1. Introduction
1.1. Background
Robotic technology has been introduced as a type of minimally invasive surgical approach to reducing the physical and economic burden on patients. The novel operation method using robotic technology is expected to reduce the physical burden on surgeons, and to achieve more accurate operations that are difficult to perform under conventional conditions. One of the surgical fields in which this robotic technology is expected to be introduced is the pediatric surgical field. In pediatric surgery, patients ranging from newborn babies to children who are approximately 15 years old are treated. In particular, treatment during the newborn period is important because it can suppress the onset of acquired symptoms. However, the insertion of a hand by the surgeon into the body of a newborn baby is difficult due to the small size of the patient’s body and the space available for treatment. In addition, this operation makes it difficult because the target organs of newborn babies are very soft, fragile, and underdeveloped when compared with those of adult patients. Hence, a procedure in pediatric surgery is required to carry out delicate movements within a restricted space. To solve this problem, robotic technology for pediatric surgery is required, given that the robot can miniature the size of its own mechanism in addition to performing an accurate movement using a control system.
Commonly used surgical instruments are designed to treat adult patients; thus, there is a critical problem in that the instruments are as large as the tools used for treatment in pediatric surgery. Therefore, the da Vinci
® Surgical System (Intuitive Surgical Inc.) was developed as a clinical application robot. In the case report about the da Vinci
® Surgical System used in pediatric endoscopic surgery, Meehan and Sandler [
1] and Meehan [
2] reported that complex procedures can be carried out by surgeons using a surgical assisted robot, and that the application of robotic technology to pediatric surgery is effective. In addition, compared with conventional laparoscopic surgery, the effectiveness of the robot was reported regarding the three-dimensional (3D) high-quality vision, advanced instrument movement, and improved ergonomic position of the surgery in the field of pediatric surgery [
3,
4]. Moreover, the advantages to the surgeon’s intuitive and delicate procedure were presented with respect to the multi-degree-of-freedom mechanism of the surgical tool, the scaling function, and the operative field obtained using a 3D image.
By taking advantage of the surgical assisted robot, the burden on the surgeon can be reduced, even in a pediatric environment with a small surgical workspace. In addition, the patient can undergo treatment in the same manner, irrespective of their physical constitution. However, given that the da Vinci
® Surgical System was also developed for adult patients, it is difficult to directly apply this robot to pediatric surgery. The size of the surgical instrument is excessively large when this device is applied to newborns and infants. Moreover, it was highlighted that the following issues have a significant influence on the treatment outcome: the limitation of the surgical tool’s operation [
3,
4,
5], the obstruction of endoscopic vision [
2], and the position of trocars [
6]. As one of the commercial examples, the Endo Wrist
®, which has a forceps diameter of 5 mm, was developed for the da Vinci
® Surgical System to solve these drawbacks as a surgical tool for pediatric surgery. However, Najmaldin reported that the size of the surgical workspace slightly exceeded that of the workspace using surgical tools for adult surgery due to structural problems [
7]. Candela et al. performed the verification of the safety and accuracy of the Neuromate
® stereotactic robot for deep brain stimulation in childhood [
8].
In related works concerning robotic instruments, a forceps manipulator using a pneumatic soft actuator for a bending joint to solve wire-driven mechanism problem and magnetic resonance (MR)-compatible tools to maintain surgical accuracy and safety for pediatric bone biopsy were developed [
9,
10]. Fujii et al. [
11] and Tagazawa et al. [
12] focused on developing surgical tools for pediatric surgery, and reported on the handling problem of a suturing needle. In related works about surgical workspace creation, Sun et al. developed a da Vinci
® Surgical System simulator and used it to identify a suitable workspace based on the trocar point on the human body [
13,
14]. Using this system, they reported that a suitable position for the surgical robot can be calculated for individual patients, which includes pediatric surgery patients. Nouaille et al. studied the modeling and geometrical validation of surgical assistance tools [
15] and demonstrated that the configuration of surgical robots can be verified with respect to a mechanical structure. Sun and Yeung considered that the placement of trocars is critical when creating a surgical workspace, and then conducted research to verify the optimal trocar position for the adult environment [
16]. In related works regarding the size of surgical instruments, those instruments with diameters of 3 to 8 mm have been verified for pediatric surgery [
17,
18,
19,
20]. From these results, it has been reported that the effectiveness varies depending on the case used.
1.2. Previous Works
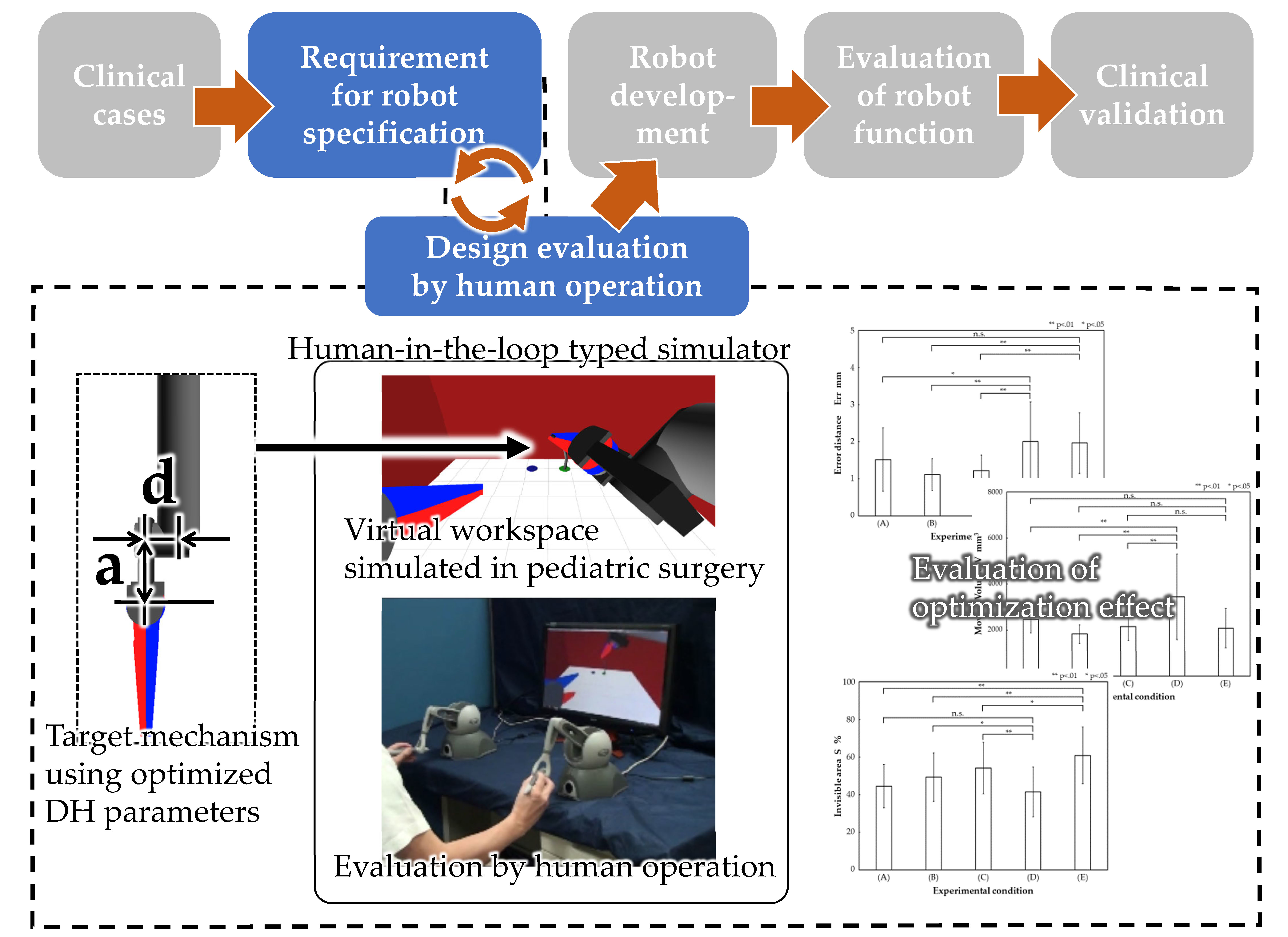
To apply a surgery-assisted robot to pediatric surgery, two drawbacks must be solved, namely, the movement volume and the lack of vision field information. These drawbacks are factors that affect human operation. In the conventional development method for a robot, a scrap and build method is adopted, in which a prototype is produced and evaluated repeatedly. In the case of development using this method, the robot is manufactured as a real machine and then a human evaluation is carried out using the robot. It is difficult to manufacture a surgical assisted robot in the field of pediatric surgery using the conventional development method, taking into account the abovementioned limitations for the human evaluation carried out after developing the actual machine. Therefore, a design method was developed to obtain a surgical assisted robot that could be applied to a narrow surgical workspace with a decreased burden on the surgeon during operation [
21]. In that study, a human-in-the-loop type simulator was constructed to reproduce a virtual surgical workspace in which a surgeon could handle the designed robot in real time. In the surgical robot’s development process, this simulator was proposed for use in the design stage (
Figure 1). Using this simulator, Kawamura et al. focused on the behavior of the tip of the forceps and measured the manipulability of each joint of the forceps manipulator to verify the ease of movement of the mechanism when used in virtual space. It was confirmed that the load applied to the forceps mechanism differs depending on the procedure [
22]. Seno et al. verified the operational influence of the forceps manipulator from the perspective of differences in the tip mechanism on surgical procedures [
23]. Based on the results, it was confirmed that the difference in the mechanism resulted in a change in the forceps tips’ trajectory. In addition, it was also confirmed that the distance between the joint for the bending movement and the next joint toward the tip had an influence on the accuracy of the needle handling and the workspace when carrying out a procedure involving needle insertion.
1.3. Objectives
When carrying out the needle-hooking operation, the surgeon achieves needle handling using the movement of the wrist, given that the suture needle is curved. The wrist joint of the forceps manipulator plays an important role in the development of a master-slave control-type surgical assisted robot handled by a surgeon. Therefore, it was considered that an easy-to-use robot could be created by optimizing the mechanical design parameters based on the information related to the movement of this part by the surgeon. In the previous research studies [
21,
22,
23,
24], the needle-hooking motion used for esophageal anastomosis was examined during the application of a surgical assisted robot to an assumed congenital esophageal atresia procedure. The aim of this study was to verify the influence on the needle-hooking motion in a procedure that imitated esophagus anastomosis in congenital esophageal atresia using the forceps manipulator, optimizing the mechanical parameters of the tip joint obtained in the previous research [
24]. Moreover, the effectiveness of the design optimization of the forceps manipulator based on the human operation was verified.
2. Materials and Methods
2.1. Experimental Conditions
In this study, the virtual environment that assumed a congenital esophageal atresia procedure in pediatric surgery was constructed using the surgical workspace reproduction simulator developed in our previous works [
21]. From a discussion with a pediatric surgeon, we learned that it was necessary to carry out treatment within a very narrow workspace of 40 × 40 × 50 mm for congenital esophageal atresia. In this experiment, the 40 × 40 × 50 mm workspace was reproduced by arranging the virtual wall on the left, right, and back side under the virtual environment (
Figure 2).
To define the coordinate system for the robot, the left and right pivot points (
PR and
PL) were set, in addition to the initial coordinates of the left and right surgical tooltips and the initial posture (
MR and
ML), the coordinates of the endoscope tip position (
E), and the insertion angle of the endoscope (θ) with respect to the floor plane (
Figure 3). The forceps manipulator was set to 5 mm in diameter in this experiment. The detailed values are shown in
Table 1 and
Table 2.
The surgical procedure of congenital esophageal atresia, as targeted in this study, includes the suturing task of the upper esophagus and the lower esophagus, the ligation task, and the everting task of the esophagus for the placement of a needle on the back. Among these tasks, the suturing task in the upper esophagus and lower esophagus is considered difficult, and it is desirable to apply a surgical assisted robot. Therefore, in this experiment, the operation of the needle placement on the target point shown in the virtual environment (
Figure 2) was used as the procedure of this experiment. As shown in
Figure 2, the target point was set as target point (A) when inserting the needle, and target point (B) when extracting the needle.
The parameters for the target points were set. In this experiment, the radius r of the target point and the distance l (
Figure 2) between the target points are shown in
Table 3. In congenital esophageal atresia, it is necessary to provide 8–12 sutures for the upper esophagus with diameters of approximately 10 mm, and for the lower esophagus with diameters of approximately 5 mm. Therefore, the radius r of the target point was set to 1 mm. The distance l between the target points was set as 8 mm, based on a discussion with a pediatric surgeon. Moreover, Geomagic Touch
™ (3D Systems, Rock Hill, SC, USA) was used as the operation input device, and force feedback was not provided in this experiment. Considering a task within a very narrow environment, the ratio of the operation input amount to the operation amount was set as 10:1. In this experiment, the computer specification was as follows: central processing unit (CPU) with Intel Core i7 2.8 GHz, 16.0 GB of memory, Windows 7 operating system (OS) (Microsoft Corporation, Redmond, WA, USA); graphics processing unit (GPU), nVidia Quadro FX 580 (NVIDIA Corporation, Santa Clara, CA, USA) and display using OpenGL Version 3.3.0 (Khronos Group, Beaverton, OR, USA) and GLFW Version 2.6 (
https://www.glfw.org).
2.2. Mechanical Parameters
In this experiment, five mechanisms were selected using the results of the Pareto optimal solution in the previous research [
24]. In this optimization calculation, the moving volume and the invisible area rate were used. The moving volume was the volume of the range through which the forceps moved in the body. The invisible area rate was the ratio of the amount that was not actually seen to the situation where the blade portion at the tip of the forceps was all visible [
24].
The following three types of mechanisms were selected as mechanisms that satisfied the Pareto optimal solution. In the Pareto frontier, Condition (A) denoted the mechanism that minimizes the invisible area rate, Condition (B) denoted the mechanism where the invisible area rate and the moving volume are intermediate, and Condition (C) denotes the mechanism that minimizes the moving volume. In addition to these mechanisms, the mechanisms that did not satisfy the Pareto optimal solution were selected. We confirmed that the variables used for optimization were in a trade-off relationship with each other in the previous study [
24]. Hence, we selected the parameter that maximized the moving volume (Condition (D)) and the parameter that maximized the invisible area rate (Condition (E)). Condition (D) was the mechanism with a = 10.0 and d = 5.0, which had the largest operating range before optimization. Condition (E) was the mechanism where a = 0 and d = 0, which had the largest invisible area rate.
Table 4,
Table 5,
Table 6,
Table 7 and
Table 8 present the values of the Denavit–Hartenberg (DH) parameters set to reproduce these five types of mechanisms. As for the arrangement of the degrees of freedom, all five types of mechanisms were arranged as shown in
Figure 4.
2.3. Subjects
Four subjects participated in this experiment to verify the effectiveness of the mechanical design parameter optimization for the forceps manipulator. These subjects included a pediatric surgeon and three non-surgeons. In this experiment, all the subjects received an explanation of the procedures and possible risks of the study, after which they provided written informed consent. This study was conducted in accordance with the Declaration of Helsinki.
2.4. Experimental Methods
The mechanical design was optimized based on the movement of the tip of the forceps manipulator when the suturing task was carried out. Therefore, the effect on the suturing motion was verified. In this experiment, each subject carried out the needle-hooking task in the virtual environment shown in
Section 2.1. using the forceps manipulator with the DH parameters shown in
Section 2.2.
In this experiment, the needle-hooking task was set as a task to manipulate a needle from the entry point (A) to the exit point (B), as shown in
Figure 2. Each subject carried out five operations for each mechanism.
The errors at the exit point were compared when the needle setting operation was carried out. In this experiment, the error distance Err (
Figure 5) was defined between the point passed on the floor by the needle tip and the center of the exit point. The effectiveness as indexes in the optimization of mechanical design was verified by measuring the moving volume and invisible area rate, and by comparing them with each other. The moving volume and invisible area rate were measured using the same method as in the previous work.
For an analysis of these results, the accuracy at the exit point under the conditions using each optimization mechanism (Conditions (A), (B), and (C)) was compared with that under the conditions using each non-optimization mechanism (Conditions (D) and (E)) using the Wilcoxon signed-rank test. The results of the moving volume and invisible area rate under the condition using each optimization mechanism (Conditions (A), (B), and (C)) were also compared with those under the conditions using each non-optimization mechanism (Conditions (D) and (E)) using the Wilcoxon signed-rank test. For this study, p-values of <0.05 were considered statistically significant. All statistical analyses were performed using the R Version 3.6.0 (R Foundation for Statistical Computing, Vienna, Austria).
3. Results
3.1. Accuracy of Needle-Hooking Task
Figure 6 presents the results of the error distance at the exit point and the comparison results for each condition. The vertical axis indicates the error distance, and the horizontal axis indicates the type of mechanism used. From the results, Condition (A) was 1.52 mm (SD 0.85), Condition (B) was 1.12 mm (SD 0.42), Condition (C) was 1.22 mm (SD 0.42), Condition (D) was 2.00 mm (SD 1.06), and Condition (E) was 1.96 mm (SD 0.82). In comparison with Condition (D), a significant difference was confirmed between Condition (A) at
p < 0.05 and Conditions (B) and (C) at
p < 0.01. In comparison with Condition (E), a significant difference was confirmed between Conditions (B) and (C) at
p < 0.05. Based on the results, an improvement in the accuracy of the needle-hooking task was observed. However, no significant differences were observed for Condition (A) when compared with Condition (E).
3.2. Result of Moving Volume
Figure 7 presents the results of the moving volume of the tip of the forceps manipulator in the body and the comparison results for each condition. The vertical axis represents the moving volume, which indicates the operating range, whereas the horizontal axis represents the type of mechanism used. From the results, Condition (A) was 2473 mm
3 (SD 590), Condition (B) was 1835 mm
3 (SD 399), Condition (C) was 2160 mm
3 (SD 603), Condition (D) was 3446 mm
3 (SD 1858), and Condition (E) was 2081 mm
3 (SD 855). In comparison with Condition (D), a significant difference was confirmed at
p < 0.01 under all conditions. However, in comparison with Condition (E), no significant difference was observed under all conditions. Based on the results, it was considered that the optimization was less effective if the moving volume was small before the optimization. Moreover, it was suggested that the effect was significant when the mechanism with a large volume was optimized.
3.3. Result of Invisible Area Rate
Figure 8 presents the results of the invisible area rate of the tip of the forceps manipulator and the comparison results for each condition. The vertical axis indicates the invisible area rate, and the horizontal axis indicates the type of mechanism used. From the results, Condition (A) was 44.5% (SD 11.6), Condition (B) was 49.3% (SD 12.9), Condition (C) was 54.1% (SD 13.7), Condition (D) was 41.4% (SD 13.3), and Condition (E) was 60.9% (SD 15.0). In comparison with Condition (D), a significant difference was confirmed under Condition (B) at
p < 0.05 and Condition (C) at
p < 0.01; however, no significant differences were confirmed under Condition (A). In comparison with Condition (E), a significant difference was confirmed under all the conditions. In particular, significant differences were observed at
p < 0.01 under Conditions (A) and (B), and at
p < 0.05 under Condition (C). Based on the results, it was highly probable that the effect for the invisible area rate would be confirmed, even if the invisible area rate was large or small before optimization.
4. Discussion
From the experimental results presented in
Figure 5, it was confirmed that the needle handling accuracy could be improved when the needle-hooking task was carried out using the optimized conditions (Conditions (A), (B), and (C)). Thus, the optimization of the mechanism with the invisible area rate of the tip of the forceps manipulator and the moving volume as variables was suggested.
Among the conditions compared in this experiment, no significant difference was found when Conditions (A) and (E) were compared, as shown in
Figure 6. From the results in
Figure 7 and
Figure 8, a significant difference in the invisible area rate was not observed when comparing Conditions (A) and (D). Moreover, a significant difference in the moving volume was confirmed. In contrast, a significant difference was confirmed in the invisible area rate when compared with Condition (E). However, no significant difference was confirmed in the moving volume.
Condition (D) was the mechanism with the largest moving volume under all the conditions. Although the invisible area rate was similar between the compared conditions, it was considered that the operation accuracy was improved by the ease of operation, given that the moving volume of Condition (A) was reduced by optimization.
In contrast, Condition (E) was the mechanism with the largest invisible area rate. The invisible area rate under Condition (A) was improved by optimization; however, it was larger than that under Condition (E). Moreover, no significant difference was confirmed when comparing the moving volumes of Conditions (A) and (E). Based on the results, it was considered that the improvement of the needle handling accuracy was not confirmed because the difficulty of the operation was not resolved, given that the improvement of the moving volume was not sufficiently achieved.
Condition (A) was the mechanism in which the invisible area rate was the smallest among the Pareto optimal solutions. Hence, it was considered that the visual field information of the tip of the forceps manipulator could be obtained clearly when performing the task under Condition (A).
In the case where such visual field information can be clearly obtained, the linear trajectory of the tip of needle from the initial position to the insertion point was confirmed. When the needle was moved linearly and hooked at the target point, as shown in
Figure 9, the visual field information of the needle was blocked by the near side of the surgical tool.
If the visual field information of the needle was blocked, the operator could not recognize the motion of the needle. As a result, the accuracy of the needle hooking at the exit point decreased. In addition, the variations occurred easily.
Therefore, it was considered that the error distance Err under Condition (A) was not significantly shortened when compared with the mechanism that did not satisfy the Pareto optimal solution. Based on the above, it is necessary to consider the blocking ratio of the tip of the surgical tool and the visual field information of the needle. However, this study has potential limitations. The effectiveness of the optimization we described in this paper is based on the difference in the length of the tip joint of forceps manipulator and the motion of the needle-hooking task. For designing, the other DH parameters should be verified. For developing, the physical size of the instruments should be optimized. The surgical robot is also required to apply other surgical tasks for congenital esophageal atresia in pediatric surgery. For example, the surgical technique involves the cooperation of the left and right forceps manipulator. Given that the required motions differ between the left and right forceps manipulator, it is necessary to carry out the optimization for each mechanism of the manipulator based on the task required by each manipulator. Thus, in the future, we will optimize and evaluate under those conditions. In addition, we will also develop the quantitative evaluation method for the operability of surgical robot to select the parameters suitable for the surgeon’s operation. In this experiment, the number of subjects was only four, including the non-surgeons. To optimize and derive mechanisms more suitable for pediatric surgery, we must perform this with the pediatric surgeons, as well as increase the number of subjects.
5. Conclusions
In this study, a design method was established using a human-in-the-loop type simulator for the development of a surgical robot applicable to pediatric surgery. In previous research, the focus was on the moving volume and invisible area rate when carrying out the procedure in a narrow workspace. In addition, the tip mechanism of the forceps manipulator commonly used when suturing with a needle was optimized.
The aim of this study was the verification of the optimization of the mechanical parameters based on human operation for needle-hooking operations in pediatric surgery. A needle-hooking task was carried out by four subjects with five types of mechanisms using the results of the Pareto optimal solution obtained in the previous research. In addition, the accuracy of the needle tip manipulation was verified.
The accuracy was defined as an error distance between the needle tip position and the exit point. It was confirmed that the accuracy was higher when operating the mechanism that satisfied the Pareto optimal solution than when operating the mechanism that did not satisfy the Pareto optimal solution.
Given that the operation was performed using the movement of the forceps manipulator in the direction of the arm, the rotational movement around this axis was restrained, and the moving volume decreased. Therefore, it was considered that the accuracy of the hooking was improved.
Based on the results, the verification of the moving volume and invisible area rate, which represent one of the critical problems in the field of pediatric surgery, was conducted in the virtual environment at the design stage of the actual machine. Moreover, the optimization of the mechanism of the surgical tool suitable for the target operating environment was considered effective.
However, in this experiment, the targets for which the effectiveness was evaluated, which included the targets for optimization, were limited to only the hooking motion. Moreover, other procedures were not verified.
When considering the actual surgical technique, there are other techniques to be considered, in addition to the technique that involves the cooperation of the left and right forceps manipulator. Given that the required motions differ between the left and right forceps manipulator, it is necessary to carry out the optimization for each mechanism of the manipulator based on the task required by each manipulator. Therefore, it was considered necessary to carry out optimization based on the cooperated operation and its evaluation index, to derive the mechanism of the surgical tool that is more suitable for pediatric surgery.
In future research, the optimization will be carried out, and the effectiveness evaluation of the mechanism for the procedures that require both hands will be verified.

 ,
, 










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}