
Effects of Cognitive Training Programs on Executive Function in Children and Adolescents with Autism Spectrum Disorder: A Systematic Review

 , , and
, , and
Abstract
:1. Introduction
2. Executive Functions and Autism Spectrum Disorder
2.1. EF Heterogeneity in ASD
2.2. EFs and Social Skills
3. Cognitive Training of EFs in ASD
3.1. Methods
3.2. Eligibility Criteria
3.3. Search
Source of Data and Search Terms
3.4. Data Selection and Extraction
3.5. Quality Assessment
4. Results
4.1. Results of the Search
4.2. Characteristics of Included Studies
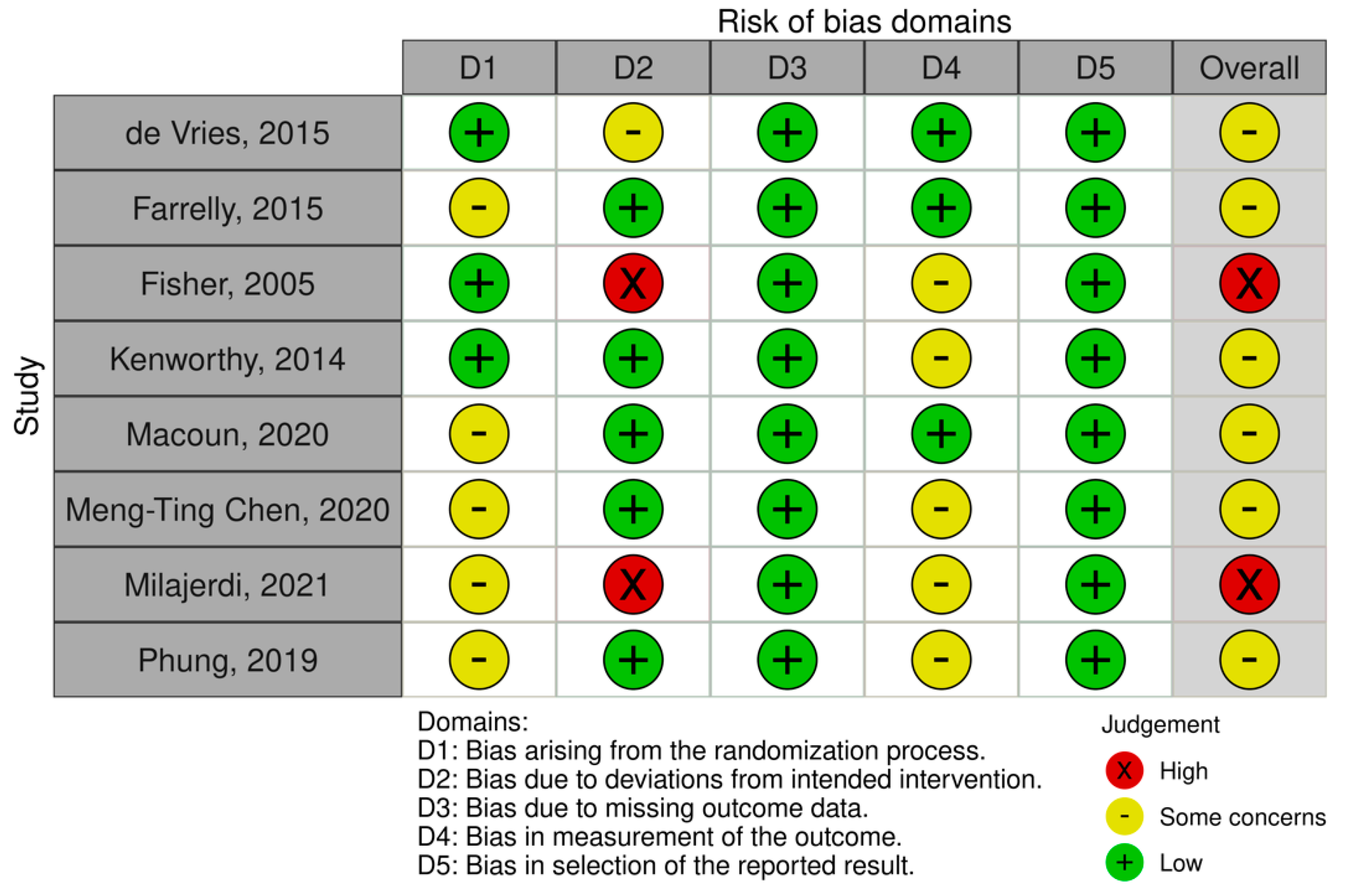
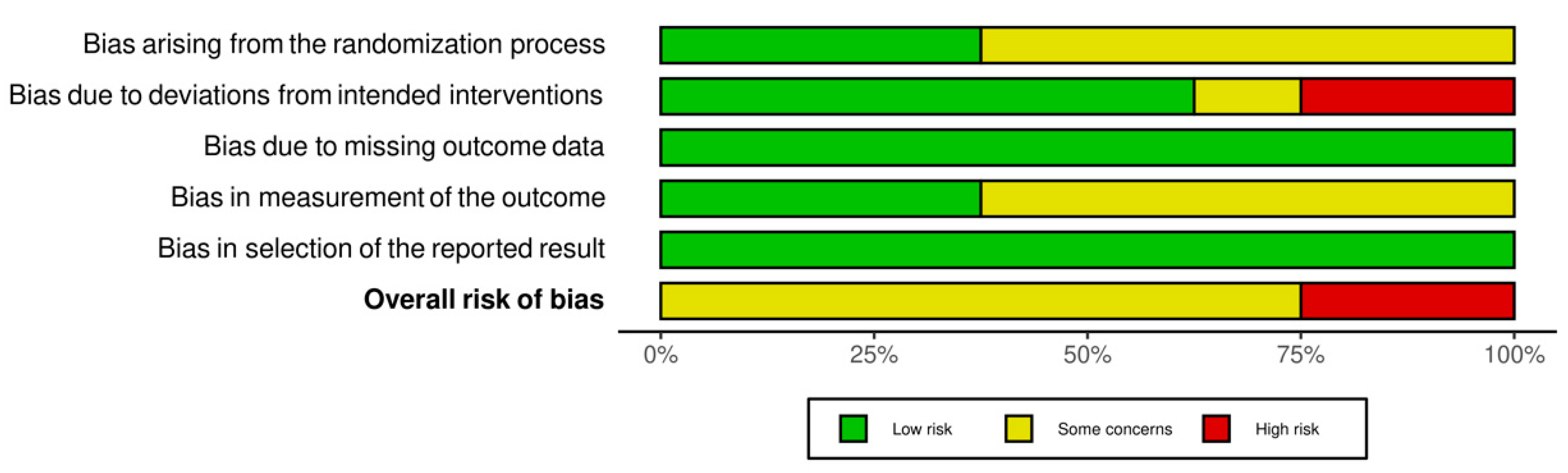
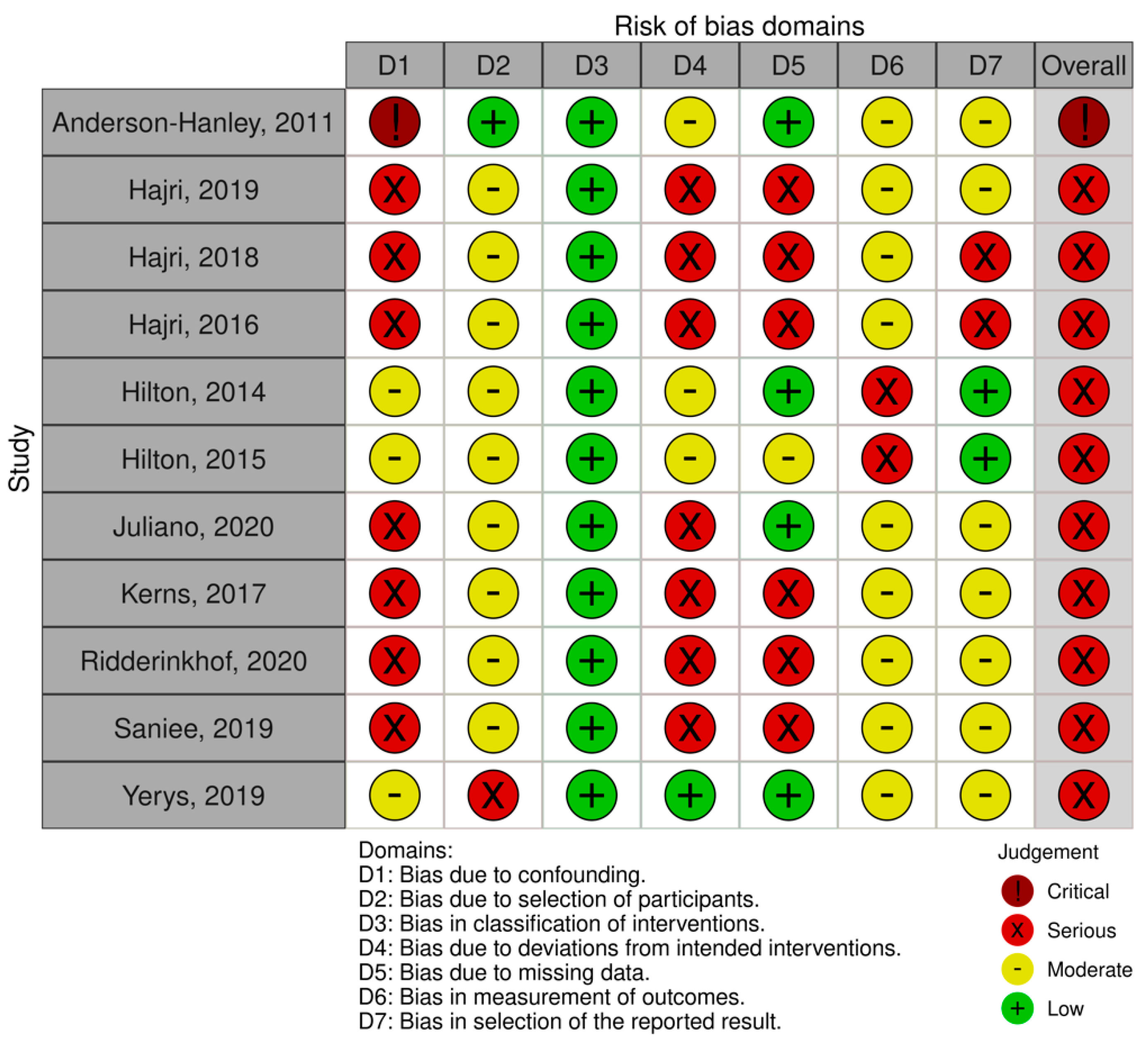
4.2.1. Methodological Quality and Risk of Bias
4.2.2. Participant Characteristics
4.2.3. Study Characteristics
4.3. Characteristics of Non-Computerized Trainings
4.4. Effects on Non-Computerized Training Outcomes
4.4.1. Primary Outcomes
4.4.2. Secondary Outcomes
4.5. Characteristics of Computerized Trainings
4.6. Effects on Computerized Training Outcomes
4.6.1. Primary Outcomes
4.6.2. Secondary Outcomes
5. Discussion
Clinical Implications
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; ISBN 9780890425558. [Google Scholar]
- Lai, M.-C.; Lombardo, M.V.; Baron-Cohen, S. Autism. Lancet 2014, 383, 896–910. [Google Scholar] [CrossRef]
- Happé, F.; Frith, U. Annual Research Review: Looking Back to Look Forward-Changes in the Concept of Autism and Implications for Future Research. J. Child. Psychol. Psychiatry 2020, 61, 218–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pender, R.; Fearon, P.; Heron, J.; Mandy, W. The Longitudinal Heterogeneity of Autistic Traits: A Systematic Review. Res. Autism Spectr. Disord. 2020, 79, 101671. [Google Scholar] [CrossRef]
- Wolfers, T.; Floris, D.L.; Dinga, R.; van Rooij, D.; Isakoglou, C.; Kia, S.M.; Zabihi, M.; Llera, A.; Chowdanayaka, R.; Kumar, V.J.; et al. From Pattern Classification to Stratification: Towards Conceptualizing the Heterogeneity of Autism Spectrum Disorder. Neurosci. Biobehav. Rev. 2019, 104, 240–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedman, L.; Sterling, A. A Review of Language, Executive Function, and Intervention in Autism Spectrum Disorder. Semin. Speech Lang. 2019, 40, 291–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demetriou, E.A.; Lampit, A.; Quintana, D.S.; Naismith, S.L.; Song, Y.J.C.; Pye, J.E.; Hickie, I.; Guastella, A.J. Autism Spectrum Disorders: A Meta-Analysis of Executive Function. Mol. Psychiatry 2018, 23, 1198–1204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engle, R.W. Working Memory Capacity as Executive Attention. Curr. Dir. Psychol. Sci. 2002, 11, 19–23. [Google Scholar] [CrossRef]
- Miyake, A.; Friedman, N.P.; Emerson, M.J.; Witzki, A.H.; Howerter, A.; Wager, T.D. The Unity and Diversity of Executive Functions and Their Contributions to Complex “Frontal Lobe” Tasks: A Latent Variable Analysis. Cognit. Psychol. 2000, 41, 49–100. [Google Scholar] [CrossRef] [Green Version]
- Miyake, A.; Friedman, N.P. The Nature and Organization of Individual Differences in Executive Functions: Four General Conclusions. Curr. Dir. Psychol. Sci. 2012, 21, 8–14. [Google Scholar] [CrossRef]
- Diamond, A. Executive Functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [Green Version]
- Zimmerman, D.L.; Ownsworth, T.; O’Donovan, A.; Roberts, J.; Gullo, M.J. Independence of Hot and Cold Executive Function Deficits in High-Functioning Adults with Autism Spectrum Disorder. Front. Hum. Neurosci. 2016, 10, 24. [Google Scholar] [CrossRef] [Green Version]
- Benso, F.; Moretti, S.; Bellazzini, V.; Benso, E.; Ardu, E.; Gazzellini, S. Principles of Integrated Cognitive Training for Executive Attention: Application to an Instrumental Skill. Front. Psychol. 2021, 12, 647749. [Google Scholar] [CrossRef]
- Brown, H.M.; Stahmer, A.C.; Dwyer, P.; Rivera, S. Changing the Story: How Diagnosticians Can Support a Neurodiversity Perspective from the Start. Autism 2021, 25, 1171–1174. [Google Scholar] [CrossRef] [PubMed]
- Leadbitter, K.; Buckle, K.L.; Ellis, C.; Dekker, M. Autistic Self-Advocacy and the Neurodiversity Movement: Implications for Autism Early Intervention Research and Practice. Front. Psychol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Miller, E.K.; Cohen, J.D. An Integrative Theory of Prefrontal Cortex Function. Annu. Rev. Neurosci. 2001, 24, 167–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espy, K.A. Using Developmental, Cognitive, and Neuroscience Approaches to Understand Executive Control in Young Children. Dev. Neuropsychol. 2004, 26, 379–384. [Google Scholar] [CrossRef]
- Burgess, P.; Simons, J. 18 Theories of Frontal Lobe Executive Function: Clinical Applications. In The Effectiveness of Rehabilitation for Cognitive Deficits; Halligan, W.P., Wade, D.T., Eds.; Oxford University Press: Oxford, UK, 2005; pp. 211–231. [Google Scholar] [CrossRef]
- Hill, E.L. Executive Dysfunction in Autism. Trends Cogn. Sci. 2004, 8, 26–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, C.L.E.; Lau, Z.; Lui, S.S.Y.; Lok, E.; Tam, V.; Chan, Q.; Cheng, K.M.; Lam, S.M.; Cheung, E.F.C. Meta-Analysis of Neuropsychological Measures of Executive Functioning in Children and Adolescents with High-Functioning Autism Spectrum Disorder. Autism Res. 2017, 10, 911–939. [Google Scholar] [CrossRef] [PubMed]
- Dawson, G.; Meltzoff, A.N.; Osterling, J.; Rinaldi, J. Neuropsychological Correlates of Early Symptoms of Autism. Child. Dev. 1998, 69, 1276–1285. [Google Scholar] [CrossRef] [Green Version]
- Dawson, G.; Munson, J.; Estes, A.; Osterling, J.; McPartland, J.; Toth, K.; Carver, L.; Abbott, R. Neurocognitive Function and Joint Attention Ability in Young Children with Autism Spectrum Disorder versus Developmental Delay. Child. Dev. 2002, 73, 345–358. [Google Scholar] [CrossRef]
- McEvoy, R.E.; Rogers, S.J.; Pennington, B.F. Executive Function and Social Communication Deficits in Young Autistic Children. J. Child. Psychol. Psychiatry 1993, 34, 563–578. [Google Scholar] [CrossRef] [PubMed]
- Griffith, E.M.; Pennington, B.F.; Wehner, E.A.; Rogers, S.J. Executive Functions in Young Children with Autism. Child. Dev. 1999, 70, 817–832. [Google Scholar] [CrossRef]
- Goldstein, S.; Naglieri, J.A. Handbook of Executive Functioning; Springer: New York, NY, USA, 2014; ISBN 978-1-4614-8105-8. [Google Scholar]
- Rabbitt, P. Introduction: Methodologies and Models in the Study of Executive Function. In Methodology of Frontal and Executive Function; Routledge: London, UK, 1997; pp. 1–38. [Google Scholar]
- Bernstein, J.H.; Waber, D.P. Executive Capacities from a Developmental Perspective. In Executive Function in Education: From Theory to Practice, 1st ed.; Guilford Press: New York, NY, USA, 2007; pp. 39–54. [Google Scholar]
- Engle, R.W.; Kane, M.J. Executive Attention, Working Memory Capacity, and a Two-Factor Theory of Cognitive Control. Psychol. Learn. Motiv. 2004, 44, 145–199. [Google Scholar]
- McCabe, D.P.; Roediger, H.L.; McDaniel, M.A.; Balota, D.A.; Hambrick, D.Z. The Relationship between Working Memory Capacity and Executive Functioning: Evidence for a Common Executive Attention Construct. Neuropsychology 2010, 24, 222–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pennington, B.F.; Ozonoff, S. Executive Functions and Developmental Psychopathology. J. Child. Psychol. Psychiatry 1996, 37, 51–87. [Google Scholar] [CrossRef]
- Snyder, H.R.; Miyake, A.; Hankin, B.L. Advancing Understanding of Executive Function Impairments and Psychopathology: Bridging the Gap between Clinical and Cognitive Approaches. Front. Psychol. 2015, 6, 328. [Google Scholar] [CrossRef] [Green Version]
- Morra, S.; Panesi, S.; Traverso, L.; Usai, M.C. Which Tasks Measure What? Reflections on Executive Function Development and a Commentary on Podjarny, Kamawar, and Andrews (2017). J. Exp. Child. Psychol. 2018, 167, 246–258. [Google Scholar] [CrossRef]
- Posner, M.I.; DiGirolamo, G.J. Executive Attention: Conflict, Target Detection, and Cognitive Control. In The Attentive Brain; The MIT Press: Cambridge, MA, USA, 1998; pp. 401–423. ISBN 0262161729. [Google Scholar]
- Engle, R.W.; Kane, M.J.; Tuholski, S.W. Individual Differences in Working Memory Capacity and What They Tell Us About Controlled Attention, General Fluid Intelligence, and Functions of the Prefrontal Cortex. In Models of Working Memory: Mechanisms of Active Maintenance and Executive Control; Cambridge University Press: New York, NY, USA, 1999; pp. 102–134. ISBN 052158325X. [Google Scholar]
- Rueda, M.R.; Rothbart, M.K.; McCandliss, B.D.; Saccomanno, L.; Posner, M.I. Training, Maturation, and Genetic Influences on the Development of Executive Attention. Proc. Natl. Acad. Sci. USA 2005, 102, 14931–14936. [Google Scholar] [CrossRef] [Green Version]
- Kane, M.J.; Engle, R.W. The Role of Prefrontal Cortex in Working-Memory Capacity, Executive Attention, and General Fluid Intelligence: An Individual-Differences Perspective. Psychon. Bull. Rev. 2002, 9, 637–671. [Google Scholar] [CrossRef] [Green Version]
- Repovs, G.; Baddeley, A. The Multi-Component Model of Working Memory: Explorations in Experimental Cognitive Psychology. Neuroscience 2006, 139, 5–21. [Google Scholar] [CrossRef]
- Geurts, H.; Sinzig, J.; Booth, R.; Happe, F. Neuropsychological Heterogeneity in Executive Functioning in Autism Spectrum Disorders. Int. J. Dev. Disabil. 2014, 60, 155–162. [Google Scholar] [CrossRef]
- Wallace, G.L.; Yerys, B.E.; Peng, C.; Dlugi, E.; Anthony, L.G.; Kenworthy, L. Assessment and Treatment of Executive Function Impairments in Autism Spectrum Disorder: An Update. In International Review of Research in Developmental Disabilities; Hodapp, R.M., Fidler, D.J., Eds.; Elsevier Academic Press Inc.: San Diego, CA, USA, 2016; Volume 51, pp. 85–122. ISBN 9780128051771. [Google Scholar]
- Hollocks, M.J.; Jones, C.R.G.; Pickles, A.; Baird, G.; Happé, F.; Charman, T.; Simonoff, E. The Association between Social Cognition and Executive Functioning and Symptoms of Anxiety and Depression in Adolescents with Autism Spectrum Disorders. Autism Res. 2014, 7, 216–228. [Google Scholar] [CrossRef] [PubMed]
- Demetriou, E.A.; Song, C.Y.; Park, S.H.; Pepper, K.L.; Naismith, S.L.; Hermens, D.F.; Hickie, I.B.; Thomas, E.E.; Norton, A.; White, D.; et al. Autism, Early Psychosis, and Social Anxiety Disorder: A Transdiagnostic Examination of Executive Function Cognitive Circuitry and Contribution to Disability. Transl. Psychiatry 2018, 8, 200. [Google Scholar] [CrossRef]
- Toplak, M.E.; West, R.F.; Stanovich, K.E. Practitioner Review: Do Performance-Based Measures and Ratings of Executive Function Assess the Same Construct? J. Child. Psychol. Psychiatry 2013, 54, 131–143. [Google Scholar] [CrossRef] [PubMed]
- Toplak, M.E.; Bucciarelli, S.M.; Jain, U.; Tannock, R. Executive Functions: Performance-Based Measures and the Behavior Rating Inventory of Executive Function (BRIEF) in Adolescents with Attention Deficit/Hyperactivity Disorder (ADHD). Child Neuropsychol. 2009, 15, 53–72. [Google Scholar] [CrossRef]
- Kenworthy, L.; Yerys, B.E.; Anthony, L.G.; Wallace, G.L. Understanding Executive Control in Autism Spectrum Disorders in the Lab and in the Real World. Neuropsychol. Rev. 2008, 18, 320–338. [Google Scholar] [CrossRef] [Green Version]
- Ozonoff, S. Reliability and Validity of the Wisconsin Card Sorting Test in Studies of Autism. Neuropsychology 1995, 9, 491–500. [Google Scholar] [CrossRef]
- Joseph, R.M.; Keehn, B.; Connolly, C.; Wolfe, J.M.; Horowitz, T.S. Why Is Visual Search Superior in Autism Spectrum Disorder? Dev. Sci. 2009, 12, 1083–1096. [Google Scholar] [CrossRef]
- Di Martino, A.; Ross, K.; Uddin, L.Q.; Sklar, A.B.; Castellanos, F.X.; Milham, M.P. Functional Brain Correlates of Social and Nonsocial Processes in Autism Spectrum Disorders: An Activation Likelihood Estimation Meta-Analysis. Biol. Psychiatry 2009, 65, 63–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uddin, L.; Supekar, K.; Menon, V. Reconceptualizing Functional Brain Connectivity in Autism from a Developmental Perspective. Front. Hum. Neurosci. 2013, 7, 458. [Google Scholar] [CrossRef] [Green Version]
- Jones, C.R.G.; Simonoff, E.; Baird, G.; Pickles, A.; Marsden, A.J.S.; Tregay, J.; Happé, F.; Charman, T. The Association between Theory of Mind, Executive Function, and the Symptoms of Autism Spectrum Disorder. Autism Res. 2018, 11, 95–109. [Google Scholar] [CrossRef]
- Kouklari, E.-C.; Tsermentseli, S.; Auyeung, B. Executive Function Predicts Theory of Mind but Not Social Verbal Communication in School-Aged Children with Autism Spectrum Disorder. Res. Dev. Disabil. 2018, 76, 12–24. [Google Scholar] [CrossRef]
- Pugliese, C.E.; Anthony, L.G.; Strang, J.F.; Dudley, K.; Wallace, G.L.; Naiman, D.Q.; Kenworthy, L. Longitudinal Examination of Adaptive Behavior in Autism Spectrum Disorders: Influence of Executive Function. J. Autism Dev. Disord. 2016, 46, 467–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmerman, D.; Ownsworth, T.; O’Donovan, A.; Roberts, J.; Gullo, M.J. Associations between Executive Functions and Mental Health Outcomes for Adults with Autism Spectrum Disorder. Psychiatry Res. 2017, 253, 360–363. [Google Scholar] [CrossRef] [PubMed]
- Wallace, G.L.; Budgett, J.; Charlton, R.A. Aging and Autism Spectrum Disorder: Evidence from the Broad Autism Phenotype. Autism Res. 2016, 9, 1294–1303. [Google Scholar] [CrossRef] [PubMed]
- Leung, R.C.; Zakzanis, K.K. Brief Report: Cognitive Flexibility in Autism Spectrum Disorders: A Quantitative Review. J. Autism Dev. Disord. 2014, 44, 2628–2645. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, Y.; Liu, L.; Cui, J.; Wang, J.; Shum, D.H.K.; van Amelsvoort, T.; Chan, R.C.K. A Meta-Analysis of Working Memory Impairments in Autism Spectrum Disorders. Neuropsychol. Rev. 2017, 27, 46–61. [Google Scholar] [CrossRef]
- Van den Bergh, S.F.W.M.; Scheeren, A.M.; Begeer, S.; Koot, H.M.; Geurts, H.M. Age Related Differences of Executive Functioning Problems in Everyday Life of Children and Adolescents in the Autism Spectrum. J. Autism Dev. Disord. 2014, 44, 1959–1971. [Google Scholar] [CrossRef]
- Hill, E.L. Evaluating the Theory of Executive Dysfunction in Autism. Dev. Rev. 2004, 24, 189–233. [Google Scholar] [CrossRef] [Green Version]
- Russell, J. How Executive Disorders Can Bring About an Inadequate “Theory of Mind”. In Autism as an Executive Disorder; Oxford University Press: New York, NY, USA, 1997; pp. 256–304. ISBN 9780198523499. [Google Scholar]
- Perone, S.; Almy, B.; Zelazo, P.D. Toward an Understanding of the Neural Basis of Executive Function Development. In The Neurobiology of Brain and Behavioral Development; Academic Press: Cambridge, MA, USA, 2018; pp. 291–314. [Google Scholar]
- Zelazo, P.D.; Carlson, S.M. Hot and Cool Executive Function in Childhood and Adolescence: Development and Plasticity. Child. Dev. Perspect. 2012, 6, 354–360. [Google Scholar] [CrossRef]
- Lewis, M.D.; Todd, R.M. The Self-Regulating Brain: Cortical-Subcortical Feedback and the Development of Intelligent Action. Cogn. Dev. 2007, 22, 406–430. [Google Scholar] [CrossRef] [Green Version]
- Fong, V.C.; Iarocci, G. The Role of Executive Functioning in Predicting Social Competence in Children with and without Autism Spectrum Disorder. Autism Res. 2020, 13, 1856–1866. [Google Scholar] [CrossRef]
- Leung, R.C.; Vogan, V.M.; Powell, T.L.; Anagnostou, E.; Taylor, M.J. The Role of Executive Functions in Social Impairment in Autism Spectrum Disorder. Child. Neuropsychol. 2016, 22, 336–344. [Google Scholar] [CrossRef] [PubMed]
- Gilotty, L.; Kenworthy, L.; Sirian, L.; Black, D.O.; Wagner, A.E. Adaptive Skills and Executive Function in Autism Spectrum Disorders. Child. Neuropsychol. 2002, 8, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Pugliese, C.E.; Anthony, L.; Strang, J.F.; Dudley, K.; Wallace, G.L.; Kenworthy, L. Increasing Adaptive Behavior Skill Deficits from Childhood to Adolescence in Autism Spectrum Disorder: Role of Executive Function. J. Autism Dev. Disord. 2015, 45, 1579–1587. [Google Scholar] [CrossRef]
- Cascia, J.; Barr, J.J. Associations among Vocabulary, Executive Function Skills and Empathy in Individuals with Autism Spectrum Disorder. J. Appl. Res. Intellect. Disabil. 2017, 30, 627–637. [Google Scholar] [CrossRef]
- Kerns, K.A.; Macoun, S.; MacSween, J.; Pei, J.; Hutchison, M. Attention and Working Memory Training: A Feasibility Study in Children with Neurodevelopmental Disorders. Appl. Neuropsychol. Child. 2017, 6, 120–137. [Google Scholar] [CrossRef]
- De Vries, M.; Prins, P.J.M.; Schmand, B.A.; Geurts, H.M. Working Memory and Cognitive Flexibility-Training for Children with an Autism Spectrum Disorder: A Randomized Controlled Trial. J. Child. Psychol. Psychiatry 2015, 56, 566–576. [Google Scholar] [CrossRef]
- Sohlberg, M.M.; Mateer, C.A. Cognitive Rehabilitation: An Integrative Neuropsychological Approach; Guilford Press: New York, NY, USA, 2001; ISBN 9781572306134. [Google Scholar]
- Takeuchi, H.; Sekiguchi, A.; Taki, Y.; Yokoyama, S.; Yomogida, Y.; Komuro, N.; Yamanouchi, T.; Suzuki, S.; Kawashima, R. Training of Working Memory Impacts Structural Connectivity. J. Neurosci. 2010, 30, 3297–3303. [Google Scholar] [CrossRef]
- Diamond, A.; Ling, D.S. Conclusions about Interventions, Programs, and Approaches for Improving Executive Functions That Appear Justified and Those That, Despite Much Hype, Do Not. Dev. Cogn. Neurosci. 2016, 18, 34–48. [Google Scholar] [CrossRef] [Green Version]
- Au, J.; Sheehan, E.; Tsai, N.; Duncan, G.J.; Buschkuehl, M.; Jaeggi, S.M. Improving Fluid Intelligence with Training on Working Memory: A Meta-Analysis. Psychon. Bull. Rev. 2015, 22, 366–377. [Google Scholar] [CrossRef] [Green Version]
- Melby-Lervåg, M.; Hulme, C. Is Working Memory Training Effective? A Meta-Analytic Review. Dev. Psychol. 2013, 49, 270–291. [Google Scholar] [CrossRef] [Green Version]
- Karbach, J.; Verhaeghen, P. Making Working Memory Work: A Meta-Analysis of Executive-Control and Working Memory Training in Older Adults. Psychol. Sci. 2014, 25, 2027–2037. [Google Scholar] [CrossRef] [Green Version]
- Schwaighofer, M.; Fischer, F.; Bühner, M. Does Working Memory Training Transfer? A Meta-Analysis Including Training Conditions as Moderators. Educ. Psychol. 2015, 50, 138–166. [Google Scholar] [CrossRef]
- Melby-Lervåg, M.; Redick, T.S.; Hulme, C. Working Memory Training Does Not Improve Performance on Measures of Intelligence or Other Measures of “Far Transfer”: Evidence from a Meta-Analytic Review. Perspect. Psychol. Sci. 2016, 11, 512–534. [Google Scholar] [CrossRef] [Green Version]
- Schubert, T.; Strobach, T.; Karbach, J. New Directions in Cognitive Training: On Methods, Transfer, and Application. Psychol. Res. 2014, 78, 749–755. [Google Scholar] [CrossRef]
- Grynszpan, O.; Weiss, P.L.T.; Perez-Diaz, F.; Gal, E. Innovative Technology-Based Interventions for Autism Spectrum Disorders: A Meta-Analysis. Autism Int. J. Res. Pract. 2014, 18, 346–361. [Google Scholar] [CrossRef]
- Kapp, K. The Gamification of Learning and Instruction: Game-Based Methods and Strategies for Training and Education; Pfeiffer: San Francisco, CA, USA, 2012; ISBN 978-1-118-09634-5. [Google Scholar]
- Lin, C.-S.; Chang, S.-H.; Liou, W.-Y.; Tsai, Y.-S. The Development of a Multimedia Online Language Assessment Tool for Young Children with Autism. Res. Dev. Disabil. 2013, 34, 3553–3565. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A Comparison Study of Specificity and Sensitivity in Three Search Tools for Qualitative Systematic Reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A Tool for Assessing Risk of Bias in Non-Randomised Studies of Interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Hilton, C.L.; Cumpata, K.; Klohr, C.; Gaetke, S.; Artner, A.; Johnson, H.; Dobbs, S. Effects of Exergaming on Executive Function and Motor Skills in Children with Autism Spectrum Disorder: A Pilot Study. Am. J. Occup. Ther. 2014, 68, 57–65. [Google Scholar] [CrossRef] [Green Version]
- Hilton, C.; Attal, A.; Best, J.; Reistetter, T.; Trapani, P.; Collins, D. Exergaming to Improve Physical and Mental Fitness in Children and Adolescents with Autism Spectrum Disorders: Pilot Study. Int. J. Sports Exerc. Med. 2015, 1, 017. [Google Scholar] [CrossRef]
- Chen, M.-T.; Chang, Y.-P.; Marraccini, M.E.; Cho, M.-C.; Guo, N.-W. Comprehensive Attention Training System (CATS): A Computerized Executive-Functioning Training for School-Aged Children with Autism Spectrum Disorder. Int. J. Dev. Disabil. 2020, 1–10. [Google Scholar] [CrossRef]
- Yerys, B.E.; Bertollo, J.R.; Kenworthy, L.; Dawson, G.; Marco, E.J.; Schultz, R.T.; Sikich, L. Brief Report: Pilot Study of a Novel Interactive Digital Treatment to Improve Cognitive Control in Children with Autism Spectrum Disorder and Co-Occurring ADHD Symptoms. J. Autism Dev. Disord. 2019, 49, 1727–1737. [Google Scholar] [CrossRef]
- Phung, J.N.; Goldberg, W.A. Promoting Executive Functioning in Children with Autism Spectrum Disorder Through Mixed Martial Arts Training. J. Autism Dev. Disord. 2019, 49, 3669–3684. [Google Scholar] [CrossRef]
- Kenworthy, L.; Anthony, L.G.; Naiman, D.Q.; Cannon, L.; Wills, M.C.; Luong-Tran, C.; Werner, M.A.; Alexander, K.C.; Strang, J.; Bal, E.; et al. Randomized Controlled Effectiveness Trial of Executive Function Intervention for Children on the Autism Spectrum. J. Child. Psychol. Psychiatry 2014, 55, 374–383. [Google Scholar] [CrossRef]
- Fisher, N.; Happé, F. A Training Study of Theory of Mind and Executive Function in Children with Autistic Spectrum Disorders. J. Autism Dev. Disord. 2005, 35, 757–771. [Google Scholar] [CrossRef]
- Anderson-Hanley, C.; Tureck, K.; Schneiderman, R.L. Autism and Exergaming: Effects on Repetitive Behaviors and Cognition. Psychol. Res. Behav. Manag. 2011, 4, 129–137. [Google Scholar] [CrossRef] [Green Version]
- Ridderinkhof, A.; de Bruin, E.I.; van den Driesschen, S.; Bögels, S.M. Attention in Children with Autism Spectrum Disorder and the Effects of a Mindfulness-Based Program. J. Atten. Disord. 2020, 24, 681–692. [Google Scholar] [CrossRef] [Green Version]
- Rafiei Milajerdi, H.; Sheikh, M.; Najafabadi, M.G.; Saghaei, B.; Naghdi, N.; Dewey, D. The Effects of Physical Activity and Exergaming on Motor Skills and Executive Functions in Children with Autism Spectrum Disorder. Games Health J. 2021, 10, 33–42. [Google Scholar] [CrossRef]
- Macoun, S.J.; Schneider, I.; Bedir, B.; Sheehan, J.; Sung, A. Pilot Study of an Attention and Executive Function Cognitive Intervention in Children with Autism Spectrum Disorders. J. Autism Dev. Disord. 2020, 51, 2600–2610. [Google Scholar] [CrossRef] [PubMed]
- Saniee, S.; Pouretemad, H.R.; Zardkhaneh, S.A. Developing Set-Shifting Improvement Tasks (SSIT) for Children with High-Functioning Autism. J. Intellect. Disabil. Res. 2019, 63, 1207–1220. [Google Scholar] [CrossRef] [PubMed]
- Hajri, M.; Abbes, Z.; Ben Yahia, H.; Boudali, M.; Bouden, A.; Mrabet, A.; Amado, I. Cognitive Remediation Therapy in Autism Spectrum Disorder: Tunisian Experience. Tunis. Med. 2019, 97, 795–801. [Google Scholar] [PubMed]
- Hajri, M.; Abbes, Z.; Ben Yahia, H.; Boudali, M.; Bouden, A.; Mrabet, A.; Amado, I. Remédiation cognitive et fonctionnement scolaire chez les enfants avec trouble du spectre autistique. Neuropsychiatr. Enfance Adolesc. 2018, 67, 19–24. [Google Scholar] [CrossRef]
- Hajri, M.; Abbes, Z.; Ben Yahia, H.; Boudali, M.; Halayem, S.; Othman, S.; Bouden, A. Effects of Cognitive Remediation Therapy on Mental Flexibility in Children with Autism Spectrum Disorder. Eur. Child. Adolesc. Psychiatry 2015, 24, S249. [Google Scholar]
- Juliano, A.C.; Alexander, A.O.; DeLuca, J.; Genova, H. Feasibility of a School-Based Mindfulness Program for Improving Inhibitory Skills in Children with Autism Spectrum Disorder. Res. Dev. Disabil. 2020, 101, 103641. [Google Scholar] [CrossRef]
- Farrelly, K.; Mace, S. An Intervention to Enhance Cognitive Flexibility in Boys Aged 11–13 with Autism Spectrum Disorder. Surrey Undergrad. Res. J. 2015, 1, 1–19. [Google Scholar]
- Gioia, G.; Isquith, P.; Guy, S.C.; Kenworthy, L. Behavior Rating Inventory of Executive Function; Psychological Assessment Resources: Lutz, FL, USA, 2000. [Google Scholar]
- Heaton, R.; Chelune, C.; Talley, J.; Kay, G.; Curtiss, G. Wisconsin Card Sorting Test Manual-Revised and Expanded; Psychological Assessment Resources: Lutz, FL, USA, 1993. [Google Scholar]
- Stroop, J.R. Studies of Interference in Serial Verbal Reactions. J. Exp. Psychol. 1935, 18, 643–662. [Google Scholar] [CrossRef]
- Partington, J.E.; Leiter, R.G. Partington’s Pathways Test. Psychol. Serv. Cent. J. 1949, 1, 11–20. [Google Scholar]
- Wykes, T.; Reeder, C.; Corner, J.; Williams, C.; Everitt, B. The Effects of Neurocognitive Remediation on Executive Processing in Patients with Schizophrenia. Schizophr. Bull. 1999, 25, 291–307. [Google Scholar] [CrossRef] [Green Version]
- Hamza, M.; Abbès, Z.; Yahyia, H.B.; Fakhfekh, R.; Amado, I.; Bouden, A. The Cognitive Remediation Therapy Program among Children with ADHD: Tunisian Experience. Tunis. Med. 2018, 96, 30–35. [Google Scholar]
- Azouz, O.B.; Dellagi, L.; Kebir, O.; Johnson, I.; Amado, I.; Tabbane, K. The Tunisian Cognitive Battery for Patients with Schizophrenia. Tunis. Med. 2009, 87, 674–679. [Google Scholar]
- Shebani, M.F.A.; Van De Vijver, F.J.R.; Poortinga, Y.H. A Strict Test of the Phonological Loop Hypothesis with Libyan Data. Mem. Cognit. 2005, 33, 196–202. [Google Scholar] [CrossRef] [Green Version]
- Heaton, R.K.; Gladsjo, J.A.; Palmer, B.W.; Kuck, J.; Marcotte, T.D.; Jeste, D.V. Stability and Course of Neuropsychological Deficits in Schizophrenia. Arch. Gen. Psychiatry 2001, 58, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Gladsjo, J.A.; Schuman, C.C.; Evans, J.D.; Peavy, G.M.; Miller, S.W.; Heaton, R.K. Norms for Letter and Category Fluency: Demographic Corrections for Age, Education, and Ethnicity. Assessment 1999, 6, 147–178. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Song, L.-L.; Cheung, E.F.C.; Lui, S.S.Y.; Shum, D.H.K.; Chan, R.C.K. Bipolar Disorder and Schizophrenia Share a Similar Deficit in Semantic Inhibition: A Meta-Analysis Based on Hayling Sentence Completion Test Performance. Neuro-Psychopharmacol. Biol. Psychiatry 2013, 46, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Rueda, M.R.; Fan, J.; McCandliss, B.D.; Halparin, J.D.; Gruber, D.B.; Lercari, L.P.; Posner, M.I. Development of Attentional Networks in Childhood. Neuropsychologia 2004, 42, 1029–1040. [Google Scholar] [CrossRef] [PubMed]
- Constantino, J.; Gruber, C. Social Responsiveness Scale: SRS 2; Western Psychological Services: Torrance, CA, USA, 2012. [Google Scholar]
- Greenberg, L.; Kindschi, C.; Dupuy, T.; Corman, C. Test of Variables of Attention; Psychological Assessment Resources: Lutz, FL, USA, 1996. [Google Scholar]
- Lezak, M.D.; Howieson, D.B.; Loring, D.W.; Hannay, H.J.; Fischer, J.S. Neuropsychological Assessment, 4th ed.; Oxford University Press: New York, NY, USA, 2004; ISBN 9780195111217. [Google Scholar]
- Romine, C.B.; Lee, D.; Wolfe, M.E.; Homack, S.; George, C.; Riccio, C.A. Wisconsin Card Sorting Test with Children: A Meta-Analytic Study of Sensitivity and Specificity. Arch. Clin. Neuropsychol. 2004, 19, 1027–1041. [Google Scholar] [CrossRef]
- Reitan, R.M. The Relation of the Trail Making Test to Organic Brain Damage. J. Consult. Psychol. 1955, 19, 393–394. [Google Scholar] [CrossRef]
- Gresham, F.; Elliott, S.N. Social Skills Improvement System (SSIS) Rating Scales; Pearson Education Inc.: San Antonio, TX, USA, 2007. [Google Scholar]
- Hartman, C.A.; Luteijn, E.; Serra, M.; Minderaa, R. Refinement of the Children’s Social Behavior Questionnaire (CSBQ): An Instrument That Describes the Diverse Problems Seen in Milder Forms of PDD. J. Autism Dev. Disord. 2006, 36, 325–342. [Google Scholar] [CrossRef]
- DuPaul, G.J.; Power, T.J.; Anastopoulos, A.D.; Reid, R. ADHD Rating Scale-IV: Checklists, Norms, and Clinical Interpretation; Guilford Press: New York, NY, USA, 1998; ISBN 9781572304239. [Google Scholar]
- Epstein, M.H. The Behavioral and Emotional Rating Scale: A Strength-Based Approach to Assessment. Diagnostique 2000, 25, 249–256. [Google Scholar] [CrossRef]
- Conners, K.C., III. Conners 3rd Edition Manual; Multi-Health Systems: New York, NY, USA, 2008. [Google Scholar]
- Gilliam, J. Gilliam Autism Rating Scale, 2nd ed.; Pro-Ed: Austin, TX, USA, 2006. [Google Scholar]
- Oosterlaan, J.; Scheres, A.; Antrop, I.; Roeyers, H.; Sergeant, J.A. Handleiding Bij de Vragenlijst Voor Gedragsproblemen Bij Kinderen VvGK; Swets Test Publishers: Amsterdam, The Netherlands, 2000. [Google Scholar]
- Gilliam, J.E. GARS: Gilliam Autism Rating Scale; Pro-Ed: Austin, TX, USA, 1995. [Google Scholar]
- Hosp, M.K.; Hosp, J.L.; Howell, K.W. The ABCs of CBM: A Practical Guide to Curriculum-Based Measurement; Practical Intervention in the Schools Series; Guilford Press: New York, NY, USA, 2007. [Google Scholar]
- Shinn, M.; Michelle, M. AIMSweb Training Workbook Administration and Scoring of Reading Curriculum-Based Measurement (R-CBM) for Use in General Outcome Measurement; Edformation: Eden Prairie, MN, USA, 2002. [Google Scholar]
- Woodcock, R.W.; McGrew, K.S.; Mather, N. Woodcock-Johnson III Normative Update (NU) Tests of Achievement, Forms A and B; Riverside Publishing: Rolling Meadows, IL, USA, 2007. [Google Scholar]
- Zwaigenbaum, L.; Bauman, M.L.; Choueiri, R.; Kasari, C.; Carter, A.; Granpeesheh, D.; Mailloux, Z.; Smith Roley, S.; Wagner, S.; Fein, D.; et al. Early Intervention for Children with Autism Spectrum Disorder Under 3 Years of Age: Recommendations for Practice and Research. Pediatrics 2015, 136, 60–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landa, R.J. Efficacy of Early Interventions for Infants and Young Children with, and at Risk for, Autism Spectrum Disorders. Int. Rev. Psychiatry 2018, 30, 25–39. [Google Scholar] [CrossRef] [PubMed]
- Bierman, K.L.; Torres, M. Promoting the Development of Executive Functions through Early Education and Prevention Programs. In Executive Function in Preschool-Age Children: Integrating Measurement, Neurodevelopment and Translational Research; Griffin, J.A., McCardle, P., Freund, L.S., Eds.; American Psychological Association: Washington, DC, USA, 2016; pp. 299–326. ISBN 9781433818264. [Google Scholar]
- Traverso, L.; Viterbori, P.; Usai, M.C. Effectiveness of an Executive Function Training in Italian Preschool Educational Services and Far Transfer Effects to Pre-Academic Skills. Front. Psychol. 2019, 10, 2053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baron-Cohen, S.; Golan, O.; Ashwin, E. Educational Cognitive Neuroscience: Designing Autism-Friendly Methods to Teach Emotion Recognition. In Neuroscience in Education: The Good, the Bad and the Ugly; Oxford University Press: Oxford, UK, 2012. [Google Scholar] [CrossRef]
- Swettenham, J. Can Children with Autism Be Taught to Understand False Belief Using Computers? J. Child. Psychol. Psychiatry 1996, 37, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.; Taylor, J. Interactive Multimedia Systems for Students with Autism. J. Educ. Media 2000, 25, 169–177. [Google Scholar] [CrossRef]
- Murray, D. Autism and Information Technology: Therapy with Computers. In Autism and Learning; Routledge: London, UK, 1997; ISBN 185346421X. [Google Scholar]
- Fletcher-Watson, S.; Pain, H.; Hammond, S.; Humphry, A.; McConachie, H. Designing for Young Children with Autism Spectrum Disorder: A Case Study of an IPad App. Int. J. Child-Comput. Interact. 2016, 7, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Barajas, A.O.; Al Osman, H.; Shirmohammadi, S. A Serious Game for Children with Autism Spectrum Disorder as a Tool for Play Therapy. In Proceedings of the 2017 IEEE 5th International Conference on Serious Games and Applications for Health, Perth, Australia, 2–4 April 2017; pp. 1–7. [Google Scholar]
- Engle, R.W. Working Memory and Executive Attention: A Revisit. Perspect. Psychol. Sci. 2018, 13, 190–193. [Google Scholar] [CrossRef]
- Seltzer, M.M.; Shattuck, P.; Abbeduto, L.; Greenberg, J.S. Trajectory of Development in Adolescents and Adults with Autism. Ment. Retard. Dev. Disabil. Res. Rev. 2004, 10, 234–247. [Google Scholar] [CrossRef] [PubMed]
- Wetherby, A.M.; Guthrie, W.; Woods, J.; Schatschneider, C.; Holland, R.D.; Morgan, L.; Lord, C. Parent-Implemented Social Intervention for Toddlers with Autism: An RCT. Pediatrics 2014, 134, 1084–1093. [Google Scholar] [CrossRef] [Green Version]
- Green, J.; Charman, T.; Pickles, A.; Wan, M.W.; Elsabbagh, M.; Slonims, V.; Taylor, C.; McNally, J.; Booth, R.; Gliga, T.; et al. Parent-Mediated Intervention versus No Intervention for Infants at High Risk of Autism: A Parallel, Single-Blind, Randomised Trial. Lancet Psychiatry 2015, 2, 133–140. [Google Scholar] [CrossRef]
- Oono, I.P.; Honey, E.J.; McConachie, H. Parent-Mediated Early Intervention for Young Children with Autism Spectrum Disorders (ASD). Evid. Based Child. Health Cochrane Rev. J. 2013, 8, 2380–2479. [Google Scholar] [CrossRef]
- Rispoli, K.M.; Malcolm, A.L.; Nathanson, E.W.; Mathes, N.E. Feasibility of an Emotion Regulation Intervention for Young Children with Autism Spectrum Disorder: A Brief Report. Res. Autism Spectr. Disord. 2019, 67, 101420. [Google Scholar] [CrossRef]
- Fuller, E.A.; Oliver, K.; Vejnoska, S.F.; Rogers, S.J. The Effects of the Early Start Denver Model for Children with Autism Spectrum Disorder: A Meta-Analysis. Brain Sci. 2020, 10, 368. [Google Scholar] [CrossRef]
- Bradshaw, J.; Koegel, L.K.; Koegel, R.L. Improving Functional Language and Social Motivation with a Parent-Mediated Intervention for Toddlers with Autism Spectrum Disorder. J. Autism Dev. Disord. 2017, 47, 2443–2458. [Google Scholar] [CrossRef]
- Sandbank, M.; Bottema-Beutel, K.; Crowley, S.; Cassidy, M.; Dunham, K.; Feldman, J.I.; Crank, J.; Albarran, S.A.; Raj, S.; Mahbub, P.; et al. Project AIM: Autism Intervention Meta-Analysis for Studies of Young Children. Psychol. Bull. 2020, 146, 1–29. [Google Scholar] [CrossRef]
- Perry, A.; Blacklock, K.; Dunn Geier, J. The Relative Importance of Age and IQ as Predictors of Outcomes in Intensive Behavioral Intervention. Res. Autism Spectr. Disord. 2013, 7, 1142–1150. [Google Scholar] [CrossRef]
- Fanelli, D. Negative Results Are Disappearing from Most Disciplines and Countries. Scientometrics 2012, 90, 891–904. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Eligibility Criteria | |
|---|---|
| Population | Individuals (up to 23 years of age) diagnosed with Autism Spectrum Disorder (ASD). |
| Intervention | Computerized and non-computerized interventions aimed to target executive functions. The training could be administered individually or in a small group, with different durations and frequencies, in different settings (home, clinics, community, school). In addition, it could be delivered with the support of different figures (psychologists, teachers, parents, speech therapists, health care professionals). |
| Comparisons | Other types of intervention which did not target executive functions, other interventions that were considered “treatment as usual”, waiting list, no intervention group. |
| Outcomes | Primary outcomes: Improvement in executive function domains, measured with standardized tests. Secondary outcomes: A core feature of ASD o related cognitive domains/ social skills. |
| Settings | Any setting (e.g., home, clinics, community, school) |
| Study design | Randomized control trials (RCTs). If no RCTs were available: quasi-experimental studies or single-group studies were also included. We considered only systematic reviews (SR) or meta-analyses that (1) were included in at least one database (e.g., PubMed); (2) reported the participants inclusion criteria; (3) conducted quality or risk of bias assessment on included studies; and (4) provided a list and synthesis of included studies. |
| Limits | The SR focused on studies published between 2000 and 2020 with no publication language limit. |
| Exclusion criteria | Individuals with traumatic brain injuries, primary disorders (sensory, neurological, psychiatric). Editorials, Opinions and Commentaries. Qualitative studies. Single case studies. |
| First Author and Year of Publication | Sample Characteristics/ Attrition Rate | Age (Years) | Study Design | Intervention Type | Intervention Target | Intervention Duration | Setting/ Trainer | Outcomes | Pre- and Posttest | Findings | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Primary | Secondary | ||||||||||
| Milajerdi, 2021 | n = 60 | 6–10 | RCT | Computerized “Kinect” | motor skills, EFs | tot hrs = 14 schedule = 3 sess. x week for 8 weeks | N/A/ research assistant | cognitive flexibility | N/A | WCST | Positive |
| Macoun, 2020 | n = 23 (2 with ADHD, 2 with tics/sensory)/ 13% | 6–12 | RCT | Computerized “Caribbean Quest” | WM, inhibitory control, selective attention, and sustained attention | tot hrs = 12 schedule = 3 sess. x week for 8 weeks | school/ research assistant | attention; visual and verbal WM; EF daily life | academic achievement; behavioral symptoms; social skills | KiTAP; SSP and DS; ORF; WJ-III; BRIEF; CRS-3; BERS-2; SSRS; GARS-2 | Mixed |
| Meng-Ting Chen, 2020 | n = 25 (9 with ADHD) | 6–12 | RCT | Computerized Comprehensive Attention Training System | sustained attention, sensory selection, response selection and control, attention | tot hrs = 6.6 schedule = once sess. per week for 8 weeks | clinic/ graduate student | cognitive flexibility | social adaptability | WCST; TMT; VABS | Positive |
| Ridderinkhof, 2020 | n = 100 | 8–23 | RCT | Non Computerized mindfulness-based program | focused and sustained attention | tot hrs = 15 scheduleNA | N/A/ mindfulness trainer | attention | N/A | ANT | Null |
| Juliano, 2020 | n = 29 (18 with ADHD, 11 with Anxiety Disorder, 3 with Sensory Processing Disorder, 1 with Language Disorder)/ 6.8% | 10–17 | QE | Non Computerized mindfulness-based program | attention, inhibition | tot hrs = 8 schedule = 2 sess. x week for 8 weeks | school/ educator | attention; inhibition | N/A | CWIT; W/DW; CN | Positive |
| Yerys, 2019 | n = 19 (with ADHD symptoms) | 9–13 | QE | Computerized “Project EVO” | attention, cognitive control | tot hrs = 8.3 schedule = 5 sess. x week for 4 weeks | home/ parents | attention; impulsivity; spatial WM; EF daily life | social skills; ADHD symptoms | TOVA; CANTAB; ADHD-RS-IV; BRIEF-2; SSIS | Mixed |
| Saniee, 2019 | n = 24 | 5–7 | QE | Computerized “Tatka” + Non Computerized home tasks | set-shifting ability | tot hrs = 56 schedule = 4 sess. x day for 2 months | home/ parents | cognitive flexibility | autism symptoms | MCS; BFRS-R; GARS; ATEC | Positive |
| Phung, 2019 | n = 34 | 8–11 | RCT | Non Computerized Mixed Martial Arts | behavioral inhibition, WM, cognitive fexibility | tot hrs = 19.5 schedule = 2 sess. x week for 13 weeks | school/ instructor | behavioral inhibition, WM, cognitive fexibility; EF daily life | N/A | HFT; BRIEF | Positive |
| Hajri, 2019 | n = 24/ 33.3% | 6–21 | QE | Non Computerized CRT | cognitive flexibility, WM, planning | tot hrs = 18 schedule = once sess. per week for 5–6 months | clinic/ therapist | cognitive flexibility; WM | non verbal intelligence; autism symtomps; academic results | SVFT; DSF and DSB; CARS; CMP; academic results | Positive |
| Hajri, 2018 | n = 25/ 36% | 6–21 | QE | Non Computerized CRT | cognitive flexibility, WM, planning | tot hrs = 13.5–18 schedule = once sess. per week for 6 months | clinic/ therapist | cognitive flexibility; WM; planning; inhibition | academic results | SVFT; DSF and DSB; ROCF; HSCT; CAAT; academic results | Mixed |
| Kerns, 2017 | n = 23/ 26% | 6–13 | QE | Computerized “Caribbean Quest” | WM, attention | tot hrs = 12–18 schedule = 2–3 sess. x week for 8–12 weeks | school/ educator | attention; WM; EF daily life | academic results; behavioral symptoms | KiTAP, WMTB-C; SSP and DS; AIMSweb; BRIEF; CRS-3; BERS-2 | Positive |
| Hajri, 2016 | n = 25/ 36% | 6–21 | QE | Non Computerized CRT | Cognitive flexibility, WM, planning | tot hrs = 18 schedule = once sess. per week for 6 months | clinic/ therapist | cognitive flexibility; WM; | non verbal intelligence; autism symptoms; academic results | SVFT; DSF and DSB; CARS; CPM; academic results | Positive |
| de Vries, 2015 | n= 121/ 26% | 8–12 | RCT | Computerized “Braingame Brian” | cognitive flexibility, WM | tot hrs = NA schedule = 25 sess. per 6 weeks | home/ parents | cognitive flexibility; WM; inhibition; attention; EF daily life | social skills; ADHD symptoms | Task-Switching; Corsi-BTT; N-back; Stop task; SART; BRIEF; CSBQ; DBDRS-ADHD | Mixed |
| Farrelly, 2015 | n = 20/ 10% | 11–13 | RCT | Non Computerized cognitive flexibility intervention | cognitive flexibility | tot hrs = 1.5 schedule = 3 sess. per 3 weeks | school/ investigator | cognitive flexibility | N/A | TMT | Positive |
| Hilton, 2015 | n = 17/ 5.5 % | 8–18 | QE | Computerized “Makoto Arena” | motor skills, EFs | tot hrs = 0.5 schedule = 3 sess. x week for 5 weeks | school/ graduate student | EF daily life | N/A | BRIEF | Positive |
| Hilton, 2014 | n = 8/ 12.5% | 6–13 | QE | Computerized “Makoto Arena” | motor skills, EFs | tot hrs = 0.5 schedule = 3 sess. x week for 5 weeks | school/ graduate student | EF daily life | N/A | BRIEF | Positive |
| Kenworthy, 2014 | n = 67/ 5% | 7–11 | RCT | Non Computerized “Unstuck and On Target” | physical/mental flexibility, goal setting, planning | tot hrs = 14–18.6 schedule = 28 sess. during 1 school-year | school/ teacher, parent, interventionist | cognitive/behavioral flexibility; planning; EF daily life | social skills | WBD; CT; BRIEF; SRS | Positive |
| Anderson-Hanley, 2011 | n = 24/ 8.3% | 8–21 | QE | Computerized “Cybercycling” or “Dance Dance Revolution” | EFs, exercise behaviors | tot hrs = 0.3 schedule = NA | N/A | WM; switching; inhibition | repetitive and stereotyped behaviors | DSF and DSB; CTT; Stroop task; videotapes according to the RBS of the GARS-2 | Mixed |
| Fisher, 2005 | n= 27 | 6–15 | RCT | Non Computerized EF training programme | inhibition, set-shifting | tot hrs = 2–4 schedule = one sess. for 5–10 days | school/ investigator | set-shifting; EF daily life | ToM | CST; TMT; ToM and EF questionnaire; FB tasks | Mixed |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pasqualotto, A.; Mazzoni, N.; Bentenuto, A.; Mulè, A.; Benso, F.; Venuti, P. Effects of Cognitive Training Programs on Executive Function in Children and Adolescents with Autism Spectrum Disorder: A Systematic Review. Brain Sci. 2021, 11, 1280. https://doi.org/10.3390/brainsci11101280
Pasqualotto A, Mazzoni N, Bentenuto A, Mulè A, Benso F, Venuti P. Effects of Cognitive Training Programs on Executive Function in Children and Adolescents with Autism Spectrum Disorder: A Systematic Review. Brain Sciences. 2021; 11(10):1280. https://doi.org/10.3390/brainsci11101280
Chicago/Turabian StylePasqualotto, Angela, Noemi Mazzoni, Arianna Bentenuto, Anna Mulè, Francesco Benso, and Paola Venuti. 2021. "Effects of Cognitive Training Programs on Executive Function in Children and Adolescents with Autism Spectrum Disorder: A Systematic Review" Brain Sciences 11, no. 10: 1280. https://doi.org/10.3390/brainsci11101280