Abstract
This study aimed to comprehensively evaluate the effects of intermittent hypoxic training (IHT) on anaerobic performance in young, untrained men. Young men (n = 48) were randomly divided into two training groups and a control group. The training groups performed the same submaximal interval training (three times a week for 4 weeks) in normoxia (200 m asl) or in hypoxia (IHT) (FIO2 = 14.4%). The workloads for the interval training corresponded to the intensity of the ventilatory thresholds determined in a graded test. Participants performed a supramaximal all-out sprint test in normoxia twice: before and after the training. Significant improvement in both absolute peak power (p < 0.001; ES = 0.34) and relative peak power (p < 0.001; ES = 0.54) was noted after IHT. Similar changes were not observed either after training in normoxia (p = 0.14 and p = 0.26, for absolute and relative peak power, respectively) or in the control group (p = 0.34 and p = 0.51, for absolute and relative peak power, respectively). Compared to baseline, there were no significant changes in the absolute and relative mean power of either group after training. Intermittent hypoxic training in young, untrained men can be effective in improving their peak power, but does not significantly affect their mean power.
1. Introduction
Hypoxic training is considered one of the training methods that can effectively improve sea-level performance. This training method is becoming increasingly popular among elite athletes [1]. Several hypoxic training models are used in practice, and their effectiveness is constantly being verified and their training methods optimized [2]. The effects of hypoxic training on aerobic endurance are well described [3,4], and the reason for the improvement in aerobic capacity (endurance performance) is primarily attributed to improvements in hematological indices, i.e., an increase in erythrocyte count, blood hemoglobin concentration or blood oxygen capacity [2]. Training in hypoxia also produces beneficial non-hematological effects such as increased skeletal muscle mitochondrial density and fiber cross-sectional area, or an improved capillary-to-fiber ratio [4,5], enhanced glycolysis [6] and improved buffering capacity [7]. These reported non-hematological effects of training in hypoxia suggest that hypoxic training may also be effective in improving anaerobic performance. Previous studies on the effects of hypoxic training on anaerobic capacity are scarce (compared to the number of studies on the effects of hypoxia on endurance performance) [1], and the data presented are inconclusive, and often contradictory. Previous studies have reported both improvements in peak power [8,9], and no effect of training in hypoxia on anaerobic performance [1,10]. The ambiguity in the effectiveness of training in hypoxia is usually explained by the use of different hypoxic training models, participant inclusion criteria, or the ‘dose’ of hypoxia [4]. One of the more currently popular training methods is intermittent hypoxic training (IHT), whereby the athlete only trains under hypoxia (usually a few tens of minutes) and lives in normoxia. The advantage of this method is that it does not interfere with athletes’ lifestyle, sleep and post-exercise recovery, and that it is relatively low cost [11,12]. This form of training (IHT) is classified as part of the ‘Live Low-Train High’ training model.
Many sports are combined (aerobic and anaerobic) in nature, so hypoxic training may prove to be a universal training method used to improve not only aerobic but also anaerobic capacity [13,14,15]. Typical anaerobic efforts rely on the alactic energy system (ATP and phosphocreatine (PCr)) (up to 8–10 s of supramaximal exercise) and/or the lactic (glycolytic) energy system (usually 20–90 s of supramaximal exercise) [16]. In analyzing an anaerobic effort of supramaximal intensity lasting several tens of seconds, a number of phases can be distinguished in it, which finally determine the sports result in competition. In an ideal effort, after starting the effort from a stationary start, the athlete must reach maximal power as quickly as possible (short time to reach maximal power), and the maximal power itself must be as high as possible, determining the anaerobic alactic performance [17]. Once maximal power is reached, as the exercise progresses, the key is to maintain maximal power for as long as possible and to have the smallest possible power decrease per second of exercise. A small drop in the power and fatigue rate indicate a high efficiency of the glycolytic energy system and good anaerobic endurance [17]. During such an effort, the athlete should perform as much work as possible, and the average power from the entire effort should also be high. Thus, there are a number of parameters that characterize anaerobic performance, and have practical applications in sports training. These parameters are relatively rarely reported, and the authors of previous papers [1,9] have focused only on maximal or mean power. The purpose of this study was to comprehensively determine the effects of IHT on anaerobic performance in young healthy men. We hypothesized that IHT can significantly improve both their peak and mean power.
2. Methods
2.1. Study Design
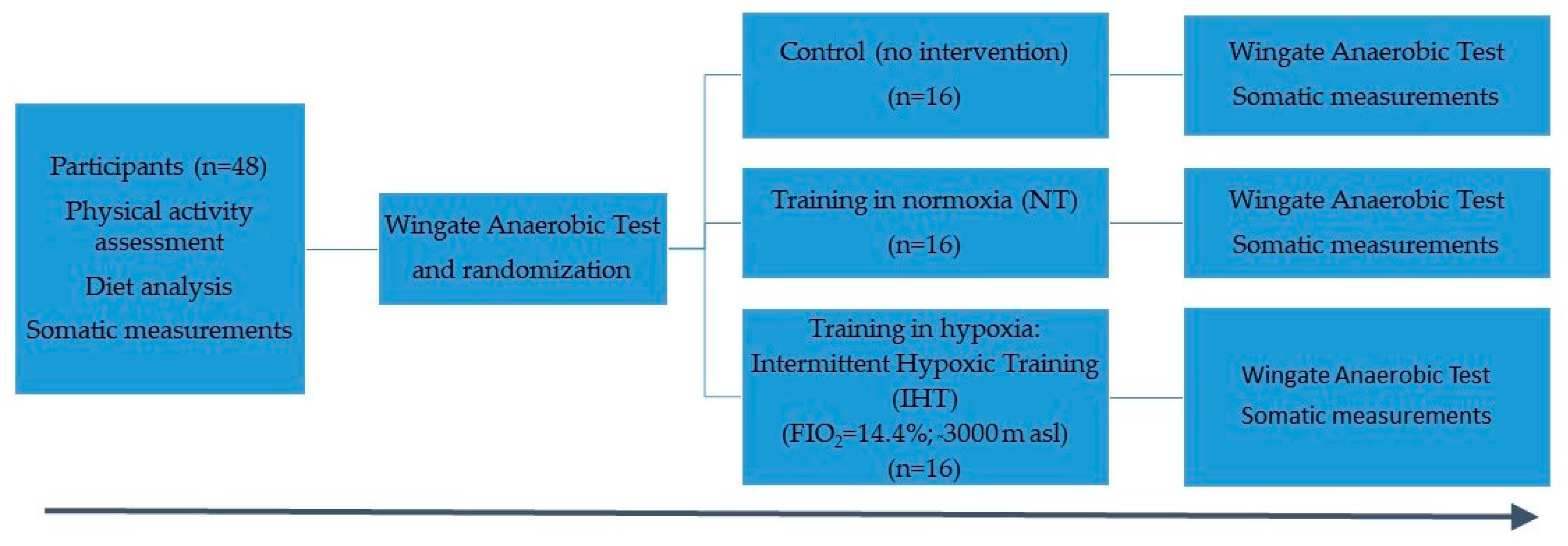
Forty-eight men volunteered to participate in the study. The main criterion for inclusion was the absence of medical contraindications to high-intensity physical exertion. All participants were healthy for the performance testing and training. Recruited men, prior to the start of the intervention, participated in a medical examination to exclude medical contraindications to participation in the study. The medical examination included an exercise ECG and blood tests to exclude anemia or low hemoglobin and iron concentrations. Another exclusion criterion was also any training (including hypoxia training or exposure) performed in the 6 months prior to the beginning of the intervention. Participants were randomly divided into three groups: group training in normoxia (200 m asl) (NT), group training in in hypoxia (IHT) (FIO2 = 14.4%) and the control group (ctrl). Randomization was based on the participant drawing a group (ctrl, NT, IHT). In each group there were 16 participants. Training groups performed the same submaximal interval training (3 times per week for 4 weeks). The workloads for interval training corresponded to the intensity of ventilatory thresholds. The participants performed a Wingate Anaerobic Test (WAnT) in normoxia twice: before and 7–10 days after the training. Somatic measurements were taken on the same day that the all-out test was performed. Habitual diet and physical activity were assessed for each participant (Figure 1). The participants were instructed to maintain their habitual diet and physical activity during intervention. Before the intervention began, participants were familiarized with the all-out test procedure. They also performed a trial supramaximal anaerobic all-out test. Participants had to abstain from eating 2 h before testing, and were asked not to participate in any stressful exercise 24 h before the test. No alcohol or caffeinated drinks were allowed before the tests. This study was approved by the Bioethical Commission of the Regional Medical Chamber in Krakow, Poland (opinion no. 47/KB/OIL/2022). The study was performed in accordance with the ethical standards of the Declaration of Helsinki. All participants provided written informed consent after being informed about the study protocol.
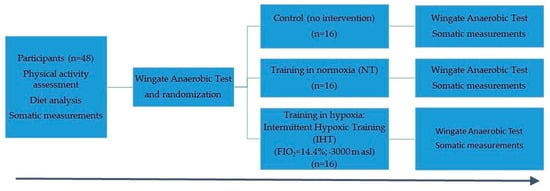
Figure 1.
Study flow.
2.2. Somatic Measurements
Somatic measurements took place on the first day of the study, and included a measurement of body mass (BM), body composition and body height (BH). Body mass and body composition were measured using a body composition analyzer (Jawon Medical, IOI-353, Seoul, Republic of Korea). Measurements were taken in the morning, participants were properly hydrated, and the participants’ feet and hands were degreased just before the measurement. The body composition analysis involved the measurement of fat mass (FM), body fat (%FAT) and lean body mass (LBM). For each participant their body mass index (BMI) was calculated. A stadiometer (Seca 217, Hamburg, Germany) was used for BH measurement. Body mass was measured to an accuracy of 0.1 kg, and body height to 1 mm.
2.3. Physical Activity and Diet
The long version of the International Physical Activity Questionnaire (IPAQ) was used to assess the self-declared physical activity of participants [18,19]. The volume of activity was computed by its energy requirements, defined in multiples of the resting metabolic rate (METs), and scored in MET-minutes per week. The MET-minute was computed by multiplying the MET score of an activity by the minutes performed. Participants were instructed how to complete the questionnaire, and it was filled out in the presence of a researcher, who clarified any doubts, if necessary. The data represent physical activity before the training intervention.
Caloric intake was estimated using the Fitatu (Fitatu 3.37, Poznan, Poland) application [20]. During the first week of the observation, participants kept food diaries for 7 days, entering the type of food consumed and its volume or weight into the diary. Caloric intake was presented as the number of kilocalories per week (kcal/week).
2.4. Training
The workloads (intensity) for interval training were individually determined by the results of an incremental test, and corresponded to the intensity of ventilatory thresholds.
Participants performed the graded test on a cyclergometer (eBike, GE Health Care, Chicago, IL, USA). The aim of this test was to determine individual training workloads in relation to the first ventilatory threshold (VT1) and second ventilatory threshold (VT2). The ventilatory thresholds were determined using the respiratory equivalents method [21,22]. The ramp protocol was used. After a 4 min warm-up at 60 watts, power was increased by 15 watts/min, and the test was preformed until volitional exhaustion. The respiratory indicators, e.g., oxygen uptake (VO2), carbon dioxide production (VCO2), pulmonary ventilation (VE), fractional concentrations of expired CO2 (%FECO2) and O2 (%FEO2), ventilatory equivalent ratio for oxygen (VE/VO2) and carbon dioxide (VE/VCO2) were measured using the breath by breath method (MetaLyzer 3R ergospirometer, Cortex, Leipzig, Germany). The criteria for the determination of the ventilatory thresholds were as follows: for VT1—minimal level of FEO2 and VE/VO2; for VT2—maximal level of FECO2, minimal level of VE/VCO2 and a non-linear increase in VE [21,22].
Interval training at submaximal intensity was performed on a cycloergometer (Wattbike, Nottingham, UK) in a hypoxic chamber (Hypoxico, Bickenbach, Germany) (3000 m above sea level, FIO2 = 14.4%), or in normoxia, and lasted 60 min. After a 6 min warm-up with intensity at VT1, the participant performed 6 series of bouts of exercise in a pattern of 6 min of effort with the intensity at VT2, and 3 min of active recovery with the intensity at VT1. Workouts took place at a room temperature of 21 ± 0.5 °C and humidity of 40 ± 1%.
2.5. Supramaximal All-Out Test—Wingate Anaerobic Test
The Wingate Anaerobic Test [23] was performed twice: before the first training session and after the last training session (7–10 days). The supramaximal all-out sprint test was conducted on a cyclergometer (E834, Monark, Vansbro, Sweden). The cyclergometer was equipped with a rotation timer and connected to a computer. Software (MCE 5.1, JBA Staniak, Warsaw, Poland) was used to calculate the following indicators: peak power (PP), time to reach peak power (TTR-PP), peak power maintenance time (TM-PP), mean power (MP), fatigue index (FI), power decrease (PD) and total work (TW). After the seat height was set, a 5 min warm-up with a 90 W load was initiated, during which the participant performed two (in the 3rd and 5th minute) maximal accelerations lasting about 5–6 s. After the warm-up there was a 5 min passive recovery break and then the participant performed an all-out test. The all-out test consisted of performing a 30 s sprint with a load equal to 7.5% of body mass. The participant’s task was to reach their maximal pedaling speed in the shortest possible time from a stationary start [24], and then maintain it until the end of the test. During the test, the participant was vigorously verbally encouraged to perform a supramaximal effort. During the test, the participant had to be in a sitting position.
Compared to the original version of the WAnT the only difference here was the method of starting the effort used in the test: in the original version of the WAnT, it was a flying start, while in the version we used it was a stationary start, i.e., the participant waited in a stationary position for the signal to start the test. This simulated the method of starting used in real competitions, which is from a stationary starting position. At the same time, it allowed us to measure additional parameters (e.g., TTR-PP), which are additionally helpful in assessing anaerobic performance [25].
2.6. Participants
The study included 48 healthy young men, aged 19–26, who declared moderate physical activity, performed up to 3 times a week. None of them were professionally involved in sports.
2.7. Statistics
For each variable, the mean and standard deviation were calculated. The Shapiro–Wilk test was used to test the data distribution and Levene’s test was used to assess the homogeneity of variance. An ANOVA with repeated measures or one-way ANOVA was used to detect the differences between groups, differences between the testing points (change in time) and to assess the effect size (ηp2). The ANOVA analyzed the effect of the main factors: group, training (change in time) and the interaction between the two main factors. The effect size (ηp2) was interpreted as small (0.01), medium (0.06) or large (0.14) [21]. If the AVOVA results were significant, the Tukey test was used for post hoc analysis. In addition, if the results of the post hoc analysis were significant, an effect size (ES) was additionally determined between baseline and post training using Cohen’s d. The ES was interpreted as small (0.20), medium (0.50) or large (0.80) [ES] [26]. The STATISTICA 13 package (StatSoft, Inc., Tulsa, OK, USA) was used for statistical analysis. Differences were considered significant when p < 0.05.
The sample size was determined a priori using G*Power version 3.1.9.7 (Dusseldorf, Germany). The following options were selected in the software: test family = f tests; statistical test = ANOVA-repeated measures, within–between interactions; type of power analysis = computed required sample size—given α, power and effect size. Input parameters into the software were as follows: effect size f: 0.25; α error probability: 0.05; power: 0.85; number of groups: 3; number of measurements: 2; correlation among measures: 0.5; nonsphericity correction: 1.0). The required sample size was 16 participants per group (total sample size = 48).
3. Results
The groups did not differ (f = 0.13, p = 0.88, ηp2 = 0.005) in self-declared physical activity, which was 6376.5 ± 1881.3 MET-min/week (IHT), 6154.9 ± 2509.5 MET-min/week (NT) and 6582.7 ± 2831.0 MET-min/week (ctrl).
Participants did not differ significantly (f = 0.16, p = 0.85, ηp2 = 0.01) in weekly caloric intake (IHT: 20,707 ± 3656 kcal/week, NT: 21,233 ± 3352 kcal/week, ctrl: 21,291 ± 2434 kcal/week).
Participants did not differ significantly in body composition (Table 1). Moreover, neither body mass nor body composition changed significantly after the training intervention (Table 1, [27]).

Table 1.
Characteristics of participants (data are presented as mean ± SD) [27].
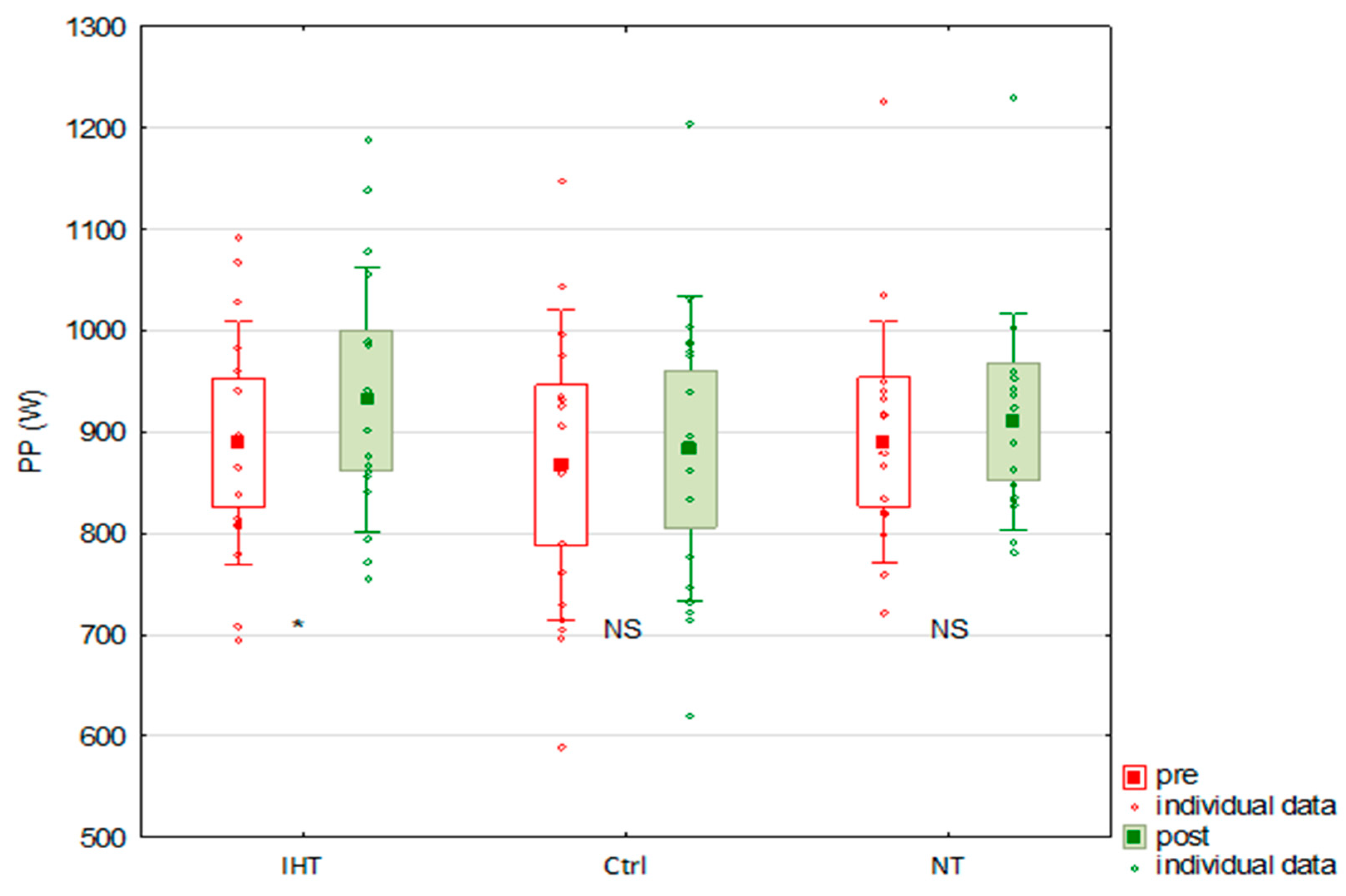
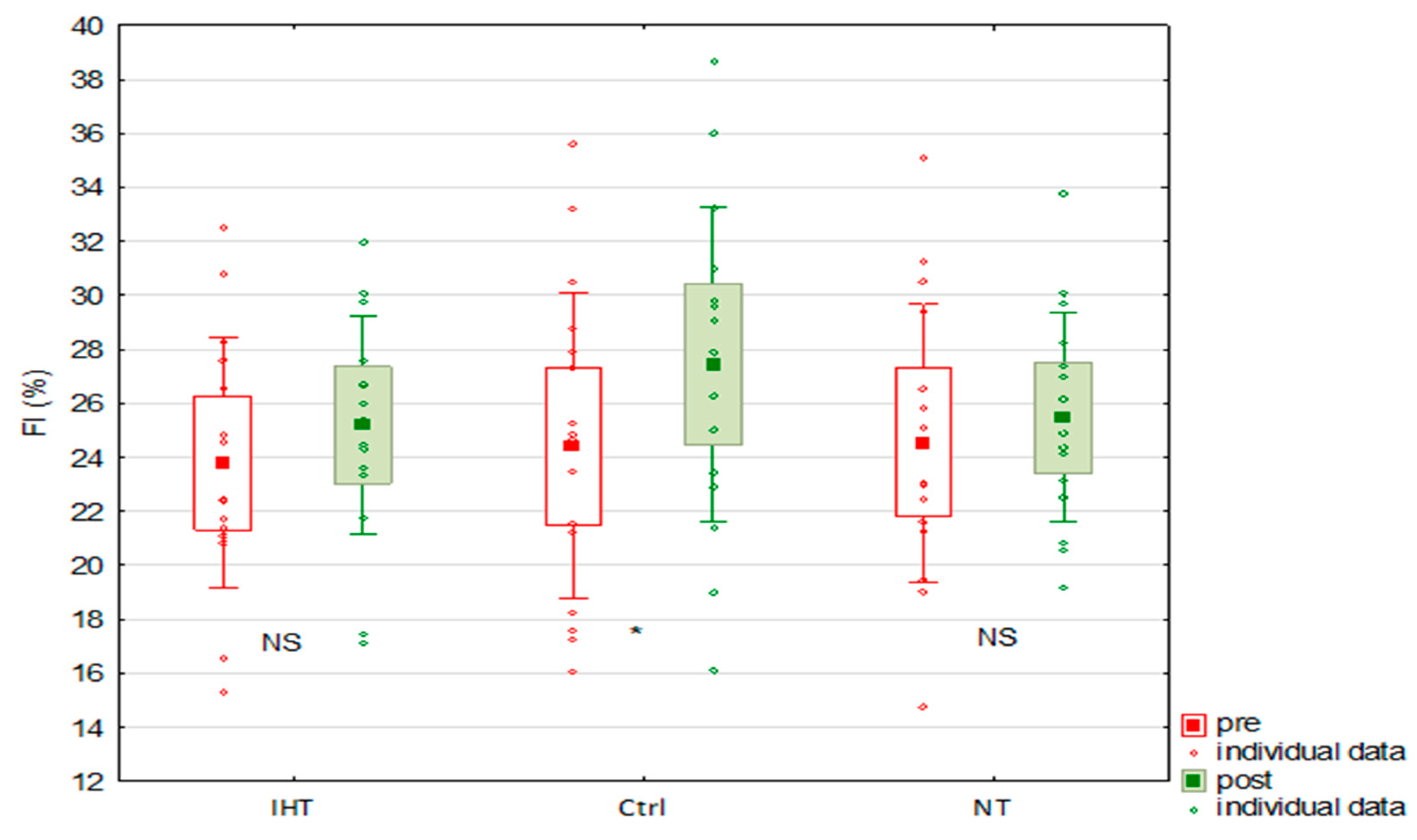
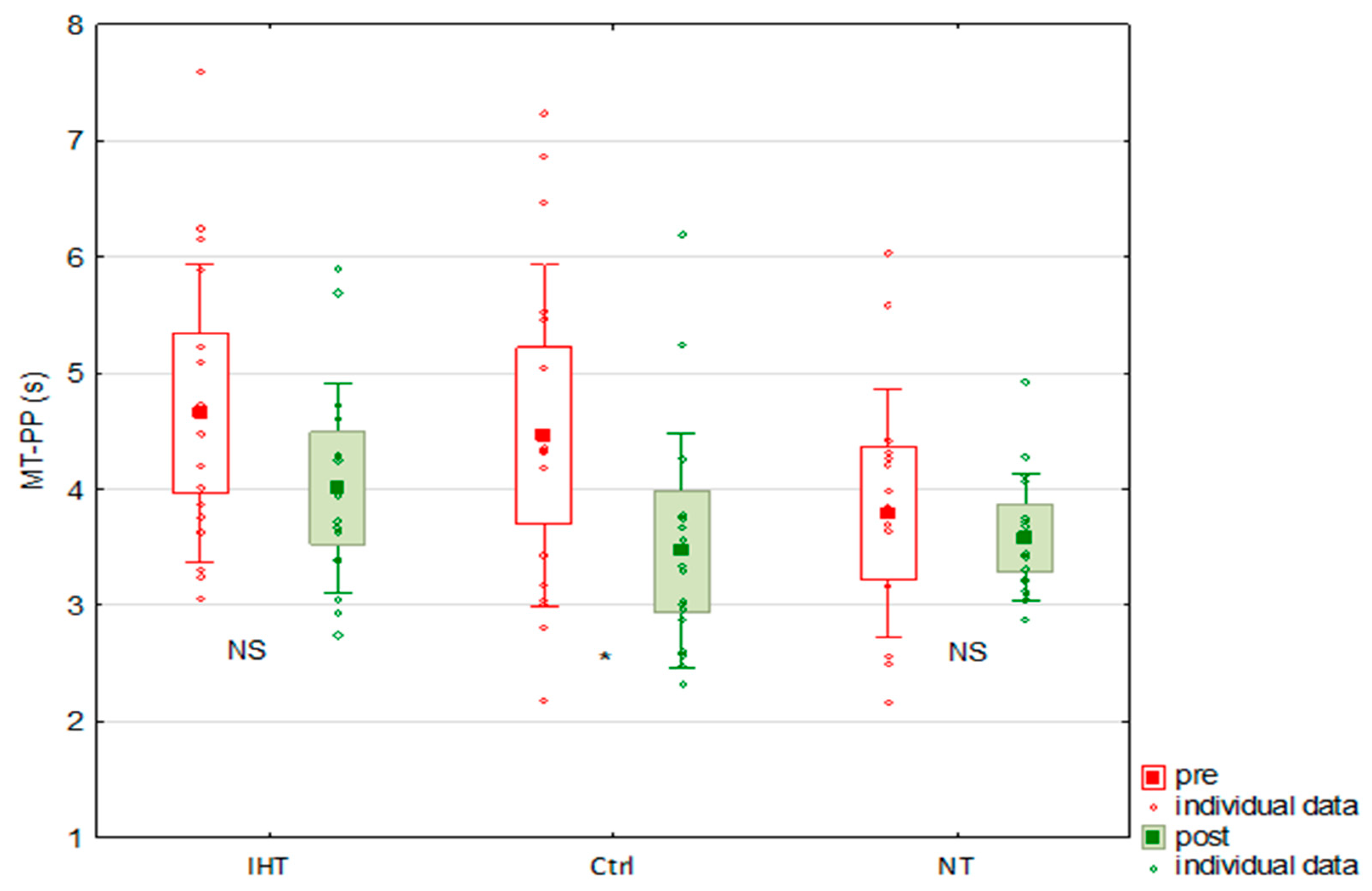
The effects of the IHT were a significant improvement in both absolute peak power (p < 0.001; ES = 0.34) (Figure 2) and relative peak power (p < 0.001; ES = 0.54) in this group. Similar changes were not observed either after training in normoxia (p = 0.14 and p = 0.26, for absolute and relative peak power, respectively) or in the control group (p = 0.34 and p = 0.51, for absolute and relative peak power, respectively). Compared to baseline, there were no significant changes in either group after training in their mean power (absolute and relative), power decrease or total work (Table 2). The time to reach peak power significantly shortened during observation (f = 13.08, p < 0.001), and although post hoc analysis showed no significant change in each group, the IHT group, compared to the other groups, had the greatest reduction in this time (by about 0.5 s on average) after the training. In the control group, the fatigue index increased significantly, and the time to maintain peak power was significantly reduced during observation. Similar changes were not observed in any training group (Figure 3 and Figure 4 and Table 2).
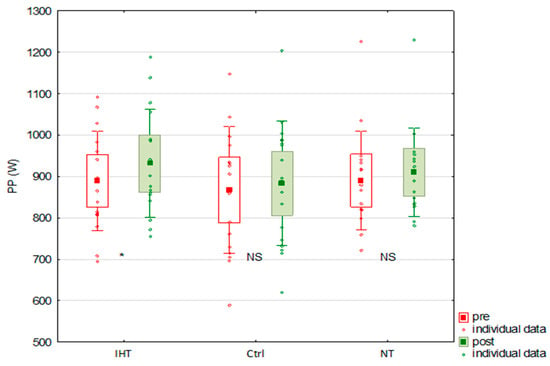
Figure 2.
Changes in absolute peak power (PP) under the influence of training in normoxia (NT) and in hypoxia (IHT), and in control group (ctrl) (*: p < 0.05; NS: non-significant; boxes indicate 0.95 confidence interval; vertical bars indicate standard deviation; squares indicate mean value).
Table 2.
Effects of interval training performed in normoxia and hypoxia on parameters measured in anaerobic all-out sprint test (data are presented as mean ± SD).
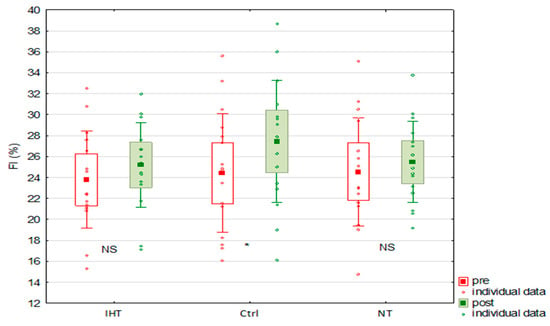
Figure 3.
Changes in fatigue index (FI) under the influence of training in normoxia (NT) and in hypoxia (IHT), and in control group (ctrl) (*: p < 0.05; NS: non-significant; boxes indicate 0.95 confidence interval; vertical bars indicate standard deviation; squares indicate mean value).
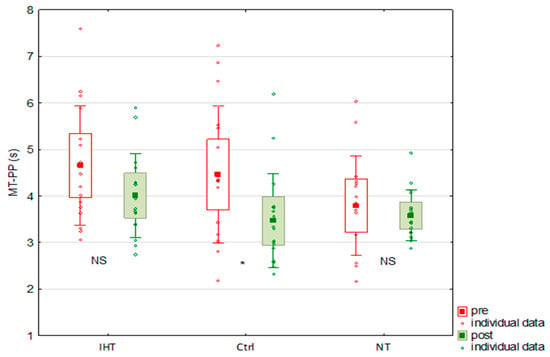
Figure 4.
Changes in peak power maintenance time (MT-PP) under the influence of training in normoxia (NT) and in hypoxia (IHT), and in control group (ctrl) (*: p < 0.05; NS: non-significant; boxes indicate 0.95 confidence interval; vertical bars indicate standard deviation; squares indicate mean value).
4. Discussion
The purpose of this study was to evaluate the effects of IHT on anaerobic performance in young men. Our study showed that after interval training in hypoxia (12 workouts for 4 weeks; 12 h of training in hypoxia) only peak power (absolute and relative) was significantly improved in the IHT group. In the control and normoxia training groups a similar effect was not observed. The increase in peak power indicates an improvement in the alactic (phosphagen) energy system’s efficiency. On the other hand, after training, no significant changes in parameters informing the efficiency of the lactic (glycolytic) energy system, i.e., mean power, fatigue index or power decrease, were observed in any of the training groups (IHT, NT). The applied intervention also did not significantly affect the participants’ speed (dynamics)—peak power was noted in all groups at a similar time from the start of test, both before and after training. However, there was a noticeable tendency for the time to reach peak power to shorten with training. Our results suggest that IHT may have had a significant beneficial effect only on peak power. To our knowledge, this is one of the few studies to comprehensively evaluate the effects of IHT on anaerobic performance in young, untrained men. Previous studies [8,9,10] were performed with athletes, which could have significantly influenced the results, due to the high volume training and good physical capacity of the participants.
In repeated WAnTs, the practice effect is observed [28]. For this reason, at least one familiarization session with the test is recommended, which, in these studies, was performed a few days before the start of the pivotal test. During a WAnT the fractions of the energy from alactic, lactic and aerobic metabolism, are 31.1%, 50.3% and 18.6%, respectively [29]. This suggests that the improvement in anaerobic performance in a WAnT under hypoxic training may be due to improvements in anaerobic, as well as in aerobic, metabolism.
In this study, we focused on evaluating the effects of IHT on anaerobic performance, and we did not investigate the mechanisms underlying the observed effects. Changes in anaerobic performance under hypoxia are primarily attributed to the non-hematological effects of hypoxic training. It is indicated that as an effect of IHT, greater muscle adaptation occurs than during exercise in normoxia [3]. The lower oxygen partial pressure in muscle tissue during IHT may lead to a larger upregulation of hypoxia-inducible factor 1α (HIF-1α) [5]. An increased citrate synthase activity, mitochondrial density, fiber cross-sectional area and capillary-to-fiber ratio were noted after IHT. Moreover, the upregulation of factors of mitochondrial biogenesis or enzymes implicated in carbohydrate and mitochondrial metabolism, oxidative stress defense and pH regulation were observed in the participants [3,5,30,31,32].
Potentially favorable adaptations to anaerobic exercises after IHT were also reported, e.g., improved tissue perfusion, mitochondrial efficiency, better control of muscle O2 homeostasis and mitochondrial respiration [31,33], angiogenesis [34] and improved muscle buffering capacity [7]. Unfortunately, the translation of these adaptations into enhanced performance is not always observed, and may be irrelevant for sports [3]. In hypoxia training studies, a decrease in Na+-K+ -ATPase pump activity has been observed [35], and training in hypoxia might be detrimental to muscle contractility [36]. The inclusion of hypoxia in training can also affect PCr re-synthesis [3]. After training in hypoxia a quicker recovery of phosphocreatine was observed [37,38]. Hypoxia also induces vasodilation [39] to maintain normal pO2, especially in fast-twitch fibers [40]. An elevated microvascular pO2 reduces PCr breakdown and speeds up PCr recovery kinetics [41], which can affect the power generated [3].
Our study does not confirm the results presented by Hamlin et al. [6], who indicated a 3% increase in mean power in the Wingate Anaerobic Test, linking this to enhanced glycolysis. Our results are similar to results reported by Millet et al. [1], who showed no effect of IHT on mean power in the anaerobic test. At the same time, Millet et al. [1] also showed no change in peak power after hypoxic training, which is not confirmed by our study, as we observed an increase in PP. Millet et al. [1] found that not only was the hypoxic stimulus ineffective on anaerobic performance, but it was also ineffective for monocarboxylate transporters’ (MCT) expression after hypoxic training. An increase in these proteins’ expression is likely to decrease intracellular pH perturbation [42].
The effects of training depend on both the hypoxic training model used and the form of physical training [3]. The participants in our study performed interval training lasting 60 min. The training was not strictly anaerobic in nature, but rather was a form of submaximal training (6 min of submaximal exercise/3 min of active rest). The workout was designed so that the athletes could perform it for 60 min under normobaric hypoxia (at 3000 m asl). A shorter workout could have been completely ineffective due to too short a hypoxic stimulation. However, the training intensity, matched to VT2, was intended to improve lactate tolerance and lactate clearance—the intensity at VT2 is the highest work intensity at which the balance between lactate clearance and lactate production still exists [22]. With increasing exercise intensity glycolytic muscle fibers are preferentially recruited, while at intensities below VT2 oxidative slow-twitch and fast-twitch muscle fibers are engaged. High-intensity training under hypoxic conditions stimulates glucose-dependent metabolic pathways to a greater extent than low-intensity training. Very high intensity training increases the activity of phosphofructokinase and other glycolytic enzymes more than lower intensity training [5]. Currently, research is also being undertaken to evaluate the effectiveness of typically anaerobic training performed under hypoxia; this method is referred to as repeated sprint training in hypoxia (RSH) [43].
The Limitation of the Study
In this study, we focused on the effects of IHT on anaerobic capacity. We did not investigate the potential non-hematological and hematological mechanisms that may underlie the reported changes. Our results only apply to untrained men and should be confirmed in athletes.
5. Conclusions
Intermittent hypoxic interval training in young, untrained men can be effective in improving their peak power, but does not significantly affect their mean power.
Author Contributions
Methodology, M.M., T.P. and M.W.; conceptualization, M.M. and T.P.; formal analysis, M.M.; validation, M.M. and T.P.; investigation, M.M., T.P., S.M. and Z.S.; data curation, M.M.; resources, M.M. and T.P.; writing—original draft preparation, M.M.; writing—review and editing, T.P. and M.W.; visualization, M.M.; supervision, M.M. and T.P.; funding acquisition, M.M. and T.P.; project administration, M.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research and APC was funded by the Ministry of Education and Science (Poland), grant number MEIN 2021/DPI/229.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki, and approved by the Bioethical Commission of the Regional Medical Chamber in Krakow, Poland (opinion no. 47/KB/OIL/2022; date 11 April 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets analyzed during the study are available from the corresponding author (M.M.) upon reasonable request. The data are not publicly available due to privacy.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Millet, G.; Bentley, D.J.; Roels, B.; Mc Naughton, L.R.; Mercier, J.; Cameron-Smith, D. Effects of intermittent training on anaerobic performance and MCT transporters in athletes. PLoS ONE 2014, 9, e95092. [Google Scholar] [CrossRef] [PubMed]
- Saunders, P.U.; Garvican-Lewis, L.A.; Chapman, R.F.; Périard, J.D. Special environments: Altitude and heat. Int. J. Sport Nutr. Exerc. Metab. 2019, 29, 210–219. [Google Scholar] [CrossRef] [PubMed]
- Faiss, R.; Girard, O.; Millet, G.P. Advancing hypoxic training in team sports: From intermittent hypoxic training to repeated sprint training in hypoxia. Br. J. Sports Med. 2013, 47 (Suppl. S1), i45–i50. [Google Scholar] [CrossRef] [PubMed]
- Wilber, R.L. Application of altitude/hypoxic training by elite athletes. Med. Sci. Sports Exerc. 2007, 39, 1610–1624. [Google Scholar] [CrossRef] [PubMed]
- Vogt, M.; Puntschart, A.; Geiser, J.; Zuleger, C.; Billeter, R.; Hoppeler, H. Molecular adaptations in human skeletal muscle to endurance training under simulated hypoxic conditions. J. Appl. Physiol. 2001, 91, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Hamlin, M.J.; Marshall, H.C.; Hellemans, J.; Ainslie, P.N.; Anglem, N. Effect of intermittent hypoxic training on 20 km time trial and 30 s anaerobic performance. Scand. J. Med. Sci. Sports 2010, 20, 651–661. [Google Scholar] [CrossRef]
- Gore, C.J.; Hahn, A.G.; Aughey, R.J.; Martin, D.T.; Ashenden, M.J.; Clark, S.A.; Garnham, A.P.; Roberts, A.D.; Slater, G.J.; McKenna, M.J. Live high: Train low increases muscle buffer capacity and submaximal cycling efficiency. Acta Phys. Scand. 2001, 173, 275–286. [Google Scholar] [CrossRef]
- Ambroży, T.; Maciejczyk, M.; Klimek, A.T.; Wiecha, S.; Stanula, A.; Snopkowski, P.; Palka, T.; Jaworski, J.; Ambrozy, D.; Rydzik, L.; et al. The effects of intermittent hypoxic training on anaerobic and aerobic power in boxers. Int. J. Environ. Res. Public Health 2020, 17, 9361. [Google Scholar] [CrossRef]
- Czuba, M.; Wilk, R.; Karpiński, J.; Chalimoniuk, M.; Zajac, A.; Langfort, J. Intermittent hypoxic training improves anaerobic performance in competitive swimmers when implemented into a direct competition mesocycle. PLoS ONE 2017, 12, e0180380. [Google Scholar] [CrossRef]
- Morton, J.P.; Cable, N.T. The effects of intermittent hypoxic training on aerobic and anaerobic performance. Ergonomics 2005, 48, 1535–1546. [Google Scholar] [CrossRef]
- Girard, O.; Brocherie, F.; Goods, P.S.; Millet, G.P. An updated panorama of “living low-training high” altitude/hypoxic methods. Front. Sports Act. Living 2020, 2, 26. [Google Scholar] [CrossRef] [PubMed]
- McLean, B.D.; Gore, C.J.; Kemp, J. Application of ‘live low-train high’for enhancing normoxic exercise performance in team sport athletes. Sports Med. 2014, 44, 1275–1287. [Google Scholar] [CrossRef] [PubMed]
- Dolci, F.; Hart, N.H.; Kilding, A.E.; Chivers, P.; Piggott, B.; Spiteri, T. Physical and energetic demand of soccer: A brief review. Strength Cond. J. 2020, 42, 70–77. [Google Scholar] [CrossRef]
- Franchini, E. Energy system contributions during Olympic combat sports: A narrative review. Metabolites 2023, 13, 297. [Google Scholar] [CrossRef] [PubMed]
- Bertuzzi, R.C.D.M.; Franchini, E.; Kokubun, E.; Kiss, M.A.P.D.M. Energy system contributions in indoor rock climbing. Eur. J. Appl. Physiol. 2007, 101, 293–300. [Google Scholar] [CrossRef]
- Hargreaves, M.; Spriet, L.L. 2020 Skeletal muscle energy metabolism during exercise. Nat. Metab. 2009, 2, 817–828. [Google Scholar] [CrossRef]
- Maciejczyk, M.; Szymura, J.; Wiecek, M.; Szygula, Z.; Kepinska, M.; Ochalek, K.; Pokrywka, A. Effects of eccentric exercise on anaerobic power, starting speed and anaerobic endurance. Kinesiology 2015, 47, 44–50. [Google Scholar]
- Available online: https://sites.google.com/view/ipaq/home (accessed on 18 February 2022).
- Biernat, E.; Stupnicki, R.; Lebiedziński, B.; Janczewska, L. Assessment of physical activity by applying IPAQ questionnaire. Phys. Educ. Sport 2008, 52, 83–89. [Google Scholar] [CrossRef]
- Mistura, L.; Comendador Azcarraga, F.J.; D’Addezio, L.; Martone, D.; Turrini, A. An Italian case study for assessing nutrient intake through nutrition-related mobile apps. Nutrients 2021, 13, 3073. [Google Scholar] [CrossRef]
- Bhambhani, Y.; Singh, M. Ventilatory thresholds during a graded exercise test. Respiration 1985, 47, 120–128. [Google Scholar] [CrossRef]
- Binder, R.K.; Wonisch, M.; Corra, U.; Cohen-Solal, A.; Vanhees, L.; Saner, H.; Schmid, J. Methodological approach to the first and second lactate threshold in incremental cardiopulmonary exercise testing. Eur. J. Cardiovasc. Prev. Rehabil. 2008, 15, 726–734. [Google Scholar] [CrossRef] [PubMed]
- Inbar, O.; Bar-Or, O.; Skinner, J.S. The Wingate Anaerobic Test; Human Kinetics: Champaign, IL, USA, 1996. [Google Scholar]
- Coleman, S.; Hale, T.; Hamley, E. A comparison of power outputs with rolling and stationary starts in the Wingate anaerobic test. J. Sports Sci. 1985, 3, 207–208. [Google Scholar]
- Hofman, N.; Orie, J.; Hoozemans, M.J.M.; Foster, C.; deKoning, J.J. Wingate test is a strong predictor of 1500m performance in elite speed skaters. Int. J. Sports Physiol. Perform. 2017, 12, 1288–1292. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge Academic: New York, NY, USA, 1988. [Google Scholar]
- Maciejczyk, M.; Palka, T.; Wiecek, M.; Szymura, J.; Kusmierczyk, J.; Bawelski, M.; Masel, S.; Szygula, Z. Effects of intermittent hypoxic training on aerobic capacity and second ventilatory threshold in untrained men. Appl. Sci. 2023, 13, 9954. [Google Scholar] [CrossRef]
- Barfield, J.P.; Sells, P.D.; Rowe, D.A.; Hannigan-Downs, K. Practice effect of the Wingate anaerobic test. J. Strength Cond. Res. 2002, 16, 472–473. [Google Scholar] [PubMed]
- Beneke, R.; Pollmann, C.H.; Bleif, I.; Leithäuser, R.; Hütler, M. How anaerobic is the Wingate Anaerobic Test for humans? Eur. J. Appl. Physiol. 2002, 87, 388–392. [Google Scholar] [PubMed]
- Hoppeler, H.; Vogt, M. Muscle tissue adaptations to hypoxia. J. Exp. Biol. 2001, 204 Pt 18, 3133–3139. [Google Scholar] [CrossRef] [PubMed]
- Desplanches, D.; Hoppeler, H.; Linossier, M.T.; Denis, C.; Claassen, H.; Dormois, D.; Lacour, J.R.; Geyssant, A. Effects of training in normoxia and normobaric hypoxia on human muscle ultrastructure. Pflugers Arch. 1993, 425, 263–267. [Google Scholar] [CrossRef]
- Terrados, N.; Melichna, J.; Sylvén, C.; Jansson, E.; Kaijser, L. Effects of training at simulated altitude on performance and muscle metabolic capacity in competitive road cyclists. Eur. J. Appl. Physiol. Occup. Physiol. 1988, 57, 203–209. [Google Scholar] [CrossRef]
- Roels, B.; Thomas, C.; Bentley, D.J.; Mercier, J.; Hayot, M.; Millet, G. Effects of intermittent hypoxic training on amino and fatty acid oxidative combustion in human permeabilized muscle fibers. J. Appl. Physiol. 2007, 102, 79–86. [Google Scholar] [CrossRef]
- Toffoli, S.; Roegiers, A.; Feron, O.; Van Steenbrugge, M.; Ninane, N.; Raes, M.; Michiels, C. Intermittent hypoxia is an angiogenic inducer for endothelial cells: Role of HIF-1. Angiogenesis 2009, 12, 47–67. [Google Scholar] [CrossRef] [PubMed]
- Sandiford, S.D.; Green, H.J.; Duhamel, T.A.; Perco, J.G.; Schertzer, J.D.; Ouyang, J. Inactivation of human muscle Na+-K+-ATPase in vitro during prolonged exercise is increased with hypoxia. J. Appl. Physiol. 2004, 96, 1767–1775. [Google Scholar] [CrossRef] [PubMed]
- Vogt, M.; Hoppeler, H. Is hypoxia training good for muscles and exercise performance? Prog. Cardiovasc. Dis. 2010, 52, 525–533. [Google Scholar] [CrossRef]
- Kuno, S.Y.; Inaki, M.; Tanaka, K.; Itai, Y.; Asano, K. Muscle energetics in short-term training during hypoxia in elite combination skiers. Eur. J. Appl. Physiol. Occup. Physiol. 1994, 69, 301–304. [Google Scholar] [CrossRef] [PubMed]
- Holliss, B.A.; Fulford, J.; Vanhatalo, A.; Pedlar, C.R.; Jones, A.M. Influence of intermittent hypoxic training on muscle energetics and exercise tolerance. J. Appl. Physiol. 2013, 114, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Casey, D.P.; Joyner, M.J. Compensatory vasodilatation during hypoxic exercise: Mechanisms responsible for matching oxygen supply to demand. J. Physiol. 2012, 590, 6321–6326. [Google Scholar] [CrossRef]
- Cleland, S.M.; Murias, J.M.; Kowalchuk, J.M.; Paterson, D.H. Effects of prior heavy-intensity exercise on oxygen uptake and muscle deoxygenation kinetics of a subsequent heavy-intensity cycling and knee-extension exercise. Appl. Physiol. Nutr. Metab. 2012, 37, 138–148. [Google Scholar] [CrossRef]
- Haseler, L.J.; Hogan, M.C.; Richardson, R.S. Skeletal muscle phosphocreatine recovery in exercise-trained humans is dependent on O2 availability. J. Appl. Physiol. 1999, 86, 2013–2018. [Google Scholar] [CrossRef]
- Juel, C.; Halestrap, A.P. Lactate transport in skeletal muscle—Role and regulation of the monocarboxylate transporter. J. Physiol. 1999, 517 Pt 3, 633–642. [Google Scholar] [CrossRef]
- Millet, G.P.; Girard, O.; Beard, A.; Brocherie, F. Repeated sprint training in hypoxia–an innovative method. Dtsch. Z. Sportmed. 2019, 5, 115–122. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).