1. Introduction
As an important sector in developed countries, healthcare buildings play a major role in their economy because of the large quantities of energy they use. In particular, the public healthcare sector expense in Spain reached €70,635.7 million, which represented 6.5% of its Gross Domestics Product (GDP) in 2017, in which 4.71% belonged to the public sector (with about 108,000 beds) and 1.80% corresponded to the private sector (52,000 beds approximately) [
1]. The public expenditure on health reached €1521 per inhabitant in Spain.
In the last few years, the energy intensity in Spain has increased, while it has regularly been decreasing in most of the EU. While Spain is dependent on primary energy at about 80%, it only represents 50% on average in the EU [
2]. For this reason, it has become urgent and necessary to establish efficiency measures in order to save energy in all the sectors of consumption, and particularly in hospitals [
3].
Madrid Energy Foundation (2010) indicated that the annual energy consumption in a small hospital reached 40,000 kWh, with an annual expense of €8400 [
4].
Kolokotsa et al. (2012) reported that up to 10% of primary energy consumed could be save by implementing simple energy saving techniques. In order to do that, high-cost energy categories should be controlled and monitored [
5].
Santamouris et al. (1994) quantified the potential global energy savings in 30 healthcare buildings in Hellas (Greece) by energy audits analysis. They concluded that up to 20% of energy could be saved [
6]. Murray et al. (2008) argued that depending on the building, energy consumption varied broadly. They proposed that a benchmark of 0.2 GJ/m
3 would be realistic [
7].
Vanhoudt et al. (2011) demonstrated in a hospital in Belgium that it is possible to save up to 71% of the primary energy by using stored thermal energy in combination with a heat pump, instead of conventional gas-based boilers and water chillers [
8]. Yun et al. (2012) showed that a change in the occupancy patterns of a building with respect to the initial design settings might result in higher rates of energy consumption for lighting purposes, which could potentially represent up to 50% energy savings [
9].
Martini et al. (2007) reported on the energy behaviour of different types of health service facilities within Argentinian Public Health Network, and assessed correlations between energy consumption rates and several related variables, including space, usage, infrastructure and equipment [
10]. However, no specific energy saving measures were proposed.
Bonnema et al. (2010) worked in the Advanced Energy Design Guide, which aimed to save 30% in energy, as required by ANSI/ASHRAE/IESNA, applied to small hospitals and healthcare facilities. The guide provided user-friendly assistance and recommendations for the design and construction of buildings [
11].
Szklo et al. (2004) studied energy consumption indicators in hospitals in Brazil [
12]. They found that the average ratio between thermal and electric loads was appropriate to use cogeneration systems. In addition, by analysing a non-optimized cogeneration system, they predicted substantial potential energy savings and CO
2 reduction.
However, none of the above-mentioned authors either analysed or quantified any possible annual economic saving derived from optimizing and managing the energy needed in this type of building.
The purpose of this article is to estimate the economic and environmental impacts of energy consumption derived from healthcare buildings and proposes several energy-saving options in the sector. The results of this study will be used to development a suitable tool both in the fields of project-management of new hospitals and cost-optimisation in existing healthcare buildings.
2. Materials and Methods
Between 2005 and 2013, an analytical study was performed in 12 hospitals and 70 healthcare centres belonging to the Public Health System in Spain, which were built between 1980 and 2005, all located in Extremadura, a region in the southwest of Spain. The original energy consumption of all those buildings was analysed by using the data collected through audits carried out during the period 2005–2012 by the Extremadura Energy Agency. The final energy consumption, after energy efficiency modifications, was obtained by considering the mean saving values for the following three years. The economic and environmental impacts of energy saving were assessed as well.
The design conditions of the facilities were evaluated by analysing the building construction projects. Additionally, those architects and engineers responsible for the construction were interviewed for information purposes.
The energy savings measures were assessed after some previous meetings with the hospital’s maintenance engineers, which involved a detailed analysis of the records, the measurement of energy flows, individual surveys on energy consumption and monitoring of habits of patients, visitors, and staff as related to energy consumption in the building.
For research purposes, the hospitals were classified into two categories: those with more than 5000 m
2, with hospitalization beds; and health centres without hospitalization beds, with less than 5000 m
2 [
13].
The average emissions of CO
2, sulphur dioxide (SO
2), and nitrogen oxide (NO
x) were estimated as 331.0 g/kWh, 0.61 g/kWh and 0.4325 g/kWh, respectively [
14]. Additionally, it was taken into account that 1 kWh of primary energy in Spain is equivalent to 2.368 kWh of final energy.
To quantify the energy consumption in all healthcare building, network analysers, digital luxometers, flowmeters, combustion gas analysers, thermographic cameras, digital thermometers, hygrometers, and energy counters were used [
15]. Field inspections were carried out to analyse the initial conditions and check the development of the implemented measures.
To calculate annual consumption of gas and electricity, billings from supply companies were analysed [
16]. The electric energy, domestic water heating (DWH), air conditioning systems (HVAC), lighting system, external enclosures, maintenance strategy and renewable energy generation were also analysed.
The useful floor area of each hospital was regarded as that of the outer perimeter of a covered space, subtracting the constructive elements related to the building’s closures, partitions, structure, and installations. Built and useful floor areas of the hospitals under study were obtained from the construction projects.
In the course of the investigation, certain parameters were identified in the relationship between planned savings and other functional and operating costs for each healthcare building, such as construction year, construction surface area, number of workers, number of medical visits, and assistance activity, by means of mathematical techniques.
3. Results
According to the potential energy saving achieved by healthcare building facilities, a series of interesting results were obtained.
3.1. Optimization of Electric Energy Installations
The electric installation in a healthcare building is of major importance, since these buildings play a vital role in public health service [
17]. San José et al. (2009) valued that the annual average consumption of electricity in a hospital with less than 300 beds was 8.88 kWh, and 10.04 kWh for a hospital with more than 300 [
18]. García Sanz-Calcedo et al. (2011) evaluated that the annual energy consumption in a healthcare centre in Spain—in normal operational conditions and functioning—was 90 kWh/m
2 for this type of building and 150 kWh/m
2 for hospitals [
19].
With the objective of determining the positive economic and environmental impacts, thanks to optimizing electric energy installations, the annual average saving and investment for the whole set of buildings was quantified for a three-year period.
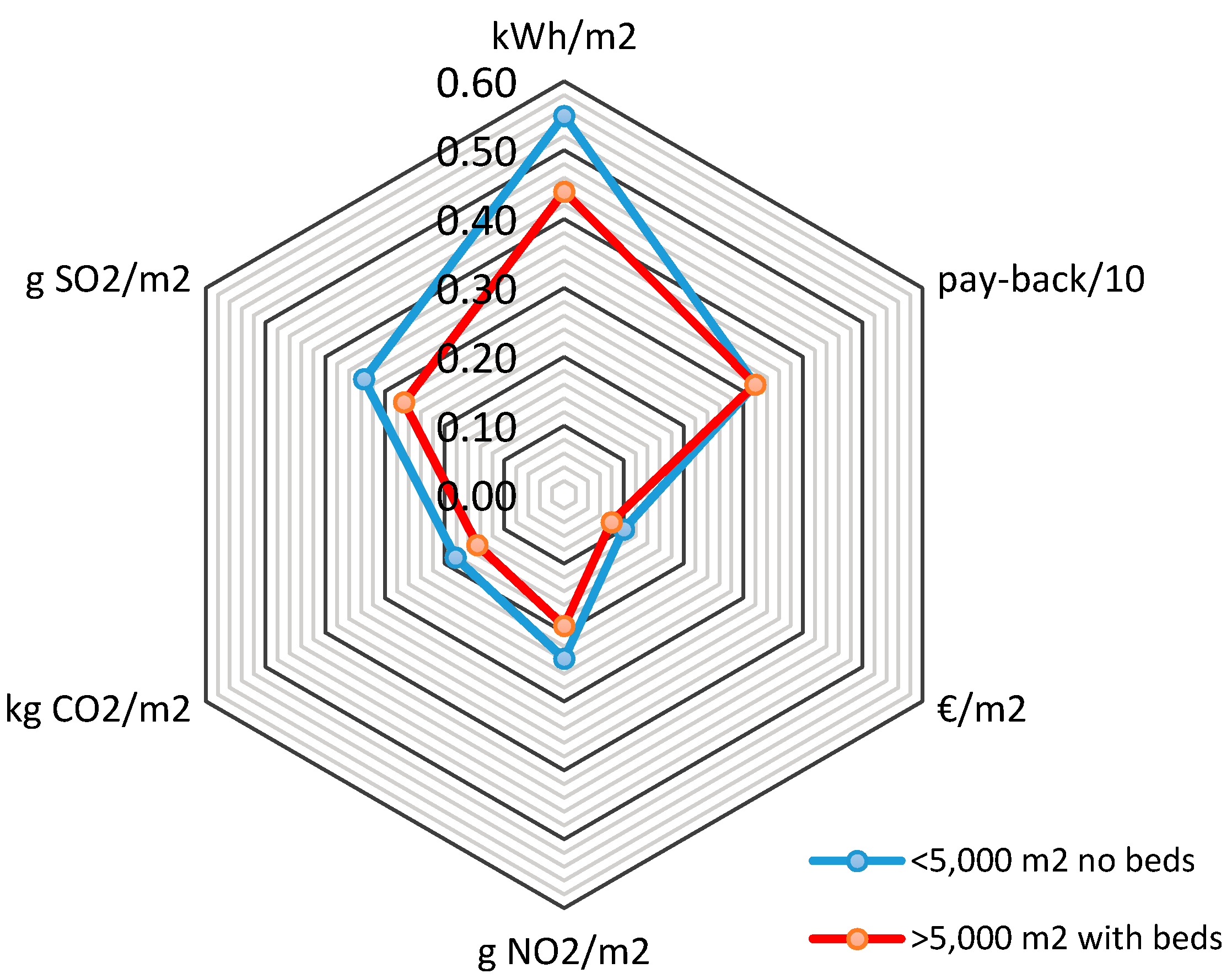
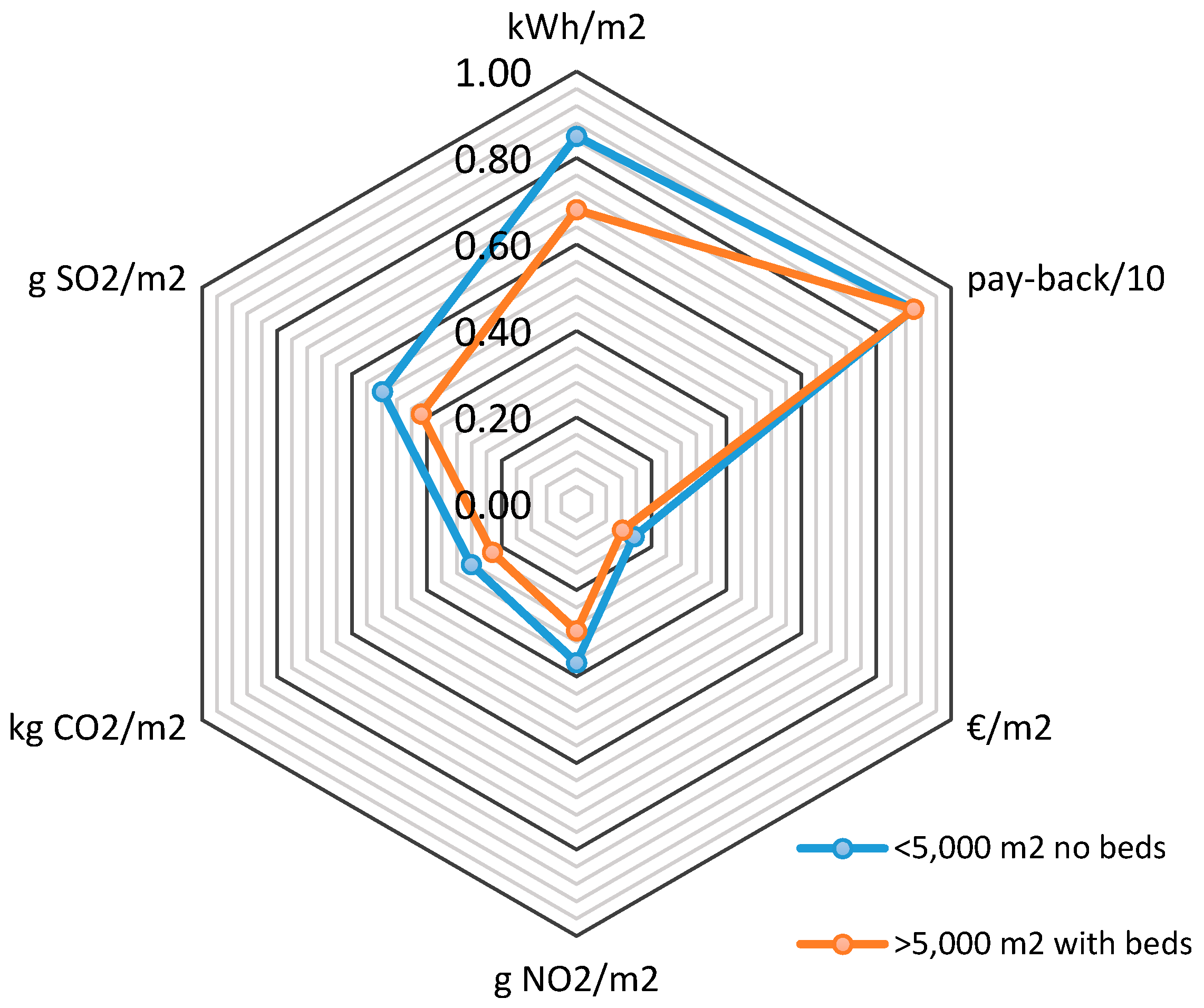
Figure 1 shows the potential mean energy saving per built surface area (m
2) through the optimization of the electric installations in healthcare buildings with less than 5000 m
2 (no beds) and hospitals larger than 5000 m
2 (with beds). An annual average energy saving of 0.45 kWh and 0.55 kWh per built surface area (m
2), with a payback lower than 3.5 years, was achieved, respectively.
The specific energy saving measures applied were the following: installation of power capacitors for reactive power compensation, improvement of the electricity contract conditions, and appropriate choice of electric power.
3.2. Improvement of Air Conditioning and Heating Systems (HVAC)
Hu et al. (2004) studied the consumption of energy of a hospital in Taiwan, concluding that the use of Air conditioning and heating systems (HVAC) has a great influence in the consumption of energy, since HVAC represents over 50% of the total amount of energy consumed [
20]. Studies performed by Natural Resources Canada pointed out that the highest energy consumption was generated by the use of the heating, lighting, and ventilation [
21].
Kappor et al. (2011) studied that HVAC generated the highest consumption of energy in hospitals, about 30–65% [
22]. After a study of a suburban hospital, the Health Department in Australia concluded the HVAC is the highest contributor to energy consumption and CO
2 emissions, at 65% and 47%, respectively [
23]. Teke et al. (2014) show hospitals represent approximately 6% of total energy consumption in the service buildings sector [
24].
In healthcare buildings, most energy consumption is consumed by HVAC facilities. Fraile et al. (2014) realized a study about energy efficiency improvements in a boiler room in a 600-bed hospital complex. They monitored six gas-fired boilers of heat and hot water over a six-month period and actions were implemented in the hospital boiler room control system to increase the efficiency of the heat production facilities [
25].
To determine the positive economic and environmental impacts due to improvement of HVAC facilities, the annual average saving and investment for the whole set of buildings was quantified for a three-year period, in five hospitals and 20 healthcare centres.
The contribution of natural ventilation as an energy-efficient technique for hospital was studied by Quian et al. (2010). The author suggest that up to 70% of net floor area of small to medium sized hospital could be naturally ventilated. A high ventilation rate helps reduce cross-infection of airborne diseases [
26].
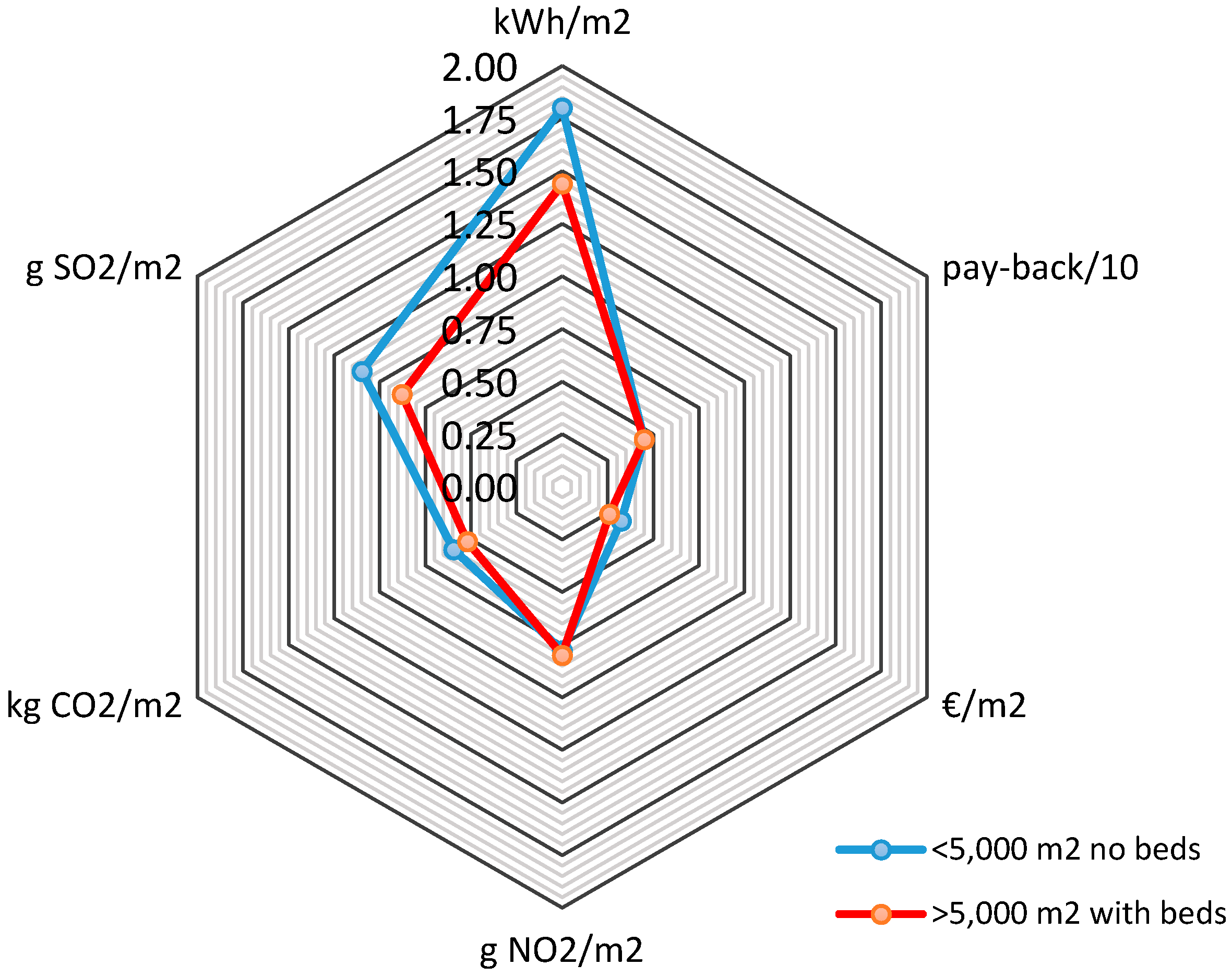
Figure 2 represents the potential mean average energy saving per built surface area (m
2), by means of upgrading HVAC installations, in healthcare buildings with less than 5000 m
2 (no beds) and hospitals larger than 5000 m
2 (with beds). An annual average energy saving of 1.50 kWh and 1.80 kWh per built surface area (m
2), with a payback lower than 2.5 years, was achieved, respectively.
The following specific energy saving measures were applied: introduction of efficient air conditioning technologies that minimize energy consumption is proposed and replacement of low-performing machines aged more than eight years by new, high-performance models was suggested. Other feasible measures to be carried out in this area are the following: maintenance of air-conditioning systems, zoning according to air conditioning units, and installation of air-handling system adjustable thermostats.
3.3. Domestic Water Heating (DWH)
The studies show that the annual average per hospital bed varies between 29 m
3/bed and 47 m
3/bed in Europe and between 36 and 55 m
3/bed in the USA [
27]. In Greece, the annual consumption of water varies between 32.85 and 43.8 m
3/bed [
28]. Bujak (2010) calculated that the average consumption of DWH in a hospital per year was between 40 and 60 m
3/bed [
29].
Gaglia et al. (2007) studied the empirical assessment non-residential building stock in Greece, energy consumption, emissions, and potential energy savings [
30]. Their energy conservation measures proposed were: installation of solar collectors for DWH production, addition of thermal insulation of exposed external walls in hotels and healthcare, replacement of old inefficient boilers, installation of building management systems, and regular maintenance of central heating boilers.
In order to quantify the economic and environmental impact from energy saving by optimizing DWH facilities, a total of 10 hospitals and 50 healthcare centres were analysed for a three-year period.
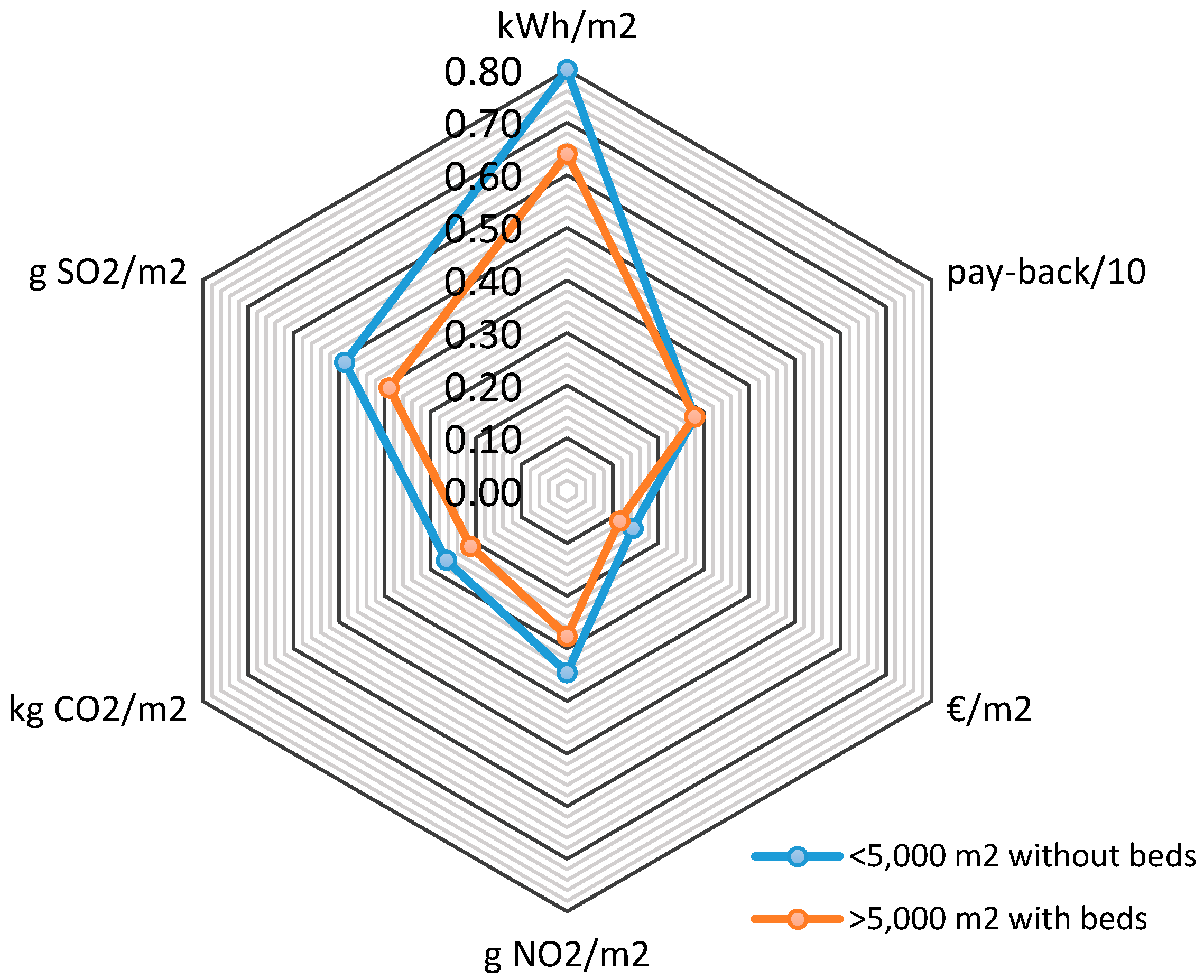
Figure 3 shows the potential average energy saving per built surface area (m
2) through the optimization of the DWH facilities, in healthcare buildings with less than 5000 m
2 (no beds) and hospitals larger than 5000 m
2 (with beds). A potential average saving between 0.65 kWh and 0.80 kWh per built surface area is detected, in a payback period of less than three years.
Here are the specific energy saving measures used: timers with programmed disconnection for DWH system production by means of water heaters, or storage tanks, in order to interrupt operation when no activity takes place. Installation of low consumption taps and tanks with double push buttons to reduce cold water for human consumption (CWHC) consumption.
3.4. Optimization of Lighting System
Lightening consumption in the Spanish health sector is about 1000 GWh/year, which means 0.6% of the national energy consumption, with an emission of 600,000 annual tons of CO
2 [
31]. Therefore, it is very important to use efficient lighting with high-performance lights, incorporating low consumption equipment and high-regulation lumen-per-watt lamps.
Lighting installation in a healthcare building must take two aspects into account: a qualitative aesthetic aspect and a quantitative engineering character. The aesthetic issue guarantees a friendly space and distribution of lights and shade inside. The technical issues control the amount of light needed for each activity in the different rooms and/or buildings [
32]. Clearly, deficient levels of light could cause professionals to make mistakes in diagnoses and dispensing errors [
33].
With the objective of determining the positive economic and environmental impacts thanks to optimizing lighting systems, the annual average saving and investment for the whole set of buildings was quantified for a three-year period.
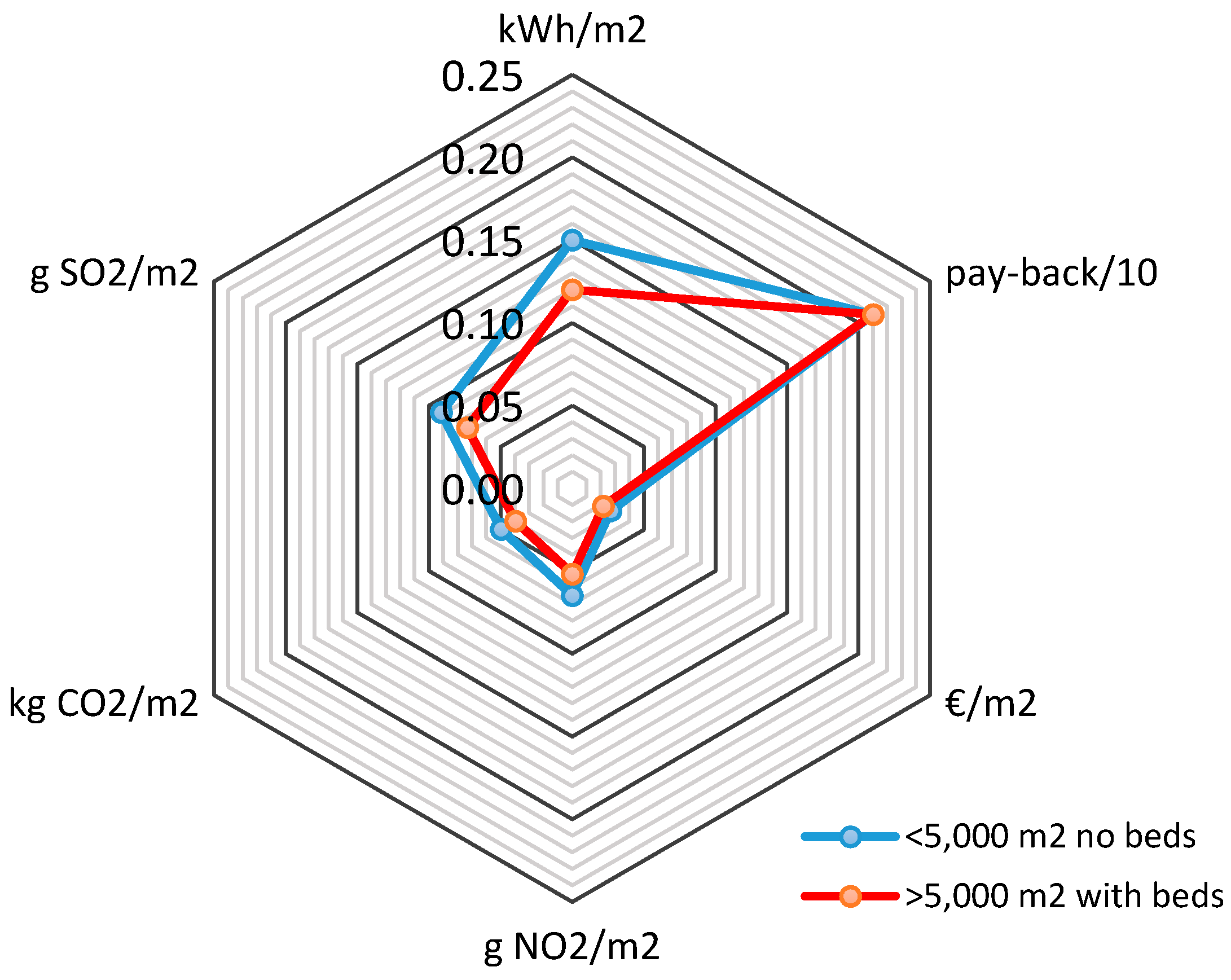
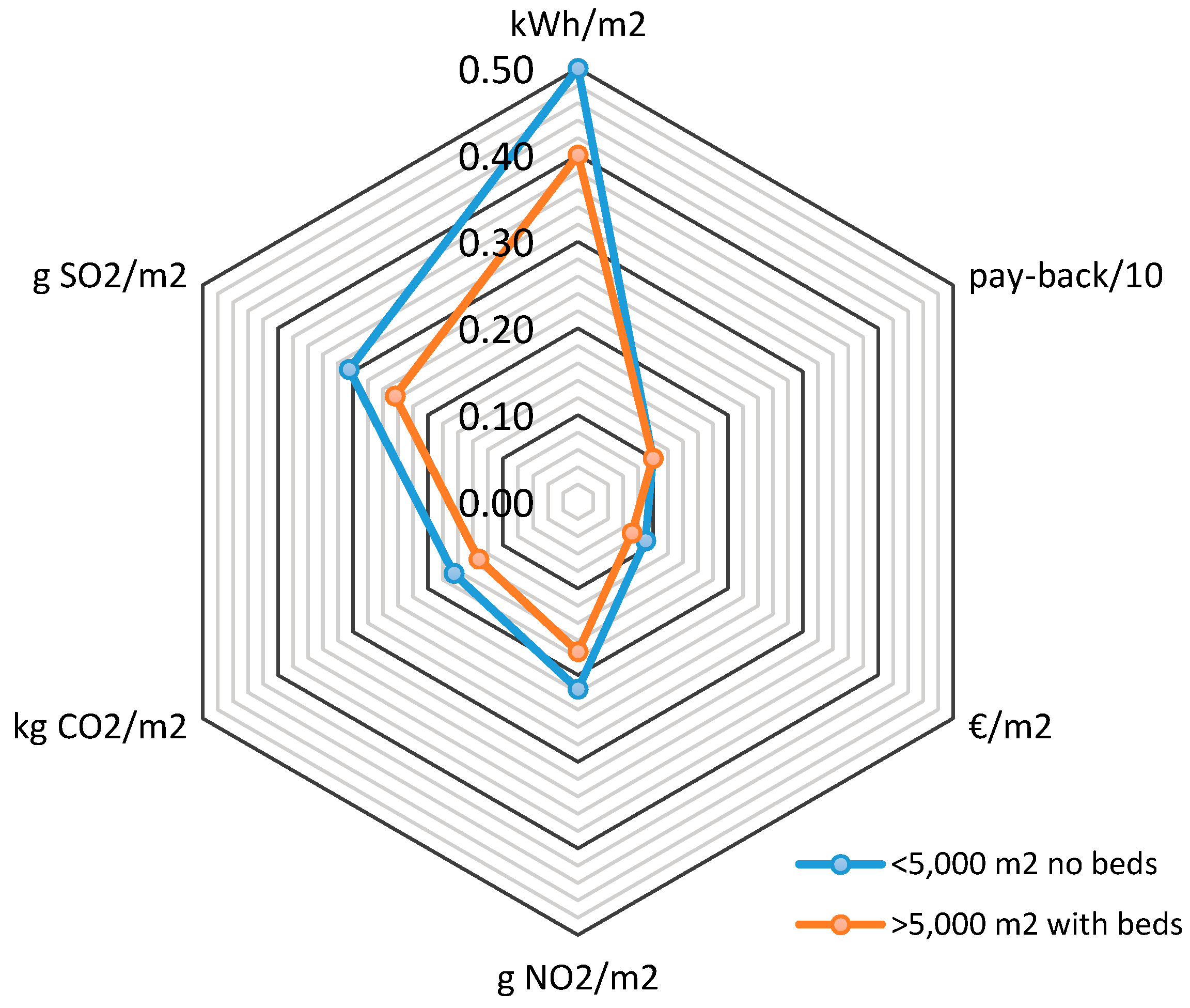
Figure 4 shows the potential average energy saving per built surface area (m
2), by means of improving lighting system performance, in healthcare buildings with less than 5000 m
2 (no beds) and hospitals larger than 5000 m
2 (with beds). An annual average energy saving of 0.12 kWh and 0.15 kWh per built surface area (m
2), with a payback of less than 2.2 years, was achieved, respectively.
The specific energy saving measures applied were installation of electronic ballast in fluorescent lamps, replacement of fluorescent and incandescent lamps by light-emitting diodes (LEDs), organization of lighting according to activity type, and the limitation of intensity and timing of the controlled lighting by using occupancy sensors.
3.5. Usage of Renewable Energies
Kantola et al. (2013) studied the facilities of the Espoo Hospital (Finland), and they concluded that the most affordable renewable solutions were biogas energy, wood chip heating, and ground source heating. Biogas energy was the most affordable solution although it is only suitable for large-scale projects since the system is not yet commonly used and some risk of uncertainty must be added [
34]. Solar electricity was the most expensive method and snow storage cooling needs to entail certain societal benefits for it to be cost-effective.
The current biomass energy conversion technology ensures the efficient operation of the facilities [
35]. In the combustion of biomass, CO
2 emissions are almost neutral provided it is part of the base that the plants retain a higher volume of CO
2 during their growth as compared with that released during combustion.
The use of solar thermal energy for hot water generation allows a reduction of energy consumption and a decrease of greenhouse gas emissions. In smaller buildings, hot water demand is relatively low and, therefore, the current systems usually do not use central distribution networks [
36], provided such demand is satisfied by the electric hot water heater, near the consumption points. Installation of solar collectors on roofs ensures a drastic reduction of energy consumption and is regarded as an efficient energy supply alternative. If larger buildings with higher associated energy consumption rates are accounted for, remarkable efficiency of solar thermal energy equipment has been reported [
37].
Power generated by a photovoltaic field is fed into the public grid, allowing the production of electricity from solar energy; it is a solution that can serve to considerably lower energy costs and contribute to the overall decrease in emissions [
38].
Use of low-temperature geothermal energy is based on the fact that the ground below a depth of 7–10 m is maintained at a stable temperature, about 17 °C, regardless of the time of year or weather conditions. This energy source allows increasing the performance of the air conditioning equipment and has been set as a renewable energy in Europe since 2009 [
39].
Renedo et al. (2006) analysed the different possibilities for providing heating, air conditioning and hot tap water to a Spanish hospital. They considered several cogeneration systems with diesel engines and gas turbines. They observed that the most important parameter is the electricity produced and concluded that the control strategy and the size of the facility have a strong influence on the energy system [
40].
In order to quantify the economic and environmental impact from energy saving by usage of renewable energies, a total of eight hospitals and 25 healthcare centres were analysed for a three-year period.
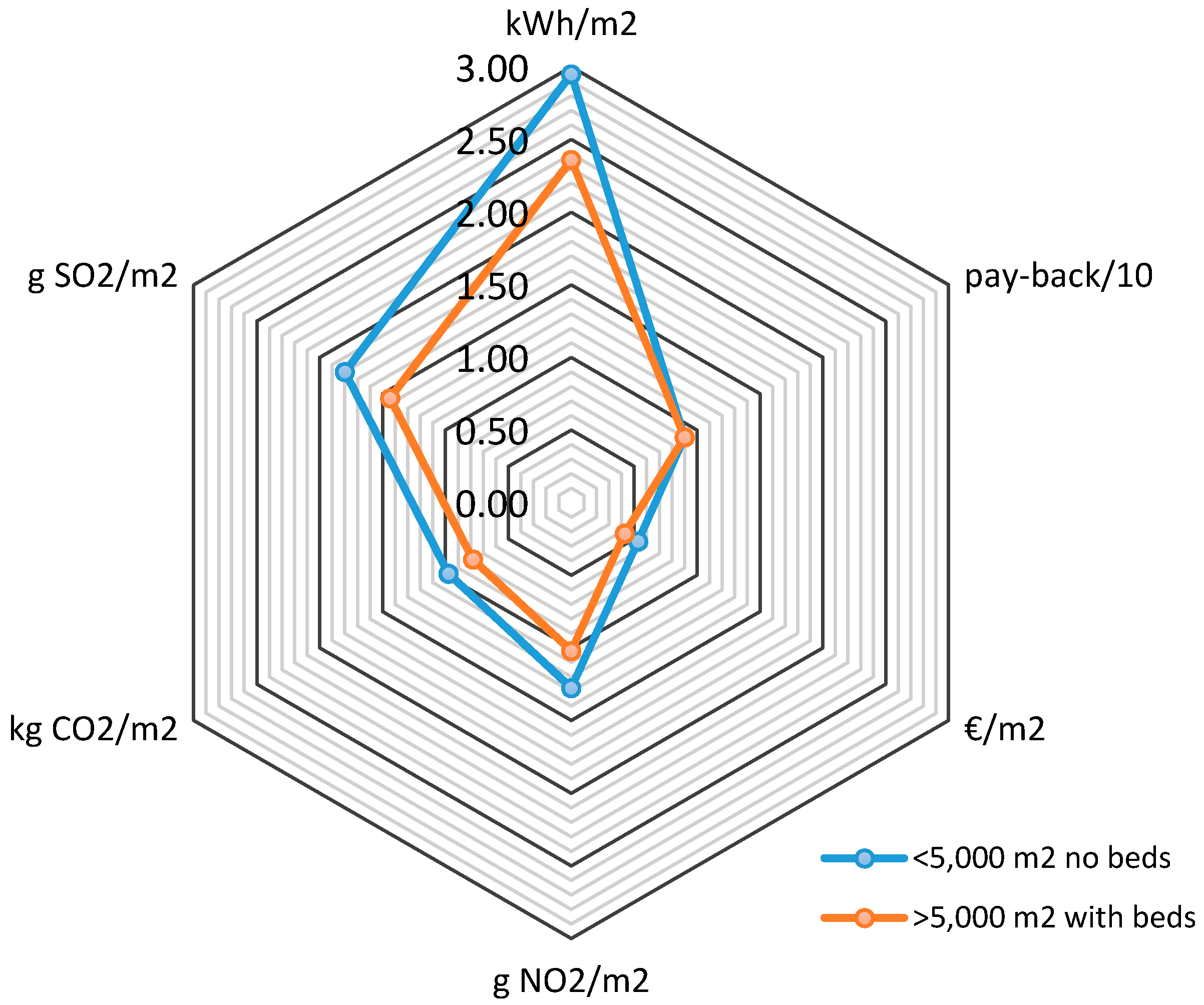
Figure 5 represents the potential average energy saving per built surface (m
2) area through the installation of renewable energy systems in healthcare buildings with less than 5000 m
2 (no beds) and hospitals larger than 5000 m
2 (with beds). A potential average saving between 2.5 kWh and 3 kWh per built surface area is observed, in a payback period lower than 10 years. Subsidies and grants can substantially reduce the time of the investment’s amortization.
The specific energy saving measures used were the following: replacement of heating boilers using fossil fuels, diesel or natural gas, with biomass boilers, use of solar thermal energy for DWH generation and installation of solar collectors on roofs ensures a drastic reduction of energy consumption.
3.6. Maintenance Management
The perception of maintenance management on healthcare facilities was analysed by Abd Rani et al. (2015). They provide an overview of the types of maintenance strategies applied to maintain facilities and a relationship between the types of maintenance strategies implemented and end user satisfaction was determined [
41].
Shohet et al. (2003) analysed the maintenance incidence in a hospital through a survey [
42]. The communication and low voltage system, condition exterior envelope, interior finishing, water and waste-water, and HVAC were in deteriorating condition.
Maintenance costs throughout the useful life of a facility are very important when choosing the appropriate HVAC system to be installed in healthcare buildings. The central equipment show lower maintenance costs than partial systems [
43]. The annual energy saving through monitoring and control procedures [
44] are estimated between 5% and 15% according to the International Performance Measurement and Verification Protocol (IPMVP). The maintenance costs represent between 2% and 10% of the original investment on equipment, depending on the complexity of the system [
45].
Economic and environmental impact of energy saving was determined through maintenance engineer interviews.
Figure 6 shows the potential average energy saving per built surface area (m
2) through the optimization of the maintenance management in healthcare buildings with less than 5000 m
2 (no beds) and hospitals larger than 5000 m
2 (with beds). An annual average energy saving of 0.45 kWh and 0.50 kWh per built surface area (m
2), with a payback less than one year was achieved.
A series of energy-saving measures were used, including the development of a tailor-made maintenance plan for each hospital, implementation of predictive maintenance techniques, processes for monitoring and control of facilities, and the usage of qualified labour.
3.7. Thermal Insulation Improvement
In a building of more than 20 years, it is estimated that, with thermal rehabilitation, a saving of 50% of the energy consumed for heating and/or cooling [
46] could be achieved. A suitable thermal insulation can be a significant annual savings because it minimizes energy losses and air leakage from the building.
With the objective of determining the positive economic and environmental impacts thanks to thermal insulation improvement, the annual average saving and investment for the whole set of buildings was quantified for a three-year period.
Figure 7 represents the potential average energy saving per built surface area (m
2) through the upgrade of the thermal insulation improvement in healthcare buildings with less than 5000 m
2 (no beds) and hospitals larger than 5000 m
2 (with beds). A potential average saving between 0.65 kWh and 0.85 kWh per built surface area is observed, in a payback period less than nine years.
The proposed measures include the following actions: increasing the insulation level of roofs, sealing doors and windows to prevent infiltrations, installing blinds to reduce direct solar radiation, installing overhangs, replacing single glazing with double glazing, and applying protective glazing films. The main thermal losses in hallways, waiting rooms, and corridors were observed to occur when access doors remained open, provided that the most usual type of access to healthcare centres consists of windshield partition doors, a system that loses effectiveness as doors might even remain open during the busiest periods in the building.
3.8. Optimal Sizing of Buildings
Garcia Sanz-Calcedo et al. (2014) analysed the energy impact, determining it to be the incorrect dimension of a healthcare centre [
47] and determined the optimal ratio between the area per user and the number of users. For a smaller number of users, more space is needed for each. This is because there are certain healthcare units that need a minimal space independently of the number of users. It is possible to achieve annual savings by optimizing the built surface area.
In order to quantify the economic and environmental impact from energy saving by optimizing building sizing, a total of five hospitals and 30 healthcare centres were analysed. In this study, those over-dimensioned zones were identified by applying standard correlations between the area per user and the number of users.
Table 1 shows the potential average energy saving per built surface area (m
2), through the optimal sizing of buildings for healthcare buildings of less than 5000 m
2 (no beds) and hospitals larger than 5000 m
2 (with beds).
Table 1 shows that it is possible to obtain a mean saving value between 0.24 kWh and 0.30 kWh per built surface area in a four-year payback period.
4. Discussion
The above results show that it is possible to save a large amount of energy in healthcare buildings in Spain. The application of efficient energy saving techniques would decrease the global energy intensity and harmful gas emissions into the atmosphere.
In the healthcare sector there are buildings that consume great quantities of energy, so the energy management in healthcare centres will not only help to find a solution to reduce the energy intensity if not to also benefit the Spanish Health System, then economic reasons can be used in improving the medical attention of patients.
Several energy saving measures have been found to be easily implemented without the need of investment, including an efficient management of the buildings and improvement of the electricity contract conditions. Therefore, they should be implemented immediately.
For those energy measures that require an investment, finance viability and payback time must be taken into account. On the other hand, since LEDs are more efficient lighting systems and require a shorter payback time, they should be considered as well.
Local subsidies are also interesting in order to introduce saving measures, particularly those related to renewable energy in buildings; the implementation of renewable energies has proved to be an appropriate strategy in order to reduce gas emissions into the atmosphere. However, at present, Spain does not offer the possibility to incorporate the surplus energy into to the public grid. Therefore, it is necessary to design these facilities with a self-consumption purpose, based on their annual operative period.
Building design, efficient thermal insulation, and adequate sizing of buildings are key factors to keep in mind in future healthcare construction projects. These measures, thus, guarantee the well-being and satisfaction of the staff, patients, and managers.
The energy system of a healthcare building is very complex and must strictly respect the regulations. The indoor climatic conditions, ventilation, and lighting level must be determined by medical activities [
48]. Specific measures to improve the energy efficiency of a particular building should consider climatic and local conditions, the indoor climate environment, and amortization in terms of both economic and environmental aspects.
Healthcare engineering plays a role of growing importance in almost every aspect of healthcare, and it will also be a major factor that advances healthcare [
49]. Healthcare engineering professionals will face major challenges associated with issues, such as the continued rise in healthcare costs, the quality and safety of healthcare, management of common diseases, and the impact of high technology (biomedical, information, etc.).
The results of this study are extrapolated to similar buildings with limitations due to the wide variety of healthcare building designs mainly based on architectural conception, climate conditions, and interior facilities. Future developments must focus on: (i) the development of healthcare infrastructures that use renewable energies; (ii) implementation of Healthcare 4.0 technologies; and (iii) making progress towards smart communities. Additionally, a reference set of indicators must be produced in order to evaluate energy consumption in a given healthcare building. In this manner, saving and efficiency energy policies could be implemented in the sector.
5. Conclusions
Economic and environmental impacts of energy saving in healthcare buildings were quantified in this study. From the research, we can conclude that it is possible to save up to 8.60 kWh/m2 per year in a healthcare building under 5000 m2 and no beds, which represents an expense of 1.55 €/m2, and an approximate annual emission of 6.88 kg of CO2 into the atmosphere.
Potentially, a healthcare building larger than 5000 m2 is able to save up to 6.88 kWh/m2 per year, which represents an expense of 1.247 €/m2, and an annual emission of 4.82 kg of CO2 into the atmosphere, approximately.
To sum up, in a given healthcare building of 30,000 m2 of built surface area, it is possible to obtain an annual saving of up to €37,152, compared to €6192 in a 4000 m2 building.
It has become evident that a periodic energy audit is an appropriate strategy to optimize real energy consumption in healthcare buildings. Furthermore, these inspections are useful to prioritize those measures needed to reduce operating costs and energy consumption.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}