J.P.; Pitney, W.A. An Electromyography Enalysis of 3 Muscles Surrounding the Shoulder Joint during the Performance of a Chest Press Exercise at Several Angles. J. Strength Cond. Res. 2010, 24, 1925–1930. [Google Scholar] [CrossRef]
- Lee, H.; Jung, M.; Lee, K.-K.; Lee, S. A 3D Human-Machine Integrated Design and Analysis Framework for Squat Exercises with a Smith Machine. Sensors 2017, 17, 299. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, A.M.; Ghigiarelli, J.J.; Sell, K.M.; Shone, E.W.; Kelly, C.F.; Mangine, G.T. Muscle Activation during Resistance Exercise at 70% and 90% 1-repetition Maximum in Resistance-trained Men. Muscle Nerve 2017, 56, 505–509. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.-I.; Lee, D.H.; Hong, S.; Jo, S.; Won, Y.; Jeon, J.Y. Six Weeks of Combined Aerobic and Resistance Exercise Using Outdoor Exercise Machines Improves Fitness, Insulin Resistance, and Chemerin in the Korean Elderly: A Pilot Randomized Controlled Trial. Arch. Gerontol. Geriatr. 2018, 75, 59–64. [Google Scholar] [CrossRef]
- Liu, Y.-C.; Yang, W.-W.; Fang, I.-Y.; Pan, H.L.-L.; Chen, W.-H.; Liu, C. Training Program with Outdoor Fitness Equipment in Parks Offers No Substantial Benefits for Functional Fitness in Active Seniors: A Randomized Controlled Trial. J. Aging Phys. Act. 2020, 28, 828–835. [Google Scholar] [CrossRef] [PubMed]
- Chow, H.W.; Chang, K.T.; Fang, I.Y. Evaluation of the Effectiveness of Outdoor Fitness Equipment Intervention in Achieving Fitness Goals for Seniors. Int. J. Environ. Res. Public Health 2021, 18, 12508. [Google Scholar] [CrossRef]
- Bhalerao, S.; Kadam, P. Sample Size Calculation. Int. J. Ayurveda Res. 2010, 1, 55. [Google Scholar] [CrossRef]
- Schoenfeld, B.J.; Contreras, B.; Willardson, J.M.; Fontana, F.; Tiryaki-Sonmez, G. Muscle Activation during Low- versus High-Load Resistance Training in Well-Trained Men. Eur. J. Appl. Physiol. 2014, 114, 2491–2497. [Google Scholar] [CrossRef]
- Esparza-Ros, F.; Vaquero-Cristóbal, R.; Marfell-Jones, M.J. International Standards for Anthropometric Assessment -Full Profile-; International Society for Advancement in Kinanthropometry: Murcia, Spain, 2019. [Google Scholar]
- Miller, T.A. NSCA’s Guide to Tests and Assessments; Human Kinetics: Champaign, IL, USA, 2012. [Google Scholar]
- López-Vivancos, A.; González-Gálvez, N.; Orquín-Castrillón, F.J.; Vale, R.G.d.S.; Marcos-Pardo, P.J. Electromyographic Activity of the Pectoralis Major Muscle during Traditional Bench Press and Other Variants of Pectoral Exercises: A Systematic Review and Meta-Analysis. Appl. Sci. 2023, 13, 5203. [Google Scholar] [CrossRef]
- Stegeman, D.F.; Hermens, H.J. Standards for Surface Electromyography: The European Project “Surface EMG for Non-Invasive Assessment of Muscles (SENIAM)”; Roessingh Research and Development: Enschede, The Netherlands, 2007. [Google Scholar]
- Snarr, R.L.; Esco, M.R. Electromyographic Comparison of Traditional and Suspension Push-Ups. J. Hum. Kinet. 2013, 39, 75–83. [Google Scholar] [CrossRef]
- Carius, D.; Kugler, P.; Kuhwald, H.-M.; Wollny, R. Absolute and Relative Intrasession Reliability of Surface EMG Variables for Voluntary Precise Forearm Movements. J. Electromyogr. Kinesiol. 2015, 25, 860–869. [Google Scholar] [CrossRef]
- Mitchell, L.J.; Argus, C.K.; Taylor, K.-L.; Sheppard, J.M.; Chapman, D.W. The Effect of Initial Knee Angle on Concentric-Only Squat Jump Performance. Res. Q. Exerc. Sport 2017, 88, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Rossi, F.E.; Schoenfeld, B.J.; Ocetnik, S.; Young, J.; Vigotsky, A.; Contreras, B.; Krieger, J.W.; Miller, M.G.; Cholewa, J. Strength, Body Composition, and Functional Outcomes in the Squat versus Leg Press Exercises. J. Sports Med. Phys. Fit. 2018, 58, 263–270. [Google Scholar] [CrossRef]
- Andersen, V.; Fimland, M.S.; Mo, D.A.; Iversen, V.M.; Vederhus, T.; Rockland Hellebø, L.R.; Nordaune, K.I.; Saeterbakken, A.H. Electromyographic Comparison of Barbell Deadlift, Hex Bar Deadlift, and Hip Thrust Exercises: A Cross-over Study. J. Strength Cond. Res. 2018, 32, 587–593. [Google Scholar] [CrossRef]
- Picerno, P.; Iannetta, D.; Comotto, S.; Donati, M.; Pecoraro, F.; Zok, M.; Tollis, G.; Figura, M.; Varalda, C.; Di Muzio, D.; et al. 1RM Prediction: A Novel Methodology Based on the Force–Velocity and Load–Velocity Relationships. Eur. J. Appl. Physiol. 2016, 116, 2035–2043. [Google Scholar] [CrossRef] [PubMed]
- Padulo, J.; Annino, G.; Tihanyi, J.; Calcagno, G.; Vando, S.; Smith, L.; Vernillo, G.; La Torre, A.; D’ottavio, S. Uphill Racewalking at Iso-Efficiency Speed. J. Strength Cond. Res. 2013, 27, 1964–1973. [Google Scholar] [CrossRef] [PubMed]
- dos Santos Albarello, J.C.; Cabral, H.V.; Leitão, B.F.M.; Halmenschlager, G.H.; Lulic-Kuryllo, T.; da Matta, T.T. Non-Uniform Excitation of Pectoralis Major Induced by Changes in Bench Press Inclination Leads to Uneven Variations in the Cross-Sectional Area Measured by Panoramic Ultrasonography. J. Electromyogr. Kinesiol. 2022, 67, 102722. [Google Scholar] [CrossRef] [PubMed]
- Hahn, D. Lower Extremity Extension Force and Electromyography Properties as a Function of Knee Angle and Their Relation to Joint Torques: Implications for Strength Diagnostics. J. Strength Cond. Res. 2011, 25, 1622–1631. [Google Scholar] [CrossRef]
- Cotterman, M.L.; Darby, L.A.; Skelly, W.A. Comparison of Muscle Force Production Using the Smith Machine and Free Weights for Bench Press and Squat Exercises. J. Strength Cond. Res. 2005, 19, 169. [Google Scholar] [CrossRef]
- Bobet, J.; Norman, R.W. Use of the Average Electromyogram in Design Evaluation Investigation of a Whole-Body Task. Ergonomics 1982, 25, 1155–1163. [Google Scholar] [CrossRef]
- Camara, K.D.; Coburn, J.W.; Dunnick, D.D.; Brown, L.E.; Galpin, A.J.; Costa, P.B. An Examination of Muscle Activation and Power Characteristics While Performing the Deadlift Exercise with Straight and Hexagonal Barbells. J. Strength Cond. Res. 2016, 30, 1183–1188. [Google Scholar] [CrossRef]
- Jo, E.; Valenzuela, K.A.; Leyva, W.; Rivera, J.; Tomlinson, K.; Zeitz, E. Electromyographic Examination of Hip and Knee Extension Hex Bar Exercises Varied by Starting Knee and Torso Angles. Int. J. Exerc. Sci. 2022, 15, 541–551. [Google Scholar] [PubMed]
- Kristiansen, E.; Larsen, S.; Haugen, M.E.; Helms, E.; van den Tillaar, R. A Biomechanical Comparison of the Safety-Bar, High-Bar and Low-Bar Squat around the Sticking Region among Recreationally Resistance-Trained Men and Women. Int. J. Environ. Res. Public Health 2021, 18, 8351. [Google Scholar] [CrossRef] [PubMed]
- Uzun, B.; Taylan, O.; Gültekin, B.; Havıtçıoğlu, H. Dynamic Measurements of Musculus Tibialis Anterior Ligaments with Different Angles. J. Biomech. 2011, 44, 2. [Google Scholar] [CrossRef]
- Mehr, K. Surface Electromyography in Orthodontics—A Literature Review. Med. Sci. Monit. 2013, 19, 416–423. [Google Scholar] [CrossRef] [PubMed]
- Cormie, P.; McGuigan, M.R.; Newton, R.U. Developing Maximal Neuromuscular Power Part 1—Biological Basis of Maximal Power Production. Sports Med. 2011, 41, 17–38. [Google Scholar] [CrossRef]
- Yavuz, H.U.; Erdağ, D.; Amca, A.M.; Aritan, S. Kinematic and EMG Activities during Front and Back Squat Variations in Maximum Loads. J. Sports Sci. 2015, 33, 1058–1066. [Google Scholar] [CrossRef]
- Oshikawa, T.; Morimoto, Y.; Kaneoka, K. Lumbar Lordosis Angle and Trunk and Lower-Limb Electromyographic Activity Comparison in Hip Neutral Position and External Rotation during Back Squats. J. Phys. Ther. Sci. 2018, 30, 434–438. [Google Scholar] [CrossRef] [PubMed]
- Von Werder, S.C.F.A.; Kleiber, T.; Disselhorst-Klug, C. A Method for a Categorized and Probabilistic Analysis of the Surface Electromyogram in Dynamic Contractions. Front. Physiol. 2015, 6, 30. [Google Scholar] [CrossRef]
- Vøllestad, N.K. Measurement of Human Muscle Fatigue. J. Neurosci. Methods 1997, 74, 219–227. [Google Scholar] [CrossRef]
- Kim, H.; Lee, J.; Kim, J. Electromyography-Signal-Based Muscle Fatigue Assessment for Knee Rehabilitation Monitoring Systems. Biomed. Eng. Lett. 2018, 8, 345–353. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1RM | 60% 1RM | 75% 1RM | |
|---|---|---|---|
| SLP (kg) | 201.51 ± 35.35 | 120.91 ± 21.21 | 151.14 ± 26.51 |
| BIOFIT-LP (kg) | 56.31 ± 13.72 | 31.85 ± 11.27 | 39.82 ± 14.09 |
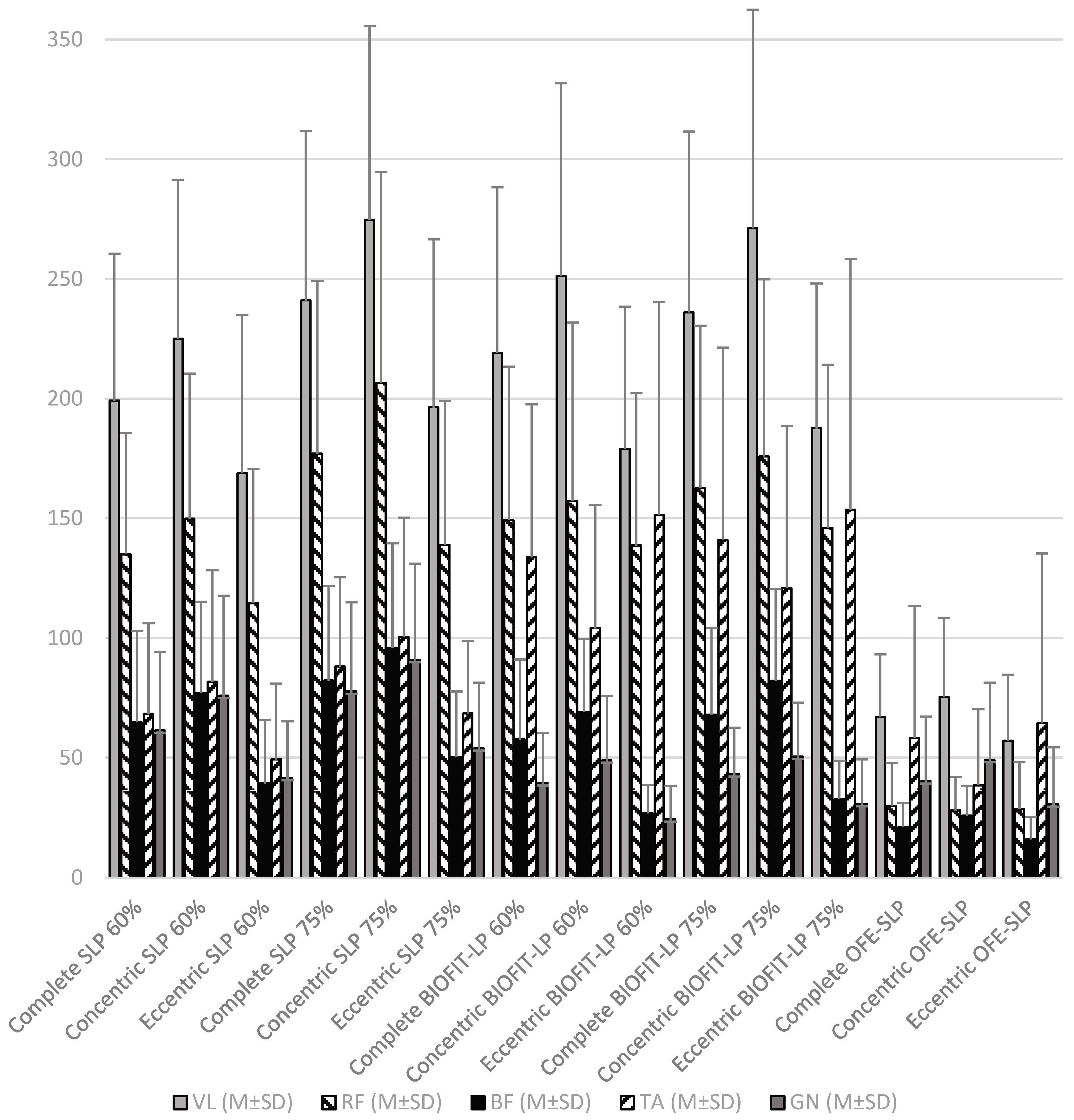
| VL (M ± SD) | RF (M ± SD) | BF (M ± SD) | TA (M ± SD) | GN (M ± SD) | |
|---|---|---|---|---|---|
| Complete | |||||
| SLP 60% | 199.17 ± 61.46 | 134.96 ± 50.57 | 64.77 ± 38.23 | 68.29 ± 37.92 | 61.43 ± 32.66 |
| SLP 75% | 241.01 ± 70.83 | 176.98 ± 72.18 | 82.17 ± 39.51 | 88.08 ± 37.27 | 77.65 ± 37.31 |
| BIOFIT-LP 60% | 219.09 ± 69.23 | 149.25 ± 64.14 | 57.51 ± 33.48 | 133.69 ± 63.86 | 39.48 ± 20.78 |
| BIOFIT-LP 75% | 235.99 ± 75.52 | 162.60 ± 67.85 | 67.91 ± 36.25 | 140.83 ± 80.50 | 43.11 ± 19.41 |
| OFE-SLP | 66.89 ± 26.28 | 30.00 ± 17.76 | 21.22 ± 10.04 | 58.18 ± 55.18 | 40.18 ± 26.93 |
| Concentric | |||||
| SLP 60% | 224.98 ± 66.44 | 149.84 ± 60.63 | 77.11 ± 38.01 | 81.63 ± 46.72 | 75.83 ± 41.86 |
| SLP 75% | 274.71 ± 80.92 | 206.55 ± 88.28 | 95.83 ± 43.83 | 100.44 ± 49.77 | 90.85 ± 40.21 |
| BIOFIT-LP 60% | 251.12 ± 80.71 | 157.21 ± 74.59 | 69.14 ± 30.52 | 104.11 ± 51.47 | 48.86 ± 26.96 |
| BIOFIT-LP 75% | 271.15 ± 91.27 | 175.80 ± 74.10 | 82.08 ± 38.36 | 120.86 ± 67.79 | 50.45 ± 22.55 |
| OFE-SLP | 75.26 ± 32.99 | 28.09 ± 13.92 | 25.92 ± 12.39 | 38.52 ± 31.77 | 49.11 ± 32.26 |
| Eccentric | |||||
| SLP 60% | 168.86 ± 66.04 | 114.56 ± 56.17 | 39.28 ± 26.53 | 49.32 ± 31.60 | 41.51 ± 23.71 |
| SLP 75% | 196.34 ± 70.17 | 138.85 ± 60.05 | 50.26 ± 27.46 | 68.47 ± 30.36 | 53.89 ± 27.49 |
| BIOFIT-LP 60% | 179.06 ± 59.44 | 138.64 ± 63.56 | 26.94 ± 11.79 | 151.36 ± 89.07 | 24.41 ± 13.89 |
| BIOFIT-LP 75% | 187.59 ± 60.51 | 146.03 ± 68.19 | 32.87 ± 15.79 | 153.58 ± 104.76 | 30.84 ± 18.44 |
| OFE-SLP | 57.08 ± 27.61 | 28.70 ± 19.35 | 16.00 ± 9.36 | 64.52 ± 70.84 | 30.65 ± 23.68 |
| Complete Repetition | SLP 60% | SLP 75% | BIOFIT-LP 60% | BIOFIT-LP 75% | OFE-SLP | |
|---|---|---|---|---|---|---|
| Vastus Lateralis | SLP 60% | - | −41.84 ± 4.48 ⴕ | −19.92 ± 8.38 | −36.82 ± 9.80 ** | 132.285 ± 8.82 ⴕ |
| SLP 75% | 41.84 ± 4.48 ⴕ | - | 21.91 ± 8.16 | 5.01 ± 9.93 | 174.12 ± 10.91 ⴕ | |
| BIOFIT-LP 60% | 19.92 ± 8.38 | −21.91 ± 8.16 | - | −16.90 ± 5.03 * | 152.21 ± 9.76 ⴕ | |
| BIOFIT-LP 75% | 36.82 ± 9.80 ** | −5.01 ± 9.93 | 16.90 ± 5.03 * | - | 169.11 ± 10.82 ⴕ | |
| OFE-SLP | −132.29 ± 8.82 ⴕ | −174.12 ± 10.91 ⴕ | −152.21 ± 9.76 ⴕ | −169.11 ± 10.82 ⴕ | - | |
| Rectus Femoris | SLP 60% | - | −42.02 ± 5.84 ⴕ | −14.30 ± 8.89 | −27.64 ± 10.59 | 104.96 ± 8.03 ⴕ |
| SLP 75% | 42.02 ± 5.84 ⴕ | - | 27.73 ± 10.74 | 14.38 ± 13.28 | 146.98 ± 11.84 ⴕ | |
| BIOFIT-LP 60% | 14.30 ± 8.89 | −27.73 ± 10.74 | - | −13.34 ± 6.40 | 119.26 ± 10.04 ⴕ | |
| BIOFIT-LP 75% | 27.64 ± 10.59 | −14.38 ± 13.28 | 13.34 ± 6.40 | - | 132.60 ± 10.86 ⴕ | |
| OFE-SLP | −104.96 ± 8.03 ⴕ | −146.98 ± 11.84 ⴕ | −119.26 ± 10.04 ⴕ | −132.60 ± 10.86 ⴕ | - | |
| Biceps Femoris | SLP 60% | - | −17.40 ± 3.41 ⴕ | 7.25 ± 5.70 | −3.14 ± 6.75 | 43.55 ± 6.82 ⴕ |
| SLP 75% | 17.40 ± 3.41 ⴕ | - | 24.65 ± 5.99 ** | 14.26 ± 6.80 | 60.94 ± 6.75 ⴕ | |
| BIOFIT-LP 60% | −7.25 ± 5.70 | −24.65 ± 5.99 ** | - | −10.39 ± 2.83 * | 36.29 ± 6.11 ⴕ | |
| BIOFIT-LP 75% | 3.14 ± 6.75 | −14.26 ± 6.80 | 10.39 ± 2.83 * | - | 46.68 ± 6.44 ⴕ | |
| OFE-SLP | −43.55 ± 6.82 ⴕ | −60.94 ± 6.75 ⴕ | −36.29 ± 6.11 ⴕ | −46.68 ± 6.44 ⴕ | - | |
| Tibialis Anterior | SLP 60% | - | −19.78 ± 3.35 ⴕ | −65.39 ± 10.69 ⴕ | −72.54 ± 13.67 ⴕ | 10.12 ± 9.63 |
| SLP 75% | 19.78 ± 3.35 ⴕ | - | −45.61 ± 10.58 ** | −52.75 ± 12.87 ** | 29.90 ± 10.28 | |
| BIOFIT-LP 60% | 65.39 ± 10.69 ⴕ | 45.61 ± 10.58 ** | - | −7.14 ± 8.37 | 75.51 ± 10.48 ⴕ | |
| BIOFIT-LP 75% | 72.54 ± 13.67 ⴕ | 52.75 ± 12.87 ** | 7.14 ± 8.37 | - | 82.65 ± 14.59 ⴕ | |
| OFE-SLP | −10.12 ± 9.63 | −29.90 ± 10.28 | −75.51 ± 10.48 ⴕ | −82.65 ± 14.59 ⴕ | - | |
| Gastrocnemius | SLP 60% | - | −16.22 ± 3.80 ** | 21.96 ± 5.64 ** | 18.32 ± 5.72 * | 21.25 ± 5.78 ** |
| SLP 75% | 16.22 ± 3.80 ** | - | 38.17 ± 5.93 ⴕ | 34.54 ± 6.42 ⴕ | 37.46 ± 6.87 ⴕ | |
| BIOFIT-LP 60% | −21.96 ± 5.64 ** | −38.17 ± 5.93 ⴕ | - | −6.63 ± 2.40 | −0.71 ± 5.56 | |
| BIOFIT-LP 75% | −18.32 ± 5.72 * | −34.54 ± 6.42 ⴕ | 6.63 ± 2.40 | - | 2.93 ± 5.28 | |
| OFE-SLP | −21.25 ± 5.78 ** | −37.46 ± 6.87 ⴕ | 0.71 ± 5.56 | −2.93 ± 5.28 | - | |
| Concentric Phase | SLP 60% | SLP 75% | BIOFIT-LP 60% | BIOFIT-LP 75% | OFE-SLP | |
|---|---|---|---|---|---|---|
| Vastus Lateralis | SLP 60% | - | −49.73 ± 7.90 ⴕ | −26.14 ± 11.69 | −46.17 ± 14.00 * | 149.72 ± 10.35 ⴕ |
| SLP 75% | 49.73 ± 7.90 ⴕ | - | 23.59 ± 10.00 | 3.56 ± 13.40 | 199.45 ± 13.69 ⴕ | |
| BIOFIT-LP 60% | 26.14 ± 11.69 | −23.59 ± 10.00 | - | −20.03 ± 6.41 * | 175.86 ± 13.00 ⴕ | |
| BIOFIT-LP 75% | 46.17 ± 14.00 * | −3.56 ± 13.40 | 20.03 ± 6.41 * | - | 195.89 ± 14.67 ⴕ | |
| OFE-SLP | −149.72 ± 10.35 ⴕ | −199.45 ± 13.69 ⴕ | −175.86 ± 13.00 ⴕ | −195.89 ± 14.67 ⴕ | - | |
| Rectus Femoris | SLP 60% | - | −56.72 ± 8.37 ⴕ | −7.37 ± 11.84 | −25.96 ± 14.09 | 121.75 ± 10.01 ⴕ |
| SLP 75% | 56.72 ± 8.37 ⴕ | - | 49.35 ± 14.86 * | 30.76 ± 17.70 | 178.46 ± 15.09 ⴕ | |
| BIOFIT-LP 60% | 7.37 ± 11.84 | −49.35 ± 14.86 * | - | −18.59 ± 8.61 | 129.11 ± 12.32 ⴕ | |
| BIOFIT-LP 75% | 25.96 ± 14.09 | −30.76 ± 17.70 | 18.59 ± 8.61 | - | 147.71 ± 12.19 ⴕ | |
| OFE-SLP | −121.75 ± 10.01 ⴕ | −178.46 ± 15.09 ⴕ | −129.11 ± 12.32 ⴕ | −147.71 ± 12.19 ⴕ | - | |
| Biceps Femoris | SLP 60% | - | −18.72 ± 4.68 ** | 7.97 ± 7.31 | −4.98 ± 8.76 | 51.19 ± 7.05 ⴕ |
| SLP 75% | 18.72 ± 4.68 ** | - | 26.69 ± 7.99 * | 13.75 ± 8.90 | 69.91 ± 7.75 ⴕ | |
| BIOFIT-LP 60% | −7.97 ± 7.31 | −26.69 ± 7.99 * | - | −12.94 ± 3.82 * | 43.22 ± 5.72 ⴕ | |
| BIOFIT-LP 75% | 4.98 ± 8.76 | −13.75 ± 8.90 | 12.94 ± 3.82 * | - | 56.17 ± 7.00 ⴕ | |
| OFE-SLP | −51.19 ± 7.05 ⴕ | −69.91 ± 7.75 ⴕ | −43.22 ± 5.72 ⴕ | −56.17 ± 7.00 ⴕ | - | |
| Tibialis Anterior | SLP 60% | - | −18.82 ± 3.91 ⴕ | −22.49 ± 9.25 | −39.24 ± 13.60 | 43.11 ± 8.65 ⴕ |
| SLP 75% | 18.82 ± 3.91 ⴕ | - | −3.67 ± 8.61 | −20.42 ± 12.53 | 61.92 ± 9.58 ⴕ | |
| BIOFIT-LP 60% | 22.49 ± 9.25 | 3.67 ± 8.61 | - | −16.75 ± 9.42 | 68.59 ± 9.80 ⴕ | |
| BIOFIT-LP 75% | 39.24 ± 13.60 | 20.42 ± 12.53 | 16.75 ± 9.42 | - | 82.34 ± 13.03 ⴕ | |
| OFE-SLP | −43.11 ± 8.65 ⴕ | −61.92 ± 9.58 ⴕ | −68.59 ± 9.80 ⴕ | −82.34 ± 13.03 ⴕ | - | |
| Gastrocnemius | SLP 60% | - | −15.02 ± 4.80 * | 26.96 ± 7.39 * | 25.38 ± 7.21 * | 26.72 ± 7.11 ** |
| SLP 75% | 15.02 ± 4.80 * | - | 41.98 ± 6.56 ⴕ | 40.40 ± 6.91 ⴕ | 41.74 ± 6.85 ⴕ | |
| BIOFIT-LP 60% | −26.96 ± 7.39 * | −41.98 ± 6.56 ⴕ | - | −1.59 ± 3.29 | −0.24 ± 6.95 | |
| BIOFIT-LP 75% | −25.38 ± 7.21 * | −40.40 ± 6.91 ⴕ | 1.59 ± 3.29 | - | 1.35 ± 6.40 | |
| OFE-SLP | −26.72 ± 7.11 ** | −41.74 ± 6.85 ⴕ | 0.24 ± 6.95 | −1.35 ± 6.40 | - | |
| Eccentric Phase | SLP 60% | SLP 75% | BIOFIT-LP 60% | BIOFIT-LP 75% | OFE-SLP | |
|---|---|---|---|---|---|---|
| Vastus Lateralis | SLP 60% | - | −27.48 ± 3.49 ⴕ | −10.20 ± 7.63 | −18.73 ± 7.11 | 111.79 ± 8.78 ⴕ |
| SLP 75% | 27.48 ± 3.49 ⴕ | - | 17.28 ± 8.74 | 8.75 ± 8.02 | 139.27 ± 9.61 ⴕ | |
| BIOFIT-LP 60% | 10.20 ± 7.63 | −17.28 ± 8.74 | - | −8.53 ± 4.09 | 121.99 ± 7.41 ⴕ | |
| BIOFIT-LP 75% | 18.73 ± 7.11 | −8.75 ± 8.02 | 8.53 ± 4.09 | - | 130.52 ± 7.55 ⴕ | |
| OFE-SLP | −111.79 ± 8.78 ⴕ | −139.27 ± 9.61 ⴕ | −121.99 ± 7.41 ⴕ | −130.52 ± 7.55 ⴕ | - | |
| Rectus Femoris | SLP 60% | - | −24.29 ± 6.01 ** | −24.08 ± 11.08 | −31.47 ± 11.64 | 85.86 ± 8.64 ⴕ |
| SLP 75% | 24.29 ± 6.01 ** | - | 0.21 ± 10.15 | −7.18 ± 11.48 | 110.15 ± 9.63 ⴕ | |
| BIOFIT-LP 60% | 24.08 ± 11.08 | −0.21 ± 10.15 | - | −7.39 ± 6.28 | 109.94 ± 9.10 ⴕ | |
| BIOFIT-LP 75% | 31.47 ± 11.64 | 7.18 ± 11.48 | 7.39 ± 6.28 | - | 117.33 ± 10.15 ⴕ | |
| OFE-SLP | −85.86 ± 8.64 ⴕ | −110.15 ± 9.63 ⴕ | −109.94 ± 9.10 ⴕ | −117.33 ± 10.15 ⴕ | - | |
| Biceps Femoris | SLP 60% | - | −10.97 ± 2.70 ** | 12.35 ± 4.19 | 6.41 ± 4.27 | 23.28 ± 4.46 ⴕ |
| SLP 75% | 10.97 ± 2.70 ** | - | 23.32 ± 4.43 ⴕ | 17.38 ± 4.58 ** | 34.25 ± 4.15 ⴕ | |
| BIOFIT-LP 60% | −12.35 ± 4.19 | −23.32 ± 4.43 ⴕ | - | −5.94 ± 1.51 ** | 10.94 ± 2.41 ** | |
| BIOFIT-LP 75% | −6.41 ± 4.27 | −17.38 ± 4.58 ** | 5.94 ± 1.51 ** | - | 16.87 ± 2.92 ⴕ | |
| OFE-SLP | −23.28 ± 4.46 ⴕ | −34.25 ± 4.15 ⴕ | −10.94 ± 2.41 ** | −16.87 ± 2.92 ⴕ | - | |
| Tibialis Anterior | SLP 60% | - | −19.16 ± 3.49 ⴕ | −102.04 ± 14.40 ⴕ | −104.26 ± 16.56 ⴕ | −15.20 ± 11.15 |
| SLP 75% | 19.16 ± 3.49 ⴕ | - | −82.89 ± 15.02 ⴕ | −85.11 ± 16.76 ⴕ | 3.95 ± 11.70 | |
| BIOFIT-LP 60% | 102.04 ± 14.40 ⴕ | 82.89 ± 15.02 ⴕ | - | −2.22 ± 9.75 | 86.84 ± 13.62 ⴕ | |
| BIOFIT-LP 75% | 104.26 ± 16.56 ⴕ | 85.11 ± 16.76 ⴕ | 2.22 ± 9.75 | - | 89.06 ± 17.86 ⴕ | |
| OFE-SLP | 15.20 ± 11.15 | −3.95 ± 11.70 | −86.84 ± 13.62 ⴕ | −89.06 ± 17.86 ⴕ | - | |
| Gastrocnemius | SLP 60% | - | −12.38 ± 2.44 ⴕ | 17.11 ± 4.54 ** | 10.67 ± 4.70 | 10.86 ± 4.30 |
| SLP 75% | 12.38 ± 2.44 ⴕ | - | 29.48 ± 5.20 ⴕ | 23.04 ± 5.32 ** | 23.24 ± 4.90 ** | |
| BIOFIT-LP 60% | −17.11 ± 4.54 ** | −29.48 ± 5.20 ⴕ | - | −6.44 ± 1.73 ** | −6.25 ± 3.94 | |
| BIOFIT-LP 75% | −10.67 ± 4.70 | −23.04 ± 5.32 ** | 6.44 ± 1.73 ** | - | 0.19 ± 4.47 | |
| OFE-SLP | −10.86 ± 4.30 | −23.24 ± 4.90 ** | 6.25 ± 3.94 | −0.19 ± 4.47 | - | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abelleira-Lamela, T.; Marcos-Pardo, P.J.; Abraldes, J.A.; González-Gálvez, N.; Espeso-García, A.; Esparza-Ros, F.; Vaquero-Cristóbal, R. Comparative Electromyographic Analysis in Leg Press of Traditional Fitness Equipment, Traditional Outdoor Fitness Equipment, and a New Model of Outdoor Fitness Equipment in Trained Young Men. Appl. Sci. 2024, 14, 7390. https://doi.org/10.3390/app14167390
Abelleira-Lamela T, Marcos-Pardo PJ, Abraldes JA, González-Gálvez N, Espeso-García A, Esparza-Ros F, Vaquero-Cristóbal R. Comparative Electromyographic Analysis in Leg Press of Traditional Fitness Equipment, Traditional Outdoor Fitness Equipment, and a New Model of Outdoor Fitness Equipment in Trained Young Men. Applied Sciences. 2024; 14(16):7390. https://doi.org/10.3390/app14167390
Chicago/Turabian StyleAbelleira-Lamela, Tomás, Pablo Jorge Marcos-Pardo, José Arturo Abraldes, Noelia González-Gálvez, Alejandro Espeso-García, Francisco Esparza-Ros, and Raquel Vaquero-Cristóbal. 2024. "Comparative Electromyographic Analysis in Leg Press of Traditional Fitness Equipment, Traditional Outdoor Fitness Equipment, and a New Model of Outdoor Fitness Equipment in Trained Young Men" Applied Sciences 14, no. 16: 7390. https://doi.org/10.3390/app14167390