Slump in Hospital Admissions for Stroke, a Fact of an Uncertain Nature That Requires Explanation

 ,
, 
 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Health System and Stroke Organization
2.2. Planning for Pandemic of Coronavirus Disease 2019 (COVID-19)
2.3. Quality Indicators for Stroke Care and Data Collection
2.4. Ethical Considerations
2.5. Statistical Analysis
3. Results
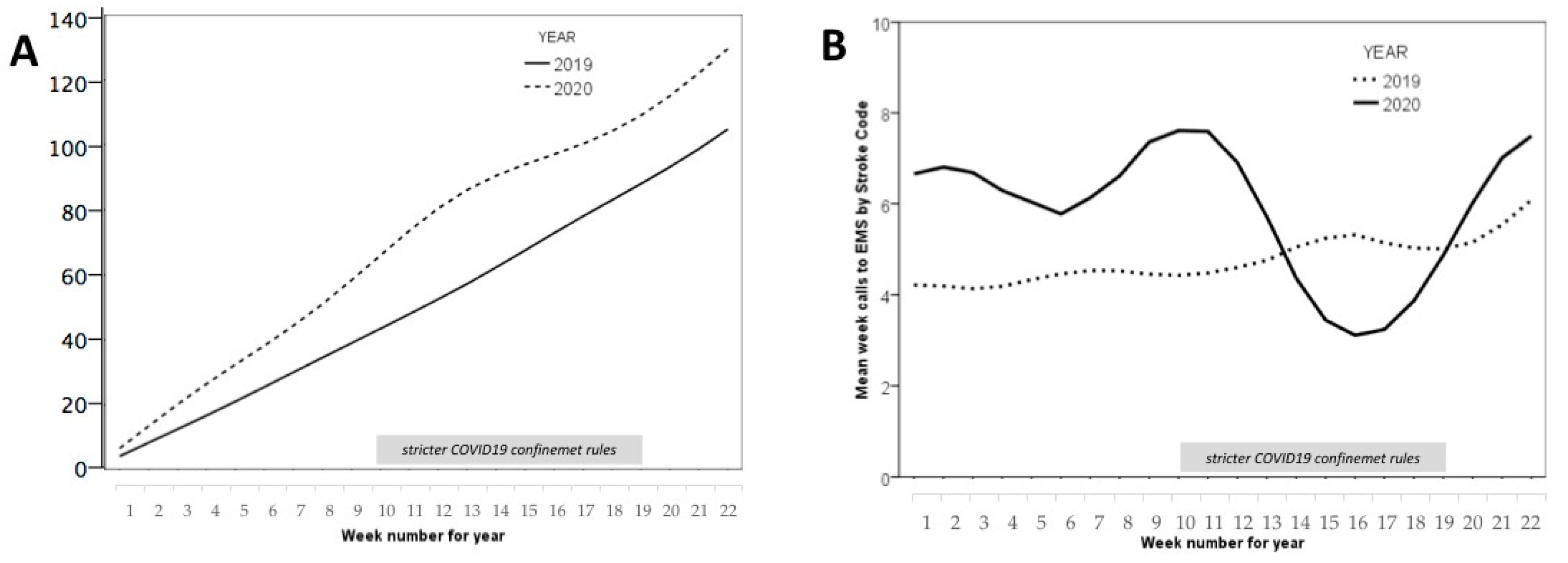
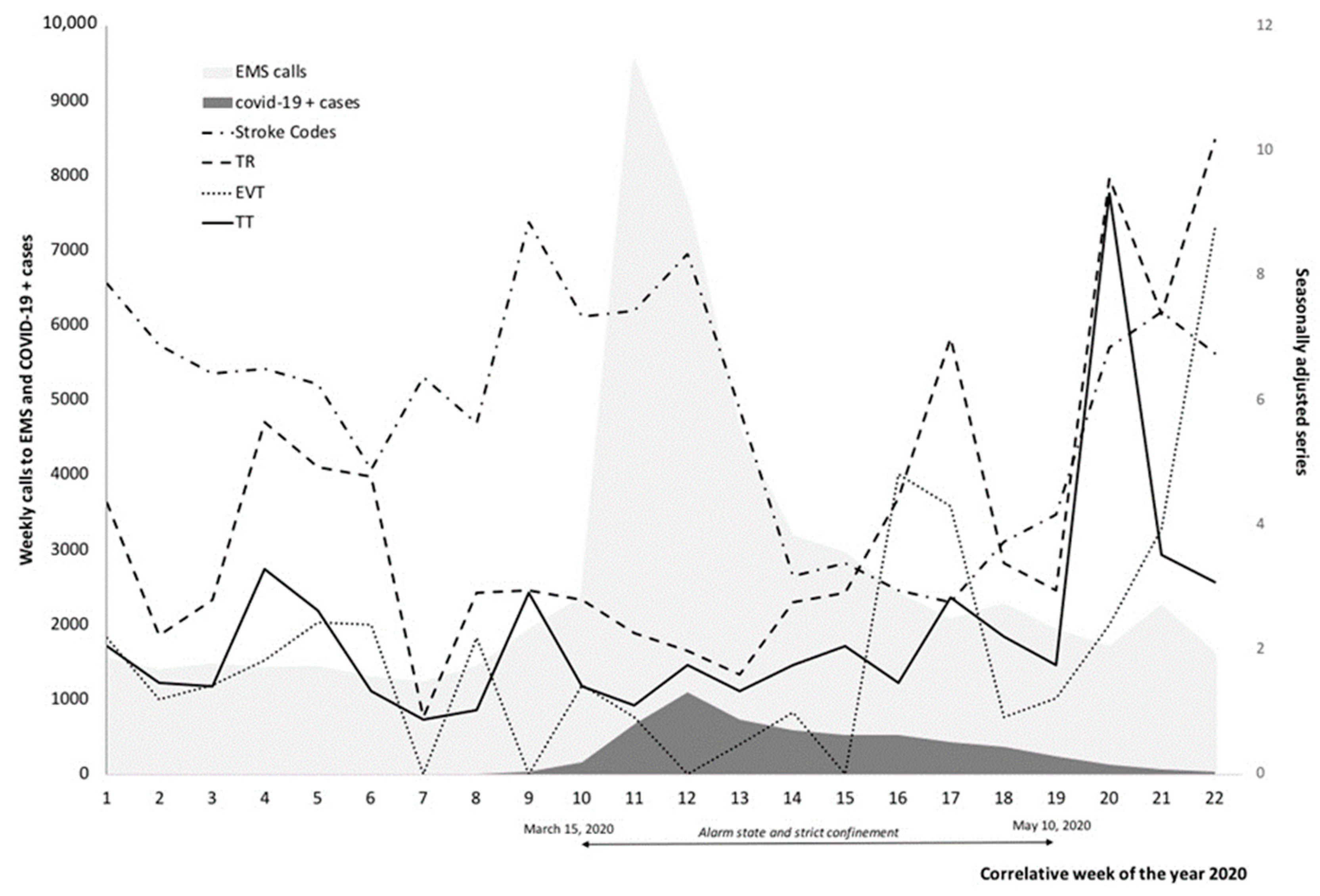
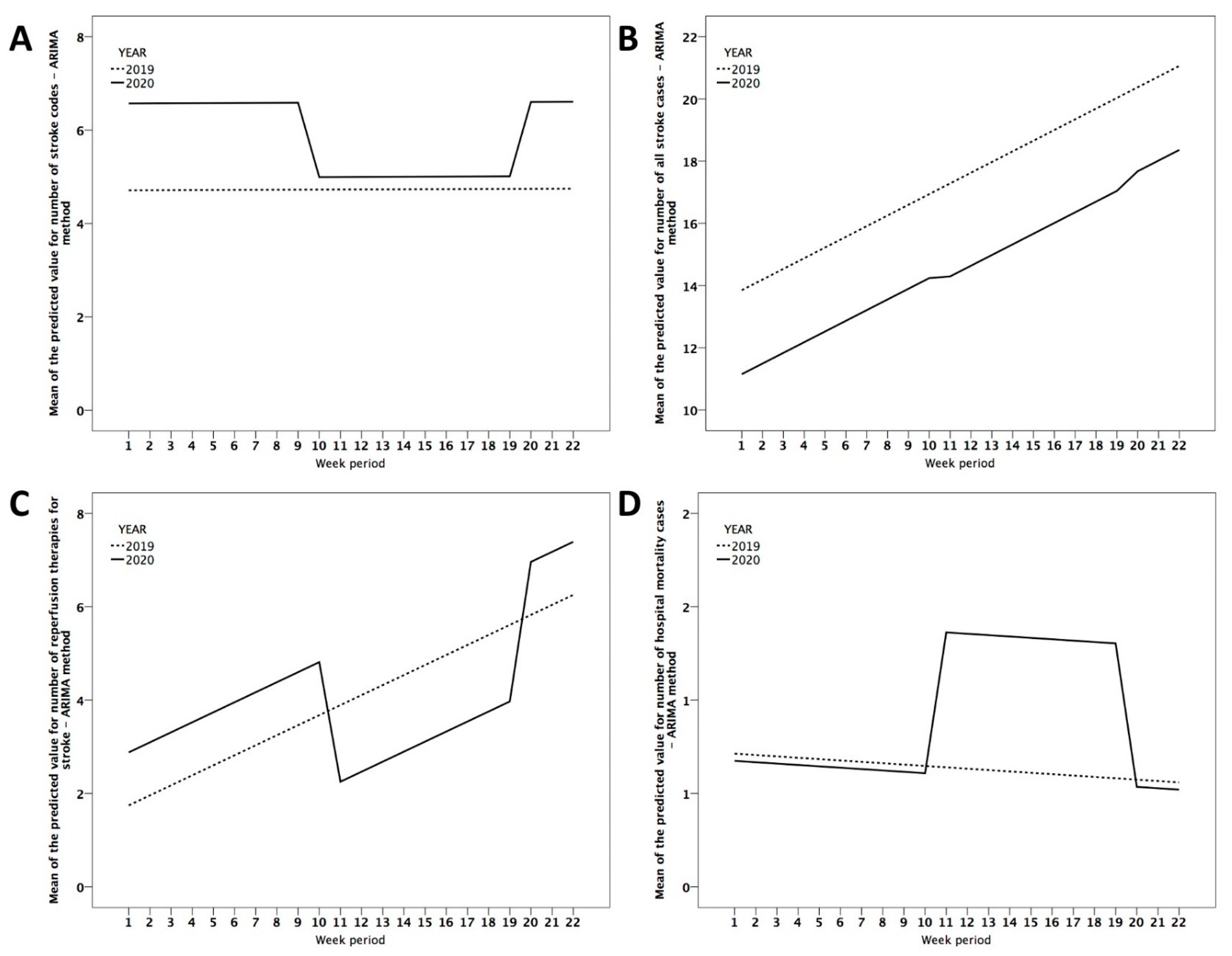
3.1. Stroke Code Activations
3.2. Stroke Admission to Stroke Units
3.3. Stroke Severity
3.4. Reperfusion Therapies
3.5. Use of a Telestroke Service
3.6. Stroke Prognosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus–Infected Pneumonia. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- De Oliveira Andrade, R. Covid-19 Is Causing the Collapse of Brazil’s National Health Service. BMJ 2020. [Google Scholar] [CrossRef] [PubMed]
- Jyotsana, N.; King, M.R. The Impact of COVID-19 on Cancer Risk and Treatment. Cell. Mol. Bioeng. 2020. [Google Scholar] [CrossRef] [PubMed]
- Metzler, B.; Siostrzonek, P.; Binder, R.K.; Bauer, A.; Reinstadler, S.J. Decline of Acute Coronary Syndrome Admissions in Austria since the Outbreak of COVID-19: The Pandemic Response Causes Cardiac Collateral Damage. Eur. Heart J. 2020. [Google Scholar] [CrossRef] [PubMed]
- Meza, H.T.; Lambea Gil, Á.; Saldaña, A.S.; Martínez-Zabaleta, M.; de la Riva Juez, P.; Martínez, E.L.C.; Apilánez, M.C.; Isasi, M.H.; Enguita, J.M.; de Lera Alfonso, M.; et al. Impact of COVID-19 Outbreak on Ischemic Stroke Admissions and in-Hospital Mortality in North-West Spain. Int. J. Stroke 2020. [Google Scholar] [CrossRef]
- World Health Organization (WHO). WHO Director-General’s Opening Remarks at the Mission Briefing on COVID-19. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-mission-briefing-on-covid-19 (accessed on 1 March 2020).
- Rodríguez-Pardo, J.; Fuentes, B.; de Leciñana, M.A.; Campollo, J.; Castaño, P.C.; Ruiz, J.C.; Herrero, J.E.; Leal, R.G.; Gil Núñez, A.; Cerezo, J.F.G.; et al. Acute Stroke Care during the COVID-19 Pandemic. Ictus Madrid Program Recommendations. Neurologia 2020. [Google Scholar] [CrossRef]
- Spanish Government. Real Decreto 463/2020, de 14 de Marzo, por el que se Declara el Estado de Alarma para la Gestión de la Situación de Crisis Sanitaria Ocasionada por el COVID-19. Available online: https://boe.es/boe/dias/2020/03/11/pdfs/BOE-A-2020-3434.pdf (accessed on 15 March 2020).
- Kuderer, N.M.; Choueiri, T.K.; Shah, D.P.; Shyr, Y.; Rubinstein, S.M.; Rivera, D.R.; Shete, S.; Hsu, C.Y.; Desai, A.; de Lima Lopes, G.; et al. Clinical Impact of COVID-19 on Patients with Cancer (CCC19): A Cohort Study. Lancet 2020. [Google Scholar] [CrossRef]
- De Filippo, O.; D’Ascenzo, F.; Angelini, F.; Bocchino, P.P.; Conrotto, F.; Saglietto, A.; Secco, G.G.; Campo, G.; Gallone, G.; Verardi, R.; et al. Reduced Rate of Hospital Admissions for ACS during Covid-19 Outbreak in Northern Italy. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Zhao, J.; Li, H.; Kung, D.; Fisher, M.; Shen, Y.; Liu, R. Impact of the COVID-19 Epidemic on Stroke Care and Potential Solutions. Stroke 2020. [Google Scholar] [CrossRef]
- Sweid, A.; Hammoud, B.; Weinberg, J.H.; Oneissi, M.; Raz, E.; Shapiro, M.; DePrince, M.; Tjoumakaris, S.; Gooch, M.R.; Herial, N.A.; et al. Letter: Thrombotic Neurovascular Disease in Covid-19 Patients. Neurosurgery 2020. [Google Scholar] [CrossRef]
- Belani, P.; Schefflein, J.; Kihira, S.; Rigney, B.; Delman, B.N.; Mahmoudi, K.; Mocco, J.; Majidi, S.; Yeckley, J.; Aggarwal, A.; et al. COVID-19 Is an Independent Risk Factor for Acute Ischemic Stroke. Am. J. Neuroradiol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Morelli, N.; Rota, E.; Terracciano, C.; Immovilli, P.; Spallazzi, M.; Colombi, D.; Zaino, D.; Michieletti, E.; Guidetti, D. The Baffling Case of Ischemic Stroke Disappearance from the Casualty Department in the COVID-19 Era. Eur. Neurol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Kansagra, A.P.; Goyal, M.S.; Hamilton, S.; Albers, G.W. Collateral Effect of Covid-19 on Stroke Evaluation in the United States. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Montaner, J.; Barragán-Prieto, A.; Pérez-Sánchez, S.; Escudero-Martínez, I.; Moniche, F.; Sánchez-Miura, J.A.; Ruiz-Bayo, L.; González, A. Break in the Stroke Chain of Survival Due to COVID-19. Stroke 2020. [Google Scholar] [CrossRef]
- Rudilosso, S.; Laredo, C.; Vera, V.; Vargas, M.; Renú, A.; Llull, L.; Obach, V.; Amaro, S.; Urra, X.; Torres, F.; et al. Acute Stroke Care Is at Risk in the Era of COVID-19: Experience at a Comprehensive Stroke Center in Barcelona. Stroke 2020. [Google Scholar] [CrossRef]
- Teo, K.C.; Leung, W.C.Y.; Wong, Y.K.; Liu, R.K.C.; Chan, A.H.Y.; Choi, O.M.Y.; Kwok, W.M.; Leung, K.K.; Tse, M.Y.; Cheung, R.T.F.; et al. Delays in Stroke Onset to Hospital Arrival Time during COVID-19. Stroke 2020. [Google Scholar] [CrossRef]
- Hoyer, C.; Ebert, A.; Huttner, H.B.; Puetz, V.; Kallmünzer, B.; Barlinn, K.; Haverkamp, C.; Harloff, A.; Brich, J.; Platten, M.; et al. Acute Stroke in Times of the COVID-19 Pandemic: A Multicenter Study. Stroke 2020. [Google Scholar] [CrossRef]
- Sabatino, J.; de Rosa, S.; Di Salvo, G.; Indolfi, C. Impact of Cardiovascular Risk Profile on COVID-19 Outcome. A Meta-Analysis. PLoS ONE 2020. [Google Scholar] [CrossRef]
- Riggs, J.E. The Decline of Mortality Due to Stroke: A Competitive and Deterministic Perspective. Neurology 1991. [Google Scholar] [CrossRef]
- Rinkel, L.A.; Prick, J.C.M.; Slot, R.E.R.; Sombroek, N.M.A.; Burggraaff, J.; Groot, A.E.; Emmer, B.J.; Roos, Y.B.W.E.M.; Brouwer, M.C.; van den Berg-Vos, R.M.; et al. Impact of the COVID-19 Outbreak on Acute Stroke Care. J. Neurol. 2020. [Google Scholar] [CrossRef]
- Huang, J.F.; Greenway, M.R.F.; Nasr, D.M.; Chukwudelunzu, F.E.; Demaerschalk, B.M.; O’Carroll, C.B.; Nord, C.A.; Pahl, E.A.; Barrett, K.M.; Williams, L.N. Telestroke in the Time of COVID-19: The Mayo Clinic Experience. Mayo Clin. Proc. 2020. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.O.; Dharia, R.; Stazi, J.; DePrince, M.; Rosenwasser, R.H. Rapid Decline in Telestroke Consults in the Setting of COVID-19. Telemed. eHealth 2020. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Moreno, J.M.; Vega, P.M.; Espada, S.; Alberca, S.B.; Aguirre, J.; Peral, D. Association between Self-Perceived Psychological Stress and Transitory Ischaemic Attack and Minor Stroke: A Case-Control Study. Neurologia 2017. [Google Scholar] [CrossRef]
- Dimsdale, J.E. Psychological Stress and Cardiovascular Disease. J. Am. Coll. Cardiol. 2008. [Google Scholar] [CrossRef] [PubMed]
- Dhand, A.; Luke, D.; Lang, C.; Tsiaklides, M.; Feske, S.; Lee, J.M. Social Networks and Risk of Delayed Hospital Arrival after Acute Stroke. Nat. Commun. 2019. [Google Scholar] [CrossRef] [PubMed]
- Sacco, S.; Ricci, S.; Ornello, R.; Eusebi, P.; Petraglia, L.; Toni, D. Reduced Admissions for Cerebrovascular Events during COVID-19 Outbreak in Italy. Stroke 2020. [Google Scholar] [CrossRef]
- Siegler, J.E.; Zha, A.M.; Czap, A.L.; Ortega-Gutierrez, S.; Farooqui, M.; Liebeskind, D.S.; Desai, S.M.; Hassan, A.E.; Starosciak, A.K.; Linfante, I.; et al. Influence of the COVID-19 Pandemic on Treatment Times for Acute Ischemic Stroke: The Society of Vascular and Interventional Neurology Multicenter Collaboration. Stroke 2020. [Google Scholar] [CrossRef]
- Ramírez-Moreno, J.M.; Alonso-González, R.; Peral-Pacheco, D.; Millán-Núñez, M.V.; Aguirre-Sánchez, J.J. Stroke Awareness Is Worse among the Old and Poorly Educated: A Population-Based Survey. J. Stroke Cerebrovasc. Dis. 2015, 24. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Max | q75 | Median | q25 | Min | Mean | SD |
|---|---|---|---|---|---|---|---|
| Age (years old) | 77.7 | 72.9 | 71.1 | 68.6 | 64.8 | 70.9 | 2.9 |
| Stroke code activations | 9 | 6 | 5.1 | 4.2 | 3 | 5.5 | 1.5 |
| All stroke admissions | 28 | 18 | 16 | 13 | 8 | 16.1 | 4.0 |
| Ischemic stroke | 23 | 14 | 12 | 9.5 | 7 | 12.3 | 3.3 |
| Hemorrhagic stroke | 6 | 2 | 1 | 1 | 0 | 1.6 | 1.3 |
| Transient Ischemic Attack | 4 | 3 | 2 | 1 | 0 | 1.2 | 1.2 |
| Tele-stroke consultations | 6 | 3 | 2 | 1 | 0 | 2.3 | 1.7 |
| Stroke severity (NIHSS) | 11 | 8 | 7 | 5.3 | 2 | 6.8 | 1.8 |
| Thrombolytic therapy | 7 | 3 | 2 | 1 | 0 | 2.4 | 2.4 |
| Endovascular therapy | 5 | 2.5 | 1 | 1 | 0 | 1.5 | 1.4 |
| Reperfusion therapy | 12 | 5.5 | 3 | 2 | 1 | 4.0 | 2.4 |
| In-hospital mortality | 3 | 1 | 1 | 0 | 0 | 0.8 | 0.8 |
| Length stay (days) | 19 | 11 | 9.5 | 8 | 6 | 9.5 | 2.4 |
| Jan–May 2019 (Weekly) | Jan–May 2020 (Weekly) | p | Confi2019 (Weekly) | Confi2020 (Weekly) | p | |
|---|---|---|---|---|---|---|
| Calls EMS Center | 1245 | 2631 | 0.006 | 1225 | 3908 | 0.011 |
| Stroke code activations | 4.7 | 5.9 | 0.009 | 4.9 | 5.0 | 0.936 |
| All stroke admissions | 17.5 | 14.6 | 0.020 | 20.5 | 16.2 | 0.011 |
| Ischemic stroke | 13.1 | 11.5 | 0.097 | 15.5 | 12.4 | 0.039 |
| Hemorrhagic stroke | 1.8 | 1.5 | 0.441 | 2.2 | 2.0 | 0.791 |
| Transient Ischemic Attack | 2.5 | 1.7 | 0.026 | 2.8 | 1.8 | 0.086 |
| Tele-stroke consultations | 2.4 | 2.2 | 0.728 | 3.8 | 2.7 | 0.089 |
| Stroke severity score | 6.8 | 6.8 | 0.934 | 6.7 | 7.1 | 0.621 |
| Thrombolytic therapy | 2.6 | 2.2 | 0.367 | 3.5 | 1.7 | 0.003 |
| Endovascular therapy | 1.4 | 1.8 | 0.346 | 1.3 | 1.3 | 1.000 |
| Reperfusion therapy | 4.0 | 4.0 | 1.000 | 4.8 | 3.0 | 0.068 |
| In-hospital mortality | 0.6 | 0.9 | 0.247 | 0.9 | 1.2 | 0.464 |
| Length stay (days) | 10.8 | 8.4 | 0.001 | 9.8 | 8.0 | 0.009 |
| Variable | COVID | Code | All-S | IS | HS | TIA | T-S | TT | EVT | RT |
|---|---|---|---|---|---|---|---|---|---|---|
| COVID | . | −0.090 | 0.198 | 0.060 | 0.349 | −0.026 | 0.165 | −0.409 * | −0.455 * | −0.525 * |
| Code | −0.090 | . | 0.392 | 0.391 | −0.080 | 0.230 | −0.099 | 0.422 | −0.027 | 0.219 |
| All-S | 0.198 | 0.392 | . | 0.810 * | 0.267 | 0.468 * | 0.452 * | 0.203 | 0.021 | 0.127 |
| IS | 0.060 | 0.391 | 0.810 * | . | −0.237 | 0.082 | 0.569 * | 0.285 | 0.122 | 0.239 |
| HS | 0.349 | −0.080 | 0.267 | −0.237 | . | 0.102 | 0.035 | −0.184 | −0.231 | −0.253 |
| TIAs | −0.026 | 0.230 | 0.468 * | 0.082 | 0.102 | . | −0.192 | 0.089 | 0.041 | 0.077 |
| T-S | 0.165 | −0.099 | 0.452 * | 0.569 * | 0.035 | −0.192 | . | 0.283 | 0.382 | 0.407 |
| TT | −0.409 * | 0.422 | 0.203 | 0.285 | −0.184 | 0.089 | 0.283 | . | 0.362 | 0.796 * |
| EVT | −0.455 * | −0.027 | 0.021 | 0.122 | −0.231 | 0.041 | 0.382 | 0.362 | . | 0.853 * |
| RT | −0.525 * | 0.219 | 0.127 | 0.239 | −0.253 | 0.077 | 0.407 | 0.796 * | 0.853 * | . |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramírez-Moreno, J.M.; Portilla-Cuenca, J.C.; Hariramani-Ramchandani, R.; Rebollo, B.; Bermejo Casado, I.; Macías-Sedas, P.; Ceberino, D.; Roa-Montero, A.M.; González-Plata, A.; Casado, I.; et al. Slump in Hospital Admissions for Stroke, a Fact of an Uncertain Nature That Requires Explanation. Brain Sci. 2021, 11, 92. https://doi.org/10.3390/brainsci11010092
Ramírez-Moreno JM, Portilla-Cuenca JC, Hariramani-Ramchandani R, Rebollo B, Bermejo Casado I, Macías-Sedas P, Ceberino D, Roa-Montero AM, González-Plata A, Casado I, et al. Slump in Hospital Admissions for Stroke, a Fact of an Uncertain Nature That Requires Explanation. Brain Sciences. 2021; 11(1):92. https://doi.org/10.3390/brainsci11010092
Chicago/Turabian StyleRamírez-Moreno, José M., Juan Carlos Portilla-Cuenca, Roshan Hariramani-Ramchandani, Belen Rebollo, Inés Bermejo Casado, Pablo Macías-Sedas, David Ceberino, Ana M. Roa-Montero, Alberto González-Plata, Ignacio Casado, and et al. 2021. "Slump in Hospital Admissions for Stroke, a Fact of an Uncertain Nature That Requires Explanation" Brain Sciences 11, no. 1: 92. https://doi.org/10.3390/brainsci11010092
APA StyleRamírez-Moreno, J. M., Portilla-Cuenca, J. C., Hariramani-Ramchandani, R., Rebollo, B., Bermejo Casado, I., Macías-Sedas, P., Ceberino, D., Roa-Montero, A. M., González-Plata, A., Casado, I., & Fernández de Alarcón, L. (2021). Slump in Hospital Admissions for Stroke, a Fact of an Uncertain Nature That Requires Explanation. Brain Sciences, 11(1), 92. https://doi.org/10.3390/brainsci11010092