Abstract
Background: In addition to being highly distressing, chronic migraine headaches are a major socioeconomic challenge. Like other pain syndromes, migraine headaches are associated with psychological and physiological impairments, including sensorimotor and somatosensory deficits. Aim: This study aims to explore whether patients with high-frequency or chronic migraine differ from a healthy population in the areas of laterality recognition (LAT) and facial emotion recognition (FER) and whether there are correlations between these areas and central sensitization of pain and psychological components like stress, depression, anxiety, and alexithymia. Methods: Using a cross-sectional design, individuals with high-frequency or chronic (ICHD classification) migraine (migraine group MG = 45) and healthy individuals (control group CG = 25) were studied using LAT testing (hand, neck, and face); FER testing; and questionnaires, including the Central Sensitization Inventory (CSI) and the Toronto Alexithymia Scale (TAS-20). Results: Data from 70 participants were collected for analysis. Statistically significant differences were found only in the assessment of central sensitization (p < 0.001). Weak to moderate monotonic correlations were found for the MG, especially between alexithymia detection (TAS-20) and facial emotion recognition (FER test). Discussion: The methodological procedure and its accompanying challenges can be seen as limitations of this study. The lack of significant effects must be mentioned, but the selection of the collected questionnaires, the uniform diagnostics, and the statistical processing of a large amount of data represent methodological strengths. Conclusion: The CSI and the TAS-20 could be used in combination with FER to assess chronic migraine. Implementing the described sensorimotor parameters as a therapeutic intervention requires further investigation.
1. Introduction
Migraine is a common, disabling primary headache disorder with significant socio-economic and personal impact [1,2,3]. Chronic headaches are among the most common health disorders, alongside back pain [4]. The Global Burden of Disease Study identified chronic migraine (CM) as a major pain disorder worldwide with significant socio-economic consequences [5]. Chronic migraine affects 1–2% of the global population, with about 2.5% of episodic migraine sufferers developing CM annually [4]. In women under 50, migraine is the leading cause of disability, surpassing back pain and depression [6]. Chronic headaches, including CM, are among the most challenging pain syndromes [7,8]. Besides pain, sufferers report significant limitations in daily activities and social interactions, leading to mood disorders and depression [9,10]. Like other chronic pain syndromes, sufferers withdraw from society and avoid occupational, recreational, and sporting activities. These components are accompanied by mood disorders that can lead to severe depression [10].
In addition to exhibiting fear-avoidance behavior towards movement, individuals with chronic headaches often display compromised movement planning abilities [11,12]. This encompasses a disrupted capacity for laterality recognition (or left–right recognition (LAT)), which may be a quality of (facial) body distortion. So-called (facial) somatosensory distortions can be defined as a pattern observed during prolonged trigeminal sensitivity, affecting classical headaches and chronic orofacial pain (COFP) [13]. This distortion is characterized by dysfunctional pain processing within the central nervous system, leading to hyperexcitation and neuroplastic changes [13,14]. These changes are part of the central sensitization phenomenon, which includes generalized mechanical hyperalgesia across the head, face, neck, and other body areas. Additionally, there are alterations in pain modulation, increased pain area expansion, and the presence of psychological factors [15,16]. Central sensitization itself is a complex physiological process associated with sustained nociception and may result in prolonged pain perception [17]. It is crucial not to assume a causal phenomenon and to pathologize this physiological phenomenon but to understand it as a contribution in the course of a possible chronification of pain [18]. Thus, in chronic migraine, central sensitization may also play a role in sustaining pain perception, in addition to the previously mentioned mechanisms [19].
Normally, LAT is defined as the ability to judge the right and left side of a depicted body part (e.g., hand or neck movement or facial activity; see Figure 1, Figure 2 and Figure 3) and is important for a functioning body schema and movement planning [20,21,22,23]. It is a well-observed phenomenon in several clinical conditions, like complex regional pain syndrome, chronic facial pain [11], shoulder pain [24],and low back and neck pain [20,25]. There is only one study exploring laterality recognition in individuals with episodic migraine [26]. Further information regarding this topic is provided in Appendix A.

Figure 1.
Left–right recognition of hands. Reprinted with permission from ref. [27]. Copyright 2012 Noigroup Publications.

Figure 2.
Left–right recognition of neck movements. Reprinted with permission from ref. [27]. Copyright 2012 Noigroup Publications.
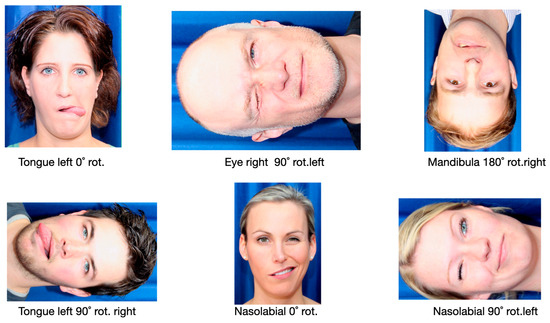
Figure 3.
Left–right recognition of facial activity. Example illustrations from the CRAFTA® Laterality Detection Program for the detection of left and right facial activity [11].
Alexithymia, another possible association with chronic headache, is a well-described phenomenon in persistent pain syndromes. It is characterized by difficulty recognizing and processing emotional signals and is associated with chronic headaches and a reduction in facial reflexes [28]. Although there is a demonstrated correlation between alexithymia and emotion perception, the degree of alexithymia does not significantly correlate with emotion perception [29].
Facial emotion recognition (FER) is important for non-verbal communication concerning the facial reflex during interactions between two people [12]. For example, people suffering from complex regional pain syndrome (CRPS), low back pain, atypical facial pain, carpal tunnel syndrome, or other persistent pain syndromes show a deficit in left–right assessment of the affected body parts, as well as a dysfunctional recognition of basic emotions via facial expressions [20,24,30,31]. It can be inferred that difficulties in recognizing emotions and impaired motor processing of facial muscles may further contribute to the persistence of head and/or facial pain [11]. Figure 4 shows the possible basic emotions a test subject should recognize in a certain time frame and with the highest accuracy possible. Further information regarding this topic is provided in Appendix B.

Figure 4.
Facial emotion recognition. Images from the CRAFTA® emotion recognition program for recognizing emotional expressions in faces (Happy, Sad, Surprised, Anger, Disgust, Fear) [12].
Corresponding changes in the cortical matrix in response to abnormal LAT and FER are described in the scientific literature. Patients with features of alexithymia show significantly less activity in the emotion-processing centers of the brain [32]. Neuronal networks in the premotor cortex, which are necessary for a physiological body schema and the proper functioning of a body part, are thought to show alterations [27]. Studies have shown that neuroplastic adaptations in different brain areas, e.g., the limbic system, the somatosensory and sensorimotor cortex, the prefrontal cortex, and the premotor cortex, preserve pain and correlate with deficits in LAT and FER [33].
In addition to pharmacological treatment, effective pain management in clinical practice necessitates the integration of appropriate communication strategies; behavioral therapy techniques; and motor, sensory, and cognitive training. This approach requires a comprehensive understanding of the neurophysiological and psychosocial elements of pain. Specifically, in treating patients with chronic headaches, incorporating laterality training and facial emotion recognition can enhance therapy. Laterality training, as part of a graded motor imagery program, has shown promising results in several clinical trials, notably in reducing pain and improving motor function and quality of life [23,34,35,36,37]. However, before starting sensorimotor or cognitive training, it is necessary to investigate the nature and degree of LAT and FER limitations in the population of interest.
This cross-sectional study aims to investigate changes in laterality recognition, facial emotion recognition, alexithymia, stress levels, depression, anxiety, and headache impact (days and severity) in individuals with high-frequency or chronic migraine compared to healthy subjects.
2. Materials and Methods
2.1. Participants
From 2nd January 2022 to 30th August 2022, patients diagnosed with “chronic migraine” (≥15 days/month) or “high-frequency migraine” (10–14 days/month) according to the ICHD-3 criteria were examined using the test battery described below. During this period, a control group without headache or other persistent pain disorders was also tested using the same paradigm, excluding three questionnaires. Both male and female subjects aged 18 to 65 with high-frequency or chronic migraine without aura were included, as this demographic represents the primarily affected working-age population [4]. Diagnoses were based on the current classification of the International Headache Society (ICHD-3) [38].
The research sample included in our study consisted of individuals diagnosed with chronic migraine by a specialized headache neurologist. Participants did not need to be pain-free during measurements, but they were only tested if their last debilitating migraine attack had occurred at least 24 h prior. Pain levels were primarily assessed using the Graded Chronic Pain Scale (GCPS). Medications and their usage were recorded in the demographic questionnaire. Exclusion criteria included severe psychiatric diagnoses such as schizophrenia, bipolar disorder, borderline syndrome, current substance abuse, or dementia. Given the common comorbidity of depression and anxiety disorders with chronic headaches, these were not exclusion criteria. Additionally, patients with a history of traumatic or severe neurological events, such as a massive traumatic brain injury, were excluded.
2.2. Recruitment
The migraine group (MG) was recruited through the headache outpatient clinic (Neurology) at the Christian Doppler Clinic Salzburg—University Hospital of Paracelsus Medical University. The healthy control group (CG) was recruited via the FH JOANNEUM Graz email distribution list, with a small portion of the migraine group recruited through a neurologist in private practice in Graz, Austria.
All participants were initially informed by telephone about the study’s background and the final testing process. Further information, questionnaires, and the data sheet were sent by email only after verbal and written consent to participate was obtained. Participants were free to cancel or discontinue the test at any time without providing specific reasons.
2.3. Ethics
After reviewing the requested information, the review committee of the responsible ethics committee for the federal state of Salzburg (Sebastian-Stief-Gasse 2—5020 Salzburg) issued a positive vote on the ethics application and approved it on 30 August 2021, with the authorization being valid for one year (EC no. 1122/2021).
2.4. Study Locations
Most of the measurements of the test subjects in the migraine group were carried out on the premises of the headache outpatient clinic of the Christian Doppler Clinic Salzburg—University Hospital of Paracelsus Medical University. The healthy control group and part of the migraine group were tested on the premises of the FH JOANNEUM Graz physiotherapy department. Both rooms were well-lit and quiet, measuring approximately 12 m2 in size, and included a window to ensure regular ventilation. The rooms themselves each contained a desk for discussing the questionnaires and testing using tablets or notebooks, as well as two armchairs.
2.5. Course of the Study
After clinical and neurological examination conducted by a neurologist (S.L.) with more than 20 years of experience in using IHS classification, all the test subjects were evaluated by the first assessor (B.T.), a physical therapist with more than 15 years of experience in head and face pain. Following an explanation about the examination and after addressing the participants’ questions, the first four tests were conducted using an iPad and a notebook. The room was regularly ventilated between each test phase, and the lighting was adjusted to ensure it was not overly irritating, particularly for participants in the migraine group. The processing of data and statistics was performed by a professional mathematician (W.L.) specialized in biostatistics.
2.5.1. Questionnaires
Previous studies indicate that individuals diagnosed with chronic migraine have a diminished ability to recognize emotions, expression difficulties, heightened levels of depression and anxiety, and increased central sensitization [19,39]. Consequently, the following three questionnaires were added to this study: The Toronto-Alexithymia-Scale 20 Items (TAS-20), the Depression-Anxiety and Stress Scale (DASS), and the Central Sensitization Inventory (CSI).
Toronto-Alexithymia-Scale 20 Items (TAS-20). The TAS-20 records alexithymia, i.e., so-called emotional blindness, using a questionnaire with a total of 20 items. The German translation of the original English scale [40,41] showed adequate validity and reliability in a sample analysis [42]. The scale is recommended for the assessment of alexithymia [43]. However, in the course of an investigation into the psychometric properties in the application of the scale in somatoform pain disorders, the originally propagated 3-factor model was not recommended, and only the use of the total values was recommended for interpretation and recording [44].
Depression Anxiety Stress Scales (DASS). The DASS is a self-report instrument designed to measure three related negative emotional states, namely depression, anxiety, and stress. Each of these states is assessed by a set of 14 items, for a total of 42 items. The questionnaire uses a 4-point severity/frequency scale to assess the extent to which an individual has experienced each state over the past week. Overall, the DASS is both reliable and valid and is recommended in its short form for patients with persistent pain [45,46].
Central Sensitization Inventory (CSI). This questionnaire is available in a validated German version and contains 25 items, which are rated with a range of 0–4 points. The cut-off value for the hypothesis of the existence of a central sensitization of pain is 40 points. In an empirical study on the validity of the German tool called “Zentrale Sensibilisierung Screeningtool” (ZSS), the Neck Disability Index (NDI) was used as a comparable gold standard in a population that suffered from persistent, non-specific neck pain. The Spearman rank correlation showed a statistically significant correlation between NDI and ZSS of ρ = 0.557 (p < 0.01). With a Cronbach’s alpha of α = 0.867 and a total of 25 items, the internal consistency of the ZSS can be rated as good, confirming its validity [47].
2.5.2. Laterality Recognition
In our study, the NOI® recognise “Hands” program of the Neuroorthopaedic Institute® (Adelaide) was used to record the LAT of the hands. This application has good reliability and validity [48,49]. The necessary hardware consisted of a 13-inch Apple™ iPad Pro (3rd generation). After a test run, which each participant carried out before the actual test, the final test run was carried out with 50 randomly arranged pictures of 25 left hands and 25 right hands in the so-called “Vanilla” sub-program. The participants received the following instructions:
“Judge intuitively, as quickly but also as accurately as possible, the pictures of hands, whether it is a right or a left hand. Carry out the task calmly”.
Any questions were clarified in all sections of the test in order not to unsettle the participants and to still achieve valid results. The test leader (B.T.) sat about two meters away from the desk for the test to avoid a controlling test character. The test results were then noted by hand on a prefabricated documentation sheet and transferred to a database using an Excel spreadsheet after the test. In total, this part of the test took a maximum of three minutes.
The left–right recognition of neck movements was also carried out on the same device using the NOI® recognise APP described above. After a new test run using ten images, the test persons were introduced with the same instructions.
“Judge intuitively, as quickly but also as accurately as possible, the images of neck movements, whether it is a movement of the neck to the right or the left. Keep in mind the first-person perspective. Carry out the task calmly”.
The final test, again, included 50 images from the “Vanilla” sub-program. After the end of the test, the results were first noted down again on paper, then transferred to the Excel spreadsheet. This section of the test also took no longer than three minutes.
For the LAT of facial motor functions, the “myfacetraining” (© My Face Training 1.0, 2018) laterality program was applied. The necessary hardware consisted of a Lenovo™ T490s notebook and a Dell™ control mouse. To familiarize themselves with the user interface, all test persons performed a test run of ten faces. The following instructions were provided:
“Judge intuitively, as quickly but also as accurately as possible the images of faces, whether the activity in the face is on the left or right side. The first-person perspective must be considered. Carry out the task calmly”.
The activities took place in the eye area and around the nose, with tongue and chin movements. All test persons had to judge 48 pictures, which, like the previous test pictures, were partly rotated by 90°, 180°, and 270° (See Figure 3). The test sequence of the 48 images was always the same. After the end of the test, the results were first noted down again on paper, then transferred to the Excel spreadsheet. This part of the test took no longer than three minutes. To date, reference values for healthy control groups show a mean response time of (±SD) 2.54 sec ± 1.20 s and a mean accuracy of (±SD) 89.55% ± 11.45% [11].
2.5.3. Facial Basic Emotion Recognition
In our study, the test of facial basic emotion recognition (FER) was carried out with the help of the “myfacetraining” program. After a short explanation of this part of the test and the following instructions, a total of 42 pictures were assessed by the test persons:
“Judge intuitively, as quickly but also as accurately as possible, the images of faces now shown and the emotions visible in them, happy, surprised, frightened, disgusted, angry, and sad. Carry out the task calmly and don’t be irritated by the picture jumping to the next picture. Just keep doing the task”.
The sequence of the 42 pictures (7 pictures per emotion) was the same for all subjects. After a picture of a face with a neutral expression, the same face changed into an emotional expression, which then had to be assessed. We utilized the “myfacetraining” application, which has been shown to produce significant differences in outcomes in two independent studies, especially in terms of laterality and basic emotion recognition. The consistency of these findings across various studies might indicate that “myfacetraining” is effective in assessing the specific areas it targets [50,51]. Additionally, the app is highly user-friendly for both therapists and patients, making it particularly valuable for seamless integration into therapeutic settings, as it allows patients to easily use it on smartphones.
3. Statistical Analysis
The data were calculated, as already mentioned, by a second assessor—a trained mathematician specialized in biostatistics (W.L.). Sample size calculation was performed for the reaction time in laterality detection as the primary outcome. Equal variances were assumed in the headache group and the control group. Estimates of effect size (ES) and standard deviation (SD) were obtained by averaging the corresponding measures from Schmid and Coppieters (2012) [31], where individuals with carpal tunnel syndrome were compared with healthy controls on laterality ratings of images of hands. The estimated ES and SD were 122 ms and 207 ms, respectively. Similar values were found in a comparison between patients with a history of back pain and those with a history or the presence of back pain [52]. Using the formula to calculate the sample size for the two-tailed t-test for two independent samples, assuming alpha = 0.05, beta = 0.2, and equal-sized groups, the total sample size was n = 92 (i.e., 46 persons per group). With unequal group sizes, the total sample size would increase to n = 102 and n = 122 if the ratio of group sizes were 2:1 and 3:1, respectively. Assuming a dropout rate of 10% (cf. [31]), it was originally planned to recruit 102 subjects (i.e., 51 subjects per group).
To describe the differences in outcome variables between the migraine and control groups, five-number summaries were visualized using box plots for descriptive analysis. Non-parametric ANOVA tests with a two-sided significance level of alpha = 0.05 were applied [53]. To adjust for multiple comparisons, the Bonferroni–Holm method was used. For the statistical analysis, we considered whether to calculate correlations using Pearson or Spearman coefficients. Given the ordinal scale level of many variables, Spearman coefficients were used to capture monotonic correlations. All analyses were conducted using the R statistical software package (Version 4.4.1) [54].
4. Results
4.1. Demographic Characteristics of the Compared Groups
Table 1 presents the baseline characteristics of all test subjects. In addition to general demographic information, including origin and educational background, the extent of headache burden was also documented.

Table 1.
Baseline characteristics of all test subjects.
In addition to the general characteristics of the respondents, Table 2 attempts to capture potential confounders that must be considered when interpreting the results.
Table 2.
Possible confounders to be considered.
4.2. Questionnaires
Out of the three questionnaires that were compared (CSI, DASS, and TAS-20), only the questionnaire recording central sensitization (CSI) shows a statistically significant difference between the migraine group and the control group, with a p value of p < 0.001. The remaining parameters from the TAS-20 and DASS questionnaires show no statistically significant differences between the two groups in this study (p = 0.24 and p = 0.39) (Figure 5).
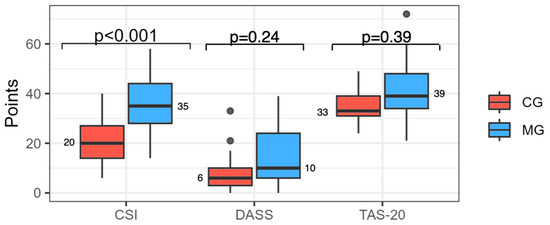
Figure 5.
Box plot of CSI, DASS, and TAS-20 questionnaires between the migraine group (MG) and control group (CG) (figures in points). Numbers next to the boxes represent the medians.
4.3. Laterality Recognition
The accuracy in judging the laterality of hands was similar between the control group (CG) and the migraine group (MG), with no significant differences. For left hands, the median (MD) accuracy was 84% in the CG and 76% in the MG. For right hands, the median accuracy was 88% in the CG and 80% in the MG, with a p value of 1.00, indicating non-significant differences. Likewise, there were no significant differences in the speed of this task. The median time for recognizing left hands was 1.90 s in the CG and 2.20 s in the MG, while for the judgment of right hands, it was 2.10 s in the CG and 2.00 s in the MG (p = 1.00).
The accuracy in judging the laterality of neck movements showed no significant differences between the control group (CG) and the test group (MG). For left neck movements, the median (MD) accuracy was 92% in the CG and 84% in the MG (p = 0.62). For right neck movements, the median accuracy was 88% in the CG and 80% in the MG (p = 1.00). Similarly, no significant differences were observed in the speed of this task. The median time for left neck movements was 1.80 s in the CG and 1.90 s in the MG, while for right neck movements, it was 1.70 s in the CG and 2.00 s in the MG (p = 1.00).
The accuracy in recognizing right facial activity had a median (MD) of 96% in the control group (CG) and 88% in the test group (MG), with a p value of 0.39, indicating a non-significant difference. Left facial activity also showed no significant difference (p = 1.00) between the groups, with a median accuracy of 92% in both the MG and CG. There was no statistically significant difference in the speed of recognizing facial activity on either the right or left side. The median (MD) time for recognizing left-side activity was 1.89 s in the control group (CG) and 2.29 s in the test group (MG). For the right side, the median times were 1.90 s (CG) and 2.18 s (MG), with a p value of 1.00 for both comparisons.
4.4. Facial Emotion Recognition
In the area of FER, there was no statistically significant difference between the two groups after the evaluation of the measurement results (Table 3 and Figure 6 and Figure 7)). Descriptively, the emotion “SAD” (p > 0.05) and the emotion “DISGUST” (p > 0.05) tend to have a lower score in the MG than in the CG.
Table 3.
Results of the facial emotion recognition task between the migraine group (MG) and control group (CG).
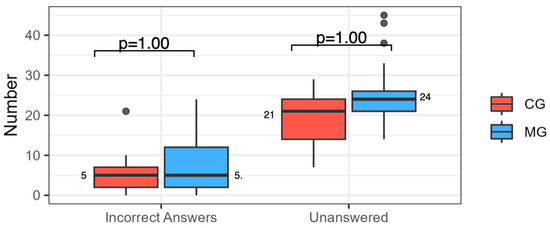
Figure 6.
Number of unanswered/incorrect facial emotion recognition (FER) and answers between the migraine group (MG) and control group (CG).
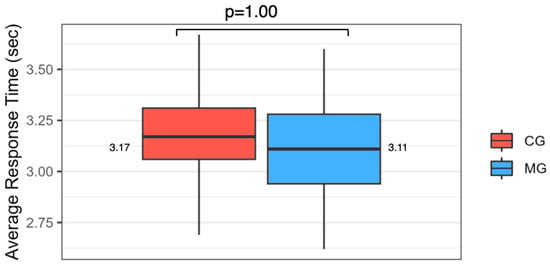
Figure 7.
Average facial emotion recognition (FER) response time between the migraine group (MG) and control group (CG). Numbers next to the boxes represent the medians.
4.5. Correlation of Alexithymia and Facial Emotion Recognition
In the following, possible correlations between the results of the TAS-20 for alexithymic traits and facial emotion recognition are presented. Weak to moderate monotonic correlations were found in both the migraine group and the control group, as shown in Table 4.
Table 4.
Correlations between TAS-20 and facial emotion recognition.
Except for the emotion “DISGUST”, weak to moderate monotonic correlations were found for all emotion expressions in the migraine group, indicating the connection between an increased score on the alexithymia questionnaire and reduced accuracy in the recognition of these facial emotions. Compared to the CG, these weak correlations are more frequent in the MG.
5. Discussion
This study aimed to investigate the associations between high-frequency or chronic migraine without aura and impairments in laterality assessment; facial emotion recognition; and abnormalities in alexithymia, stress, anxiety, depression, and central pain sensitization as measured by questionnaires. Additionally, this study sought to determine whether these aspects correlate with headache-related impairments and to explore the inter-relationships among questionnaire results, facial emotion recognition, and laterality judgment.
Significant differences between the groups can be seen in the test of central sensitization, which was recorded with the CSI questionnaire. The remaining questionnaires did not show a significant statistical result. Above all, the recording of correlations reveals weak monotonic correlations. The recording of alexithymia using TAS-20, as well as facial emotion recognition, also shows weak monotonic correlations for the emotions of FEAR, SAD, and HAPPY. Considerations and reasons for these findings are subsequently discussed methodologically and in terms of content. In doing so, both the limitations and strengths of the present work are presented and reflected upon. These results lead to considerations and suggestions for future research and potential studies in this area while also being evaluated for their clinical and therapeutic relevance, with an outlook presented.
5.1. Methodology
With respect to the questionnaires used in this study, it cannot be excluded that the inclusion of further or other questionnaires could have had an impact of the interpretation of the results. Alexithymia is primarily assessed using TAS-20 or TAS-26, which are, therefore, an adequate choice for assessing emotional blindness in this study. The same applies to the Central Sensitization Inventory (CSI), although it reflects psychological hypervigilance rather than increased responsiveness of nociceptive neurons [55]. In contrast, an assessment of psychological characteristics such as depression, anxiety, and stress is still possible with a variety of other questionnaires, such as the Beck Depression Inventory (BDI), the Beck Anxiety Inventory (BAI), or the Perceived Stress Questionnaire (PSQ) [56]. However, the abundance of questionnaires already to be answered prompted the study author to use the DASS to cover a wider range of psychological aspects with one questionnaire and to avoid possible non-compliance when completing the questionnaires. In addition, it must be repeated that within the DASS, the depression scale alone, with a sensitivity of 77% and a specificity of 83%, achieves an equally good and partly even better result than the described scores to validly detect depression utilizing a questionnaire.
The NOI® Recognise programs represent the best available application for this purpose. Additionally, using these programs facilitates comparability with other studies that have also employed them [11,20,26]. In contrast, the CRAFTA® “myfacetraining” program remains insufficiently studied. Consequently, comparing the present results with other studies is challenging. The most common method for assessing emotion recognition is the FEEL test (Facially Expressed Emotion Labeling—Test), which has already been used in several psychiatric–psychological studies, as well as comparable physiotherapeutic studies [57,58,59,60,61,62]. To date, there is a lack of meaningful correlation studies that support the validity of CRAFTA® “myfacetraining” and can, thus, clarify the results of this study. This program was chosen for its ease of accessibility, user-friendliness, and evaluation parameters of speed and accuracy. However, further research is needed. The good standardization of the test battery enhances the results’ significance. Notably, this study adds ideas and reflects possible challenges for further research on this topic by exploring facial emotion recognition in the context of chronic migraine—an area not previously researched.
This study’s cross-sectional design presents certain limitations, such as the inability to make clear causal determinations or consider risk factors fully. Additionally, recording rare pathologies and diseases requires a large number of subjects, which was challenging in this work. Despite these limitations, this study provides data and considerations for further studies with prospective or retrospective approaches, such as cohort or case–control studies [63].
Based on the considerations mentioned above, a further methodological criticism of this study is the low number of test subjects. Even if the number of cases is calculated against the background of similar studies [31,52] related to laterality recognition, the calculated number of test persons could not be reached. The reasons for this are the lack of funding and the resulting lack of personnel to carry out measurements and elaborate the results. Although speculative, the non-significant results between the two groups are a limitation of this work and must be considered for further work with the aim of obtaining meaningful results.
The healthy CG also presents confounding factors that could influence the results. While the baseline characteristics, such as age and gender distribution, are comparable, differences exist in medication usage and additional complaints or diseases. These factors might affect the participants’ ability to respond accurately and quickly in the tests used in this study.
5.2. Comparison of the Results with Existing Literature
In contrast to the present study, data from a meta-analysis on alexithymia show differences between people with migraine and healthy subjects. The results of the present study cannot reproduce the differences shown by Taxer et al. (2024). It should be noted, however, that the studies examined in this presentation of the meta-analysis all show a high risk of bias, and the results must, therefore, be viewed critically from this perspective [39].
The lack of differences in the area of psychological components is surprising, as large-scale reviews indicate an increased occurrence of these phenomena [64,65], and studies indicate the effectiveness of psychological interventions in the management of migraine [66]. To improve this study, it may be advisable to tighten the inclusion criteria for the healthy group by using multidimensional questionnaires, such as the DASS, to better filter and compare participants without psychological abnormalities. This approach could also be applied more generally to participant selection. If one considers this aspect from a therapeutic clinical point of view, the so-called Örebro Musculoskeletal Screening Questionnaire (OMSQ) is often used in other persistent musculoskeletal syndromes, such as back pain, and screening is subsequently continued with more specific unidimensional questionnaires in the case of abnormalities. As mentioned, this would have added clinical value from a therapeutic point of view [67,68].
The assessment of central sensitization using CSI is not standard in migraine studies. However, intervention studies, in particular, are increasingly using this tool to capture another objectifiable outcome parameter, in addition to limitations with and due to headache frequency or medication use [69]. In detecting possible overlap with other pain syndromes, such as restless leg syndrome, craniomandibular dysfunction, or cranial autonomic symptoms associated with migraine (e.g., runny nose, tearing, and nasal congestion), this questionnaire can indicate the underlying pathomechanism [70,71,72]. Nevertheless, the CSI might be more helpful in detecting psychological hypervigilance than the increased responsiveness of nociceptive neurons [55].
Lüdtke and Edlhaimb (2021) examined LAT of hand and neck movements in patients with episodic migraine over 30 days, recording accuracy and speed of examination and differences in individual pain phases. They found correlations between the headache phases and worsening accuracy but not speed [26]. However, the lack of case-number calculation suggests an insufficient number of subjects, like the present study. Larger studies with more test persons and clearer inclusion and exclusion criteria are needed to obtain meaningful results.
The study of facial emotion recognition in musculoskeletal manifestations is currently limited to syndromes such as low back pain (LBP) [59] and syndromes affecting the orofacial region, such as craniomandibular dysfunction [73] or (chronic) orofacial pain [11,12,57]. A comprehensive review [74] showed that FER has been investigated in psychological studies of healthy subjects and studies of psychiatric and neurological disorders, such as somatoform pain disorder [58], eating disorders [60], and Parkinson’s syndrome [75]. This review concluded that alexithymia could be responsible for deficits in the context of FER, which, in turn, can occur in clinical disorders. The authors described previous studies showing that the correlation of impairment in FER with high scores in alexithymia testing may be partly due to depression and anxiety. In addition, behavioral and neuroimaging studies suggest that alexithymia is associated with processing deficits at the perceptual level [74]. More specifically, FER processing might be particularly impaired in correlation with marked alexithymia when the images are presented briefly and/or the image is degraded. However, the results of previous studies do not allow us to determine whether alexithymia is associated with impairments in processing FER of a particular emotion [74].
These statements are consistent with the results of the present study regarding correlations between alexithymia scores and FER; weak to moderate correlations were found for all emotion expressions, except for the emotion “DISGUST” in the MG. This represents a possible connection between an increased score on the TAS-20 and reduced accuracy in the recognition of these facial emotions, which could not be shown in comparison to the healthy CG. Our study also identified a weak to moderate negative correlation (ρ = −0.26) between DASS questionnaire scores and the ability to recognize the emotion of “FEAR” in the migraine group. This finding suggests that higher levels of depression, anxiety, and stress are associated with poorer fear recognition in this group. No such correlation was observed in the control group. Therefore, using the DASS in the migraine group and subsequently testing facial emotion recognition when higher scores are present could implicate a need for training to address suspected body distortions. To confirm this hypothesis, further specific research is necessary.
5.3. Interpretation of the Results and Outlook
The non-significant results between the two groups do not allow any interpretations or considerations of tendencies in a certain direction from a statistical point of view. Reasons for these results range from the group size not being reached to the still under-researched methods concerning LAT and FER.
The testing of central sensitization using the German version [47] of the CSI questionnaire [76] provides the only statistically significant difference in the study of the two groups. The implementation of this questionnaire would be relevant in a scientific context, as well as in clinical practice, and interesting for possible treatment courses. Although primarily a screening tool, the CSI could be useful as a follow-up parameter during studies and treatments, providing clinical clues to other physical and psychological symptoms for a holistic approach to the patient’s problems. The presentation of confounders also suggests that persistent central sensitization can be associated with various other syndromes. Among others, associations with clinical pictures such as restless leg syndrome and craniomandibular dysfunction, cranial autonomic syndromes, a general sensitivity to pain in subjects with episodic and chronic migraine are linked to the neurophysiological phenomenon of central sensitization in the literature [70,71,72,77]. All too often, there is a danger of pathologizing a physiological phenomenon such as central sensitization and blaming it for a clinical problem [18]. This should be avoided, given current considerations with respect to the IASP concept of nociplastic pain [78] and the new ICD-11 classification of chronic primary pain as a diagnosis in its own right, in that it is defined not only by purely neurophysiological adaptations but also by the existence of functional and emotional impairments [79].
The most frequent additional musculoskeletal disorder in the migraine group (n = 10) is cervical spine-shoulder syndrome. These results go hand in hand with studies on the overlapping of headache syndromes and other complaints pertaining to the musculoskeletal system, particularly in the shoulder–neck region [80,81,82,83]. Central sensitization seems to play an important role in the chronification of pain [84] and is also consistent with considerations of other described persistent syndromes, such as irritable bowel syndrome (n = 1) or chronic gastritis (n = 2). The use of the CSI questionnaire seems even more justified.
In addition to the confounding factors of other symptoms, the difference in the highest level of education also stands out. While 100% of the participants in the healthy control group have a high school diploma (Matura) or a university degree, this applies to 69% of the migraine group. The other 31% of the migraine group have a primary school degree. Socio-economic and educational factors are discussed with respect to (chronic) migraine below. Migraine is indirectly proportionally more common in social classes with lower levels of education and income [85].
A higher score on the TAS-20 questionnaire for alexithymic traits seems to be weakly correlated with poorer recognition of the emotions of FEAR, SAD, HAPPY, SURPRISED, and ANGRY. Compared to the CG, these weak to moderate monotonic correlations could be detected for almost all basic emotions (except DISGUST), which would clinically justify screening for alexithymia in combination with FER. Subsequently, training could influence existing alexithymia. How this might affect the intensity or frequency of migraine cannot be inferred from existing data. This would require actual intervention studies with the mentioned parameters. On a psychological level, the calculation of monotonic correlations for the migraine group between the DASS questionnaire and facial emotion recognition showed a weak to moderately negative monotonic correlation only in the recognition of the emotion of FEAR. The aspect of fear in the course of emotional stress may play a greater role in sufferers with chronic migraine than other emotional stresses, as already indicated by earlier studies and, thus, also supported by the results of this study [86,87,88].
Matamala-Gomez et al. (2022) investigated whether exposure to different visual feedback conditions can modulate pain perception through visually induced analgesia in patients with chronic migraine. The observation of a positive emotional face was sufficient to modulate pain perception. This may be through the mediation of emotional regulation for positive emotions. This study provides a way to integrate cognitive–behavioral interventions into the management of chronic migraine based on the assumption of visually induced analgesia to modulate pain perception in chronic migraine patients [89].
Including the CSI and assessing high alexithymia scores could be relevant for physiotherapeutic possibilities and advanced examination tools. These tests warrant further investigation for definitive recommendations.
5.4. Clinical Implementation
A recent narrative review examines the neurophysiological mechanisms involved in orofacial pain and headaches, emphasizing the importance of assessing facial somatosensory, cognitive-affective, and motor impairments. This review advocates for a multimodal treatment approach that integrates somatosensory reintegration, motor function enhancement, and patient education, showing promise in migraine management when combined with conventional physical therapy [90]. While sensorimotor approaches are increasingly applied in rehabilitation, the evidence supporting laterality training for migraines is limited. However, facial emotion recognition training, specialized orofacial therapy, and pain neuroscience education [91] may offer potential benefits, although further research is necessary.
6. Conclusions
- The chronic migraine group is characterized by clear central sensitization but not by a significant difference in alexithymia compared with the control group.
- There is a weak to moderate correlation between alexithymia in the migraine group and emotion recognition for all basic emotions, except disgust.
- In the control group, there is a moderate correlation between alexithymia and the emotions of fear, disgust, and surprise.
- Particularly high scores on the Central Sensitization Inventory (CSI) and the Toronto Alexithymia Scale-20 (TAS-20) may suggest facial somatosensory distortion, which is expressed in association reduced facial emotion recognition.
- These results should be interpreted with caution but offer innovative ideas for further clinical research.
Author Contributions
Conceptualization—B.T. and H.v.P.; Design—B.T., H.v.P., W.L., M.C., and S.L.; Data collection—B.T.; Interpretation—B.T., H.v.P., W.L., M.C., and S.L.; Logistics—B.T. and S.L. All authors discussed the results and contributed to the manuscript. The final draft was written by B.T. and H.v.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the ethical committee for the federal state of Salzburg (Sebastian-Stief-Gasse 2—5020 Salzburg) on 30 August 2021, valid for one year (EC no. 1122/2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Supporting (raw) data of this study can be requested from the corresponding or first author.
Conflicts of Interest
B.T. and H.v.P. are members of the CRAFTA® research and teaching faculty. H.v.P. was the main creator of the myfacetraining® program, which was used in this study.
Appendix A. Laterality Recognition
Laterality recognition (LAT), or left–right recognition, describes the mental ability or implicit idea of movement of left or right areas of the body or directions of movement of parts of the body [27,92,93]. Parsons (2001) described these phenomena by observing left and right hands with and without movements and made connections to cognitive psychology, neurology, and neuroimaging sciences [92].
The concept of Graded Motor Imagery (GMI) is based on these ideas and clinical research. Particularly good data are available for Complex Regional Pain Syndrome Type 1 (CRPS Type 1), as well as for other chronic pain syndromes, including normative values for detection speed and accuracy in determining LAT [52,94,95,96]. Clinical applicability, i.e., left–right recognition training using various tools, such as flash cards or mobile apps, has been investigated for CRPS type 1 to date and included in existing guidelines for the treatment of this chronic pain disorder [21,36,37,97].
Other pain syndromes and clinical phenomena that have been investigated using laterality detection are shoulder pain [98], facial pain [11,12], carpal tunnel syndrome [31], back pain [20], neck pain [99], hand osteoarthritis [100], knee osteoarthritis [101], persistent musculoskeletal pain [102], and dizziness [103].
In a large-scale study, Wallwork et al. (2013) were able to collect reference values for a healthy population (n = 1622) regarding right–left recognition of hands. Accordingly, the values for response time were measured, with a mean response time (±SD) of 1.983 s ± 0.557 s and a mean accuracy of (±SD) 87.74 ± 10.63% [99]. This work on norm values of LAT for hands was also able to record reference values for neck movements in a healthy population (n = 1414) and showed a mean response time (±SD) of 1.62 s ± 0.50 s and a mean accuracy (±SD) of 89.75 ± 11.25% [99].
Concerning headache, only one study on laterality recognition has been conducted so far. In a longitudinal cohort study, Lüdtke and Edlhaimb (2021) investigated left–right recognition of hand and neck movements in patients who had suffered from migraine for at least two years and reported more than six attacks per year as inclusion criteria (n = 34) compared to a very small, healthy control group (n = 4). The results show a tendency towards poorer performance on the test in terms of accuracy and speed in the headache group. However, there were no correlations with the dominant headache side. In addition, there was a dependency on the attack phase, in that the test persons showed abnormalities in the test [26].
Appendix B. Facial Emotion Recognition
Paul Ekman, an American anthropologist and psychologist known for his research on non-verbal communication, described six basic emotions expressed through the face. These six emotions—sad, happy, disgust, anger, fear, and surprised—are independent of gender, age, and culture and are very important for the so-called facial reflex in non-verbal communication [104]. In addition to correlating with alexithymia, facial emotion recognition (FER) is impaired in people with chronic facial pain, somatoform disorders, and low back pain [12,58,59,105]. The FER examination works through special visual programs in which people see a series of pictures of faces with the described emotional expressions. They then must accurately name the emotion shown at a given time.
Psychiatric disorders or impairments with a psychiatric background have already been extensively investigated for possible abnormalities in facial emotion recognition. Studies on anorexia nervosa, depression, somatoform disorders, substance abuse, anxiety, and panic disorders, as well as studies on the autism spectrum, show tendencies towards abnormalities, but reliable and reproducible data are lacking [58,60,61,106,107,108]. Studies do support the hypothesis that alexithymia may be responsible for the deficits in FER that occur in some clinical disorders. However, the literature also shows that impairments in processing FER that occur in association with high levels of alexithymia may be partly due to depression and anxiety. Furthermore, behavioral and neuroimaging studies suggest that alexithymia is already associated with processing deficits at the perceptual level. More specifically, FER processing may be particularly impaired in the context of severe alexithymia when test images are presented very briefly and/or when images are of poor quality. Downgraded semantic representations of emotional concepts could also be responsible for the deficits in processing FER in severe alexithymia [74].
In the spectrum of neurological diseases such as stroke, Parkinson’s disease, and other neurodegenerative diseases, studies on FER also show trends towards impairment, which could justify both screenings for and treatment of these deficits [51,62,75,109]. Facial emotion recognition has not yet been studied in the context of chronic migraine. However, the work of Yetkin-Ozdin et al. (2015) showed poorer performance in patients with episodic migraine in both face recognition and visuospatial perception. The authors attributed these results to functional differences in the brains of those affected or to genetic changes [110].
In a functional magnetic resonance imaging (fMRI) study, subjects suffering from episodic migraine showed increased neural activation, primarily in response to fearful faces compared to neutral faces in the right-middle frontal gyrus and frontal area compared to healthy controls. In addition, higher migraine attack frequency was found to be associated with increased activation, primarily in the right primary somatosensory cortex (corresponding to the facial area) for fearful expressions and in the right dorsal striatal regions for happy faces. In both analyses, activation differences remained significant, even after controlling for anxiety and depressive symptoms. These results suggest that an enhanced response to emotional stimuli may explain the migraine-triggering effect of psychosocial stressors, which gradually leads to an enhanced somatosensory response to emotional stimuli and, thus, contributes to the progression or chronification of migraine [111].
References
- Edmeads, J.; Mackell, J.A. The Economic Impact of Migraine: An Analysis of Direct and Indirect Costs. Headache J. Head Face Pain 2002, 42, 501–509. [Google Scholar] [CrossRef] [PubMed]
- Saylor, D.; Steiner, T. The Global Burden of Headache. Semin. Neurol. 2018, 38, 182–190. [Google Scholar] [CrossRef]
- Vos, T.; Allen, C.; Arora, M.; Barber, R.M.; Bhutta, Z.A.; Brown, A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; et al. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 310 Diseases and Injuries, 1990–2015: A Systematic Analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1545–1602. [Google Scholar] [CrossRef] [PubMed]
- Burch, R.C.; Buse, D.C.; Lipton, R.B. Migraine: Epidemiology, Burden, and Comorbidity. Neurol. Clin. 2019, 37, 631–649. [Google Scholar] [CrossRef] [PubMed]
- Fuensalida-Novo, S.; Palacios-Ceña, M.; Fernández-Muñoz, J.J.; Castaldo, M.; Wang, K.; Catena, A.; Arendt-Nielsen, L.; Fernández-de-las-Peñas, C. The Burden of Headache Is Associated to Pain Interference, Depression and Headache Duration in Chronic Tension Type Headache: A 1-Year Longitudinal Study. J. Headache Pain 2017, 18, 119. [Google Scholar] [CrossRef]
- Steiner, T.J.; Stovner, L.J.; Jensen, R.; Uluduz, D.; Katsarava, Z. Migraine Remains Second among the World’s Causes of Disability, and First among Young Women: Findings from GBD2019. J. Headache Pain 2020, 21, 137. [Google Scholar] [CrossRef] [PubMed]
- Grande, R.B.; Aaseth, K.; Gulbrandsen, P.; Lundqvist, C.; Russell, M.B. Prevalence of Primary Chronic Headache in a Population-Based Sample of 30- to 44-Year-Old Persons. Neuroepidemiology 2008, 30, 76–83. [Google Scholar] [CrossRef]
- Jull, G.; Sterling, M.; Falla, D.; Treleaven, J.; O’Leary, S. Whiplash, Headache and Neck Pain—Research Based Directions for Physical Therapies; Chruchill Livingstone Elsevier: Amsterdam, The Netherlands, 2008; ISBN 978-0-443-10047-5. [Google Scholar]
- Ashina, S.; Buse, D.C.; Bjorner, J.B.; Bendtsen, L.; Lyngberg, A.C.; Jensen, R.H.; Lipton, R.B. Health-Related Quality of Life in Tension-Type Headache: A Population-Based Study. Scand. J. Pain 2021, 21, 778–787. [Google Scholar] [CrossRef]
- Malmberg-Ceder, K.; Haanpää, M.; Korhonen, P.E.; Kautiainen, H.; Veromaa, V.; Soinila, S. The Role of Psychosocial Risk Factors in the Burden of Headache. J. Pain Res. 2019, 12, 1733–1741. [Google Scholar] [CrossRef]
- von Piekartz, H.; Wallwork, S.B.; Mohr, G.; Butler, D.S.; Moseley, G.L. People with Chronic Facial Pain Perform Worse than Controls at a Facial Emotion Recognition Task, but It Is Not All about the Emotion. J. Oral. Rehabil. 2015, 42, 243–250. [Google Scholar] [CrossRef]
- von Piekartz, H.; Mohr, G. Reduction of Head and Face Pain by Challenging Lateralization and Basic Emotions: A Proposal for Future Assessment and Rehabilitation Strategies. J. Man. Manip. Ther. 2014, 22, 24–35. [Google Scholar] [CrossRef] [PubMed]
- Ziegeler, C.; Schulte, L.H.; May, A. Altered Trigeminal Pain Processing on Brainstem Level in Persistent Idiopathic Facial Pain. Pain 2021, 162, 1374. [Google Scholar] [CrossRef] [PubMed]
- Harper, D.E.; Schrepf, A.; Clauw, D.J. Pain Mechanisms and Centralized Pain in Temporomandibular Disorders. J. Dent. Res. 2016, 95, 1102–1108. [Google Scholar] [CrossRef] [PubMed]
- Lin, C. Brain Signature of Chronic Orofacial Pain: A Systematic Review and Meta-Analysis on Neuroimaging Research of Trigeminal Neuropathic Pain and Temporomandibular Joint Disorders. PLoS ONE 2014, 9, e94300. [Google Scholar] [CrossRef] [PubMed]
- La Touche, R.; Paris-Alemany, A.; Hidalgo-Pérez, A.; López-de-Uralde-Villanueva, I.; Angulo-Diaz-Parreño, S.; Muñoz-García, D. Evidence for Central Sensitization in Patients with Temporomandibular Disorders: A Systematic Review and Meta-Analysis of Observational Studies. Pain Pract. 2018, 18, 388–409. [Google Scholar] [CrossRef]
- Woolf, C.J. Central Sensitization: Implications for the Diagnosis and Treatment of Pain. Pain 2011, 152, S2–S15. [Google Scholar] [CrossRef]
- van Griensven, H.; Schmid, A.; Trendafilova, T.; Low, M. Central Sensitization in Musculoskeletal Pain: Lost in Translation? J. Orthop. Sports Phys. Ther. 2020, 50, 592–596. [Google Scholar] [CrossRef]
- Nijs, J.; George, S.Z.; Clauw, D.J.; Fernández-de-las-Peñas, C.; Kosek, E.; Ickmans, K.; Fernández-Carnero, J.; Polli, A.; Kapreli, E.; Huysmans, E.; et al. Central Sensitisation in Chronic Pain Conditions: Latest Discoveries and Their Potential for Precision Medicine. Lancet Rheumatol. 2021, 3, e383–e392. [Google Scholar] [CrossRef]
- Linder, M.; Michaelson, P.; Röijezon, U. Laterality Judgments in People with Low Back Pain—A Cross-Sectional Observational and Test–Retest Reliability Study. Man. Ther. 2016, 21, 128–133. [Google Scholar] [CrossRef]
- Moseley, G.L. Graded Motor Imagery for Pathologic Pain: A Randomized Controlled Trial. Neurology 2006, 67, 2129–2134. [Google Scholar] [CrossRef]
- Reinersmann, A.; Haarmeyer, G.S.; Blankenburg, M.; Frettlöh, J.; Krumova, E.K.; Ocklenburg, S.; Maier, C. Left Is Where the L Is Right. Significantly Delayed Reaction Time in Limb Laterality Recognition in Both CRPS and Phantom Limb Pain Patients. Neurosci. Lett. 2010, 486, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Walz, A.D.; Usichenko, T.; Moseley, G.L.; Lotze, M. Graded Motor Imagery and the Impact on Pain Processing in a Case of CRPS. Clin. J. Pain 2013, 29, 276–279. [Google Scholar] [CrossRef] [PubMed]
- Breckenridge, J.D.; McAuley, J.H.; Butler, D.S.; Stewart, H.; Moseley, G.L.; Ginn, K.A. The Development of a Shoulder Specific Left/Right Judgement Task: Validity & Reliability. Musculoskelet. Sci. Pract. 2017, 28, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Richter, H.O.; Röijezon, U.; Björklund, M.; Djupsjöbacka, M. Long-Term Adaptation to Neck/Shoulder Pain and Perceptual Performance in a Hand Laterality Motor Imagery Test. Perception 2010, 39, 119–130. [Google Scholar] [CrossRef]
- Luedtke, K.; Edlhaimb, J. Laterality Judgements in Patients with Frequent Episodic Migraine. Musculoskelet. Sci. Pract. 2021, 51, 102316. [Google Scholar] [CrossRef] [PubMed]
- Moseley, G.L.; Butler, D.S.; Beames, T. (Eds.) The Graded Motor Imagery Handbook; Noigroup Publ.: Adelaide, Australia, 2012; ISBN 978-0-9872467-5-2. [Google Scholar]
- Aaron, R.V.; Fisher, E.A.; de la Vega, R.; Lumley, M.A.; Palermo, T.M. Alexithymia in Individuals with Chronic Pain and Its Relation to Pain Intensity, Physical Interference, Depression, and Anxiety: A Systematic Review and Meta-Analysis. Pain 2019, 160, 994. [Google Scholar] [CrossRef]
- Montebarocci, O.; Surcinelli, P.; Rossi, N.; Baldaro, B. Alexithymia, Verbal Ability and Emotion Recognition. Psychiatr. Q. 2011, 82, 245–252. [Google Scholar] [CrossRef]
- Alazmi, L.; Gadsby, G.E.; Heneghan, N.R.; Punt, T.D. Do Trunk-Based Left/Right Judgment Tasks Elicit Motor Imagery? Musculoskelet. Sci. Pract. 2018, 35, 55–60. [Google Scholar] [CrossRef]
- Schmid, A.B.; Coppieters, M.W. Left/Right Judgment of Body Parts Is Selectively Impaired in Patients with Unilateral Carpal Tunnel Syndrome. Clin. J. Pain 2012, 28, 615–622. [Google Scholar] [CrossRef]
- Kano, M.; Fukudo, S. The Alexithymic Brain: The Neural Pathways Linking Alexithymia to Physical Disorders. Biopsychosoc. Med. 2013, 7, 1. [Google Scholar] [CrossRef]
- Moseley, G.L.; Butler, D.S. Explain Pain Supercharged—The Clinician’s Handbook. Noigroup Publications: Adelaide, Australia, 2017; ISBN 978-0-6480227. [Google Scholar]
- Moseley, G.L.; Zalucki, N.; Birklein, F.; Marinus, J.; van Hilten, J.J.; Luomajoki, H. Thinking about Movement Hurts: The Effect of Motor Imagery on Pain and Swelling in People with Chronic Arm Pain. Arthritis Rheum. 2008, 59, 623–631. [Google Scholar] [CrossRef] [PubMed]
- Moseley, G.L.; Sim, D.F.; Henry, M.L.; Souvlis, T. Experimental Hand Pain Delays Recognition of the Contralateral Hand—Evidence That Acute and Chronic Pain Have Opposite Effects on Information Processing? Cogn. Brain Res. 2005, 25, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Moseley, L.G. Graded Motor Imagery Is Effective for Long-Standing Complex Regional Pain Syndrome: A Randomised Controlled Trial. Pain 2004, 108, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Moseley, L.G. Is Successful Rehabilitation of Complex Regional Pain Syndrome Due to Sustained Attention to the Affected Limb? A Randomised Clinical Trial: Pain 2005, 114, 54–61. [Google Scholar] [CrossRef] [PubMed]
- International Headache Society International Classification of Headache Disorders, 3rd Edition. Cephalalgia 2018, 38, 1–211. [CrossRef]
- Taxer, B.; De Castro-Carletti, E.M.; Von Piekartz, H.; Leis, S.; Christova, M.; Armijo-Olivo, S. Facial Recognition, Laterality Judgement, Alexithymia and Resulting Central Nervous System Adaptations in Chronic Primary Headache and Facial Pain—A Systematic Review and Meta-analysis. J. Oral. Rehabil. 2024, 51, 1881–1897. [Google Scholar] [CrossRef]
- Bagby, R.M.; Taylor, G.J.; Parker, J.D. The Twenty-Item Toronto Alexithymia Scale—II. Convergent, Discriminant, and Concurrent Validity. J. Psychosom. Res. 1994, 38, 33–40. [Google Scholar] [CrossRef]
- Bagby, R.M.; Parker, J.D.; Taylor, G.J. The Twenty-Item Toronto Alexithymia Scale—I. Item Selection and Cross-Validation of the Factor Structure. J. Psychosom. Res. 1994, 38, 23–32. [Google Scholar] [CrossRef]
- Bach, M.; Bach, D.; de Zwaan, M.; Serim, M. Validierung Der Deutschen Version Der 20-Item Toronto-Alexithymie-Skala Bei Normalpersonen Und Psychiatrischen Patienten. [Validation of the German Version of the 20-Item Toronto Alexithymia Scale in Normal Adults and Psychiatric Inpatients.]. PPmP Psychother. Psychosom. Med. Psychol. 1996, 46, 23–28. [Google Scholar]
- Bagby, R.M.; Parker, J.D.A.; Taylor, G.J. Twenty-Five Years with the 20-Item Toronto Alexithymia Scale. J. Psychosom. Res. 2020, 131, 109940. [Google Scholar] [CrossRef]
- Koch, A.S.; Kleiman, A.; Wegener, I.; Zur, B.; Imbierowicz, K.; Geiser, F.; Conrad, R. Factorial Structure of the 20-Item Toronto Alexithymia Scale in a Large Sample of Somatoform Patients. Psychiatry Res. 2015, 225, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Antony, M.M.; Bieling, P.J.; Cox, B.J.; Enns, M.W.; Swinson, R.P. Psychometric Properties of the 42-Item and 21-Item Versions of the Depression Anxiety Stress Scales in Clinical Groups and a Community Sample. Psychol. Assess. 1998, 10, 176–181. [Google Scholar] [CrossRef]
- Nilges, P.; Essau, C. Die Depressions-Angst-Stress-Skalen: Der DASS—Ein Screeningverfahren nicht nur für Schmerzpatienten. Der Schmerz 2015, 29, 649–657. [Google Scholar] [CrossRef]
- Schumacher, S.; Waschescio, H.J. Validierung einer deutschen Version des „Central Sensitization Inventory“ zur Identifizierung zentralnervöser Schmerzentwicklungen. Manuelletherapie 2019, 23, 129–133. [Google Scholar] [CrossRef]
- Dey, A.; Barnsley, N.; Mohan, R.; McCormick, M.; McAuley, J.H.; Moseley, G.L. Are Children Who Play a Sport or a Musical Instrument Better at Motor Imagery than Children Who Do Not? Br. J. Sports Med. 2012, 46, 923–926. [Google Scholar] [CrossRef] [PubMed]
- Bray, H.; Moseley, G.L. Disrupted Working Body Schema of the Trunk in People with Back Pain. Br. J. Sports Med. 2011, 45, 168–173. [Google Scholar] [CrossRef]
- Kuttenreich, A.-M.; Volk, G.F.; Guntinas-Lichius, O.; von Piekartz, H.; Heim, S. Facial Emotion Recognition in Patients with Post-Paralytic Facial Synkinesis—A Present Competence. Diagnostics 2022, 12, 1138. [Google Scholar] [CrossRef]
- Kuttenreich, A.-M.; von Piekartz, H.; Heim, S. Is There a Difference in Facial Emotion Recognition after Stroke with vs. without Central Facial Paresis? Diagnostics 2022, 12, 1721. [Google Scholar] [CrossRef]
- Bowering, K.J.; O’Connell, N.E.; Tabor, A.; Catley, M.J.; Leake, H.B.; Moseley, G.L.; Stanton, T.R. The Effects of Graded Motor Imagery and Its Components on Chronic Pain: A Systematic Review and Meta-Analysis. J. Pain 2013, 14, 3–13. [Google Scholar] [CrossRef]
- Brunner, E.; Bathke, A.C.; Konietschke, F. Rank and Pseudo-Rank Procedures for Independent Observations in Factorial Designs: Using R and SAS; Springer Series in Statistics; Springer International Publishing: Cham, 2018; ISBN 978-3-030-02912-8. [Google Scholar]
- R Core Team. European Environment Agency. 2020. Available online: https://www.eea.europa.eu/data-and-maps/indicators/oxygen-consuming-substances-in-rivers/r-development-core-team-2006 (accessed on 17 January 2023).
- Adams, G.R.; Gandhi, W.; Harrison, R.; Van Reekum, C.M.; Wood-Anderson, D.; Gilron, I.; Salomons, T.V. Do “Central Sensitization” Questionnaires Reflect Measures of Nociceptive Sensitization or Psychological Constructs? A Systematic Review and Meta-Analyses. Pain 2023, 164, 1222–1239. [Google Scholar] [CrossRef]
- Shahid, A.; Wilkinson, K.; Marcu, S.; Shapiro, C.M. Perceived Stress Questionnaire (PSQ). In STOP, THAT and One Hundred Other Sleep Scales; Shahid, A., Wilkinson, K., Marcu, S., Shapiro, C.M., Eds.; Springer: New York, NY, USA, 2011; pp. 273–274. ISBN 978-1-4419-9892-7. [Google Scholar]
- Piekartz, H.V.; Mohr, G.; Limbrecht, K.; Traue, H.; Kessler, H. Recognition of Emotional Facial Expressions and Alexithymia in Patients with Chronic Facial Pain. Ann. Psychiatry Ment. Health 2018, 6, 1134. [Google Scholar]
- Pedrosa Gil, F.; Ridout, N.; Kessler, H.; Neuffer, M.; Schoechlin, C.; Traue, H.C.; Nickel, M. Facial Emotion Recognition and Alexithymia in Adults with Somatoform Disorders. Depress. Anxiety 2008, 25, E133–E141. [Google Scholar] [CrossRef] [PubMed]
- von Korn, K.; Richter, M.; von Piekartz, H. [Changes in basic emotion recognition in patients with chronic low back pain. A cross-sectional study analyzing emotion recognition and alexithymia]. Schmerz 2014, 28, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Kessler, H.; Schwarze, M.; Filipic, S.; Traue, H.C.; von Wietersheim, J. Alexithymia and Facial Emotion Recognition in Patients with Eating Disorders. Int. J. Eat. Disord. 2006, 39, 245–251. [Google Scholar] [CrossRef]
- Kessler, H.; Roth, J.; von Wietersheim, J.; Deighton, R.M.; Traue, H.C. Emotion Recognition Patterns in Patients with Panic Disorder. Depress. Anxiety 2007, 24, 223–226. [Google Scholar] [CrossRef]
- Braun, M.; Traue, H.C.; Frisch, S.; Deighton, R.M.; Kessler, H. Emotion Recognition in Stroke Patients with Left and Right Hemispheric Lesion: Results with a New Instrument—The FEEL Test. Brain Cogn. 2005, 58, 193–201. [Google Scholar] [CrossRef]
- Lesser, M.L. Design and Interpretation of Observational Studies: Cohort, Case–Control, and Cross-Sectional Designs. In Principles of Research Methodology; Supino, P.G., Borer, J.S., Eds.; Springer: New York, NY, USA, 2012; pp. 55–77. ISBN 978-1-4614-3359-0. [Google Scholar]
- Amiri, S.; Behnezhad, S.; Azad, E. Migraine Headache and Depression in Adults: A Systematic Review and Meta-Analysis. Neuropsychiatrie 2019, 33, 131–140. [Google Scholar] [CrossRef]
- Cologno, D.; Buzzi, M.G.; Carlesimo, G.A.; Cicinelli, P.; Costa, A.; Fadda, L.; Formisano, R.; Marconi, B.; Pero, S.; Caltagirone, C. Psychiatric Disorders and Pain Location in Unilateral Migraineurs. J. Headache Pain 2005, 6, 227–230. [Google Scholar] [CrossRef]
- Sullivan, A.; Cousins, S.; Ridsdale, L. Psychological Interventions for Migraine: A Systematic Review. J. Neurol. 2016, 263, 2369–2377. [Google Scholar] [CrossRef]
- Lin, I.; Wiles, L.; Waller, R.; Goucke, R.; Nagree, Y.; Gibberd, M.; Straker, L.; Maher, C.G.; O’Sullivan, P.P.B. What Does Best Practice Care for Musculoskeletal Pain Look like? Eleven Consistent Recommendations from High-Quality Clinical Practice Guidelines: Systematic Review. Br. J. Sports Med. 2020, 54, 79–86. [Google Scholar] [CrossRef]
- Veirman, E.; Van Ryckeghem, D.M.L.; De Paepe, A.; Kirtley, O.J.; Crombez, G. Multidimensional Screening for Predicting Pain Problems in Adults: A Systematic Review of Screening Tools and Validation Studies. Pain Rep. 2019, 4, e775. [Google Scholar] [CrossRef] [PubMed]
- Butt, M.N.; Maryum, M.; Amjad, I.; Khan, O.J.; Awan, L. Effects of Aerobic Exercise and Progressive Muscle Relaxation on Migraine. J. Pak. Med. Assoc. 2022, 72, 1153–1157. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Suzuki, S.; Haruyama, Y.; Okamura, M.; Shiina, T.; Fujita, H.; Kobashi, G.; Sairenchi, T.; Uchiyama, K.; Hirata, K. Central Sensitization in Migraine Is Related to Restless Legs Syndrome. J. Neurol. 2021, 268, 1395–1401. [Google Scholar] [CrossRef]
- Danno, D.; Wolf, J.; Ishizaki, K.; Kikui, S.; Hirata, K.; Takeshima, T. Cranial Autonomic Symptoms in Migraine Are Related to Central Sensitization: A Prospective Study of 164 Migraine Patients at a Tertiary Headache Center. BMC Neurol. 2022, 22, 89. [Google Scholar] [CrossRef] [PubMed]
- Do Vale Braido, G.V.; Svensson, P.; Dos Santos Proença, J.; Mercante, F.G.; Fernandes, G.; de Godoi Gonçalves, D.A. Are Central Sensitization Symptoms and Psychosocial Alterations Interfering in the Association between Painful TMD, Migraine, and Headache Attributed to TMD? Clin. Oral. Investig. 2022, 27, 681–690. [Google Scholar] [CrossRef]
- Haas, J.; Eichhammer, P.; Traue, H.C.; Hoffmann, H.; Behr, M.; Crönlein, T.; Pieh, C.; Busch, V. Alexithymic and Somatisation Scores in Patients with Temporomandibular Pain Disorder Correlate with Deficits in Facial Emotion Recognition. J. Oral. Rehabil. 2013, 40, 81–90. [Google Scholar] [CrossRef]
- Grynberg, D.; Chang, B.; Corneille, O.; Maurage, P.; Vermeulen, N.; Berthoz, S.; Luminet, O. Alexithymia and the Processing of Emotional Facial Expressions (EFEs): Systematic Review, Unanswered Questions and Further Perspectives. PLoS ONE 2012, 7, e42429. [Google Scholar] [CrossRef]
- Wabnegger, A.; Ille, R.; Schwingenschuh, P.; Katschnig-Winter, P.; Kögl-Wallner, M.; Wenzel, K.; Schienle, A. Facial Emotion Recognition in Parkinson’s Disease: An fMRI Investigation. PLoS ONE 2015, 10, e0136110. [Google Scholar] [CrossRef]
- Nijs, J.; Goubert, D.; Ickmans, K. Recognition and Treatment of Central Sensitization in Chronic Pain Patients: Not Limited to Specialized Care. J. Orthop. Sports Phys. Ther. 2016, 46, 1024–1028. [Google Scholar] [CrossRef] [PubMed]
- Palacios-Ceña, M.; Lima Florencio, L.; Natália Ferracini, G.; Barón, J.; Guerrero, Á.L.; Ordás-Bandera, C.; Arendt-Nielsen, L.; Fernández-de-Las-Peñas, C. Women with Chronic and Episodic Migraine Exhibit Similar Widespread Pressure Pain Sensitivity. Pain Med. 2016, 17, 2127–2133. [Google Scholar] [CrossRef]
- IASP. IASP Terminology—IASP. Available online: https://www.iasp-pain.org/terminology?navItemNumber=576#Pain (accessed on 9 March 2021).
- Nicholas, M.; Vlaeyen, J.W.S.; Rief, W.; Barke, A.; Aziz, Q.; Benoliel, R.; Cohen, M.; Evers, S.; Giamberardino, M.A.; Goebel, A.; et al. The IASP Classification of Chronic Pain for ICD-11: Chronic Primary Pain. Pain 2019, 160, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Liang, Z.; Galea, O.; Thomas, L.; Jull, G.; Treleaven, J. Cervical Musculoskeletal Impairments in Migraine and Tension Type Headache: A Systematic Review and Meta-Analysis. Musculoskelet. Sci. Pract. 2019, 42, 67–83. [Google Scholar] [CrossRef]
- Luedtke, K.; Boissonnault, W.; Caspersen, N.; Castien, R.; Chaibi, A.; Falla, D.; Fernández-de-las-Peñas, C.; Hall, T.; Hirsvang, J.R.; Horre, T.; et al. International Consensus on the Most Useful Physical Examination Tests Used by Physiotherapists for Patients with Headache: A Delphi Study. Man. Ther. 2016, 23, 17–24. [Google Scholar] [CrossRef]
- Lüdtke, K. Evidenzorientierte Untersuchungs- und Behandlungsmethoden für Migränepatienten. Der Schmerzpatient 2018, 1, 76–81. [Google Scholar] [CrossRef][Green Version]
- Castien, R.; De Hertogh, W. A Neuroscience Perspective of Physical Treatment of Headache and Neck Pain. Front. Neurol. 2019, 10, 276. [Google Scholar] [CrossRef]
- Adams, L.M.; Turk, D.C. Central Sensitization and the Biopsychosocial Approach to Understanding Pain. J. Appl. Biobehav. Res. 2018, 0, e12125. [Google Scholar] [CrossRef]
- Stewart, W.F.; Roy, J.; Lipton, R.B. Migraine Prevalence, Socioeconomic Status, and Social Causation. Neurology 2013, 81, 948–955. [Google Scholar] [CrossRef] [PubMed]
- Probyn, K.; Bowers, H.; Caldwell, F.; Mistry, D.; Underwood, M.; Matharu, M.; Pincus, T. Prognostic Factors for Chronic Headache. Neurology 2017, 89, 291–301. [Google Scholar] [CrossRef]
- Bottiroli, S.; Galli, F.; Viana, M.; Sances, G.; Tassorelli, C. Traumatic Experiences, Stressful Events, and Alexithymia in Chronic Migraine With Medication Overuse. Front. Psychol. 2018, 9, 704. [Google Scholar] [CrossRef]
- Yalınay Dikmen, P.; Onur Aysevener, E.; Kosak, S.; Ilgaz Aydınlar, E.; Sağduyu Kocaman, A. Relationship between MIDAS, Depression, Anxiety and Alexithymia in Migraine Patients. Acta Neurol. Belg. 2020, 120, 837–844. [Google Scholar] [CrossRef]
- Matamala-Gomez, M.; Bottiroli, S.; Sances, G.; Allena, M.; De Icco, R.; Ghiotto, N.; Guaschino, E.; Sandrini, G.; Tassorelli, C. Facial Expressions Modulate Pain Perception in Patients with Chronic Migraine. Cephalalgia 2022, 42, 739–748. [Google Scholar] [CrossRef] [PubMed]
- Von Piekartz, H.; Paris-Alemany, A. Assessment and Brain Training of Patients Experiencing Head and Facial Pain with a Distortion of Orofacial Somatorepresentation: A Narrative Review. Appl. Sci. 2021, 11, 6857. [Google Scholar] [CrossRef]
- Meise, R.; Carvalho, G.F.; Thiel, C.; Luedtke, K. Additional Effects of Pain Neuroscience Education Combined with Physiotherapy on the Headache Frequency of Adult Patients with Migraine: A Randomized Controlled Trial. Cephalalgia 2023, 43, 3331024221144781. [Google Scholar] [CrossRef] [PubMed]
- Parsons, L.M. Integrating Cognitive Psychology, Neurology and Neuroimaging. Acta Psychol. 2001, 107, 155–181. [Google Scholar] [CrossRef]
- Osuagwu, B.A.; Vuckovic, A. Similarities between Explicit and Implicit Motor Imagery in Mental Rotation of Hands: An EEG Study. Neuropsychologia 2014, 65, 197–210. [Google Scholar] [CrossRef]
- Moseley, L.G. I Can’t Find It! Distorted Body Image and Tactile Dysfunction in Patients with Chronic Back Pain. Pain 2008, 140, 239–243. [Google Scholar] [CrossRef]
- Limakatso, K.; Corten, L.; Parker, R. The Effects of Graded Motor Imagery and Its Components on Phantom Limb Pain and Disability in Upper and Lower Limb Amputees: A Systematic Review Protocol. Syst. Rev. 2016, 5, 145. [Google Scholar] [CrossRef]
- Lagueux, E.; Charest, J.; Lefrançois-Caron, E.; Mauger, M.-E.; Mercier, E.; Savard, K.; Tousignant-Laflamme, Y. Modified Graded Motor Imagery for Complex Regional Pain Syndrome Type 1 of the Upper Extremity in the Acute Phase: A Patient Series. Int. J. Rehabil. Res. 2012, 35, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Birklein, F.; Humm, A.; Maier, C.; Maihöfner, C.; Middeldorf, S.; Quasthoff, S.; Siemers, F.; Sommer, C. Diagnostik und Therapie komplexer regionaler Schmerzsyndrome (CRPS), S1-Leitlinie 2018; in Deutsche Gesellschaft für Neurologie (Hrsg.), Leitlinien für Diagnostik und Therapie in der Neurologie. Mainz, Deutschland. Available online: https://www.dgn.org/leitlinien (accessed on 24 April 2024).
- Breckenridge, J.D.; McAuley, J.H.; Butler, D.S.; Stewart, H.; Moseley, G.L.; Ginn, K.A. Shoulder Left/Right Judgement Task: Development and Establishment of a Normative Dataset. Physiotherapy 2015, 101, e169–e170. [Google Scholar] [CrossRef]
- Wallwork, S.B.; Butler, D.S.; Fulton, I.; Stewart, H.; Darmawan, I.; Moseley, G.L. Left/Right Neck Rotation Judgments Are Affected by Age, Gender, Handedness and Image Rotation. Man. Ther. 2013, 18, 225–230. [Google Scholar] [CrossRef]
- Magni, N.E.; McNair, P.J.; Rice, D.A. Sensorimotor Performance and Function in People with Osteoarthritis of the Hand: A Case–Control Comparison. Semin. Arthritis Rheum. 2018, 47, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Stanton, T.R.; Lin, C.-W.C.; Bray, H.; Smeets, R.J.E.M.; Taylor, D.; Law, R.Y.W.; Moseley, G.L. Tactile Acuity Is Disrupted in Osteoarthritis but Is Unrelated to Disruptions in Motor Imagery Performance. Rheumatology 2013, 52, 1509–1519. [Google Scholar] [CrossRef] [PubMed]
- von Piekartz, H.; Lüers, J.; Daumeyer, H.; Mohr, G. Is kinesiophobia associated with changes in left/right judgment and emotion recognition during a persisting pain condition?: A cross-sectional study. Schmerz 2017, 31, 483–488. [Google Scholar] [CrossRef] [PubMed]
- Wallwork, S.B.; Butler, D.S.; Moseley, G.L. Dizzy People Perform No Worse at a Motor Imagery Task Requiring Whole Body Mental Rotation; A Case-Control Comparison. Front. Hum. Neurosci. 2013, 7, 258. [Google Scholar] [CrossRef]
- Ekman, P. Basic Emotions. In Handbook of Cognition and Emotion; John Wiley & Sons Inc.: Hoboken, NJ, USA, 1999. [Google Scholar]
- Jongen, S.; Axmacher, N.; Kremers, N.A.W.; Hoffmann, H.; Limbrecht-Ecklundt, K.; Traue, H.C.; Kessler, H. An Investigation of Facial Emotion Recognition Impairments in Alexithymia and Its Neural Correlates. Behav. Brain Res. 2014, 271, 129–139. [Google Scholar] [CrossRef]
- Galderisi, S.; Mancuso, F.; Mucci, A.; Garramone, S.; Zamboli, R.; Maj, M. Alexithymia and Cognitive Dysfunctions in Patients with Panic Disorder. Psychother. Psychosom. 2008, 77, 182–188. [Google Scholar] [CrossRef]
- Kätsyri, J.; Saalasti, S.; Tiippana, K.; von Wendt, L.; Sams, M. Impaired Recognition of Facial Emotions from Low-Spatial Frequencies in Asperger Syndrome. Neuropsychologia 2008, 46, 1888–1897. [Google Scholar] [CrossRef]
- Mann, L.S.; Wise, T.N.; Trinidad, A.; Kohanski, R. Alexithymia, Affect Recognition, and Five Factors of Personality in Substance Abusers. Percept. Mot. Ski. 1995, 81, 35–40. [Google Scholar] [CrossRef]
- Marco-Garcia, S.; Ferrer-Quintero, M.; Usall, J.; Ochoa, S.; Del Cacho, N.; Huerta-Ramos, E. Facial emotion recognition in neurological disorders: A narrative review. Rev. Neurol. 2019, 69, 207–219. [Google Scholar] [CrossRef]
- Yetkin-Ozden, S.; Ekizoglu, E.; Baykan, B. Face Recognition in Patients with Migraine. Pain Pract. 2015, 15, 319–322. [Google Scholar] [CrossRef]
- Szabó, E.; Galambos, A.; Kocsel, N.; Édes, A.E.; Pap, D.; Zsombók, T.; Kozák, L.R.; Bagdy, G.; Kökönyei, G.; Juhász, G. Association between Migraine Frequency and Neural Response to Emotional Faces: An fMRI Study. NeuroImage: Clin. 2019, 22, 101790. [Google Scholar] [CrossRef] [PubMed]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).