
The Efficacy of Utilizing Platelet-Rich Fibrin for Managing Periodontal Intrabony Defects in Conjunction with Graft Material: A Systematic Review and Meta-Analysis



Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Sources of Information and Search Methodology
2.4. Assessment of the Risk of Bias
2.5. Missing Data Imputation
2.6. Synthesis and Analysis of Data
3. Results
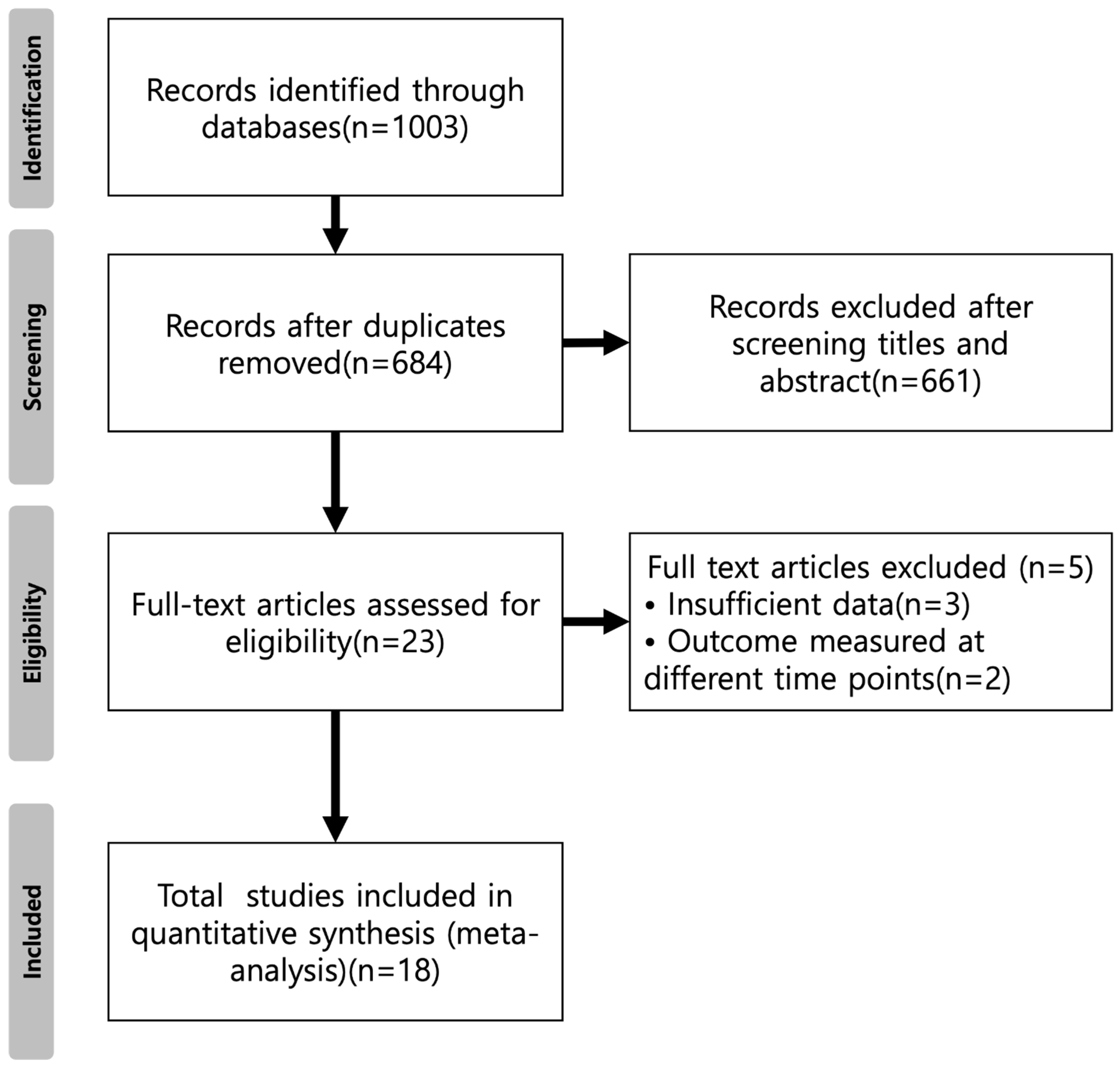
3.1. Study Selection
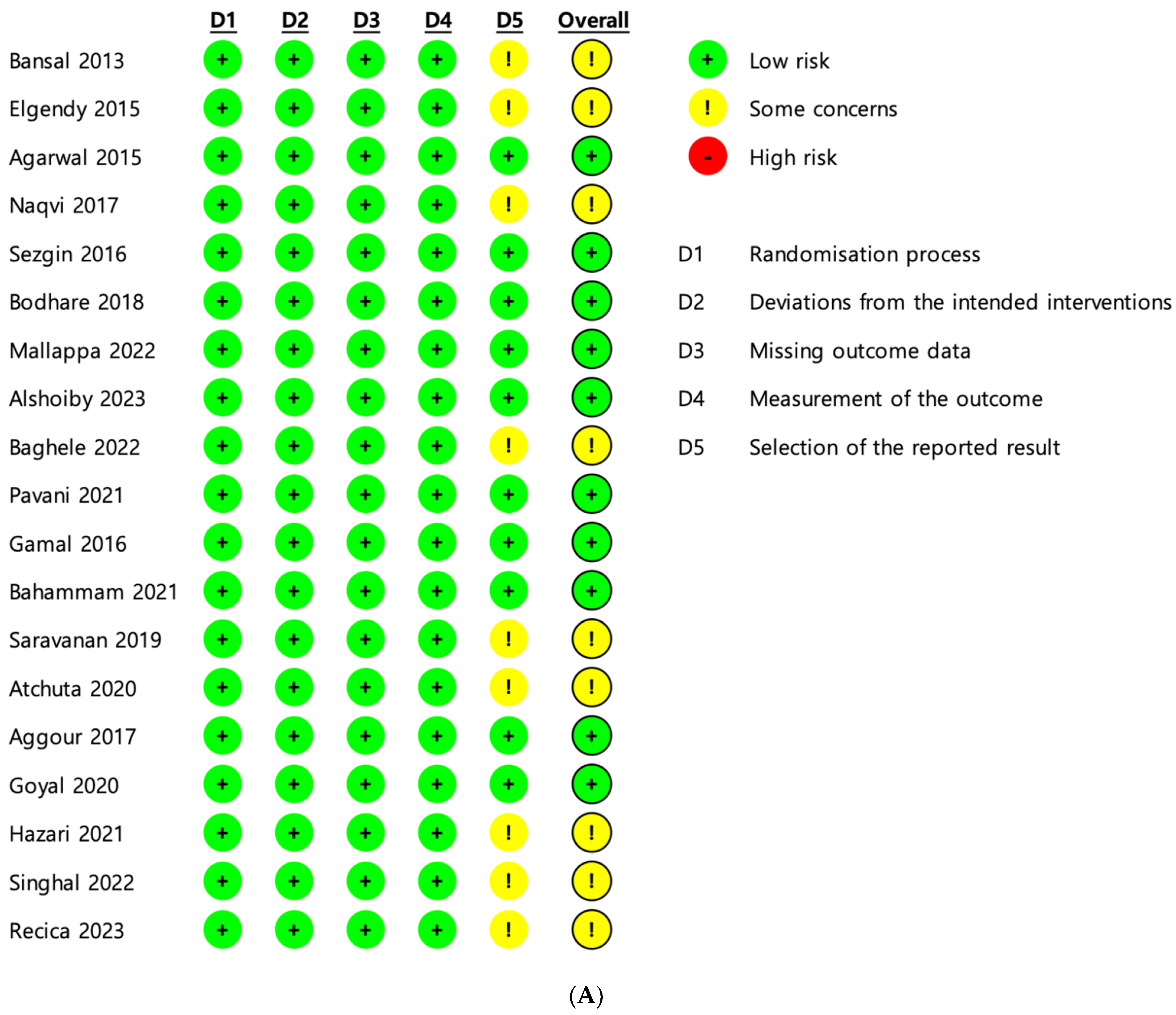
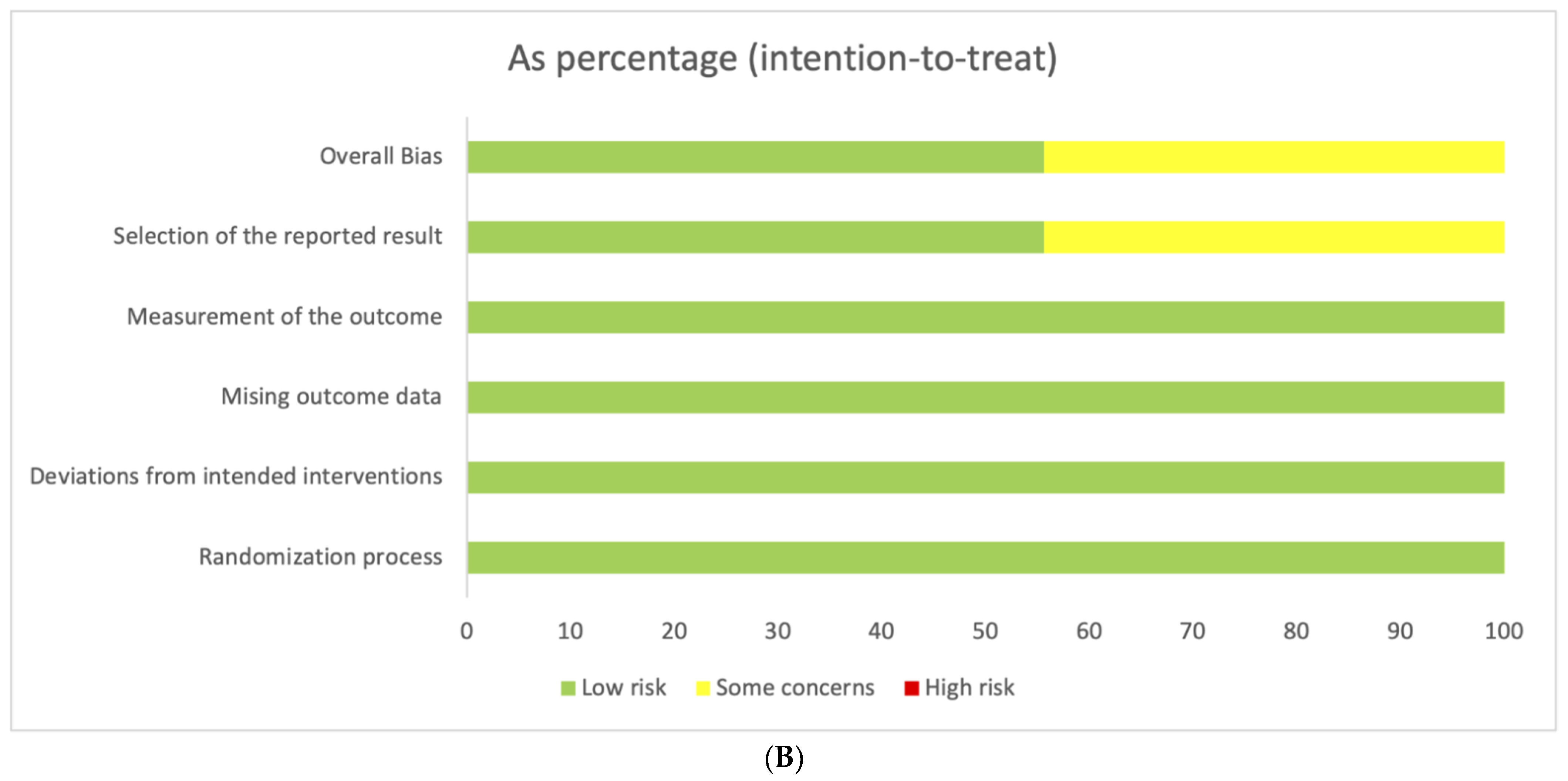
3.2. Risk of Bias
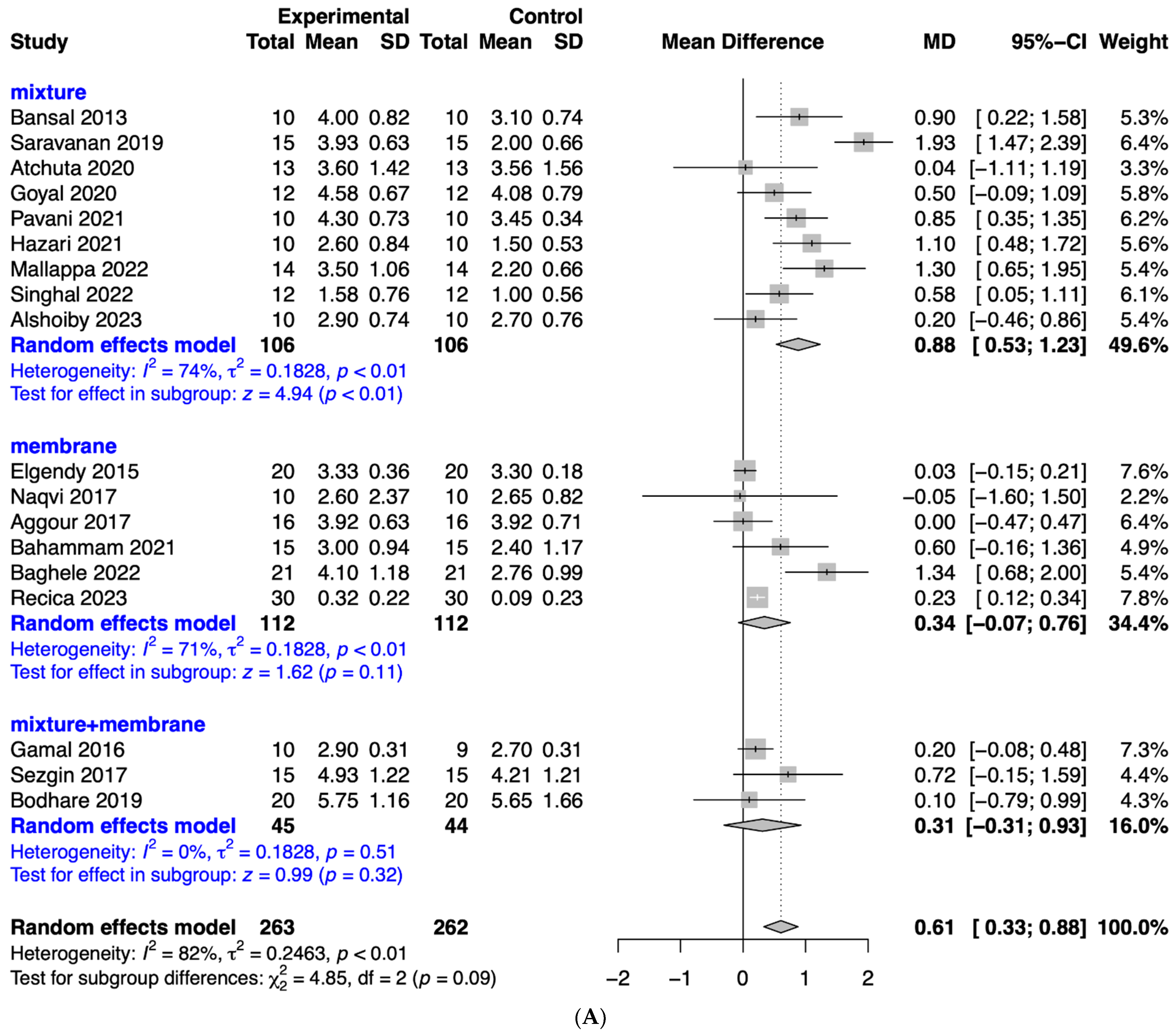
3.3. Meta-Analysis
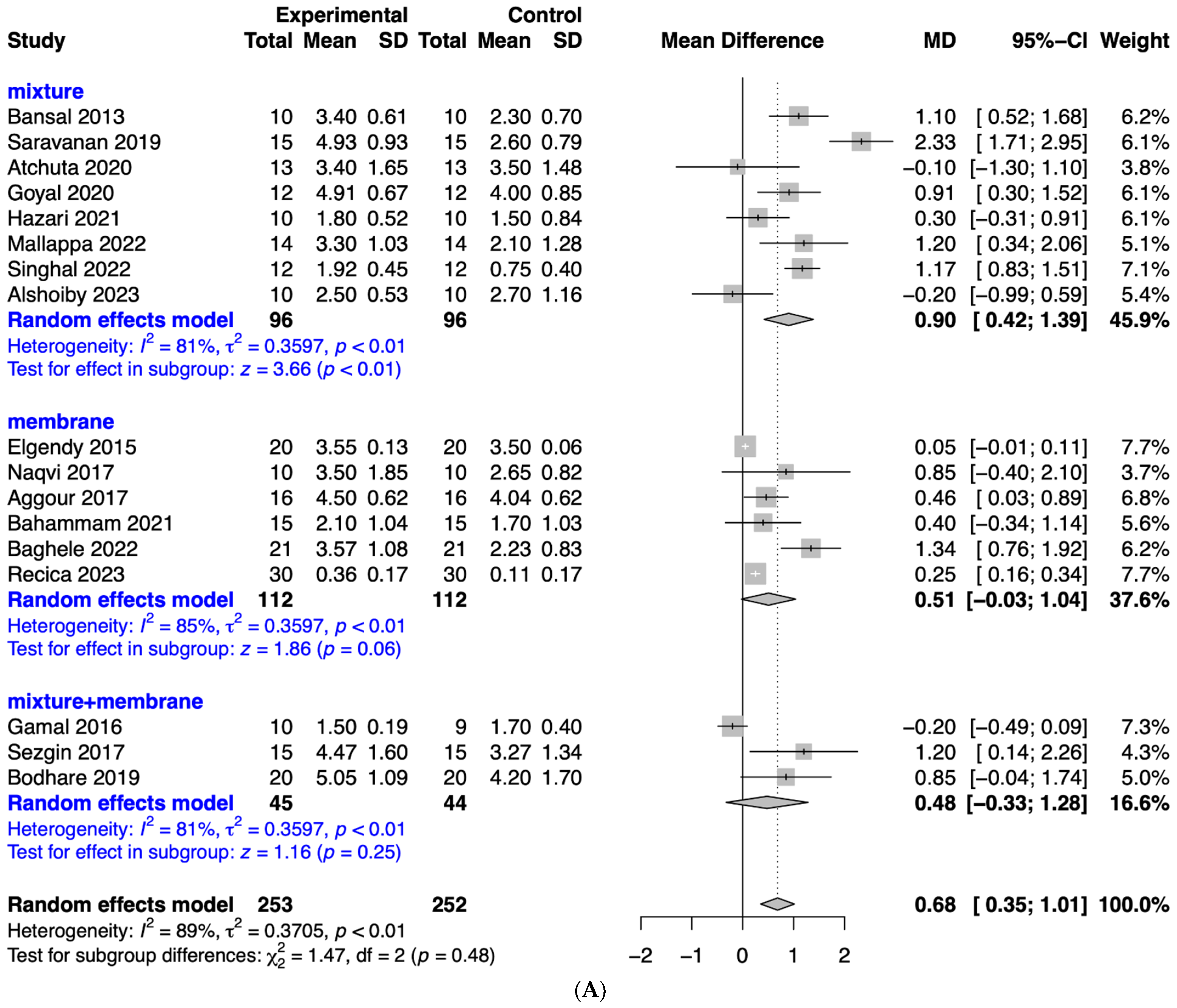
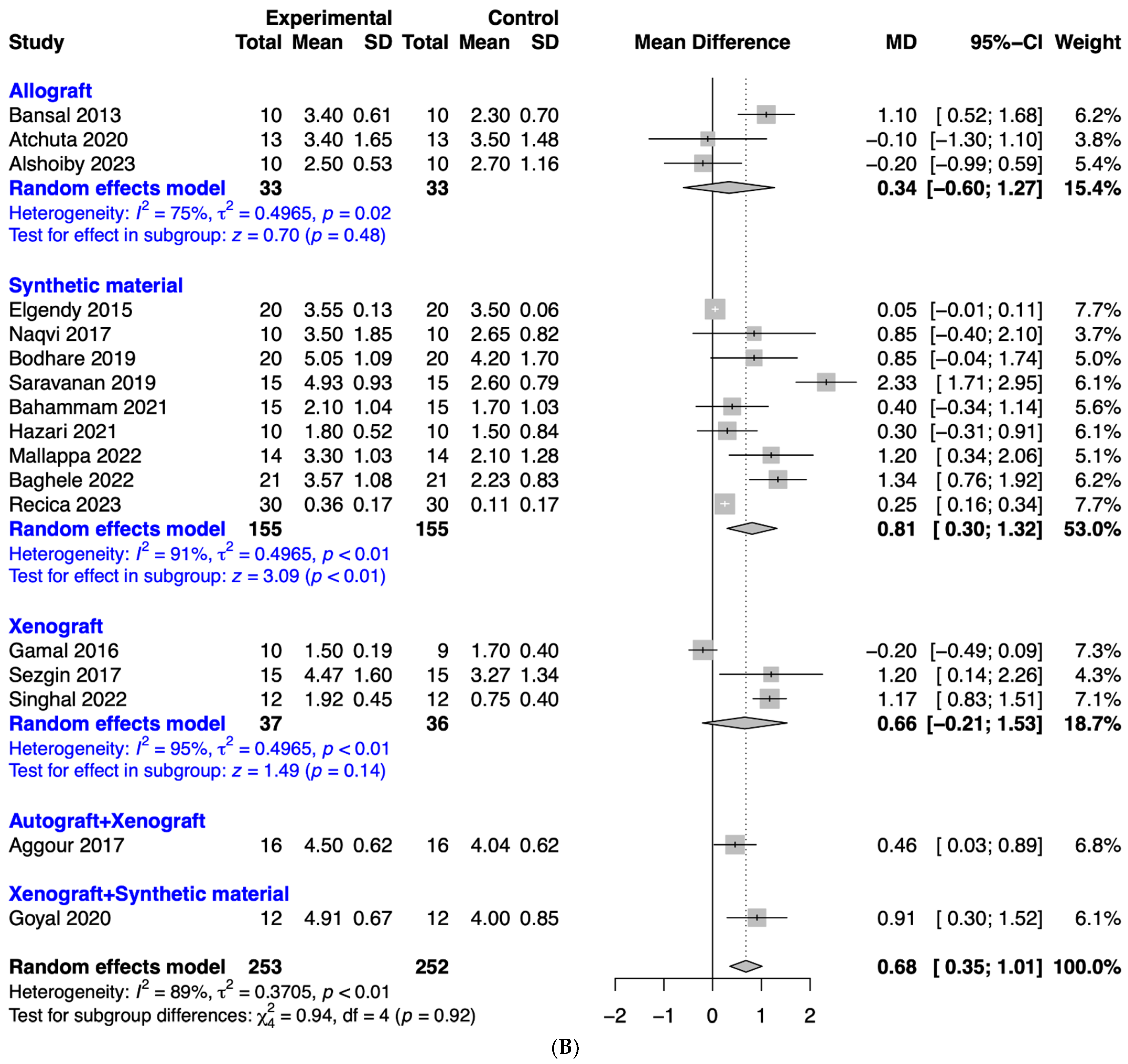
3.4. Evaluation of the Effects of Platelet-Rich Fibrin on Periodontal Probing Depth
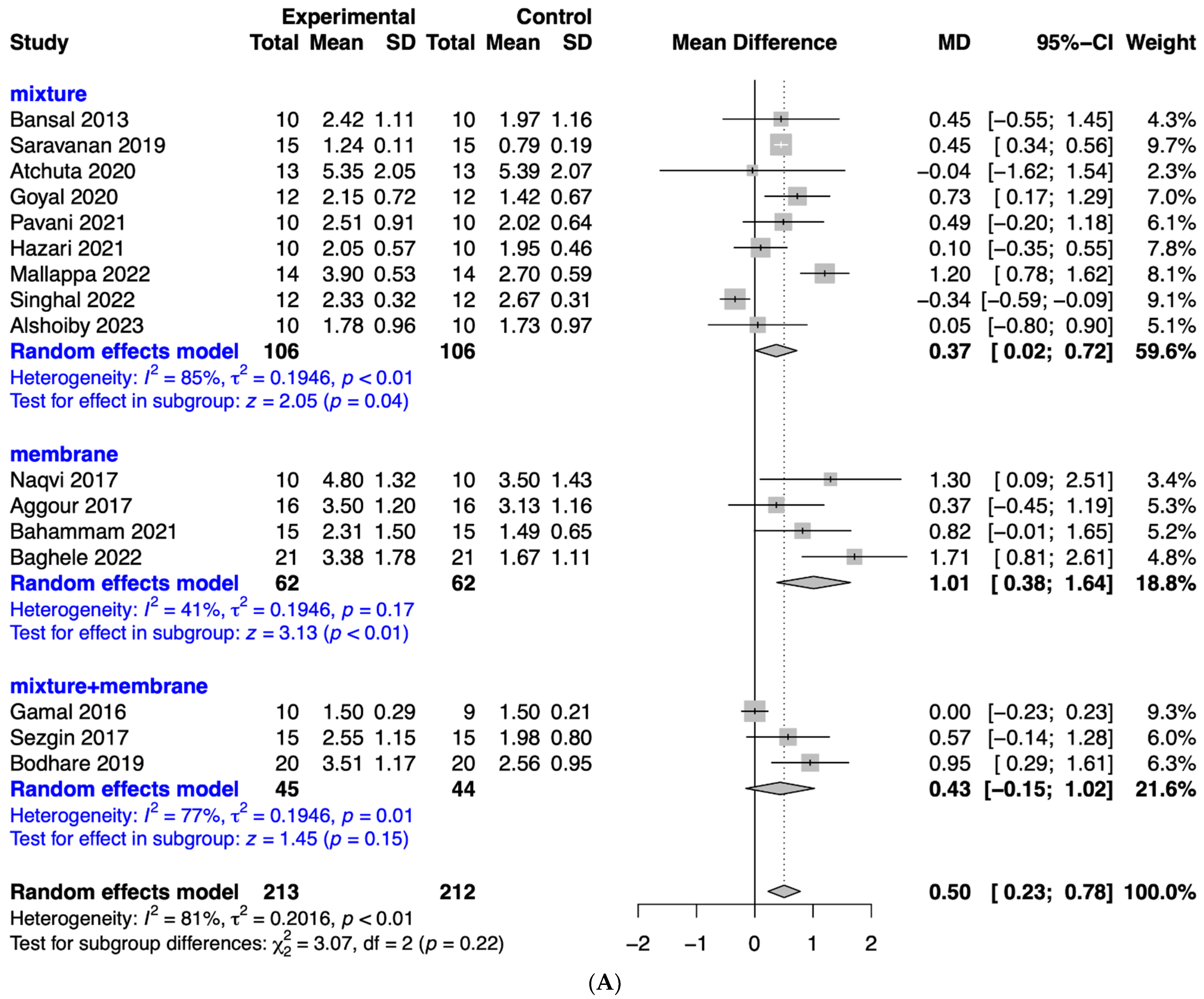
3.5. Analysis of the Effects of Platelet-Rich Fibrin on Clinical Attachment Level
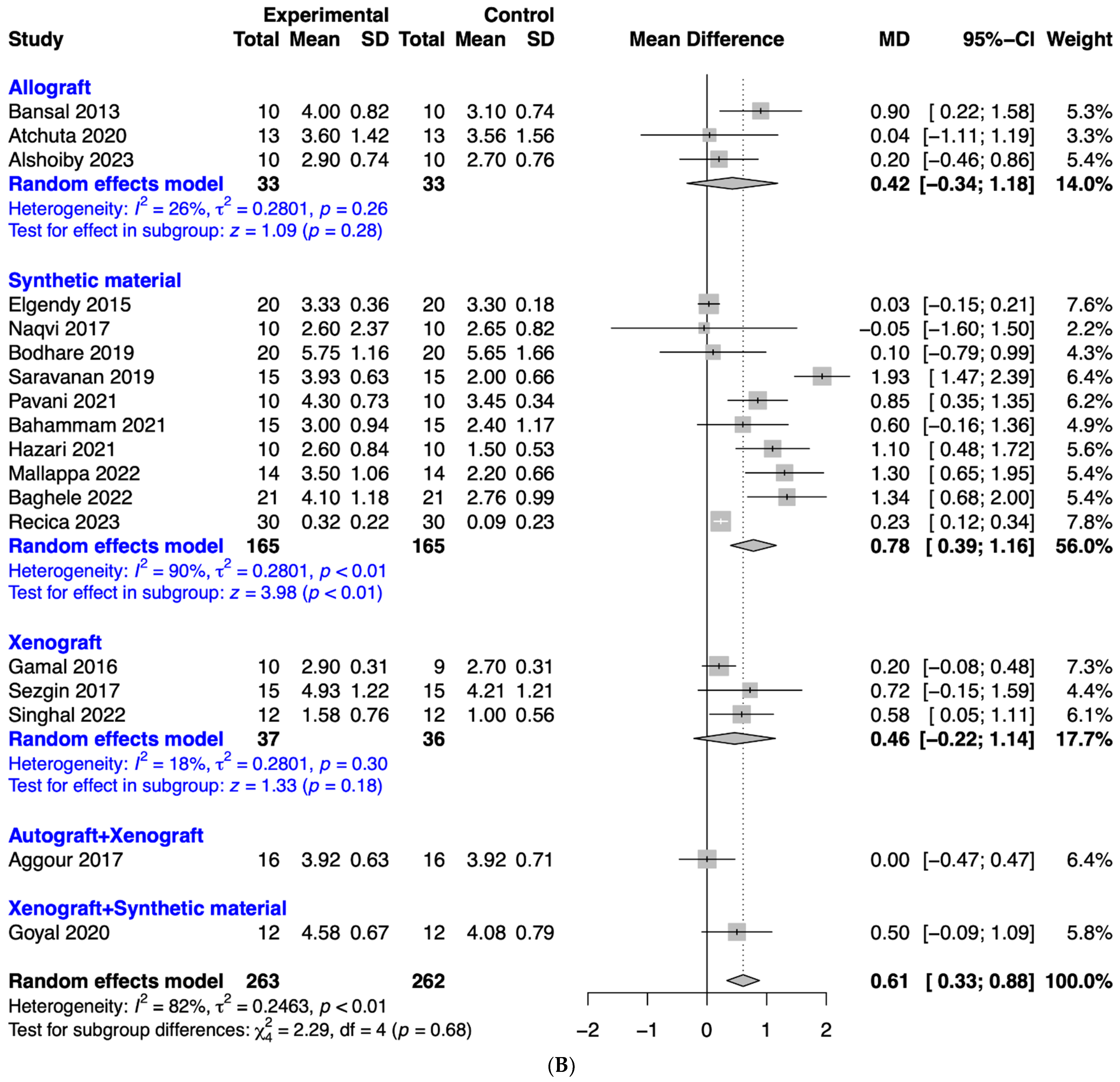
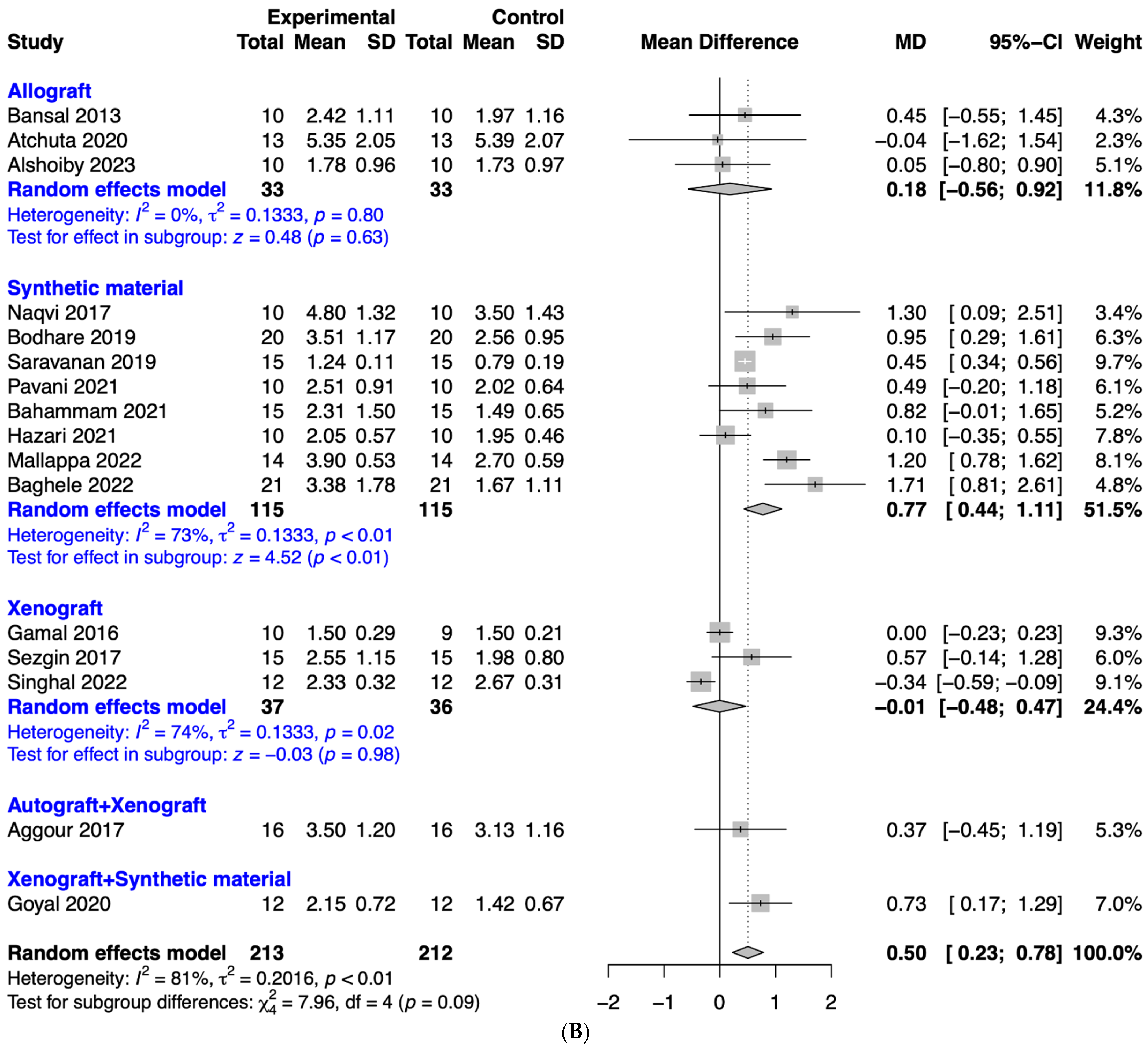
3.6. Evaluation of the Effects of Platelet-Rich Fibrin on Bone Fill
4. Discussion
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Egierska, D.; Perszke, M.; Mazur, M.; Duś-Ilnicka, I. Platelet-rich plasma and platelet-rich fibrin in oral surgery: A narrative review. Dent. Med. Probl. 2023, 60, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Pavlovic, V.; Ciric, M.; Jovanovic, V.; Trandafilovic, M.; Stojanovic, P. Platelet-rich fibrin: Basics of biological actions and protocol modifications. Open Med. 2021, 16, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Narayanaswamy, R.; Patro, B.P.; Jeyaraman, N.; Gangadaran, P.; Rajendran, R.L.; Nallakumarasamy, A.; Jeyaraman, M.; Ramani, P.; Ahn, B.C. Evolution and Clinical Advances of Platelet-Rich Fibrin in Musculoskeletal Regeneration. Bioengineering 2023, 10, 58. [Google Scholar] [CrossRef] [PubMed]
- Miron, R.J.; Fujioka-Kobayashi, M.; Sculean, A.; Zhang, Y. Optimization of platelet-rich fibrin. Periodontol. 2000, 2023; early view. [Google Scholar] [CrossRef]
- Mourão, C.F.; Lowenstein, A.; Mello-Machado, R.C.; Ghanaati, S.; Pinto, N.; Kawase, T.; Alves, G.G.; Messora, M.R. Standardization of Animal Models and Techniques for Platelet-Rich Fibrin Production: A Narrative Review and Guideline. Bioengineering 2023, 10, 482. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, A.A. Platelet rich fibrin is not a barrier membrane! Or is it? World J. Clin. Cases 2023, 11, 2396–2404. [Google Scholar] [CrossRef] [PubMed]
- Ye, L.; Mashrah, M.A.; Ge, L.; Fang, Y.; Guo, X.; Ge, Q.; Wang, L. Network meta-analysis of platelet-rich fibrin in periodontal intrabony defects. J. Oral. Pathol. Med. Off. Publ. Int. Assoc. Oral. Pathol. Am. Acad. Oral. Pathol. 2023, 52, 206–215. [Google Scholar] [CrossRef] [PubMed]
- Alrayyes, Y.; Al-Jasser, R. Regenerative Potential of Platelet Rich Fibrin (PRF) in Socket Preservation in Comparison with Conventional Treatment Modalities: A Systematic Review and Meta-Analysis. Tissue Eng. Regen. Med. 2022, 19, 463–475. [Google Scholar] [CrossRef]
- Patel, B.; Joshi, S.; Nagrani, T.; Girdhar, G.A.; Patel, H.; Sinha, S.; Haque, M.; Kumar, S.; Haq, M.A. Clinical and Radiographic Evaluation of Autologous Platelet-Rich Fibrin With or Without Demineralized Bone Matrix in the Treatment of Grade II Furcation Defects. Cureus 2023, 15, e44394. [Google Scholar] [CrossRef]
- Gollapudi, M.; Bajaj, P.; Oza, R.R. Injectable Platelet-Rich Fibrin—A Revolution in Periodontal Regeneration. Cureus 2022, 14, e28647. [Google Scholar] [CrossRef]
- Al-Sharabi, N.; Gruber, R.; Sanz, M.; Mohamed-Ahmed, S.; Kristoffersen, E.K.; Mustafa, K.; Shanbhag, S. Proteomic Analysis of Mesenchymal Stromal Cells Secretome in Comparison to Leukocyte- and Platelet-Rich Fibrin. Int. J. Mol. Sci. 2023, 24, 13057. [Google Scholar] [CrossRef]
- Mudalal, M.; Wang, Z.; Mustafa, S.; Liu, Y.; Wang, Y.; Yu, J.; Wang, S.; Sun, X.; Zhou, Y. Effect of Leukocyte-Platelet Rich Fibrin (L-PRF) on Tissue Regeneration and Proliferation of Human Gingival Fibroblast Cells Cultured Using a Modified Method. Tissue Eng. Regen. Med. 2021, 18, 895–904. [Google Scholar] [CrossRef]
- Xu, J.; Gou, L.; Zhang, P.; Li, H.; Qiu, S. Platelet-rich plasma and regenerative dentistry. Aust. Dent. J. 2020, 65, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Martu, M.A.; Maftei, G.A.; Luchian, I.; Stefanescu, O.M.; Scutariu, M.M.; Solomon, S.M. The Effect of Acknowledged and Novel Anti-Rheumatic Therapies on Periodontal Tissues-A Narrative Review. Pharmaceuticals 2021, 14, 1209. [Google Scholar] [CrossRef]
- Park, J.B.; Kim, I.; Lee, W.; Kim, H. Evaluation of the regenerative capacity of stem cells combined with bone graft material and collagen matrix using a rabbit calvarial defect model. J. Periodontal Implant. Sci. 2023, 53, 467–477. [Google Scholar] [CrossRef]
- Cortese, A.; Pantaleo, G.; Borri, A.; Caggiano, M.; Amato, M. Platelet-rich fibrin (PRF) in implant dentistry in combination with new bone regenerative technique in elderly patients. Int. J. Surg. Case Rep. 2016, 28, 52–56. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 6.4. 2023. [Updated August 2023]. Available online: https://training.cochrane.org/handbook (accessed on 17 September 2023).
- Bansal, C.; Bharti, V. Evaluation of efficacy of autologous platelet-rich fibrin with demineralized-freeze dried bone allograft in the treatment of periodontal intrabony defects. J. Indian Soc. Periodontol. 2013, 17, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Elgendy, E.A.; Abo Shady, T.E. Clinical and radiographic evaluation of nanocrystalline hydroxyapatite with or without platelet-rich fibrin membrane in the treatment of periodontal intrabony defects. J. Indian Soc. Periodontol. 2015, 19, 61–65. [Google Scholar] [CrossRef]
- Gamal, A.Y.; Abdel Ghaffar, K.A.; Alghezwy, O.A. Crevicular Fluid Growth Factors Release Profile Following the Use of Platelet-Rich Fibrin and Plasma Rich Growth Factors in Treating Periodontal Intrabony Defects: A Randomized Clinical Trial. J. Periodontol. 2016, 87, 654–662. [Google Scholar] [CrossRef] [PubMed]
- Naqvi, A.; Gopalakrishnan, D.; Bhasin, M.T.; Sharma, N.; Haider, K.; Martande, S. Comparative Evaluation of Bioactive Glass Putty and Platelet Rich Fibrin in the Treatment of Human Periodontal Intrabony Defects: A Randomized Control Trial. J. Clin. Diagn. Res. 2017, 11, ZC09–ZC13. [Google Scholar] [CrossRef]
- Sezgin, Y.; Uraz, A.; Taner, I.L.; Culhaoglu, R. Effects of platelet-rich fibrin on healing of intra-bony defects treated with anorganic bovine bone mineral. Braz. Oral. Res. 2017, 31, e15. [Google Scholar] [CrossRef] [PubMed]
- Aggour, R.L.; Abd El-Hady, H.M.G. Platelet-Rich Fibrin for the Treatment of Intrabony Periodontal Defects in Patients with Generalized Aggressive Periodontitis: A Randomized Controlled Clinical Study. J. Int. Acad. Periodontol. 2017, 19, 28–34. [Google Scholar] [PubMed]
- Bodhare, G.H.; Kolte, A.P.; Kolte, R.A.; Shirke, P.Y. Clinical and radiographic evaluation and comparison of bioactive bone alloplast morsels when used alone and in combination with platelet-rich fibrin in the treatment of periodontal intrabony defects-A randomized controlled trial. J. Periodontol. 2019, 90, 584–594. [Google Scholar] [CrossRef] [PubMed]
- Saravanan, D.; Rethinam, S.; Muthu, K.; Thangapandian, A. The Combined Effect of Bioactive Glass and Platelet-Rich Fibrin in Treating Human Periodontal Intrabony Defects—A Clinicoradiographic Study. Contemp. Clin. Dent. 2019, 10, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Atchuta, A.; Gooty, J.R.; Guntakandla, V.R.; Palakuru, S.K.; Durvasula, S.; Palaparthy, R. Clinical and radiographic evaluation of platelet-rich fibrin as an adjunct to bone grafting demineralized freeze-dried bone allograft in intrabony defects. J. Indian Soc. Periodontol. 2020, 24, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Goyal, J.; Sachdeva, S.; Salaria, S.K.; Vakil, N.; Mittal, A. Comparative assessment of periodontal regeneration in periodontal intraosseous defects treated with PepGen P-15 unaided or in blend with platelet-rich fibrin: A clinical and high-resolution computed tomography scan-assisted volumetric analysis. J. Indian Soc. Periodontol. 2020, 24, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Pavani, M.P.; Reddy, K.; Reddy, B.H.; Biraggari, S.K.; Babu, C.H.C.; Chavan, V. Evaluation of platelet-rich fibrin and tricalcium phosphate bone graft in bone fill of intrabony defects using cone-beam computed tomography: A randomized clinical trial. J. Indian Soc. Periodontol. 2021, 25, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Bahammam, M.A.; Attia, M.S. Expression of Vascular Endothelial Growth Factor Using Platelet Rich Fibrin (PRF) and Nanohydroxyapatite (nano-HA) in Treatment of Periodontal Intra-Bony Defects—A Randomized Controlled Trial. Saudi J. Biol. Sci. 2021, 28, 870–878. [Google Scholar] [CrossRef] [PubMed]
- Hazari, V.; Choudhary, A.; Mishra, R.; Chandrashekar, K.T.; Trivedi, A.; Pathak, P.K. Clinical and Radiographic Analysis of Novabone Putty with Platelet-Rich Fibrin in the Treatment of Periodontal Intrabony Defects: A Randomized Control Trial. Contemp. Clin. Dent. 2021, 12, 150–156. [Google Scholar] [CrossRef]
- Mallappa, J.; Vasanth, D.; Gowda, T.M.; Shah, R.; Gayathri, G.V.; Mehta, D.S. Clinicoradiographic evaluation of advanced-platelet rich fibrin block (A PRF + i PRF + nanohydroxyapatite) compared to nanohydroxyapatite alone in the management of periodontal intrabony defects. J. Indian Soc. Periodontol. 2022, 26, 359–364. [Google Scholar] [CrossRef]
- Baghele, O.N.; Thorat, M.S.; Malpani, P.S. Clinical and radiographic evaluation of platelet rich fibrin and bone graft material (beta-tricalcium phosphate + hydroxyapatite) in the treatment of intrabony defects of periodontitis patients—A randomized controlled trial. Quintessence Int. 2023, 54, 472. [Google Scholar] [CrossRef] [PubMed]
- Singhal, D.; Bali, S.; Aggarwal, P.; Nautiyal, A.; Pal, K. Comparative Evaluation of Anorganic Bovine Bone Matrix (ABBM) with or without Platelet Rich Fibrin intreatment of Intrabony Defects:A Randomized Controlled Trial. J. Pharm. Negat. Results 2022, 224, 1703–1710. [Google Scholar] [CrossRef]
- Alshoiby, M.M.; Fawzy El-Sayed, K.M.; Elbattawy, W.; Hosny, M.M. Injectable platelet-rich fibrin with demineralized freeze-dried bone allograft compared to demineralized freeze-dried bone allograft in intrabony defects of patients with stage-III periodontitis: A randomized controlled clinical trial. Clin. Oral. Investig. 2023, 27, 3457–3467. [Google Scholar] [CrossRef] [PubMed]
- Recica, B.; Bukleta, D.; Popovska, M.; Tefiku, U.; Ahmedi, J.; Stubljar, D. Comparative analysis of the effect of 4MATRIX with and without PRF on regeneration of infrabony periodontal pockets. Saudi Dent. J. 2023, 35, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Lekovic, V.; Camargo, P.M.; Weinlaender, M.; Nedic, M.; Aleksic, Z.; Kenney, E.B. A comparison between enamel matrix proteins used alone or in combination with bovine porous bone mineral in the treatment of intrabony periodontal defects in humans. J. Periodontol. 2000, 71, 1110–1116. [Google Scholar] [CrossRef] [PubMed]
- Zucchelli, G.; Amore, C.; Montebugnoli, L.; De Sanctis, M. Enamel matrix proteins and bovine porous bone mineral in the treatment of intrabony defects: A comparative controlled clinical trial. J. Periodontol. 2003, 74, 1725–1735. [Google Scholar] [CrossRef]
- Finkemeier, C.G. Bone-grafting and bone-graft substitutes. J. Bone Jt. Surg. Am. Vol. 2002, 84, 454–464. [Google Scholar] [CrossRef]
- Cheah, C.W.; Al-Namnam, N.M.; Lau, M.N.; Lim, G.S.; Raman, R.; Fairbairn, P.; Ngeow, W.C. Synthetic Material for Bone, Periodontal, and Dental Tissue Regeneration: Where Are We Now, and Where Are We Heading Next? Materials 2021, 14, 6123. [Google Scholar] [CrossRef]
- Zhao, R.; Yang, R.; Cooper, P.R.; Khurshid, Z.; Shavandi, A.; Ratnayake, J. Bone Grafts and Substitutes in Dentistry: A Review of Current Trends and Developments. Molecules 2021, 26, 3007. [Google Scholar] [CrossRef]
- Mohan, S.P.; Jaishangar, N.; Devy, S.; Narayanan, A.; Cherian, D.; Madhavan, S.S. Platelet-Rich Plasma and Platelet-Rich Fibrin in Periodontal Regeneration: A Review. J. Pharm. Bioallied Sci. 2019, 11, S126–S130. [Google Scholar] [CrossRef]
- Varshney, S.; Dwivedi, A.; Dwivedi, V. Comparing efficacies of autologous platelet concentrate preparations as mono-therapeutic agents in intra-bony defects through systematic review and meta-analysis. J. Oral. Biol. Craniofacial Res. 2023, 13, 671–681. [Google Scholar] [CrossRef] [PubMed]
- Sinha, A.; Jain, A.K.; Rao, R.D.; Sivasailam, S.; Jain, R. Effect of platelet-rich fibrin on periapical healing and resolution of clinical symptoms in patients following periapical surgery: A systematic review and meta-analysis. J. Conserv. Dent. 2023, 26, 366–376. [Google Scholar]
- Rahul, M.; Lokade, A.; Tewari, N.; Mathur, V.; Agarwal, D.; Goel, S.; Keshari, P.; Sharma, S.; Bansal, K. Effect of Intracanal Scaffolds on the Success Outcomes of Regenerative Endodontic Therapy—A Systematic Review and Network Meta-analysis. J. Endod. 2023, 49, 110–128. [Google Scholar] [CrossRef] [PubMed]
- Riaz, A.; Shah, F.A. Regenerating the Pulp-Dentine Complex Using Autologous Platelet Concentrates: A Critical Appraisal of the Current Histological Evidence. Tissue Eng. Regen. Med. 2021, 18, 37–48. [Google Scholar] [CrossRef]
- Long, T.; Li, C.; Xu, F.; Xiao, J. Therapeutic efficacy of platelet-rich fibrin on surgical site wound healing in patients undergoing oral carcinoma resection: A meta-analysis. Int. Wound J. 2023, 21, e14386. [Google Scholar] [CrossRef] [PubMed]
- Zafar, A.; Tripathi, V.; Khan, M.; Manglam, K.K.; Rastogi, P.; Almotreb, A.M. To Evaluate the Antimicrobial Activity of PRP and PRF with and without Nanosilver. J. Pharm. Bioallied Sci. 2023, 15, S892–S894. [Google Scholar] [CrossRef]
- Tabassum, S.; Raj, S.C.; Rath, H.; Mishra, A.K.; Mohapatra, A.; Patnaik, K. Effect of platelet rich fibrin on stability of dental implants: A systematic review and meta-analysis. Int. J. Health Sci. 2022, 16, 58–68. [Google Scholar]
- Cheng, B.; Feng, F.; Shi, F.; Huang, J.; Zhang, S.; Quan, Y.; Tu, T.; Liu, Y.; Wang, J.; Zhao, Y.; et al. Distinctive Roles of Wnt Signaling in Chondrogenic Differentiation of BMSCs under Coupling of Pressure and Platelet-Rich Fibrin. Tissue Eng. Regen. Med. 2022, 19, 823–837. [Google Scholar] [CrossRef]
- Singhal, L.; Belludi, S.A.; Pradhan, N.; Manvi, S. A comparative evaluation of the effect of platelet rich fibrin matrix with and without peripheral blood mesenchymal stem cells on dental implant stability: A randomized controlled clinical trial. J. Tissue Eng. Regen. Med. 2022, 16, 422–430. [Google Scholar] [CrossRef] [PubMed]
- La Rosa, G.R.M.; Marcianò, A.; Priolo, C.Y.; Peditto, M.; Pedullà, E.; Bianchi, A. Effectiveness of the platelet-rich fibrin in the control of pain associated with alveolar osteitis: A scoping review. Clin. Oral. Investig. 2023, 27, 3321–3330. [Google Scholar] [CrossRef]
- Carrera, T.M.I.; Machado, L.M.; Soares, M.T.R.; Passos, G.P.; Oliveira, G.J.P.; Ribeiro Júnior, N.V.; Soares, P.B.F.; Pigossi, S.C. Root coverage with platelet-rich fibrin or connective tissue graft: A split-mouth randomized trial. Braz. Oral. Res. 2023, 37, e084. [Google Scholar] [CrossRef] [PubMed]
- Öngöz Dede, F.; Bozkurt Doğan, Ş.; Çelen, K.; Çelen, S.; Deveci, E.T.; Seyhan Cezairli, N. Comparison of the clinical efficacy of concentrated growth factor and advanced platelet-rich fibrin in the treatment of type I multiple gingival recessions: A controlled randomized clinical trial. Clin. Oral. Investig. 2023, 27, 645–657. [Google Scholar] [CrossRef]
- Al-Hamed, F.S.; Tawfik, M.A.-M.; Abdelfadil, E. Clinical effects of platelet-rich fibrin (PRF) following surgical extraction of lower third molar. Saudi J. Dent. Res. 2017, 8, 19–25. [Google Scholar] [CrossRef]
- Madi, M.; Elakel, A.M. The clinical implications of platelet-rich fibrin on periodontal regeneration: A systematic review. Saudi Dent. J. 2021, 33, 55–62. [Google Scholar] [CrossRef]
- Kornsuthisopon, C.; Pirarat, N.; Osathanon, T.; Kalpravidh, C. Autologous platelet-rich fibrin stimulates canine periodontal regeneration. Sci. Rep. 2020, 10, 1850. [Google Scholar] [CrossRef] [PubMed]
- Abd-Elkawi, M.; Sharshar, A.; Misk, T.; Elgohary, I.; Gadallah, S. Effect of calcium carbonate nanoparticles, silver nanoparticles and advanced platelet-rich fibrin for enhancing bone healing in a rabbit model. Sci. Rep. 2023, 13, 15232. [Google Scholar] [CrossRef]
- Li, T.; Long, H.; Niu, W.; Feng, B. The repair and regeneration mechanism of platelet-rich fibrin-promoting tissue after alveolar bone defect through the notch pathway. Cell. Mol. Biol. 2023, 69, 85–90. [Google Scholar] [CrossRef]
- Ozgul, O.; Senses, F.; Er, N.; Tekin, U.; Tuz, H.H.; Alkan, A.; Kocyigit, I.D.; Atil, F. Efficacy of platelet rich fibrin in the reduction of the pain and swelling after impacted third molar surgery: Randomized multicenter split-mouth clinical trial. Head. Face Med. 2015, 11, 37. [Google Scholar] [CrossRef]
- Sánchez-Meca, J.; Marín-Martínez, F.; López-López, J.A.; Núñez-Núñez, R.M.; Rubio-Aparicio, M.; López-García, J.J.; López-Pina, J.A.; Blázquez-Rincón, D.M.; López-Ibáñez, C.; López-Nicolás, R. Improving the reporting quality of reliability generalization meta-analyses: The REGEMA checklist. Res. Synth. Methods 2021, 12, 516–536. [Google Scholar] [CrossRef]
- Sutton, A.J.; Duval, S.J.; Tweedie, R.L.; Abrams, K.R.; Jones, D.R. Empirical assessment of effect of publication bias on meta-analyses. BMJ 2000, 320, 1574–1577. [Google Scholar] [CrossRef]
- Liu, K.; Huang, Z.; Chen, Z.; Han, B.; Ouyang, X. Treatment of periodontal intrabony defects using bovine porous bone mineral and guided tissue regeneration with/without platelet-rich fibrin: A randomized controlled clinical trial. J. Periodontol. 2021, 92, 1546–1553. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, I.; Chandran, S.; Nadig, P. Comparative evaluation of the efficacy of platelet-rich fibrin and calcium phosphosilicate putty alone and in combination in the treatment of intrabony defects: A randomized clinical and radiographic study. Contemp. Clin. Dent. 2017, 8, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Mlachkova, A.; Dosseva-Panova, V.; Ivanov, I.; Parvanov, D.; Maynalovska, H. Application of platelet rich fibrin in surgical periodontal therapy: A controlled clinical trial. J. IMAB 2022, 28, 4–9. [Google Scholar] [CrossRef]
- Chaudhary, B.; Singh, R.; Manjunath, R.; Subramanyam, S. Injectable platelet-rich fibrin polymerized with hydroxyapatite bone graft for the treatment of three-wall intrabony defects: A randomized control clinical trial. J. Indian Soc. Periodontol. 2023, 27, 174–179. [Google Scholar]
- Agarwal, A.; Gupta, N.; Jain, A. Platelet rich fibrin combined with decalcified freeze-dried bone allograft for the treatment of human intrabony periodontal defects: A randomized split mouth clinical trail. Acta odontol. Scand. 2016, 74, 36–43. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Study Design | Sample Size (Control:Intervention) | Type of Graft Material | Platelet-Rich Fibrin Preparation Method (Centrifuge System) | Application Method | Follow-Up Period |
|---|---|---|---|---|---|---|
| Bansal 2013 [19] | RCT (split-mouth) | 10:10 | Allograft (DFDBA) | 3000 rpm for 10 min (NR) | Mixture of PRF with graft material | 6 months |
| Elgendy 2015 [20] | RCT (split-mouth) | 20:20 | Synthetic material | 3000 rpm for 10 min (NR) | Membrane | 6 months |
| Gamal 2016 [21] | RCT (parallel) | 9:10 | Xenograft | 2500 rpm for 10 min (NR) | Mixture of PRF with graft material & membrane | 6, 9 months |
| Naqvi 2017 [22] | RCT (split-mouth) | 10:10 | Synthetic material | 400× g for 10 min (NR) | Membrane | 3, 6, 9 months |
| Sezgin 2017 [23] | RCT(split-mouth) | 15:15 | Xenograft | 2700 rpm (approximately 400× g) for 12 min (PC-02 table centrifuge, Process for PRF, Nice, France)) | Mixture of PRF with graft material & membrane | 6 months |
| Aggour 2017 [24] | RCT (split-mouth) | 16:16 | Autograft + xenograft | 400× g for 10 min (tabletop centrifuge, Shanghai Medical Instruments, Shanghai, China) | Membrane | 6 months |
| Bodhare 2019 [25] | RCT (split-mouth) | 20:20 | Synthetic material | 3000 rpm for 10 min (REMI® Laboratories, Mumbai, Maharashtra, India) | Membrane & graft material mixed with few drops of top layer of straw-colored acellular plasma | 3, 6 months |
| Saravanan 2019 [26] | RCT (split-mouth) | 15:15 | Synthetic material | 3000 rpm for 10 min (NR) | Mixture of PRF with graft material | 6 months |
| Atchuta 2020 [27] | RCT (parallel) | 13:13 | Allograft (DFDBA) | 3000 rpm for 10 min (NR) | Mixture of PRF with graft material | 3, 6 months |
| Goyal 2020 [28] | RCT (split-mouth) | 12:12 | Xenograft + synthetic material | 2700 rpm for 10 min (REMI® Laboratories, Mumbai, Maharashtra, India) | Mixture of PRF with graft material | 3, 6 months |
| Pavani 2021 [29] | RCT (parallel) | 10:10 | Synthetic material | 3000 rpm for 10 min (NR) | Mixture of PRF with graft material | 6 months |
| Bahammam 2021 [30] | RCT (parallel) | 15:15 | Synthetic material | 3000 rpm for 10 min (NR) | Membrane | 6 months |
| Hazari 2021 [31] | RCT (parallel) | 10:10 | Synthetic material | 3000 rpm for 10 min (NR) | Mixture of PRF with graft material | 3, 6 months |
| Mallappa 2022 [32] | RCT (parallel) | 14:14 | Synthetic material | 1500 rpm for 14 min (A-PRF) 700 rpm for 3 min (i-PRF) (Process for PRF, Nice, France) | Mixture of A-PRF, i-PRF and graft material | 6 months |
| Baghele 2022 [33] | RCT (parallel) | 21:21 | Synthetic material | 3000 rpm for 10 min (NR) | Membrane | 6 months |
| Singhal 2022 [34] | RCT (parallel) | 12:12 | Xenograft | 3000 rpm for 12 min (NR) | Mixture of PRF with graft material | 3, 6 months |
| Alshoiby 2023 [35] | RCT (parallel) | 10:10 | Allograft (DFDBA) | 60× g (700 rpm) for 3 min (i-PRF) (VE-4000, Velab, Pharr, TX, USA) | mixture of PRF with graft material | 6, 9 months |
| Recica 2023 [36] | RCT (split-mouth) | 30:30 | Synthetic material | (NR) | Membrane | 6, 12, 18 months |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, W.-J.; Han, S.-H.; Kim, N.J.; Park, J.-B. The Efficacy of Utilizing Platelet-Rich Fibrin for Managing Periodontal Intrabony Defects in Conjunction with Graft Material: A Systematic Review and Meta-Analysis. Appl. Sci. 2024, 14, 3371. https://doi.org/10.3390/app14083371
Park W-J, Han S-H, Kim NJ, Park J-B. The Efficacy of Utilizing Platelet-Rich Fibrin for Managing Periodontal Intrabony Defects in Conjunction with Graft Material: A Systematic Review and Meta-Analysis. Applied Sciences. 2024; 14(8):3371. https://doi.org/10.3390/app14083371
Chicago/Turabian StylePark, Won-Jong, Sung-Hoon Han, Na Jin Kim, and Jun-Beom Park. 2024. "The Efficacy of Utilizing Platelet-Rich Fibrin for Managing Periodontal Intrabony Defects in Conjunction with Graft Material: A Systematic Review and Meta-Analysis" Applied Sciences 14, no. 8: 3371. https://doi.org/10.3390/app14083371
APA StylePark, W.-J., Han, S.-H., Kim, N. J., & Park, J.-B. (2024). The Efficacy of Utilizing Platelet-Rich Fibrin for Managing Periodontal Intrabony Defects in Conjunction with Graft Material: A Systematic Review and Meta-Analysis. Applied Sciences, 14(8), 3371. https://doi.org/10.3390/app14083371