Abstract
Background. Brain metastases are one of the leading causes of death in melanoma patients. This systematic review and meta-analysis aimed to look at the variables that affect melanoma patients’ intracranial treatment responses to immunotherapy and targeted therapy. Methods. A systematic search of PubMed and Scopus up to December 2023 was conducted to identify trials investigating treatment response of melanoma brain metastasis. This meta-analysis presents summary estimates (SEs) of treatment response and odd ratios (ORs) for the comparison between symptomatic and asymptomatic metastases. Generalised linear mixed models were used for the SE of the proportion of clinical responses and 95% CIs are reported. We investigated between-study heterogeneity using meta-regression. Results. We included 19 independent clinical trials for a total of 1074 patients with brain metastases. The SE of the overall response was 36% 95%CI [27%; 47%], I2 = 84%, similar to the SE for symptomatic metastases: SE = 29% 95%CI [16%; 47%], I2 = 80%. A significantly higher response of symptomatic metastases was observed between patients who had previously received immunotherapy compared to those who had not (47% vs. 9%, p-value = 0.001). The SE was greater for asymptomatic metastases (38% 95%CI [29%; 49%], I2 = 80%), and among these, patients that received the combo-immunotherapy importantly responded more than those who had received monotherapy (45% vs. 26.1%, p-value = 0.002). The major limit of our analysis is the absence of data about the specific intracranial response separately in asymptomatic and symptomatic patients in seven studies. Conclusions. This study shows the importance of starting immunotherapy as early as possible in asymptomatic patients. Randomised trials with greater statistical power are needed to find the best strategies for symptomatic and asymptomatic brain metastases.
1. Introduction
One of the primary factors contributing to the mortality of patients with metastatic melanoma is brain metastasis, which is considered among the major factors of poor prognosis [1]. After breast and lung cancer, melanoma causes the most metastases to the brain. During their clinical history, more than half of subjects’ brain metastases are detectable during staging scans. [2]. Central nervous system involvement is characterised in approximately 15% of stage III melanoma [3] and 75% of stage IV.
Prognostic factors in individuals with melanoma are based not only on the presence or absence of brain involvement but also on the metastases’ number and localisation, intra- and extracranial disease extension, leptomeningeal involvement, Eastern Cooperative Oncology Group (ECOG) performance status, patient’s age, LDH levels, and mostly the tumour burden. BRAF mutation presence or absence, the patient’s clinical conditions, ECOG performance status, comorbidities, and eventual autoimmune disease are factors that may influence the therapeutic strategy.
Chemotherapeutics, such as fotemustine [4], temozolomide [5], carmustine, and dacarbazine [6], were the first drugs tested for the treatment of melanoma brain metastases. Nevertheless, due to the inconsistent evidence of chemotherapy efficacy, in recent years, we have been exploring the path of immunotherapy, targeted therapy, and more recently adoptive therapy. Moreover, different drugs such as BRAF/MEK inhibitors have been tested in several studies with encouraging results [7,8,9,10,11,12,13]. Recent findings of trials that tested immunotherapy [14,15,16,17,18] have opened a new scenario and led to new studies on the combination of immunotherapy and targeted therapy (TT) [19,20,21,22] or chemotherapy [23]. Locoregional treatments, such as surgery and radiotherapy, have been considered the gold standard for the treatment of melanoma brain metastases for several years. Recent discoveries of the efficacy of BRAK/MEK inhibitors and immunotherapy in the central nervous system changed the systemic treatment of metastatic melanoma. The most recent studies have shown the effectiveness of combining radiotherapy and immune check-point inhibitors [23,24,25]. The efficacy of stereotactic radiotherapy within 6 months of receiving anti-PD-1 nivolumab in 26 pretreated patients with advanced resected and unresectable melanoma with brain metastases was demonstrated in a retrospective study by Ahmed et al. [23]. This retrospective analysis showed a 12-month local brain metastasis control rate in 85% of cases and a distant brain metastasis control rate in 53% of cases, due to a synergic effect with the anti-PD-1 inhibitor and stereotactic radiation. Furthermore, they demonstrated a median OS of 12 months from the date of immunotherapy initiation and 11.8 months from the date of radiation. Interestingly, the administration of nivolumab before, during, or after the radiotherapy showed a lower rate of neurotoxicities compared to the exclusive radiation treatment [24]. Williams et al. performed a phase I study involving 16 eligible patients, with the aim of evaluating the maximum tolerable dose (MTD) and safety of ipilimumab with stereotactic radiosurgery (SRS) or whole-brain radiotherapy (WBRT) in patients with brain metastases (BMs) from melanoma. Five patients were treated with whole-brain radiation therapy (WBRT) (arm A) and eleven with stereotactic radiosurgery (SRS) (arm B). Seven patients overall in arms A and B received ipilimumab 3 mg/kg and nine patients received a dose of 10 mg/kg. The authors concluded that the concomitance of ipilimumab 3 mg/kg and 10/kg with SRS is safe. The overall intracranial response, defined by the irRC, was immune-related SD in five patients (3%) and immune-related PR in one patient (7%) [25].
This systematic review and meta-analysis aimed to estimate intracranial responses to different treatments in melanoma metastatic to the brain and investigate factors influencing responses to immunotherapy and targeted therapy in brain metastases. Summary estimates of treatment responses from the most recent literature, including results from the most recently conducted trials, are presented. Unfortunately, there was a substantial lack of data from trials comparing immune check-point inhibitors with combinations of targeted therapies.
2. Materials and Methods
We performed a systematic review and meta-analysis of randomised studies published until December 2023.
2.1. Search Strategy
We reviewed published reports using validated search strategies from PubMed (http://www.ncbi.nlm.nih.gov/entrez/query.fcgi, accessed on 1 December 2023) and Scopus (https://www.scopus.com/search/form.uri?display=basic#basic, accessed on 1 December 2023) databases using the following search terms and syntax: (brain metastases OR cerebrum OR cerebral OR brain) AND (melanoma) AND (clinical study OR trial) AND (therapy OR treatment OR therapeutics). We searched Medline and Scopus databases using the search terms “brain metastases”, “melanoma”, “trial”, “target therapy”, and “immunotherapy.” We also performed manual searches of references cited in the retrieved articles and preceding reviews on the topic. Presentations given at international conferences were also retrieved (American Society of Clinical Oncology, American Association for Cancer Research, European Society of Medical Oncology, European Cancer Organization, Society for Melanoma Research, and European Association of Dermato-Oncology). We did not exclude studies based on the date of publication or the language of the article. Additional studies found in the bibliography of relevant articles were also included. Patients were enrolled in international multicentric trials from every continent.
2.2. Inclusion and Exclusion Criteria
We included articles describing clinical trials and reporting data regarding the radiological response of brain metastases in melanoma patients. All studies had to be independent to avoid including duplicate data in the summary estimation. In the case of multiple reports from the same study, we considered estimates from the most recent publication. We considered as eligibility criteria clinical trials assessing immunotherapy and brain radiation therapy in symptomatic and asymptomatic patients with melanoma brain metastases, including intracranial response/benefit.
2.3. Data Retrieval and Quality Assessment
We collected frequencies of treatment responses of brain metastases in asymptomatic and symptomatic patients. Two researchers independently retrieved the data and cross-checked them. If there was a discrepancy, these two compared the search results and found a consensus. We recorded the first author, year of publication, trial name and registration number, study phase, treatment, type of immunotherapy (if performed), and information regarding local therapy, previous immunotherapy, and previous TT, and ECOG performance status. The authors did not specify any type of neurological symptoms, but they divided patients based on whether local treatment or high-dose corticosteroids were needed or not. Consequently, we considered asymptomatic patients to be all the subjects with evaluable radiological intracranial tumour burden without neurological symptoms and who did not request either a local treatment (radiotherapy or neurosurgery) or the use of corticosteroids. On the other hand, the dose and duration of corticosteroid treatment for symptomatic patients were directly proportional to both the size and number of brain metastases and peritumoural oedema. The quality of our systematic review was assessed according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) checklist [26] (Supplementary Table S1). We used the Cochrane risk-of-bias tool to assess the quality of clinical studies included in the analysis (Supplementary Table S2).
2.4. Statistical Analysis
Generalised linear mixed models were used for the summary estimation (SE) of the proportion of clinical responses and 95% CIs, as well as summary of odds ratios (SORs) and 95% Cis, to assess differences between the responses of patients with asymptomatic and symptomatic brain metastases. The percentage of variability due to heterogeneity between studies was evaluated with the index [27]: < 50% was interpreted as an indication that the heterogeneity found between studies was not statistically significant [27]. Subgroup analyses and meta-regression were used to investigate sources of between-study heterogeneity in terms of type of treatment, type of immunotherapy (if performed), local therapy, previous immunotherapy, previous TT, ECOG PS, sample size, and publication year. In addition, sensitivity analyses were carried out to investigate the stability of the summary estimates concerning each study by excluding individual studies from the analysis. Egger’s linear regression [28], Begg’s correlation test [29], and visual inspection of funnel plots were used to assess the presence of publication bias. All reported p-values were two-sided and a p-value < 0.05 was considered statistically significant. Meta-analyses were carried out using the RStudio software (R version 4.0.0).
3. Results
3.1. Characteristics of Eligible Studies
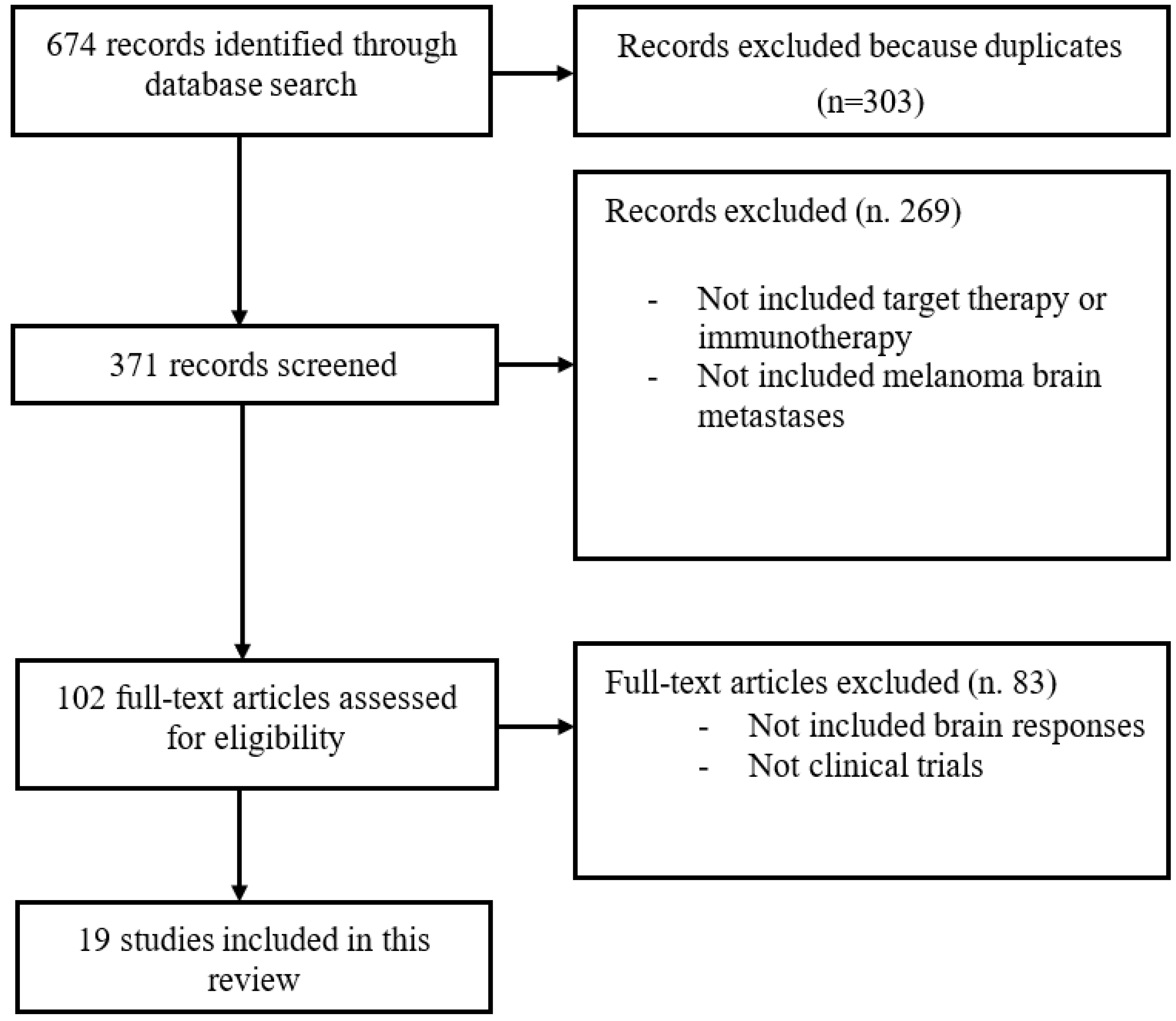
Based on the search strategy, we initially identified 674 articles. Full-text review was undertaken for 102 potentially suitable articles, while 83 studies were excluded because they did not include brain responses or were not clinical trials. After the application of the inclusion and exclusion criteria (Figure 1), there were 19 independent studies included in the review.
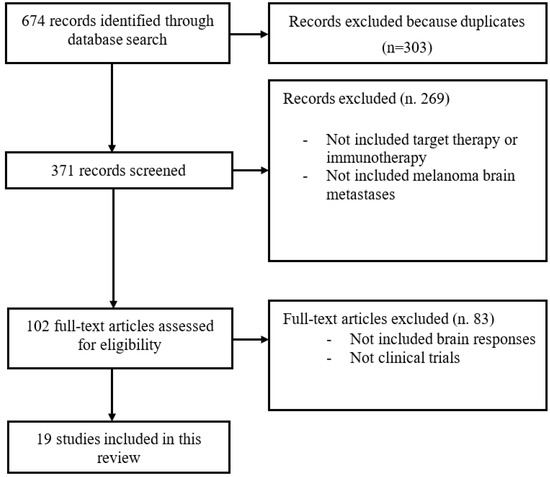
Figure 1.
Flowchart of study selection process.
A total of 1074 patients were included in the quantitative analyses. The main characteristics of the selected studies are presented in Table 1. Information regarding the responses in the symptomatic and asymptomatic brain metastasis patients is reported in Table 2. Patients were enrolled from each country. No relevant differences in demographic terms were detected.

Table 1.
Characteristics of the 19 studies included, comprising provided 36 and 1074 patients.
Table 2.
Total symptomatic and asymptomatic metastases and correspondent clinical responses.
3.2. Overall Response
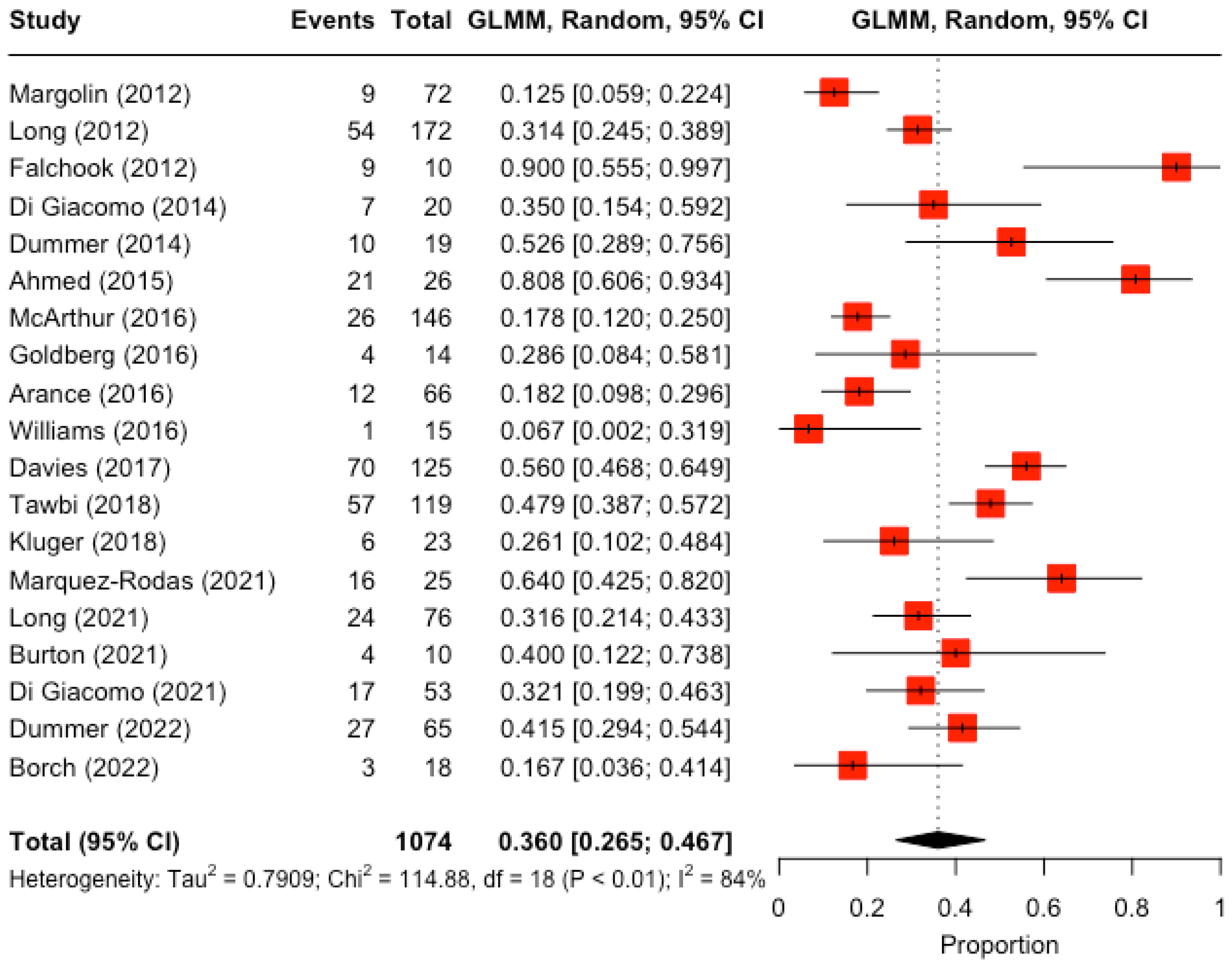
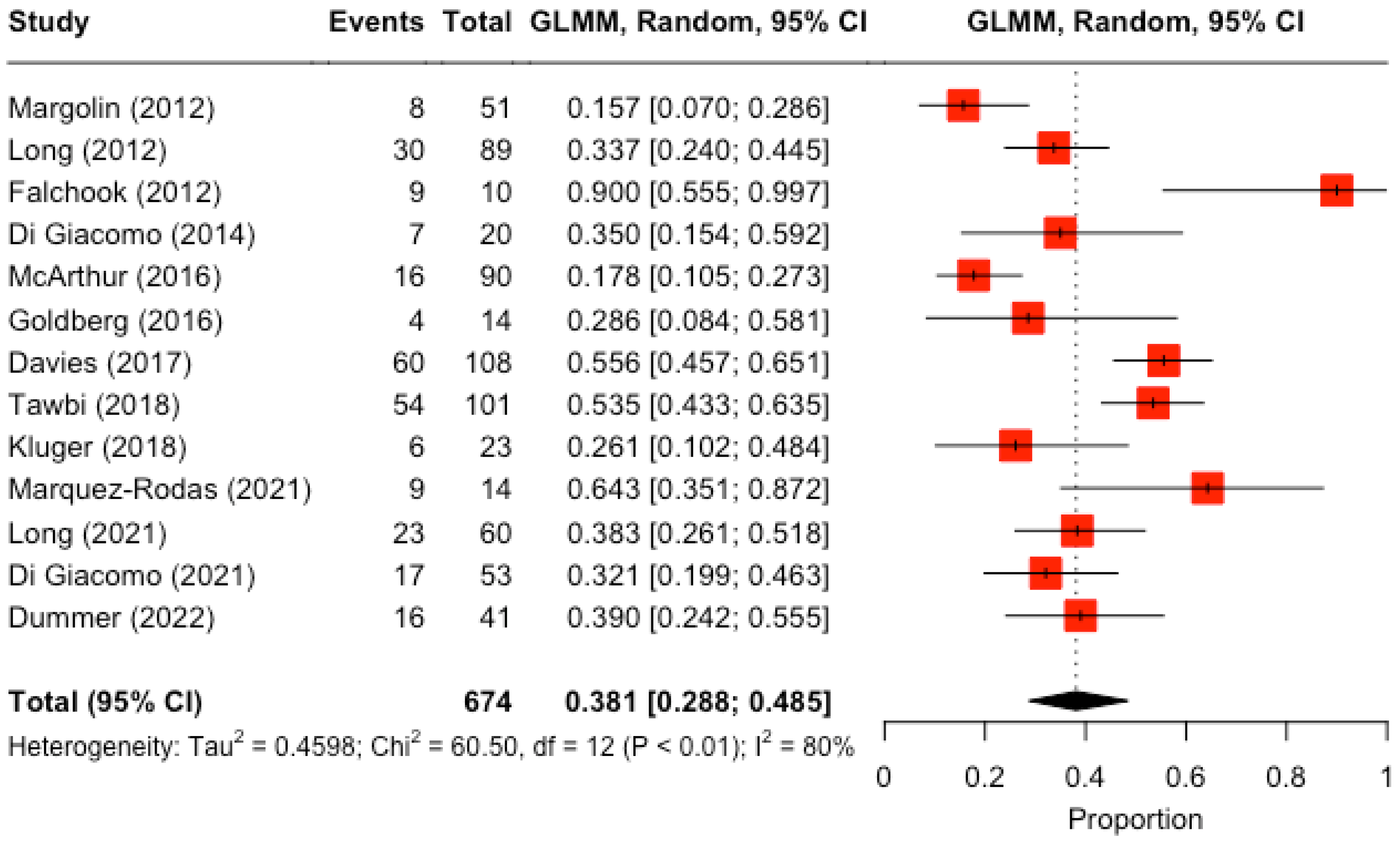
In the analysis of overall response, 19 papers were considered in which there was information on treatment clinical response. The SE of the overall response was 36% (95% CI 27%; 47%, Figure 2). Between-study heterogeneity was significant (I2 = 84%). There were no significant differences in response by type of treatment, type of immunotherapy (if performed), local therapy, previous immunotherapy, previous TT, or ECOG PS (Table 3).
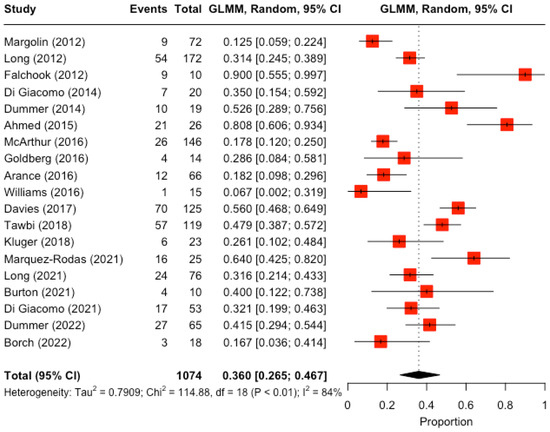
Figure 2.
Overall treatment responses of brain metastases in melanoma patients. Reported measures of heterogeneity: Tau2 (prespecified value for the square root of the between-study variance, restricted maximum-likelihood estimator).
Table 3.
Subgroup analysis for the overall treatment responses of brain metastases in melanoma patients.
We also carried out a leave-one-out analysis and did not find any significant change. In particular, excluding Ahmed, a retrospective analysis of two trials designed not to assess brain metastasis responses, the summary estimate did not change (33.5% (5% CI 25.3%; 43%), I2 = 83%).
3.3. Response of Symptomatic Metastases
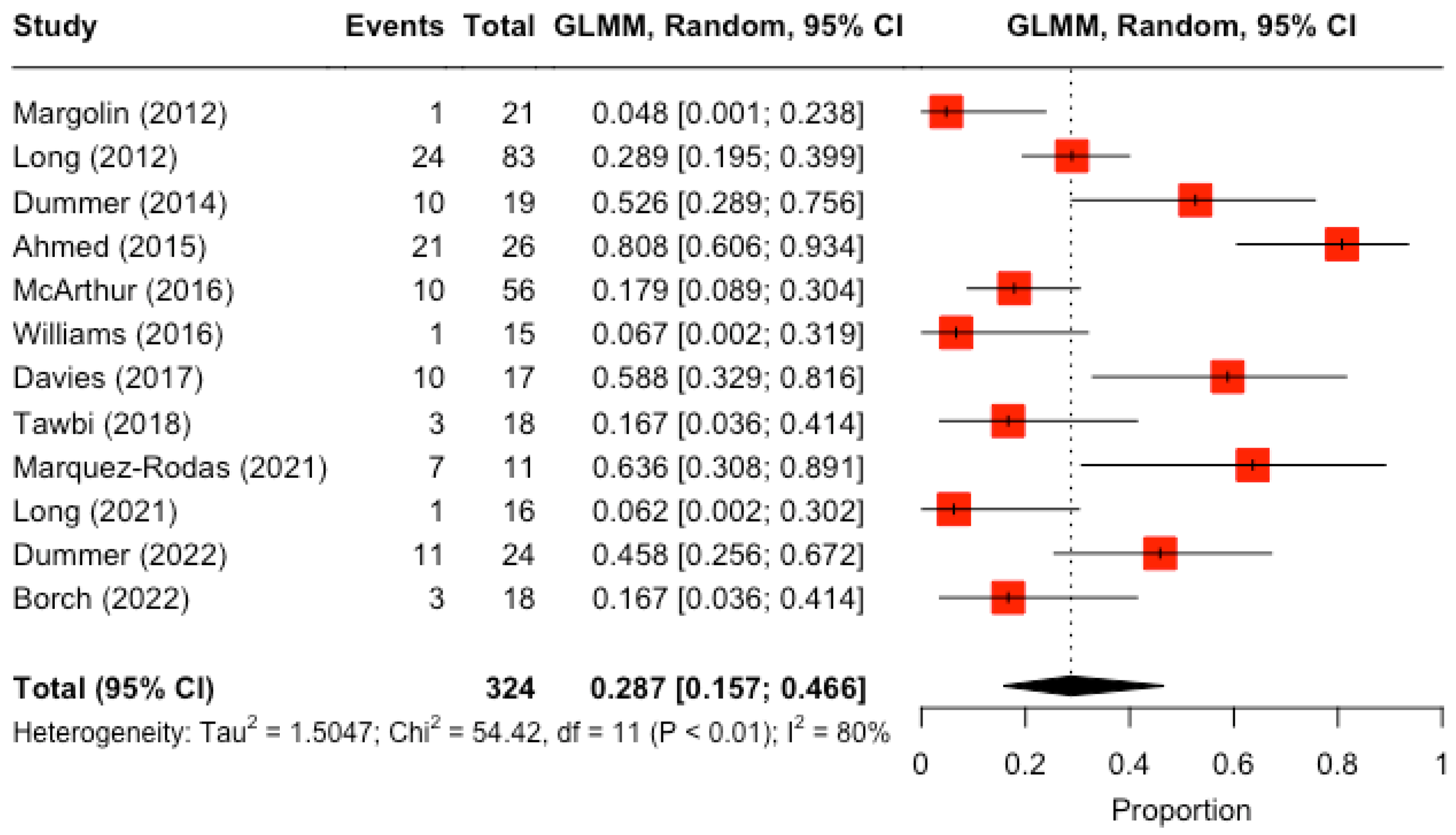
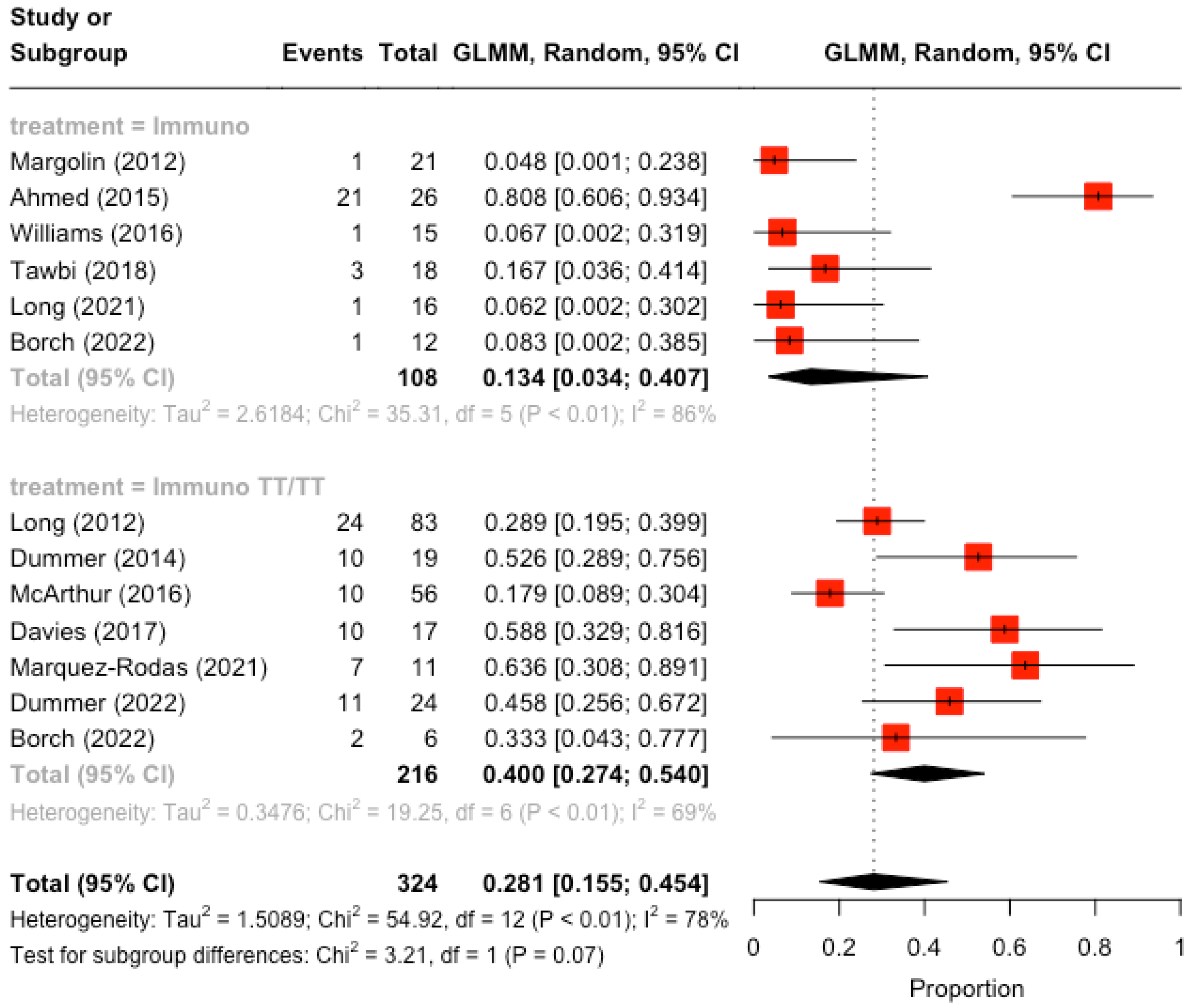
In the analysis concerning the response of symptomatic metastases, 12 studies are included. The summary estimate of the overall response was 29% (95% CI [16%; 47%], Figure 3), with high between-study heterogeneity (I2 = 80%). A significant difference in response was observed for patients who had previously received immunotherapy, who responded significantly more than those who had not (47% vs. 9%, p-value = 0.001, Table 4, Figure 4). A borderline significant difference was found in the clinical response for those who had had immunotherapy plus TT or TT alone who responded more and those who had had immunotherapy alone (40% vs. 13%, p-value = 0.07, Table 4, Figure 5).
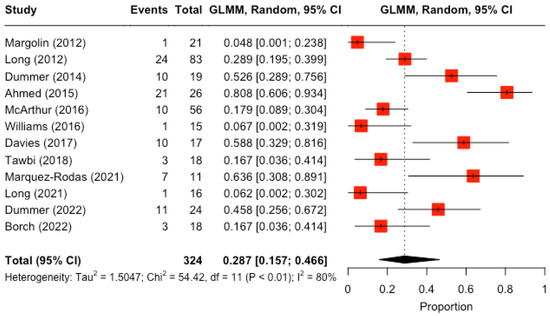
Figure 3.
Treatment responses of symptomatic brain metastases in melanoma patients. Reported measures of heterogeneity: Tau2 (prespecified value for the square root of the between-study variance, restricted maximum-likelihood estimator).
Table 4.
Subgroup analysis for treatment responses of symptomatic brain metastases in melanoma patients.
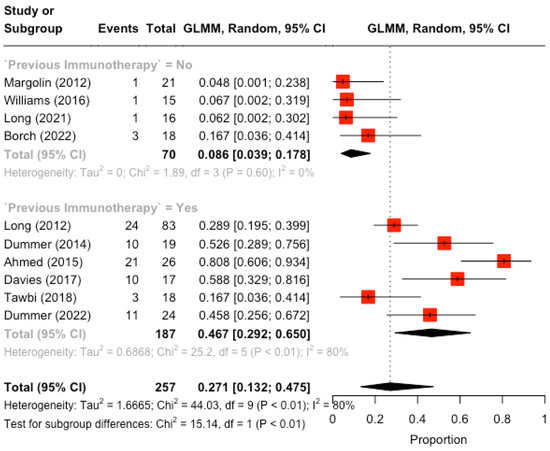
Figure 4.
Subgroup analysis for treatment responses of symptomatic brain metastases in melanoma patients. Reported measures of heterogeneity: Tau2 (prespecified value for the square root of the between-study variance, restricted maximum-likelihood estimator).
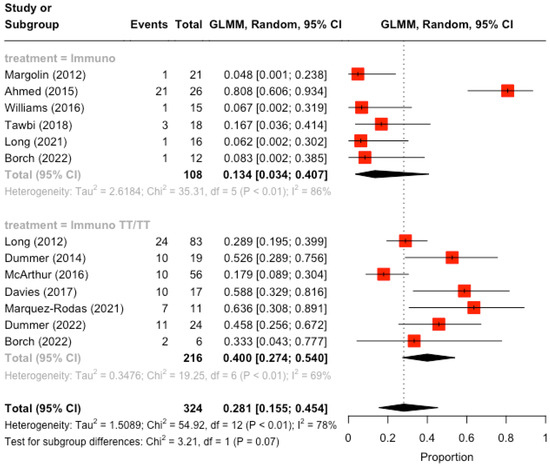
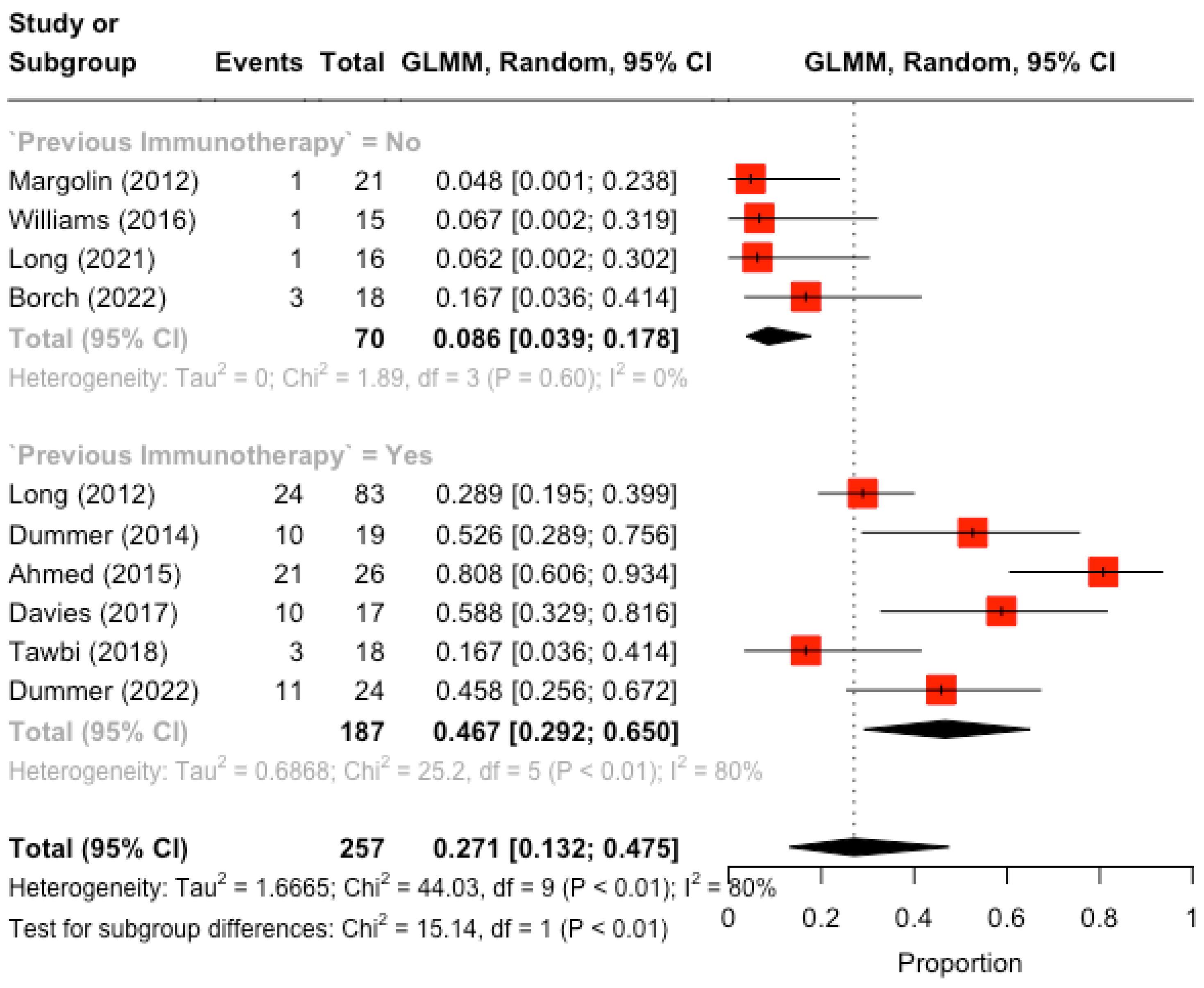
Figure 5.
Subgroup analysis for treatment responses of symptomatic brain metastases in melanoma patients by previous immunotherapy. Reported measures of heterogeneity: Tau2 (prespecified value for the square root of the between-study variance, restricted maximum-likelihood estimator).
3.4. Response of Asymptomatic Metastases
In the analysis concerning asymptomatic metastases, 13 were analysed. The SE of the overall response was greater than for symptomatic metastases (38% 95% CI [29%; 49%], Figure 6), with high between-study heterogeneity (I2 = 80%). A significant difference in response was observed for patients who received immunotherapy: patients who received the combo-immunotherapy obtained a deeper response than those who had received monotherapy (45% vs. 26.1%, p-value = 0.002, Table 5). Patients with ECOG PS of 2 responded objectively more than patients with an ECOG PS of 1 (52 % vs. 30%, p-value = 0.01, Table 5); however, this effect was lost in a multivariate meta-regression model controlling for the treatment. Neither sample size nor publication year was significantly associated with response (p-value = 0.74 and p-value = 0.63, respectively).
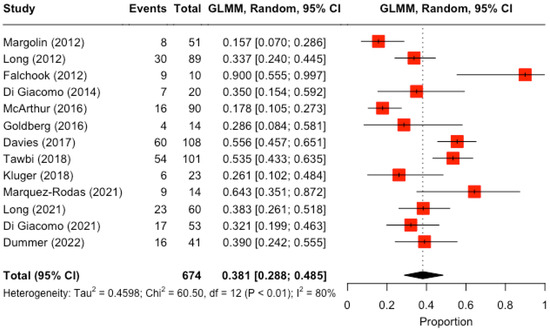
Figure 6.
Treatment responses of asymptomatic brain metastases in melanoma patients. Reported measures of heterogeneity: Tau2 (prespecified value for the square root of the between-study variance, restricted maximum-likelihood estimator).
Table 5.
Subgroup analysis for treatment responses of asymptomatic brain metastases in melanoma patients.
3.5. Comparison between Symptomatic and Asymptomatic
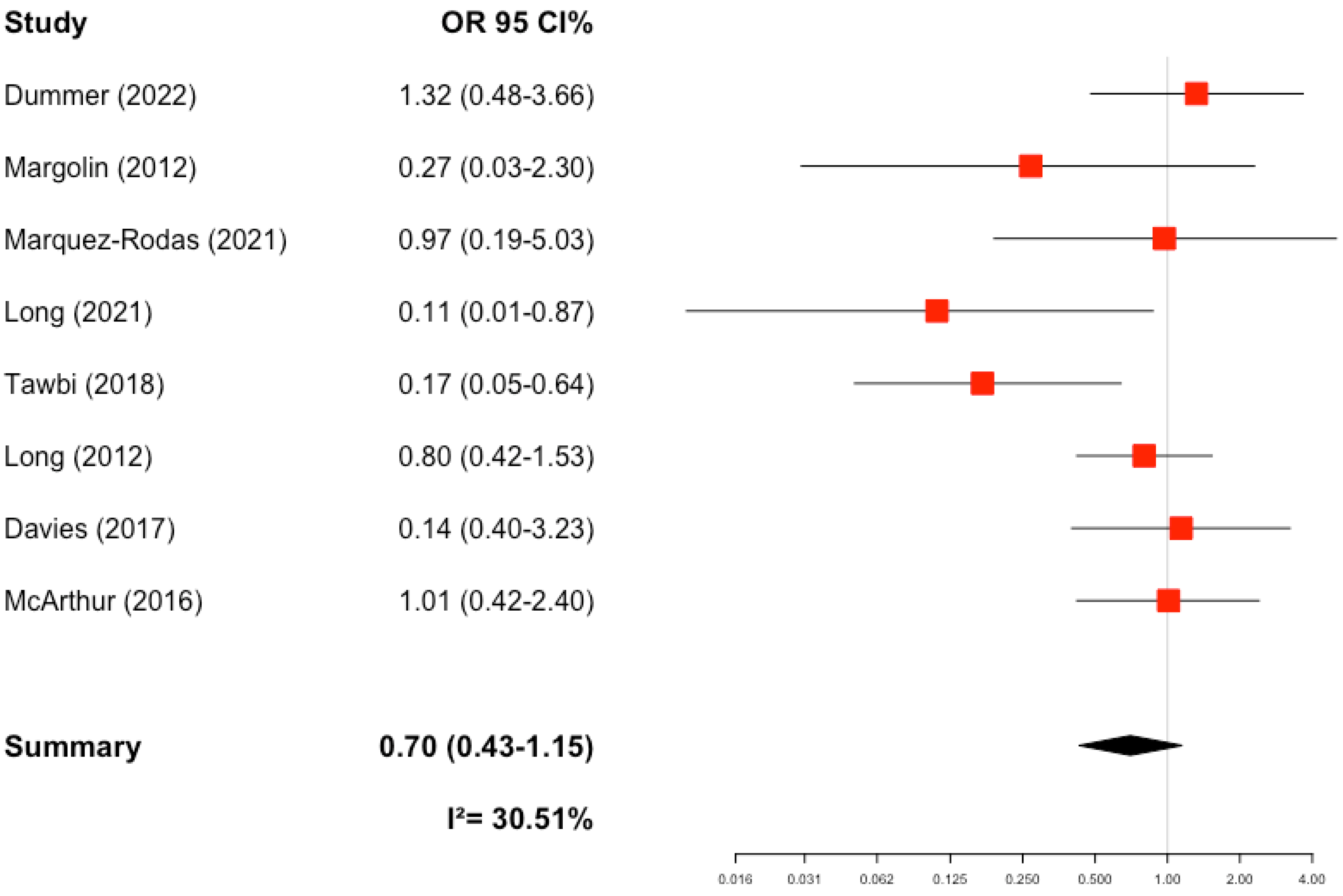
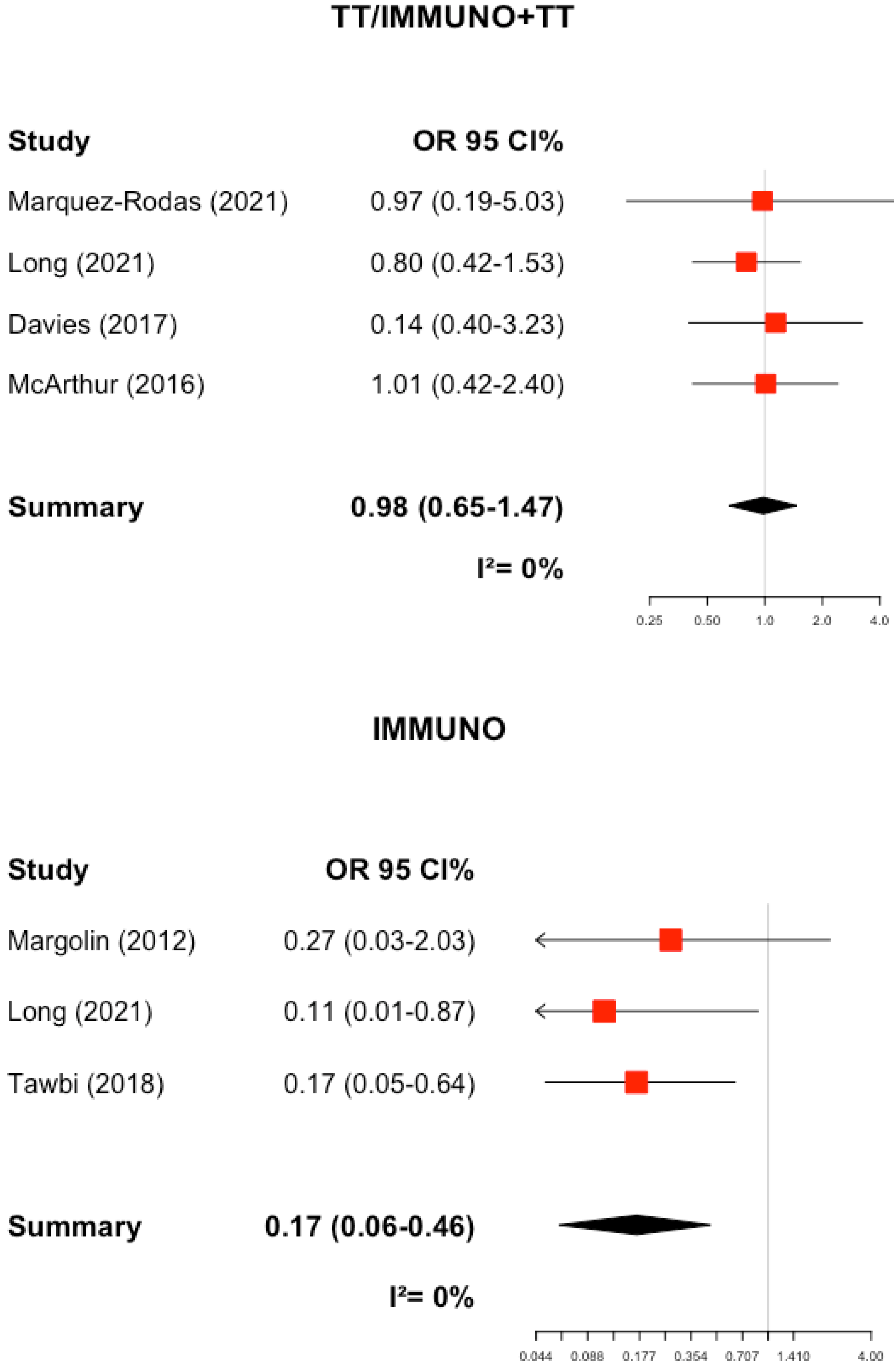
The SE of the OR for the comparison between symptomatic and asymptomatic was not significant (0.70, 95%CI [0.43–1.15], I2 = 30.5, Figure 7), and no publication bias emerged. However, in the subgroup analysis (Table 6), there was a significant reduction in the likelihood of responding to treatment in those who had had only immunotherapy and were symptomatic compared with asymptomatic (ORImmuno+TT/TT = 0.98 vs. ORImmuno = 0.17, p-value = 0.001, Figure 8) and a significant reduction in the probability of response among patients that had previously received immunotherapy (ORprevious immuno = 0.74 vs. ORno previous immuno = 0.17, p-value = 0.05).
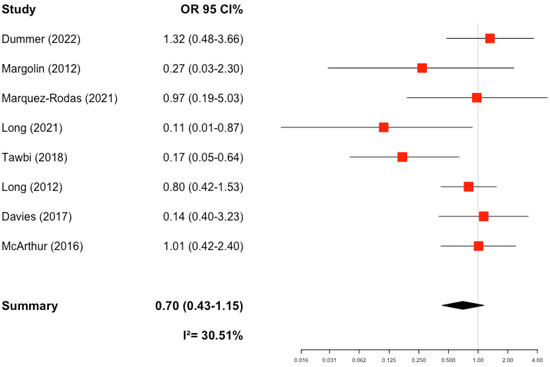
Figure 7.
Odds ratios for treatment responses of symptomatic vs. asymptomatic brain metastases in melanoma patients. Reported measures of heterogeneity: Tau2 (prespecified value for the square root of the between-study variance, restricted maximum-likelihood estimator).
Table 6.
Subgroup analysis for treatment responses of symptomatic vs. asymptomatic brain metastases in melanoma patients.
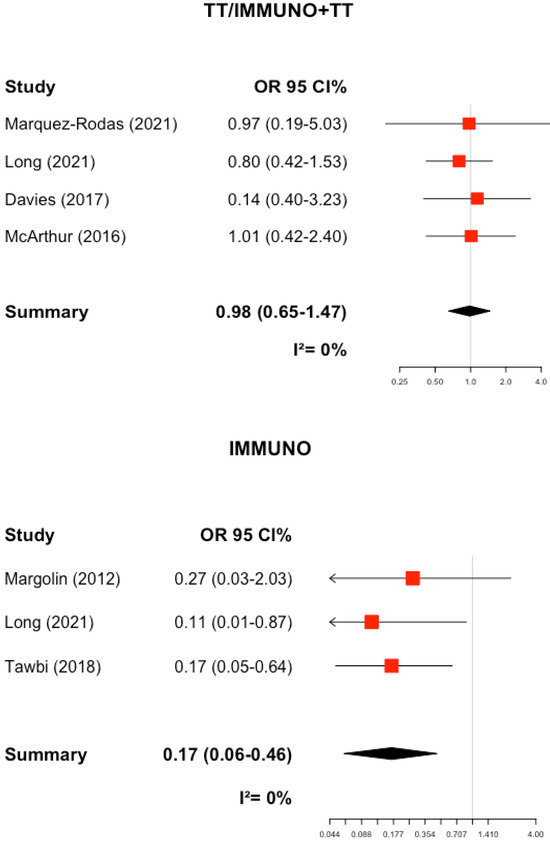
Figure 8.
Odds ratios for treatment responses of symptomatic vs. asymptomatic brain metastases in melanoma patients by treatment. Reported measures of heterogeneity: Tau2 (prespecified value for the square root of the between-study variance, restricted maximum-likelihood estimator).
We investigated also the influence of previous radiotherapy, but we did not find any significant differences.
3.6. Methodological Quality
The full data regarding quality assessment according to the Cochrane Collaboration risk-of-ias tool (CCRBT) are described in Supplementary material Table S2. Overall, we found a low risk of bias, and this is not surprising, since only three studies were phase III randomised trials.
4. Discussion
This is the largest comprehensive systematic review and meta-analysis carried out. We show that overall, the SE of the treatment response is low (36% with 95% CI 27%-47%), indicating that less than half of the patients responded; however, there is a large heterogeneity due to treatment and type of disease. Although we do not observe a meaningful difference between intracranial benefit in asymptomatic and symptomatic patients, subgroup analysis and meta-regression found a statistically significant better brain metastasis response in symptomatic patients who received immunotherapy compared to patients who received a combination (immunotherapy and TT): 47% vs. 9%, p-value = 0.001. Reduction in number of asymptomatic metastases was more substantial when patients received the combo-immunotherapy compared to those who had received monotherapy: 45% vs. 26.1%, p-value = 0.002.
Our hypothesis is that maybe T-cell activation by immune check-point inhibitors should be more effective in at early stage of intracranial dissemination or in an asymptomatic disease. The onset of cerebral oedema could adversely affect the intracranial immune activity. The authors did not provide in-depth data regarding the different responses to immunotherapy in terms of gender and age. The lack of comparative trials between oral targeted therapy versus intravenous immunotherapy represents the main limitation influencing physician choice in clinical practice.
For several years, locoregional treatment of melanoma brain metastases, such as surgery and radiotherapy, was considered the gold standard. The current analysis has provided a quantification of intracranial benefit for each type of treatment, aiming to find the best strategy in melanoma patients affected by brain metastasis.
Similar to what was found in Rulli’s meta-analyses [30], which considered intracranial response for 12 clinical trials, there was no considerable difference in asymptomatic patients versus symptomatic ones. However, we observed that the clinical remission or partial response to different types of treatment exclusively depends on neurological symptoms. An important observation concerns the response of patients who have not previously received first-line immunotherapy, as this response is different in patients with symptomatic or asymptomatic brain metastases.
The first randomised phase III trial [17] already showed that patients with untreated asymptomatic brain metastasis immunotherapy (p-value = 0.017) had significantly improved overall survival (OS) compared to fotemustine: patients receiving ipilimumab plus nivolumab, had a 4-year OS rate that was significantly higher than those receiving fotemustine (41% vs. 11%). Additionally, patients receiving ipilimumab plus nivolumab experienced significantly fewer high-grade adverse events (AEs) (30%) than those receiving either of the fotemustine-containing arms (48% and 69%, respectively). Furthermore, Hussein Tawbi and co-authors [14] reported in the CheckMate 204 trial a remarkable rate of 72% for asymptomatic patients, with 3-year OS when treated with nivolumab plus ipilimumab. These impressive data on long-term outcomes turn dogma upside down, because the melanoma patients in this group have historically had very poor therapeutic outcomes and have been difficult to treat. Patients with melanoma and brain metastases were previously routinely excluded from industry-sponsored clinical trials with immune check-point inhibitors because of their poor prognosis and the prevailing dogma that the blood–brain barrier would prevent effector immune cells from migrating to the brain. Patients with untreated brain metastases have a better prognosis due to both a limited number and small metastases, which can be translated into a reduction in intracranial oedema and neurological symptoms. This explains the higher response rate to check-point inhibitors in asymptomatic patients. On the opposite side, an individual with symptomatic disease may have a poor prognosis because of reduced compliance with pharmacological interventions, request for an invasive treatment such as neurosurgery, one or more visits to radiotherapy departments, and need for high-dose steroids and drugs for preventing convulsions and reducing brain oedema. In conclusion, early immunotherapy for asymptomatic patients may quickly reduce the spread of intracranial malignant melanocyte dissemination and the consequential deterioration of the systemic clinical conditions. Symptomatic metastases require high doses of steroids, which can decrease the effectiveness of T lymphocytes against cancer cells. This could reduce the check-point inhibitors activity in symptomatic patients.
Given that clinical response and survival from asymptomatic brain metastases are higher, it may be possible to omit radiation in selected patients. For symptomatic brain metastases, outcomes are worse with immunotherapy and localised treatment such as stereotactic radiosurgery should be suggested for control. It is suggested that immunotherapy be started as soon as possible [30].
Check-point inhibitor treatment response can be obtained in patients on lower doses of steroids, while daily steroid doses above 25 mg appear incompatible with CPI benefit, as demonstrated by Borch et al. in the initial report from the MEMBRAINS trial, where patients treated with lower daily doses of corticosteroids obtained a better response in comparison to those receiving high doses [20].
The effectiveness of combining radiotherapy and immune check-point inhibitors for brain metastases has been shown in recent trials. Ahmed et al. [23] wrote a retrospective analysis of a clinical trial primarily designed to assess the neurotoxicity of nivolumab, not brain benefit. The very high response rate for stereotactic radiotherapy within 6 months of receiving anti-PD-1 nivolumab in 26 pretreated patients with advanced resected and unresectable melanoma may be due to the study design. In fact, some patients were pretreated on protocol NCT01176461, with 10 a peptide vaccine, and 7 patients were treated on protocol NCT01176474 in an adjuvant setting with a peptide vaccine. Some received cytotoxic chemotherapy before starting nivolumab, and some received prior immunotherapies or targeted agents. Anyway, the exclusion of this trial did not change our summary results.
Gender and age are recognised risk factors linked to the development of melanoma brain metastases, in particular male gender and age over 60 years. Several publications showed in general a female advantage that gives women significantly longer survival compared to men, confirmed by pooled clinical trials and multivariate analyses [31]. Considering the known advantages of the female immune system, it is not easy to understand why the recently developed immunotherapies showed better improvements in men than in women [32,33]. On the other hand, standard combo treatment for brain metastases does not show a significantly different effect by gender.
The major limit of our analyses is the absence of data about the specific intracranial response separately in asymptomatic and symptomatic patients in seven studies. In addition, we considered symptomatic patients who had received a previous surgical or radiant treatment and who were treated with high doses of steroids. Another limitation is the absence of a randomised trial that directly compares the intracranial benefit with TT vs. immunotherapy. Moreover, the mixture of phase I, II, and III trials introduces heterogeneity due to the patient’s performance status, dose level received, number of cycles received, use of steroids allowed or not, and number and type of previous therapeutic interventions.
In conclusion, the current meta-analyses described groups of patients affected by melanoma brain metastasis with symptomatic and asymptomatic disease, and found different results from the administration of immunotherapies or targeted therapies. Randomised trials with more statistical power should be designed to identify the best strategies for symptomatic and asymptomatic brain metastases considering the toxicity and the activation of T cells induced by immunotherapy, which could result in cerebral peritumoural oedema.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/app14062222/s1, Table S1: Preferred Reporting Items for Systematic Reviews and Meta-Analyses) checklist; Table S2: Cochrane Collaboration Risk of Bias Tool (CCRBT).
Author Contributions
Data curation: L.O., investigation: L.O. and A.G. and O.D.; writing—original draft preparation: L.O. and A.G., formal analysis A.G. and O.D., methodology A.G., O.D. and S.G., software A.G. and O.D. visualisation A.G., O.D. and S.G., writing and editing: G.C., Supervision: P.Q. and S.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
IEO: the European Institute of Oncology, is partially supported by the Italian Ministry of Health (with “Ricerca Corrente” and “5 × 1000” funds) and A.G. was supported by a Fondazione IEO-Monzino Fellowship.
Conflicts of Interest
Paola Queirolo had a consultant advisory role for Roche, NOVARTIS, Pierre Fabre, MSD, BMS, Merck Serono, Sun pharma, Sanofi Regeneron.
References
- Davies, M.A.; Liu, P.; McIntyre, S.; Kim, K.B.; Papadopoulos, N.; Hwu, W.; Hwu, P.; Bedikian, A. Prognostic factors for survival in melanoma patients with brain metastases. Cancer 2010, 117, 1687–1696. [Google Scholar] [CrossRef]
- Zakrzewski, J.; Geraghty, L.N.; Rose, A.E.; Christos, P.J.; Mazumdar, M.; Polsky, D.; Shapiro, R.; Berman, R.; Darvishian, F.; Hernando, E.; et al. Clinical variables and primary tumor characteristics predictive of the development of melanoma brain metastases and post-brain metastases survival. Cancer 2011, 117, 1711–1720. [Google Scholar] [CrossRef]
- Addeo, R.; Zappavigna, S.; Luce, A.; Facchini, S.; Caraglia, M. Chemotherapy in the management of brain metastases: The emerging role of fotemustine for patients with melanoma and NSCLC. Expert Opin Drug Saf. 2013, 12, 729–740. [Google Scholar] [CrossRef]
- Li, R.-H.; Hou, X.; Yang, C.-S.; Liu, W.-L.; Tang, J.-Q.; Liu, Y.-Q.; Jiang, G. Temozolomide for Treating Malignant Melanoma. J Coll Physicians Surg Pak. 2015, 25, 680–688. [Google Scholar]
- Douglas, J.G.; Margolin, K. The treatment of brain metastases from malignant melanoma. Semin Oncol. 2002, 29, 518–524. [Google Scholar] [CrossRef]
- Long, G.V.; Trefzer, U.; Davies, M.A.; Kefford, R.F.; Ascierto, P.A.; Chapman, P.B.; Puzanov, I.; Hauschild, A.; Robert, C.; Algazi, A.; et al. Dabrafenib in patients with Val600Glu or Val600Lys BRAF-mutant melanoma metastatic to the brain (BREAK-MB): A multicentre, open-label, phase 2 trial. Lancet Oncol. 2012, 13, 1087–1095. [Google Scholar] [CrossRef]
- Falchook, G.S.; Long, G.V.; Kurzrock, R.; Kim, K.B.; Arkenau, T.H.; Brown, M.P.; Hamid, O.; Infante, J.R.; Millward, M.; Pavlick, A.C.; et al. Dabrafenib in patients with melanoma, untreated brain metastases, and other solid tumours: A phase 1 dose-escalation trial. Lancet 2012, 379, 1893–1901. [Google Scholar] [CrossRef]
- Dummer, R.; Goldinger, S.M.; Turtschi, C.P.; Eggmann, N.B.; Michielin, O.; Mitchell, L.; Veronese, L.; Hilfiker, P.R.; Felderer, L.; Rinderknecht, J.D. Vemurafenib in patients with BRAF(V600) mutation-positive melanoma with symptomatic brain metastases: Final results of an open-label pilot study. Eur. J. Cancer 2014, 50, 611–621. [Google Scholar] [CrossRef] [PubMed]
- Arance, A.M.; Berrocal, A.; Lopez-Martin, J.A.; de la Cruz-Merino, L.; Soriano, V.; Algarra, S.M.; Alonso, L.; Cerezuela, P.; La Orden, B.; Espinosa, E. Safety of vemurafenib in patients with BRAF V600 mutated metastatic melanoma: The Spanish experience. Clin Transl Oncol. 2016, 18, 1147–1157. [Google Scholar] [CrossRef] [PubMed]
- McArthur, G.A.; Maio, M.; Arance, A.; Nathan, P.; Blank, C.; Avril, M.-F.; Garbe, C.; Hauschild, A.; Schadendorf, D.; Hamid, O.; et al. Vemurafenib in metastatic melanoma patients with brain metastases: An open-label, single-arm, phase 2, multicentre study. Ann Oncol. 2016, 28, 634–641. [Google Scholar] [CrossRef] [PubMed]
- Davies, M.A.; Saiag, P.; Robert, C.; Grob, J.-J.; Flaherty, K.T.; Arance, A.; Chiarion Sileni, V.; Thomas, L.; Lesimple, T.; Mortier, L.; et al. Dabrafenib plus trametinib in patients with BRAFV600-mutant melanoma brain metastases (COMBI-MB): A multicentre, multicohort, open-label, phase 2 trial. Lancet Oncol. 2017, 18, 863–873. [Google Scholar] [CrossRef] [PubMed]
- Marquez-Rodas, I.; Arance, A.; Berciano Guerrero, M.A.; Díaz Beveridge, R.; Alamo, M.D.C.; Garcia Castaño, A.; Gonzalez Cao, M.; Vidal, J.; Puertolas Hernandez, T.; Soria, A.; et al. Intracranial activity of encorafenib and binimetinib followed by radiotherapy in patients with BRAF mutated melanoma and brain metastasis: Preliminary results of the GEM1802/ EBRAIN-MEL phase II clinical trial. Ann. Oncol. 2021, 32, S870. [Google Scholar] [CrossRef]
- Margolin, K.; Ernstoff, M.S.; Hamid, O.; Lawrence, D.; McDermott, D.; Puzanov, I.; Wolchok, J.D.; Clark, J.I.; Sznol, M.; Logan, T.F.; et al. Ipilimumab in patients with melanoma and brain metastases: An open-label, phase 2 trial. Lancet Oncol. 2012, 13, 459–465. [Google Scholar] [CrossRef]
- Tawbi, H.A.; Forsyth, P.A.; Hodi, F.S.; Algazi, A.P.; Hamid, O.; Lao, C.D.; Moschos, S.J.; Atkins, M.B.; Lewis, K.; A Postow, M.; et al. Long-term outcomes of patients with active melanoma brain metastases treated with combination nivolumab plus ipilimumab (CheckMate 204): Final results of an open-label, multicentre, phase 2 study. Lancet Oncol. 2021, 22, 1692–1704. [Google Scholar] [CrossRef]
- Kluger, H.M.; Chiang, V.; Mahajan, A.; Zito, C.R.; Sznol, M.; Tran, T.; Weiss, S.A.; Cohen, J.V.; Yu, J.; Hegde, U.; et al. Long-Term Survival of Patients With Melanoma With Active Brain Metastases Treated With Pembrolizumab on a Phase II Trial. J. Clin. Oncol. 2019, 37, 52–60. [Google Scholar] [CrossRef]
- Long, G.V.; Atkinson, V.; Lo, S.; Sandhu, S.; Guminski, A.D.; Brown, M.P.; Wilmott, J.S.; Edwards, J.; Gonzalez, M.; Scolyer, R.A.; et al. Combination nivolumab and ipilimumab or nivolumab alone in melanoma brain metastases: A multicentre randomised phase 2 study. Lancet Oncol. 2018, 19, 672–681. [Google Scholar] [CrossRef] [PubMed]
- Di Giacomo, A.M.; Chiarion-Sileni, V.; Del Vecchio, M.; Ferrucci, P.F.; Guida, M.; Quaglino, P.; Guidoboni, M.; Marchetti, P.; Cutaia, O.; Amato, G.; et al. Primary Analysis and 4-Year Follow-Up of the Phase III NIBIT-M2 Trial in Melanoma Patients With Brain Metastases. Clin. Cancer Res. 2021, 27, 4737–4745. [Google Scholar] [CrossRef]
- Burton, E.M.; Amaria, R.N.; Glitza, I.C.; Milton, D.R.; Diab, A.; Patel, S.P.; McQuade, J.L.; Honaker, V.; Wong, M.K.; Hwu, P.; et al. Phase II Study of TRIplet combination Nivolumab (N) with Dabrafenib (D) and Trametinib (T) (TRIDeNT) in patients (pts) with PD-1 naïve or refractory BRAFmutated metastatic melanoma (MM) with or without active brain metastases. J. Clin. Oncol. 2021, 39 (Suppl. S15), 9520. [Google Scholar] [CrossRef]
- Dummer, R.; Queirolo, P.; Guijarro, A.M.A.; Hu, Y.; Wang, D.; de Azevedo, S.J.; Robert, C.; Ascierto, P.A.; Chiarion-Sileni, V.; Pronzato, P.; et al. Atezolizumab, vemurafenib, and cobimetinib in patients with melanoma with CNS metastases (TRICOTEL): A multicentre, open-label, single-arm, phase 2 study. Lancet Oncol. 2022, 23, 1145–1155. [Google Scholar] [CrossRef]
- Borch, T.; Schmidt, H.; Bastholt, L.; Ellebæk, E.; Donia, M.; Svane, I.-M. Efficacy of immunotherapy in melanoma patients with symptomatic brain metastases treated with steroids: Initial report from the MEMBRAINS trial. Ann. Oncol. 2022, 33, S928. [Google Scholar] [CrossRef]
- Goldberg, S.B.; Gettinger, S.N.; Mahajan, A.; Chiang, A.C.; Herbst, R.S.; Sznol, M.; Tsiouris, A.J.; Cohen, J.; Vortmeyer, A.; Jilaveanu, L.; et al. Pembrolizumab for patients with melanoma or non-small-cell lung cancer and untreated brain metastases: Early analysis of a non-randomised, open-label, phase 2 trial. Lancet Oncol. 2016, 17, 976–983. [Google Scholar] [CrossRef] [PubMed]
- Di Giacomo, A.; Ascierto, P.; Queirolo, P.; Pilla, L.; Ridolfi, R.; Santinami, M.; Testori, A.; Simeone, E.; Guidoboni, M.; Maurichi, A.; et al. Three-year follow-up of advanced melanoma patients who received ipilimumab plus fotemustine in the Italian Network for Tumor Biotherapy (NIBIT)-M1 phase II study. Ann Oncol. 2015, 26, 798–803. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, K.; Stallworth, D.; Kim, Y.; Johnstone, P.S.; Harrison, L.; Caudell, J.; Yu, H.; Etame, A.; Weber, J.; Gibney, G.T. Clinical outcomes of melanoma brain metastases treated with stereotactic radiation and anti-PD-1 therapy. Ann Oncol. 2016, 27, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Williams, N.L.; Wuthrick, E.J.; Kim, H.; Palmer, J.D.; Garg, S.; Eldredge-Hindy, H.; Daskalakis, C.; Feeney, K.J.; Mastrangelo, M.J.; Kim, L.J.; et al. Phase 1 Study of Ipilimumab Combined With Whole Brain Radiation Therapy or Radiosurgery for Melanoma Patients With Brain Metastases. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Altman, and the PRISMA Group, Reprint—Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Phys. Ther. 2009, 89, 873–880. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G. Quantifying Heterogeneity in a Meta-Analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple. Graph. Test BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Begg, C.B.; Mazumdar, M. Operating Characteristics of a Rank Correlation Test for Publication Bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- Rulli, E.; Legramandi, L.; Salvati, L.; Mandala, M. The impact of targeted therapies and immunotherapy in melanoma brain metastases: A systematic review and meta-analysis. Cancer 2019, 125, 3776–3789. [Google Scholar] [CrossRef]
- Eroglu, Z.; Topcu, T.; Yu, H.; Margolin, K.A. How I treat brain metastases of melanoma. ESMO Open 2022, 7, 100598. [Google Scholar] [CrossRef]
- D’ecclesiis, O.; Caini, S.; Martinoli, C.; Raimondi, S.; Gaiaschi, C.; Tosti, G.; Queirolo, P.; Veneri, C.; Saieva, C.; Gandini, S.; et al. Gender-Dependent Specificities in Cutaneous Melanoma Predisposition, Risk Factors, Somatic Mutations, Prognostic and Predictive Factors: A Systematic Review. Int. J. Env. Res. Public Health 2021, 18, 7945. [Google Scholar] [CrossRef] [PubMed]
- Mandalà, M.; Lorigan, P.; Sergi, M.C.; Benannoune, N.; Serra, P.; Vitale, M.G.; Giannarelli, D.; Arance, A.M.; Couselo, E.M.; Neyns, B.; et al. Combined immunotherapy in melanoma patients with brain metastases: A multicenter international study. Eur. J. Cancer 2024, 199, 113542. [Google Scholar] [CrossRef] [PubMed]
- Conforti, F.; Pala, L.; Bagnardi, V.; De Pas, T.; Martinetti, M.; Viale, G.; Gelber, R.D.; Goldhirsch, A. Cancer immunotherapy efficacy and patients’ sex: A systematic review and meta-analysis. Lancet Oncol. 2018, 19, 737–746. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).