Featured Application
We found that more students could reproduce therapeutic movement techniques by practicing with a robot that simulates the patient’s pathological movements than by performing simulation exercises with other students. These results suggest that the use of simulation robots that can reproduce the pathological movements of patients may be effective in teaching therapeutic movement techniques. Furthermore, we believe that it is an effective new learning method for therapeutic movement techniques considering interpersonal infections.
Abstract
We aimed to compare the effects of practical learning using an educational robot arm (Samothrace: SAMO) and a student simulating a patient in students’ acquisition of therapeutic motion techniques. For this study, twenty-five fourth-year students and eight therapists were included. Students were randomly assigned to the robot practice (Robo) group (n = 13) or conventional practice (Human) group (n = 12), wherein students practiced among themselves. The experimental procedure comprised a pre-practice test, practice, and post-practice test. We calculated the peak angle ratio, peak velocity, and movement time during flexion and extension using the elbow joint angle data. Machine learning was performed on students’ pre-practice and used therapists’ data to create identifiers that distinguish students and therapists to determine whether the students’ skills improved to the level of a therapist. However, regarding other kinematics data, there were no main effects or interactions between groups pre- and post-practice. Identifiers were created from machine learning of kinematics data pre-practice, and the effect was evaluated post-practice. A higher number of students in the Robo group were determined to possess skills at a therapist’s level. This study suggests the effectiveness of a simulation robot that can reproduce a patient’s pathological motions in educating students on upper limb exercise therapy.
1. Introduction
Students aiming to become rehabilitation therapists (e.g., occupational and physical therapists) are educated at rehabilitation training schools to acquire exercise therapy techniques. These students have to acquire theoretical knowledge on therapeutic motion techniques from textbooks and learn techniques from video teaching materials. Furthermore, during practical training, students perform simulations by taking turns to imitate patients with movement disorders. However, in the current learning method, there is a significant discrepancy between exercise therapy techniques employed by students and those employed by therapists [1]. Students believe that they lack the skills to independently practice as therapists and that they need more practice to improve their technical skills [2]. In the existing learning method, students cannot practice on an actual patient, making it difficult to understand patients’ pathological motions (e.g., stiffness of muscles and ligaments).
The effectiveness of simulation education using a patient robot has been demonstrated in the field of medical education [3,4]. Based on this, we developed a robot arm (development code: Samothrace: SAMO; Patent No. 6307210) that can be applied in the field of rehabilitation education [1]. Because SAMO can reproduce the pathological motion of a stroke patient, students can practice repeatedly with the robot in a state similar to the patient’s pathological motion. In addition, since the movement of the robot’s joints can be recorded, it is possible to observe and monitor the students’ level of proficiency when performing the exercise therapy techniques [5]. Owing to the recent infectious disease epidemic, telemedicine and remote education are becoming more common [6]. Future epidemics may make it difficult for students to perform practical exercises that require other students to simulate a patient. The use of a patient robot such as SAMO allows students to receive practical education similar to clinical practice even in such situations. However, simulation education robots such as SAMO have not been used in the field of rehabilitation; further, the effectiveness of SAMO for learning remains unclear. In addition, it is unclear whether the use of a patient robot is more effective than conventional simulation exercises among students.
Therefore, the present study aimed to clarify which learning method—learning using SAMO or simulation practice among students—is a more effective method for the practice of therapeutic motion techniques, as well as to examine exercise therapy education methods. To validate the findings, this study assessed changes in features of motor therapy techniques before and after practice and whether students’ techniques matched those of therapists after practice.
The uniqueness of this study lies in constructing an educational system that assesses clinical knowledge and skills from the early stages of students’ training by visualizing the acquisition of rehabilitation techniques. Simulation robots with capabilities for motor therapy education are not yet used in educational settings worldwide. Furthermore, with the advancement of education utilizing simulation robots, students are expected to acquire proficient techniques at an earlier stage, even before obtaining their qualifications.
2. Materials and Methods
2.1. Participants
Study participants comprised 25 fourth-year students who had undergone clinical training at an occupational therapist training school and eight occupational or physical therapists with ≥5 years of clinical experience. Fourth-year students were selected because they had learned about therapeutic motion techniques in the training school and in a clinical setting, and they were assumed to possess knowledge and skill levels close to those of therapists. Therapists had >5 years of clinical experience because of the required years for basic and incumbent training, as specified by the Japanese Association of Occupational Therapists, and the period for which they are eligible for the optional program for authorized occupational therapists [7]. In addition, a standard minimum of 5 years of experience is required to become a clinical training instructor [8,9]. The sample size for this study was estimated a priori using the statistical software package G* Power (a tool used to perform statistical power analysis, F-tests analysis of variance [ANOVA]) based on available data and subjected to the set levels of α = 0.05 and 1 − β = 0.95; effect size f = 0.85 [10,11]. The minimum number of required participants was eight.
This study was approved by the Ethics Committee of Saitama Prefectural University (approval no. 27112) and implemented in accordance with the Declaration of Helsinki. Prior to this study, all participants received a thorough explanation of the experiment and provided written consent for participation in this study.
2.2. Experimental Procedure
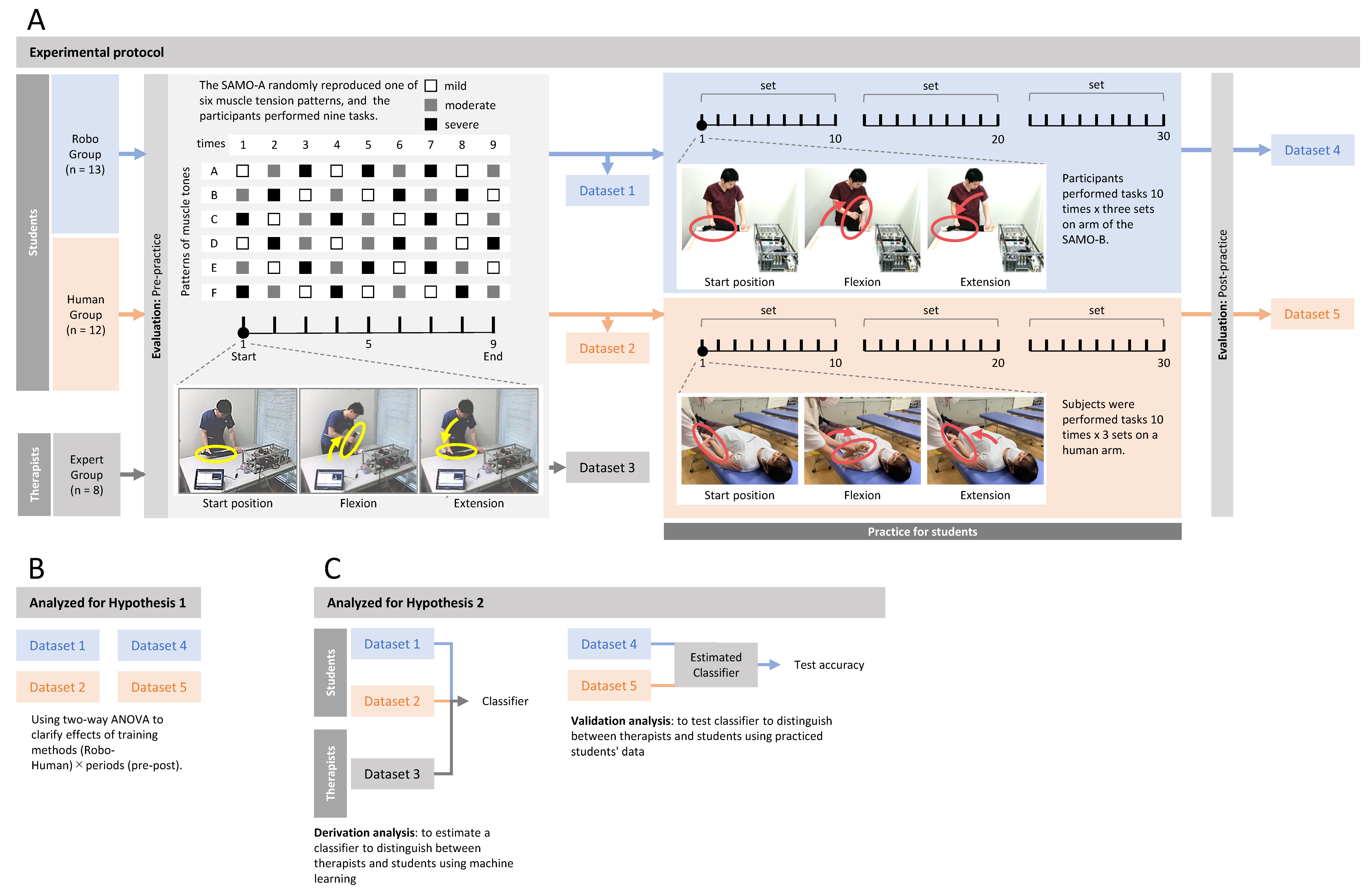
Figure 1 shows the experimental procedure. The experimental procedure comprised a pre-practice test, practice, and post-practice test. To demonstrate the effect of different practice methods for learning therapeutic motion techniques, 13 students were randomly assigned to the robot practice (Robo) group, wherein therapeutic motion techniques were practiced using SAMO, and 12 students were randomly assigned to the student practice (Human) group. Due to the random assignment of students to the Robo and Human groups, there was a possibility of introducing biases that could affect the results. However, since the students had studied the same content, the impact of these biases was expected to be minimal. Additionally, to reduce the impact on measurement results before and after practice, randomization was not only employed to divide the subjects but also to create six patterns of muscle tone levels (A–F) as shown in Figure 1, with random assignment within these patterns. In addition, only eight therapists performed the pre-practice test to determine whether the students’ therapeutic motion techniques were comparable to those of the therapists.
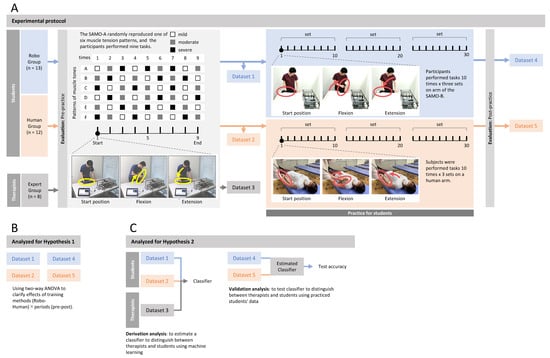
Figure 1.
Therapists and students therapeutic motion data collection protocol and analysis methods. The upper panel (A) is the experimental protocol, the lower left panel (B) is the analysis for hypothesis 1, and the lower right panel (C) is the analysis for hypothesis 2.
2.2.1. Movement Task
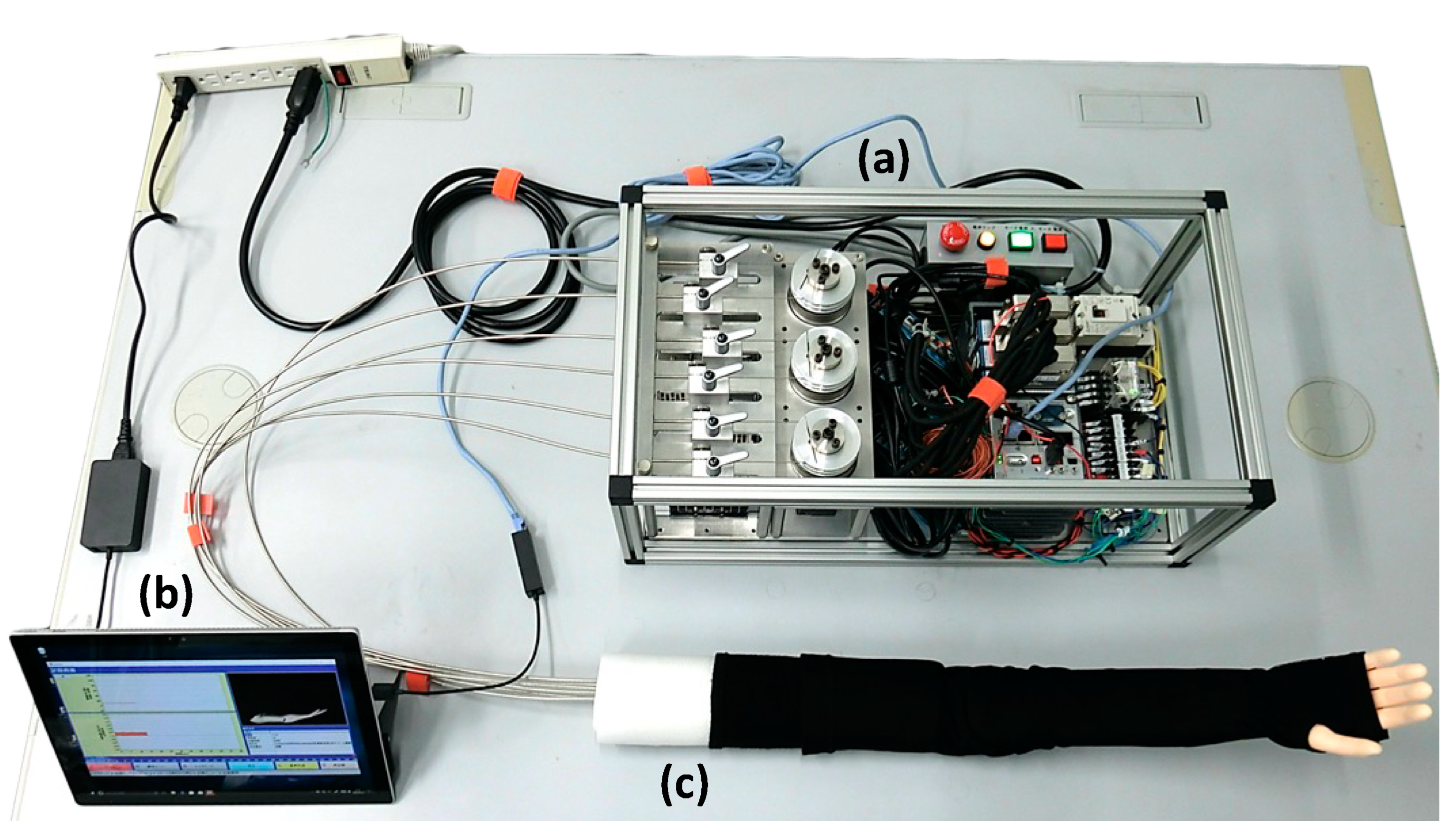
The therapeutic motion tasks for the pre- and post-practice tests were as follows: For the SAMO-A elbow joint (for data acquisition) (Figure 2), the peak extension position was set as the starting position, and the task was to return to the starting position by moving the elbow joint to achieve peak flexion, then back to peak extension. Participants were allowed to select the posture, movement speed, and grasping position of the robot arm, and three degrees of muscle tension (mild, moderate, and severe) were set. The pre- and post-practice tests were randomly performed three times for each degree of muscle tension, and a total of nine tasks were performed. Muscle tension was set to a resistance of 2.4 N for mild, 3.9 N for moderate, and 5.4 N for severe as the axial value of the actuator. The measurement items were the SAMO elbow joint angle and movement time during the pre- and post-practice tests, which were recorded over time using the SAMO-A at 100 Hz.
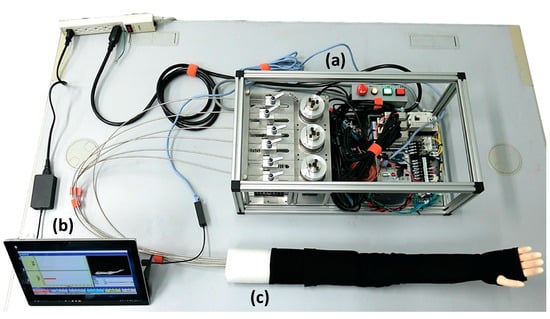
Figure 2.
The SAMO therapeutic arm motion evaluation and training system in the present study. (a) Actuator and control driver unit. (b) Display and application for controller with data correction. (c) The right-arm robot unit. Three modes of spasticity, rigidity, and relaxation can be switched by the controller application. Elbow joint torque is converted from voltage values of wire-bound actuators. Elbow angle data are estimated from the rotation angle of pulleys tethered to actuators. The endoskeleton of an arm robot is constructed of aluminum alloy, while the outer skin and hand are made from synthetic resin. The spastic, rigid, and relaxed modes are reproduced by adjusting and driving wire-coupled actuators using an application program. In this study, two SAMOs were used: SAMO-A for evaluation and SAMO-B for training. The panel displays SAMO-A. Among the structures and systems of SAMO-A and SAMO-B, (a,c) are slightly different. Regarding (a), SAMO-A exhibits a “sticky” movement when moving the elbow joint, resembling the movement of muscle tension in stroke patients, but SAMO-B exhibits a mechanical movement akin to a gear. This is slightly different from the movement of muscle tension in stroke patients. Regarding (c), SAMO-A has a simplified structure to efficiently express the stroke patient’s muscle tone pathology, but SAMO-B has a structure that imitates human bones.
2.2.2. Therapeutic Motion Technique Practice
In the practice task, the same task the student performed in the pre- and post-practice test was performed by the Robo group using SAMO-B (for practice) (Figure 2), which differs from SAMO-A that was used before and after practice. The same task was performed by patients in the Human group, using the elbow of another student. The task was repeated 10 times for three sets. The number of sets was specific to determine the effect of methods on the number of sets that can be performed in one class period. In the Human group, it was difficult to change the degree of muscle tension because the students acted as patients; therefore, only 1 degree of muscle tension (moderate) was used in the Robo group with SAMO-B. During practice, both groups were instructed to (1) move slowly and gently and (2) move the joints over the entire range of motion. These instructions were determined based on the results of an existing study that clarified differences in therapeutic motion techniques between students and therapists, such as high speed of joint movement, short movement time, and insufficient movement of the full range of motion [12].
2.3. Statistical Analysis
2.3.1. Extraction of Feature Quantity and Analysis Method
Figure 1 shows the analysis method employed in this study. Using the recorded elbow joint angle and movement time, we calculated the peak velocity, peak angle ratio, and movement time during flexion and extension as features of the therapeutic motion techniques and used them as analysis items. The peak angle ratio during flexion and extension was calculated by dividing the peak angle recorded during each therapeutic motion task by the peak physical angle of SAMO. The peak physical flexion angle and peak extension angle of SAMO were measured as calibration data before measurement. The movement time was defined as the interval from the onset of the exercise to the end of the exercise. The onset of the exercise was defined as the value when the average resting angular velocity for 3 s before the task was continuously exceeded for ≥50 ms. The end of the exercise was defined as the time when the joint angle became constant after the completion of elbow flexion and extension. To clarify the effect of practice due to differences in practice methods, the peak velocity, peak angle ratio, and movement time during elbow joint flexion and extension were compared between and within the two groups before and after practice using a repeated measures two-way ANOVA. Thereafter, multiple comparisons were performed using the Bonferroni method.
2.3.2. Verification of Students’ Learning Effects through Practice of Therapeutic Motion Techniques
To determine whether the practice improved students’ therapeutic motion techniques to a level comparable to that of therapists, we performed machine learning on students’ pre-practice and therapists’ data and created a discriminant index to distinguish between students and therapists using Support Vector Machine (SVM) and Random Forest (RF) classification. These powerful classification methods can discriminate nonlinearly separable data using kernel functions to map the data to a higher-dimensional space wherein the data become more separable [13,14]. While simple statistical analysis of the data before and after practice can determine how each feature has changed, this analysis cannot assess whether students’ techniques have comprehensively approached those of therapists. Therefore, SVM and RM classification were also implemented. In the present study, the SVM and RF algorithms focused on peak velocity, peak angle ratio, and movement time during flexion and extension in the pre-practice data and found the hypersurface that maximized the margin between the therapist’s and student’s distributions to classify the data into two groups. Using the SVM algorithm, the kinematics data were randomly classified into 24 training and nine testing data points. In the RF classification, the kinematics data were randomly classified into 19 training and five testing data points. The SVM and RF algorithms were formulated based on the training dataset to establish the classification model. Thereafter, to investigate an improvement in the students’ skills after therapeutic motion practice to a therapist’s level, the students’ movement data after practice were distinguished as students = 0 and therapists = 1 using identifiers created by SVM and RF, respectively. For the discrimination results, the number of students who were judged to be students = 0 and therapists = 1 after practicing with SAMO and humans was subjected to the χ2 test.
2.3.3. Statistics Software
Statistical analysis was performed using JASP (JASP Team, 2022, Amsterdam, The Netherlands) [15], with a 5% risk rate for all tests.
3. Results
3.1. Participants
Table 1 shows the general characteristics of the participants of this study. In total, 25 students (nine men, 16 women) and eight therapists (seven men, one woman) were included. Among them, students were randomly distributed to the Robo (13 participants: five men, eight women) and Human (12 participants: four men, eight women) groups. The average clinical experience of therapists was 12.0 ± 3.7 years.

Table 1.
Participants characteristics.
3.2. Comparison of Kinematics Data before and after Exercise Training in the Robo and Human Groups
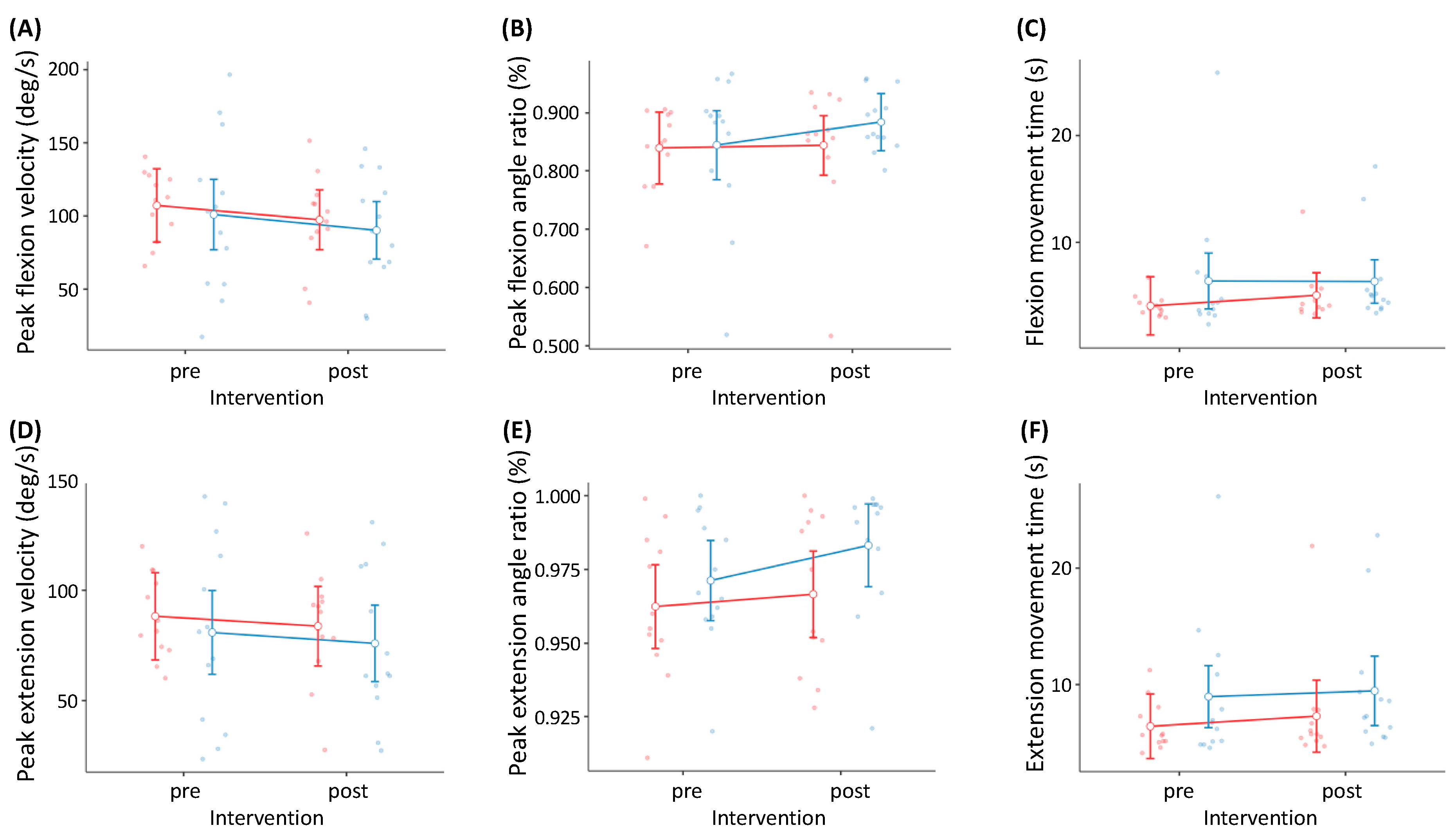
Table 2 and Figure 3 show the comparison of the kinematics data before and after practice for the Robo and Human groups. The main effect before and after practice was observed on the peak angle ratio during elbow extension using SAMO (p = 0.019, η2 = 0.027). However, for other items, there were no main effects or interactions between groups before and after practice.
Table 2.
Comparisons of kinematics data in manual therapy pre- and post-implementation of different methods of exercises.
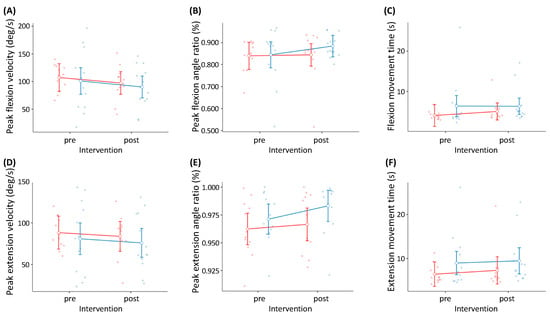
Figure 3.
Multiple comparison of features of therapeutic motion techniques before and after exercise with different exercise methods. (A) Peak flexion velocity; (B) peak flexion angle ratio; (C) flexion movement time; (D) peak extension velocity; (E) peak extension angle ratio; (F) extension movement time. Blue dots: Robo group (n = 13); red dots: Human group (n = 12). Blue-outlined circles: mean values of the Robo group; red-outlined circles: mean values of the Human group; vertical bars: standard deviation. Blue solid line: the slope between the pre- and post-intervention values in the Robo group; red solid line: the slope between the pre- and post-intervention values in the Human group.
3.3. Creation of Identifiers Using Machine Learning and Assessment of the Effect of Therapeutic Motion Technique
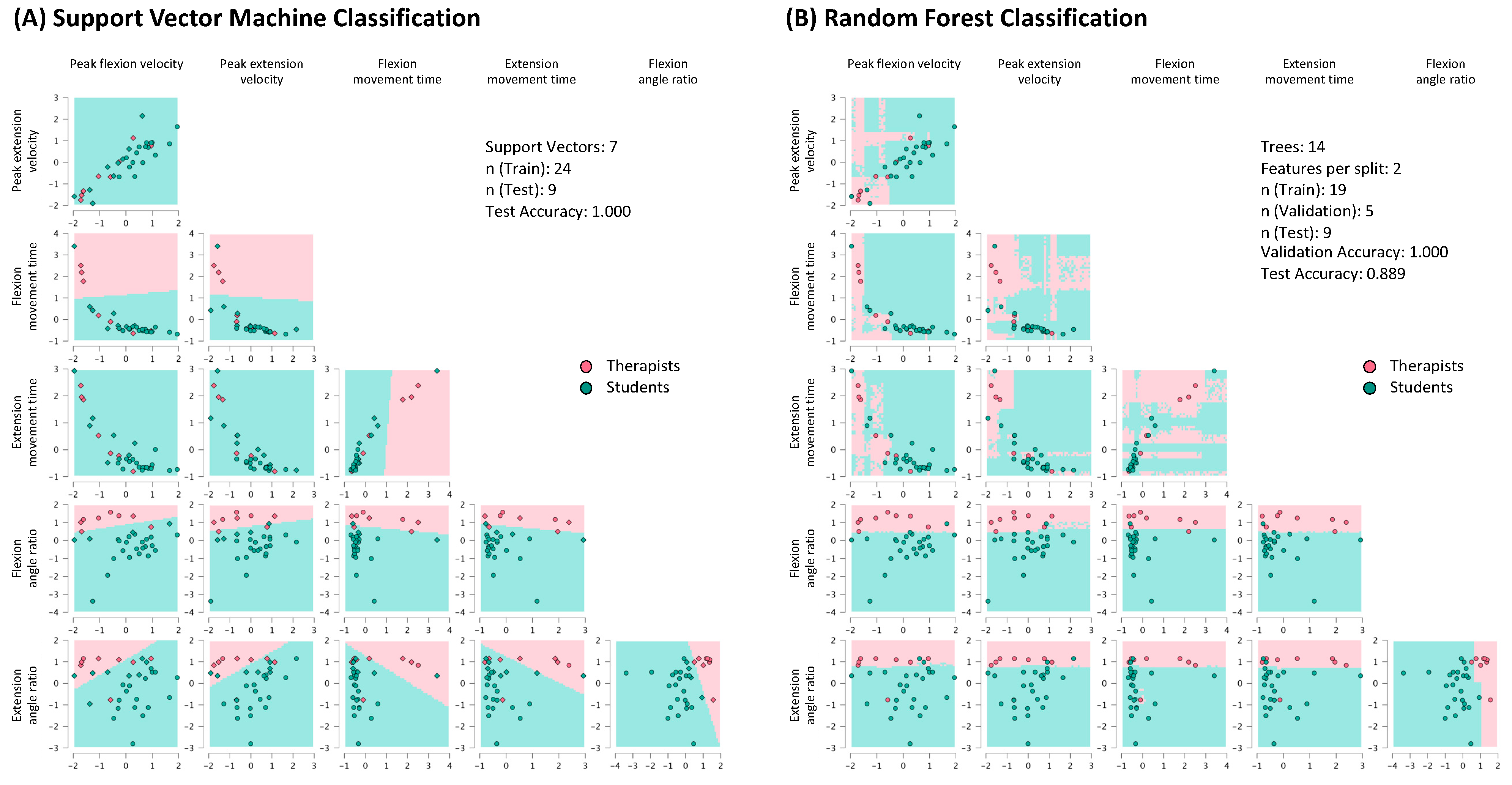
Figure 4 shows the diagram obtained by creating identifiers using machine learning for exercise therapy techniques among students and therapists. Based on identifiers created by machine learning, among the students who had not practiced therapeutic motion techniques, one (7.7%) student in the Robo group and 0 (0.0%) students in the Human group were judged to be at a level similar to the therapists in terms of therapeutic motion techniques, indicating that many students did not possess sufficient skills before practice. Similar results were obtained using the SVM and RF algorithms. Using SVM, five (38.5%) students in the Robo group and 0 (0.0%) students in the Human group were judged to be at a level similar to that of the therapists in terms of exercise therapy techniques. Using RF, seven (53.8%) students in the Robo group and 0 (0.0%) students in the Human group were determined to be at a level similar to therapists in exercise therapy techniques. Compared to the Human group, the Robo group had significantly more students who were judged to have similar therapeutic motion techniques to the therapists (Table 3). For the SVM and RF classifiers, after supervised learning was conducted, accuracy was assessed using test data. The results confirmed an accuracy of 1.000 for SVM and 0.889 for RF.
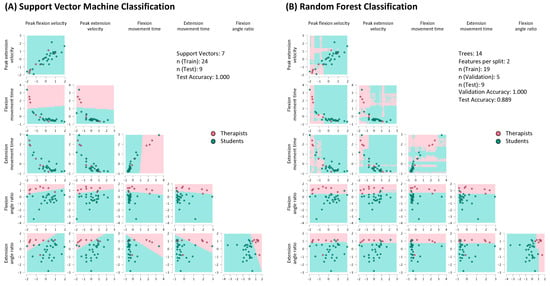
Figure 4.
Creation of identifiers by machine learning in therapeutic motion techniques of students and therapists. (A) Support Vector Machine Classification; (B) Random Forest Classification. Pink dots: therapist group (n = 8), light blue dots: student group (n = 25). In both classifiers (A,B), the pink-shaded regions represent the classification space where data points from the therapist group (pink dots) are predicted, while the blue-shaded regions represent the classification space for the student group (blue dots). These regions visually depict how the machine learning models distinguish between therapists and students based on their performance in therapeutic motion techniques.
Table 3.
Comparisons of the kinematic data of students judged to be comparable to therapists after practicing therapeutic movement techniques.
4. Discussion
In the present study, we demonstrated an effective learning method (practice using a simulation robot vs. practice among students) for teaching therapeutic motion techniques to university students. The results revealed no significant change in the kinematics data after practice in the Robo and Human groups; in addition, the results showed no significant differences between the two groups across any domains. These results suggest that there was no change in the upper limb therapeutic motion techniques in both practice methods. However, the machine learning data of students and therapists showed that there were significantly more students in the Robo group than in the Human group who, after practice, were judged to have the same therapeutic motion techniques as the therapists. Although there was no difference in the kinematics data between the two groups, it was suggested that the number of students who practiced using a robot showed greater improvement in their therapeutic motion techniques than did those who practiced among students.
Muscle tone in hemiplegic stroke patients tends to be speed-dependent, which means that muscle tone tends to increase when the participant moves rapidly [16]. The SAMO used in this study incorporates a speed-dependent mechanism; when the elbow joint is moved rapidly, the resistance received by the operator increases. As the resistance experienced by the operator increases, they would need to apply a greater force to move the elbow joint. Meanwhile, when the operator moves the elbow joint slowly, the corresponding resistance decreases, resulting in a decrease in the force exerted on the operator to move the elbow joint. Therefore, we speculated that the students felt a sense of resistance from the robot during the practice and performed exercise therapy while determining the speed that allowed easy movement. However, in practice between students, the student playing the role of the patient was not sick; therefore, the student playing the role of the therapist did not feel any resistance when moving the elbow joint. Thus, we deduced that the student had difficulty understanding the appropriate movement speed for the patient and that the treatment objective was unclear.
Students are educated via various methods. Among these methods, it is effective to provide education that meets the differences and needs of each learner, such as learning style, culture, language, gender, personality, preferences, and living environment, as well as learning ability. This educational method is called differentiated instruction [17,18]. The results of this study revealed that some students improved their therapeutic motion techniques by practicing with a robot alone. However, other students could not improve their therapeutic motion techniques even after practicing with the same robot. While moving the elbow joint of the robot, students were divided into those who read various information and applied it to their techniques and those who had difficulty applying this information to their techniques. This difference seems to be associated with the ability of individual students. Therefore, it is important to provide education according to the degree of acquisition of therapeutic motion techniques by students, based on the differentiated instruction method.
This study had three main limitations. The first was regarding the relatively small number of practice sets. The number of practice sets in the present study was set to determine the effectiveness of the number of practice sets that could be performed during one class period, and a total of 30 sets were established for both groups. Studies on the effect of practice aimed at skill improvement reported that a practice effect was noted after 20 sets of a free-throw task in basketball [19] and after 40 practice sets of throwing darts at a target [20]. These results show that skills can be improved with a small number of practice sets. In the task of hitting a golf ball accurately, a practice effect was achieved after 60 sets [21]; therefore, the effect of a small number of practice sets cannot be denied. The second limitation was regarding the practice instructions. A study [22] reported that external focus was more effective than internal focus in improving the effectiveness of practice. Instructions during practice in the present study were (1) to move slowly and gently and (2) to move the joints over the entire range of motion. These instructions correspond to the external focus that has been reported to be effective. However, the instructions were abstract rather than specific, as they did not state how slowly to move and how far to move; therefore, the participants may have failed to correctly recognize the intention of the exercise. In our next study, we aim to focus on verification for optimizing the number of practice sets and movement instructions to incorporate robots in the simulation education of upper extremity exercise therapy. The third limitation concerns students’ individual knowledge levels regarding the practice methods. Although we targeted students who had received the same educational content, there was no indication whether the amount of knowledge provided differed. Moreover, it was not determined whether students have fully acquired this knowledge, and it is unclear whether there were differences in individual knowledge levels. Future research should include evaluations of prior knowledge to enable more tailored assessments for students.
Lastly, the use of simulation robots like SAMO allows for repeated, consistent training before working with actual patients, which is one of the advantages of robot-assisted practice. However, practicing solely with robots makes experiencing essential human interaction aspects, such as how to talk to patients, handle their arms, and move them gently, challenging. As a solution, features that enable dialogue may be included. In recent years, the development of communication robots has advanced, and many robots now have conversational capabilities, which allows this solution to be implemented [23]. The benefits and drawbacks of robots should be considered, and over-reliance on them should be discouraged. Education and explanations on proper usage, including mindful consideration of how the robot’s actions translate to patient care, are necessary. In the future, the effects of practice should be verified under various muscle tone conditions to make the training closer to that of actual clinical patients. Although this study focuses on motor therapy for the elbow joint, its findings can be generalized to other joints, such as the fingers, wrist, hip, knee, and ankle joints. Additionally, from the perspective of using simulation robots, this study’s approach could apply to other educational content as well. Therefore, this research can potentially be utilized and expanded in various directions in the future.
5. Conclusions
The results of this study suggest that more students can replicate the therapeutic motion techniques of a therapist by practicing with a robot simulating the pathological motion of a patient than performing simulation practice with other students. Therefore, we believe that the use of a simulation robot that can reproduce a patient’s pathological motion may be effective in teaching therapeutic motion techniques. Furthermore, we believe that it is an effective new learning method for therapeutic motion techniques while limiting interpersonal infection. However, we presumed that the amount of practice is insufficient to reach the skill level of therapists in clinical practice; therefore, further verification of the number of practice sets and instruction methods is required to improve students’ therapeutic motion techniques to the level required for clinical practice.
6. Patents
The educational arm robot (development code Samothrace: SAMO) used in this study is patented (Patent No. 6307210).
Author Contributions
Conceptualization, Y.K. and T.H.; methodology, Y.K. and T.H.; software, Y.K., Y.T. and T.H.; validation, Y.K., A.O., Y.T. and T.H.; formal analysis, Y.K. and T.H.; investigation, Y.K. and T.H.; resources, Y.K., A.O., Y.T. and T.H.; data curation, Y.K., A.O., Y.T. and T.H.; writing—original draft preparation, Y.K.; writing—review and editing, T.H.; visualization, Y.K., A.O., Y.T. and T.H.; supervision, T.H.; project administration, Y.K. and T.H.; funding acquisition, Y.K. and T.H. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Grant-in-Aid for Leading-Edge Industry Design Project sponsored by the Saitama Prefecture 2015–2017 to Toyohiro Hamaguchi and Grant-in-Aid JSPS KAKENHI, grant numbers 17K13059 and 20K11286 to Yuji Koike.
Institutional Review Board Statement
The design of this study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of Saitama Prefectural University (#27112, 4 April 2016).
Informed Consent Statement
Informed consent was obtained from all participants involved in this study.
Data Availability Statement
The datasets generated and/or analyzed during the present study are available from the corresponding author on reasonable request. The data contains personally identifiable information and is not publicly available due to privacy protection concerns.
Acknowledgments
We would like to thank Airi Hiraga and Chiharu Kobayashi, occupational therapy students at Saitama Prefectural University, who participated in the research.
Conflicts of Interest
Author Akihisa Okino was employed by the company Okino Robotics Industries Ltd. Author Yasuhiro Takanami was employed by the company Peritec Corporation. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. This study was supported technically and with supplies by Okino Robotics Industries, Ltd., Peritec Corporation Co., Ltd., and Takei Scientific Instruments Co., Ltd. The funders had no role in the design of this study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Correction Statement
This article has been republished with a minor correction to the readability of Figure 1. This change does not affect the scientific content of the article.
Abbreviations
| ANOVA | analysis of variance |
| JASP | Jeffreys’s Amazing Statistics Program |
| JSPS | Japan Society for the Promotion of Science |
| SAMO | Samothrace |
| SVM | support vector machine |
| RF | random forest |
References
- Koike, Y.; Suzuki, M.; Okino, A.; Takeda, K.; Takanami, Y.; Hamaguchi, T. Differences in manual exercise therapy skills between students and therapists. J. Ergon. Technol. 2019, 19, 35–44. [Google Scholar]
- Hodgetts, S.; Hollis, V.; Triska, O.; Dennis, S.; Madill, H.; Taylor, E. Occupational therapy students’ and graduates’ satisfaction with professional education and preparedness for practice. Can. J. Occup. Ther. 2007, 74, 148–160. [Google Scholar] [CrossRef] [PubMed]
- Tanzawa, T.; Futaki, K.; Kurabayashi, H.; Goto, K.; Yoshihama, Y.; Hasegawa, T.; Yamamoto, M.; Inoue, M.; Miyazaki, T.; Maki, K. Medical emergency education using a robot patient in a dental setting. Eur. J. Dent. Educ. 2013, 17, e114–e119. [Google Scholar] [CrossRef]
- Takanobu, H.; Takanishi, A.; Ozawa, D.; Ohtsuki, K.; Ohnishi, M.; Okino, A. Integrated dental robot system for mouth opening and closing training. In Proceedings of the 2002 IEEE International Conference on Robotics and Automation, Washington, DC, USA, 11–15 May 2002; pp. 1428–1433. [Google Scholar] [CrossRef]
- Koike, Y.; Suzuki, M.; Okino, A.; Takeda, K.; Takanami, Y.; Hamaguchi, T. Distinction of students and expert therapists based on therapeutic motions on a robotic device using support vector machine. J. Med. Biol. Eng. 2020, 40, 790–797. [Google Scholar] [CrossRef]
- Escalon, M.X.; Raum, G.; Francio, V.T.; Eubanks, J.E.; Verduzco-Gutierrez, M. The immediate impact of the coronavirus pandemic and resulting adaptations in physical medicine and rehabilitation medical education and practice. Pm R 2020, 12, 1015–1023. [Google Scholar] [CrossRef] [PubMed]
- Japanese Association of Occupational Therapists. JAOT Post-Qualification Education System. Available online: https://www.jaot.or.jp/en/activities/ (accessed on 12 August 2022).
- Ministry of Health. Labour and Welfare. Available online: https://www.mhlw.go.jp/file/05-Shingikai-10803000-Iseikyoku-Ijika/0000197493.pdf (accessed on 12 August 2022). (In Japanese).
- Japanese Association of Occupational Therapists. Available online: https://www.jaot.or.jp/files/shishin2018.tebiki2022.pdf (accessed on 12 August 2022). (In Japanese).
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Koike, Y.; Okino, A.; Takeda, K.; Takanami, Y.; Hamaguchi, T. Comparison of manipulative indicators of students and therapists using a robotic arm: A feasibility study. Appl. Sci. 2021, 11, 9403. [Google Scholar] [CrossRef]
- Davatzikos, C.; Ruparel, K.; Fan, Y.; Shen, D.G.; Acharyya, M.; Loughead, J.W.; Gur, R.C.; Langleben, D.D. Classifying spatial patterns of brain activity with machine learning methods: Application to lie detection. Neuroimage 2005, 28, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Mohammadpoory, Z.; Nasrolahzadeh, M.; Haddadnia, J. Epileptic seizure detection in EEGs signals based on the weighted visibility graph entropy. Seizure 2017, 50, 202–208. [Google Scholar] [CrossRef] [PubMed]
- JASP Team. JASP. 0.16.3. 2022. Available online: https://jasp-stats.org/ (accessed on 4 September 2024).
- Lance, J.W. Spasticity: Disordered motor control. In Symposium Synopsis; Feldman, R., Young, R., Koells, W., Eds.; Yearbook Medical Publishers: Chicago, IL, USA, 1980; pp. 487–489. [Google Scholar]
- Olenchak, F.R. Lessons learned from gifted children about differentiation. Teach. Educ. 2010, 36, 185–198. [Google Scholar] [CrossRef]
- Tomlinson, C.A. Mapping a route toward differentiated instruction. Educ. Leadersh. 1999, 57, 12–16. [Google Scholar]
- Zachry, T.; Wulf, G.; Mercer, J.; Bezodis, N. Increased movement accuracy and reduced EMG activity as the result of adopting an external focus of attention. Brain Res. Bull. 2005, 67, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Marchant, D.C.; Clough, P.J.; Crawshaw, M. The effects of attentional focusing strategies on novice dart throwing performance and their task experiences. Int. J. Sport Exerc. Psychol. 2007, 5, 291–303. [Google Scholar] [CrossRef]
- Wulf, G.; Su, J. An external focus of attention enhances golf shot accuracy in beginners and experts. Research Q. Exerc. Sport 2007, 78, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Wulf, G.; McConnel, N.; Gartner, M.; Schwarz, A. Enhancing the learning of sport skills through external-focus feedback. J. Mot. Behav. 2002, 34, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Kok, C.L.; Ho, C.K.; Teo, T.H.; Kato, K.; Koh, Y.Y. A novel implementation of a social robot for sustainable human engagement in homecare services. Sensors 2024, 24, 4466. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).