Investigation of an Explosion at a Styrene Plant with Alkylation Reactor Feed Furnace

Abstract
:1. Introduction
2. Accident Review
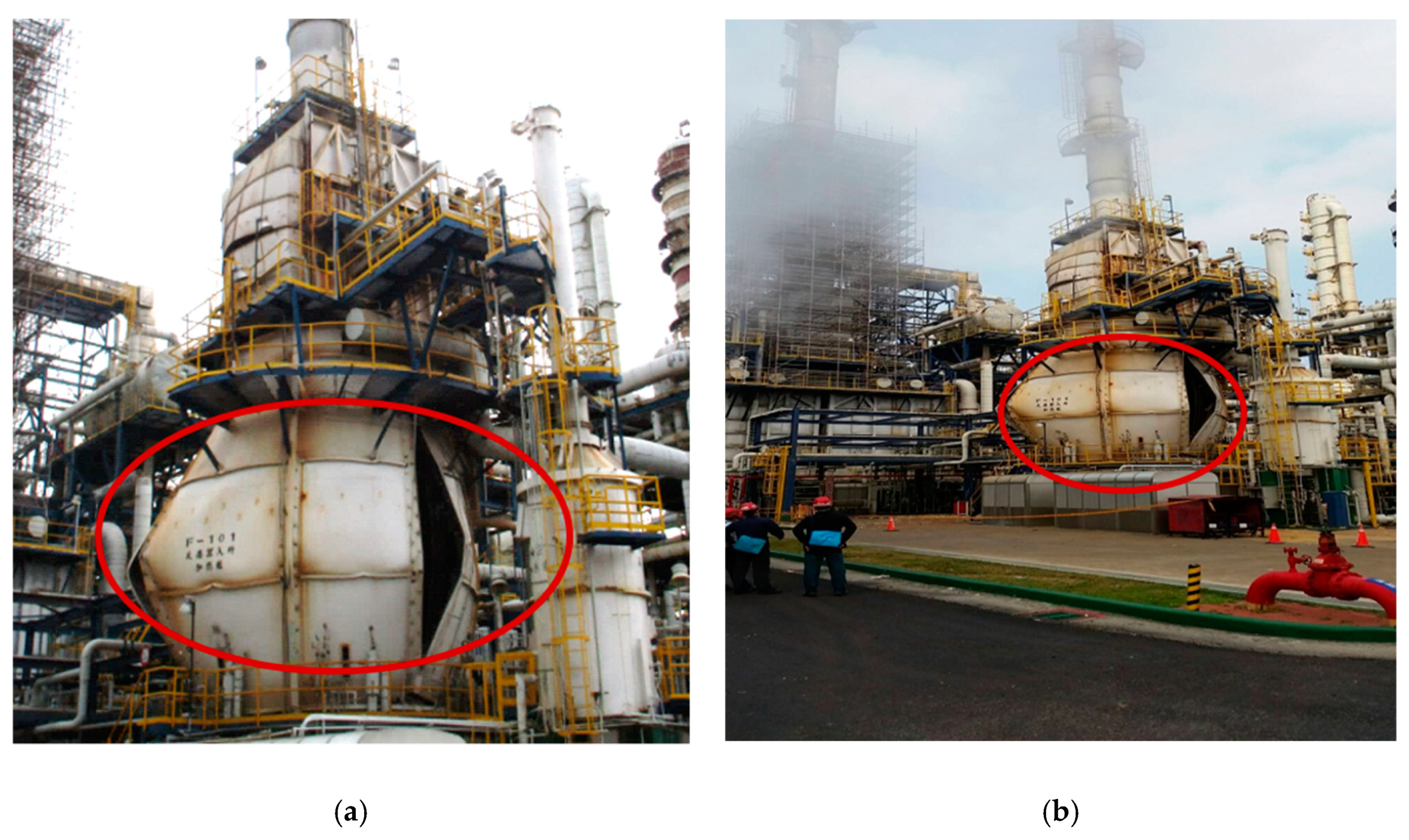
2.1. Accident Description
2.2. Process Description
3. Accident Investigation Analysis
3.1. Analysis Procedures
- Hazard identification: First, identify all process activity and find the accident hazard causes and consequences, then confirm existing protective measures.
- Assessment: Use qualitative or quantitative analysis method to implement risk assessment.
- Risk control: According to the risk assessment results compare with the critical risk value, then take control measures for risk reduction.
3.2. Fault Tree Analysis (FTA)
3.2.1. What is FTA
3.2.2. FTA Effects
- Applies deduction methods to figure out the possible cause of the system failure.
- Provides a clear graphical method, various easy ways to understand, and to count system failure.
- Points out the weaker links of the operating system.
- Renders system tools to evaluate system improvement strategies.
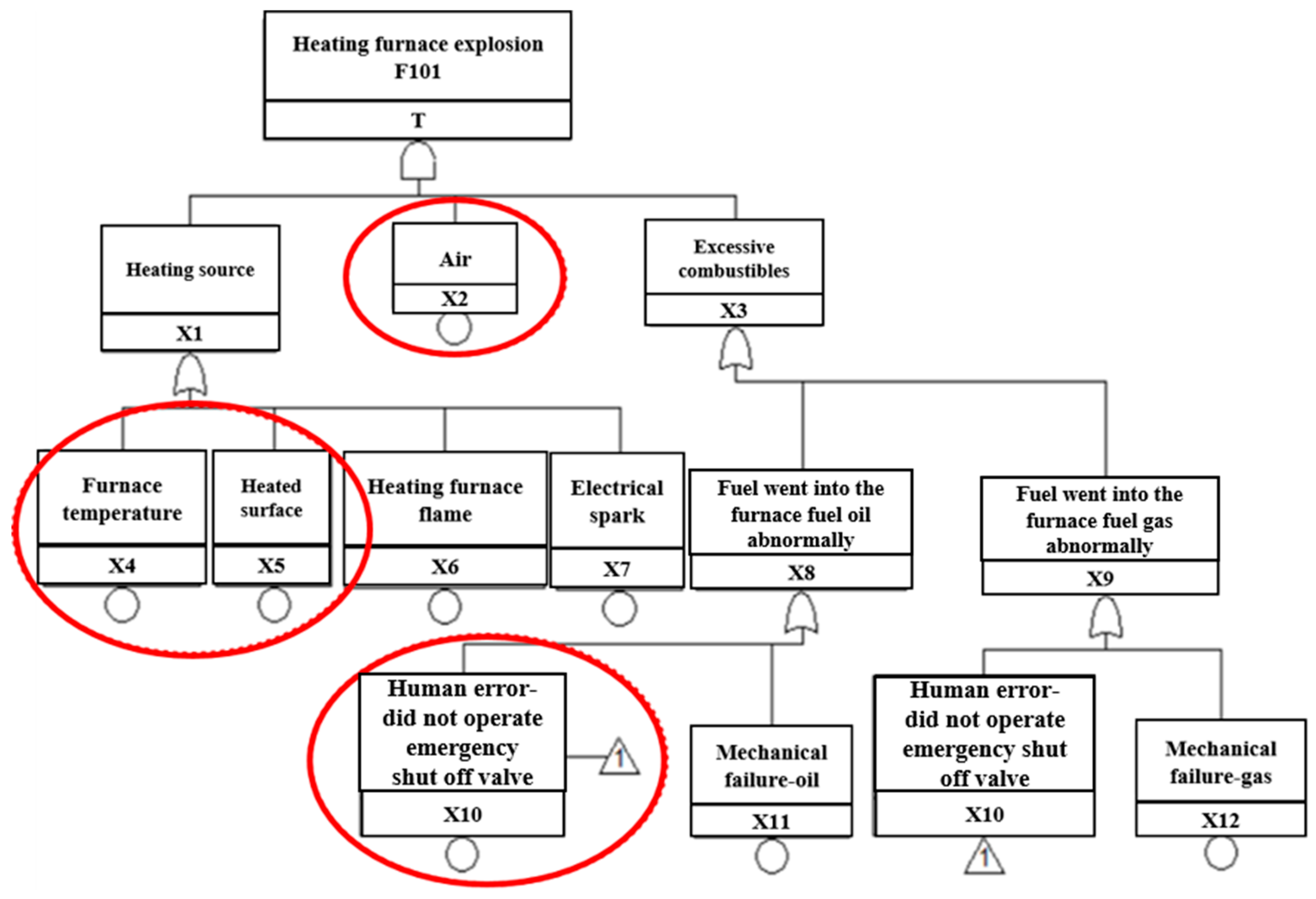
3.2.3. Fault Tree Establishment
- X1
- Heating source: One of the possible causes of the furnace accident
- X2
- Air: One of the possible causes of the furnace accident
- X3
- Excessive combustibles: One of the possible causes of the furnace accident
- X4
- Furnace temperature: One of the possible causes of heating source
- X5
- Heated surface: One of the possible causes of heating source
- X6
- Heating furnace flame: One of the possible causes of heating source
- X7
- Electrical spark: One of the possible causes of heating source
- X8
- Abnormal fuel flow into the furnace: Excessive combustibles (oil) in the furnace
- X9
- Abnormal gas flow into the furnace: Excessive combustibles (gas) in the furnace
- X10
- Human-error: Did not operate emergency shutoff valve.
- After the heating furnace (F101) explosion, the operator did not shut down the F101 according to the standard operating procedure (SOP); then the atomization of fuel and gas continued into the furnace, resulting in flash over under the high temperature.
- In the fuel adjusting period, the furnace produced black smoke. At this point, on-site staff discovered the flame extinguished and performed the adjustment, then determined the fuel gasification and caused the ignition, resulting in other burners flame extinguishing instantly.
- The on-site staff response time during the abnormal situation was too short. The staff lacked awareness of the safety of the heating furnace operation and was unwilling to shut down the heating furnace (F101), nor did the staff perform the emergency stop procedure.
- Another reason might be that the staff was unfamiliar with the operating environment and equipment.
3.3. Qualitative Analysis
X12 + X2·X7·X10 + X2·X7·X11 + X2·X7·X12
3.3.1. Importance (I) of the Basic Events
- When abnormal status happens, reduce the air concentration in heating furnace by inert gas. Then, the previous installed emergency shutdown valve would cut off fuel gas from entering the heating furnace.
- Strengthen the management of heat sources, such as hot work and static electricity.
- Enhance the improvement of personnel operation capability and equipment reliability.
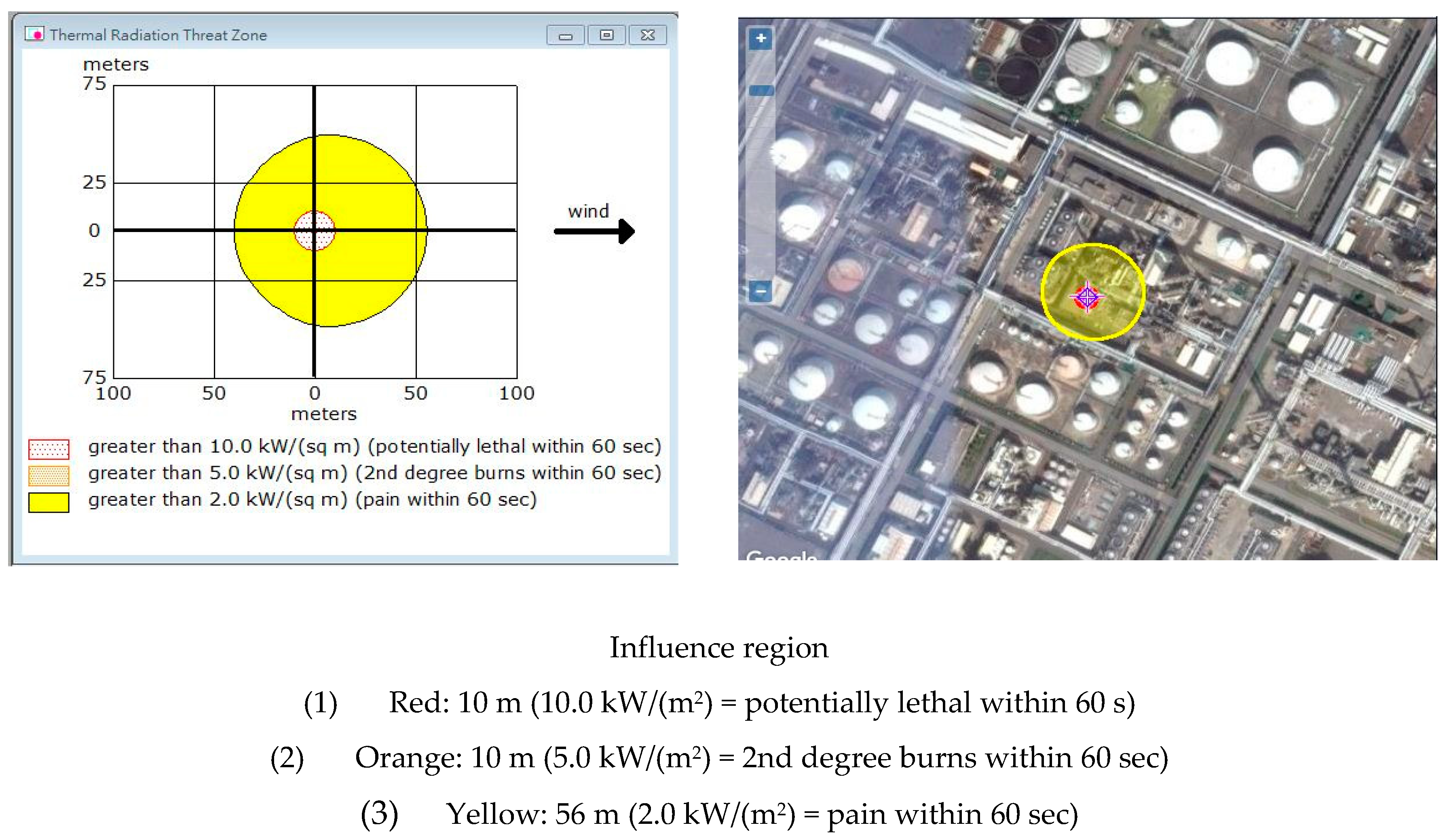
3.3.2. ALOHA Simulation Analysis
4. Results of Analysis and Discussion with the Method of Improvement
4.1. Results of Analysis
4.2. Improvement Strategy
4.2.1. Improvement of Engineering Approach
- Mechanical and equipment integrity (MI)
- Remake the furnace body and check the status of the attached equipment as well as pipelines.
- Monitor equipment integrity: Record maintenance history and regularly replace equipment components.
- Add safety improvement advice, replace fuel gas cock valve with additional limited type switch, regulate all gas burners into the burner, as all could not be reset when the fuel valve was not fully closed.
- Inherent safety design (ISD)
- (a)
- Oxygen detector
- In the original design, there was only one oxygen detector. When the process was running, the offset anomaly could not be found immediately. One oxygen detector was added to improve the O2 detection reliability of the equipment.
- Installed the other oxygen detector which was at the same height as the existing oxygen detector location; immediately notified the operator to maintain and calibrate it if the oxygen concentration difference was more than 1% original setting value.
- Checked the detector was vetted every month, which was using zero and full-scale calibration by standard gas.
- (b)
- Improvement of chimney baffle
- Made sure chimney baffle opening degree was controlled by distributed control system (DCS) in the original design. The signal was transmitted to the site controller to actuate the chimney baffle. The DCS could not detect the actual opening degree value of the chimney baffle in the field.
- Installed a positioner in the chimney baffle and transfer the actual opening degree value of the chimney baffle on site to the DCS. Then, compared the value of DCS to master the opening degree with the actual value on site, whether DCS was consistent with the actual opening degree value of the site.
- Improved flame detector setting position.
4.2.2. Improvement of Management Approach
- Rechecked the entire plant furnaces SOP, strengthen operators’ education and training.
- Established maintenance, check history, and check procedures.
- Pre-startup safety review (PSSR) for heating furnace (F101).
- Rechecked the PSSR of the heating furnace (F101). The PSSR covered four major aspects: Process, safety, and environmental protection (safety/fire protection/environmental protection), equipment (machinery) maintenance, and instrument equipment maintenance.
- Self-inspection by process and maintenance operators for the four major inspection items.
- A process hazard analysis for the heating furnace (F101). The recommendations should be implemented before startup, and modified facilities must meet the management of change requirements.
- Completed the training of each employee involved in operating a process.
4.2.3. Cost-effectiveness Analysis: As Low as Reasonably Practicable Sorting Analysis
- Safety and health guide
- Codes of practice
- Industry practice
- Manufacturer specifications and government regulations
- Compliance with international standards and codes
- Comparison with dangerous events in similar industries
- Further reduction of the cost of risk in proportion to the benefits obtained.
4.2.4. ALARP Sorting
- Rebuilt the heating furnace (F101) body and evaluated the damage status of the surrounding ancillary equipment and pipelines.
- Rechecked the furnace SOP.
- Improved worker education and training.
- Monitored equipment integrity: Recorded maintenance history and regularly replaced equipment components.
- Established maintenance, checked history, and followed procedures.
- Erected a gas feed interruption device.
- Installed a furnace combustion condition detection device.
5. Conclusions and Recommendations
- Units with different specializations must cooperate with each other to investigate accidents: Previous accident investigation reports biased in fire expertise should include chemical process and other background experts to investigate. To find the real root cause of an accident, we should establish an investigation team by accident procedure, and then take control measures to avoid the accident from happening again.
- To improve the operation safety of the equipment, including ISD, mechanical and MI.
- To develop procedures of MOC (management of change), when the heating furnace (F101) uses different fuels.
- To avoid increasing the risk of exchanging fuels (fuel oil and fuel gas), we suggest using a single fuel.
- To enhance the operators’ ability of response when the heating furnace (F101) abnormal situation occurs.
- To improve operator training and equipment regular maintenance.
- Before the heating furnace was opened, PSSR for F101 was divided into four major aspects: Process, (industrial safety/firefighting/environmental protection), equipment (mechanical) maintenance, and instrument as well as electrical section (safety) maintenance.
- Case exchanging experience should be promoted to the grassroots.
- Installing a system for nitrogen into the furnace to reduce the concentration of combustible gases.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ng, H.D.; Lee, J.H.S. Comments on explosion problems for hydrogen safety. J. Loss Prev. Process Ind. 2008, 21, 136–146. [Google Scholar] [CrossRef]
- Workplace Health, Safety and Compensation Commission (WHSCC) of New Brunswick. Accident Investigation Report on the Explosion and Fire at the Irving Oil Refinery, New Brunswick; The Commission: Fredericton, NB, Canada, 1999. [Google Scholar]
- Ranganathan, S.; Gillis, S. Oven Furnace and Dryer Explosion Incidents; Fire Protection Research Foundation: Quincy, MA, USA, 2016. [Google Scholar]
- Zhou, Y.; Zhao, X.; Zhao, J.; Chen, D. Research on Fire and Explosion Accidents of Oil Depots. Chem. Eng. Trans. 2016, 51, 163–168. [Google Scholar] [CrossRef]
- Large-Scale Petrochemical Supervision Meeting; Bureau of Industry, Ministry of Economic Affairs: Taipei, Taiwan, 2017.
- Babrauskas, V. Explosions of ammonium nitrate fertilizer in storage or transportation are preventable accidents. J. Hazard. Mater. 2016, 304, 134–149. [Google Scholar] [CrossRef] [PubMed]
- Hu, K.H.; Kao, C.S.; Duh, Y.S. Studies on the runaway reaction of ABS polymerization process. J. Hazard. Mater. 2008, 159, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Kao, C.S.; Duh, Y.S. Accident investigation of an ABS plant. J. Loss Prev. Process Ind. 2002, 15, 223–232. [Google Scholar] [CrossRef]
- ABS Powder Storage Tank (H701F) Flash Accident Report; Mai Lao PABS Plant of Taiwan Chemical Company: Yunlin, Taiwan, 2017.
- Kelly, B.D. Investigation of a hydrogen heater explosion. J. Loss Prev. Process Ind. 1997, 11, 257–259. [Google Scholar] [CrossRef]
- Siwek, R. Determination of technical safety indices and factors influencing hazard evaluation of dusts. J. Loss Prev. Process Ind. 1996, 9, 21–31. [Google Scholar] [CrossRef]
- Nedkova, S.; Lybchev, L.; Lybcheva, M.; Kolev, N. Human factor analysis in the risk management in technological processes and in A glass production plant. Sci. Technol. 2013, 3, 11–15. Available online: http://www.sustz.com/journal/VolumeIII/Number4/Papers/SabinaNedkova.pdf (accessed on 10 August 2018).
- Dugué, J. Fired equipment safety in the oil & gas industry. A review of changes in practices over the last 50 years. Energy Procedia 2017, 120, 2–19. [Google Scholar] [CrossRef]
- Mirza, N.R.; Degenkolbe, S.; Witt, W. Analysis of hydrogen incidents to support risk assessment. Int. J. Hydrogen Energy 2011, 36, 12068–12077. [Google Scholar] [CrossRef]
- Xue, Z.M. Research on FTA of fire and explosion in the crude oil gatheringtransport combination station. Procedia Eng. 2011, 11, 575–582. [Google Scholar] [CrossRef]
- Abuswer, M.; Amyotte, P.; Khan, F. A quantitative risk management framework for dust and hybrid mixture explosions. J. Loss Prev. Proc. Ind. 2013, 26, 283–289. [Google Scholar] [CrossRef] [Green Version]
- Halme, J.; Aikala, A. Fault tree analysis for maintenance needs. In Proceedings of the 25th International Congress on Condition Monitoring and Diagnostic Engineering, Huddersfield, UK, 18–20 June 2012; pp. 1031–1041. [Google Scholar] [CrossRef]
- Yasushi, N.; Rolf, L.; Philip, A. Fault tree analysis of system anomaly leading to red oil explosion in lutonium evaporator. J. Nucl. Sci. Technol. 1994, 31, 850–860. [Google Scholar] [CrossRef]
- Ruijters, E.; Stoelinga, M. Fault Tree Analysis: A survey of the state-of-the-art in modeling, analysis and tools. Comput. Sci. Rev. 2015, 15–16, 29–62. [Google Scholar] [CrossRef]
- Moreno, V.C.; Papasidero, S.; Scarponi, G.E.; Guglielmi, D.; Cozzani, V. Analysis of accidents in biogas production and upgrading. Renew. Energy 2016, 96, 1127–1134. [Google Scholar] [CrossRef]
- Fuentes-Bargues, J.L.; González-Cruz, M.C.; González-Gaya, C.; Baixauli-Pérez, M.P. Risk Analysis of a Fuel Storage Terminal Using HAZOP and FTA. Int. J. Environ. Res. Public Health 2017, 14, 705. [Google Scholar] [CrossRef] [PubMed]
- Siu, N.; Herring, J.S.; Lee, C.; Reece, W.; Byers, J. Qualitative Risk Assessment for an LNG Refueling Station and Review of Relevant Safety Issues; Idaho National Engineering and Environmental Laboratory: Idaho Falls, ID, USA, 1999.
- Mohammadfam, I.; Zarei, E. Safety risk modeling and major accidents analysis of hydrogen and natural gas releases: A comprehensive risk analysis framework. Int. J. Hydrogen Energy 2015, 40, 13653–13663. [Google Scholar] [CrossRef]
- Figueroa Jiménez, S.P.; Lombana Carmona, S.C.; Ruiz De La Cruz, I.L. Application of HAZOP, LOPA and SIL to the Alkylation Unit Catalyzed with Hydrofluoric Acid at Ecopetrol Refinery in Cartagena–Colombia; Mary Kay O’Connor Process Safety Center, Texas A&M University: College Station, TX, USA, 2015. [Google Scholar]
- Moonis, M.; Wilday, A.J.; Wardman, M.J. Semi-quantitative risk assessment of commercial scale supply chain of hydrogen fuel and implications for industry and society. Process Saf. Environ. Prot. 2010, 88, 97–108. [Google Scholar] [CrossRef]
- Linkov, I.; Bates, M.; Loney, D.; Sparrevik, M.; Bridges, T. Risk Management Practices-Cross-agency Comparisons and Tolerable Risk. In Climate: Global Change and Local Adaptation; Springer: Dordrecht, The Netherlands, 2011. [Google Scholar]
- Kletz, T.A. Looking beyond ALARP: Overcoming its limitations. Process Saf. Environ. Prot. 2005, 83, 81–84. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Date of Incident | Location | Specific Details | Explosion Details | Injuries/ Fatalities | |
|---|---|---|---|---|---|
| Cause | Consequence | ||||
| 2 November 2002 | Vernon, CA | Used for smelting lead | Weakened furnace wall (holes) compromised the integrity of the furnace | Explosion spewing hot lead slag and dust | 1 employee received 2nd and 3rd degree burns |
| 16 March 2004 | Cucamonga, CA | Electric arc furnace | Attempted maintenance on a water leak from the furnace, loud popping noise resulted in explosion | Explosion resulting in hot steam and flying debris | 1 severe injury, 2 minor burns and cuts |
| 10 March 2006 | Midlothian, TX | Melt shop furnace (steel) | Furnace was tilted forward to begin tapping when the hydraulic hose cylinder failed | Molten steel leaked out of slag door, slag pot overfilled and an explosion occurred | 1 employee was killed |
| 27 May 2007 | Coatesville, PA | Electric arc furnace | Molten steel caused a water leak to become superheated high-pressure vapor | Explosion, molten steel | 1 employee killed, 2 seriously burned |
| 29 November 2007 | Manchester, GA | Used to melt aluminum | Aluminum car rims were placed into the furnace, moisture was still on the rims and a violent explosion occurred | Explosion, molten metal | 1 fatality, 6 serious injuries |
| 21 March 2011 | Louisville, KY | Large electric arc furnace | Water leaked into furnace which caused an overpressure event | Explosion from overpressure that sent furnace contents spewing into air | 2 workers killed, 2 seriously injured |
| 21 September 2014 | Fairfield, AL | N/A | Workers were opening/closing a furnace valve that contained oxygen and hydrated lime, while the furnace was in operation | Fiery explosion | 2 workers killed, 1 critically injured |
| Date of Incident | Location | Equipment | Explosion Details | Injuries/Fatalities |
|---|---|---|---|---|
| 7 November 2006 | Mainland China | Furnace | During fuel gas into the furnace, causing the gas pipe of heating furnace to burst and explosion. | Equipment damage |
| 3 May 2008 | Mainland China | Furnace | Heating furnace tube coking. | Equipment damage |
| 6 March2017 | Taiwan SM plant | Furnace | In the diesel plant, during starting the furnace, the tube of furnace was cracked and led to explosion. | 4 seriously injured |
| 29 January 2018 | Taiwan Taoyuan Refinery | Furnace | In the diesel plant, during starting the furnace, the tube of furnace was cracked and lead to explosion. | No casualties Equipment damage |
| Factor | Meaning | Factor | Meaning |
|---|---|---|---|
| T | Heating furnace explosion | X1 | Heating source |
| X2 | Air | X3 | Excessive combustibles |
| X4 | Furnace temperature | X5 | Heated surface |
| X6 | Heating furnace flame | X7 | Electrical spark |
| X8 | Into the furnace fuel oil abnormally | X9 | Into the furnace fuel gas abnormally |
| X10 | Human errors—do not operate emergency shutoff valve | X11 | Mechanical failure—oil |
| X12 | Mechanical failure—gas |
| Basic Event Code | The Times of Occurrences in the MCS | Importance Sorting |
|---|---|---|
| X2 | 12 | 1 |
| X4 | 3 | 3 |
| X5 | 3 | 3 |
| X6 | 3 | 3 |
| X7 | 3 | 3 |
| X10 | 4 | 2 |
| X11 | 4 | 2 |
| X12 | 4 | 2 |
| Severity of Consequences | Description |
|---|---|
| 5 | Safety: One or more fatalities or permanent disabling injuries (PDIs) Environmental: Major impact, making the national news Economic: Losses greater than $10 million USD |
| 4 | Safety: PDIs, or serious injury to three or more people Environmental: Continuous large impact, making the local news Economic: Losses between $1 million and $10 million USD |
| 3 | Safety: Serious injury to one or two people, or minor injury to three or more Environmental: Moderate impact, must be reported to environmental agency Economic: Losses between $100,000 and $1 million USD |
| 2 | Safety: Minor injury to no more than two people. First aid. Environmental: Minor impact Economic: Losses less than $100,000 USD |
| 1 | Safety: No adverse health effects Environmental: No detectable impact Economic: Negligible economic impact |
| Likelihood of Occurrence | Description |
|---|---|
| 5 | The event has happened several times at the plant. Likelihood is more than once in 1 year. |
| 4 | The event has occurred at the plant and frequently in industry. Likelihood is between once in 1 year and once in 10 years. |
| 3 | Incident has occurred at the plant, but is not common in industry. Likelihood is between once in 10 years and once in 100 years. |
| 2 | Incident has occurred in industry. Likelihood is less than once in 100 years |
| 1 | The event has a remote chance of happening and is unheard of in industry. |
| Frequency of Occurrence (Likelihood) | Consequences (Severity) | ||||
|---|---|---|---|---|---|
| Catastrophic (5) | Major (4) | Serious (3) | Minor (2) | Incidental (1) | |
| Frequency (5) | 5 | 4 | 4 | 3 | 2 |
| Occasional (4) | 4 | 4 | 3 | 2 | 2 |
| Seldom (3) | 4 | 3 | 3 | 2 | 1 |
| Remote (2) | 3 | 3 | 2 | 1 | 1 |
| Unlikely (1) | 3 | 2 | 2 | r | 1 |
| Risk level | Risk Control Measures | Note | |||
| 5-extreme | Reduction risk measures need to be taken immediately, and tasks should not be started until the risk is reduced. | Unacceptable risk | |||
| 4-very high | Risk control measures must be taken within a certain period of time, and tasks cannot be started until the risk is reduced. | ||||
| 3-high | Based on cost or financial considerations, risk reduction measures should be taken gradually. | ||||
| 2-medium | There is no need to take risk reduction measures at the moment, but it is necessary to ensure the effectiveness of existing protection facilities. | Acceptable risk | |||
| 1-low | No risk reduction measures are required, but the effectiveness of existing safeguards must be ensured. | ||||
| Cost Level | Description |
|---|---|
| E | Spending more than $10 million USD for risk reduction measures. |
| D | Spending range from $1 million to $10 million USD for risk reduction measures. |
| C | Spending range from $100,000 to $1 million USD for risk reduction measures. |
| B | Spending range from $10,000 to $100,000 USD for risk reduction measures. |
| A | Spending less than $10,000 USD for risk reduction measures. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, Y.-C.; Laiwang, B.; Shu, C.-M. Investigation of an Explosion at a Styrene Plant with Alkylation Reactor Feed Furnace. Appl. Sci. 2019, 9, 503. https://doi.org/10.3390/app9030503
Wu Y-C, Laiwang B, Shu C-M. Investigation of an Explosion at a Styrene Plant with Alkylation Reactor Feed Furnace. Applied Sciences. 2019; 9(3):503. https://doi.org/10.3390/app9030503
Chicago/Turabian StyleWu, Yao-Chang, Bin Laiwang, and Chi-Min Shu. 2019. "Investigation of an Explosion at a Styrene Plant with Alkylation Reactor Feed Furnace" Applied Sciences 9, no. 3: 503. https://doi.org/10.3390/app9030503