
Developmental Language Disorder and Autism: Commonalities and Differences on Language


Abstract
1. Theoretical Premises
1.1. Developmental Language Disorder
1.2. Autism Spectrum Disorder
1.3. A Potential Overlap between ASD and DLD: Language Development in DLD
1.4. Language Ability in ASD
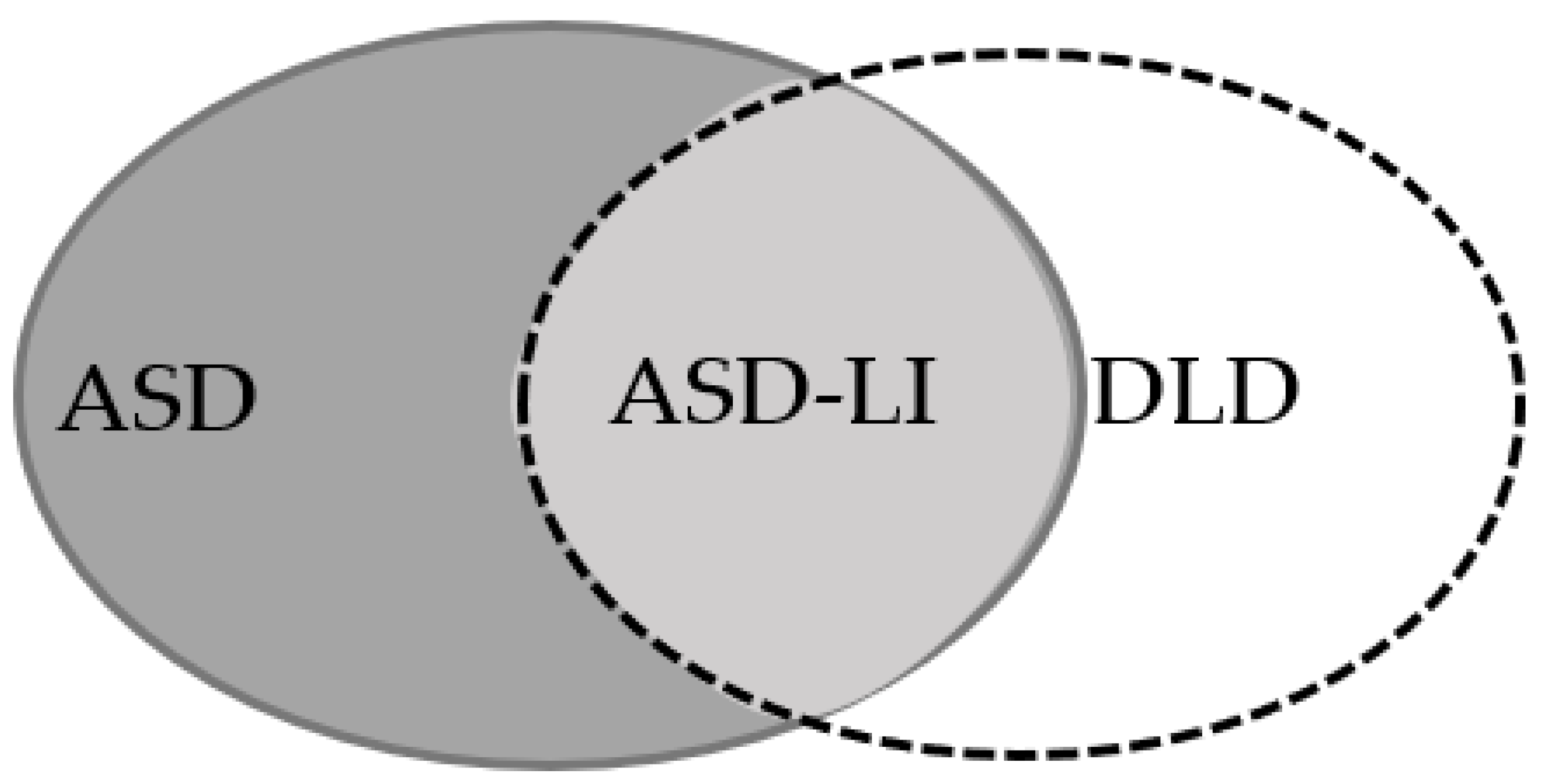
1.5. ASD and DLD Children’s Relation on Language Ability
1.5.1. Similarities
1.5.2. Differences
1.6. The Present Study
1.6.1. Purpose of the Study
1.6.2. Hypotheses
2. Materials and Methods
2.1. Participants’ Recruitment
2.1.1. Demographic Characteristics
2.1.2. Group Selection
2.1.3. Exclusion Criteria
2.2. Measures
2.2.1. Pre-Test Examination Measure
2.2.2. Assessment Measures



- “Ζήτησε να έρθει μαζί μας γεμάτος χαρά” (He asked to come with us full of joy).
- “H κατάσταση ήταν πραγματικά πολύ άσχημη για όλους” (The situation was very bad for everyone).
- “Aποφάσισαν ότι το χωράφι θα πουληθεί και τα λεφτά θα μοιραστούν στα τρία αδέλφια και τις δύο αδελφές” (They decided that the field will be sold and the money will be divided to the three brothers and the two sisters), and
2.3. Statistical Analysis
2.3.1. Preliminary Analysis
2.3.2. Power Analysis
2.3.3. Main Analysis
3. Results
4. Discussion
4.1. Limitations
4.2. Strengths of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Williams, D.; Botting, N.; Boucher, J. Language in Autism and Specific Language Impairment: Where Are the Links? Psychol. Bull. 2008, 134, 944–963. [Google Scholar] [CrossRef] [PubMed]
- Riches, N.G.; Loucas, T.; Baird, G.; Charman, T.; Simonoff, E. Sentence repetition in adolescents with Specific Language Impairments and autism: An investigation of complex syntax. Int. J. Lang. Commun. Disord. 2010, 45, 47–60. [Google Scholar] [CrossRef]
- Bishop, D.V.M. Pragmatic language impairment: A correlate of SLI, a distinct subgroup, or part of the autistic continuum? In Speech and Language Impairments in Children: Causes, Characteristics, Intervention and Outcome; Bishop, D.V.M., Leonard, L.B., Eds.; Psychology Press: Hove, UK, 2000; pp. 99–113. [Google Scholar]
- Tager-Flusberg, H.; Lord, C.; Paul, R. Language, and communication in autism. In Handbook of Autism and Pervasive Developmental Disorders, 3rd ed.; Volkmar, F., Paul, R., Klin, A., Cohen, D., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2005; pp. 335–364. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Bishop, D.V.M.; Snowling, M.J.; Thompson, P.A.; Greenhalgh, T. Phase 2 of CATALISE: A multinational and multidisciplinary Delphi consensus study of problems with language development: Terminology. J. Child Psychol. Psychiatry 2017, 58, 1068–1080. [Google Scholar] [CrossRef] [PubMed]
- Bishop, D.V.M. Uncommon Understanding: Development and Disorders of Language Comprehension in Children; Psychology Press: Hove, UK, 1997; p. 278. [Google Scholar]
- Roqueta, C.A.; Katsos, N. A distinction between linguistic and social pragmatics helps the precise characterization of pragmatic challenges in children with autism spectrum disorders and developmental language disorder. J. Speech Lang. Her Res. 2020, 63, 1494–1508. [Google Scholar] [CrossRef]
- Spanoudis, G. Theory of mind and Specific Language Impairment in school-age children. J. Commun. Disord. 2016, 61, 83–96. [Google Scholar] [CrossRef] [PubMed]
- Levy, S.E.; Giarelli, E.; Lee, L.C.; Schieve, L.A.; Kirby, R.S.; Cunniff, C.; Nicholas, J.; Reaven, J.; Rice, C.E. Autism spectrum disorder and co-occurring developmental, psychiatric, and medical conditions among children in multiple populations of the United States. J. Dev. Behav. Pediatr. 2010, 31, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Baird, G.; Simonoff, E.; Pickles, A.; Chandler, S.; Loucas, T.; Meldrum, D.; Charman, T. Prevalence of disorders of the autism spectrum in a population cohort of children in South Thames: The Special Needs and Autism Project (SNAP). Lancet 2006, 368, 210–215. [Google Scholar] [CrossRef]
- Tager-Flusberg, H. Language and understanding minds: Connections in autism. In Understanding Other Minds: Perspectives from Developmental Cognitive Neuroscience; Baron-Cohen, S., Tager-Flusberg, H., Cohen, D.J., Eds.; University Press: Oxford, UK, 2000; pp. 124–149. [Google Scholar]
- Whitehouse, A.J.O.; Barry, J.G.; Bishop, D.V.M. Further defining the language impairment of autism: Is there a Specific Language Impairment subtype? J. Commun. Disord. 2008, 41, 319–336. [Google Scholar] [CrossRef]
- Tager-Flusberg, H.; Joseph, R.M. Identifying neurocognitive phenotypes in autism. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2003, 358, 303–314. [Google Scholar] [CrossRef]
- Kjelgaard, M.M.; Tager-Flusberg, H. An investigation of language impairment in autism: Implications for genetic subgroups. Lang. Cogn. Process. 2001, 16, 287–308. [Google Scholar] [CrossRef]
- Roberts, J.A.; Rice, M.L.; Tager-Flusberg, H. Tense marking in children with autism. Appl. Psycholinguist. 2004, 25, 429–448. [Google Scholar] [CrossRef]
- Durrleman, S.; Delage, H. Autism Spectrum Disorder and Specific Language Impairment: Overlaps in Syntactic Profiles. Lang. Acquis. 2016, 23, 361–386. [Google Scholar] [CrossRef]
- Riches, N.G.; Loucas, T.; Baird, G.; Charman, T.; Simonoff, E. Non-word repetition in adolescents with Specific Language Impairment and autism plus language impairments: A qualitative analysis. J. Commun. Disord. 2011, 44, 23–36. [Google Scholar] [CrossRef]
- Bishop, D.V.M. Overlaps between autism and language impairment: Phenomimicry or shared etiology. Behav. Genet. 2010, 40, 618–629. [Google Scholar] [CrossRef] [PubMed]
- Norbury, C.F.; Gooch, D.; Wray, C.; Baird, G.; Charman, T.; Simonoff, E.; Vamvakas, G.; Pickles, A. The impact of nonverbal ability on prevalence and clinical presentation of language disorder: Evidence from a population study. J. Child Psychol. Psychiatry 2016, 11, 1247–1257. [Google Scholar] [CrossRef] [PubMed]
- Leonard, L.B. Children with Specific Language Impairment; MIT Press: Cambridge, UK, 1998. [Google Scholar]
- Montgomery, J.W. Working memory and comprehension in children with specific language impairment: What we know so far. J. Commun. Disord. 2003, 36, 221–231. [Google Scholar] [CrossRef]
- Vugs, B.; Cuperus, J.; Hendriks, M.; Verhoeven, L. Visuospatial working memory in Specific Language Impairment: A meta-analysis. Res. Dev. Disabil. 2013, 34, 2586–2597. [Google Scholar] [CrossRef] [PubMed]
- Henry, L.A.; Messer, D.J.; Nash, G. Executive functioning in children with specific language impairment. J. Child Psychol. Psychiatry 2012, 53, 37–45. [Google Scholar] [CrossRef]
- Bishop, D.V.M.; Snowling, M. Developmental dyslexia and specific language impairment: Same or different? Psychol. Bull. 2004, 130, 858–886. [Google Scholar] [CrossRef]
- Leonard, L.; Caselli, M.C.; Bortolini, U.; McGregor, K.K. Morphological Deficits, in Children with Specific Language Impairment: The Status of Features in the Underlying Grammar. Lang. Acquis. 1992, 2, 151–179. [Google Scholar] [CrossRef]
- Conti-Ramsden, G.; Botting, N.; Simkin, Z.; Knox, E. Follow-up of children attending infant language units: Outcomes at 11 years of age. Int. J. Lang. Commun. Disord. 2001, 36, 207–219. [Google Scholar] [CrossRef]
- Coady, J.; Evans, J.L. Uses and interpretations of nonword repetition tasks in children with and without Specific Language Impairment (SLI). Int. J. Lang. Commun. Disord. 2008, 43, 1–40. [Google Scholar] [CrossRef] [PubMed]
- Rice, M.L.; Wexler, K.; Cleave, P.L. Specific language impairment as a period of extended optional infinitive. J. Speech Lang. Hear. Res. 1995, 38, 850–863. [Google Scholar] [CrossRef] [PubMed]
- Marchman, V.A.; Wulfeck, B.; Ellis-Weismer, S.E. Morphological productivity in children with normal language and SLI: A study of the English past tense. J. Speech Lang. Hear. Res. 1999, 42, 206–219. [Google Scholar] [CrossRef] [PubMed]
- Simkin, Z.; Conti-Ramsden, G. Nonword repetition and grammatical morphology: Normative data for children in their final year of primary school. Int. J. Lang. Commun. Disord. 2001, 36, 395–404. [Google Scholar] [PubMed]
- Oetting, J.B.; McDonald, J.L.; Seidel, C.M.; Hegarty, M. Sentence recall by children with SLI across two mainstream dialects of English. J. Speech Lang. Hear. Res. 2016, 59, 183–194. [Google Scholar] [CrossRef]
- Stokes, S.; Wong, A.; Fletcher, P.; Leonard, L. Nonword Repetition and Sentence Repetition as Clinical Markers of Specific Language Impairment: The Case of Cantonese. J. Speech Lang. Hear. Res. 2006, 49, 219–236. [Google Scholar] [CrossRef]
- Thordardottir, E.; Kehayia, E.; Mazer, B.; Lessard, N.; Majnemer, A.; Sutton, A.; Trudeau, N.; Chilingaryan, G. Sensitivity and specificity of French language and processing measures for the identification of primary language impairment at age 5. J. Speech Lang. Hear. Res. 2011, 54, 580–597. [Google Scholar] [CrossRef]
- Leclercq, A.; Quémart, P.; Magis, D.; Maillart, C. The sentence repetition task: A powerful diagnostic tool for French children with specific language impairment. Res. Dev. Disabil. 2014, 35, 2423–2430. [Google Scholar] [CrossRef]
- Theodorou, E.; Kambanaros, M.; Grohmann, K.K. Sentence Repetition as a Tool for Screening Morphosyntactic Abilities of Bilectal Children with SLI. Front. Psychol. 2017, 8, 1–13. [Google Scholar] [CrossRef]
- Seeff-Gabriel, B.; Chiat, S.; Dodd, B. Sentence imitation as a tool in identifying expressive morphosyntactic difficulties in children with severe speech difficulties. Int. J. Lang. Commun. Disord. 2010, 45, 691–702. [Google Scholar] [CrossRef] [PubMed]
- Girbau, D. The Non-word Repetition Task as a clinical marker of Specific Language Impairment in Spanish-speaking children. First Lang. 2016, 36, 30–49. [Google Scholar] [CrossRef]
- Bortolini, U.; Arfe´, B.; Caselli, M.C.; Degasperi, L.; Deevy, P.; Leonard, L.B. Clinical markers for Specific Language Impairment in Italian: The contribution of clitics and non-word repetition. Int. J. Lang. Commun. Disord. 2006, 41, 695–712. [Google Scholar] [CrossRef] [PubMed]
- Graf Estes, K.; Evans, J.L.; Else-Quest, N.M. Differences in the Nonword Repetition Performance of Children with and Without Developmental Language Disorder: A Meta-Analysis. J. Speech Lang. Hear. Res. 2007, 50, 177–195. [Google Scholar] [CrossRef]
- Bishop, D.V.M.; Donlan, C. Nonword repetition as a behavioural marker for inherited language impairment: Evidence from a twin study. J. Child Psychol. Psychiatry 1996, 37, 391–403. [Google Scholar] [CrossRef] [PubMed]
- Conti-Ramsden, G.; Hesketh, A. Risk markers for SLI: A study of young language-learning children. Int. J. Lang. Commun. Disord. 2003, 38, 251–263. [Google Scholar] [CrossRef] [PubMed]
- Botting, N.; Conti-Ramsden, G. Autism, primary pragmatic difficulties and Specific Language Impairment: Can we distinguish them using psycholinguistic markers? Dev. Med. Child Neurol. 2003, 45, 515–545. [Google Scholar] [CrossRef]
- Bishop, D.V.M.; Chan, J.; Adams, C.; Hartley, J.; Weir, F. Conversational responsiveness in Specific Language Impairment: Evidence of disproportionate pragmatic difficulties in a subset of children. Dev. Psychopathol. 2000, 12, 177–199. [Google Scholar] [CrossRef] [PubMed]
- Friedmann, N.; Novogrodsky, R. Subtypes of Sli: Sysli, Phosli, Lesli, and Prasli. In Language Acquisition and Development; Gavarró, A., Freitas, M.J., Eds.; Cambridge Scholars Press/CSP: Newcastle, UK, 2008; pp. 205–217. [Google Scholar]
- Van der Lely, H.K. SLI in children: Movement, economy, and deficits in the computational-syntactic system. Lang. Acquis. 1998, 7, 161–192. [Google Scholar] [CrossRef]
- Stavrakaki, S. Greek neurolinguistics: The state of the art. J. Greek Linguist. 2005, 6, 187–234. [Google Scholar] [CrossRef]
- Petinou, K.; Terzi, A. Clitic misplacement among normally developing and SLI children and the status of Infl Heads. Lang. Acquis. 2002, 10, 1–28. [Google Scholar] [CrossRef]
- Stavrakaki, S.; Van der Lely, H. Production and comprehension of pronouns by Greek children with specific language impairment. Br. J. Dev. Psychol. 2010, 28, 189–216. [Google Scholar] [CrossRef] [PubMed]
- Stavrakaki, S. Comprehension of reversible relative clauses in specifically language impaired and normally developing Greek children. Brain Lang. 2001, 77, 419–431. [Google Scholar] [CrossRef] [PubMed]
- Stavrakaki, S. Developmental perspectives on Specific Language Impairment: Evidence from the production of wh-questions by Greek SLI children over time. Adv. Speech Lang. Pathol. 2006, 8, 384–396. [Google Scholar] [CrossRef]
- Tsimpli, I.M.; Stavrakaki, S. The effects of a morphosyntactic deficit in the determiner system: The case of a Greek SLI child. Lingua 1999, 108, 31–85. [Google Scholar] [CrossRef]
- Tsimpli, I.M. LF-interpretability and language development: A study of verbal and nominal features in Greek normally developing and SLI children. Brain Lang. 2001, 77, 432–448. [Google Scholar] [CrossRef]
- Theodorou, E.; Grohmann, K.K. Object clitics in Cypriot Greek children with SLI. Lingua 2015, 161, 144–158. [Google Scholar] [CrossRef]
- Manika, S.; Varlokosta, S.; Wexler, K. The lack of omission of clitics in Greek children with SLI: An experimental study. In BUCLD 35: Proceedings of the 35th Boston University Conference on Language Development; Danis, N., Mesh, K., Sung, H., Eds.; Cascadilla Press: Somerville, MA, USA, 2011; pp. 429–437. [Google Scholar]
- Varlokosta, S.; Konstantzou, K.; Nerantzini, M. Clitic production in Greek SLI. In Proceedings of the Conference Specific Language Impairment—Diagnosis, Prognosis, Intervention, Warsaw, Poland, 5–8 July 2012. [Google Scholar]
- Theodorou, E.; Grohmann, K.K. Narratives in Cypriot Greek mono- and bilingual children with SLI. In Proceedings of the 3rd ISCA Workshop Tutorial and Research Workshop on Experimental Linguistics, Athens, Greece, 25–27 August 2010; pp. 185–188. [Google Scholar]
- Spanoudis, G.; Natsopoulos, D.; Panayiotou, G. Mental verbs and pragmatic language difficulties. Int. J. Lang. Commun. Disord. 2007, 42, 487–504. [Google Scholar] [CrossRef]
- Spanoudis, G.; Papadopoulos, T.C.; Spyrou, S. Specific language impairment and dyslexia: Categorical distinction or continuum? J. Learn. Disabil. 2019, 52, 3–14. [Google Scholar] [CrossRef]
- Kanner, L. Irrelevant and metaphorical language in early infantile autism. Am. J. Psychiatry 1946, 103, 242–245. [Google Scholar] [CrossRef]
- Rutter, M. Concepts of autism: A review of research. J. Child Psychol. Psychiatry 1968, 9, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Bartolucci, G.; Albers, R.J. Deictic categories in the language of autistic children. J. Autism Child. Schiz. 1974, 4, 131–141. [Google Scholar] [CrossRef]
- Bartolucci, G.; Pierce, S. A preliminary comparison of phonological development in autistic, normal, and mentally retarded subjects. Br. J. Disord. Commun. 1977, 12, 137–147. [Google Scholar] [CrossRef]
- Bartoclucci, G.; Pierce, S.; Streiner, D.; Eppel, P. Phonological investigation of verbal autistic and mentally retarded subjects. J. Autism Child. Schiz. 1976, 6, 303–315. [Google Scholar] [CrossRef]
- Tager–Flusberg, H.; Calkins, S.; Nolin, T.; Baumberger, T.; Anderson, M.; Chadwick–Dias, A. A longitudinal study of language acquisition in autistic and Downs syndrome children. J. Autism Dev. Disord. 1990, 20, 1–21. [Google Scholar] [CrossRef]
- Tek, S.; Mesite, L.; Fein, D.; Naigles, L. Longitudinal analyses of expressive language development reveal two distinct language profiles among young children with autism spectrum disorders. J. Autism Dev. Disord. 2013, 44, 75–89. [Google Scholar] [CrossRef]
- Gernsbacher, M.A.; Morson, E.M.; Grace, E. Language and Speech in Autism. Annu. Rev. Linguist. 2016, 2, 413–425. [Google Scholar] [CrossRef]
- Tager-Flusberg, H. Defining language phenotype in autism. Clin. Neurosci. Res. 2006, 6, 219–224. [Google Scholar] [CrossRef]
- Boucher, J. Research review: Structural language in autistic spectrum disorder—Characteristics and causes. J. Child Psychol. Psychiatry 2012, 53, 219–233. [Google Scholar] [CrossRef]
- Tager-Flusberg, H.; Caronna, E. Language Disorders: Autism and Other Pervasive Developmental Disorders. Pediatr. Clin. North Am. 2007, 54, 469–481. [Google Scholar] [CrossRef]
- Ellis Weismer, S.; Kover, S.T. Preschool language variation, growth, and predictors in children on the autism spectrum. J. Child Psychol. Psychiatry 2015, 56, 1327–1337. [Google Scholar] [CrossRef] [PubMed]
- Anderson, D.K.; Lord, C.; Risi, S.; DiLavore, P.S.; Shulman, C.; Thurm, A.; Welch, K.; Pickles, A. Patterns of growth in verbal abilities among children with autism spectrum disorder. J. Consult. Clin. Psychol. 2007, 75, 594–604. [Google Scholar] [CrossRef]
- Norrelgen, F.; Fernell, E.; Eriksson, M.; Hedvall, A.; Persson, C.; Sjolin, M.; Gillberg, C.; Kjellmer, L. Children with autism spectrum disorders who do not develop phrase speech in the preschool years. Autism 2014, 19, 934–943. [Google Scholar] [CrossRef]
- Brignell, A.; Morgan, A.; Woolfenden, S.; Klopper, F.; May, T.; Sarkozy, V.; Williams, K. A systematic review and meta-analysis of the prognosis of language outcomes for individuals with autism spectrum disorder. Autism Dev. Lang. Impair. 2018, 3, 1–19. [Google Scholar] [CrossRef]
- Herlihy, L.; Knoch, K.; Vibert, B.; Fein, D. Parents’ first concerns about toddlers with autism spectrum disorder: Effect of sibling status. Autism 2015, 19, 20–28. [Google Scholar] [CrossRef]
- Hudry, K.; Chandler, S.; Bedford, R.; Pasco, G.; Gliga, T.; Elsabbagh, M.; Johnson, M.H.; Charman, T. Early language profiles in infants at high-risk for autism spectrum disorders. J. Autism Dev. Disord. 2014, 44, 154–167. [Google Scholar] [CrossRef]
- Tager-Flusberg, H. A psychological approach to understanding the social and language impairments in autism. Int. Rev. Psychiatry 1999, 11, 325–334. [Google Scholar] [CrossRef]
- Peristeri, E.; Andreou, M.; Tsimpli, I.M. Syntactic and Story Structure Complexity in the Narratives of High- and Low-Language Ability Children with Autism Spectrum Disorder. Front. Psychol. 2017, 8, 2027. [Google Scholar] [CrossRef]
- Terzi, A.; Marinis, T.; Francis, K. The Interface of Syntax with Pragmatics and Prosody in Children with Autism Spectrum Disorders. J. Autism Dev. Disord. 2016, 46, 2692–2706. [Google Scholar] [CrossRef] [PubMed]
- Kambanaros, M.; Christou, N.; Grohmann, K.K. Interpretation of compound words by Greek-speaking children with autism spectrum disorder plus language impairment (ASD–LI). Clin. Linguist. Phon. 2019, 33, 135–174. [Google Scholar] [CrossRef] [PubMed]
- Bishop, D.V.M.; Norbury, C.F. Exploring the borderlands of autistic disorder and Specific Language Impairment: A study using standardized diagnostic instruments. J. Child Psychol. Psychiatry 2002, 43, 917–929. [Google Scholar] [CrossRef] [PubMed]
- Lindgren, K.A.; Folstein, S.E.; Tomblin, J.B.; Tager-Flusberg, H. Language and reading abilities of children with autism spectrum disorders and Specific Language Impairment and their first-degree relatives. Autism Res. 2009, 2, 22–38. [Google Scholar] [CrossRef]
- Lloyd, H.; Paintin, K.; Botting, N. Performance of children with different types of communication impairment on the Clinical Evaluation of Language Fundamentals (CELF). Child Lang. Teach Ther. 2006, 22, 205–223. [Google Scholar] [CrossRef]
- Manolitsi, M.; Botting, N. Language abilities in children with autism and language impairment: Using narrative as an additional source of clinical information. Child Lang. Teach Ther. 2011, 27, 39–55. [Google Scholar] [CrossRef]
- Demouy, J.; Plaza, M.; Xavier, J.; Ringeval, J.; Chetouani, M.; Périsse, D.; Chauvin, D.; Viaux, S.; Golse, B.; Cohen, D.; et al. Differential language markers of pathology in autism, pervasive developmental disorder not otherwise specified and Specific Language Impairment. Res. Autism Spectr. Disord. 2011, 5, 1402–1412. [Google Scholar] [CrossRef]
- McGregor, K.K.; Berns, A.J.; Owen, A.J.; Michels, S.A.; Duff, D.; Bahnsen, A.J.; Lloyd, M. Associations between syntax and the lexicon among children with or without ASD and language impairment. J. Autism Dev. Disord. 2012, 42, 35–47. [Google Scholar] [CrossRef]
- Tuller, L.; Ferré, S.; Prévost, P.; Barthez, M.; Malvy, J.; Bonnet-Brilhault, F. The effect of computational complexity on the acquisition of French by children with ASD. In Innovative Investigations of Language in Autism Spectrum Disorder; Naigles, L., Ed.; Walter de Gruyter: Washington, DC, USA, 2017; pp. 115–140. [Google Scholar]
- Ramírez-Santana, G.M.; Acosta-Rodríguez, V.M.; Hernández-Expósito, S.A. Comparative study of language phenotypes in Autism Spectrum Disorder and Developmental Language Disorder. Psicothema 2019, 31, 437–442. [Google Scholar]
- Gladfelter, A.; Barron, K.L. How Children with Autism Spectrum Disorder, Specific Language Impairment, and Typical Language Learn to Produce Global and Local Semantic Features. Brain Sci. 2020, 10, 231. [Google Scholar] [CrossRef]
- Modyanova, N.; Perovic, A.; Wexler, K. Grammar is differentially impaired in subgroups of autism spectrum disorders: Evidence from an investigation of tense marking and morphosyntax. Front. Psychol. 2017, 8, 1–23. [Google Scholar] [CrossRef]
- Ellis Weismer, S.; Davidson, M.M.; Gangopadhyay, I.; Sindberg, H.; Roebuck, H.; Kaushanskaya, M. The role of nonverbal working memory in morphosyntactic processing by children with specific language impairment and autism spectrum disorders. J. Neurodev. Disord. 2017, 9, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Schaeffer, J.; Van Witteloostuijn, M.; Creemers, A. Article choice, theory of mind, and memory in children with high-functioning autism and children with Specific Language Impairment. Appl. Psycholinguist. 2018, 39, 89–115. [Google Scholar] [CrossRef]
- Norbury, C.F.; Gemmell, T.; Paul, R. Pragmatics abilities in narrative production: A cross-disorder comparison. J. Child Lang. 2014, 41, 485–510. [Google Scholar] [CrossRef]
- Conti-Ramsden, G.; Simkin, Z.; Pickles, A. Estimating familial loading in SLI: A comparison of direct assessment versus parental interview. J. Speech Lang. Hear. Res. 2006, 49, 88–101. [Google Scholar] [CrossRef]
- Leyfer, O.T.; Tager-Flusberg, H.; Dowd, M.; Tomblin, J.B.; Folstein, S.E. Overlap between autism and Specific Language Impairment: Comparison of Autism Diagnostic Interview and Autism Diagnostic Observation Schedule scores. Autism Res. 2008, 1, 284–296. [Google Scholar] [CrossRef]
- Howlin, P.; Mawhood, L.; Rutter, M. Autism and developmental receptive language disorder—A follow-up comparison in early adult life II: Social, behavioural, and psychiatric outcomes. J. Child Psychol. Psychiatry 2000, 41, 561–578. [Google Scholar] [CrossRef]
- Mawhood, L.; Howlin, P.; Rutter, M. Autism and developmental receptive language disorder—A comparative follow-up in early adult life. I: Cognitive and language outcomes. J. Child Psychol. Psychiatry 2000, 41, 547–559. [Google Scholar] [CrossRef]
- Whitehouse, A.J.O.; Barry, J.G.; Bishop, D.V.M. The broader language phenotype of autism: A comparison with Specific Language Impairment. J. Child Psychol. Psychiatry 2007, 48, 822–830. [Google Scholar] [CrossRef]
- Loucas, T.; Riches, N.; Baird, G.; Pickles, A.; Simonoff, E.; Chandler, S.; Charman, T. Spoken word recognition in adolescents with autism spectrum disorders and Specific Language Impairment. Appl. Psycholinguist. 2013, 34, 301–322. [Google Scholar] [CrossRef]
- Sukenik, N.; Friedmann, N. ASD is not DLI: Individuals with autism and individuals with syntactic DLI show similar performance level in syntactic tasks, but different error patterns. Front. Psychol. 2018, 9, 279. [Google Scholar] [CrossRef]
- Creemers, A.; Schaeffer, J.C. Specific language impairment and high functioning autism: Evidence for distinct etiologies and for modularity of grammar and pragmatics. In Proceedings of the 6th Conference on Generative Approaches to Language Acquisition North America (GALANA 2015), University of Maryland, College Park, MD, USA, 19–21 February 2015; Perkins, L., Dudley, R., Gerard, J., Hitczenko, K., Eds.; Cascadilla Proceedings Project: Somerville, MA, USA, 2016; pp. 1–12. [Google Scholar]
- Balaban, N.; Friedmann, N.; Ariel, M. The effect of theory of mind impairment on language: Referring after right hemisphere damage. Aphasiology 2016, 30, 1424–1460. [Google Scholar] [CrossRef]
- Schaeffer, J. Linguistic and cognitive abilities in children with specific language impairment as compared to children with high-functioning autism. Lang. Acquis. 2016, 25, 5–23. [Google Scholar] [CrossRef]
- Hudry, K.; Leadbitter, K.; Temple, K.; Slonims, V.; McConachie, H.; Aldred, C.; Howlin, P.; Charman, T.; PACT Consortium. Preschoolers with autism show greater impairment in receptive compared with expressive language abilities. Int. J. Lang. Commun. Disord. 2010, 45, 681–690. [Google Scholar] [CrossRef]
- Taylor, L.J.; Whitehouse, A.J.O. Autism Spectrum Disorder, Language Disorder, and Social (Pragmatic) Communication Disorder: Overlaps, Distinguishing Features, and Clinical Implications. Aust. Psychol. 2016, 51, 287–295. [Google Scholar] [CrossRef]
- Whitehouse, A.J.O.; Line, E.A.; Watt, H.J.; Bishop, D.V.M. Qualitative aspects of developmental language impairment relate to language and literacy outcome in adulthood. Int. J. Lang. Commun. Disord. 2009, 44, 489–510. [Google Scholar] [CrossRef]
- Spanoudis, G.; Pahiti, J. Expressive and Receptive Language Evaluation: 5–12 Years of Age; Department of Psychology, University of Cyprus: Nicosia, Cyprus, 2014. [Google Scholar]
- Bishop, D.V.M. Children’s Communication Checklist, 2nd ed.; The Psychological Corporation: New York, NY, USA, 2003. [Google Scholar]
- Lord, C.; Rutter, M.; DiLavore, P.C.; Risi, S.; Gotham, K.; Bishop, S. Autism Diagnostic Observation Schedule, 2nd ed.; Western Psychological Services: Torrance, CA, USA, 2012. [Google Scholar]
- Wechsler, D. Wechsler Intelligence Scale for Children, 1st ed.; The Psychological Corporation: London, UK, 1999. [Google Scholar]
- Anns, S. The Role of Declarative Memory in the Acquisition of Conceptual Semantic Knowledge in Autism Spectrum Disorder. Ph.D. Thesis, University of London, London, UK, 2016; pp. 1–242. [Google Scholar]
- Reilly, S.; Tomblin, B.; Law, J.; McKean, C.; Mensah, F.K.; Morgan, A.; Goldfeld, S.; Nicholson, J.M.; Wake, M. Specific language impairment: A convenient label for whom? Int. J. Lang. Commun. Disord. 2014, 49, 416–451. [Google Scholar] [CrossRef]
- McGregor, K.; Goffman, L.; Owen Van Horne, A.; Hogan, T.; Finestack, L. Developmental Language Disorder: Applications for Advocacy, Research, and Clinical Service. Perspect. ASHA Spec. Interest Groups 2020, 5, 38–46. [Google Scholar] [CrossRef]
- Semel, E.; Wiig, E.; Secord, W. Clinical Evaluation of Language Fundamentals-3; The Psychological Corporation: San Antonio, TX, USA, 1995. [Google Scholar]
- Spanoudis, G.; Natsopoulos, D. Memory functioning and mental verbs acquisition in children with Specific Language Impairment. Res. Dev. Disabil. 2011, 32, 2916–2926. [Google Scholar] [CrossRef]
- Glarou, E. Adaptation of Children’s Communication Checklist-2 (CCC-2; Bishop, 2003) in Greek Language and Implementation in Parents of 4-7 Years Old Children. Unpublished. Undergraduate Thesis, University of Patra, Patra, Greece, 2015; pp. 1–102. [Google Scholar]
- Norbury, C.; Nash, M.; Baird, G.; Bishop, D.V.M. Using a parental checklist to identify diagnostic groups in children with communication impairment: A validation of the Children’s Communication Checklist—2. Int. J. Lang. Commun. Disord. 2004, 39, 345–364. [Google Scholar] [CrossRef] [PubMed]
- Bishop, D.V.M.; Maybery, M.; Wong, D.; Maley, A.; Hallmayer, J. Characteristics of the broader phenotype in autism: A study of siblings using the Children’s Communication Checklist—2. Am. J. Med. Genet. B. 2006, 141B, 117–122. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods. 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Singer, J.D.; Willett, J.B. Applied Longitudinal Data Analysis: Modeling Change and Event Occurrence; Oxford University Press: New York, NY, USA, 2003. [Google Scholar]
- Collins, L.M. Analysis of longitudinal data: The integration of theoretical model, temporal design, and statistical model. Annu. Rev. Psychol. 2006, 57, 505–528. [Google Scholar] [CrossRef] [PubMed]
- Hox, J. Multilevel Analysis: Techniques and Applications; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2002. [Google Scholar]
- Tager-Flusberg, H. Defining language impairments in a subgroup of children with autism spectrum disorder. Sci. China Life Sci. 2015, 58, 1044–1052. [Google Scholar] [CrossRef] [PubMed]
- De Fossé, L.; Hodge, S.M.; Makris, N.; Kennedy, D.N.; Caviness, V.S., Jr.; McGrath, L.; Steele, S.; Ziegler, D.A.; Herbert, M.R.; Frazier, J.A.; et al. Language-association cortex asymmetry in autism and specific language impairment. Ann. Neurol. 2004, 56, 757–766. [Google Scholar] [CrossRef]
- Williams, D.; Payne, H.; Marshall, C. Non-word Repetition Impairment in Autism and Specific Language Impairment: Evidence for Distinct Underlying Cognitive Causes. J. Autism Dev. Disord. 2013, 43, 404–417. [Google Scholar] [CrossRef] [PubMed]
- Loucas, T.; Charman, T.; Pickles, A.; Simonoff, E.; Chandler, S.; Meldrum, D.; Baird, G. Autistic symptomatology and language ability in Autism Spectrum Disorder and Specific Language Impairment. J. Child Psychol. Psychiatry 2008, 49, 1184–1192. [Google Scholar] [CrossRef]
- Conti-Ramsden, G.; Crutchley, A.; Botting, N. The extent to Which Psychometric Tests Differentiate Subgroups of Children with SLI. J. Speech Lang. Hear. Res. 1997, 40, 765–777. [Google Scholar] [CrossRef] [PubMed]
- Capps, L.; Kehres, J.; Sigman, M. Conversational abilities among children with autism and children with developmental delays. Autism. 1998, 2, 325–344. [Google Scholar] [CrossRef]
- Tager-Flusberg, H. Current theory and research on language and communication in autism. J. Autism Dev. Disord. 1996, 26, 169–172. [Google Scholar] [CrossRef]
- Tager-Flusberg, H.; Cooper, J. Present and future possibilities for defining a phenotype for specific language impairment. J. Speech Lang. Hear. Res. 1999, 42, 1001–1004. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | CFD | WS | RS | FS | WC | NWR | SIDC | GCC |
|---|---|---|---|---|---|---|---|---|
| CFD | — | |||||||
| WS | 0.632 ** | — | ||||||
| RS | 0.712 ** | 0.698 ** | — | |||||
| FS | 0.806 ** | 0.741 ** | 0.891 ** | — | ||||
| WC | 0.328 | — | 0.184 | 0.425 | — | |||
| NWR | 0.679 ** | 0.674 ** | 0.662 ** | 0.694 ** | 0.393 | — | ||
| SIDC | −0.101 | 0.026 | −0.149 | −0.055 | −0.195 | −0.177 | — | |
| GCC | 0.172 | 0.208 | 0.342 ** | 0.123 | 0.139 | 0.206 | −0.324 | — |
| ASD (n = 16) | ASD-LI (n = 24) | DLD (n = 28) | TD (n = 35) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Range | Mean | SD | Range | Mean | SD | Range | Mean | SD | Range | |
| Age | 108.81 | 23.33 | 73–140 | 78.29 | 6.85 | 72–99 | 97.21 | 19.98 | 72–193 | 105.71 | 23.79 | 72–144 |
| IQ Total | 92.38 | 10.56 | 85–126 | 86.88 | 5.36 | 80–103 | 90.18 | 9.54 | 71–111 | 96.43 | 8.8 | 76–113 |
| CFD | 37.69 | 7.41 | 24–51 | 17.04 | 5.44 | 8–29 | 24.79 | 9.89 | 6–48 | 40.37 | 8.33 | 25–52 |
| WS | 14.57 | 5.16 | 9–22 | 10.46 | 4.25 | 4–21 | 12.2 | 6.09 | 0–27 | 18.06 | 3.4 | 14–23 |
| FS | 22.31 | 11.66 | 4–44 | 9 | 6.49 | 0–24 | 16.61 | 8.74 | 0–32 | 29.51 | 10.71 | 9–49 |
| RS | 39.13 | 17.47 | 3–68 | 18.33 | 10.31 | 0–43 | 30.82 | 16.08 | 0–56 | 45.89 | 12.43 | 15–69 |
| WC | 18.33 | 9.06 | 4–36 | - | - | 12.75 | 5.47 | 8–25 | 23.16 | 6.32 | 8–35 | |
| ASD (n = 16) | ASD-LI (n = 24, girls = 1) | DLD (n = 28, girls = 10) | TD (n = 35, girls = 11) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Range | Mean | SD | Range | Mean | SD | Range | Mean | SD | Range | |
| Age * | 108.81 | 23.33 | 73–140 | 78.29 | 6.85 | 72–99 | 97.21 | 19.98 | 72–193 | 105.71 | 23.79 | 72–144 |
| IQ-Total | 92.38 | 10.56 | 85–126 | 86.88 | 5.36 | 80–103 | 90.18 | 9.54 | 71–111 | 96.43 | 8.8 | 76–113 |
| SES | 1.56 | 0.51 | 1–2 | 1.58 | 0.50 | 1–2 | 1.61 | 0.50 | 1–2 | 1.60 | 0.50 | 1–2 |
| EducM | 1.75 | 0.58 | 1–3 | 1.79 | 0.78 | 1–3 | 1.68 | 0.72 | 1–3 | 1.71 | 0.72 | 1–3 |
| EducF | 1.63 | 0.72 | 1–3 | 1.80 | 0.88 | 1–4 | 1.67 | 0.68 | 1–3 | 1.44 | 0.56 | 1–3 |
| Measure | ICC | CI |
|---|---|---|
| Language Domain | ||
| NWR | 0.36 | 1.827–9.694 |
| CFD | 0.57 | 17.883–42.053 |
| WS | 0.24 | 10.053–17.516 |
| RS | 0.34 | 20.438–46.656 |
| FS | 0.37 | 9.746–28.988 |
| WC | 0.23 | 11.253–25.089 |
| GCC | 0.27 | 33.032–67.143 |
| SIDC | 0.11 | 2.585–13.449 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Georgiou, N.; Spanoudis, G. Developmental Language Disorder and Autism: Commonalities and Differences on Language. Brain Sci. 2021, 11, 589. https://doi.org/10.3390/brainsci11050589
Georgiou N, Spanoudis G. Developmental Language Disorder and Autism: Commonalities and Differences on Language. Brain Sciences. 2021; 11(5):589. https://doi.org/10.3390/brainsci11050589
Chicago/Turabian StyleGeorgiou, Natasa, and George Spanoudis. 2021. "Developmental Language Disorder and Autism: Commonalities and Differences on Language" Brain Sciences 11, no. 5: 589. https://doi.org/10.3390/brainsci11050589
APA StyleGeorgiou, N., & Spanoudis, G. (2021). Developmental Language Disorder and Autism: Commonalities and Differences on Language. Brain Sciences, 11(5), 589. https://doi.org/10.3390/brainsci11050589