Summary of over Fifty Years with Brain-Computer Interfaces—A Review

 , , ,
, , ,  ,
,  , ,
, ,  and
and 
Abstract
:1. Introduction
- cognitive psychology,
- artificial intelligence,
- neuroscience,
- linguistics,
- anthropology,
- philosophy,
- robotics,
- information technology.
- electromygraphy—EMG,
- electrooculography—EOG,
- brain signals (electroencephalograhhy—EEG and electrocorticography—ECoG)— (Brain Computer Interfaces).
- neural prostheses, which are a cybernetic alternative for a limb using nerves connected with the muscles;
- Brain-Computer Interfaces (BCI), which detect human decision through electromagnetic pulses directly from the brain.
2. Brain-Computer Interfaces
- blood oxygen measurements,
- functional resonance imaging (fMRI),
- functional infrared spectroscopy (fNIRS), etc…
- spatial resolution in the millimeters scale,
- frequency bandwidth up to 200 Hz or higher,
- amplitude up to 100 μV,
- reduced sensitivity to movement and myoelectrical artifacts.
2.1. History of Brain-Computer Interfaces
- Epilepsy,
- Attention Deficit Disorder (ADD),
- Attention-Deficit/Hyperactivity Disorder (ADHD),
- concentration problems,
- Parkinson’s Disease (PD),
- Multiple Sclerosis,
- sleep problems,
- various mental disorders.
2.2. Invasive Brain-Computer Interfaces
2.3. Non-Invasive BCI Systems
- ERD—associated with motor imagery (MI),
- ERP—event-related potentials (P300 and other components),
- SSVEP—steady-state visual evoked potentials,
- ASSR—auditory steady-state response,
- SCP—slow cortical potentials,
- SMR—sensorimotor oscillations,
- various hybrid systems (based on more than one input signal).
- magnetoencephalography (MEG)—requires large, unhandy equipment;
- functional Magnetic Resonance Imaging (fMRI)—large, expensive, unhandy device, poor temporal resolution;
- near infrared spectroscopy (NIRS)—poor temporal resolution;
- positron emission tomography (PET)—large, expensive, unhandy equipment.
- Classic P300 BCIs;
- P300 BCIs using tactile stimulation through small discs (tactors) places over specific areas;
- Hybrid P300-BCIs—combining various types of BCI systems;
- chronic pain,
- motor diseases,
- psychopathy,
- social phobia,
- depression.
- performance of higher-order cognitive tasks such as e.g., mental calculation,
- language-related tasks conversion such as e.g., mental speech and/or mental singing,
- performance of imagery tasks such as e.g., motor, visual, auditory, tactile, and emotion imagery,
- performance of selective attention tasks such as e.g., visual, auditory, and tactile attention.
2.4. BCI Systems—Recording Devices—Brief Review
- safety—,
- effect accuracy ,
- wearing comfort .
- Emotiv Inc. (San Francisco, CA, USA),
- Ant Neuro (Hengelo, Netherlands),
- Cognionics (San Diego, CA, USA),
- Neurosky Inc. (San Jose, CA, USA),
- OpenBCI (Brooklyn, NY, USA),
- interaXon (Toronto, Canada),
- g.tec (Schiedlberg, Austria),
- CREmedical (Kingston, RI, USA).
- Emotiv EPOC (2009) and Emotiv EPOC+ NeuroHeadset (2013)—14-channels device, with 2 referential sensors, wireless Bluetooth connection, battery, and a USB port;
- Emotiv Insight (2015)—a simpler 5-channel wireless EEG device, designed for everyday use with advanced electronics and full optimization, designed for everyday use by individuals;
- Emotiv EPOC Flex (2019)—equipped with 32 measuring sensors available in two options: gel- and saline-sensors. It has wireless technology, is elastic, and adjusts to the head shape;
- Emotiv EPOC X (2020)—14-channel wireless headset.
- MindSet (2009),
- MindWave (2011),
- MindWave Mobile (2012),
- MindWave Mobile 2 (2018).
- electroencephalography (EEG),
- electromyography (EMG),
- electrocardiography (ECG).
- 21-channel EEG Electrode Cap Kit (2019) with Ag/AgCl coated electrodes;
- 16-channel All-in-One Biosensing R&D Bundle (2014) with different approaches EEG data acquisition:
- dry electrodes—EEG Headset,
- wet electrodes—gold cup electrodes;
- 8-channel OpenBCI EEG Headband Kit (2018) with dry electrodes.
- OpenBCI Galea (announced in Novemebr 2020)—combines mixed reality (XR) headsets with state-of-the-art biosensing and BCIs with several types of sensors:
- electroencephalography (EEG),
- electrooculography (EOG),
- electromyography (EMG),
- electrodermal activity (EDA),
- photoplethysmography (PPG).
- Muse (2014)—a 7-sensors device designed with dry sensors, which do not require any liquid;
- Muse 2 (2018)—device with 4 EEG electrodes, heart sensors (PPG + Pulse Oximetry), accelerometer, and gyroscope.
- g.NAUTILUS PRO—available with prefixed dry or wet EEG electrodes with 3-axis accelerometer.
- g.NAUTILUS RESEARCH—a hybrid (dry and wet EEG electrode) version and a gel EEG electrode version with EEG channels. This device is non-certified (for potential clinical applications), which results in a lower price of this device for only neuroscience research.
- g.NAUTILUS fNIRS—it enables simultaneous recordings of both EEG and fNIRS (functional near-infrared spectroscopy) signals. It provides the top-quality EEG recordings from g.SCARABEO EEG channels and 8 fNIRS channels within a few minutes.
- g.NAUTILUS MULTI PURPOSE—multiple EEG and biosignal amplifier, which can connect to other body sensors such as ECG/EOG/EMG electrodes to measure GSR, respiration, and many other biosignals.
- g.tec amplifiers;
- Porti7 (TMSI);
- Nuamp amplifier;
- BrainAmp128DC;
- BioNomadix amplifier (Biopac);
3. The Newest Trends and Further Development Paths in BCIs
- Active BCIs—are controlled by the user through a specific mental task performance:
- motor imagery—the user has to imagine movement of a limb, which can be later translated into appropriate command;
- blinking—eye blinking registered in the EEG can be used as a control command.
- Reactive BCIs—the user produces brain signals as a response to external stimulations such as visual or audio stimuli:
- Event-Related Potential—natural brain’s response to a specified event or a stimulation;
- Visual Evoked Potential—a form of ERP, which depends on visual stimuli.
- Passive BCIs—a system, which focuses on the cognitive feedback of the users’ brains’ activity. The system works partially autonomous:
- emotions—emotion recognition, recognized by the BCI system;
- mental state—the BCI system is able to recognize and analyse the user’s mental state and provide him/her with appropriate feedback.
4. Advanced Signal Processing Methods for BCI Systems
- stationary:
- ergodic,
- non-ergodic.
- non-stationary.
- conventional and high density EEG with different montages:
- bipolar,
- Laplacian,
- common average references.
- some methods of linear spatial filtering such as inter alia:
- Principle Component Analysis (PCA),
- Independent Component Analysis (ICA).
- different hardware electrodes such as inter alia:
- a bipolar electrode with five points finite difference method (FPM),
- quasi-bipolar concentric electrode,
- tri-polar concentric electrode.
- wet electrodes:
- silver-chloride electrodes (Ag/AgCl):
- -
- low cost,
- -
- popular and widely used by current market products,
- -
- they have low contact impedance,
- -
- they require removing outer skin layer of the scalp and using conductor gels or pastes,
- -
- they require longer preparation time,
- -
- they may be uncomfortable for potential patients,
- dry electrodes:
- they do not require any type of skin preparation,
- they do not need using any types of conductive gel or paste,
- they may provide worse signal quality to the wet electrodes.
- external:
- -
- Apparatus: broken electrode wire, bad contact of the electrode with the surface of the scalp, detachment of the electrode, etc.
- -
- power artifact: 50 Hz (Europe) or 60 Hz (US).
- internal—physiological artifacts generated by the body of the examined person:
- -
- EOG artifacts—caused by the eye movements;
- -
- cardiac artifacts—related to the ECG;
- -
- muscle artifacts—related to the EMG;
- -
- movement artifacts—caused by the subject’s body movements;
- -
- artifacts related to the sweat gland activity;
- -
- respiratory artifacts.
- advanced/sophisticated signal processing methods:
- discrete and continuous Fourier Transforms,
- Wavelet Transforms (WT),
- Time-Frequency Analysis (TFA),
- Blind Source Separation (BSS) methods:
- -
- Principal Component Analysis (PCA),
- -
- Independent Component Analysis (ICA),
- -
- Empirical Mode Decomposition (EMD).
- Fuzzy Logic.
- Artificial Neural Networks:
- -
- Convolutional Neural Networks;
- -
- Deep Learning Networks.
- basic/simple simple digital and adaptive filtering methods;
- various modifications and combinations—the so-called “hybrid methods”.
- Fourier Transform (FT);
- Discrete Fourier Transform (DFT)—enables decomposition of discrete time signals into sinusoidal components, were their frequencies are multiples of a fundamental frequency;
- Fast Fourier Transform (FFT)—frequently applied in analysis of any deterministic bio-signal’s spectral content, which is also a faster version of the Fourier (FT) and the Discrete Fourier (DFT) Transform. It is not designed for short-duration signals;
- Short-Time Fourier Transform (STFT)—involves multiplication of the analysed signal by a short-duration time window, which is slid along the time axis of the signal in order to cover the whole duration of it and to obtain estimate of the signal’s spectral content. Within the short-duration window the signal is assumed to be stationary. The STFT can be also considered as a kind of method for signal filtering using a band-pass filter centered around a given frequency f, where the impulse response is the FT of the short-duration window modulated to that frequency. It is also known as Gabor Transform;
- Discrete Hartley Transform (DHT)—very popular in various BCI applications. It is similar to the DFT;
- Fast Hartley transform (FHT)—faster DHT, twice as fast as the FFT;
- the Discrete Cosine Transform;
- the Discrete Hilbert Transform;
- the Discrete Fractional Hilbert Transform;
- the Discrete-Time Wavelet Transform;
- the Discrete Walsh Transform;
- the Discrete Hadamard Transform;
- Wavelet Transforms (WT)—popular in processing of biomedical images and biomedical signals. Used for conversion of the complex signals from the time- into the frequency-domain. Is computationally heavy, which makes them unsuitable for implementation on embedded platforms. Contrary to the STFT the WT provides a more flexible way of signal’s time-frequency representation by allowing the use of variable sized windows. There are numerous types of Wavelet Transforms such as inter alia:
- -
- Continuous Wavelet Transform (CWT),
- -
- Discrete Wavelet Transform (DWT);
- -
- Tunable-Q Wavelet Transform.
- Morlet Wavelet—works well with signals with short duration of the high-frequency components and long duration of the low-frequency components, such as the EEG signal;
- Daubechies Wavelet function—were investigated for the analysis of epileptic EEG recordings;
- Harmonic Wavelet function—enables to achieve exact band separation in the frequency domain.
- Hamming,
- Hanning,
- Kaiser,
- Barlett.
- the source signals are statistically independent from each other and instantaneously mixed;
- the dimensions of the analysed signals have to be greater than or equal to the source signal;
- the sources
- only the original IC (Independent Component) can have the Gaussian distribution;
- only for the n-dimensional data vector it is possible to find a maximum of the n-dependent components with the use of the ICA method;
- it is impossible to determine the order of the original components with the ICA method.
- logical,
- fuzzy-set-theoretic,
- relational,
- epistemic.
- low-pass filters—exclude the unwanted higher values in the signal;
- high-pass filters—exclude the unwanted lower values in signals;
- band-pass filters—pass signals within a certain range of frequencies without distorting the input signal or introducing extra noise;
- band-stop filters (notch)—reject signals within a specific frequency band called the stop band frequency range and passes the signals above and below this band.
- Butterworth,
- Chebyshev (Type and II),
- Elliptic,
- Bessel.
- Savitzky-Golay filter (S-G),
- Median filter,
- Bessel smoothing filter.
- Convolutional Neural Network (CNN)—relies on linear operation known as convolution. Provides good results during processing of images, audio, video and biomedical signals such as EEG;
- Recurrent Neural Network (RNN)—This type of network involves inbuilt memory cells for preserving the previous output states and uses it for processing purposes.
5. Discussion and Conclusions
- ALS (Amyotrophic Lateral Sclerosis),
- cerebral palsy,
- brainstem stroke,
- spinal-cord injuries,
- muscular dystrophies,
- chronic peripheral neuropathies,
- psychiatric disorders.
- signal-acquisition hardware,
- BCI validation and dissemination,
- reliability.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ADD | Attention Deficit Disorder |
| ADHD | Attention-Deficit/Hyperactivity Disorder |
| ALS | Amyotrophic Lateral Sclerosis |
| ANN | Artificial Neural Networks |
| AR | Augmented Reality |
| ASSR | auditory steady-state response |
| BCI | Brain-Computer Interfaces |
| BCS | Brain-inspired Cognitive System |
| BOLD | blood oxygen level-dependent signals |
| BSS | Blind Source Separation |
| CNN | Convolutional Neural Network |
| CNS | central nervous system |
| CWT | Continuous Wavelet Transform |
| DC | direct current |
| DFT | Discrete Fourier Transform |
| DHT | Discrete Hartley Transform |
| DL | Deep Learning |
| DNN | Deep Neural Networks |
| DSP | digital signal processing |
| DBD | Duchenne Muscular Dystrophy |
| DWT | Discrete Wavelet Transform |
| ECG | Electrocardiography |
| EDA | electrodermal activity |
| ECoG | electrocorticography |
| EEG | electroencephalography |
| EMD | Empirical Mode Decomposition |
| EMG | electromygraphy |
| EOG | electrooculography |
| ERD | event related desynchronisation |
| ERP | event-related potentials |
| ERS | Event-Related Synchronisation |
| FES | functional electrical stimulation |
| FFT | Fast Fourier Transform |
| FHT | Fast Hartley transform |
| FL | Fuzzy Logic |
| fMRI | functional resonance imaging |
| fNIRS | functional infrared spectroscopy |
| FT | Fourier Transform |
| HMI | Human-Machine Interfaces |
| ICA | Independent Component Analysis |
| LIS | Locked-in Syndrome |
| MEG | magnetoencephalography |
| ME | motor execution |
| MI | motor imagery |
| mVEPs | motion-onset visually evoked potentials |
| NN | Neural Networks |
| PCA | Principal Component Analysis |
| PD | Parkinson’s Disease |
| PET | positron emission tomography |
| PPG | hotoplethysmography |
| RNN | Recurrent Neural Network |
| SCP | slow cortical potentials |
| sEEG | stereoencephalography |
| SG | Savitzky-Golay filter |
| SMR | sensorimotor rhythm |
| SNR | signal-to-noise ratio |
| SMA II | Spinal Muscular Atrophy type II |
| SSVEP | steady-state visual evoked potentials |
| STFT | Short-Time Fourier Transform |
| TFA | Time-Frequency Analysis |
| VR | virtual reality |
| XR | mixed reality |
| WT | Wavelet Transform |
References
- Shortliffe, E.H.; Barnett, G.O. Biomedical data: Their acquisition, storage, and use. In Biomedical Informatics; Springer: Berlin/Heidelberg, Germany, 2006; pp. 46–79. [Google Scholar]
- Kübler, A. The history of BCI: From a vision for the future to real support for personhood in people with locked-in syndrome. Neuroethics 2019, 13, 163–180. [Google Scholar] [CrossRef]
- Kawala-Janik, A. Efficiency Evaluation of External Environments Control Using Bio-Signals. Ph.D. Thesis, University of Greenwich, London, UK, 2013. [Google Scholar]
- Wolpaw, J.; Wolpaw, E.W. Brain-Computer Interfaces: Principles and Practice; OUP USA: Oxford, UK, 2012. [Google Scholar]
- Ma, T.; Li, H.; Deng, L.; Yang, H.; Lv, X.; Li, P.; Li, F.; Zhang, R.; Liu, T.; Yao, D.; et al. The hybrid BCI system for movement control by combining motor imagery and moving onset visual evoked potential. J. Neural Eng. 2017, 14, 026015. [Google Scholar] [CrossRef] [PubMed]
- Van Dokkum, L.; Ward, T.; Laffont, I. Brain computer interfaces for neurorehabilitation–its current status as a rehabilitation strategy post-stroke. Ann. Phys. Rehabil. Med. 2015, 58, 3–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castro, N.; Siew, C.S. Contributions of Modern Network Science to the Cognitive Sciences: Revisiting research spirals of representation and process. Proc. R. Soc. A 2020, 476, 20190825. [Google Scholar] [CrossRef]
- Wang, Y.; Kwong, S.; Leung, H.; Lu, J.; Smith, M.H.; Trajkovic, L.; Tunstel, E.; Plataniotis, K.N.; Yen, G.G.; Kinsner, W. Brain-Inspired Systems: A Transdisciplinary Exploration on Cognitive Cybernetics, Humanity, and Systems Science Toward Autonomous Artificial Intelligence. IEEE Syst. Man Cybern. Mag. 2020, 6, 6–13. [Google Scholar] [CrossRef]
- Schirmann, F. “The wondrous eyes of a new technology”—A history of the early electroencephalography (EEG) of psychopathy, delinquency, and immorality. Front. Hum. Neurosci. 2014, 8, 232. [Google Scholar] [CrossRef] [Green Version]
- Martins, N.R.; Angelica, A.; Chakravarthy, K.; Svidinenko, Y.; Boehm, F.J.; Opris, I.; Lebedev, M.A.; Swan, M.; Garan, S.A.; Rosenfeld, J.V.; et al. Human brain/cloud interface. Front. Neurosci. 2019, 13, 112. [Google Scholar] [CrossRef]
- Collinger, J.L.; Wodlinger, B.; Downey, J.E.; Wang, W.; Tyler-Kabara, E.C.; Weber, D.J.; McMorland, A.J.; Velliste, M.; Boninger, M.L.; Schwartz, A.B. High-performance neuroprosthetic control by an individual with tetraplegia. Lancet 2013, 381, 557–564. [Google Scholar] [CrossRef] [Green Version]
- Theis, F.J.; Meyer-Bäse, A. Biomedical Signal Analysis: Contemporary Methods and Applications; MIT Press: Cambridge, MA, USA, 2010. [Google Scholar]
- Kawala-Sterniuk, A.; Podpora, M.; Pelc, M.; Blaszczyszyn, M.; Gorzelanczyk, E.J.; Martinek, R.; Ozana, S. Comparison of smoothing filters in analysis of EEG data for the medical diagnostics purposes. Sensors 2020, 20, 807. [Google Scholar] [CrossRef] [Green Version]
- Milanizadeh, S.; Safaie, J. EOG Based HCI System for Quadcopter Navigation. IEEE Trans. Instrum. Meas. 2020, 69, 8992–8999. [Google Scholar] [CrossRef]
- Saravanakumar, D.; Reddy, R. A high performance asynchronous EOG speller system. Biomed. Signal Process. Control 2020, 59, 101898. [Google Scholar]
- Li, K.; Zhang, J.; Wang, L.; Zhang, M.; Li, J.; Bao, S. A review of the key technologies for sEMG-based human-robot interaction systems. Biomed. Signal Process. Control 2020, 62, 102074. [Google Scholar] [CrossRef]
- Yao, D.; Qin, Y.; Hu, S.; Dong, L.; Vega, M.L.B.; Sosa, P.A.V. Which reference should we use for EEG and ERP practice? Brain Topogr. 2019, 32, 530–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bamdad, M.; Zarshenas, H.; Auais, M.A. Application of BCI systems in neurorehabilitation: A scoping review. Disabil. Rehabil. Assist. Technol. 2015, 10, 355–364. [Google Scholar] [CrossRef] [PubMed]
- Epstein, R. The empty brain. Aeon 2016, 18, 2016. [Google Scholar]
- Hassan, M.A.; Rizvi, Q.M. Computer vs human brain: An analytical approach and overview. Computer 2019, 6, 580–583. [Google Scholar]
- Collinger, J.L.; Kryger, M.A.; Barbara, R.; Betler, T.; Bowsher, K.; Brown, E.H.; Clanton, S.T.; Degenhart, A.D.; Foldes, S.T.; Gaunt, R.A.; et al. Collaborative approach in the development of High-Performance Brain–Computer interfaces for a neuroprosthetic arm: Translation from animal models to human control. Clin. Transl. Sci. 2014, 7, 52–59. [Google Scholar] [CrossRef]
- Miller, K.J.; Hermes, D.; Staff, N.P. The current state of electrocorticography-based brain–computer interfaces. Neurosurg. Focus 2020, 49, E2. [Google Scholar] [CrossRef]
- Shih, J.J.; Krusienski, D.J.; Wolpaw, J.R. Brain-computer interfaces in medicine. In Mayo Clinic Proceedings; Elsevier: Amsterdam, The Netherlands, 2012; Volume 87, pp. 268–279. [Google Scholar]
- Zhang, H.; Wang, H. Study on classification and recognition of multi-lead EEG signals. Comput. Eng. Appl. 2008, 24, 228–230. [Google Scholar]
- Yu, X.; Qi, W. A user study of wearable EEG headset products for emotion analysis. In Proceedings of the 2018 International Conference on Algorithms, Computing and Artificial Intelligence, Sanya, China, 21 December 2018; pp. 1–7. [Google Scholar]
- Adeli, H.; Zhou, Z.; Dadmehr, N. Analysis of EEG records in an epileptic patient using wavelet transform. J. Neurosci. Methods 2003, 123, 69–87. [Google Scholar] [CrossRef]
- Leuthardt, E.C.; Miller, K.J.; Schalk, G.; Rao, R.P.; Ojemann, J.G. Electrocorticography-based brain computer interface-the Seattle experience. IEEE Trans. Neural Syst. Rehabil. Eng. 2006, 14, 194–198. [Google Scholar] [CrossRef] [PubMed]
- Dubey, A.; Ray, S. Cortical Electrocorticogram (ECoG) is a local signal. J. Neurosci. 2019, 39, 4299–4311. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.T.; King, C.E.; McCrimmon, C.M.; Lin, J.J.; Sazgar, M.; Hsu, F.P.; Shaw, S.J.; Millet, D.E.; Chui, L.A.; Liu, C.Y.; et al. Comparison of decoding resolution of standard and high-density electrocorticogram electrodes. J. Neural Eng. 2016, 13, 026016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chakrabarti, S.; Sandberg, H.M.; Brumberg, J.S.; Krusienski, D.J. Progress in speech decoding from the electrocorticogram. Biomed. Eng. Lett. 2015, 5, 10–21. [Google Scholar] [CrossRef]
- Graimann, B.; Allison, B.Z.; Pfurtscheller, G. Brain-Computer Interfaces: Revolutionizing Human-Computer Interaction; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2010. [Google Scholar]
- Villamar, M.F.; Al-Bakri, A.F.; Haddix, C.; Albuja, A.C.; Bensalem-Owen, M.; Sunderam, S. T157. Seizure prediction with autonomic measurements versus intracranial EEG in patients with refractory epilepsy. Clin. Neurophysiol. 2018, 129, e63. [Google Scholar] [CrossRef]
- Wittevrongel, B.; Khachatryan, E.; Carrette, E.; Boon, P.; Meurs, A.; Van Roost, D.; Van Hulle, M.M. High-gamma oscillations precede visual steady-state responses: A human electrocorticography study. Hum. Brain Mapp. 2020, 41, 5341–5355. [Google Scholar] [CrossRef]
- Amaral, P.; Paulo, J.; Cunha, S.; Dias, P.; Maria, J. Multimodal Application for Visualization and Manipulation of Electrocorticography Data. 2007. [Google Scholar]
- Kingwell, K. Neurally controlled robotic arm enables tetraplegic patient to drink coffee of her own volition. Nat. Rev. Neurol. 2012, 8, 353. [Google Scholar] [CrossRef]
- Ethier, C.; Oby, E.R.; Bauman, M.J.; Miller, L.E. Restoration of grasp following paralysis through brain-controlled stimulation of muscles. Nature 2012, 485, 368–371. [Google Scholar] [CrossRef] [Green Version]
- Millett, D. Hans Berger: From psychic energy to the EEG. Perspect. Biol. Med. 2001, 44, 522–542. [Google Scholar] [CrossRef]
- Gloor, P. Hans Berger on electroencephalography. Am. J. EEG Technol. 1969, 9, 1–8. [Google Scholar] [CrossRef]
- Berger, H. Über das Elektrenkephalogramm des Menschen. XIV. Archiv für Psychiatrie und Nervenkrankheiten 1938, 108, 407–431. [Google Scholar] [CrossRef]
- Ocak, H. Automatic detection of epileptic seizures in EEG using discrete wavelet transform and approximate entropy. Expert Syst. Appl. 2009, 36, 2027–2036. [Google Scholar] [CrossRef]
- Lopez-Gordo, M.A.; Sanchez-Morillo, D.; Valle, F.P. Dry EEG electrodes. Sensors 2014, 14, 12847–12870. [Google Scholar] [CrossRef] [PubMed]
- Beatty, J.; Greenberg, A.; Deibler, W.P.; O’Hanlon, J.F. Operant control of occipital theta rhythm affects performance in a radar monitoring task. Science 1974, 183, 871–873. [Google Scholar] [CrossRef]
- Tudor, M.; Tudor, L.; Tudor, K.I. Hans Berger (1873–1941)–the history of electroencephalography. Acta Medica Croat. Cas. Hravatske Akad. Med. Znan. 2005, 59, 307–313. [Google Scholar]
- Haas, L.F. Hans berger (1873–1941), richard caton (1842–1926), and electroencephalography. J. Neurol. Neurosurg. Psychiatry 2003, 74, 9. [Google Scholar] [CrossRef] [Green Version]
- Coenen, A.; Zayachkivska, O. Adolf Beck: A pioneer in electroencephalography in between Richard Caton and Hans Berger. Adv. Cogn. Psychol. 2013, 9, 216. [Google Scholar] [CrossRef]
- Kułak, W.; Sobaniec, W. Historia odkrycia EEG. Neurol. Dziecięca 2006, 15, 53–56. [Google Scholar]
- Marshall, L.H.; Magoun, H.W. Discoveries in the Human Brain: Neuroscience Prehistory, Brain Structure, and Function; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Babkin, B. Sechenov and Pavlov. Russ. Rev. 1946, 5, 24–35. [Google Scholar] [CrossRef]
- Grigoriev, A.; Grigorian, N. IM Sechenov: The patriarch of Russian physiology. J. Hist. Neurosci. 2007, 16, 19–29. [Google Scholar] [CrossRef]
- Stone, J.L.; Hughes, J.R. Early history of electroencephalography and establishment of the American Clinical Neurophysiology Society. J. Clin. Neurophysiol. 2013, 30, 28–44. [Google Scholar] [CrossRef] [PubMed]
- Ebersole, J.S.; Pedley, T.A. Current Practice of Clinical Electroencephalography; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2003. [Google Scholar]
- Hazarika, N.; Chen, J.Z.; Tsoi, A.C.; Sergejew, A. Classification of EEG signals using the wavelet transform. Signal Process. 1997, 59, 61–72. [Google Scholar] [CrossRef]
- Aydemir, E.; Tuncer, T.; Dogan, S. A Tunable-Q wavelet transform and quadruple symmetric pattern based EEG signal classification method. Med. Hypotheses 2020, 134, 109519. [Google Scholar] [CrossRef] [PubMed]
- Shahriari, Y.; Besio, W.; Hosni, S.I.; Zisk, A.H.; Borgheai, S.B.; Deligani, R.J.; McLinden, J. Electroencephalography. In Neural Interface Engineering; Springer: Berlin/Heidelberg, Germany, 2020; pp. 1–16. [Google Scholar]
- Wojcik, G.M.; Masiak, J.; Kawiak, A.; Schneider, P.; Kwasniewicz, L.; Polak, N.; Gajos-Balinska, A. New protocol for quantitative analysis of brain cortex electroencephalographic activity in patients with psychiatric disorders. Front. Neuroinform. 2018, 12, 27. [Google Scholar] [CrossRef] [PubMed]
- Ursuţiu, D.; Samoilă, C.; Drăgulin, S.; Constantin, F.A. Investigation of music and colours influences on the levels of emotion and concentration. In Online Engineering & Internet of Things; Springer: Berlin/Heidelberg, Germany, 2018; pp. 910–918. [Google Scholar]
- Robin, M. A Handbook for Yogasana Teachers: The Incorporation of Neuroscience, Physiology, and Anatomy Into the Practice; Wheatmark, Inc.: Tucson, Arizona, 2009. [Google Scholar]
- Akin, M. Comparison of wavelet transform and FFT methods in the analysis of EEG signals. J. Med. Syst. 2002, 26, 241–247. [Google Scholar] [CrossRef]
- Jurcak, V.; Tsuzuki, D.; Dan, I. 10/20, 10/10, and 10/5 systems revisited: Their validity as relative head-surface-based positioning systems. Neuroimage 2007, 34, 1600–1611. [Google Scholar] [CrossRef]
- Rangayyan, R.M. Biomedical Signal Analysis; John Wiley & Sons: Hoboken, NJ, USA, 2015; Volume 33. [Google Scholar]
- Merletti, R.; Parker, P.J. Electromyography: Physiology, Engineering, and Non-Invasive Applications; John Wiley & Sons: Hoboken, NJ, USA, 2004; Volume 11. [Google Scholar]
- Fajkus, M.; Nedoma, J.; Martinek, R.; Vasinek, V.; Nazeran, H.; Siska, P. A non-invasive multichannel hybrid fiber-optic sensor system for vital sign monitoring. Sensors 2017, 17, 111. [Google Scholar] [CrossRef]
- Sidikova, M.; Martinek, R.; Kawala-Sterniuk, A.; Ladrova, M.; Jaros, R.; Danys, L.; Simonik, P. Vital Sign Monitoring in Car Seats Based on Electrocardiography, Ballistocardiography and Seismocardiography: A Review. Sensors 2020, 20, 5699. [Google Scholar] [CrossRef]
- Clerc, M.; Bougrain, L.; Lotte, F. Brain-Computer Interfaces; John Wiley & Sons: Hoboken, NJ, USA, 2016. [Google Scholar]
- Weisz, N.; Schandry, R.; Jacobs, A.M.; Mialet, J.P.; Duschek, S. Early contingent negative variation of the EEG and attentional flexibility are reduced in hypotension. Int. J. Psychophysiol. 2002, 45, 253–260. [Google Scholar] [CrossRef] [Green Version]
- Walter, W.G.; Cooper, R.; Aldridge, V.; McCallum, W.; Winter, A. Contingent negative variation: An electric sign of sensori-motor association and expectancy in the human brain. Nature 1964, 203, 380–384. [Google Scholar] [CrossRef]
- Sterman, M.B.; Howe, R.C.; Macdonald, L.R. Facilitation of spindle-burst sleep by conditioning of electroencephalographic activity while awake. Science 1970, 167, 1146–1148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuhlman, W.N. Functional topography of the human mu rhythm. Electroencephalogr. Clin. Neurophysiol. 1978, 44, 83–93. [Google Scholar] [CrossRef]
- Farwell, L.A.; Donchin, E. Talking off the top of your head: Toward a mental prosthesis utilizing event-related brain potentials. Electroencephalogr. Clin. Neurophysiol. 1988, 70, 510–523. [Google Scholar] [CrossRef]
- Nguyen, T.; Hettiarachchi, I.; Khosravi, A.; Salaken, S.M.; Bhatti, A.; Nahavandi, S. Multiclass EEG data classification using fuzzy systems. In Proceedings of the 2017 IEEE International Conference on Fuzzy Systems (FUZZ-IEEE), Naples, Italy, 9–12 July 2017; pp. 1–6. [Google Scholar]
- Arafat, I. Brain-Computer Interface: Past, Present & Future; International Islamic University Chittagong (IIUC): Chittagong, Bangladesh, 2013. [Google Scholar]
- Kolhe, S.; Khemani, D.; Bhatt, C.; Dubey, N. Automation of appliances using electro-encephalography. In Emerging Technologies for Health and Medicine: Virtual Reality, Augmented Reality, Artificial Intelligence, Internet of Things, Robotics, Industry 4.0; John Wiley & Sons: Beverly, MA, USA, 2018; p. 225. [Google Scholar]
- Birbaumer, N.; Ghanayim, N.; Hinterberger, T.; Iversen, I.; Kotchoubey, B.; Kübler, A.; Perelmouter, J.; Taub, E.; Flor, H. A spelling device for the paralysed. Nature 1999, 398, 297–298. [Google Scholar] [CrossRef]
- Rezeika, A.; Benda, M.; Stawicki, P.; Gembler, F.; Saboor, A.; Volosyak, I. Brain–computer interface spellers: A review. Brain Sci. 2018, 8, 57. [Google Scholar] [CrossRef] [Green Version]
- Hochberg, L.R.; Bacher, D.; Jarosiewicz, B.; Masse, N.Y.; Simeral, J.D.; Vogel, J.; Haddadin, S.; Liu, J.; Cash, S.S.; Van Der Smagt, P.; et al. Reach and grasp by people with tetraplegia using a neurally controlled robotic arm. Nature 2012, 485, 372–375. [Google Scholar] [CrossRef] [Green Version]
- Gollahalli, A.R. Brain-Computer Interfaces for Virtual Quadcopters Based on a Spiking-Neural Network Architecture-Neucube. Ph.D. Thesis, Auckland University of Technology, Auckland, New Zealand, 2015. [Google Scholar]
- Bouton, C.E.; Shaikhouni, A.; Annetta, N.V.; Bockbrader, M.A.; Friedenberg, D.A.; Nielson, D.M.; Sharma, G.; Sederberg, P.B.; Glenn, B.C.; Mysiw, W.J.; et al. Restoring cortical control of functional movement in a human with quadriplegia. Nature 2016, 533, 247–250. [Google Scholar] [CrossRef]
- Ganzer, P.D.; Colachis, S.C., 4th; Schwemmer, M.A.; Friedenberg, D.A.; Dunlap, C.F.; Swiftney, C.E.; Jacobowitz, A.F.; Weber, D.J.; Bockbrader, M.A.; Sharma, G. Restoring the Sense of Touch Using a Sensorimotor Demultiplexing Neural Interface. Cell 2020, 181, 763–773.e12. [Google Scholar] [CrossRef]
- Ajiboye, A.B.; Willett, F.R.; Young, D.R.; Memberg, W.D.; Murphy, B.A.; Miller, J.P.; Walter, B.L.; Sweet, J.A.; Hoyen, H.A.; Keith, M.W.; et al. Restoration of reaching and grasping movements through brain-controlled muscle stimulation in a person with tetraplegia: A proof-of-concept demonstration. Lancet 2017, 389, 1821–1830. [Google Scholar] [CrossRef] [Green Version]
- Willett, F.R.; Young, D.R.; Murphy, B.A.; Memberg, W.D.; Blabe, C.H.; Pandarinath, C.; Stavisky, S.D.; Rezaii, P.; Saab, J.; Walter, B.L.; et al. Principled BCI decoder design and parameter selection using a feedback control model. Sci. Rep. 2019, 9, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Schwemmer, M.A.; Skomrock, N.D.; Sederberg, P.B.; Ting, J.E.; Sharma, G.; Bockbrader, M.A.; Friedenberg, D.A. Meeting brain–computer interface user performance expectations using a deep neural network decoding framework. Nat. Med. 2018, 24, 1669–1676. [Google Scholar] [CrossRef] [PubMed]
- Sitaram, R.; Caria, A.; Veit, R.; Gaber, T.; Rota, G.; Kuebler, A.; Birbaumer, N. FMRI brain-computer interface: A tool for neuroscientific research and treatment. Comput. Intell. Neurosci. 2007, 2007, 025487. [Google Scholar] [CrossRef] [PubMed]
- Birbaumer, N. Breaking the silence: Brain–computer interfaces (BCI) for communication and motor control. Psychophysiology 2006, 43, 517–532. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Lee, J.; Han, C.; Park, K. An Instant Donning Multi-Channel EEG Headset (with Comb-Shaped Dry Electrodes) and BCI Applications. Sensors 2019, 19, 1537. [Google Scholar] [CrossRef] [Green Version]
- Velasco-Álvarez, F.; Sancha-Ros, S.; García-Garaluz, E.; Fernández-Rodríguez, Á.; Medina-Juliá, M.T.; Ron-Angevin, R. UMA-BCI speller: An easily configurable P300 speller tool for end users. Comput. Methods Programs Biomed. 2019, 172, 127–138. [Google Scholar] [CrossRef]
- Mowla, M.R.; Gonzalez-Morales, J.D.; Rico-Martinez, J.; Ulichnie, D.A.; Thompson, D.E. A Comparison of Classification Techniques to Predict Brain-Computer Interfaces Accuracy Using Classifier-Based Latency Estimation. Brain Sci. 2020, 10, 734. [Google Scholar] [CrossRef]
- Al-Saegh, A.; Dawwd, S.A.; Abdul-Jabbar, J.M. Deep learning for motor imagery EEG-based classification: A review. Biomed. Signal Process. Control 2021, 63, 102172. [Google Scholar] [CrossRef]
- Yoo, S.S.; Fairneny, T.; Chen, N.K.; Choo, S.E.; Panych, L.P.; Park, H.; Lee, S.Y.; Jolesz, F.A. Brain—Computer interface using fMRI: Spatial navigation by thoughts. Neuroreport 2004, 15, 1591–1595. [Google Scholar] [CrossRef]
- Montagna, F. Optimized Biosignals Processing Algorithms for New Designs of Human Machine Interfaces on Parallel Ultra-Low Power Architectures. Ph.D. Thesis, University of Bologna, Bologna, Italy, 2020. [Google Scholar]
- Maymandi, H.; Perez-Benitez, J.; Gallegos-Funesa, F.; Perez-Benitez, J. A Novel Monitor for Practical Brain-Computer Interface Applications Based on Visual Evoked Potential. 2020; in preprint. [Google Scholar]
- Hasan, M.A.; Khan, M.U.; Mishra, D. A Computationally Efficient Method for Hybrid EEG-fNIRS BCI Based on the Pearson Correlation. BioMed Res. Int. 2020, 2020, 1838140. [Google Scholar] [CrossRef]
- Wolpaw, J.; McFarland, D. Development of an EEG-based brain-computer interface (BCI). Rehabil. Eng. Soc. N. Am. 1995, 15, 645–648. [Google Scholar]
- Flotzinger, D.; Kalcher, J.; Wolpaw, J. Off-Line Classification of EEG from the “New York Brain-Computer Interface (BCI)”; Technische Universität Graz/Österreichische Computer Gesellschaft: Graz, Austria, 1993. [Google Scholar]
- McFarland, D.; Sarnacki, W.; Wolpaw, J. EEG-based brain-computer interface (BCI): Multiple selections with one dimensional control. Soc. Neurosci. Abstr. 1998, 23, 656. [Google Scholar]
- Pfurtscheller, G.; Flotzinger, D.; Kalcher, J. Brain-computer interface—A new communication device for handicapped persons. J. Microcomput. Appl. 1993, 16, 293–299. [Google Scholar] [CrossRef]
- Cecotti, H. Spelling with non-invasive Brain–Computer Interfaces–Current and future trends. J. Physiol.-Paris 2011, 105, 106–114. [Google Scholar] [CrossRef] [PubMed]
- DEL R. MILLÁN, J.; Ferrez, P.W.; Galán, F.; Lew, E.; Chavarriaga, R. Non-invasive brain-machine interaction. Int. J. Pattern Recognit. Artif. Intell. 2008, 22, 959–972. [Google Scholar]
- Tangermann, M.W.; Krauledat, M.; Grzeska, K.; Sagebaum, M.; Vidaurre, C.; Blankertz, B.; Müller, K.R. Playing pinball with non-invasive BCI. In Proceedings of the 21st International Conference on Neural Information Processing Systems; Curran Associates Inc.: Nice, France, 2008; pp. 1641–1648. [Google Scholar]
- McFarland, D.J.; Lefkowicz, A.T.; Wolpaw, J.R. Design and operation of an EEG-based brain-computer interface with digital signal processing technology. Behav. Res. Methods Instrum. Comput. 1997, 29, 337–345. [Google Scholar] [CrossRef] [Green Version]
- Miner, L.A.; McFarland, D.J.; Wolpaw, J.R. Answering questions with an electroencephalogram-based brain-computer interface. Arch. Phys. Med. Rehabil. 1998, 79, 1029–1033. [Google Scholar] [CrossRef]
- Schalk, G.; McFarland, D.J.; Hinterberger, T.; Birbaumer, N.; Wolpaw, J.R. BCI2000: A general-purpose brain-computer interface (BCI) system. IEEE Trans. Biomed. Eng. 2004, 51, 1034–1043. [Google Scholar] [CrossRef]
- Millán, J.D.R.; Renkens, F.; Mourino, J.; Gerstner, W. Non-invasive brain-actuated control of a mobile robot. In Proceedings of the 18th International Joint Conference on Artificial Intelligence, Acapulco, Mexico, 9–15 August 2003. number CONF. [Google Scholar]
- Kapgate, D. Future of EEG Based Hybrid Visual Brain Computer Interface Systems in Rehabilitation of People with Neurological Disorders. Int. Res. J. Adv. Sci. Hub 2020, 2, 15–20. [Google Scholar] [CrossRef]
- Pfurtscheller, G.; Neuper, C.; Guger, C.; Harkam, W.; Ramoser, H.; Schlogl, A.; Obermaier, B.; Pregenzer, M. Current trends in Graz brain-computer interface (BCI) research. IEEE Trans. Rehabil. Eng. 2000, 8, 216–219. [Google Scholar] [CrossRef]
- Blankertz, B.; Dornhege, G.; Krauledat, M.; Müller, K.R.; Curio, G. The non-invasive Berlin brain–computer interface: Fast acquisition of effective performance in untrained subjects. NeuroImage 2007, 37, 539–550. [Google Scholar] [CrossRef]
- Vaughan, T.M.; McFarland, D.J.; Schalk, G.; Sarnacki, W.A.; Krusienski, D.J.; Sellers, E.W.; Wolpaw, J.R. The wadsworth BCI research and development program: At home with BCI. IEEE Trans. Neural Syst. Rehabil. Eng. 2006, 14, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Pfurtscheller, G.; Neuper, C.; Muller, G.; Obermaier, B.; Krausz, G.; Schlogl, A.; Scherer, R.; Graimann, B.; Keinrath, C.; Skliris, D.; et al. Graz-BCI: State of the art and clinical applications. IEEE Trans. Neural Syst. Rehabil. Eng. 2003, 11, 1–4. [Google Scholar] [CrossRef] [PubMed]
- del R Millan, J.; Mouriño, J.; Franzé, M.; Cincotti, F.; Varsta, M.; Heikkonen, J.; Babiloni, F. A local neural classifier for the recognition of EEG patterns associated to mental tasks. IEEE Trans. Neural Netw. 2002, 13, 678–686. [Google Scholar] [CrossRef] [Green Version]
- Cincotti, F.; Mattia, D.; Aloise, F.; Bufalari, S.; Schalk, G.; Oriolo, G.; Cherubini, A.; Marciani, M.G.; Babiloni, F. Non-invasive brain–computer interface system: Towards its application as assistive technology. Brain Res. Bull. 2008, 75, 796–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schembri, P.; Pelc, M.; Ma, J. The effect that auditory distractions have on a visual P300 speller while utilizing low-cost off-the-shelf equipment. Computers 2020, 9, 68. [Google Scholar] [CrossRef]
- Schembri, P.; Pelc, M.; Ma, J. The Effect that Auxiliary Taxonomized Auditory Distractions have on a P300 Speller while utilising Low Fidelity Equipment. In Proceedings of the 2019 11th Computer Science and Electronic Engineering (CEEC), Colchester, UK, 18–20 September 2019; pp. 118–123. [Google Scholar]
- Allison, B.Z.; Kübler, A.; Jin, J. 30+ years of P300 brain–computer interfaces. Psychophysiology 2020, 57, e13569. [Google Scholar] [CrossRef] [PubMed]
- Ravi, A.; Beni, N.H.; Manuel, J.; Jiang, N. Comparing user-dependent and user-independent training of CNN for SSVEP BCI. J. Neural Eng. 2020, 17, 026028. [Google Scholar] [CrossRef]
- Li, K.; Sankar, R.; Arbel, Y.; Donchin, E. Single trial independent component analysis for P300 BCI system. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 4035–4038. [Google Scholar]
- Jin, J.; Allison, B.Z.; Kaufmann, T.; Kübler, A.; Zhang, Y.; Wang, X.; Cichocki, A. The changing face of P300 BCIs: A comparison of stimulus changes in a P300 BCI involving faces, emotion, and movement. PLoS ONE 2012, 7, e49688. [Google Scholar] [CrossRef]
- Fouad, I.A.; Labib, F.E.Z.M.; Mabrouk, M.S.; Sharawy, A.A.; Sayed, A.Y. Improving the performance of P300 BCI system using different methods. Netw. Model. Anal. Health Inform. Bioinform. 2020, 9, 1–13. [Google Scholar] [CrossRef]
- Eidel, M.; Kübler, A. Wheelchair Control in a Virtual Environment by Healthy Participants Using a P300-BCI Based on Tactile Stimulation: Training Effects and Usability. Front. Hum. Neurosci. 2020, 14, 265. [Google Scholar] [CrossRef]
- Liu, B.; Huang, X.; Wang, Y.; Chen, X.; Gao, X. BETA: A Large Benchmark Database Toward SSVEP-BCI Application. Front. Neurosci. 2020, 14, 627. [Google Scholar] [CrossRef] [PubMed]
- Chailloux Peguero, J.D.; Mendoza-Montoya, O.; Antelis, J.M. Single-Option P300-BCI Performance Is Affected by Visual Stimulation Conditions. Sensors 2020, 20, 7198. [Google Scholar] [CrossRef] [PubMed]
- Berlad, I.; Pratt, H. P300 in response to the subject’s own name. Electroencephalogr. Clin. Neurophysiol. Potentials Sect. 1995, 96, 472–474. [Google Scholar] [CrossRef]
- Polich, J.; Margala, C. P300 and probability: Comparison of oddball and single-stimulus paradigms. Int. J. Psychophysiol. 1997, 25, 169–176. [Google Scholar] [CrossRef]
- Dutt-Mazumder, A.; Huggins, J.E. Performance comparison of a non-invasive P300-based BCI mouse to a head-mouse for people with SCI. Brain-Comput. Interfaces 2020, 7, 1–10. [Google Scholar] [CrossRef]
- Cortez, S.A.; Flores, C.; Andreu-Perez, J. A Smart Home Control Prototype Using a P300-Based Brain–Computer Interface for Post-stroke Patients. In Proceedings of the 5th Brazilian Technology Symposium; Springer: Berlin/Heidelberg, Germany, 2020; pp. 131–139. [Google Scholar]
- Bulat, M.; Karpman, A.; Samokhina, A.; Panov, A. Playing a P300-BCI VR game based leads to changes in cognitive function of healthy adults. bioRxiv 2020. [Google Scholar] [CrossRef]
- Mouli, S.; Palaniappan, R.; Molefi, E.; McLoughlin, I. In-Ear Electrode EEG for Practical SSVEP BCI. Technologies 2020, 8, 63. [Google Scholar] [CrossRef]
- Peters, B.; Bedrick, S.; Dudy, S.; Eddy, B.; Higger, M.; Kinsella, M.; McLaughlin, D.; Memmott, T.; Oken, B.; Quivira, F.; et al. SSVEP BCI and eye tracking use by individuals with late-stage ALS and visual impairments. Front. Hum. Neurosci. 2020, 14, 457. [Google Scholar] [CrossRef]
- Hwang, H.J.; Lim, J.H.; Jung, Y.J.; Choi, H.; Lee, S.W.; Im, C.H. Development of an SSVEP-based BCI spelling system adopting a QWERTY-style LED keyboard. J. Neurosci. Methods 2012, 208, 59–65. [Google Scholar] [CrossRef]
- Muller-Putz, G.R.; Pfurtscheller, G. Control of an electrical prosthesis with an SSVEP-based BCI. IEEE Trans. Biomed. Eng. 2007, 55, 361–364. [Google Scholar] [CrossRef]
- Horki, P.; Solis-Escalante, T.; Neuper, C.; Müller-Putz, G. Combined motor imagery and SSVEP based BCI control of a 2 DoF artificial upper limb. Med. Biol. Eng. Comput. 2011, 49, 567–577. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Zhao, B.; Wang, Y.; Gao, X. Combination of high-frequency SSVEP-based BCI and computer vision for controlling a robotic arm. J. Neural Eng. 2019, 16, 026012. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.S.; Jiang, Z.Y. Implementing remote presence using quadcopter control by a non-invasive BCI device. Comput. Sci. Inf. Technol. 2015, 3, 122–126. [Google Scholar] [CrossRef] [Green Version]
- Cho, J.H.; Jeong, J.H.; Shim, K.H.; Kim, D.J.; Lee, S.W. Classification of hand motions within EEG signals for non-invasive BCI-based robot hand control. In Proceedings of the 2018 IEEE International Conference on Systems, Man, and Cybernetics (SMC), Miyazaki, Japan, 7–10 October 2018; pp. 515–518. [Google Scholar]
- Hiremath, S.V.; Chen, W.; Wang, W.; Foldes, S.; Yang, Y.; Tyler-Kabara, E.C.; Collinger, J.L.; Boninger, M.L. Brain computer interface learning for systems based on electrocorticography and intracortical microelectrode arrays. Front. Integr. Neurosci. 2015, 9, 40. [Google Scholar] [CrossRef] [Green Version]
- Angelakis, E.; Hatzis, A.; Panourias, I.; Sakas, D. Brain-computer interface: A reciprocal self-regulated neuromodulation. In Operative Neuromodulation; Springer: Berlin/Heidelberg, Germany, 2007; pp. 555–559. [Google Scholar]
- Sorger, B.; Goebel, R. Real-time fMRI for brain-computer interfacing. In Handbook of Clinical Neurology; Elsevier: Berlin/Heidelberg, Germany, 2020; Volume 168, pp. 289–302. [Google Scholar]
- Weiskopf, N.; Mathiak, K.; Bock, S.W.; Scharnowski, F.; Veit, R.; Grodd, W.; Goebel, R.; Birbaumer, N. Principles of a brain-computer interface (BCI) based on real-time functional magnetic resonance imaging (fMRI). IEEE Trans. Biomed. Eng. 2004, 51, 966–970. [Google Scholar] [CrossRef]
- Sitaram, R.; Veit, R.; Stevens, B.; Caria, A.; Gerloff, C.; Birbaumer, N.; Hummel, F. Acquired control of ventral premotor cortex activity by feedback training: An exploratory real-time FMRI and TMS study. Neurorehabilit. Neural Repair 2012, 26, 256–265. [Google Scholar] [CrossRef]
- Rota, G.; Handjaras, G.; Sitaram, R.; Birbaumer, N.; Dogil, G. Reorganization of functional and effective connectivity during real-time fMRI-BCI modulation of prosody processing. Brain Lang. 2011, 117, 123–132. [Google Scholar] [CrossRef]
- Sitaram, R.; Weiskopf, N.; Caria, A.; Veit, R.; Erb, M.; Birbaumer, N. fMRI brain-computer interfaces. IEEE Signal Process. Mag. 2007, 25, 95–106. [Google Scholar] [CrossRef]
- Liberati, G.; Veit, R.; Kim, S.; Birbaumer, N.; Von Arnim, C.; Jenner, A.; Lulé, D.; Ludolph, A.C.; Raffone, A.; Belardinelli, M.O.; et al. Development of a binary fMRI-BCI for Alzheimer patients: A semantic conditioning paradigm using affective unconditioned stimuli. In Proceedings of the 2013 Humaine Association Conference on Affective Computing and Intelligent Interaction, Geneva, Switzerland, 2–5 September 2013; pp. 838–842. [Google Scholar]
- Simon, J.; Fishbein, P.; Zhu, L.; Roberts, M.; Martin, I. Functional Magnetic Resonance Imaging-Based Brain Computer Interfaces. In Neural Interface Engineering; Springer: Berlin/Heidelberg, Germany, 2020; pp. 17–47. [Google Scholar]
- Rieke, J.D.; Matarasso, A.K.; Yusufali, M.M.; Ravindran, A.; Alcantara, J.; White, K.D.; Daly, J.J. Development of a Combined, Sequential Real-Time fMRI and fNIRS Neurofeedback System Enhance Motor Learning After Stroke. J. Neurosci. Methods 2020, 341, 108719. [Google Scholar] [CrossRef]
- Almulla, L.; Al-Naib, I.; Althobaiti, M. Hemodynamic responses during standing and sitting activities: A study toward fNIRS-BCI. Biomed. Phys. Eng. Express 2020, 6, 055005. [Google Scholar] [CrossRef]
- Nazeer, H.; Naseer, N.; Khan, R.A.; Noori, F.M.; Qureshi, N.K.; Khan, U.S.; Khan, M.J. Enhancing classification accuracy of fNIRS-BCI using features acquired from vector-based phase analysis. J. Neural Eng. 2020, 17, 056025. [Google Scholar] [CrossRef] [PubMed]
- Mandal, S.; Singh, B.; Thakur, K. Classification of working memory loads using hybrid EEG and fNIRS in machine learning paradigm. Electron. Lett. 2020, 56, 1386–1389. [Google Scholar] [CrossRef]
- Ghonchi, H.; Fateh, M.; Abolghasemi, V.; Ferdowsi, S.; Rezvani, M. Spatio-temporal deep learning for EEG-fNIRS brain computer interface. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 124–127. [Google Scholar]
- Li, F.; Tao, Q.; Peng, W.; Zhang, T.; Si, Y.; Zhang, Y.; Yi, C.; Biswal, B.; Yao, D.; Xu, P. Inter-subject P300 variability relates to the efficiency of brain networks reconfigured from resting-to task-state: Evidence from a simultaneous event-related EEG-fMRI study. NeuroImage 2020, 205, 116285. [Google Scholar] [CrossRef] [PubMed]
- Martini, M.L.; Oermann, E.K.; Opie, N.L.; Panov, F.; Oxley, T.; Yaeger, K. Sensor modalities for brain-computer interface technology: A comprehensive literature review. Neurosurgery 2020, 86, E108–E117. [Google Scholar] [CrossRef]
- Jerbi, K.; Vidal, J.; Mattout, J.; Maby, E.; Lecaignard, F.; Ossandon, T.; Hamamé, C.; Dalal, S.; Bouet, R.; Lachaux, J.P.; et al. Inferring hand movement kinematics from MEG, EEG and intracranial EEG: From brain-machine interfaces to motor rehabilitation. Irbm 2011, 32, 8–18. [Google Scholar] [CrossRef]
- LaRocco, J.; Le, M.D.; Paeng, D.G. A systemic review of available low-cost EEG headsets used for drowsiness detection. Front. Neuroinform. 2020, 14, 42. [Google Scholar] [CrossRef]
- de Lissa, P.; Sörensen, S.; Badcock, N.; Thie, J.; McArthur, G. Measuring the face-sensitive N170 with a gaming EEG system: A validation study. J. Neurosci. Methods 2015, 253, 47–54. [Google Scholar] [CrossRef]
- Doudou, M.; Bouabdallah, A.; Cherfaoui, V. A Light on Physiological Sensors for Efficient Driver Drowsiness Detection System. Sens. Transducers J. 2018, 224, 39–50. [Google Scholar]
- Aghaei-Lasboo, A.; Inoyama, K.; Fogarty, A.S.; Kuo, J.; Meador, K.J.; Walter, J.J.; Le, S.T.; Graber, K.D.; Razavi, B.; Fisher, R.S. Tripolar concentric EEG electrodes reduce noise. Clin. Neurophysiol. 2020, 131, 193–198. [Google Scholar] [CrossRef]
- Liu, X.; Makeyev, O.; Besio, W. Improved Spatial Resolution of Electroencephalogram Using Tripolar Concentric Ring Electrode Sensors. J. Sens. 2020, 2020, 6269394. [Google Scholar] [CrossRef]
- g.tec Medical Engineering | Brain-Computer Interfaces and Neurotechnology. Available online: https://www.gtec.at/ (accessed on 29 October 2020).
- Vasiljevic, G.A.M.; de Miranda, L.C. Brain–computer interface games based on consumer-grade EEG Devices: A systematic literature review. Int. J. Hum.-Comput. Interact. 2020, 36, 105–142. [Google Scholar] [CrossRef]
- Chi, Y.M.; Wang, Y.T.; Wang, Y.; Maier, C.; Jung, T.P.; Cauwenberghs, G. Dry and noncontact EEG sensors for mobile brain–computer interfaces. IEEE Trans. Neural Syst. Rehabil. Eng. 2011, 20, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Gu, X.; Cao, Z.; Jolfaei, A.; Xu, P.; Wu, D.; Jung, T.P.; Lin, C.T. EEG-based Brain-Computer Interfaces (BCIs): A Survey of Recent Studies on Signal Sensing Technologies and Computational Intelligence Approaches and their Applications. arXiv 2020, arXiv:2001.11337. [Google Scholar]
- Belkacem, A.N.; Jamil, N.; Palmer, J.A.; Ouhbi, S.; Chen, C. Brain computer interfaces for improving the quality of life of older adults and elderly patients. Front. Neurosci. 2020, 14, 692. [Google Scholar] [CrossRef]
- OpenBCI—Open Source Biosensing Tools (EEG, EMG, EKG, and more). Available online: https://openbci.com/ (accessed on 27 October 2020).
- EMOTIV | Brain Data Measuring Hardware and Software Solutions. Available online: https://www.emotiv.com/ (accessed on 27 October 2020).
- Muse™—Meditation Made Easy with the Muse Headband. Available online: https://choosemuse.com/ (accessed on 27 October 2020).
- Stytsenko, K.; Jablonskis, E.; Prahm, C. Evaluation of consumer EEG device Emotiv EPOC. In MEi: CogSci Conference 2011; Universitat Wien: Ljubljana, Slovenia, 2011. [Google Scholar]
- Liu, Y.; Jiang, X.; Cao, T.; Wan, F.; Mak, P.U.; Mak, P.I.; Vai, M.I. Implementation of SSVEP based BCI with Emotiv EPOC. In Proceedings of the 2012 IEEE International Conference on Virtual Environments Human-Computer Interfaces and Measurement Systems (VECIMS) Proceedings, Tianjin, China, 2–4 July 2012; pp. 34–37. [Google Scholar]
- EEG—ECG—Biosensors. Available online: http://neurosky.com/ (accessed on 27 October 2020).
- Crowley, K.; Sliney, A.; Pitt, I.; Murphy, D. Evaluating a brain-computer interface to categorise human emotional response. In Proceedings of the 2010 10th IEEE International Conference on Advanced Learning Technologies, Sousse, Tunisia, 5–7 July 2010; pp. 276–278. [Google Scholar]
- Lakhan, P.; Banluesombatkul, N.; Changniam, V.; Dhithijaiyratn, R.; Leelaarporn, P.; Boonchieng, E.; Hompoonsup, S.; Wilaiprasitporn, T. Consumer grade brain sensing for emotion recognition. IEEE Sens. J. 2019, 19, 9896–9907. [Google Scholar] [CrossRef] [Green Version]
- Frey, J. Comparison of a consumer grade EEG amplifier with medical grade equipment in BCI applications. Proceedins of the 2016 6th International BCI Meeting – BCI Past, Present and Future, Asilomar Conference Center, Pacific Grove, CA, USA, 30 May–3 June 2016. [Google Scholar]
- Frey, J. Comparison of an open-hardware electroencephalography amplifier with medical grade device in brain-computer interface applications. arXiv 2016, arXiv:1606.02438. [Google Scholar]
- Haddix, C.; Bahrani, A.A.; Kawala-Janik, A.; Besio, W.G.; Yu, G.; Sunderam, S. Trial measurement of movement-related cortical dynamics using electroencephalography and diffuse correlation spectroscopy. In Proceedings of the 2017 22nd International Conference on Methods and Models in Automation and Robotics (MMAR), Miedzyzdroje, Poland, 28–31 August 2017; pp. 642–645. [Google Scholar]
- Makeyev, O.; Ding, Q.; Kay, S.M.; Besio, W.G. Sensor integration of multiple tripolar concentric ring electrodes improves pentylenetetrazole-induced seizure onset detection in rats. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 5154–5157. [Google Scholar]
- Makeyev, O.; Ding, Q.; Martínez-Juárez, I.E.; Gaitanis, J.; Kay, S.M.; Besio, W.G. Multiple sensor integration for seizure onset detection in human patients comparing conventional disc versus novel tripolar concentric ring electrodes. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 17–20. [Google Scholar]
- Müller-Putz, G.R.; Scherer, R.; Pfurtscheller, G.; Rupp, R. EEG-based neuroprosthesis control: A step towards clinical practice. Neurosci. Lett. 2005, 382, 169–174. [Google Scholar] [CrossRef]
- Kuś, R.; Duszyk, A.; Milanowski, P.; Łabęcki, M.; Bierzyńska, M.; Radzikowska, Z.; Michalska, M.; Żygierewicz, J.; Suffczyński, P.; Durka, P.J. On the quantification of SSVEP frequency responses in human EEG in realistic BCI conditions. PLoS ONE 2013, 8, e77536. [Google Scholar] [CrossRef] [Green Version]
- Volosyak, I.; Valbuena, D.; Malechka, T.; Peuscher, J.; Gräser, A. Brain–computer interface using water-based electrodes. J. Neural Eng. 2010, 7, 066007. [Google Scholar] [CrossRef]
- Chabuda, A.; Durka, P.; Żygierewicz, J. High frequency SSVEP-BCI with hardware stimuli control and phase-synchronized comb filter. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 26, 344–352. [Google Scholar] [CrossRef]
- Tung, S.W.; Guan, C.; Ang, K.K.; Phua, K.S.; Wang, C.; Zhao, L.; Teo, W.P.; Chew, E. Motor imagery BCI for upper limb stroke rehabilitation: An evaluation of the EEG recordings using coherence analysis. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 261–264. [Google Scholar]
- Onose, G.; Grozea, C.; Anghelescu, A.; Daia, C.; Sinescu, C.; Ciurea, A.; Spircu, T.; Mirea, A.; Andone, I.; Spânu, A.; et al. On the feasibility of using motor imagery EEG-based brain–computer interface in chronic tetraplegics for assistive robotic arm control: A clinical test and long-term post-trial follow-up. Spinal Cord 2012, 50, 599–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katona, J.; Kovari, A. The evaluation of bci and pebl-based attention tests. Acta Polytech. Hung. 2018, 15, 225–249. [Google Scholar]
- Fazli, S.; Danóczy, M.; Popescu, F.; Blankertz, B.; Müller, K.R. Using rest class and control paradigms for brain computer interfacing. In International Work-Conference on Artificial Neural Networks; Springer: Berlin/Heidelberg, Germany, 2009; pp. 651–665. [Google Scholar]
- Bancaud, J.; Dell, M. Technics and method of stereotaxic functional exploration of the brain structures in man (cortex, subcortex, central gray nuclei). Rev. Neurol. 1959, 101, 213. [Google Scholar] [PubMed]
- Herff, C.; Krusienski, D.J.; Kubben, P. The Potential of Stereotactic-EEG for Brain-Computer Interfaces: Current Progress and Future Directions. Front. Neurosci. 2020, 14, 123. [Google Scholar] [CrossRef] [Green Version]
- Guenot, M.; Isnard, J.; Ryvlin, P.; Fischer, C.; Ostrowsky, K.; Mauguiere, F.; Sindou, M. Neurophysiological monitoring for epilepsy surgery: The Talairach SEEG method. Stereotact. Funct. Neurosurg. 2001, 77, 29–32. [Google Scholar] [CrossRef]
- Allen, P.; Fish, D.; Smith, S. Very high-frequency rhythmic activity during SEEG suppression in frontal lobe epilepsy. Electroencephalogr. Clin. Neurophysiol. 1992, 82, 155–159. [Google Scholar] [CrossRef]
- Sharma, A.; Rai, J.K.; Tewari, R.P. Scalp electroencephalography (sEEG) based advanced prediction of epileptic seizure time and identification of epileptogenic region. Biomed. Eng. Tech. 2020, 65, 705–720. [Google Scholar] [CrossRef]
- Chandrasekaran, S.; Bickel, S.; Herrero, J.L.; Kim, J.W.; Markowitz, N.; Espinal, E.; Bhagat, N.A.; Ramdeo, R.; Xu, J.; Glasser, M.F.; et al. Evoking highly focal percepts in the fingertips through targeted stimulation of sulcal regions of the brain for sensory restoration. medRxiv 2020. [Google Scholar] [CrossRef]
- Talukdar, U.; Hazarika, S.M.; Gan, J.Q. Adaptation of Common Spatial Patterns based on mental fatigue for motor-imagery BCI. Biomed. Signal Process. Control 2020, 58, 101829. [Google Scholar] [CrossRef]
- Wong, C.M.; Wang, B.; Wang, Z.; Lao, K.F.; Rosa, A.; Wan, F. Spatial Filtering in SSVEP-based BCIs: Unified Framework and New Improvements. IEEE Trans. Biomed. Eng. 2020, 67, 3057–3072. [Google Scholar] [CrossRef]
- Gaber, A.; Ghazali, M. Trends in Brain Computer Interfaces. EURASIP J. Adv. Signal Process. 2005, 2005, 861614. [Google Scholar]
- Zander, T.O.; Kothe, C.; Jatzev, S.; Gaertner, M. Enhancing human-computer interaction with input from active and passive brain-computer interfaces. In Brain-Computer Interfaces; Springer: Berlin/Heidelberg, Germany, 2010; pp. 181–199. [Google Scholar]
- Andreessen, L.M.; Gerjets, P.; Meurers, D.; Zander, T.O. Toward neuroadaptive support technologies for improving digital reading: A passive BCI-based assessment of mental workload imposed by text difficulty and presentation speed during reading. User Model. User-Adapt. Interact. 2020, 1–30. [Google Scholar] [CrossRef]
- Elsawy, A.S.; Eldawlatly, S.; Taher, M.; Aly, G.M. MindEdit: A P300-based text editor for mobile devices. Comput. Biol. Med. 2017, 80, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Jijun, T.; Peng, Z.; Ran, X.; Lei, D. The portable P300 dialing system based on tablet and Emotiv Epoc headset. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 566–569. [Google Scholar]
- Tahmasebzadeh, A.; Bahrani, M.; Setarehdan, S.K. Development of a robust method for an online P300 Speller Brain Computer Interface. In Proceedings of the 2013 6th International IEEE/EMBS Conference on Neural Engineering (NER), San Diego, CA, USA, 6–8 November 2013; pp. 1070–1075. [Google Scholar]
- Meshriky, M.R.; Eldawlatly, S.; Aly, G.M. An intermixed color paradigm for P300 spellers: A comparison with gray-scale spellers. In Proceedings of the 2017 IEEE 30th International Symposium on Computer-Based Medical Systems (CBMS), Thessaloniki, Greece, 22–24 June 2017; pp. 242–247. [Google Scholar]
- Browarska, N.; Kawala-Sterniuk, A.; Zygarlicki, J. Initial study on changes in activity of brain waves during audio stimulation using noninvasive brain—Computer interfaces: Choosing the appropriate filtering method. Bio-Algorithms Med-Syst. 2020, 20200051. [Google Scholar] [CrossRef]
- Worthen-Chaudhari, L.C.; McNally, M.P.; Deshpande, A.; Bakaraju, V. In-Home Neurogaming: Demonstrating the impact of valid gesture recognition method on high volume kinematic outcomes. J. Biomech. 2020, 104, 109726. [Google Scholar] [CrossRef]
- Beveridge, R.; Wilson, S.; Callaghan, M.; Coyle, D. Neurogaming with motion-onset visual evoked potentials (mVEPs): Adults versus teenagers. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 572–581. [Google Scholar] [CrossRef]
- Putze, F.; Vourvopoulos, A.; Lécuyer, A.; Krusienski, D.; i Badia, S.B.; Mullen, T.; Herff, C. Brain-Computer Interfaces and Augmented/Virtual Reality. Front. Hum. Neurosci. 2020, 14, 144. [Google Scholar] [CrossRef]
- Putze, F.; Weiß, D.; Vortmann, L.M.; Schultz, T. Augmented Reality Interface for Smart Home Control using SSVEP-BCI and Eye Gaze. In Proceedings of the IEEE International Conference on Systems, Man, and Cybernetics, Bari, Italy, 6–9 October 2019. [Google Scholar]
- Juarez, D.; Tur-Viñes, V.; Mengual, A. Neuromarketing Applied to Educational Toy Packaging. Front. Psychol. 2020, 11, 2077. [Google Scholar] [CrossRef]
- Nilashi, M.; Samad, S.; Ahmadi, N.; Ahani, A.; Abumalloh, R.A.; Asadi, S.; Abdullah, R.; Ibrahim, O.; Yadegaridehkordi, E. Neuromarketing: A Review of Research and Implications for Marketing. J. Soft Comput. Decis. Support Syst. 2020, 7, 23–31. [Google Scholar]
- Hsu, L.; Chen, Y.J. Music and wine tasting: An experimental neuromarketing study. Br. Food J. 2019, 122. [Google Scholar] [CrossRef] [Green Version]
- Aldayel, M.; Ykhlef, M.; Al-Nafjan, A. Deep Learning for EEG-Based Preference Classification in Neuromarketing. Appl. Sci. 2020, 10, 1525. [Google Scholar] [CrossRef] [Green Version]
- Shahriari, M.; Feiz, D.; Zarei, A.; Kashi, E. The meta-analysis of neuro-marketing studies: Past, present and future. Neuroethics 2020, 13, 261–273. [Google Scholar] [CrossRef]
- Luth, T.; Ojdanic, D.; Friman, O.; Prenzel, O.; Graser, A. Low level control in a semi-autonomous rehabilitation robotic system via a brain-computer interface. In Proceedings of the 2007 IEEE 10th International Conference on Rehabilitation Robotics, Noordwijk, The Netherlands, 13–15 June 2007; pp. 721–728. [Google Scholar]
- Xiong, M.; Hotter, R.; Nadin, D.; Patel, J.; Tartakovsky, S.; Wang, Y.; Patel, H.; Axon, C.; Bosiljevac, H.; Brandenberger, A.; et al. A Low-Cost, Semi-Autonomous Wheelchair Controlled by Motor Imagery and Jaw Muscle Activation. In Proceedings of the 2019 IEEE International Conference on Systems, Man and Cybernetics (SMC), Bari, Italy, 6–9 October 2019; pp. 2180–2185. [Google Scholar]
- Stephe, S.; Kumar, T.J.K.V. Imagery Recognition of EEG Signal Using Cuckoo-Search Masking Empirical Mode Decomposition. Int. J. Innov. Technol. Explor. Eng. (IJITEE) 2019, 8, 2717–2720. [Google Scholar]
- Zgallai, W.; Brown, J.T.; Ibrahim, A.; Mahmood, F.; Mohammad, K.; Khalfan, M.; Mohammed, M.; Salem, M.; Hamood, N. Deep learning AI application to an EEG driven BCI smart wheelchair. In Proceedings of the 2019 Advances in Science and Engineering Technology International Conferences (ASET), Dubai, UAE, 26 March–10 April 2019; pp. 1–5. [Google Scholar]
- Rebsamen, B.; Guan, C.; Zhang, H.; Wang, C.; Teo, C.; Ang, M.H.; Burdet, E. A brain controlled wheelchair to navigate in familiar environments. IEEE Trans. Neural Syst. Rehabil. Eng. 2010, 18, 590–598. [Google Scholar] [CrossRef] [Green Version]
- Leaman, J.; La, H.M. A comprehensive review of smart wheelchairs: Past, present, and future. IEEE Trans. Hum.-Mach. Syst. 2017, 47, 486–499. [Google Scholar] [CrossRef] [Green Version]
- Murugappan, M.; Ramachandran, N.; Sazali, Y. Classification of human emotion from EEG using discrete wavelet transform. J. Biomed. Sci. Eng. 2010, 3, 390. [Google Scholar] [CrossRef] [Green Version]
- Vortmann, L.M.; Putze, F. Attention-Aware Brain Computer Interface to avoid Distractions in Augmented Reality. In Proceedings of the 2020 CHI Conference on Human Factors in Computing Systems, Honolulu, HI, USA, 25 April 2020. [Google Scholar]
- Browarska, N.; Kawala-Sterniuk, A.; Chechelski, P.; Zygarlicki, J. Analysis of brain waves changes in stressful situations based on horror game with the implementation of virtual reality and brain-computer interface system: A case study. Bio-Algorithms Med-Syst. 2020, 1. [Google Scholar] [CrossRef]
- Kołodziej, M.; Tarnowski, P.; Sawicki, D.; Majkowski, A.; Rak, R.; Bala, A.; Pluta, A. Fatigue Detection Caused by Office Work with the Use of EOG Signal. IEEE Sens. J. 2020, 20, 15213–15223. [Google Scholar] [CrossRef]
- Wolska, A.; Sawicki, D.; Nowak, K.; Wisełka, M.; Kołodziej, M. Method of Acute Alertness Level Evaluation after Exposure to Blue and Red Light (based on EEG): Technical Aspects. In Proceedings of the 6th International Congress on Neurotechnology, Electronics and Informatics (NEUROTECHNIX 2018), Seville, Spain, 20–21 September 2018; pp. 19–21. [Google Scholar]
- Kubacki, A.; Jakubowski, A. Controlling the industrial robot model with the hybrid BCI based on EOG and eye tracking. In AIP Conference Proceedings; AIP Publishing LLC: Melville, NY, USA, 2018; Volume 2029, p. 020032. [Google Scholar]
- Garcia, A.P.; Schjølberg, I.; Gale, S. EEG control of an industrial robot manipulator. In Proceedings of the 2013 IEEE 4th International Conference on Cognitive Infocommunications (CogInfoCom), Budapest, Hungary, 2–5 December 2013; pp. 39–44. [Google Scholar]
- Mason, C.; Gadzicki, K.; Meier, M.; Ahrens, F.; Kluss, T.; Maldonado, J.; Putze, F.; Fehr, T.; Zetzsche, C.; Herrmann, M.; et al. From Human to Robot Everyday Activity. In Proceedings of the 2020 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS), Las Vegas, NV, USA (Virtual), 25–29 October 2020; pp. 8997–9004. [Google Scholar]
- Kosmyna, N.; Tarpin-Bernard, F.; Bonnefond, N.; Rivet, B. Feasibility of BCI control in a realistic smart home environment. Front. Hum. Neurosci. 2016, 10, 416. [Google Scholar] [CrossRef] [Green Version]
- Saboor, A.; Rezeika, A.; Stawicki, P.; Gembler, F.; Benda, M.; Grunenberg, T.; Volosyak, I. SSVEP-based BCI in a smart home scenario. In International Work-Conference on Artificial Neural Networks; Springer: Cham, Switzerland, 2017; pp. 474–485. [Google Scholar]
- Carabalona, R.; Grossi, F.; Tessadri, A.; Castiglioni, P.; Caracciolo, A.; de Munari, I. Light on! Real world evaluation of a P300-based brain–computer interface (BCI) for environment control in a smart home. Ergonomics 2012, 55, 552–563. [Google Scholar] [CrossRef]
- Kim, H.J.; Lee, M.H.; Lee, M. A BCI based Smart Home System Combined with Event-related Potentials and Speech Imagery Task. In Proceedings of the 2020 8th International Winter Conference on Brain-Computer Interface (BCI), Gangwon, Korea, 26–28 February 2020; pp. 1–6. [Google Scholar]
- Alrajhi, W.; Alaloola, D.; Albarqawi, A. Smart home: Toward daily use of BCI-based systems. In Proceedings of the 2017 International Conference on Informatics, Health & Technology (ICIHT), Riyadh, Saudi Arabia, 21–23 February 2017; pp. 1–5. [Google Scholar]
- Ang, K.K.; Guan, C. Brain–computer interface for neurorehabilitation of upper limb after stroke. Proc. IEEE 2015, 103, 944–953. [Google Scholar] [CrossRef]
- Zieliński, T.P. Cyfrowe Przetwarzanie Sygnałów: Od Teorii do Zastosowań; Wydawnictwa Komunikacji Łączności: Warsaw, Poland, 2005. [Google Scholar]
- Miao, G.J.; Clements, M.A. Digital Signal Processing and Statistical Classification; Artech House: Norwood, MA, USA, 2002. [Google Scholar]
- Enderle, J.; Bronzino, J. Introduction to Biomedical Engineering; Academic Press: Cambridge, MA, USA, 2012. [Google Scholar]
- Kang, H.J.; Kawasawa, Y.I.; Cheng, F.; Zhu, Y.; Xu, X.; Li, M.; Sousa, A.M.; Pletikos, M.; Meyer, K.A.; Sedmak, G.; et al. Spatio-temporal transcriptome of the human brain. Nature 2011, 478, 483–489. [Google Scholar] [CrossRef] [Green Version]
- Kawala-Janik, A.; Pelc, M.; Podpora, M. Method for EEG signals pattern recognition in embedded systems. Elektron. Elektrotechnika 2015, 21, 3–9. [Google Scholar] [CrossRef] [Green Version]
- Rodin, E.; Funke, M.; Berg, P.; Matsuo, F. Magnetoencephalographic spikes not detected by conventional electroencephalography. Clin. Neurophysiol. 2004, 115, 2041–2047. [Google Scholar] [CrossRef]
- Wang, G.; Worrell, G.; Yang, L.; Wilke, C.; He, B. Interictal spike analysis of high-density EEG in patients with partial epilepsy. Clin. Neurophysiol. 2011, 122, 1098–1105. [Google Scholar] [CrossRef] [Green Version]
- Breitling, C.; Zaehle, T.; Dannhauer, M.; Tegelbeckers, J.; Flechtner, H.H.; Krauel, K. Comparison between conventional and HD-tDCS of the right inferior frontal gyrus in children and adolescents with ADHD. Clin. Neurophysiol. 2020, 131, 1146–1154. [Google Scholar] [CrossRef]
- Alhaddad, M.J. Common average reference (CAR) improves P300 speller. Int. J. Eng. Technol. 2012, 2, 21. [Google Scholar]
- Laiho, J. Recognizing Thoughts from Bioelectric Patterns? A Brain-Computer Interface with Deep Learning. Master’s Thesis, Perustieteiden korkeakoulu, Espoo, Finland, 2020. [Google Scholar]
- Wang, L.; Huang, W.; Yang, Z.; Hu, X.; Zhang, C. A method from offline analysis to online training for the brain-computer interface based on motor imagery and speech imagery. Biomed. Signal Process. Control 2020, 62, 102100. [Google Scholar] [CrossRef]
- Grozea, C.; Voinescu, C.D.; Fazli, S. Bristle-sensors—Low-cost flexible passive dry EEG electrodes for neurofeedback and BCI applications. J. Neural Eng. 2011, 8, 025008. [Google Scholar] [CrossRef]
- Saab, J.; Battes, B.; Grosse-Wentrup, M.; Scherer, R.; Billinger, M.; Kreilinger, A. Simultaneous EEG Recordings with Dry and Wet Electrodes in Motor-Imagery; Citeseer: University Park, PA, USA, 2011. [Google Scholar]
- Klekowicz, H. Opis i Identyfikacja Struktur Przejściowych w Sygnale EEG. Doctoral Thesis, Warsaw University, Warsaw, Poland, 2012. [Google Scholar]
- Kutz, M. Biomedical Engineering and Design Handbook; McGraw-Hill: New York, NY, USA, 2009. [Google Scholar]
- Tumanski, S. Principles of Electrical Measurement; CRC Press: Boca Raton, FL, USA, 2006. [Google Scholar]
- Semmlow, J.L.; Griffel, B. Biosignal and Medical Image Processing; CRC Press: Boca Raton, FL, USA, 2014. [Google Scholar]
- Jiang, X.; Bian, G.B.; Tian, Z. Removal of artifacts from EEG signals: A review. Sensors 2019, 19, 987. [Google Scholar] [CrossRef] [Green Version]
- Chahid, A.; Laleg-Kirati, T.M. Optimized Biosignals Decomposition and Denoising Using Schrodinger Operator. 2020. Available online: https://repository.kaust.edu.sa/handle/10754/662791 (accessed on 27 October 2020).
- Abtahi, F.; Seoane, F.; Lindecrantz, K. Electrical bioimpedance spectroscopy in time-variant systems: Is undersampling always a problem? J. Electr. Bioimpedance 2014, 5, 28–33. [Google Scholar] [CrossRef] [Green Version]
- Causevic, E.; Morley, R.E.; Wickerhauser, M.V.; Jacquin, A.E. Fast wavelet estimation of weak biosignals. IEEE Trans. Biomed. Eng. 2005, 52, 1021–1032. [Google Scholar] [CrossRef]
- Bagchi, S.; Mitra, S.K. The Nonuniform Discrete Fourier Transform and Its Applications in Signal Processing; Kluwer Academic Publishers: Dordrecht, The Netherlands, 1999. [Google Scholar]
- Khan, A. Digital Signal Processing Fundamentals; Firewall Media: New Delhi, India, 2005. [Google Scholar]
- Baby Deepa, V.; Thangaraj, P. A study on classification of EEG Data using the Filters. Int. J. Adv. Comput. Sci. Appl. (IJACSA) 2011, 2, 1–140. [Google Scholar]
- Philips, C.L. Signals, Systems, and Transforms, 3rd ed.; Prentice Hall: Upper Saddle River, NJ, USA, 2003. [Google Scholar]
- Oppenheim, A.; Willsky, A.; Young, I. Signals and Systems; Prentice Hall: Upper Saddle River, NJ, USA, 1983. [Google Scholar]
- Bruce, E.N. Biomedical Signal Processing and Signal Modeling; John Wiley and Sons: Hoboken, NJ, USA, 2000. [Google Scholar]
- Yang, Y.; Peng, Z.; Zhang, W.; Meng, G. Parameterised time-frequency analysis methods and their engineering applications: A review of recent advances. Mech. Syst. Signal Process. 2019, 119, 182–221. [Google Scholar] [CrossRef]
- Kang, M.; Jung, J.; Shin, S.; Kang, K.H.; Kim, Y.T. Multi bio-signal based algorithm using EMD and FFT for stress analysis. In Proceedings of the 2020 IEEE International Conference on Consumer Electronics (ICCE), Las Vegas, NV, USA, 4–6 January 2020; pp. 1–4. [Google Scholar]
- Xizheng, Z.; Yin, L.; Wang, W. Wavelet Time-frequency Analysis of Electro-encephalogram (EEG) Processing. Int. J. Adv. Comput. Sci. Appl. 2010, 1. [Google Scholar] [CrossRef]
- Geetha, G.; Geethalakshmi, S. Scrutinizing different techniques for artifact removal from EEG signals. Int. J. Eng. Sci. Technol. (IJEST) 2011, 3, 1167–1172. [Google Scholar]
- George, S.T.; Subathra, M.; Sairamya, N.; Susmitha, L.; Premkumar, M.J. Classification of epileptic EEG signals using PSO based artificial neural network and tunable-Q wavelet transform. Biocybern. Biomed. Eng. 2020, 40, 709–728. [Google Scholar] [CrossRef]
- Teolis, A. Computational Signal Processing with Wavelets; Birkaeuser Boston: Boston, MA, USA, 1998. [Google Scholar]
- Kawala, A.; Khoma, V.; Zmarzły, D.; Sovyn, Y. Use of wavelet transform for qualification of rheograms characteristic points. Przegląd Elektrotechniczny 2008, 84, 132–133. [Google Scholar]
- Nishad, A.; Upadhyay, A.; Reddy, G.R.S.; Bajaj, V. Classification of epileptic EEG signals using sparse spectrum based empirical wavelet transform. Electron. Lett. 2020, 56, 1370–1372. [Google Scholar] [CrossRef]
- Desai, R.; Porob, P.; Rebelo, P.; Edla, D.R.; Bablani, A. EEG Data Classification for Mental State Analysis Using Wavelet Packet Transform and Gaussian Process Classifier. Wirel. Pers. Commun. 2020, 115, 2149–2169. [Google Scholar] [CrossRef]
- Moghavvemi, M.; Attaran, A.; Esfahani, M.M. EEG artifact signals tracking and filtering in real time for command control application. In 5th Kuala Lumpur International Conference on Biomedical Engineering 2011; Springer: Berlin/Heidelberg, Germany, 2011; pp. 503–506. [Google Scholar]
- Supratak, A.; Wu, C.; Dong, H.; Sun, K.; Guo, Y. Survey on feature extraction and applications of biosignals. In Machine Learning for Health Informatics; Springer: Berlin/Heidelberg, Germany, 2016; pp. 161–182. [Google Scholar]
- Maćkiewicz, A.; Ratajczak, W. Principal components analysis (PCA). Comput. Geosci. 1993, 19, 303–342. [Google Scholar] [CrossRef]
- Richardson, M. Principal Component Analysis. Available online: http://people.maths.ox.ac.uk/richardsonm/SignalProcPCA.pdf (accessed on 2 January 2021).
- Molla, M.K.I.; Islam, M.R.; Tanaka, T.; Rutkowski, T.M. Artifact suppression from EEG signals using data adaptive time domain filtering. Neurocomputing 2012, 97, 297–308. [Google Scholar] [CrossRef]
- Domínguez-Jiménez, J.A.; Campo-Landines, K.C.; Martínez-Santos, J.; Delahoz, E.J.; Contreras-Ortiz, S. A machine learning model for emotion recognition from physiological signals. Biomed. Signal Process. Control 2020, 55, 101646. [Google Scholar] [CrossRef]
- Elkerdawy, M.; Elhalaby, M.; Hassan, A.; Maher, M.; Shawky, D.; Badawi, A. Building Cognitive Profiles of Learners Using EEG. In Proceedings of the 2020 11th International Conference on Information and Communication Systems (ICICS), Irbid, Jordan, 7–9 April 2020; pp. 027–032. [Google Scholar]
- Martinek, R.; Kahankova, R.; Jezewski, J.; Jaros, R.; Mohylova, J.; Fajkus, M.; Nedoma, J.; Janku, P.; Nazeran, H. Comparative effectiveness of ICA and PCA in extraction of fetal ECG from abdominal signals: Toward non-invasive fetal monitoring. Front. Physiol. 2018, 9, 648. [Google Scholar] [CrossRef] [Green Version]
- Jobst, B.C.; Bartolomei, F.; Diehl, B.; Frauscher, B.; Kahane, P.; Minotti, L.; Sharan, A.; Tardy, N.; Worrell, G.; Gotman, J. Intracranial EEG in the 21st Century. Epilepsy Curr. 2020, 20, 180–188. [Google Scholar] [CrossRef]
- Reza, M.S.; Ma, J. ICA and PCA integrated feature extraction for classification. In Proceedings of the 2016 IEEE 13th International Conference on Signal Processing (ICSP), Chengdu, China, 6–10 November 2016; pp. 1083–1088. [Google Scholar]
- Pająk, M.; Muślewski, Ł.; Landowski, B.; Grządziela, A. Fuzzy identification of the reliability state of the mine detecting ship propulsion system. Pol. Marit. Res. 2019, 26, 55–64. [Google Scholar]
- Zadeh, L.A. Fuzzy logic. Computer 1988, 21, 83–93. [Google Scholar] [CrossRef]
- Al-Kadi, D.; Muhiuddin, G. Bipolar fuzzy BCI-implicative ideals of BCI-algebras. Ann. Commun. Math. 2020, 3, 88–96. [Google Scholar]
- Ghumman, M.K.; Singh, S.; Singh, N.; Jindal, B. Optimization of parameters for improving the performance of EEG-based BCI system. J. Reliab. Intell. Environ. 2020, 1–12. [Google Scholar] [CrossRef]
- Abbasi, H.; Bennet, L.; Gunn, A.J.; Unsworth, C.P. Robust wavelet stabilized ‘footprints of Uncertainty’ for fuzzy system classifiers to automatically detect sharp waves in the EEG after hypoxia ischemia. Int. J. Neural Syst. 2017, 27, 1650051. [Google Scholar] [CrossRef]
- Plerou, A.; Vlamou, E.; Papadopoulos, V. EEG Signal Pattern Recognition Analysis: Fuzzy Logic Systems Ascendancy. Adv. Fuzzy Sets Syst. 2016, 21, 107. [Google Scholar] [CrossRef]
- Krishnamurthi, R.; Goyal, M. Hybrid Neuro-fuzzy Method for Data Analysis of Brain Activity Using EEG Signals. In Soft Computing and Signal Processing; Springer: Berlin/Heidelberg, Germany, 2019; pp. 165–173. [Google Scholar]
- Jiang, Y.; Gu, X.; Ji, D.; Qian, P.; Xue, J.; Zhang, Y.; Zhu, J.; Xia, K.; Wang, S. Smart Diagnosis: A Multiple-Source Transfer TSK Fuzzy System for EEG Seizure Identification. ACM Trans. Multimed. Comput. Commun. Appl. (TOMM) 2020, 16, 1–21. [Google Scholar] [CrossRef]
- Zadeh, L.A. Is there a need for fuzzy logic? Inf. Sci. 2008, 178, 2751–2779. [Google Scholar] [CrossRef]
- Osowski, S.; Cichocki, A.; Siwek, K. MATLAB w Zastosowaniu do Obliczeń Obwodowych i Przetwarzania Sygnałów; Oficyna Wydawnicza Politechniki Warszawskiej: Warszawa, Poland, 2006. [Google Scholar]
- Kawala-Janik, A.; Bauer, W.; Żołubak, M.; Baranowski, J. Early-stage pilot study on using fractional-order calculus-based filtering for the purpose of analysis of electroencephalography signals. Stud. Log. Gramm. Rhetor. 2016, 47, 103–111. [Google Scholar] [CrossRef] [Green Version]
- Kawala-Janik, A.; Bauer, W.; Al-Bakri, A.; Haddix, C.; Yuvaraj, R.; Cichon, K.; Podraza, W. Implementation of Low-Pass Fractional Filtering for the Purpose of Analysis of Electroencephalographic Signals. In Proceedings of the Non-Integer Order Calculus and its Applications: 9th International Conference on Non-Integer Order Calculus and Its Applications, Łódź, Poland, 11 October 2018; Springer: Cham, Switzerland, 2017; Volume 496, p. 63. [Google Scholar]
- Bauer, W.; Kawala-Janik, A. Implementation of bi-fractional filtering on the arduino uno hardware platform. In Theory and Applications of Non-Integer Order Systems; Springer: Berlin/Heidelberg, Germany, 2017; pp. 419–428. [Google Scholar]
- Baranowski, J.; Bauer, W.; Zagórowska, M.; Piątek, P. On digital realizations of non-integer order filters. Circuits Syst. Signal Process. 2016, 35, 2083–2107. [Google Scholar] [CrossRef] [Green Version]
- Popović, N.B.; Miljković, N.; Šekara, T.B. Electrogastrogram and electrocardiogram interference: Application of fractional order calculus and Savitzky-Golay filter for biosignals segregation. In Proceedings of the 2020 19th International Symposium INFOTEH-JAHORINA (INFOTEH), East Sarajevo, Bosnia and Herzegovina, 18–20 March 2020; pp. 1–5. [Google Scholar]
- Baranowski, J.; Piątek, P.; Kawala-Janik, A.; Zagórowska, M.; Bauer, W.; Dziwiński, T. Non-integer order filtration of electromyographic signals. In Advances in Modelling and Control of Non-Integer-Order Systems; Springer: Berlin/Heidelberg, Germany, 2015; pp. 231–237. [Google Scholar]
- Awal, M.A.; Mostafa, S.S.; Ahmad, M. Performance analysis of Savitzky-Golay smoothing filter using ECG signal. Int. J. Comput. Inf. Technol. 2011, 1, 24. [Google Scholar]
- Trinh, P.T.; Brossier, R.; Métivier, L.; Virieux, J.; Wellington, P. Bessel smoothing filter for spectral-element mesh. Geophys. J. Int. 2017, 209, 1489–1512. [Google Scholar] [CrossRef]
- Luo, J.; Ying, K.; He, P.; Bai, J. Properties of Savitzky–Golay digital differentiators. Digit. Signal Process. 2005, 15, 122–136. [Google Scholar] [CrossRef]
- Savitzky, A.; Golay, M.J. Smoothing and differentiation of data by simplified least squares procedures. Anal. Chem. 1964, 36, 1627–1639. [Google Scholar] [CrossRef]
- Guiñón, J.L.; Ortega, E.; García-Antón, J.; Pérez-Herranz, V. Moving average and Savitzki-Golay smoothing filters using Mathcad. In Proceedings of the 2007 International Conference on Engineering Education – ICEE 2007, Coimbra, Portugal, 3–7 September 2007; pp. 84–91. [Google Scholar] [CrossRef]
- Grzechca, D.; Szczeponik, A. Comparison of Filtering Methods for Enhanced Reliability of a Train Axle Counter System. Sensors 2020, 20, 2754. [Google Scholar] [CrossRef]
- Choi, G.H.; Moon, H.M.; Pan, S.B. Biometrics system technology trends based on biosignal. J. Digit. Converg. 2017, 15, 381–391. [Google Scholar] [CrossRef] [Green Version]
- Tsoi, A.C.; So, D.; Sergejew, A. Classification of electroencephalogram using artificial neural networks. Adv. Neural Inf. Process. Syst. 1994, 6, 1151–1158. [Google Scholar]
- Ko, W.; Jeon, E.; Jeong, S.; Suk, H.I. Multi-Scale Neural network for EEG Representation Learning in BCI. arXiv 2020, arXiv:2003.02657. [Google Scholar]
- Joseph, A.F.A.; Govindaraju, C. Minimizing electrodes for effective brain computer interface. Biomed. Signal Process. Control 2021, 63, 102201. [Google Scholar] [CrossRef]
- Szczęsna, A.; Błaszczyszyn, M.; Kawala, A. Convolutional neural network in upper limb functional motion analysis after stroke. PeerJ 2020. [Google Scholar] [CrossRef]
- Garcia-Moreno, F.M.; Bermudez-Edo, M.; Rodríguez-Fórtiz, M.J.; Garrido, J.L. A CNN-LSTM Deep Learning Classifier for Motor Imagery EEG Detection Using a Low-invasive and Low-Cost BCI Headband. In Proceedings of the 2020 16th International Conference on Intelligent Environments (IE), Madrid, Spain, 20–23 July 2020; pp. 84–91. [Google Scholar]
- Sussillo, D.; Nuyujukian, P.; Fan, J.M.; Kao, J.C.; Stavisky, S.D.; Ryu, S.; Shenoy, K. A recurrent neural network for closed-loop intracortical brain–machine interface decoders. J. Neural Eng. 2012, 9, 026027. [Google Scholar] [CrossRef]
- Sussillo, D.; Stavisky, S.D.; Kao, J.C.; Ryu, S.I.; Shenoy, K.V. Making brain–machine interfaces robust to future neural variability. Nat. Commun. 2016, 7, 13749. [Google Scholar] [CrossRef]
- Skomrock, N.D.; Schwemmer, M.A.; Ting, J.E.; Trivedi, H.R.; Sharma, G.; Bockbrader, M.A.; Friedenberg, D.A. A Characterization of Brain-Computer Interface Performance Trade-Offs Using Support Vector Machines and Deep Neural Networks to Decode Movement Intent. Front. Neurosci. 2018, 12, 763. [Google Scholar] [CrossRef] [Green Version]
- Chaudhary, U.; Birbaumer, N.; Ramos-Murguialday, A. Brain–computer interfaces for communication and rehabilitation. Nat. Rev. Neurol. 2016, 12, 513. [Google Scholar] [CrossRef] [Green Version]
- Sebastián-Romagosa, M.; Cho, W.; Ortner, R.; Murovec, N.; Von Oertzen, T.; Kamada, K.; Allison, B.Z.; Guger, C. Brain Computer Interface Treatment for Motor Rehabilitation of Upper Extremity of Stroke Patients—A Feasibility Study. Front. Neurosci. 2020, 14, 591435. [Google Scholar] [CrossRef]
- Mak, J.N.; Wolpaw, J.R. Clinical applications of brain-computer interfaces: Current state and future prospects. IEEE Rev. Biomed. Eng. 2009, 2, 187–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mowla, M.R.; Cano, R.I.; Dhuyvetter, K.J.; Thompson, D.E. Affective Brain-Computer Interfaces: Choosing a Meaningful Performance Measuring Metric. Comput. Biol. Med. 2020, 126, 104001. [Google Scholar] [CrossRef] [PubMed]
- Sawangjai, P.; Hompoonsup, S.; Leelaarporn, P.; Kongwudhikunakorn, S.; Wilaiprasitporn, T. Consumer grade eeg measuring sensors as research tools: A review. IEEE Sens. J. 2019, 20, 3996–4024. [Google Scholar] [CrossRef]
- Wierzgała, P.; Zapała, D.; Wojcik, G.M.; Masiak, J. Most popular signal processing methods in motor-imagery BCI: A review and meta-analysis. Front. Neuroinform. 2018, 12, 78. [Google Scholar] [CrossRef] [Green Version]
- Grübler, G.; Al-Khodairy, A.; Leeb, R.; Pisotta, I.; Riccio, A.; Rohm, M.; Hildt, E. Psychosocial and ethical aspects in non-invasive EEG-based BCI research—a survey among BCI users and BCI professionals. Neuroethics 2014, 7, 29–41. [Google Scholar] [CrossRef]
- Schermer, M. The mind and the machine. On the conceptual and moral implications of brain-machine interaction. Nanoethics 2009, 3, 217. [Google Scholar] [CrossRef] [Green Version]
- Thinnes-Elker, F.; Iljina, O.; Apostolides, J.K.; Kraemer, F.; Schulze-Bonhage, A.; Aertsen, A.; Ball, T. Intention concepts and brain-machine interfacing. Front. Psychol. 2012, 3, 455. [Google Scholar] [CrossRef] [Green Version]

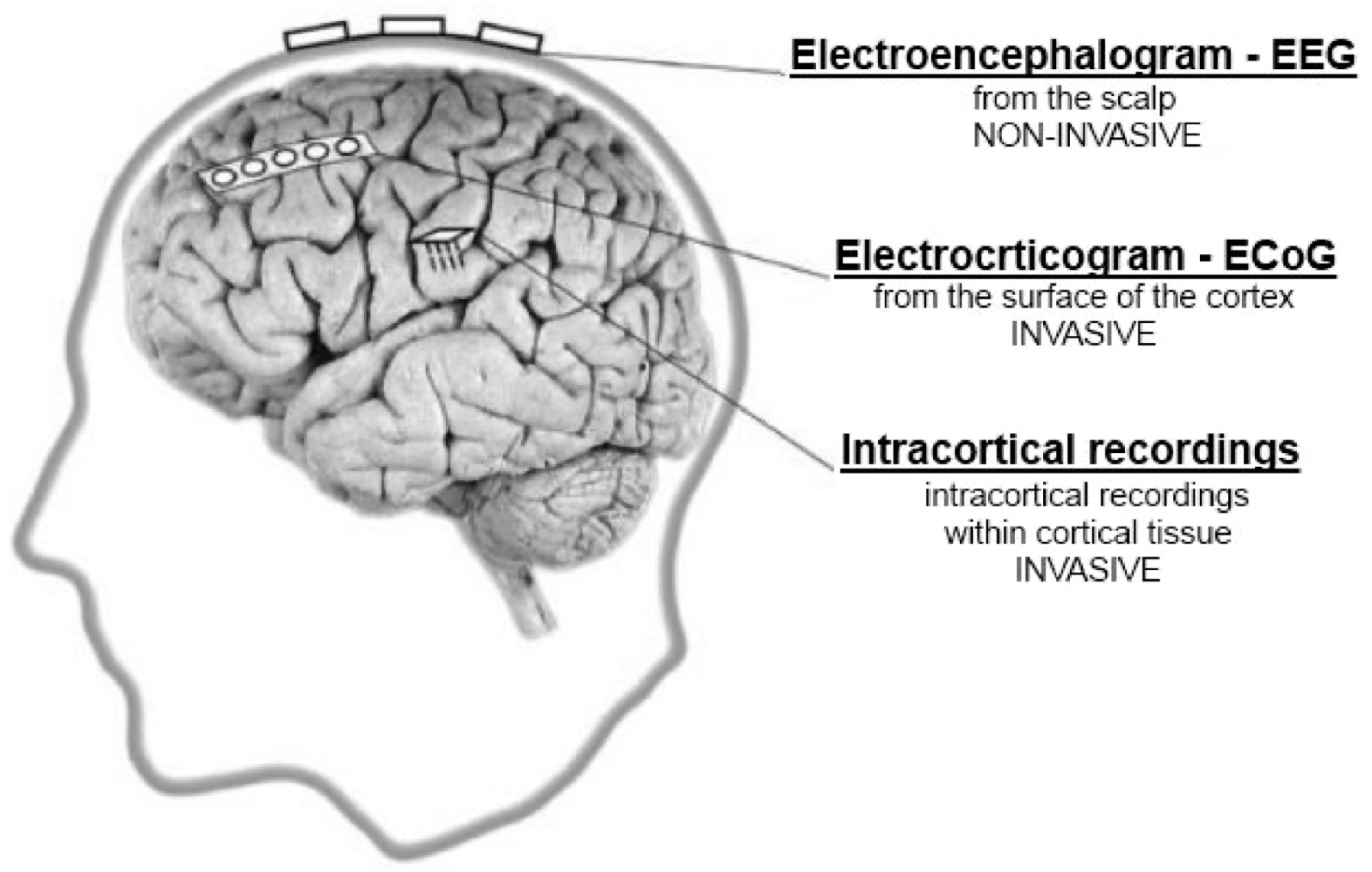

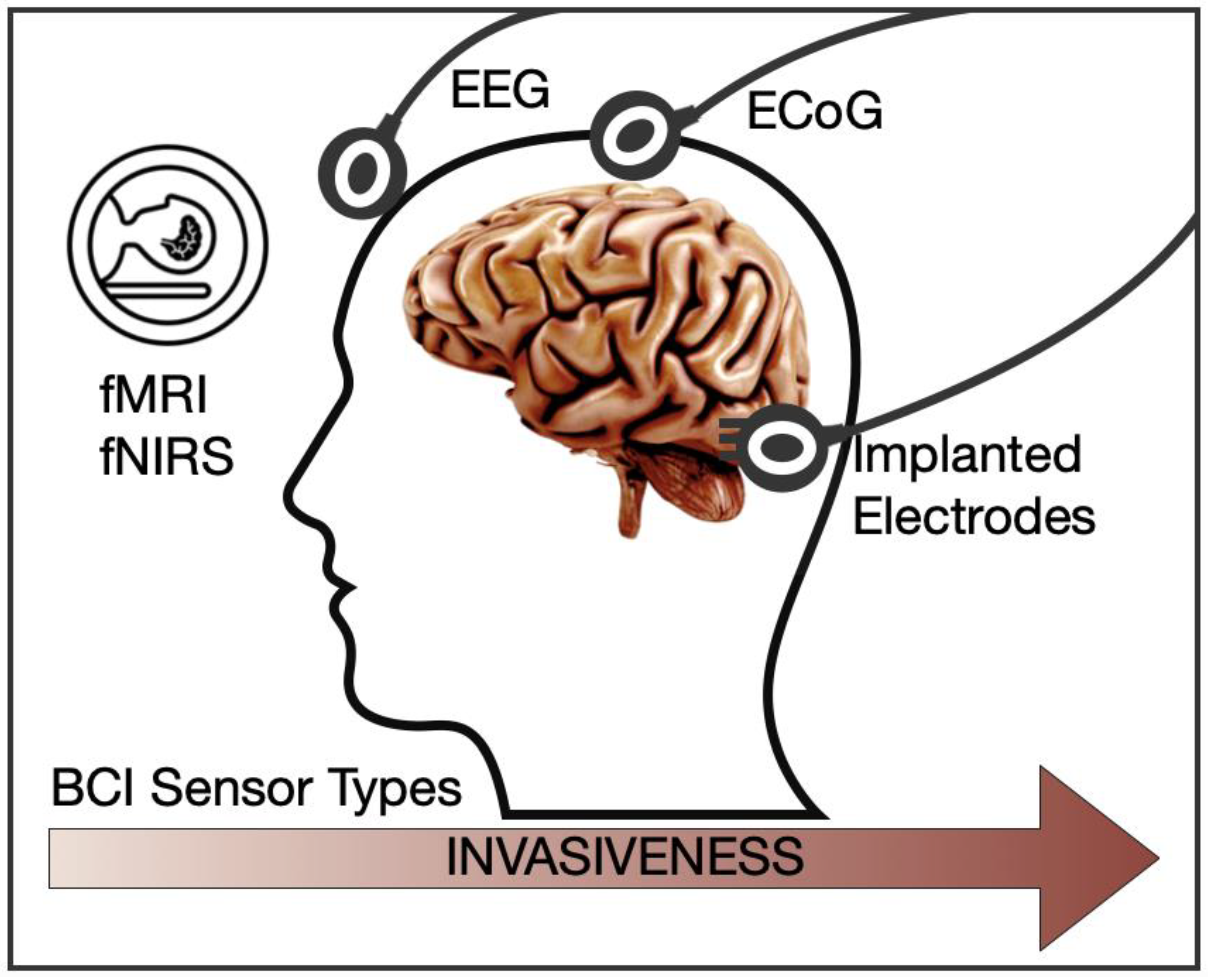




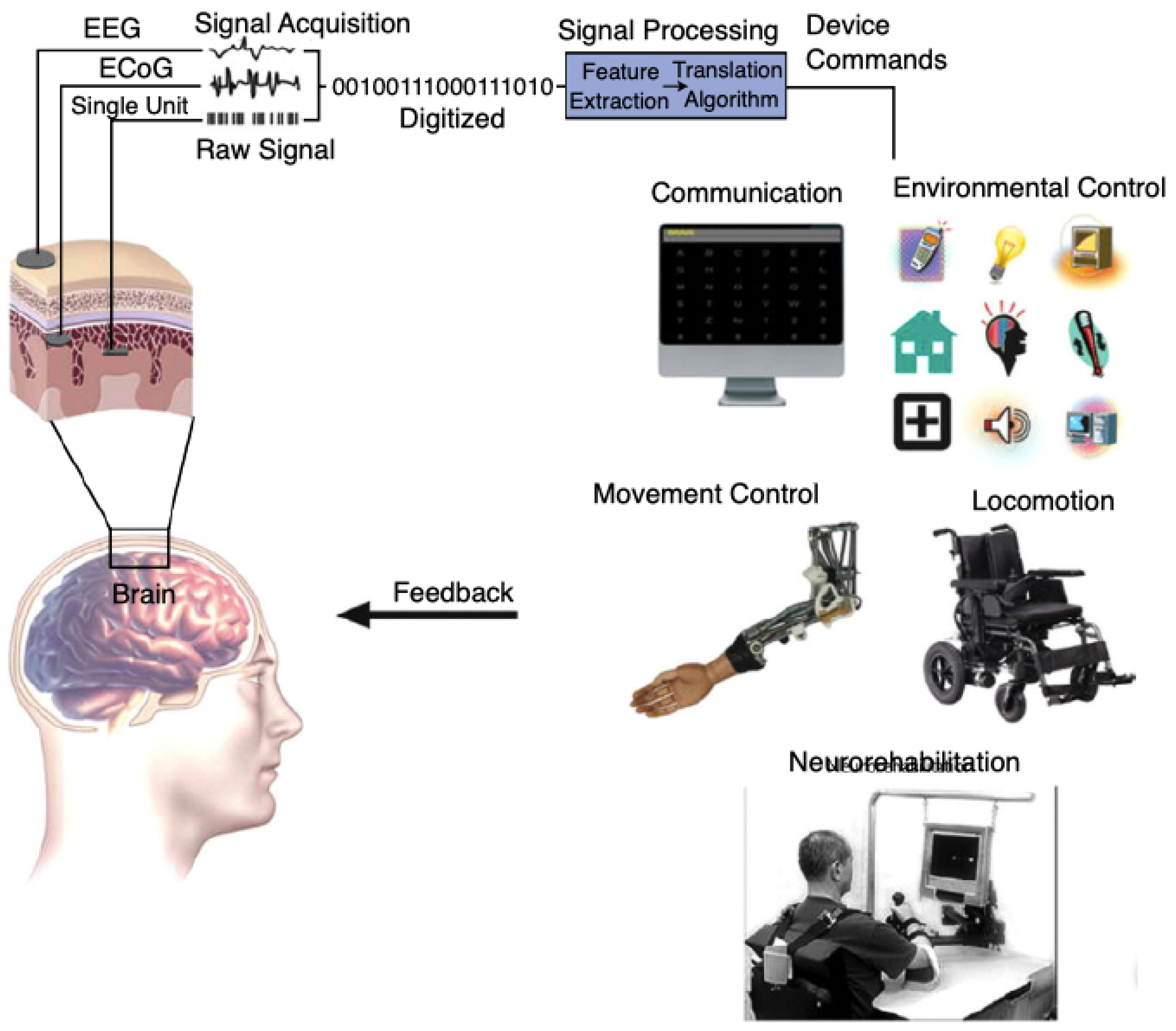{kind=link}
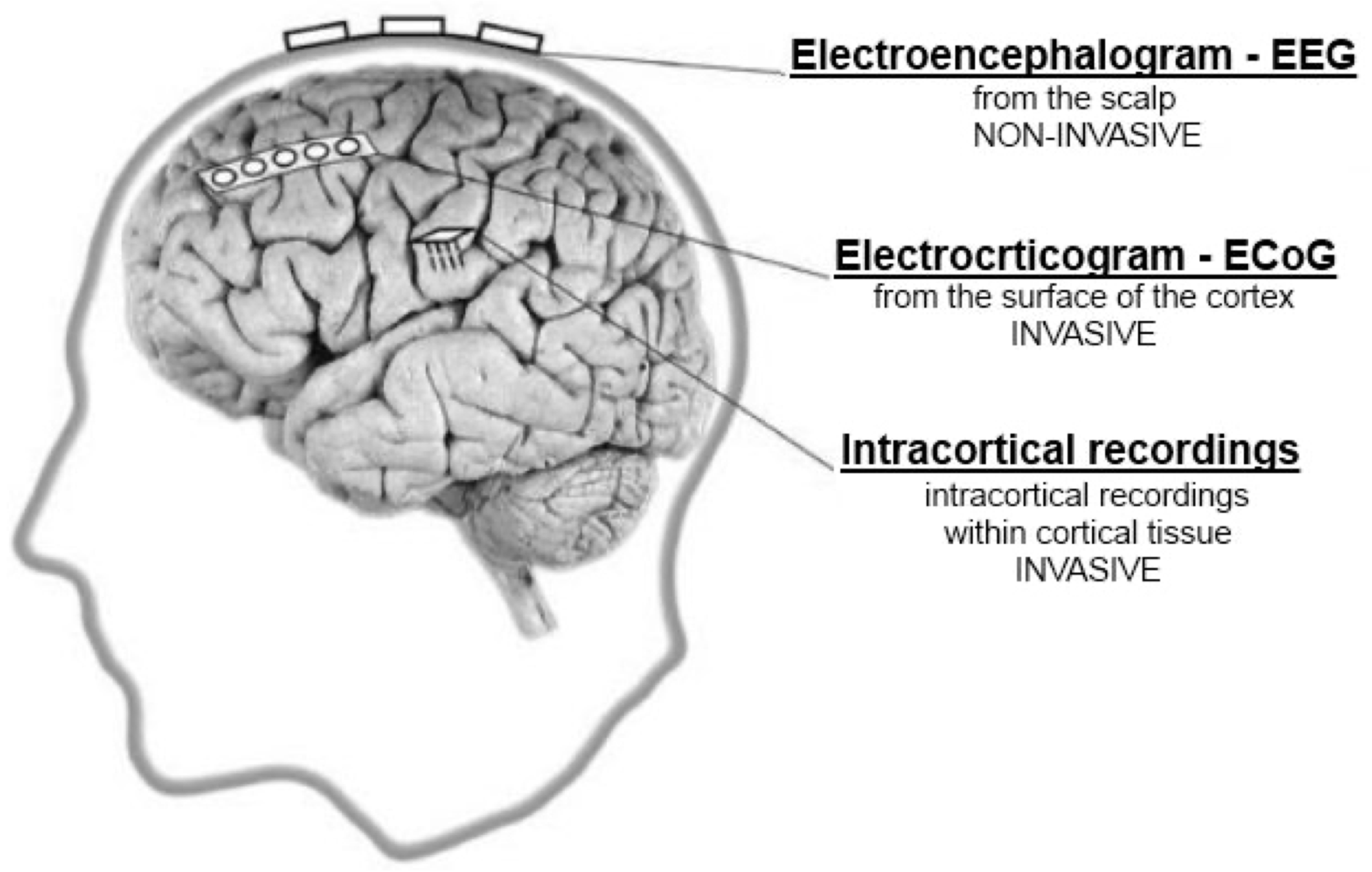{kind=link}
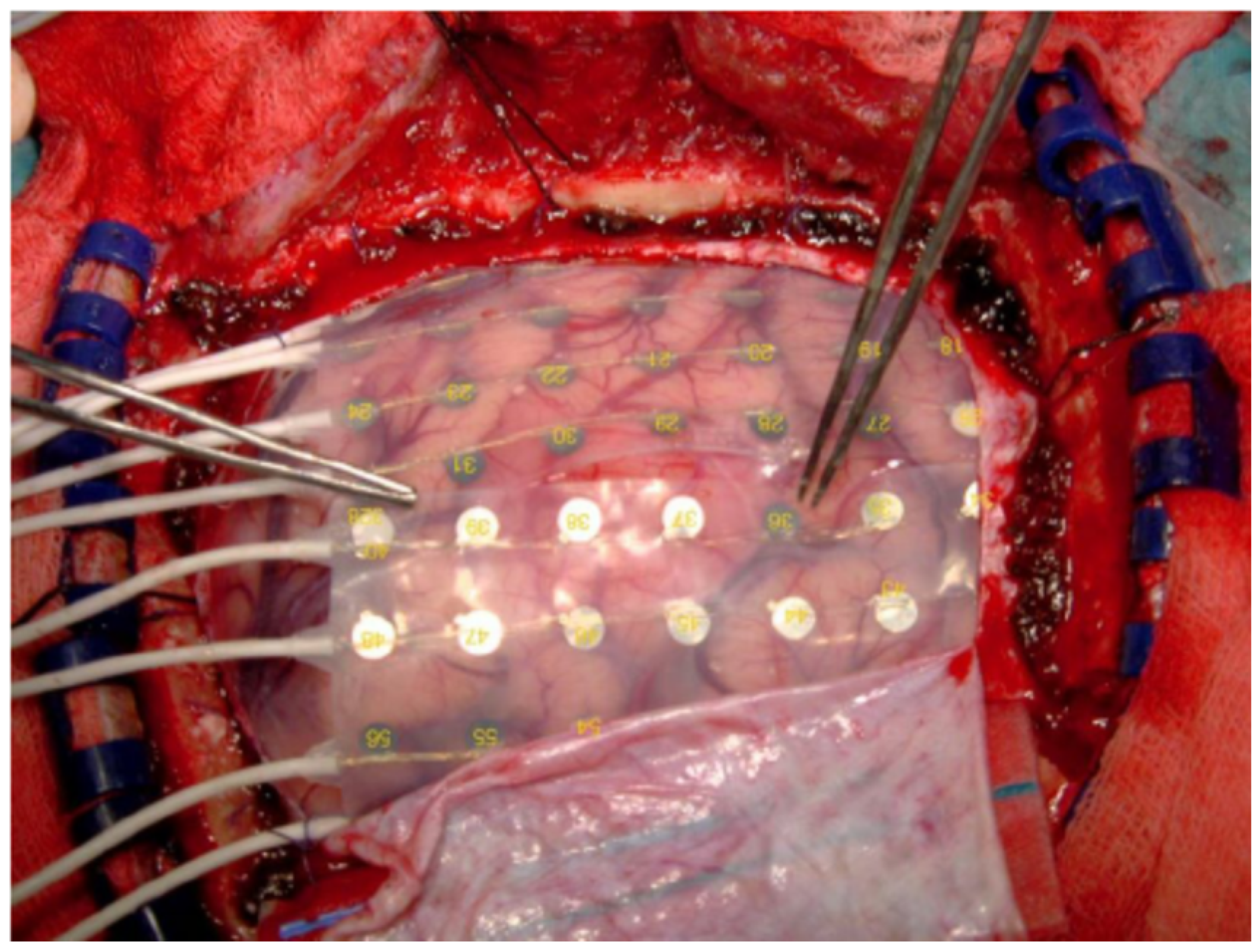{kind=link}
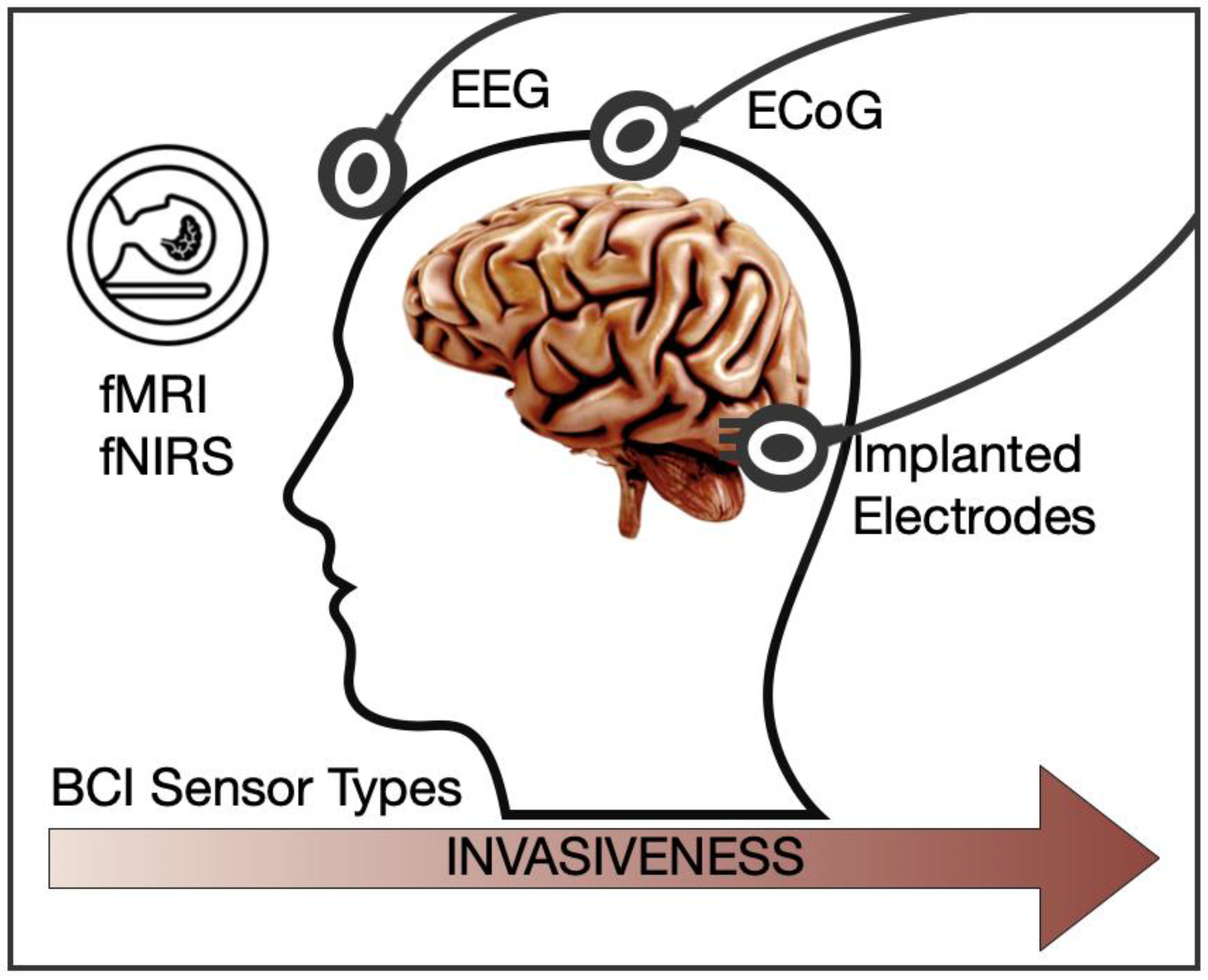{kind=link}
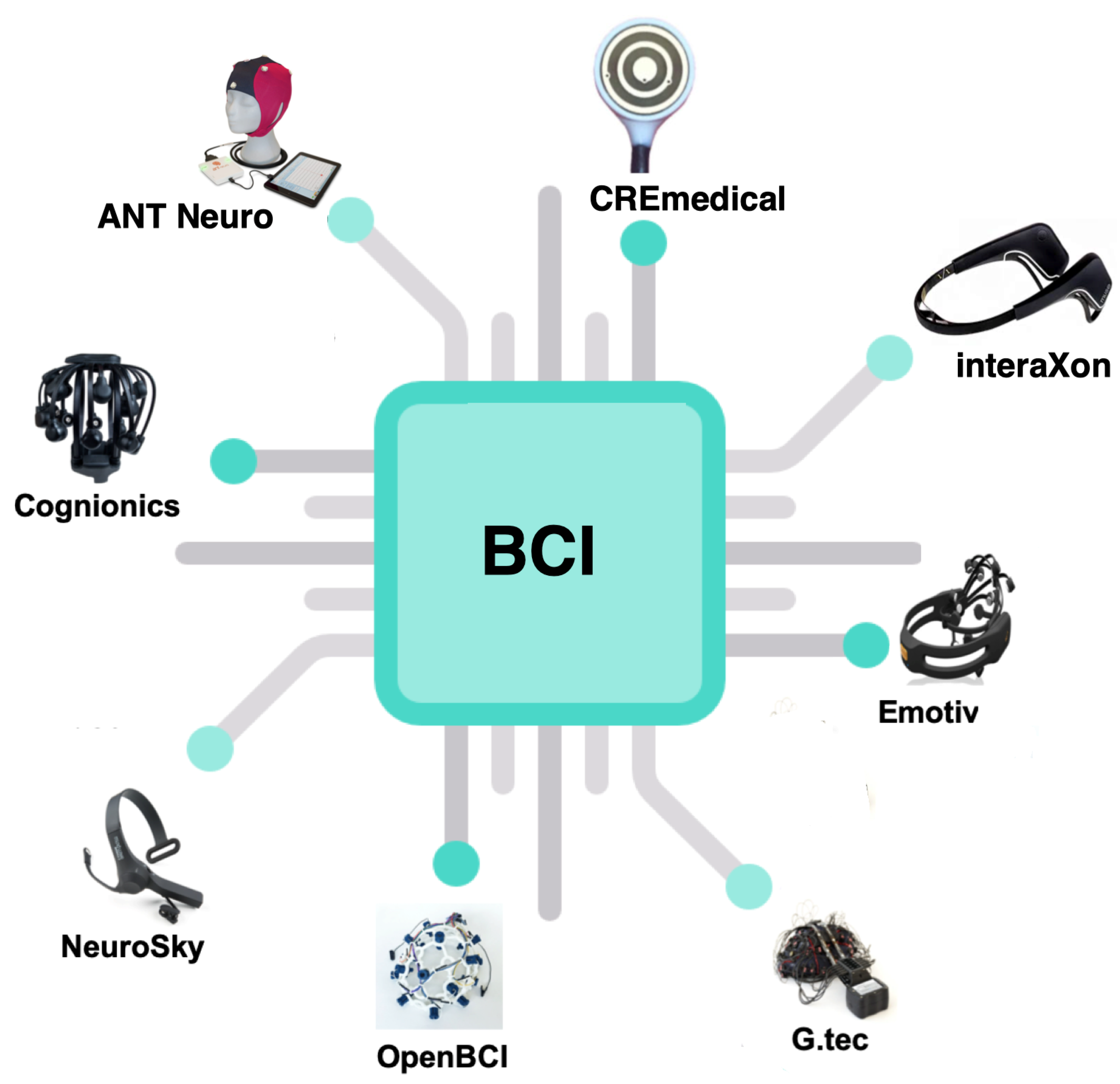{kind=link}
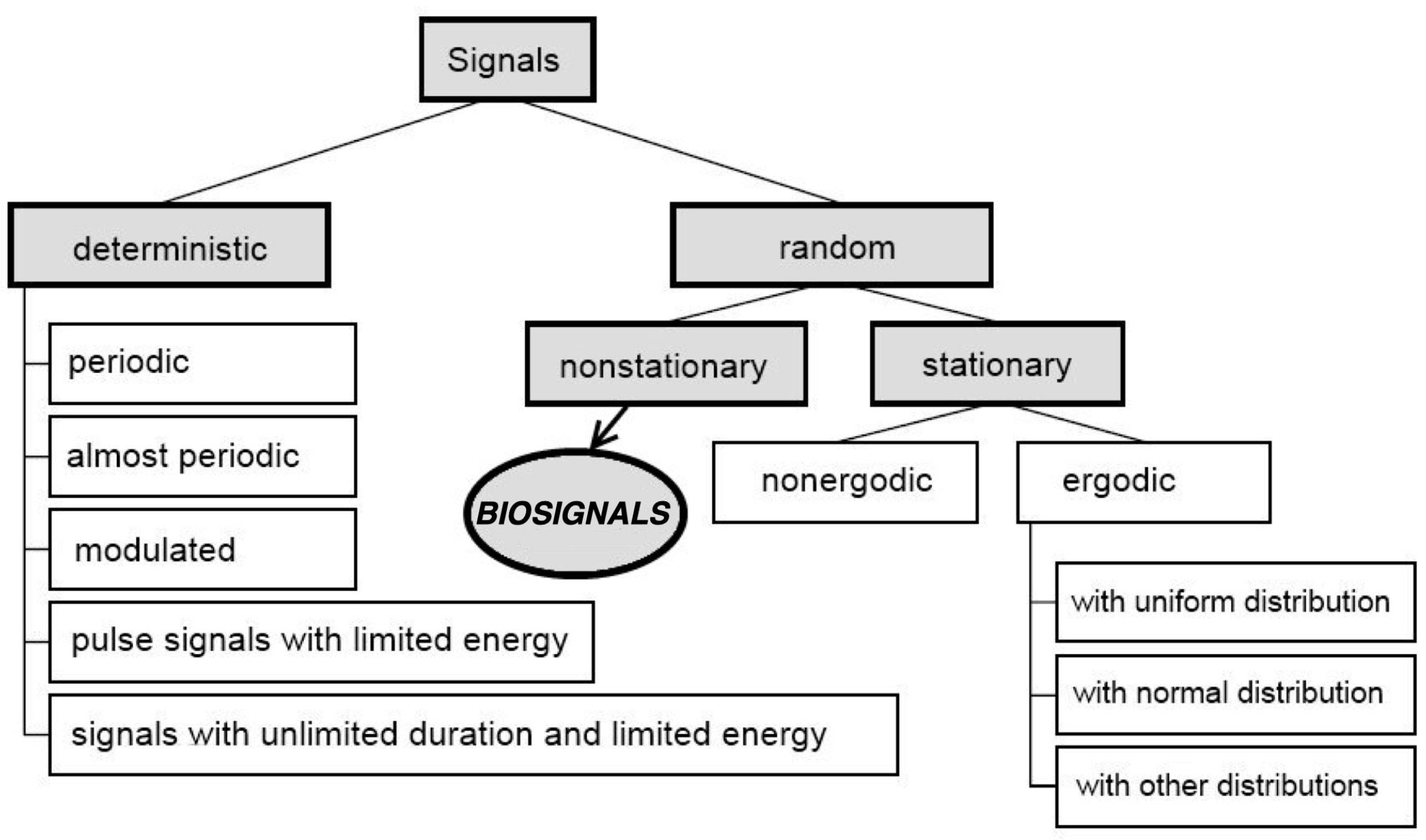{kind=link}
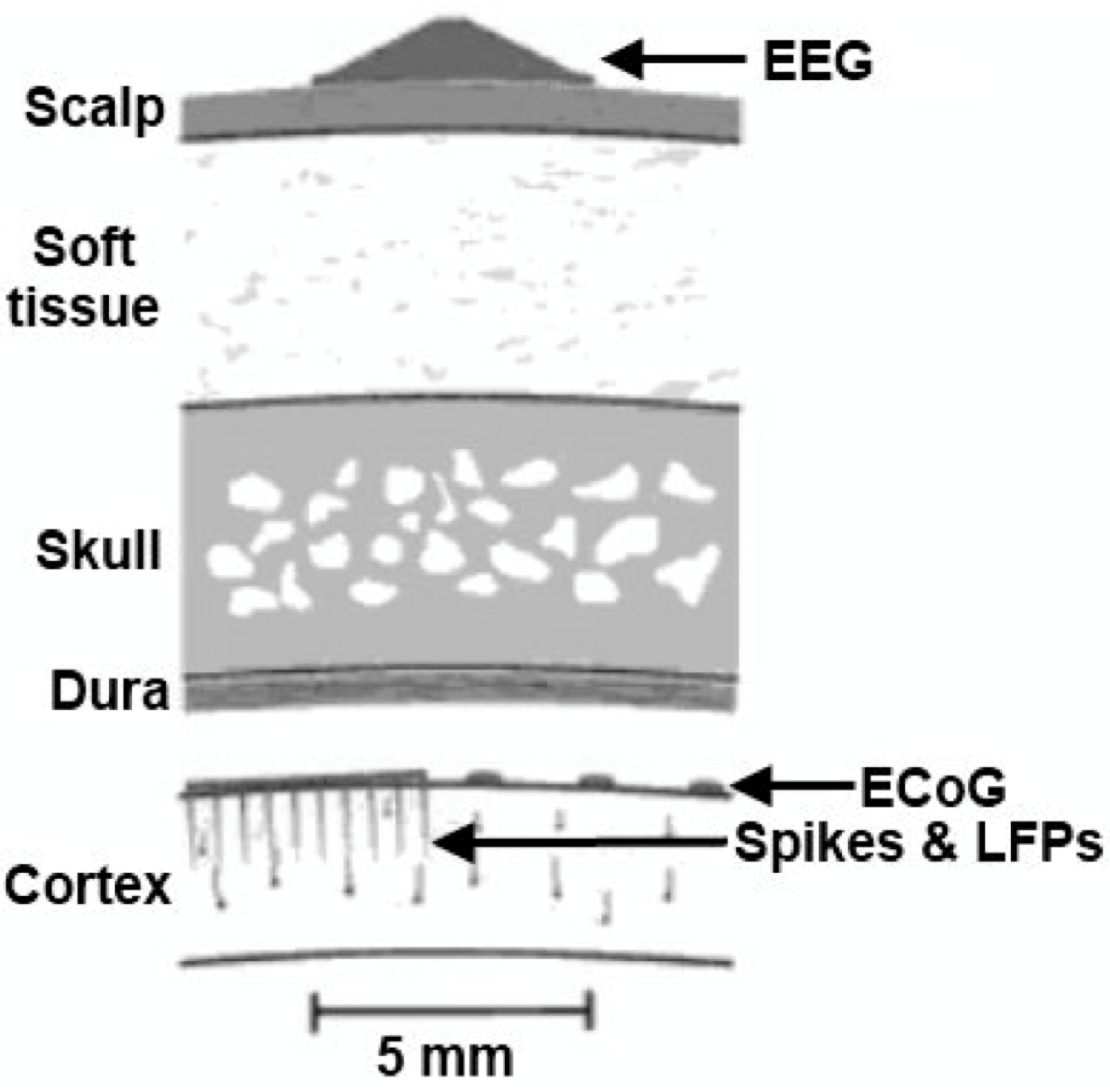{kind=link}
| Brainwave | Frequency Range | Mental Condition |
|---|---|---|
| Delta | 0–4 Hz | State of deep sleep, when there is no focus, the person is totally absent, unconscious. |
| Theta | 4–8 Hz | Deep relaxation, internal focus, meditation, intuition access to unconscious material such as imaging, fantasy, dreaming. |
| Low Alpha | 8–10 Hz | Wakeful relaxation, consciousness, awareness without attention or concentration, good mood, calmness. |
| High Alpha | 10–12 Hz | Increased self-awareness and focus, learning of new information. |
| Low Beta | 12–18 Hz | Active thinking, active attention, focus towards problem solving, judgment and decision making. |
| High Beta | 18–30 Hz | Engagement in mental activity, also alertness and agitation. |
| Low Gamma | 30–50 Hz | Cognitive processing, senses, intelligence, compassion, self-control. |
| High Gamma | 50–70 Hz | Cognitive tasks: memory, hearing, reading and speaking. |
| Sensor | Type | Spatial Resolution | Temporal Resolution | Portability |
|---|---|---|---|---|
| micro-electrode | YES | 0.05–0.50 mm | 3 ms | moderate |
| ECoG | YES | mm | 5 ms | good |
| intravascular electrode | YES | mm | 5 ms | good |
| EEG | NO | mm | 50 ms | good |
| fMRI | NO | >1 mm | 1 s | poor |
| fNIRS | NO | 1 cm | 1 s | good |
| MEG | NO | >1 mm | 1–5 ms | poor |
| PET | NO | 3–51 mm | 50–100 s | poor |
| Manufacturer | Wearable | Sensors Type | Channels Amount | Sampling Rate | Data Transfer |
|---|---|---|---|---|---|
| Neurosky | YES | Dry | 1 | 500 Hz | Bluetooth |
| Emotiv | YES | Wet/Dry | 5–32 | 500 Hz | Bluetooth |
| OpenBCI | YES | Wet/Dry | 8–21 | 250–500 Hz | Bluetooth |
| ANT Neuro | YES | Dry | 32–256 | <16 kHz | Wi-Fi |
| g.tec | YES | Wet/Dry | 8–256 | 500 Hz | Cable/Wi-Fi |
| Cognionics | YES | Dry | 8–128 | >2 kHz | Bluetooth |
| CREmedical | YES | Wet | 20 | 500 Hz | Cable |
| interaXon | YES | Wet | 4–7 | 250 Hz | Bluetooth |
| Cognionics | YES | Wet | 8–128 | <2 kHz | Bluetooth |
| Application | Description | Source Data | Analysis Method |
|---|---|---|---|
| spelling applications | One of the most basic applications of BCIs for people with disabilities used for communication purposes, where users using their brain activity choose appropriate letter [192,193,194,195]. | EEG, EOG | P300 evoked potentials |
| neurogaming and VR/AR | Controlling video games, virtual and/or augmented reality applications using BCIs. It is one of the most popular current trends in the field [196,197,198,199,200]. | EEG, EOG, EMG, heart-rate, motion control, facial expression | mVEPs, AI, DNN |
| neuromarketing | Neuromarketing methods, including EEG analysis, provide a better understanding of brain mechanisms and consumer behavior to improve marketing strategies [201,202,203,204,205]. | EEG, EOG, facial expression, heart-rate | AI, DNN, various pattern recognition-methods |
| smart wheelchairs | One of the most needed BCI applications is the ability to control a wheelchair. Such devices are destined for people with cognitive/motor/sensory impairments [206,207,208,209,210,211]. | EEG, EOG, heart-rate, facial expressions | DL, P300, SSVEP, EMD |
| emotional condition | Recognition of human emotions and/or mental states using biomedical data analysis—part of passive BCIs. Most of them are based on facial expression recognition and analysis of speech signals. It is one of the future development paths of BCIs [150,212,213,214,215,216]. | EEG, heart-rate, EOG, EMG, facial expression, speech | DWT, AI, DNN, various pattern recognition methods (e.g., KNN, LDA), SSVEPs, Fuzzy Systems |
| robotics | Improvement of multidimensional control systems with the use of BCIs [130,217,218,219]. | EEG, EMG, EOG | AI, DNN, CNN |
| ’smart’ appliances | Controlling of various domestic appliances using BCIs, such as among the others window shutters, lighting, ambiance music, TV set screens, etc. or for connecting reality with AR solution [200,220,221,222,223,224]. | EEG, EOG, heart-rate, speech | SSVEPs, P300, Fuzzy Systems, AI |
| rehabilitation | Good solution for patients with little or none functional recovery of upper limb motor function. It has strong therapeutic potential for inter alia stroke patients [18,82,83,134,135,136,137,140,142,225]. | EEG, EOG, ECoG, fMRI, fNIRS, speech | SSVEPs, P300, EP, Fuzzy Systems, AI |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kawala-Sterniuk, A.; Browarska, N.; Al-Bakri, A.; Pelc, M.; Zygarlicki, J.; Sidikova, M.; Martinek, R.; Gorzelanczyk, E.J. Summary of over Fifty Years with Brain-Computer Interfaces—A Review. Brain Sci. 2021, 11, 43. https://doi.org/10.3390/brainsci11010043
Kawala-Sterniuk A, Browarska N, Al-Bakri A, Pelc M, Zygarlicki J, Sidikova M, Martinek R, Gorzelanczyk EJ. Summary of over Fifty Years with Brain-Computer Interfaces—A Review. Brain Sciences. 2021; 11(1):43. https://doi.org/10.3390/brainsci11010043
Chicago/Turabian StyleKawala-Sterniuk, Aleksandra, Natalia Browarska, Amir Al-Bakri, Mariusz Pelc, Jaroslaw Zygarlicki, Michaela Sidikova, Radek Martinek, and Edward Jacek Gorzelanczyk. 2021. "Summary of over Fifty Years with Brain-Computer Interfaces—A Review" Brain Sciences 11, no. 1: 43. https://doi.org/10.3390/brainsci11010043
APA StyleKawala-Sterniuk, A., Browarska, N., Al-Bakri, A., Pelc, M., Zygarlicki, J., Sidikova, M., Martinek, R., & Gorzelanczyk, E. J. (2021). Summary of over Fifty Years with Brain-Computer Interfaces—A Review. Brain Sciences, 11(1), 43. https://doi.org/10.3390/brainsci11010043