
A Single-Leg Vertical Hop Test Is an Effective Tool to Measure Functional Performance after Anterior Cruciate Ligament (ACL) Reconstruction

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Population
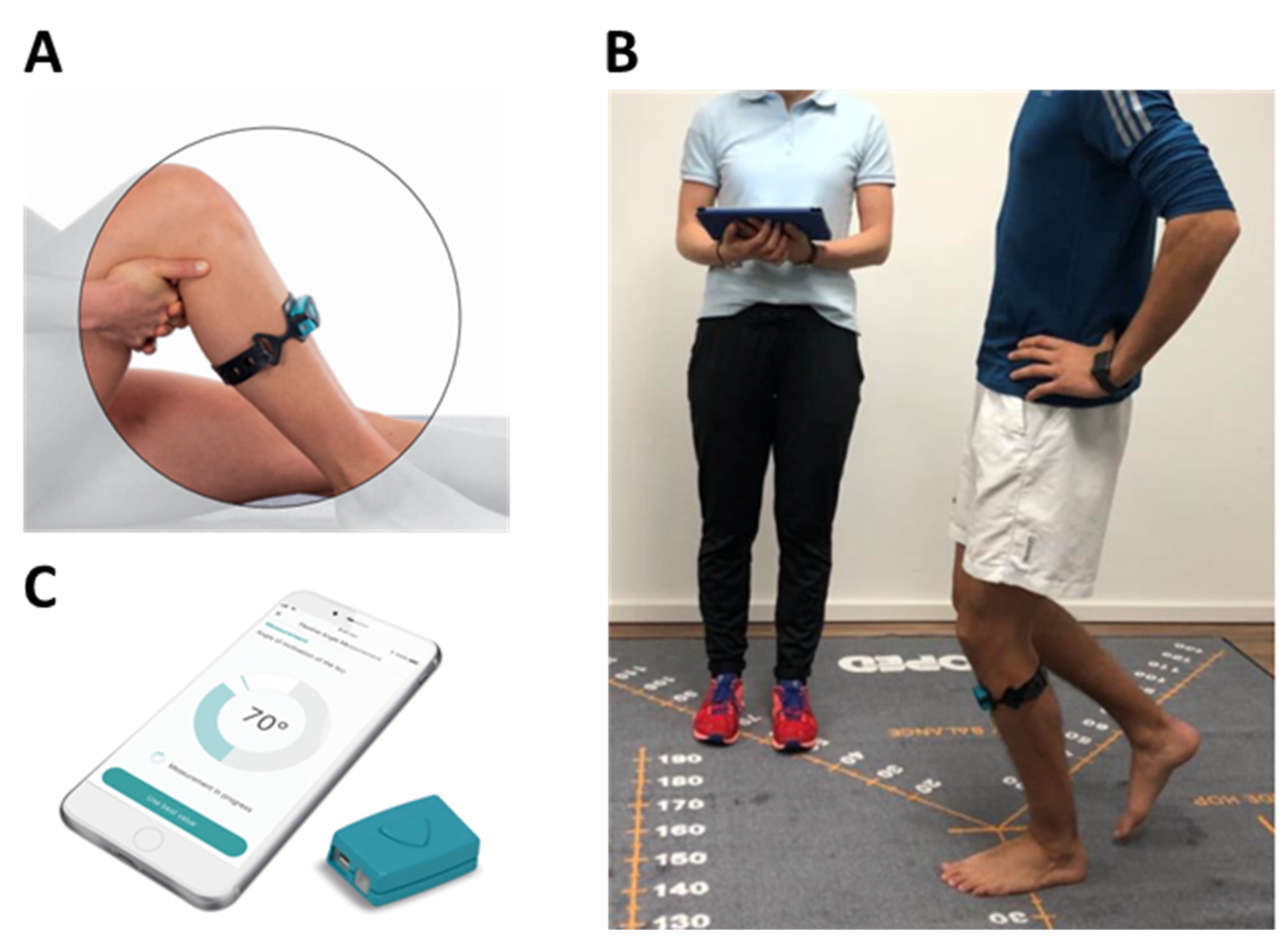
2.2. Assessment of Single-Leg Vertical Hop Test with Sensor-Based Digital Medical Device
2.3. Assessment of Distance Hop, IKDC SKF and KOOS
2.4. Statistical Methods
3. Results
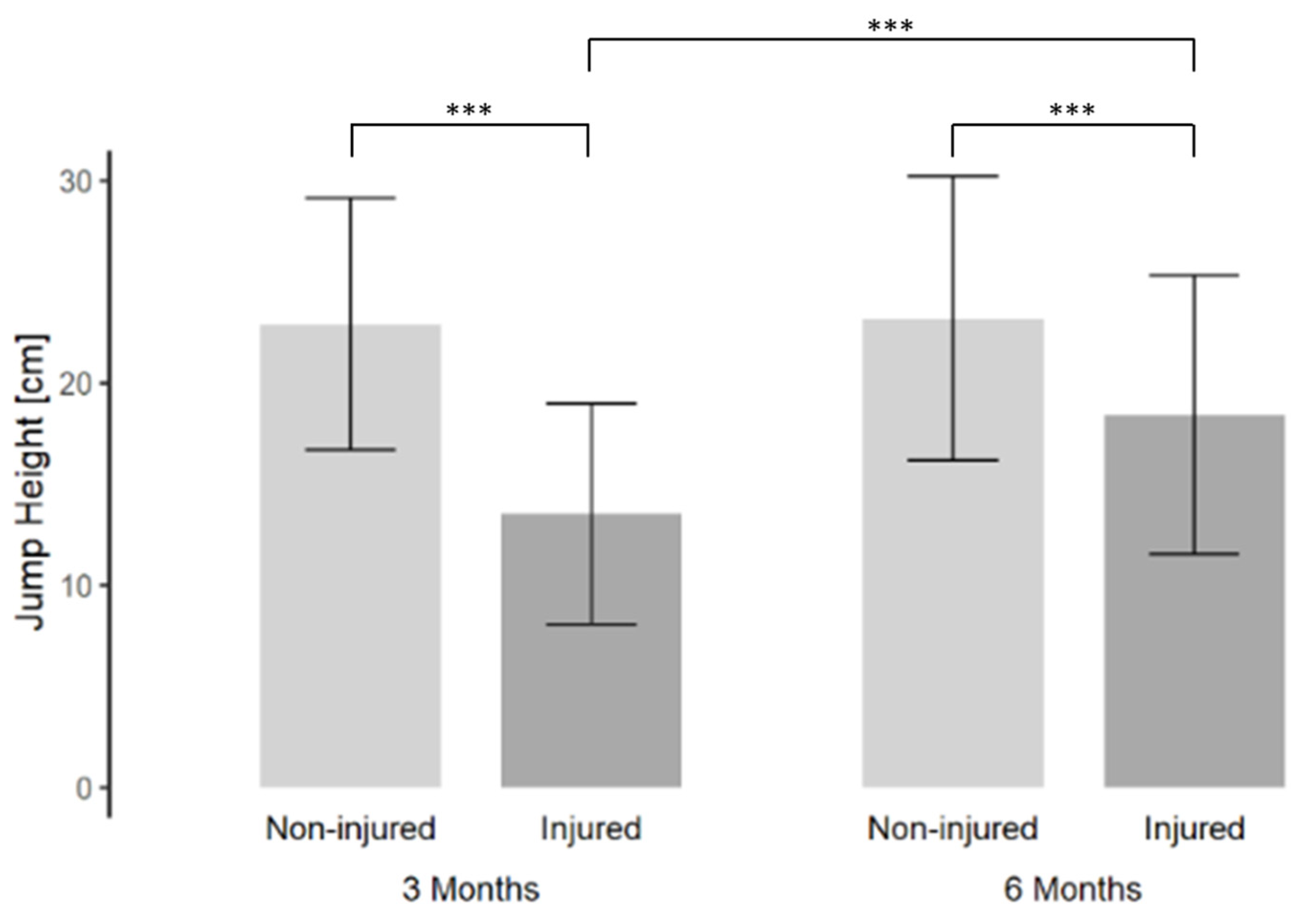
3.1. Single-Leg Vertical Hop Test
3.2. Differences in Jump Heights in the Single-Leg Vertical Hop According to Age, Gender and Injury Severity
3.3. Correlations and Regression Analysis
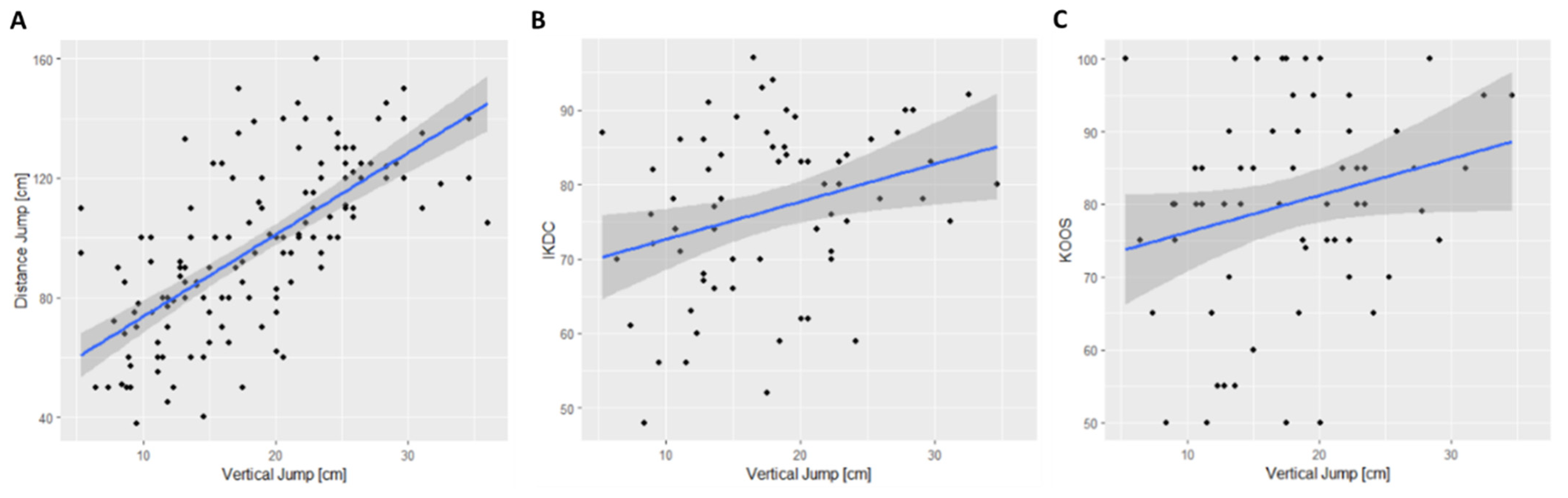
3.4. Correlation of Jump Height in SLVHT with Distance Hop, IKDC SKF and KOOS
4. Discussion
4.1. Limitations
4.2. Clinical Implications
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mehl, J.; Diermeier, T.; Herbst, E.; Imhoff, A.B.; Stoffels, T.; Zantop, T.; Petersen, W.; Achtnich, A. Evidence-based concepts for prevention of knee and ACL injuries. 2017 guidelines of the ligament committee of the German Knee Society (DKG). Arch. Orthop. Trauma Surg. 2018, 138, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Boden, B.P.; Griffin, L.Y.; Garrett, W.E., Jr. Etiology and Prevention of Noncontact ACL Injury. Phys. Sportsmed. 2000, 28, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Vereijken, A.; Aerts, I.; Jetten, J.; Tassignon, B.; Verschueren, J.; Meeusen, R.; van Trijffel, E. Association between Functional Performance and Return to Performance in High-Impact Sports after Lower Extremity Injury: A Systematic Review. J. Sports Sci. Med. 2020, 19, 564–576. [Google Scholar]
- Achtnich, A.; Akoto, R.; Petersen, W. Handlungsalgorithmus: Wiederkehr zum Sport nach Rekonstruktion des vorderen Kreuzbandes. Knie J. 2019, 1, 66–67. [Google Scholar] [CrossRef]
- Grindem, H.; Snyder-Mackler, L.; Moksnes, H.; Engebretsen, L.; Risberg, M.A. Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: The Delaware-Oslo ACL cohort study. Br. J. Sports Med. 2016, 50, 804–808. [Google Scholar] [CrossRef] [PubMed]
- Joreitz, R.; Lynch, A.; Popchak, A.; Irrgang, J. Criterion-Based Rehabilitation Program with Return to Sport Testing Following Acl Reconstruction: A Case Series. Int. J. Sports Phys. Ther. 2020, 15, 1151–1173. [Google Scholar] [CrossRef] [PubMed]
- Kyritsis, P.; Bahr, R.; Landreau, P.; Miladi, R.; Witvrouw, E. Likelihood of ACL graft rupture: Not meeting six clinical discharge criteria before return to sport is associated with a four times greater risk of rupture. Br. J. Sports Med. 2016, 50, 946–951. [Google Scholar] [CrossRef] [PubMed]
- Piussi, R.; Beischer, S.; Thomeé, R.; Hamrin Senorski, E. Hop tests and psychological PROs provide a demanding and clinician-friendly RTS assessment of patients after ACL reconstruction, a registry study. BMC Sports Sci. Med. Rehabil. 2020, 12, 32. [Google Scholar] [CrossRef]
- Petersen, W.; Diermeier, T.; Mehl, J.; Stöhr, A.; Ellermann, A.; Müller, P.; Höher, J.; Herbort, M.; Akoto, R.; Zantop, T.; et al. Prevention of knee and ACL injuries—Guidelines of the ligament commitee of the DKG (German Knee Society). OUP 2016, 10, 542–550. [Google Scholar]
- Kotsifaki, R.; Korakakis, V.; King, E.; Barbosa, O.; Maree, D.; Pantouveris, M.; Bjerregaard, A.; Luomajoki, J.; Wilhelmsen, J.; Whiteley, R. Aspetar clinical practice guideline on rehabilitation after anterior cruciate ligament reconstruction. Br. J. Sports Med. 2023, 57, 500–514. [Google Scholar] [CrossRef]
- Gustavsson, A.; Neeter, C.; Thomeé, P.; Silbernagel, K.G.; Augustsson, J.; Thomeé, R.; Karlsson, J. A test battery for evaluating hop performance in patients with an ACL injury and patients who have undergone ACL reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2006, 14, 778–788. [Google Scholar] [CrossRef] [PubMed]
- Webster, K.E.; Hewett, T.E. What is the Evidence for and Validity of Return-to-Sport Testing after Anterior Cruciate Ligament Reconstruction Surgery? A Systematic Review and Meta-Analysis. Sports Med. 2019, 49, 917–929. [Google Scholar] [CrossRef]
- Hefti, F.; Muller, W.; Jakob, R.P.; Staubli, H.U. Evaluation of knee ligament injuries with the IKDC form. Knee Surg. Sports Traumatol. Arthrosc. 1993, 1, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Irrgang, J.J.; Anderson, A.F.; Boland, A.L.; Harner, C.D.; Kurosaka, M.; Neyret, P.; Richmond, J.C.; Shelborne, K.D. Development and validation of the international knee documentation committee subjective knee form. Am. J. Sports Med. 2001, 29, 600–613. [Google Scholar] [CrossRef] [PubMed]
- Ardern, C.L.; Taylor, N.F.; Feller, J.A.; Webster, K.E. Fifty-five per cent return to competitive sport following anterior cruciate ligament reconstruction surgery: An updated systematic review and meta-analysis including aspects of physical functioning and contextual factors. Br. J. Sports Med. 2014, 48, 1543–1552. [Google Scholar] [CrossRef] [PubMed]
- van Melick, N.; van Cingel, R.E.; Brooijmans, F.; Neeter, C.; van Tienen, T.; Hullegie, W.; Nijhuis-van der Sanden, M.W. Evidence-based clinical practice update: Practice guidelines for anterior cruciate ligament rehabilitation based on a systematic review and multidisciplinary consensus. Br. J. Sports Med. 2016, 50, 1506–1515. [Google Scholar] [CrossRef] [PubMed]
- Kotsifaki, A.; Van Rossom, S.; Whiteley, R.; Korakakis, V.; Bahr, R.; Sideris, V.; Jonkers, I. Single leg vertical jump performance identifies knee function deficits at return to sport after ACL reconstruction in male athletes. Br. J. Sports Med. 2022, 56, 490–498. [Google Scholar] [CrossRef] [PubMed]
- Hegedus, E.J.; McDonough, S.; Bleakley, C.; Cook, C.E.; Baxter, G.D. Clinician-friendly lower extremity physical performance measures in athletes: A systematic review of measurement properties and correlation with injury, part 1. The tests for knee function including the hop tests. Br. J. Sports Med. 2015, 49, 642–648. [Google Scholar] [CrossRef] [PubMed]
- Scinicarelli, G.; Offerhaus, C.; Feodoroff, B.; Froboese, I.; Wilke, C. Functional performance and interlimb asymmetries of young football players during single-leg jump tests. Ger. J. Exerc. Sport Res. 2022, 52, 76–86. [Google Scholar] [CrossRef]
- Pueo, B.; Penichet-Tomas, A.; Jimenez-Olmedo, J.M. Reliability and validity of the Chronojump open-source jump mat system. Biol. Sport 2020, 37, 255–259. [Google Scholar] [CrossRef]
- Small, S.R.; Bullock, G.S.; Khalid, S.; Barker, K.; Trivella, M.; Price, A.J. Current clinical utilisation of wearable motion sensors for the assessment of outcome following knee arthroplasty: A scoping review. BMJ Open 2019, 9, e033832. [Google Scholar] [CrossRef] [PubMed]
- Prill, R.; Walter, M.; Królikowska, A.; Becker, R. A Systematic Review of Diagnostic Accuracy and Clinical Applications of Wearable Movement Sensors for Knee Joint Rehabilitation. Sensors 2021, 21, 8221. [Google Scholar] [CrossRef] [PubMed]
- Dowling, A.V.; Favre, J.; Andriacchi, T.P. A wearable system to assess risk for anterior cruciate ligament injury during jump landing: Measurements of temporal events, jump height, and sagittal plane kinematics. J. Biomech. Eng. 2011, 133, 071008. [Google Scholar] [CrossRef] [PubMed]
- Haladjian, J.; Scheuermann, C.; Bredies, K.; Bruegge, B. A smart textile sleeve for rehabilitation of knee injuries. In Proceedings of the 2017 ACM International Joint Conference on Pervasive and Ubiquitous Computing and 2017 ACM International Symposium on Wearable Computers, Maui, HI, USA, 11–15 September 2017; Association for Computing Machinery: New York, NY, USA, 2017; pp. 49–52. [Google Scholar]
- Haladjian, J.; Hodaie, Z.; Xu, H.; Yigin, M.; Bruegge, B.; Fink, M.; Hoeher, J. KneeHapp: A bandage for rehabilitation of knee injuries. In Proceedings of the 2015 ACM International Joint Conference on Pervasive and Ubiquitous Computing and 2015 ACM International Symposium on Wearable Computers, Osaka, Japan, 7–11 September 2015; Association for Computing Machinery: New York, NY, USA, 2015; pp. 181–184. [Google Scholar]
- Mitternacht, J.; Hermann, A.; Carqueville, P. Acquisition of Lower-Limb Motion Characteristics with a Single Inertial Measurement Unit-Validation for Use in Physiotherapy. Diagnostics 2022, 12, 1640. [Google Scholar] [CrossRef] [PubMed]
- Mengis, N.; Schmidt, S.; Ellermann, A.; Sobau, C.; Egloff, C.; Kreher, M.M.; Ksoll, K.; Schmidt-Lucke, C.; Rippke, J.N. A Novel Sensor-Based Application for Home-Based Rehabilitation Can Objectively Measure Postoperative Outcomes following Anterior Cruciate Ligament Reconstruction. J. Pers. Med. 2023, 13, 1398. [Google Scholar] [CrossRef] [PubMed]
- Hopper, D.M.; Goh, S.C.; Wentworth, L.A.; Chan, D.Y.K.; Chau, J.H.W.; Wootton, G.J.; Strauss, G.R.; Boyle, J.J.W. Test–retest reliability of knee rating scales and functional hop tests one year following anterior cruciate ligament reconstruction. Phys. Ther. Sport 2002, 3, 10–18. [Google Scholar] [CrossRef]
- Harman, E.A.; Rosenstein, M.T.; Frykman, P.N.; Rosenstein, R.M. The effects of arms and countermovement on vertical jumping. Med. Sci. Sports Exerc. 1990, 22, 825–833. [Google Scholar] [CrossRef] [PubMed]
- Roos, E.M.; Lohmander, L.S. The Knee injury and Osteoarthritis Outcome Score (KOOS): From joint injury to osteoarthritis. Health Qual. Life Outcomes 2003, 1, 64. [Google Scholar] [CrossRef] [PubMed]
- Kessler, S.; Lang, S.; Puhl, W.; Stöve, J. The Knee Injury and Osteoarthritis Outcome Score—A multifunctional questionnaire to measure outcome in knee arthroplasty. Z. Orthop. Ihre Grenzgeb. 2003, 141, 277–282. [Google Scholar] [CrossRef]
- Zarro, M.J.; Stitzlein, M.G.; Lee, J.S.; Rowland, R.W.; Gray, V.L.; Taylor, J.B.; Meredith, S.J.; Packer, J.D.; Nelson, C.M. Single-Leg Vertical Hop Test Detects Greater Limb Asymmetries Than Horizontal Hop Tests After Anterior Cruciate Ligament Reconstruction in NCAA Division 1 Collegiate Athletes. Int. J. Sports Phys. Ther. 2021, 16, 1405–1414. [Google Scholar] [CrossRef]
- Petersen, W.; Guenther, D.; Imhoff, A.B.; Herbort, M.; Stein, T.; Schoepp, C.; Akoto, R.; Höher, J.; Scheffler, S.; Stoehr, A.; et al. Management after acute rupture of the anterior cruciate ligament (ACL). Part 1: ACL reconstruction has a protective effect on secondary meniscus and cartilage lesions. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 1665–1674. [Google Scholar] [CrossRef]
- Petersen, W.; Häner, M.; Guenther, D.; Lutz, P.; Imhoff, A.; Herbort, M.; Stein, T.; Schoepp, C.; Akoto, R.; Höher, J.; et al. Management after acute injury of the anterior cruciate ligament (ACL), part 2: Management of the ACL-injured patient. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 1675–1689. [Google Scholar] [CrossRef] [PubMed]
- Karaszewski, W. Neue Optionen der Objektivierbaren Verlaufsbeobachtung als Basis für Individualisierte Therapieentscheidungen Während der Rehabilitation nach Vorderer Kreuzbandruptur/New Options of Objectifiable Follow-Up as a Basis for Individualised Therapy Decisions during Rehabilitation after Anterior Cruciate Ligament Rupture. Ph.D. Thesis, Charité–Universitätsmedizin Berlin, Berlin, Germany, 2024. [Google Scholar]
- Taylor, J.B.; Westbrook, A.E.; Head, P.L.; Glover, K.M.; Paquette, M.R.; Ford, K.R. The single-leg vertical hop provides unique asymmetry information in individuals after anterior cruciate ligament reconstruction. Clin. Biomech. 2020, 80, 105107. [Google Scholar] [CrossRef] [PubMed]
- Oberländer, K.D.; Brüggemann, G.P.; Höher, J.; Karamanidis, K. Altered landing mechanics in ACL-reconstructed patients. Med. Sci. Sports Exerc. 2013, 45, 506–513. [Google Scholar] [CrossRef]
- Höher, J.; Lischke, B.; Petersen, W.; Mengis, N.; Niederer, D.; Stein, T.; Stoffels, T.; Prill, R.; Schmidt-Lucke, C. Sensor-based telerehabilitation system increases patient adherence after knee surgery. PLOS Digit. Health 2023, 2, e0000175. [Google Scholar] [CrossRef] [PubMed]
- Haladjian, J.; Bredies, K.; Brügge, B. KneeHapp textile: A smart textile system for rehabilitation of knee injuries. In Proceedings of the 2018 IEEE 15th International Conference on Wearable and Implantable Body Sensor Networks (BSN), Las Vegas, NV, USA, 4–7 March 2018; pp. 9–12. [Google Scholar] [CrossRef]
- Glattke, K.E.; Tummala, S.V.; Chhabra, A. Anterior Cruciate Ligament Reconstruction Recovery and Rehabilitation: A Systematic Review. J. Bone Jt. Surg. Am. 2022, 104, 739–754. [Google Scholar] [CrossRef]
- Fischer, F.; Blank, C.; Dunnwald, T.; Gfoller, P.; Herbst, E.; Hoser, C.; Fink, C. Isokinetic Extension Strength Is Associated with Single-Leg Vertical Jump Height. Orthop. J. Sports Med. 2017, 5, 2325967117736766. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Study Population |
|---|---|
| Total [n] | 143 |
| Gender (male/female [n (%)]) | 94:49 (66%:34%) |
| Age [years] | 26.6 (8.9) |
| Height [cm] | 177.4 (8.3) |
| Weight [kg] | 76.8 (13.7) |
| BMI [kg/m2] | 24.3 (3.3) |
| Injury due to the main sport practiced [n (%)] | |
| Soccer | 66 (46%) |
| Handball | 22 (15%) |
| Other ball sports | 16 (11%) |
| Tennis | 6 (4%) |
| Winter sports | 8 (6%) |
| Other sports | 5 (4%) |
| No sports-related injury | 20 (14%) |
| Injured leg [n (%)] | |
| Right | 65 (45%) |
| Left | 78 (55%) |
| Diagnosis [n (%)] | |
| ACL-R isolated | 59 (41%) |
| ACL-R with meniscus involvement | 84 (59%) |
| Jump Height 3 Months Postoperatively | Jump Height 6 Months Postoperatively | Change in Jump Height (3 to 6 Months) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | Non-Injured Leg [cm] | Injured Leg [cm] | LSI [%] | Non-Injured Leg [cm] | Injured Leg [cm] | LSI [%] | Non-Injured Leg Absolute [cm] (Relative [%]) | Injured Leg Absolute [cm] (Relative [%]) | ||
| Total | 143 | 22.9 (6.2) | 13.5 (5.5) | 59.6 (17.7) | 23.2 (7.0) | 18.4 (6.9) a | 79.6 (17.7) a | 0.3 (2.7%) | 4.9 (44.1%) | |
| Gender | male | 94 | 25.7 (4.8) # | 15.2 (5.4) # | 59.6 (17.5) | 26.4 (5.6) # | 21.1 (6.3) #,a | 80.6 (18.5) a | 0.7 (3.5%) | 5.9 (47.8%) |
| female | 49 | 17.5 (5.0) # | 10.2 (3.8) # | 59.5 (18.0) | 17.1 (5.0) # | 13.3 (4.9) #,a | 77.8 (16.0) a | −0.5 (−1.0%) | 3.1 (36.8%) | |
| Age group | <30 years | 106 | 23.7 (6.2) § | 14.3 (5.5) § | 61.0 (18.0) | 24.0 (7.1) § | 19.5 (6.9) § | 81.0 (17.4) a | 0.3 (3.0%) | 5.2 (44.2%) |
| >30 years | 37 | 20.7 (5.7) § | 11.4 (4.9) § | 55.4 (15.9) | 20.9 (6.2) § | 15.5 (6.0) § | 75.6 (18.0) a | 0.2 (1.8%) | 4.1 (43.5%) | |
| Injury severity | ACL-R isolated | 59 | 22.3 (6.2) | 13.3 (5.5) | 59.6 (17.0) | 22.1 (6.8) | 17.8 (6.9) | 79.8 (17.1) | −0.2 (−0.4%) | 4.5 (41.3%) |
| ACL-R with meniscus involvement | 84 | 23.4 (6.2) | 13.7 (5.4) | 59.6 (18.1) | 24.0 (7.1) | 18.9 (6.9) | 79.5 (18.2) | 0.6 (4.3%) | 5.2 (46.0%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Höher, J.; Ostner, I.; Schraplau, A.; Sprenger, N.; Allers, U.; Sulprizio, H.; Düsing, A.; Fink, M.; Schmidt-Lucke, C.; Tenfelde, O. A Single-Leg Vertical Hop Test Is an Effective Tool to Measure Functional Performance after Anterior Cruciate Ligament (ACL) Reconstruction. Appl. Sci. 2024, 14, 3143. https://doi.org/10.3390/app14083143
Höher J, Ostner I, Schraplau A, Sprenger N, Allers U, Sulprizio H, Düsing A, Fink M, Schmidt-Lucke C, Tenfelde O. A Single-Leg Vertical Hop Test Is an Effective Tool to Measure Functional Performance after Anterior Cruciate Ligament (ACL) Reconstruction. Applied Sciences. 2024; 14(8):3143. https://doi.org/10.3390/app14083143
Chicago/Turabian StyleHöher, Jürgen, Isabella Ostner, Anne Schraplau, Nina Sprenger, Ulrike Allers, Helen Sulprizio, Arndt Düsing, Markus Fink, Caroline Schmidt-Lucke, and Oliver Tenfelde. 2024. "A Single-Leg Vertical Hop Test Is an Effective Tool to Measure Functional Performance after Anterior Cruciate Ligament (ACL) Reconstruction" Applied Sciences 14, no. 8: 3143. https://doi.org/10.3390/app14083143
APA StyleHöher, J., Ostner, I., Schraplau, A., Sprenger, N., Allers, U., Sulprizio, H., Düsing, A., Fink, M., Schmidt-Lucke, C., & Tenfelde, O. (2024). A Single-Leg Vertical Hop Test Is an Effective Tool to Measure Functional Performance after Anterior Cruciate Ligament (ACL) Reconstruction. Applied Sciences, 14(8), 3143. https://doi.org/10.3390/app14083143