
Three-Dimensional Assessment of the Effects of Kinesio Taping on Mandibular Condylar Volume with Skeletal Class II Malocclusions


Abstract
:1. Introduction
2. Materials and Methods
- ANB > 4°,
- Mandibular retrognathia,
- Convex profile,
- Class II division 1 dental malocclusion,
- Skeletal maturity varied between the CS2 and CS3 stages according to the Cervical Vertebral Maturation (CVM) index.
- Patients with TMJ pain or dysfunction,
- Craniofacial abnormalities,
- Limited mouth opening,
- Class II division 2 dental malocclusion,
- Significant mandibular asymmetry were excluded.
2.1. Sample Size Calculation
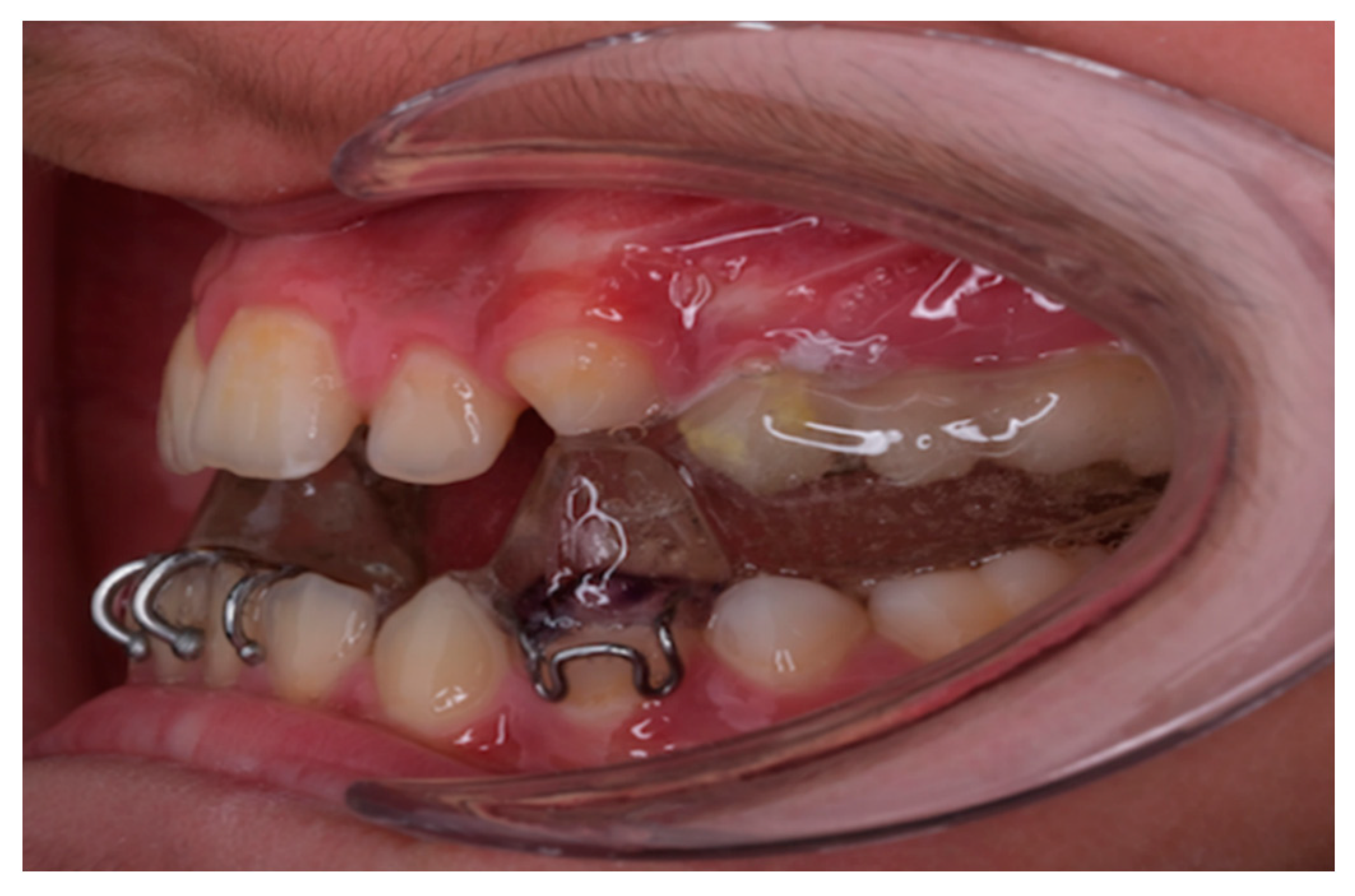
2.2. Twin Block and Kinesio Tape Applying
2.3. Imaging the Condyle
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
- Applying Twin Block therapy to patients during the growth period has significantly increased bilateral condylar volumes.
- Kinesio taping with Twin Block therapy during the three-month period had a positive impact on condylar volume.
- The application of Kinesio taping in conjunction with Twin Block therapy has slightly increased condylar volumes compared to patients received only Twin Block therapy.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Graber, T.M. Physiologic Principles of Functional Appliances; Mosby: St. Louis, MO, USA, 1985. [Google Scholar]
- Rakosi, T.; Graber, T.; Petrovic, A. Dentofacial Orthopedics with Functional Appliances; Mosby: St. Louis, MO, USA, 1985. [Google Scholar]
- Keeling, S.D.; Wheeler, T.T.; King, G.J.; Garvan, C.W.; Cohen, D.A.; Cabassa, S.; McGorray, S.P.; Taylor, M.G. Anteroposterior skeletal and dental changes after early Class II treatment with bionators and headgear. Am. J. Orthod. Dentofac. Orthop. 1998, 113, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Tulloch, J.C.; Proffit, W.R.; Phillips, C. Outcomes in a 2-phase randomized clinical trial of early Class II treatment. Am. J. Orthod. Dentofac. Orthop. 2004, 125, 657–667. [Google Scholar] [CrossRef] [PubMed]
- Raposo, R.; Peleteiro, B.; Paço, M.; Pinho, T. Orthodontic camouflage versus orthodontic-orthognathic surgical treatment in class II malocclusion: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2018, 47, 445–455. [Google Scholar] [CrossRef]
- Varlık, S.K.; Gültan, A.; Tümer, N. Comparison of the effects of Twin Block and activator treatment on the soft tissue profile. Eur. J. Orthod. 2008, 30, 128–134. [Google Scholar] [CrossRef]
- Clark, W.J. Twin-Block Functional Therapy, 2nd ed.; Mosby: St. Louis, MO, USA, 2002. [Google Scholar]
- Batista, K.B.; Thiruvenkatachari, B.; Harrison, J.E.; D O’Brien, K. Orthodontic treatment for prominent upper front teeth (Class II malocclusion) in children and adolescents. Cochrane Database Syst. Rev. 2018, 2018, CD003452. [Google Scholar] [CrossRef]
- Magno, M.B.; Nadelman, P.; Leite, K.L.d.F.; Ferreira, D.M.; Pithon, M.M.; Maia, L.C. Associations and risk factors for dental trauma: A systematic review of systematic reviews. Community Dent. Oral Epidemiol. 2020, 48, 447–463. [Google Scholar] [CrossRef]
- O’Brien, K.; Wright, J.; Conboy, F.; Chadwick, S.; Connolly, I.; Cook, P.; Birnie, D.; Hammond, M.; Harradine, N.; Lewis, D. Effectiveness of early orthodontic treatment with the Twin-block appliance: A multicenter, randomized, controlled trial. Part 2: Psychosocial effects. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 488–494. [Google Scholar] [CrossRef]
- O’brien, K.; Wright, J.; Conboy, F.; Sanjie, Y.; Mandall, N.; Chadwick, S.; Connolly, I.; Cook, P.; Birnie, D.; Hammond, M. Effectiveness of treatment for Class II malocclusion with the Herbst or twin-block appliances: A randomized, controlled trial. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 128–137. [Google Scholar] [CrossRef]
- McNamara, J.A., Jr. Functional determinants of craniofacial size and shape. Eur. J. Orthod. 1980, 2, 131–159. [Google Scholar] [CrossRef]
- O’Brien, K.; Wright, J.; Conboy, F.; Sanjie, Y.; Mandall, N.; Chadwick, S.; Connolly, I.; Cook, P.; Birnie, D.; Hammond, M. Effectiveness of early orthodontic treatment with the Twin-block appliance: A multicenter, randomized, controlled trial. Part 1: Dental and skeletal effects. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 234–243. [Google Scholar] [CrossRef]
- Akan, B.; Ünlü Kurşun, B. Structural changes in the trabecular bone of the mandibular condyle of growing patients with sagittal jaw discrepancy treated with the twin-block appliance. Orthod. Craniofacial Res. 2022, 25, 142–149. [Google Scholar] [CrossRef]
- Fushima, K.; Kitamura, Y.; Mita, H.; Sato, S.; Suzuki, Y.; Kim, Y.H.; Department of Orthodontics, Kanagawa Dental College, Yokosuka, Kanagawa, Japan. Significance of the cant of the posterior occlusal plane in Class II division I malocclusions. Eur. J. Orthod. 1996, 18, 27–40. [Google Scholar] [CrossRef]
- Koretsi, V.; Zymperdikas, V.F.; Papageorgiou, S.N.; Papadopoulos, M.A. Treatment effects of removable functional appliances in patients with Class II malocclusion: A systematic review and meta-analysis. Eur. J. Orthod. 2015, 37, 418–434. [Google Scholar] [CrossRef]
- Oyonarte, R.; Zárate, M.; Rodriguez, F. Low-intensity pulsed ultrasound stimulation of condylar growth in rats. Angle Orthod. 2009, 79, 964–970. [Google Scholar] [CrossRef]
- Hameed Mohamed, M.A.; Abdallah, K.F.; Hussein, F.A. Three-dimensional assessment of mandibular condylar volume and position subsequent to twin block functional therapy of skeletal class II malocclusion accompanied by low-level laser therapy. Dent. J. 2020, 8, 115. [Google Scholar] [CrossRef] [PubMed]
- Celiker, R.; Guven, Z.; Aydog, T.; Bagis, S.; Atalay, A.; Yagci, H.C.; Korkmaz, N. The kinesiologic taping technique and its applications/Kinezyolojik bantloma teknigi ve uygulama alanlari. Turk. J. Phys. Med. Rehabil. 2011, 57, 225–236. [Google Scholar]
- Katsavrias, E. A method for integrating facial cephalometry and corrected lateral tomography of the temporomandibular joint. Dentomaxillofac. Radiol. 2003, 32, 93–96. [Google Scholar] [CrossRef] [PubMed]
- Kadesjö, N.; Benchimol, D.; Falahat, B.; Näsström, K.; Shi, X. Evaluation of the effective dose of cone beam CT and multislice CT for temporomandibular joint examinations at optimized exposure levels. Dentomaxillofac. Radiol. 2015, 44, 20150041. [Google Scholar] [CrossRef]
- Keskinruzgar, A.; Kucuk, A.O.; Yavuz, G.Y.; Koparal, M.; Caliskan, Z.G.; Utkun, M. Comparison of kinesio taping and occlusal splint in the management of myofascial pain in patients with sleep bruxism. J. Back Musculoskelet. Rehabil. 2019, 32, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Ristow, O.; Hohlweg-Majert, B.; Kehl, V.; Koerdt, S.; Hahnefeld, L.; Pautke, C. Does elastic therapeutic tape reduce postoperative swelling, pain, and trismus after open reduction and internal fixation of mandibular fractures? J. Oral Maxillofac. Surg. 2013, 71, 1387–1396. [Google Scholar] [CrossRef]
- Bae, Y. Change the myofascial pain and range of motion of the temporomandibular joint following kinesio taping of latent myofascial trigger points in the sternocleidomastoid muscle. J. Phys. Ther. Sci. 2014, 26, 1321–1324. [Google Scholar] [CrossRef]
- Kase, K.; Wallis, J.; Kase, T. Clinical Therapeutic Applications of the Kinesio Taping Method, 2nd ed.; Kinesio Taping Association: Tokyo, Japan, 2003. [Google Scholar]
- Pautz, N.; Olivier, B.; Steyn, F. The use of parametric effect sizes in single study musculoskeletal physiotherapy research: A practical primer. Phys. Ther. Sport 2018, 32, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. The effect size. In Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988; pp. 77–83. [Google Scholar]
- Zhang, L.; Luo, J.; Wan, P.; Wu, J.; Laski, F.; Chen, J. Regulation of cofilin phosphorylation and asymmetry in collective cell migration during morphogenesis. Development 2011, 138, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, E.; Karacay, S.; Erkan, M. Condylar response to functional therapy with Twin-Block as shown by cone-beam computed tomography. Angle Orthod. 2014, 84, 1018–1025. [Google Scholar] [CrossRef] [PubMed]
- Petrovic, A.G.; Stutzmann, J.J.; Oudet, C.L. Control processes in the postnatal growth of mandibular cartilage. Rev. Iberoam Ortod. 1986, 6, 11–58. [Google Scholar] [PubMed]
- Thelen, M.D.; Dauber, J.A.; Stoneman, P.D. The clinical efficacy of kinesio tape for shoulder pain: A randomized, double-blinded, clinical trial. J. Orthop. Sports Phys. Ther. 2008, 38, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Cools, A.; Witvrouw, E.; Danneels, L.; Cambier, D. Does taping influence electromyographic muscle activity in the scapular rotators in healthy shoulders? Man. Ther. 2002, 7, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Nordström, P.; Thorsen, K.; Bergström, E.; Lorentzon, R. High bone mass and altered relationships between bone mass, muscle strength, and body constitution in adolescent boys on a high level of physical activity. Bone 1996, 19, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Khadra, M.; Kasem, N.; Haanæs, H.R.; Ellingsen, J.E.; Lyngstadaas, S.P. Enhancement of bone formation in rat calvarial bone defects using low-level laser therapy. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2004, 97, 693–700. [Google Scholar] [CrossRef]
- Chen, J.-w.; Zhou, Y.-c. Effect of low level carbon dioxide laser radiation on biochemical metabolism of rabbit mandibular bone callus. Laser Ther. 2004, 14, 0_41–40_44. [Google Scholar] [CrossRef]
- Kobu, Y. Effects of infrared radiation on intraosseous blood flow and oxygen tension in the rat tibia. Kobe J. Med. Sci. 1999, 45, 27–39. [Google Scholar] [PubMed]
- Shakeri, H.; Keshavarz, R.; Arab, A.M.; Ebrahimi, I. Clinical effectiveness of kinesiological taping on pain and pain-free shoulder range of motion in patients with shoulder impingement syndrome: A randomized, double blinded, placebo-controlled trial. Int. J. Sports Phys. Ther. 2013, 8, 800. [Google Scholar] [PubMed]
- Halski, T.; Dymarek, R.; Ptaszkowski, K.; Słupska, L.; Rajfur, K.; Rajfur, J.; Pasternok, M.; Smykla, A.; Taradaj, J. Kinesiology taping does not modify electromyographic activity or muscle flexibility of quadriceps femoris muscle: A randomized, placebo-controlled pilot study in healthy volleyball players. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2015, 21, 2232. [Google Scholar]
- Bresin, A. Effects of masticatory muscle function and bite-raising on mandibular morphology in the growing rat. Swed. Dent. J. Suppl. 2001, 150, 1–49. [Google Scholar]
- Romagnuolo, L.; Tayal, V.; Tomaszewski, C.; Saunders, T.; Norton, H.J. Optic nerve sheath diameter does not change with patient position. Am. J. Emerg. Med. 2005, 23, 686–688. [Google Scholar] [CrossRef] [PubMed]
- Malmgren, O.; Ömblus, J.; Hägg, U.; Pancherz, H. Treatment with an orthopedic appliance system in relation to treatment intensity and growth periods A study of initial effects. Am. J. Orthod. Dentofac. Orthop. 1987, 91, 143–151. [Google Scholar] [CrossRef]
- Arat, M.; Isere, H.; Ozdiler, E.; Gürbüs, F. Time factors in functional treatment of skeletal Class II. Informationen Aus Orthod. Und Kieferorthopadie Mit. Beitragen Aus. Der. Int. Lit. 1988, 20, 363–376. [Google Scholar]
- Pancherz, H.; Hägg, U. Dentofacial orthopedics in relation to somatic maturation: An analysis of 70 consecutive cases treated with the Herbst appliance. Am. J. Orthod. 1985, 88, 273–287. [Google Scholar] [CrossRef] [PubMed]
- Mills, C.M.; McCulloch, K.J. Treatment effects of the twin block appliance: A cephalometric study. Am. J. Orthod. Dentofac. Orthop. 1998, 114, 15–24. [Google Scholar] [CrossRef]
- Toth, L.R.; McNamara, J.A., Jr. Treatment effects produced by the Twin-block appliance and the FR-2 appliance of Fränkel compared with an untreated Class II sample. Am. J. Orthod. Dentofac. Orthop. 1999, 116, 597–609. [Google Scholar] [CrossRef] [PubMed]
- DeVincenzo, J.P.; Winn, M.W. Orthopedic and orthodontic effects resulting from the use of a functional appliance with different amounts of protrusive activation. Am. J. Orthod. Dentofac. Orthop. 1989, 96, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Illing, H.M.; Morris, D.O.; Lee, R.T. A prospective evaluation of Bass, Bionator and Twin Block appliances. Part I-The hard tissues. Eur. J. Orthod. 1998, 20, 501–516. [Google Scholar] [CrossRef]
- Bishara, S.E.; Ziaja, R.R. Functional appliances: A review. Am. J. Orthod. Dentofac. Orthop. 1989, 95, 250–258. [Google Scholar] [CrossRef]
- Hwang, H.-S.; Jiang, T.; Sun, L.; Lee, K.-M.; Oh, M.-H.; Biao, Y.; Oh, H.-K.; Bechtold, T.E. Condylar head remodeling compensating for condylar head displacement by orthognathic surgery. J. Cranio-Maxillofac. Surg. 2019, 47, 406–413. [Google Scholar] [CrossRef] [PubMed]
- Fuentes, M.A.; Opperman, L.A.; Buschang, P.; Bellinger, L.L.; Carlson, D.S.; Hinton, R.J. Lateral functional shift of the mandible: Part I. Effects on condylar cartilage thickness and proliferation. Am. J. Orthod. Dentofac. Orthop. 2003, 123, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Ruf, S.; Baltromejus, S.; Pancherz, H. Effective condylar growth and chin position changes in activator treatment: A cephalometric roentgenographic study. Angle Orthod. 2001, 71, 4–11. [Google Scholar]
- Hilgers, M.L.; Scarfe, W.C.; Scheetz, J.P.; Farman, A.G. Accuracy of linear temporomandibular joint measurements with cone beam computed tomography and digital cephalometric radiography. Am. J. Orthod. Dentofac. Orthop. 2005, 128, 803–811. [Google Scholar] [CrossRef]
- Herrero Solano, Y.; Espinosa Guerra, A.I.; Montoya Pedrón, A.; Soto Cantero, L.A.; Arias Molina, Y. Los bloques gemelos en el tratamiento de las maloclusiones clase III. Revisión. Multimed 2022, 26, 1–17. [Google Scholar]
- Katzberg, R.W. Temporomandibular joint imaging. Radiology 1989, 170, 297–307. [Google Scholar] [CrossRef] [PubMed]
- Hansson, L.-G.; Westesson, P.-L.; Eriksson, L. Comparison of tomography and midfield magnetic resonance imaging for osseous changes of the temporomandibular joint. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 1996, 82, 698–703. [Google Scholar] [CrossRef]
- Tsiklakis, K.; Syriopoulos, K.; Stamatakis, H. Radiographic examination of the temporomandibular joint using cone beam computed tomography. Dentomaxillofacial Radiol. 2004, 33, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Liu, X.; Leng, S.; Kofler, J.M.; Ramirez-Giraldo, J.C.; Qu, M.; Christner, J.; Fletcher, J.G.; McCollough, C.H. Radiation dose reduction in computed tomography: Techniques and future perspective. Imaging Med. 2009, 1, 65. [Google Scholar] [CrossRef] [PubMed]
- Breiman, R.S.; Beck, J.W.; Korobkin, M.; Glenny, R.; Akwari, O.E.; Heaston, D.K.; Moore, A.V.; Ram, P.C. Volume determinations using computed tomography. Am. J. Roentgenol. 1982, 138, 329–333. [Google Scholar] [CrossRef]
- Tecco, S.; Saccucci, M.; Nucera, R.; Polimeni, A.; Pagnoni, M.; Cordasco, G.; Festa, F.; Iannetti, G. Condylar volume and surface in Caucasian young adult subjects. BMC Med. Imaging 2010, 10, 28. [Google Scholar] [CrossRef] [PubMed]
- McNamara, J.A., Jr.; Carlson, D.S. Quantitative analysis of temporomandibular joint adaptations to protrusive function. Am. J. Orthod. 1979, 76, 593–611. [Google Scholar] [CrossRef] [PubMed]
- Alexander, C.; Stynes, S.; Thomas, A.; Lewis, J.; Harrison, P. Does tape facilitate or inhibit the lower fibres of trapezius? Man. Ther. 2003, 8, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Soriano, J.; Abián-Vicén, J.; Aparicio-García, C.; Ruiz-Lázaro, P.; Simón-Martínez, C.; Bravo-Esteban, E.; Fernández-Rodríguez, J.M. The effects of Kinesio taping on muscle tone in healthy subjects: A double-blind, placebo-controlled crossover trial. Man. Ther. 2014, 19, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Bicici, S.; Karatas, N.; Baltaci, G. Effect of athletic taping and kinesiotaping® on measurements of functional performance in basketball players with chronic inversion ankle sprains. Int. J. Sports Phys. Ther. 2012, 7, 154. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | p | |||
|---|---|---|---|---|
| Group I (n = 15) | Group II (n = 14) | |||
| Gender, n (%) | Female | 8 (53.3) | 8 (57.1) | a 0.837 |
| Male | 7 (46.7) | 6 (42.9) | ||
| Age (years) | Mean ± Sd | 12.78 ± 0.97 | 12.82 ± 1.21 | b 0.813 |
| Median (Min–Max) | 12.75 (11–15) | 12.66 (10–15) | ||
| Right Condyle Volume (cm3) | Group I (n = 15) | Group II (n = 14) | %95 CI | p | |
|---|---|---|---|---|---|
| Initial Condyle Volume | Mean ± Sd | 1.85 ± 0.30 | 1.77 ± 0.38 | [−0.18: 0.34] | a 0.591 |
| Median (min–max) | 1.8 (1.4–2.3) | 1.8 (1.1–2.6) | |||
| Final Condyle Volume | Mean ± Sd | 1.98 ± 0.28 | 1.93 ± 0.37 | [−0.21: 0.29] | a 0.591 |
| Median (min–max) | 2.1 (1.4–2.3) | 2 (1.4–2.6) | |||
| Difference ∆ | p | b 0.015 * | b 0.008 ** | ||
| Initial–final | Mean ± Sd | 0.13 ± 0.17 | 0.16 ± 0.17 | [−0.16: 0.09] | a 0.331 |
| Effect size | Cohen’s D | 0.652 | 0.426 | ||
| %95 CI | [0.04: 0.22] | [0.06: 0.26] | |||
| Left Condyle Volume (cm3) | Group I (n = 15) | Group II (n = 14) | %95 CI | p | |
|---|---|---|---|---|---|
| Initial Condyle Volume | Mean ± Sd | 1.63 ± 0.29 | 1.78 ± 0.58 | [−0.49: 0.19] | a 0.621 |
| Median (min–max) | 1.7 (1.2–2.1) | 1.7 (1–3) | |||
| Final Condyle Volume | Mean ± Sd | 1.93 ± 0.28 | 1.89 ± 0.40 | [−0.22: 0.30] | a 0.652 |
| Median (min–max) | 1.9 (1.4–2.4) | 1.8 (1.4–2.8) | |||
| Difference ∆ | p | b 0.001 ** | b 0.019 * | ||
| Initial–final | Mean ± Sd | 0.30 ± 0.21 | 0.11 ± 0.38 | [−0.04: 0.42] | a 0.158 |
| Effect size | Cohen’s D | 1.052 | 0.220 | ||
| %95 CI | [0.18: 0.42] | [0.11: 0.33] | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bolukbasi, M.; Baser, B.; Akkaya, S.; Ozunlu Pekyavas, N. Three-Dimensional Assessment of the Effects of Kinesio Taping on Mandibular Condylar Volume with Skeletal Class II Malocclusions. Appl. Sci. 2024, 14, 8845. https://doi.org/10.3390/app14198845
Bolukbasi M, Baser B, Akkaya S, Ozunlu Pekyavas N. Three-Dimensional Assessment of the Effects of Kinesio Taping on Mandibular Condylar Volume with Skeletal Class II Malocclusions. Applied Sciences. 2024; 14(19):8845. https://doi.org/10.3390/app14198845
Chicago/Turabian StyleBolukbasi, Merve, Baris Baser, Selcuk Akkaya, and Nihan Ozunlu Pekyavas. 2024. "Three-Dimensional Assessment of the Effects of Kinesio Taping on Mandibular Condylar Volume with Skeletal Class II Malocclusions" Applied Sciences 14, no. 19: 8845. https://doi.org/10.3390/app14198845