
Evaluation of Tooth Movement Accuracy with the F22 Aligner System: A Retrospective Study
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
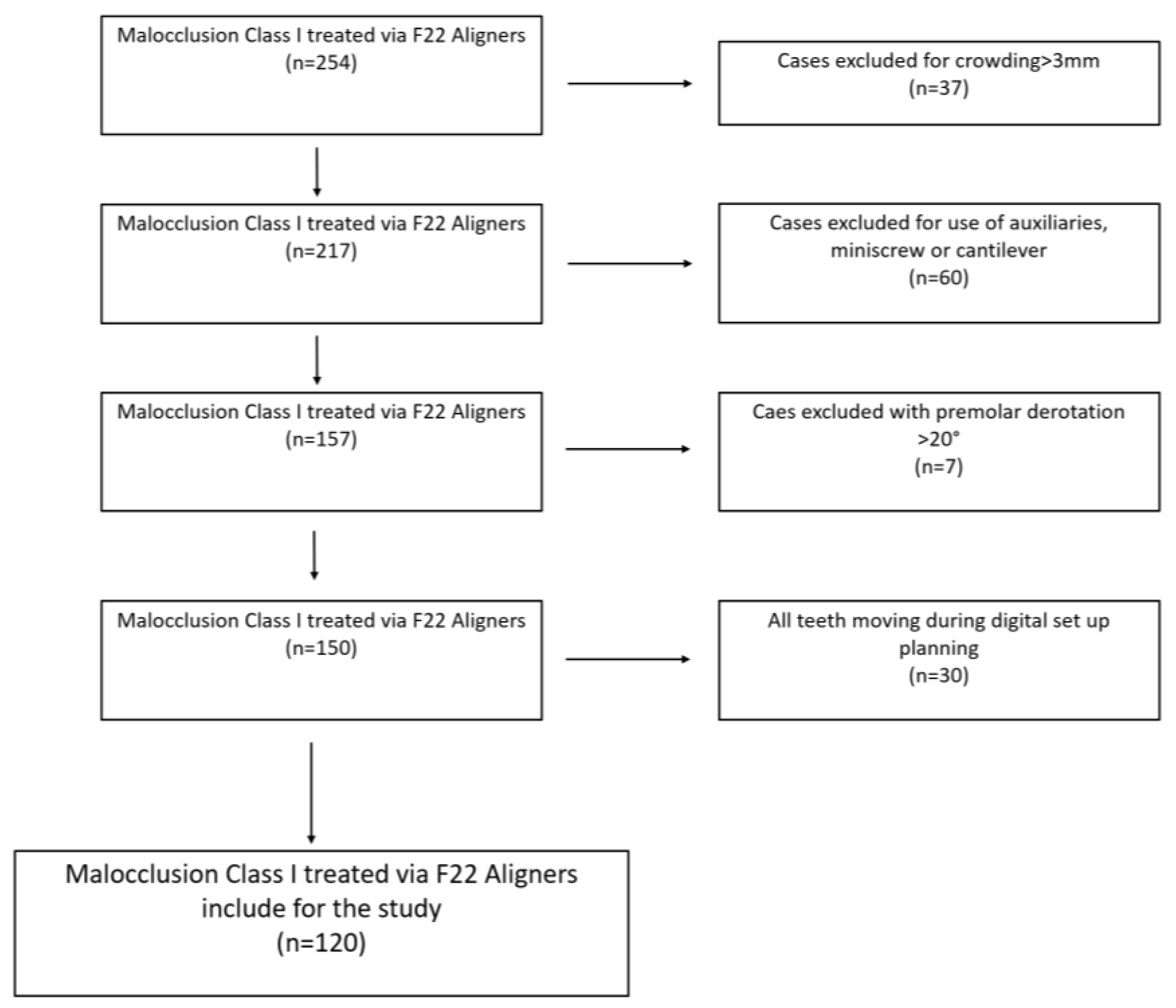
2.1. Sample Selection
- Class I dental malocclusion with minimal crowding (≤3 mm) in both arches [32], treated with a series of 12–20 aligners per arch.
- No use of auxiliaries (derotation elastomeric chains, inter-arch elastics or extrusion elastics), miniscrews, cantilevers or vestibular or lingual fixed partial appliances.
- Grip points and IPR (interproximal reduction) were permitted.
- Planned derotation of rounded teeth ≤ 20° (premolars and canines) is included.
- The use of grip points positioned for derotation ≥ 10° of rounded teeth and >20° for mandibular incisors and maxillary lateral incisors, which have a mesiodistally narrow clinical crown. The triangular grip points were applied with the long side in the direction of force application.
- No previous or active periodontal disease at the beginning of orthodontic therapy.
- Presence of at least one posterior tooth (first or second molar) per quadrant that had not been planned to move.
- F22 Aligners were worn for 2 weeks prior to passing to the following step.
- F22 Aligner therapy completed with adequate patient compliance (20–22 h per day), as documented in a personal diary.
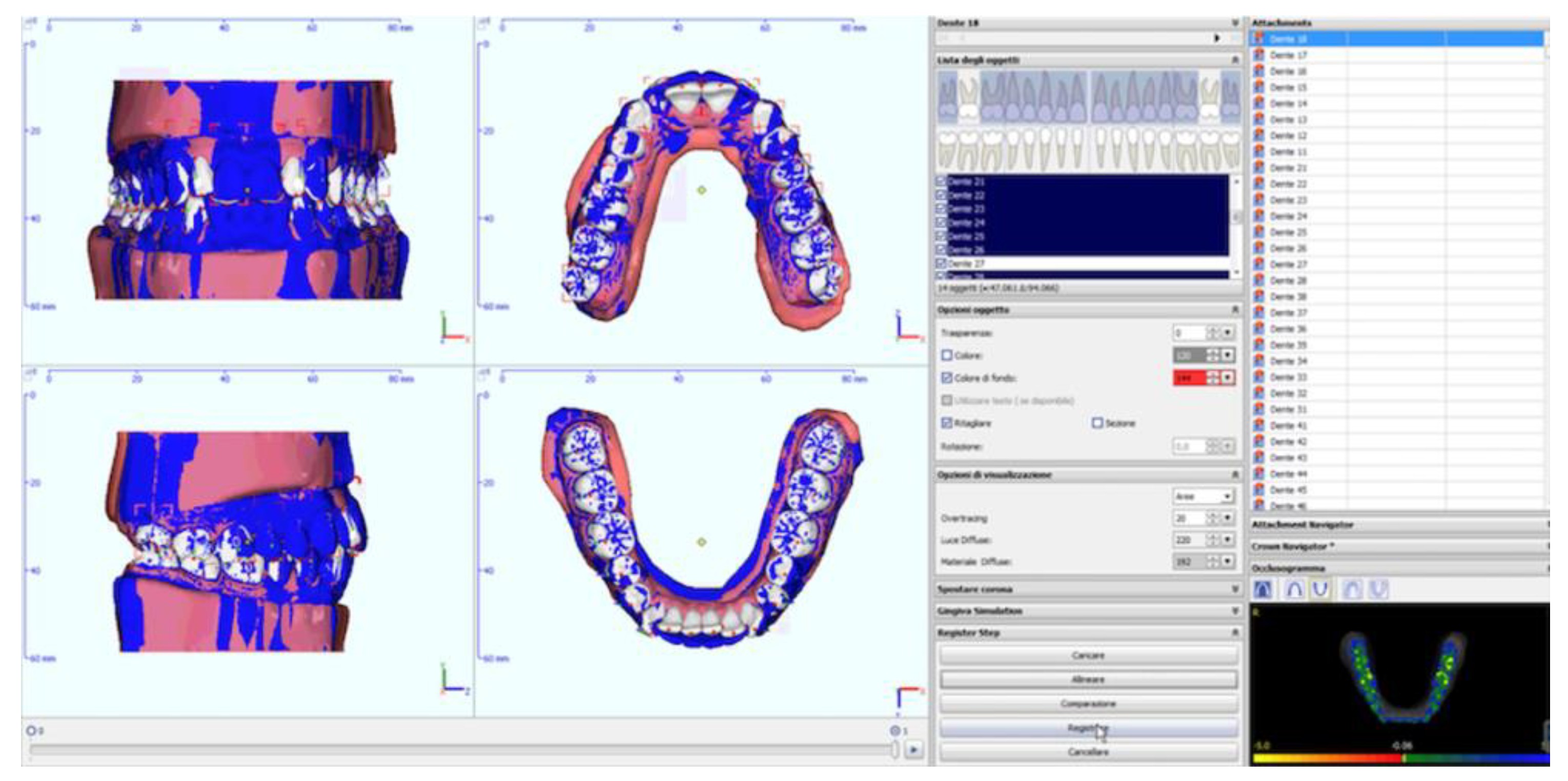
2.2. Analysis of Digital Models
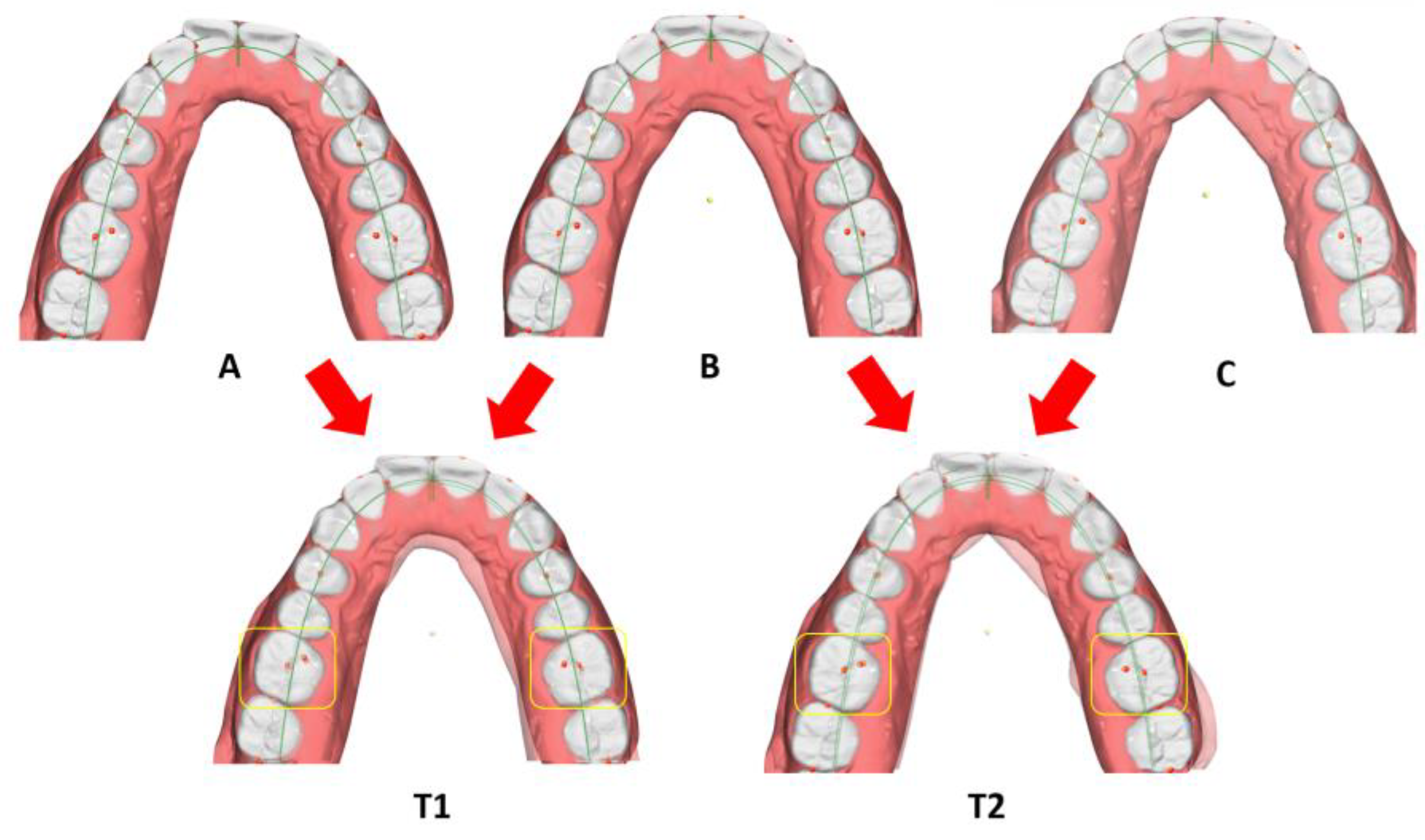
- Prescribed movements (T1): the difference between the pre-treatment and reference model;
- Achieved movements (T2): the difference between the pre-treatment and pre-finishing model (Figure 3) for each movement investigated (inclination, angulation and rotation) and for each tooth (where present, third molars were excluded).
- Inter-canine distance (Ic): measured between the tips of the canine cusps;
- Inter-premolar distance (Ip1): measured between the vestibular cusps on the first premolars;
- Inter-premolar distance (Ip2): measured between the vestibular cusps on the second premolars;
- Inter-molar distance (Im): measured between the mesiovestibular cusps on the first molars (Figure 4).
2.3. Analysis of Measurements
- Imprecision = the difference between the prescribed movement (T1) and that clinically achieved (T2), expressed as absolute values.
- Accuracy = the difference between the movement achieved (T2) and that prescribed (T1), expressed as absolute values and percentages (%).
- Imprecision = the difference between the prescribed movement (T1) and that clinically achieved (T2).
2.4. Statistical Analysis
3. Results
4. Discussion
Limitations of the Study
5. Conclusions
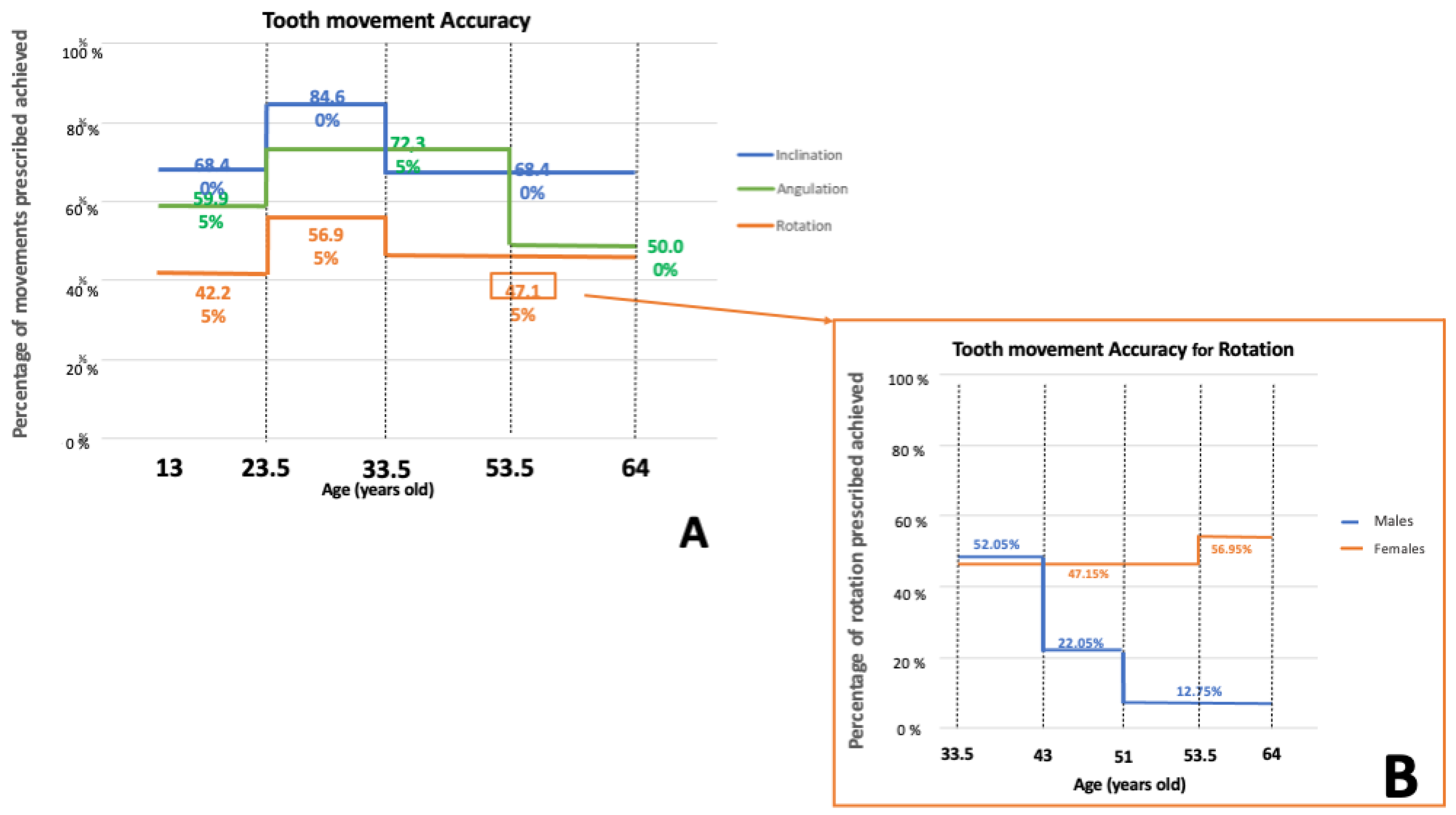
- In mild-to-moderate cases of Class I malocclusion, the F22 Aligner system displays excellent accuracy for inclination (86.76% ± 44.89%) and angulation movements (88.01% ± 55.68%), but only moderate for rotation (61.59% ± 32.54%).
- It is least accurate at the derotation of rounded teeth, in particular maxillary (49.59% ± 29.43%) and mandibular canines (57.70% ± 28.90%) and mandibular premolars (54.19% ± 35.79%). The derotation of maxillary premolars is more accurate (62.86% ± 35.03%), presumably due to their squarer crowns, and they were positively affected by the application of grip points.
- The percentage of prescribed angulation achieved depends on the amount of prescribed movement, the direction of movement (difference between distal and mesial tipping) and the tooth type (greater for maxillary premolars and canines, and mandibular incisors). Moreover, the presence or absence of grip points in mesial crown tipping presents a paradoxical effect.
- The percentage of rotation achieved depends on the tooth type, and is lowest for the rounded teeth, which is not improved by the application of grip points, with the exception of the maxillary premolars. For the remaining tooth types investigated, the accuracy is greater, and improves with the use of grip points.
- For all the movements investigated, the variables sex and age influence the percentage of movement achieved, which is greater in the intermediate age group (young adult patients). As for rotation, in the older group the trend seen in females (inverse relationship between accuracy and age) was reversed in males (direct relationship between accuracy and age).
- The F22 Aligner system seems to have a good expansive capacity, with differences between prescription and result always less than 1 mm. The only region where there is a significant difference between prescribed and achieved expansion was the distance between the mandibular first premolars, although the discrepancy was clinically minimal (0.24 mm).
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gierie, W.V. Clear aligner therapy: An overview. J. Clin. Orthod. 2018, 52, 665–674. [Google Scholar] [PubMed]
- Jeremiah, H.G.; Bister, D.; Newton, J.T. Social perceptions of adults wearing orthodontic appliances: A cross-sectional study. Eur. J. Orthod. 2011, 33, 476–482. [Google Scholar] [CrossRef] [PubMed]
- Rossini, G.; Parrini, S.; Castroflorio, T.; Deregibus, A.; Debernardi, C.L. Periodontal health during clear aligners treatment: A systematic review. Eur. J. Orthod. 2015, 37, 539–543. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.B.; McGorray, S.P.; Womack, R.; Quintero, J.C.; Perelmuter, M.; Gibson, J.; Dolan, T.A.; Wheeler, T.T. A comparison of treatment impacts between Invisalign aligner and fixed appliance therapy during the first week of treatment. Am. J. Orthod. Dentofac. Orthop. 2007, 131, 302.e1–302.e9. [Google Scholar] [CrossRef] [PubMed]
- Henick, D.; Dayan, W.; Dunford, R.; Warunek, S.; Al-Jewair, T. Effects of Invisalign (G5) with virtual bite ramps for skeletal deep overbite malocclusion correction in adults. Angle Orthod. 2021, 91, 164–170. [Google Scholar] [CrossRef]
- Vidal Bernárdez, M.L.; Vilches Arenas, Á.; Sonnemberg, B.; Solano Reina, E.; Solano Mendoza, B. EX30 vs. SmartTrack materials in maxillary expansion with the Invisalign system. J. Clin. Orthod. 2022, 56, 343–350. [Google Scholar]
- Kravitz, N.D.; Kusnoto, B.; BeGole, E.; Obrez, A.; Agran, B. How well does Invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with Invisalign. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 27–35. [Google Scholar] [CrossRef]
- Haouili, N.; Kravitz, N.D.; Vaid, N.R.; Ferguson, D.J.; Makki, L. Has Invisalign improved? A prospective follow-up study on the efficacy of tooth movement with Invisalign. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M.; Liu, R.; Ni, Z.; Yu, Z. Efficiency, effectiveness and treatment stability of clear aligners: A systematic review and meta-analysis. Orthod. Craniofac. Res. 2017, 20, 127–133. [Google Scholar] [CrossRef]
- Rossini, G.; Parrini, S.; Castroflorio, T.; Deregibus, A.; Debernardi, C.L. Efficacy of clear aligners in controlling orthodontic tooth movement: A systematic review. Angle Orthod. 2015, 85, 881–889. [Google Scholar] [CrossRef]
- Dai, F.F.; Xu, T.M.; Shu, G. Comparison of achieved and predicted crown movement in adults after 4 first premolar extraction treatment with Invisalign. Am. J. Orthod. Dentofac. Orthop. 2021, 160, 805–813. [Google Scholar] [CrossRef]
- Jiang, T.; Jiang, Y.N.; Chu, F.T.; Lu, P.J.; Tang, G.H. A cone-beam computed tomographic study evaluating the efficacy of incisor movement with clear aligners: Assessment of incisor pure tipping, controlled tipping, translation, and torque. Am. J. Orthod. Dentofac. Orthop. 2021, 159, 635–643. [Google Scholar] [CrossRef]
- Khosravi, R.; Cohanim, B.; Hujoel, P.; Daher, S.; Neal, M.; Liu, W.; Huag, G. Management of overbite with the Invisalign appliance. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 691.e2–699.e2. [Google Scholar] [CrossRef]
- Simon, M.; Keilig, L.; Schwarze, J.; Jung, B.A.; Bourauel, C. Treatment outcome and efficacy of an aligner technique—Regarding incisor torque, premolar derotation and molar distalization. BMC Oral Health 2014, 14, 68. [Google Scholar] [CrossRef]
- Zhang, X.J.; He, L.; Guo, H.M.; Tian, J.; Bai, Y.X.; Li, S. Integrated three-dimensional digital assessment of accuracy of anterior tooth movement using clear aligners. Korean J. Orthod. 2015, 45, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Papageorgiou, S.N.; Koletsi, D.; Iliadi, A.; Peltomaki, T.; Eliades, T. Treatment outcome with orthodontic aligners and fixed appliances: A systematic review with meta-analyses. Eur. J. Orthod. 2020, 42, 331–343. [Google Scholar] [CrossRef] [PubMed]
- Yassir, Y.A.; Nabbat, S.A.; McIntyre, G.T.; Bearn, D.R. Clinical effectiveness of clear aligner treatment compared to fixed appliance treatment: An overview of systematic reviews. Clin. Oral Investig. 2022, 26, 2353–2370. [Google Scholar] [CrossRef] [PubMed]
- Palone, M.; Baciliero, M.; Cervinara, F.; Maino, G.B.; Paoletto, E.; Cremonini, F.; Lombardo, L. Class II treatment of transverse maxillary deficiency with a single bone-borne appliance and hybrid clear aligner approach in an adult patient: A case report. J. World Fed. Orthod. 2022, 11, 80–94. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, L.; Palone, M.; Carlucci, A.; Siciliani, G. Clear aligner hybrid approach: A case report. J. World Fed. Orthod. 2020, 9, 32–43. [Google Scholar] [CrossRef] [PubMed]
- Houle, J.P.; Piedade, L.; Todescan, R.J.; Pinheiro, F.H. The predictability of transverse changes with Invisalign. Angle Orthod. 2017, 87, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Bilello, G.; Fazio, M.; Amato, E.; Crivello, L.; Galvano, A.; Currò, G. Accuracy evaluation of orthodontic movements with aligners: A prospective observational study. Prog. Orthod. 2022, 23, 12. [Google Scholar] [CrossRef]
- Buschang, P.H.; Ross, M.; Shaw, S.G.; Crosby, D.; Campbell, P.M. Predicted and actual end-of-treatment occlusion produced with aligner therapy. Angle Orthod. 2015, 85, 723–727. [Google Scholar] [CrossRef]
- Charalampakis, O.; Iliadi, A.; Ueno, H.; Oliver, D.R.; Kim, K.B. Accuracy of clear aligners: A retrospective study of patients who needed refinement. Am. J. Orthod. Dentofac. Orthop. 2018, 154, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, L.; Palone, M.; Longo, M.; Arveda, N.; Nacucchi, M.; De Pascalis, F.; Spedicato, G.A.; Siciliani, G. MicroCT X-ray comparison of aligner gap and thickness of six brands of aligners: An in-vitro study. Prog. Orthod. 2020, 21, 12. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, E.; Castroflorio, E.; Rossini, G.; Garino, F.; Cugliari, G.; Deregibus, A.; Castroflorio, T. Scanning electron microscopy evaluation of aligner fit on teeth. Angle Orthod. 2018, 88, 596–601. [Google Scholar] [CrossRef] [PubMed]
- Palone, M.; Longo, M.; Arveda, N.; Nacucchi, M.; Pascalis, F.; Spedicato, G.A.; Siciliani, G.; Lombardo, L. Micro-computed tomography evaluation of general trends in aligner thickness and gap width after thermoforming procedures involving six commercial clear aligners: An in vitro study. Korean J. Orthod. 2021, 51, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Cremonini, F.; Zabini, F.; Oliverio, T.; Bianchi, A.; Scalia, S.; Siciliani, G.; Lombardo, L. Optical properties of seven types of clear aligners before and after in vitro aging. J. Clin. Orthod. 2022, 56, 149–157. [Google Scholar]
- Lombardo, L.; Arreghini, A.; Maccarrone, R.; Bianchi, A.; Scalia, S.; Siciliani, G. Optical properties of orthodontic alignersߞSpectrophotometry analysis of three types before and after aging. Prog. Orthod. 2015, 16, 41. [Google Scholar] [CrossRef] [PubMed]
- Albertini, P.; Mazzanti, V.; Mollica, F.; Pellitteri, F.; Palone, M.; Lombardo, L. Stress Relaxation Properties of Five Orthodontic Aligner Materials: A 14-Day In-Vitro Study. Bioengineering 2022, 9, 349. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, L.; Martines, E.; Mazzanti, V.; Arreghini, A.; Mollica, F.; Siciliani, G. Stress relaxation properties of four orthodontic aligner materials: A 24-hour in vitro study. Angle Orthod. 2017, 87, 11–18. [Google Scholar] [CrossRef]
- Palone, M.; Pignotti, A.; Morin, E.; Pancari, C.; Spedicato, G.A.; Cremonini, F.; Lombardo, L. Analysis of overcorrection to be included for planning clear aligner therapy: A retrospective study. Angle Orthod. 2023, 93, 11–18. [Google Scholar] [CrossRef]
- Bernabé, E.; Flores-Mir, C. Estimating arch length discrepancy through Little’s Irregularity Index for epidemiological use. Eur. J. Orthod. 2006, 28, 269–273. [Google Scholar] [CrossRef]
- Proffit, W.; Fields, H.; Larson, B.; Sarver, D. Contemporary Orthodontics, 6th ed.; Mosby: Maryland Heights, MO, USA, 2018. [Google Scholar]
- Adel, S.M.; Vaid, N.R.; El-Harouni, N.; Kassem, H.; Zaher, A.R. TIP, TORQUE & ROTATIONS: How accurately do digital superimposition software packages quantify tooth movement? Prog. Orthod. 2022, 23, 8. [Google Scholar]
- Zeileis, A.; Torsten, H.; Kurt, H. Model-Based Recursive Partitioning. J. Comput. Graph. Stat. 2008, 17, 492–514. [Google Scholar] [CrossRef]
- Pandis, N.; Polychronopoulou, A.; Eliades, T. Sample size estimation: An overview with applications to orthodontic clinical trial designs. Am. J. Orthod. Dentofac. Orthop. 2011, 140, e141–e146. [Google Scholar] [CrossRef]
- Papadimitriou, A.; Mousoulea, S.; Gkantidis, N.; Kloukos, D. Clinical effectiveness of Invisalign® orthodontic treatment: A systematic review. Prog. Orthod. 2018, 19, 37. [Google Scholar] [CrossRef]
- Lombardo, L.; Arreghini, A.; Ramina, F.; Ghislanzoni, L.T.H.; Siciliani, G. Predictability of orthodontic movement with orthodontic aligners: A retrospective study. Prog. Orthod. 2017, 18, 35. [Google Scholar] [CrossRef] [PubMed]
- Misch, C.E. Contemporary Implant Dentistry, 4th ed.; Mosby: Maryland Heights, MO, USA, 2008. [Google Scholar]
- Elkholy, F.; Mikhaiel, B.; Schmidt, F.; Lapatki, B.G. Mechanical load exerted by PET-G aligners during mesial and distal derotation of a mandibular canine: An in vitro study. J. Orofac. Orthop. 2017, 78, 361–370. [Google Scholar] [CrossRef]
- Nelson, S.J. Wheeler’s Dental Anatomy, Physiology and Occlusion, 11th ed.; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Boyd, R.L. Predictability of Successful Orthodontic Treatment Using Invisalign. The Greater Philadelphia Society of Orthodontists Page. Available online: http://www.gpso.org/events/2003_outline.pdf. (accessed on 1 September 2023).
- Chisari, J.R.; McGorray, S.P.; Nair, M.; Wheeler, T.T. Variables affecting orthodontic tooth movement with clear aligners. Am. J. Orthod. Dentofac. Orthop. 2014, 145 (Suppl. S4), S82–S91. [Google Scholar] [CrossRef] [PubMed]
- Harris, E.F. Effects of patient age and sex on treatment: Correction of Class II malocclusion with the Begg technique. Angle Orthod. 2001, 71, 433–441. [Google Scholar] [PubMed]
- Dudic, A.; Giannopoulou, C.; Kiliaridis, S. Factors related to the rate of orthodontically induced tooth movement. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 616–621. [Google Scholar] [CrossRef]
- Schubert, A.; Jäger, F.; Maltha, J.C.; Bartzela, T.N. Age effect on orthodontic tooth movement rate and the composition of gingival crevicular fluid: A literature review. J. Orofac. Orthop. 2020, 81, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Torsello, F.; D’Amico, G.; Staderini, E.; Marigo, L.; Cordaro, M.; Castagnola, R. Factors Influencing Appliance Wearing Time during Orthodontic Treatments: A Literature Review. Appl. Sci. 2022, 12, 7807. [Google Scholar] [CrossRef]
- Weiss, J.; Eiser, H.M. Psychological timing of orthodontic treatment. Am. J. Orthod. Dentofac. Orthop. 1977, 72, 198–204. [Google Scholar] [CrossRef]
- Lione, R.; Paoloni, V.; Bartolommei, L.; Gazzani, F.; Meuli, S.; Pavoni, C.; Cozza, P. Maxillary arch development with Invisalign system. Angle Orthod. 2021, 91, 433–440. [Google Scholar] [CrossRef]
- Galan-Lopez, L.; Barcia-Gonzalez, J.; Plasencia, E. A systematic review of the accuracy and efficiency of dental movements with Invisalign®. Korean J. Orthod. 2019, 49, 140–149. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclination | Angulation | Rotation | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Prescribed Movements (T1) | Achieved Movements (T2) | Imprecision (|T1 − T2|) | Prescribed Movements (T1) | Achieved Movements (T2) | Imprecision (|T1 − T2|) | Prescribed Movements (T1) | Obtained Movements (T2) | Imprecision (|T1 − T2|) | ||||||||||||||
| Arch | Tooth Type | N. Observations | Mean (°) | SD (°) | Mean (°) | SD (°) | Mean (°) | SD (°) | N. Observations | Mean (°) | SD (°) | Mean (°) | SD (°) | Mean (°) | SD (°) | N. Observations | Mean (°) | SD (°) | Mean (°) | SD (°) | Mean (°) | SD (°) |
| Maxilla | Incisor | 192 | 4.31 | 1.77 | 3.85 | 2.36 | 1.70 | 1.26 | 229 | 5.92 | 3.54 | 5.04 | 3.50 | 1.97 | 1.82 | 320 | 8.66 | 6.12 | 5.33 | 4.61 | 3.49 | 2.68 |
| Canine | 92 | 4.11 | 2.01 | 3.27 | 1.98 | 1.56 | 1.34 | 97 | 4.31 | 1.86 | 3.07 | 2.00 | 1.91 | 1.60 | 128 | 8.46 | 4.99 | 4.10 | 3.20 | 4.38 | 3.23 | |
| Premolar | 159 | 4.51 | 1.85 | 3.77 | 2.08 | 1.32 | 1.11 | 42 | 3.53 | 1.70 | 3.42 | 2.42 | 1.98 | 1.32 | 152 | 5.66 | 3.40 | 3.56 | 2.62 | 2.57 | 2.16 | |
| Molar | 19 | 3.38 | 1.11 | 2.51 | 1.58 | 1.46 | 0.86 | 2 | 2.90 | 0.60 | 3.95 | 2.05 | 1.45 | 1.05 | 27 | 4.64 | 2.60 | 3.38 | 2.46 | 1.94 | 1.30 | |
| Mandible | Incisor | 238 | 5.02 | 2.73 | 4.25 | 2.84 | 1.44 | 1.11 | 216 | 4.58 | 2.47 | 4.09 | 2.72 | 1.67 | 1.29 | 307 | 8.18 | 6.14 | 5.95 | 4.94 | 2.92 | 2.37 |
| Canine | 123 | 4.51 | 1.87 | 4.07 | 2.44 | 1.60 | 1.47 | 79 | 3.66 | 1.94 | 3.17 | 1.90 | 1.60 | 1.33 | 143 | 9.79 | 5.53 | 5.50 | 3.94 | 4.48 | 3.00 | |
| Premolar | 171 | 4.32 | 2.07 | 4.03 | 2.57 | 1.52 | 1.23 | 56 | 3.57 | 1.44 | 2.94 | 2.41 | 2.04 | 1.41 | 174 | 6.95 | 4.70 | 3.75 | 2.66 | 3.90 | 3.49 | |
| Molar | 21 | 3.59 | 1.33 | 3.52 | 2.34 | 1.82 | 0.93 | 3 | 2.80 | 0.59 | 3.80 | 1.00 | 2.13 | 1.43 | 18 | 3.70 | 1.27 | 1.92 | 0.98 | 2.06 | 1.14 | |
| Maxilla | 462 | 4.30 | 1.84 | 3.65 | 2.19 | 1.53 | 1.23 | 370 | 5.21 | 3.14 | 4.34 | 3.19 | 1.96 | 1.71 | 627 | 7.72 | 5.41 | 4.57 | 3.94 | 3.38 | 2.73 | |
| Mandible | 553 | 4.64 | 2.35 | 4.11 | 2.66 | 1.51 | 1.23 | 354 | 4.20 | 2.26 | 3.70 | 2.55 | 1.72 | 1.33 | 642 | 8.08 | 5.69 | 5.16 | 4.28 | 3.52 | 2.92 | |
| Total | 1015 | 4.53 | 2.24 | 3.79 | 2.58 | 1.81 | 1.93 | 724 | 4.68 | 2.86 | 3.84 | 3.09 | 2.39 | 3.94 | 1269 | 8.30 | 5.51 | 4.81 | 4.20 | 4.18 | 3.96 | |
| Inclination | Angulation | Rotation | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Arch | Tooth Type | N. Observations | Mean (%) | SD (%) | N. Observations | Mean (%) | SD (%) | N. Observations | Mean (%) | SD (%) |
| Maxilla | Incisor | 192 | 91.25 | 53.54 | 229 | 91.16 | 58.31 | 320 | 61.28 | 28.28 |
| Canine | 92 | 82.43 | 50.86 | 97 | 72.73 | 41.45 | 128 | 49.59 | 29.43 | |
| Premolar | 159 | 84.00 | 35.87 | 42 | 98.29 | 73.42 | 152 | 62.86 | 35.03 | |
| Mandible | Incisor | 238 | 82.29 | 34.19 | 216 | 90.06 | 48.58 | 307 | 72.64 | 32.06 |
| Canine | 123 | 91.15 | 49.01 | 79 | 90.79 | 53.32 | 143 | 57.70 | 28.90 | |
| Premolar | 171 | 90.90 | 45.16 | 56 | 79.51 | 69.65 | 174 | 54.19 | 35.79 | |
| Maxilla | 443 | 86.26 | 47.39 | 368 | 87.33 | 57.14 | 600 | 59.45 | 31.31 | |
| Mandible | 532 | 87.17 | 42.68 | 351 | 88.71 | 54.11 | 624 | 63.67 | 33.56 | |
| Total | 975 | 86.76 | 44.89 | 719 | 88.01 | 55.68 | 1224 | 61.59 | 32.54 | |
| Tooth Type/Arch | Inclination | Angulation | Rotation | ||||
|---|---|---|---|---|---|---|---|
| p-Value | Significance | p-Value | Significance | p-Value | Significance | ||
| Incisor–Maxilla | Canine–Maxilla | 1.000 | NS | 0.007 | * | <0.001 | * |
| Premolar–Maxilla | 1.000 | NS | 0.421 | NS | 1.000 | NS | |
| Incisor–Mandible | 1.000 | NS | 0.931 | NS | 0.021 | * | |
| Canine–Mandible | 0.939 | NS | 0.995 | NS | 0.228 | NS | |
| Premolar–Mandible | 0.797 | NS | 0.006 | * | 0.001 | * | |
| Canine–Maxilla | Premolar–Maxilla | 0.997 | NS | 1.000 | NS | 0.038 | * |
| Incisor–Mandible | 0.997 | NS | 0.155 | NS | <0.001 | * | |
| Canine–Mandible | 0.706 | NS | 0.475 | NS | 0.609 | NS | |
| Premolar–Mandible | 0.602 | NS | 0.996 | NS | 1.000 | NS | |
| Premolar–Maxilla | Incisor–Mandible | 1.000 | NS | 0.800 | NS | 0.212 | NS |
| Canine–Mandible | 0.838 | NS | 0.920 | NS | 0.664 | NS | |
| Premolar–Mandible | 0.708 | NS | 1.000 | NS | 0.044 | * | |
| Incisor–Mandible | Canine–Mandible | 0.801 | NS | 1.000 | NS | <0.001 | * |
| Premolar–Mandible | 0.601 | NS | 0.083 | NS | <0.001 | * | |
| Canine–Mandible | Premolar–Mandible | 1.000 | NS | 0.204 | NS | 0.789 | NS |
| Initial (T0) | Prescribed (T1) | Achieved (T2) | Imprecision |(T2 − T1)| | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Arch | Linear Measurements | N. of Observations | Min (mm) | Max (mm) | Mean (mm) | SD (mm) | Min (mm) | Max (mm) | Mean (mm) | SD (mm) | Min (mm) | Max (mm) | Mean (mm) | SD (mm) | Min (mm) | Max (mm) | Mean (mm) | SD (mm) |
| Maxilla | Ic | 117 | 28.62 | 40.39 | 33.50 | 2.54 | 29.72 | 40.63 | 34.38 | 2.09 | 30.09 | 40.51 | 34.07 | 2.08 | 0.00 | 7.04 | 0.73 | 0.86 |
| Ip1 | 118 | 28.26 | 50.38 | 40.24 | 3.45 | 33.85 | 50.38 | 41.51 | 2.78 | 33.38 | 50.71 | 41.18 | 2.90 | 0.00 | 5.93 | 0.57 | 0.71 | |
| Ip2 | 115 | 34.03 | 56.76 | 45.64 | 3.63 | 34.46 | 57.12 | 46.64 | 3.35 | 34.21 | 57.11 | 46.43 | 3.32 | 0.00 | 2.14 | 0.34 | 0.36 | |
| Im | 118 | 37.74 | 58.86 | 48.55 | 3.76 | 38.06 | 58.95 | 49.10 | 3.62 | 37.90 | 58.89 | 48.95 | 3.59 | 0.00 | 1.73 | 0.32 | 0.38 | |
| Mandibular | Ic | 120 | 21.21 | 31.71 | 25.56 | 2.06 | 22.36 | 29.88 | 26.79 | 2.00 | 21.24 | 30.70 | 26.39 | 1.74 | 0.00 | 10.72 | 0.77 | 1.18 |
| Ip1 | 118 | 27.07 | 44.09 | 33.21 | 2.77 | 28.94 | 42.07 | 34.29 | 2.21 | 28.77 | 42.91 | 34.05 | 2.21 | 0.00 | 4.26 | 0.64 | 0.61 | |
| Ip2 | 117 | 30.39 | 51.29 | 38.77 | 3.15 | 33.26 | 52.97 | 39.86 | 2.77 | 33.19 | 51.45 | 39.55 | 2.78 | 0.00 | 2.13 | 0.48 | 0.44 | |
| Im | 113 | 36.52 | 54.17 | 42.23 | 3.11 | 37.46 | 54.41 | 42.82 | 3.02 | 37.05 | 53.61 | 42.59 | 2.97 | 0.00 | 1.84 | 0.37 | 0.41 | |
| T0 − T1 | T0 − T2 | T1 − T2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Arch | Linear Measurements | No. of Observations | Difference (mm) | p-Value | Significance | Difference (mm) | p-Value | Significance | Difference (mm) | p-Value | Significance |
| Maxilla | Ic | 117 | 0.88 | 0.01 | * | 0.57 | 0.13 | NS | 0.31 | 0.54 | NS |
| Ip1 | 118 | 1.27 | 0.004 | * | 0.94 | 0.05 | * | 0.33 | 0.68 | NS | |
| Ip2 | 115 | 0.99 | 0.07 | NS | 0.79 | 0.19 | NS | 0.20 | 0.89 | NS | |
| Im | 118 | 0.55 | 0.48 | NS | 0.15 | 0.95 | NS | 0.41 | 0.67 | NS | |
| Mandibular | Ic | 120 | 1.31 | <0.001 | * | 0.83 | 0.003 | * | 0.48 | 0.14 | NS |
| Ip1 | 118 | 1.08 | 0.002 | * | 0.84 | 0.02 | * | 0.24 | 0.002 | * | |
| Ip2 | 117 | 1.09 | 0.01 | * | 0.78 | 0.10 | NS | 0.31 | 0.70 | NS | |
| Im | 113 | 0.59 | 0.32 | NS | 0.23 | 0.84 | NS | 0.36 | 0.65 | NS | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mario, P.; de Villagomez, S.S.; Federica, P.; Cremonini, F.; Salvatore, R.; Lombardo, L. Evaluation of Tooth Movement Accuracy with the F22 Aligner System: A Retrospective Study. Appl. Sci. 2024, 14, 1641. https://doi.org/10.3390/app14041641
Mario P, de Villagomez SS, Federica P, Cremonini F, Salvatore R, Lombardo L. Evaluation of Tooth Movement Accuracy with the F22 Aligner System: A Retrospective Study. Applied Sciences. 2024; 14(4):1641. https://doi.org/10.3390/app14041641
Chicago/Turabian StyleMario, Palone, Silvia Squeo de Villagomez, Pellitteri Federica, Francesca Cremonini, Renato Salvatore, and Luca Lombardo. 2024. "Evaluation of Tooth Movement Accuracy with the F22 Aligner System: A Retrospective Study" Applied Sciences 14, no. 4: 1641. https://doi.org/10.3390/app14041641