
Long-Term Outcomes of Collagen Matrix versus Subepithelial Connective Tissue in Root Coverage for Multiple Teeth: A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Eligibility Criteria
- Studies involving collagen matrix and subepithelial connective tissue;
- Cases with multiple recessions;
- Studies focused on natural teeth;
- Randomized controlled trials (RCTs).
- Patients who have undergone implant procedures;
- Patients with dentures;
- Studies on root coverage that do not involve the use of either collagen matrix or subepithelial connective tissue;
- Cases involving a single gingival recession.
2.2. Information Sources and Search Strategy
2.3. Study Selection and Data Extraction
2.4. Risk of Bias Assessment
2.5. Data Synthesis and Analysis
3. Results
3.1. Study Selection and Data Extraction
3.2. Risk of Bias Assessment
3.3. Meta-Analysis
3.3.1. Type of Gingival Recession
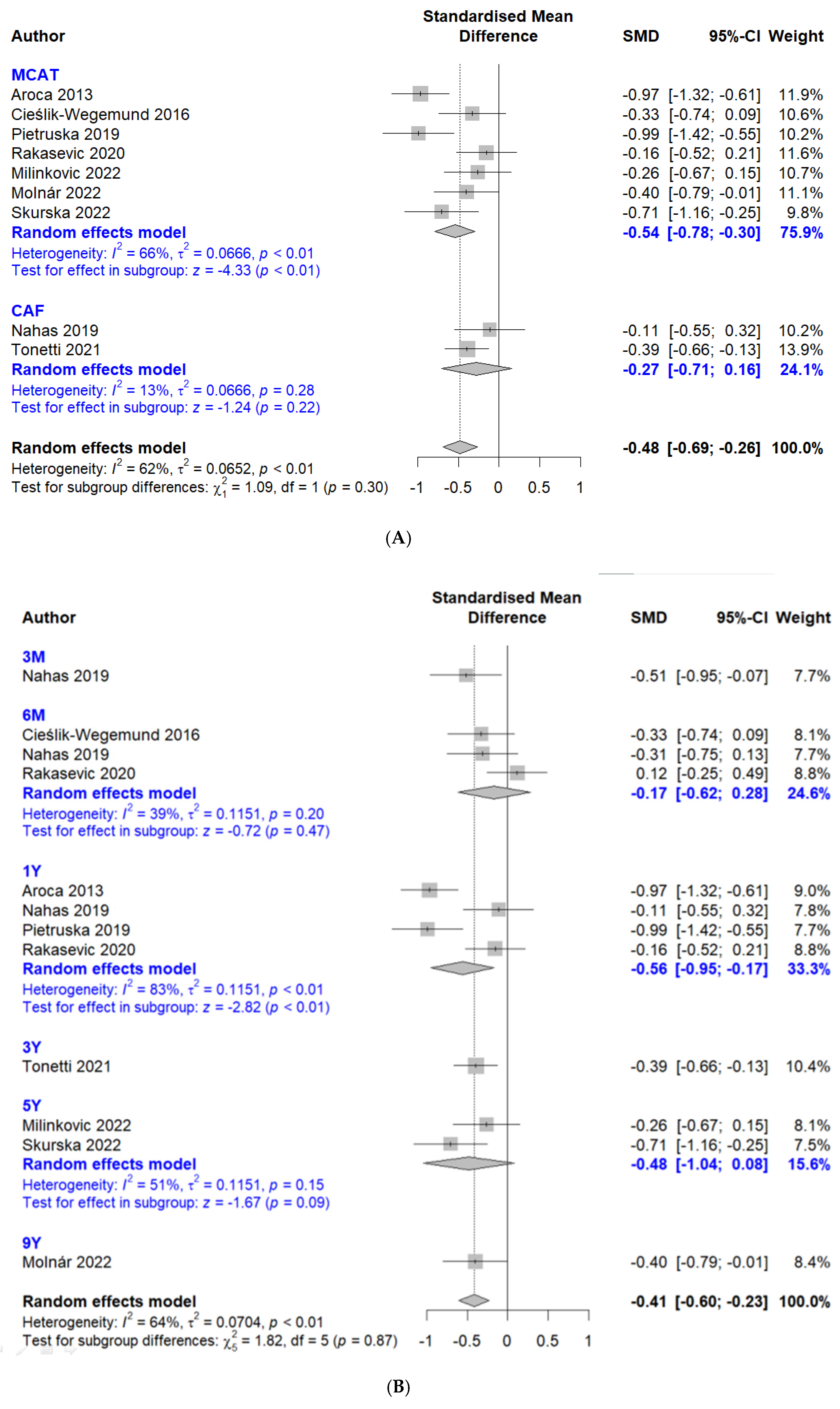
3.3.2. Mean Root Coverage
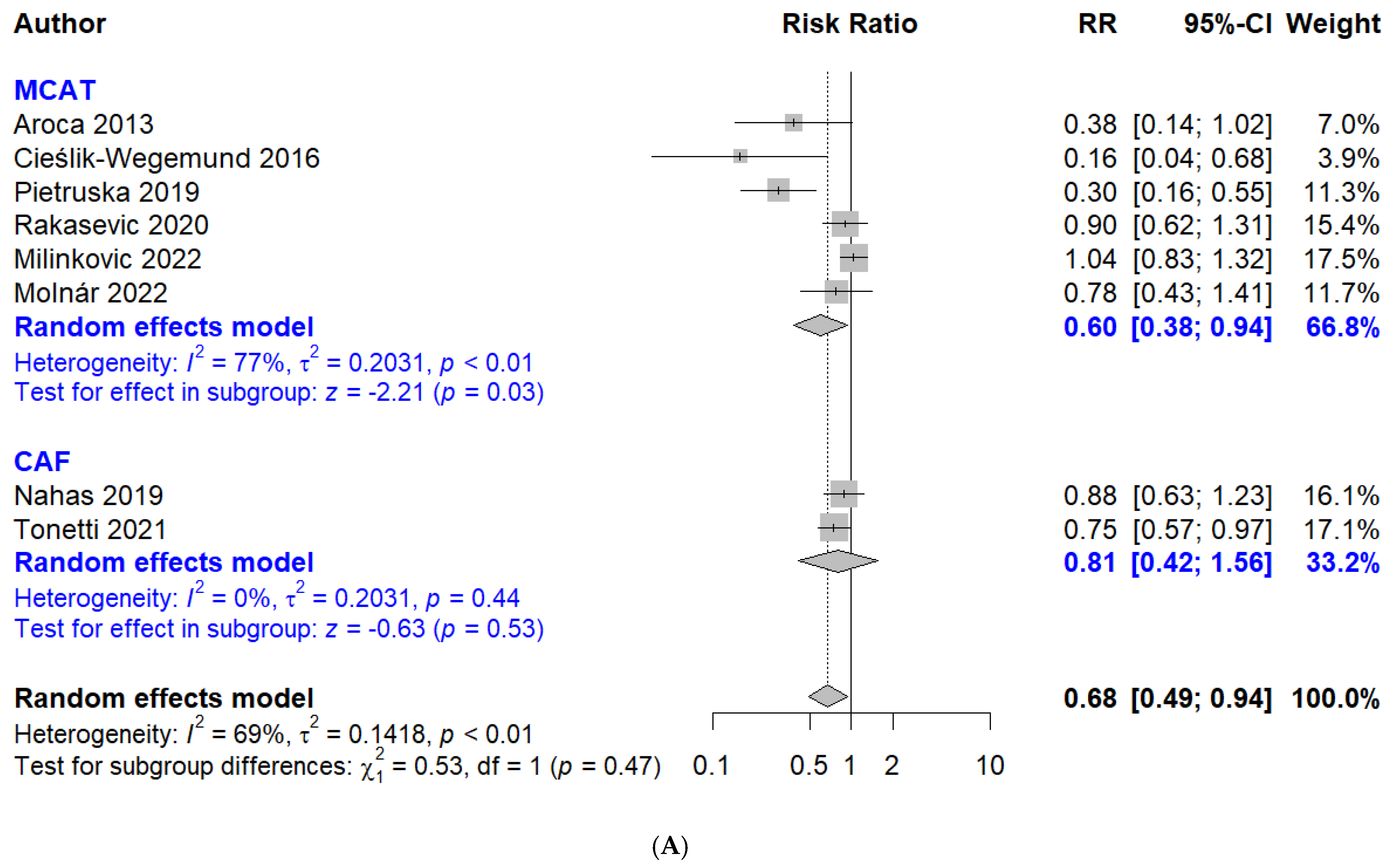
3.3.3. Complete Root Coverage
3.3.4. Width of Keratinized Tissue
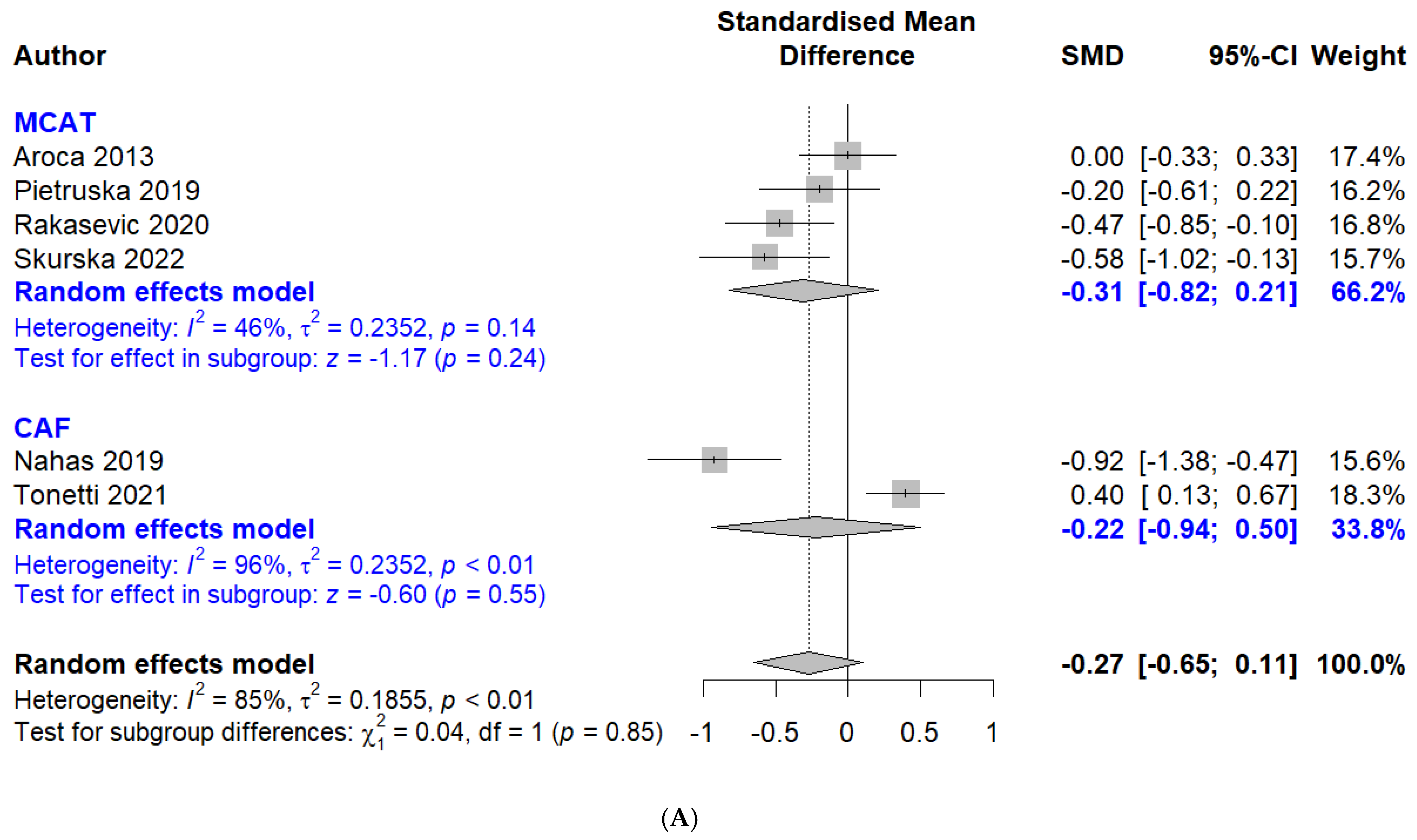
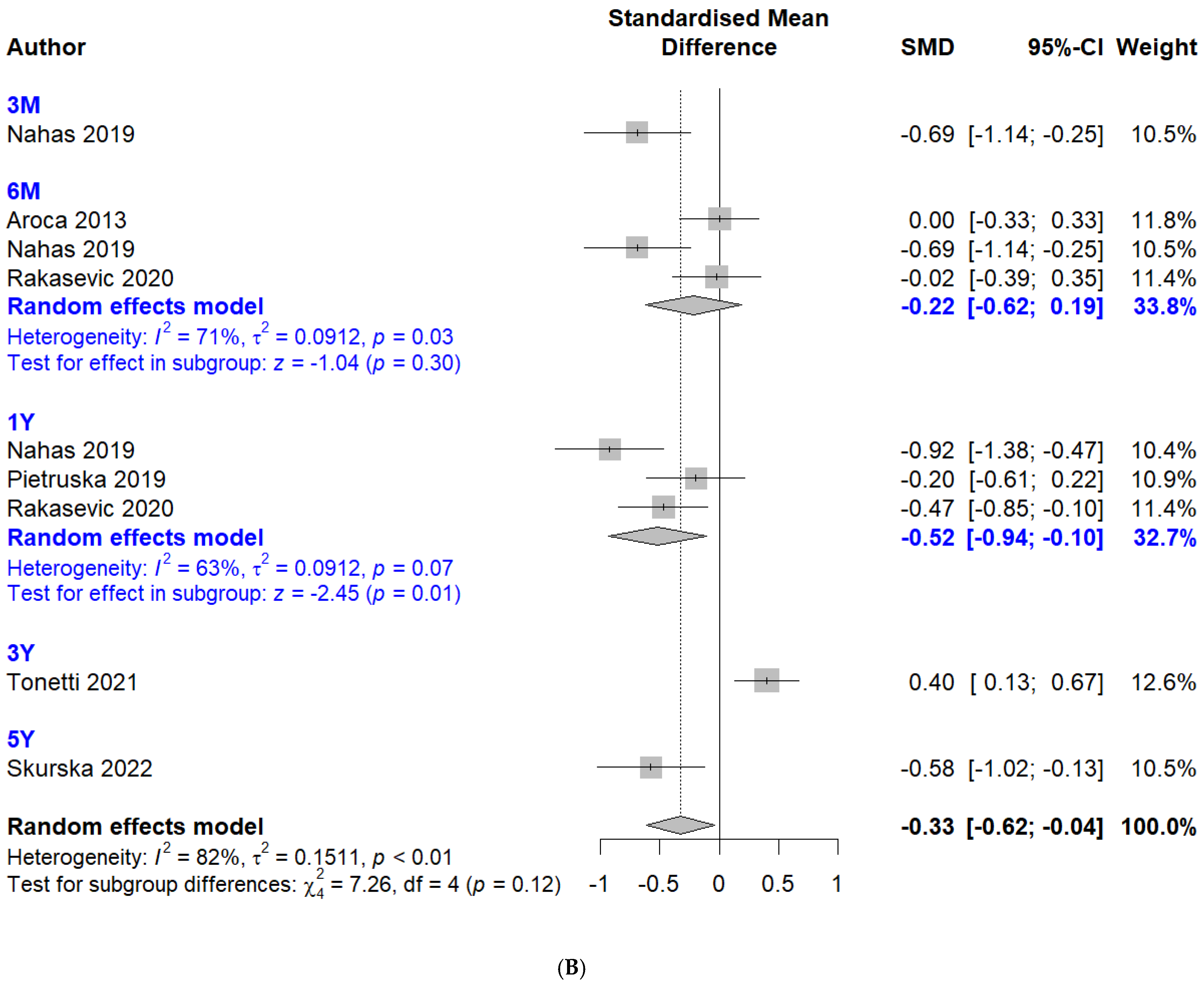
3.3.5. Probing Depth
3.3.6. Sensitivity Meta-Analysis
3.3.7. Publication Bias Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lee, C.T.; Lange, M.; Jureidini, A.; Bittner, N.; Schulze-Späte, U. Clinical and patient-reported outcomes after recession coverage using modified vestibular incision subperiosteal tunnel access with a volume-stable collagen matrix as compared to a coronally advanced flap with a subepithelial connective tissue graft. J. Periodontal Implant. Sci. 2022, 52, 466–478. [Google Scholar] [CrossRef] [PubMed]
- Mythri, S.; Arunkumar, S.M.; Hegde, S.; Rajesh, S.K.; Munaz, M.; Ashwin, D. Etiology and occurrence of gingival recession—An epidemiological study. J. Indian. Soc. Periodontol. 2015, 19, 671–675. [Google Scholar] [CrossRef]
- Jati, A.S.; Furquim, L.Z.; Consolaro, A. Gingival recession: Its causes and types, and the importance of orthodontic treatment. Dent. Press J. Orthod. 2016, 21, 18–29. [Google Scholar] [CrossRef]
- Kerner, S.; Borghetti, A.; Katsahian, S.; Etienne, D.; Malet, J.; Mora, F.; Monnet-Corti, V.; Glise, J.-M.; Bouchard, P. A retrospective study of root coverage procedures using an image analysis system. J. Clin. Periodontol. 2008, 35, 346–355. [Google Scholar] [CrossRef]
- Tian, W.; Hu, F.; Zhou, X. Comparative Evaluation of Connective Tissue Graft with Pouch/Tunnel Technique versus Connective Tissue Graft with Coronally Advanced Tunnel Flap for the Treatment of Maxillary Recession Cases in Severe Periodontitis. Tissue Eng. Regen. Med. 2021, 18, 1001–1007. [Google Scholar] [CrossRef]
- Langer, B.; Langer, L. Subepithelial connective tissue graft technique for root coverage. J. Periodontol. 1985, 56, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.T.; Chang, P.C.; Touchan, N.; Royzman, D. Root coverage with a modified laterally positioned flap combined with a subepithelial connective tissue graft in advanced recession. J. Periodontal Implant. Sci. 2014, 44, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Smirani, R.; Rémy, M.; Devillard, R.; Naveau, A. Use of Human Gingival Fibroblasts for Pre-Vascularization Strategies in Oral Tissue Engineering. Tissue Eng. Regen. Med. 2022, 19, 525–535. [Google Scholar] [CrossRef]
- Park, J.B. Treatment of multiple gingival recessions using subepithelial connective tissue grafting with a single-incision technique. J. Oral. Sci. 2009, 51, 317–321. [Google Scholar] [CrossRef]
- Lee, Y.; Lee, D.; Kim, S.; Ku, Y.; Rhyu, I.C. Modified tunneling technique for root coverage of anterior mandible using minimal soft tissue harvesting and volume-stable collagen matrix: A retrospective study. J. Periodontal Implant. Sci. 2021, 51, 398–408. [Google Scholar] [CrossRef]
- Park, J.B. Root coverage with 2 connective tissue grafts obtained from the same location using a single-incision technique. Quintessence Int. 2009, 40, 371–376. [Google Scholar]
- Godat, M.S.; Gruen, T.D.; Miller, P.D.; Craddock, R.D. Use of Tuberosity Connective Tissue for Root Coverage and Ridge Augmentation: Background and Technique. Compend. Contin. Educ. Dent. 2018, 39, 533–539; quiz 540. [Google Scholar]
- Barootchi, S.; Rodriguez, M.V.; Chan, H.L.; Kripfgans, O.D.; Wang, H.L.; Tavelli, L. Coronally Advanced Flap with Xenogeneic Collagen Matrix for the Treatment of Gingival Recessions at Sites Presenting with Cervical Restorations or Noncarious Cervical Lesions: A Clinical and Ultrasonographic Study. Int. J. Periodontics Restor. Dent. 2023, 43, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Michels, R.; Magrin, G.L.; Cruz, A.; Magini, R.S.; Benfatti, C.A.M. Functionalization of a Volume-Stable Collagen Matrix Using Liquid Platelet-Rich Fibrin: A Case Report Presenting a New Approach for Root Coverage. Case Rep. Dent. 2023, 2023, 3929269. [Google Scholar] [CrossRef]
- Parma-Benfenati, S.; Mastrangelo, F.; Cardo, F.; Roncati, M.; Parma-Benfenati, L.; Aimetti, M.; Nevins, M. Evaluation of a New Porcine Collagen Matrix for the Treatment of Buccal Gingival Recessions: A 12-Month Pilot Prospective Human Study Model. Int. J. Periodontics Restor. Dent. 2023, 43, 329–335. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions. 2023. Version 6.4. [Updated August 2023]. Available online: https://training.cochrane.org/handbook (accessed on 10 June 2024).
- Atieh, M.A.; Almatrooshi, A.; Shah, M.; Hannawi, H.; Tawse-Smith, A.; Alsabeeha, N.H.M. Airflow for initial nonsurgical treatment of peri-implantitis: A systematic review and meta-analysis. Clin. Implant. Dent. Relat. Res. 2022, 24, 196–210. [Google Scholar] [CrossRef]
- Aroca, S.; Molnár, B.; Windisch, P.; Gera, I.; Salvi, G.E.; Nikolidakis, D.; Sculean, A. Treatment of multiple adjacent Miller class I and II gingival recessions with a Modified Coronally Advanced Tunnel (MCAT) technique and a collagen matrix or palatal connective tissue graft: A randomized, controlled clinical trial. J. Clin. Periodontol. 2013, 40, 713–720. [Google Scholar] [CrossRef] [PubMed]
- Cieślik-Wegemund, M.; Wierucka-Młynarczyk, B.; Tanasiewicz, M.; Gilowski, Ł. Tunnel Technique With Collagen Matrix Compared With Connective Tissue Graft for Treatment of Periodontal Recession: A Randomized Clinical Trial. J. Periodontol. 2016, 87, 1436–1443. [Google Scholar] [CrossRef]
- Nahas, R.; Gondim, V.; Carvalho, C.V.; Calderero, L.M.; Rosa, E.F.; Sakiyama, T.; Neto, J.B.C.; Pannuti, C.M.; Romito, G.A. Treatment of multiple recessions with collagen matrix versus connective tissue: A randomized clinical trial. Braz. Oral. Res. 2019, 33, e123. [Google Scholar] [CrossRef]
- Pietruska, M.; Skurska, A.; Podlewski, Ł.; Milewski, R.; Pietruski, J. Clinical evaluation of Miller class I and II recessions treatment with the use of modified coronally advanced tunnel technique with either collagen matrix or subepithelial connective tissue graft: A randomized clinical study. J. Clin. Periodontol. 2019, 46, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Rakasevic, D.L.; Milinkovic, I.Z.; Jankovic, S.M.; Soldatovic, I.A.; Aleksic, Z.M.; Nikolic-Jakoba, N.S. The use of collagen porcine dermal matrix and connective tissue graft with modified coronally advanced tunnel technique in the treatment of multiple adjacent type I gingival recessions: A randomized, controlled clinical trial. J. Esthet. Restor. Dent. 2020, 32, 681–690. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, M.S.; Cortellini, P.; Bonaccini, D.; Deng, K.; Cairo, F.; Allegri, M.; Conforti, G.; Graziani, F.; Guerrero, A.; Halben, J.; et al. Autologous connective tissue graft or xenogenic collagen matrix with coronally advanced flaps for coverage of multiple adjacent gingival recession. 36-month follow-up of a randomized multicentre trial. J. Clin. Periodontol. 2021, 48, 962–969. [Google Scholar] [CrossRef] [PubMed]
- Milinkovic, I.; Rakasevic, D.; Nikolic-Jakoba, N.; Jankovic, S.; Aleksic, Z. Collagen tissue matrix versus connective tissue graft with modified coronally advanced tunnel technique in the multiple gingival recessions treatment: Split-mouth study with 5-year of follow-up. J. Clin. Periodontol. 2022, 49, 200. [Google Scholar]
- Molnár, B.; Aroca, S.; Dobos, A.; Orbán, K.; Szabó, J.; Windisch, P.; Stähli, A.; Sculean, A. Treatment of multiple adjacent RT 1 gingival recessions with the modified coronally advanced tunnel (MCAT) technique and a collagen matrix or palatal connective tissue graft: 9-year results of a split-mouth randomized clinical trial. Clin. Oral. Investig. 2022, 26, 7135–7142. [Google Scholar] [CrossRef]
- Skurska, A.; Milewski, R.; Pietruska, M. Long-Term Clinical Assessment of Two Modifications of Tunnel Technique in Treatment of Cairo Recession Type 1 in Lower Jaw. Int. J. Environ. Res. Public Health 2022, 19, 16444. [Google Scholar] [CrossRef]
- Miller, P.D., Jr. A classification of marginal tissue recession. Int. J. Periodontics Restor. Dent. 1985, 5, 8–13. [Google Scholar]
- Cairo, F.; Nieri, M.; Cincinelli, S.; Mervelt, J.; Pagliaro, U. The interproximal clinical attachment level to classify gingival recessions and predict root coverage outcomes: An explorative and reliability study. J. Clin. Periodontol. 2011, 38, 661–666. [Google Scholar] [CrossRef]
- Spahr, A.; Haegewald, S.; Tsoulfidou, F.; Rompola, E.; Heijl, L.; Bernimoulin, J.; Ring, C.; Sander, S.; Haller, B. Coverage of Miller class I and II recession defects using enamel matrix proteins versus coronally advanced flap technique: A 2-year report. J. Periodontol. 2005, 76, 1871–1880. [Google Scholar] [CrossRef]
- Fernández-Jiménez, A.; García-De-La-Fuente, A.M.; Estefanía-Fresco, R.; Marichalar-Mendia, X.; Aguirre-Urizar, J.M.; Aguirre-Zorzano, L.A. Complete root coverage in the treatment of Miller class III or RT2 gingival recessions: A systematic review and meta-analysis. BMC Oral. Health 2021, 21, 145. [Google Scholar]
- Amarante, E.S.; Leknes, K.N.; Skavland, J.; Lie, T. Coronally positioned flap procedures with or without a bioabsorbable membrane in the treatment of human gingival recession. J. Periodontol. 2000, 71, 989–998. [Google Scholar] [CrossRef] [PubMed]
- Dwarakanath, C.D.; Divya, B.; Sruthima, G.N.; Penmetsa, G.S. Sub-epithelial connective tissue graft for root coverage in nonsmokers and smokers: A pilot comparative clinical study. J. Indian. Soc. Periodontol. 2016, 20, 435–440. [Google Scholar] [PubMed]
- Roman, A.; Câmpian, R.; Domşa, I.; Soancă, A.; Gocan, H. Subepithelial connective tissue graft for root coverage: Clinical case reports and histologic evaluation. Rom. J. Morphol. Embryol. 2010, 51, 793–797. [Google Scholar]
- Kumari, K.; Nath, B.; Kumar, A.; Chhabada, A.K.; Kumari, R.; Prakash, G. Comparison of Root Coverage by the Subepithelial Connective Tissue Graft With and Without Root Biomodification: A Comprehensive Clinical Study. Cureus 2023, 15, e44758. [Google Scholar] [CrossRef]
- Tatarakis, N.; Gkranias, N.; Darbar, U.; Donos, N. Blood flow changes using a 3D xenogeneic collagen matrix or a subepithelial connective tissue graft for root coverage procedures: A pilot study. Clin. Oral. Investig. 2018, 22, 1697–1705. [Google Scholar] [CrossRef] [PubMed]
- Herford, A.S.; Akin, L.; Cicciu, M.; Maiorana, C.; Boyne, P.J. Use of a porcine collagen matrix as an alternative to autogenous tissue for grafting oral soft tissue defects. J. Oral. Maxillofac. Surg. 2010, 68, 1463–1470. [Google Scholar] [CrossRef]
- Petrie, K.; Cox, C.T.; Becker, B.C.; MacKay, B.J. Clinical applications of acellular dermal matrices: A review. Scars Burn. Heal. 2022, 8, 20595131211038313. [Google Scholar] [CrossRef]
- Ashurko, I.; Tarasenko, S.; Magdalyanova, M.; Bokareva, S.; Balyasin, M.; Galyas, A.; Khamidova, M.; Zhornik, M.; Unkovskiy, A. Comparative analysis of xenogeneic collagen matrix and autogenous subepithelial connective tissue graft to increase soft tissue volume around dental implants: A systematic review and meta-analysis. BMC Oral. Health 2023, 23, 741. [Google Scholar] [CrossRef]
- Raguse, J.D.; Gath, H.J. A metabolically active dermal replacement (Dermagraft) for vestibuloplasty. J. Oral. Rehabil. 2005, 32, 337–340. [Google Scholar] [CrossRef]
- De Santis, D.; Luciano, U.; Pancera, P.; Castegnaro, G.; Alberti, C.; Gelpi, F. A New Matrix for Soft Tissue Management. J. Clin. Med. 2022, 11, 4486. [Google Scholar] [CrossRef]
- Stefanini, M.; Mounssif, I.; Barootchi, S.; Tavelli, L.; Wang, H.L.; Zucchelli, G. An exploratory clinical study evaluating safety and performance of a volume-stable collagen matrix with coronally advanced flap for single gingival recession treatment. Clin. Oral. Investig. 2020, 24, 3181–3191. [Google Scholar] [CrossRef] [PubMed]
- McGuire, M.K.; Scheyer, E.T. Xenogeneic collagen matrix with coronally advanced flap compared to connective tissue with coronally advanced flap for the treatment of dehiscence-type recession defects. J. Periodontol. 2010, 81, 1108–1117. [Google Scholar] [CrossRef]
- Barakat, H.; Dayoub, S. Treatment of miller type I and II gingival recession defects using three-dimensional porcine collagen matrix with coronally advanced flap: A randomized clinical split-mouth trial (a 1-year follow-up). Indian. J. Dent. Res. 2020, 31, 209–216. [Google Scholar] [CrossRef]
- Fathiazar, A.; Shariatmadar Ahmadi, R.; Sayar, F. A Comparison between Mucoderm® and Connective Tissue Graft for Root Coverage. J. Dent. 2022, 23, 402–409. [Google Scholar]
- Schinini, G.; Molinari, A.; Romanelli, H. Clinical evaluation of root coverage using coronally positioned flap associated with acellular dermal matrix allograft in single-type recession defects. A retrospective study. Acta Odontol. Latinoam. 2021, 34, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Zeng, A.; Li, H.; Liu, J.; Wu, M. The Progress of Decellularized Scaffold in Stomatology. Tissue Eng. Regen. Med. 2022, 19, 451–461. [Google Scholar] [CrossRef] [PubMed]
- Ahn, W.B.; Lee, Y.B.; Ji, Y.H.; Moon, K.S.; Jang, H.S.; Kang, S.W. Decellularized Human Adipose Tissue as an Alternative Graft Material for Bone Regeneration. Tissue Eng. Regen. Med. 2022, 19, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Tavelli, L.; Barootchi, S.; Rodriguez, M.V.; Mancini, L.; Majzoub, J.; Travan, S.; Sugai, J.; Chan, H.L.; Kripfgans, O.; Wang, H.L.; et al. Recombinant human platelet-derived growth factor improves root coverage of a collagen matrix for multiple adjacent gingival recessions: A triple-blinded, randomized, placebo-controlled trial. J. Clin. Periodontol. 2022, 49, 1169–1184. [Google Scholar] [CrossRef]
- Toledano-Osorio, M.; Muñoz-Soto, E.; Toledano, M.; Vallecillo-Rivas, M.; Vallecillo, C.; Ramos-García, P.; Osorio, R. Treating Gingival Recessions Using Coronally Advanced Flap or Tunnel Techniques with Autografts or Polymeric Substitutes: A Systematic Review and Meta-Analysis. Polymers 2022, 14, 1453. [Google Scholar] [CrossRef]
- Shkreta, M.; Atanasovska-Stojanovska, A.; Dollaku, B.; Belazelkoska, Z. Exploring the Gingival Recession Surgical Treatment Modalities: A Literature Review. Open Access Maced. J. Med. Sci. 2018, 6, 698–708. [Google Scholar] [CrossRef]
- Mayta-Tovalino, F.; Barboza, J.J.; Pasupuleti, V.; Hernandez, A.V. Efficacy of Tunnel Technique (TUN) versus Coronally Advanced Flap (CAF) in the Management of Multiple Gingival Recession Defects: A Meta-Analysis. Int. J. Dent. 2023, 2023, 8671484. [Google Scholar] [CrossRef] [PubMed]
- Chambrone, L.; Chambrone, D.; Pustiglioni, F.E.; Chambrone, L.A.; Lima, L.A. Can subepithelial connective tissue grafts be considered the gold standard procedure in the treatment of Miller Class I and II recession-type defects? J. Dent. 2008, 36, 659–671. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Lorenzo, R.; Aranda, J.J.; Martin, C.; Orsini, M. Clinical evaluation of a new collagen matrix (Mucograft prototype) to enhance the width of keratinized tissue in patients with fixed prosthetic restorations: A randomized prospective clinical trial. J. Clin. Periodontol. 2009, 36, 868–876. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.H.; Kim, B.O.; Jang, H.S. Clinical evaluation of a collagen matrix to enhance the width of keratinized gingiva around dental implants. J. Periodontal Implant. Sci. 2010, 40, 96–101. [Google Scholar] [CrossRef]
- Naomi, R.; Ardhani, R.; Hafiyyah, O.A.; Fauzi, M.B. Current Insight of Collagen Biomatrix for Gingival Recession: An Evidence-Based Systematic Review. Polymers 2020, 12, 2081. [Google Scholar] [CrossRef]
- Monaghan, T.F.; Agudelo, C.W.; Rahman, S.N.; Wein, A.J.; Lazar, J.M.; Everaert, K.; Dmochowski, R.R. Blinding in Clinical Trials: Seeing the Big Picture. Medicina 2021, 57, 647. [Google Scholar] [CrossRef]
- Fernandez, Y.G.E.; Nguyen, H.; Duan, N.; Gabler, N.B.; Kravitz, R.L. Assessing Heterogeneity of Treatment Effects: Are Authors Misinterpreting Their Results? Health Serv. Res. 2010, 45, 283–301. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Author (Year) | Study Design | Sample Size (Test/Control) (Participants/Tooth) | Test Procedure | Control Procedure | Type of Recession | Follow-Up |
|---|---|---|---|---|---|---|
| Aroca (2013) [19] | RCT (split-mouth) | (22/78):(22/78) | CM + MCAT | CTG + MCAT | Miller class I and II | 1Y |
| Cieślik-Wegemund (2016) [20] | RCT (parallel) | (14/59):(14/47) | CM + MCAT | CTG + MCAT | Miller class I and II | 3M, 6M |
| Nahas (2019) [21] | RCT (split-mouth) | (15/42):(15/40) | CM + CAF | CTG + CAF | Miller class I | 3M, 6M, 1Y |
| Pietruska (2019) [22] | RCT (split-mouth) | (20/46):(20/45) | CM + MCAT | CTG + MCAT | Miller class I and II | 1Y |
| Rakasevic (2020) [23] | RCT (split-mouth) | (20/62):(20/52) | CM + MCAT | CTG + MCAT | Miller class I | 6M, 1Y |
| Tonetti (2021) [24] | RCT (parallel) | (44/107):(45/112) | CM + CAF | CTG + CAF | Inclusion: recession ≥ 3 mm; exclusion: inter-dental attachment loss greater than 1 mm, or furcation involvement | 3Y |
| Milinkovic (2022) [25] | RCT (split-mouth) | (15/39):(15/57) | CM + MCAT | CTG + MCAT | Recession type 1 | 5Y |
| Molnár (2022) [26] | RCT (split-mouth) | (16/57):(16/57) | CM + MCAT | CTG + MCAT | Recession type 1 | 9Y |
| Skurska (2022) [26] | RCT (split-mouth) | (18/40):(18/40) | CM + MCAT | CTG + MCAT | Recession type 1 | 5Y |
| Study Author (Year) | Mean Root Coverage | Complete Root Coverage | Keratinized Tissue Width | Probing Depth | |||||
|---|---|---|---|---|---|---|---|---|---|
| Test | Control | Test | Control | Test | Control | Test | Control | F/U Period | |
| Aroca (2013) [19] | 71.00 ± 21.00 | 90.00 ± 18.00 | 5/22 | 13/22 | 0.30 ± 0.59 | 0.70 ± 0.67 | 0.00 ± 0.26 | 0.00 ± 0.26 | 1Y |
| Cieślik-Wegemund (2016) [20] | NR | NR | NR | NR | 0.80 ± 1.67 | 1.00 ± 1.61 | NR | NR | 3M |
| Cieślik-Wegemund (2016) [20] | 91.00 ± 13.00 | 95.00 ± 11.00 | 2/14 | 10/14 | 0.80 ± 1.67 | 1.00 ± 1.61 | NR | NR | 6M |
| Nahas (2019) [21] | 66.67 ± 39.02 | 85.71 ± 34.07 | 19/42 | 26/40 | 0.40 ± 0.90 | 1.20 ± 1.30 | 0.10 ± 0.40 | 0.40 ± 0.46 | 3M |
| Nahas (2019) [21] | 77.78 ± 39.02 | 89.29 ± 34.07 | 25/42 | 32/40 | 0.40 ± 1.00 | 1.20 ± 1.00 | 0.10 ± 0.40 | 0.40 ± 0.46 | 6M |
| Nahas (2019) [21] | 77.78 ± 39.02 | 82.14 ± 36.25 | 25/42 | 27/40 | 0.30 ± 0.70 | 1.20 ± 1.10 | 0.10 ± 0.40 | 0.50 ± 0.46 | 1Y |
| Pietruska (2019) [22] | 53.20 ± 32.17 | 83.10 ± 27.63 | 9/45 | 31/46 | 0.52 ± 0.65 | 2.78 ± 1.53 | −0.10 ± 0.53 | 0.01 ± 0.58 | 1Y |
| Rakasevic (2020) [23] | 86.96 ± 18.50 | 84.60 ± 21.20 | 37/62 | 32/52 | 0.48 ± 1.15 | 0.27 ± 1.23 | −0.18 ± 0.45 | −0.17 ± 0.41 | 6M |
| Rakasevic (2020) [23] | 85.25 ± 14.90 | 87.60 ± 15.10 | 29/62 | 27/52 | 0.85 ± 1.20 | 0.84 ± 1.00 | −0.16 ± 0.05 | −0.14 ± 0.03 | 1Y |
| Tonetti (2021) [24] | 57.69 ± 57.69 | 76.92 ± 38.46 | 47/107 | 66/112 | 0.00 ± 1.20 | 0.50 ± 1.00 | 0.00 ± 0.80 | −0.30 ± 0.70 | 3Y |
| Milinkovic (2022) [25] | 82.10 ± 9.10 | 84.60 ± 9.70 | 30/39 | 42/57 | NR | NR | NR | NR | 5Y |
| Molnár (2022) [26] | 23.07 ± 44.56 | 39.30 ± 35.17 | 14/57 | 18/57 | 0.97 ± 0.93 | 1.25 ± 0.99 | NR | NR | 9Y |
| Skurska (2022) [27] | 55.25 ± 41.96 | 82.35 ± 33.59 | NR | NR | 0.65 ± 0.76 | 2.82 ± 1.51 | −0.15 ± 0.49 | 0.13 ± 0.47 | 5Y |
| Variables | Original Analysis | Trim-and-Fill Analysis | Egger’s Regression Test p-Value | |
|---|---|---|---|---|
| SMD/RR (95% CI) | SMD/RR (95% CI) | Added Studies/Total Studies | ||
| MRC | −0.48 (−0.69 to −0.26) | −0.48 (−0.69 to −0.26) | 0/9 | 0.81 |
| CRC | 0.68 (0.49 to 0.94) | 0.88 (0.56 to 1.38) | 3/11 | 0.02 |
| KTW | −0.75 (−1.25 to −0.26) | −0.58 (−1.15 to −0.01) | 1/9 | 0.10 |
| PD | −0.27 (−0.65 to 0.11) | 0.13 (−0.35 to 0.60) | 3/9 | 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, S.-H.; Song, H.-J.; Kim, N.J.; Park, W.-J.; Park, J.-B. Long-Term Outcomes of Collagen Matrix versus Subepithelial Connective Tissue in Root Coverage for Multiple Teeth: A Systematic Review and Meta-Analysis. Appl. Sci. 2024, 14, 8049. https://doi.org/10.3390/app14178049
Han S-H, Song H-J, Kim NJ, Park W-J, Park J-B. Long-Term Outcomes of Collagen Matrix versus Subepithelial Connective Tissue in Root Coverage for Multiple Teeth: A Systematic Review and Meta-Analysis. Applied Sciences. 2024; 14(17):8049. https://doi.org/10.3390/app14178049
Chicago/Turabian StyleHan, Sung-Hoon, Hye-Jung Song, Na Jin Kim, Won-Jong Park, and Jun-Beom Park. 2024. "Long-Term Outcomes of Collagen Matrix versus Subepithelial Connective Tissue in Root Coverage for Multiple Teeth: A Systematic Review and Meta-Analysis" Applied Sciences 14, no. 17: 8049. https://doi.org/10.3390/app14178049