
Antisocial Personality Problems in Emerging Adulthood: The Role of Family Functioning, Impulsivity, and Empathy




Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Recruitment and Procedure
2.2. Measures
2.2.1. Assessment of Antisocial Personality Problems of Emerging Adults
2.2.2. Assessment of Family Functioning of Emerging Adults
2.2.3. Assessment of Impulsivity of Emerging Adults
2.2.4. Assessment of Empathy of Emerging Adults
2.3. Statistical Analyses
3. Results
3.1. Sample Characteristics
3.2. Bivariate Associations between Study Variables
3.3. Main Effects of Family Functioning, Impulsivity, and Empathy on Antisocial Personality Problems
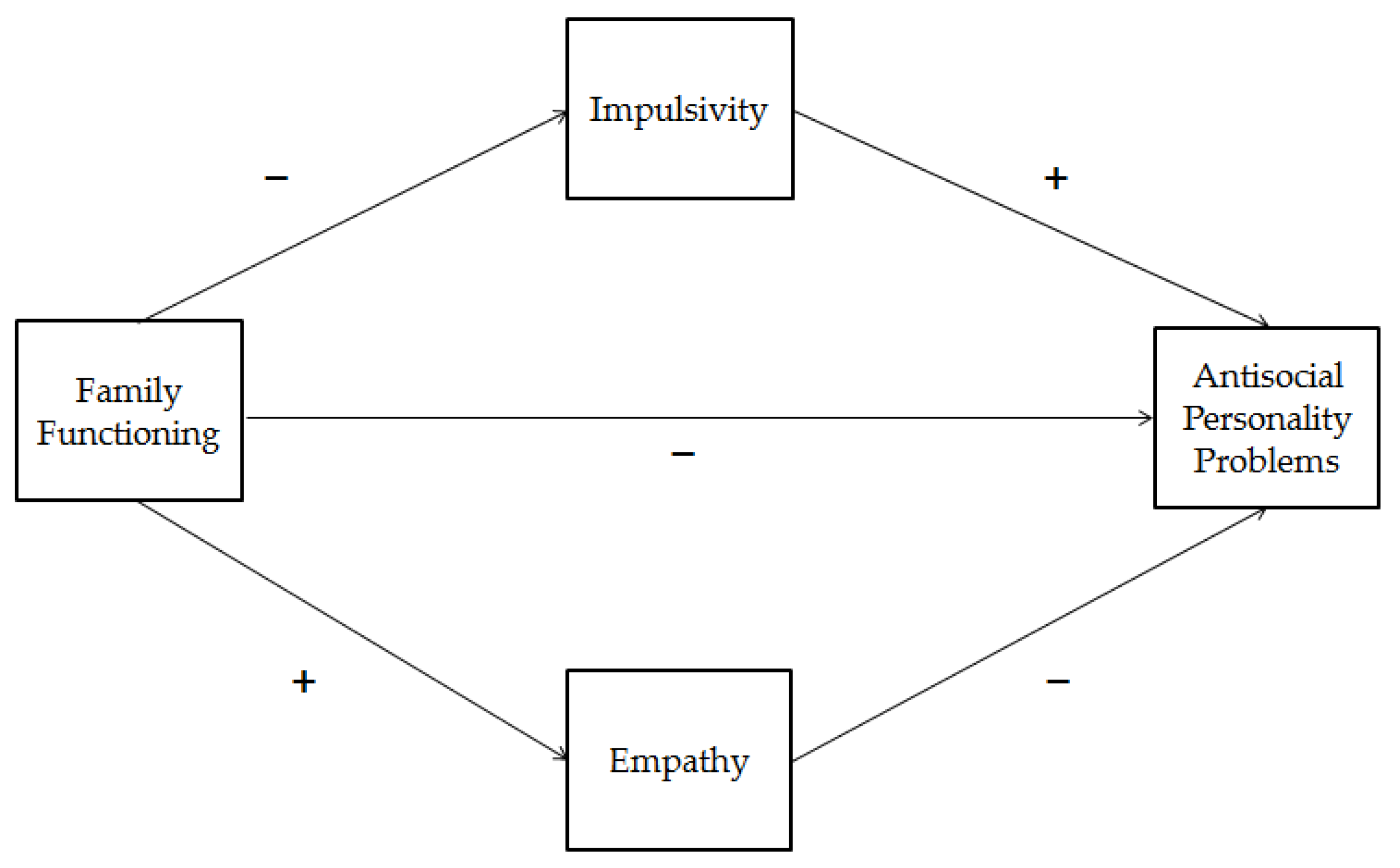
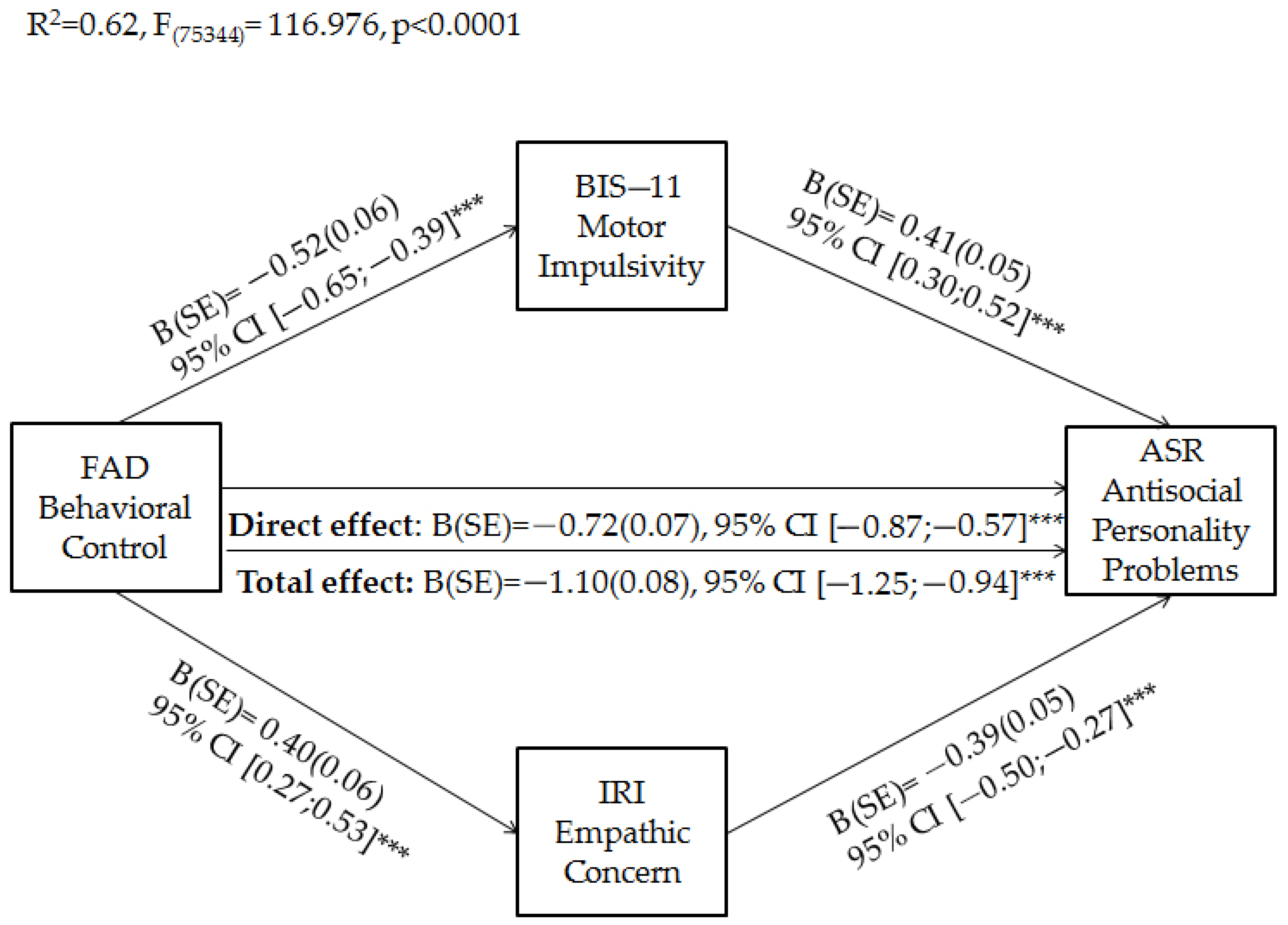
3.4. Emerging Adults’ Impulsivity and Empathy as Mediators of the Relationship between Family Functioning and Antisocial Personality Problems
4. Discussion
Limitation, Strength, and Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Raine, A. Antisocial Personality as a Neurodevelopmental Disorder. Annu. Rev. Clin. Psychol. 2018, 14, 259–289. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5); American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Delk, L.A.; Spangler, D.P.; Guerra, R.; Ly, V.; White, B.A. Antisocial Behavior: The Impact of Psychopathic Traits, Heart Rate Variability, and Gender. J. Psychopathol. Behav. Assess. 2020, 42, 637–646. [Google Scholar] [CrossRef]
- Rafiey, H.; Alipour, F.; Lebeau, R.; Salimi, Y. Development and Validation of the Antisocial Traits Scale in the General Population. Crim. Justice Behav. 2020, 47, 369–380. [Google Scholar] [CrossRef]
- Hammerton, G.; Mahedy, L.; Murray, J.; Maughan, B.; Edwards, A.C.; Kendler, K.S.; Hickman, M.; Heron, J. Effects of Excessive Alcohol Use on Antisocial Behavior Across Adolescence and Early Adulthood. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 857–865. [Google Scholar] [CrossRef] [Green Version]
- Foster, E.M.; Jones, D.E. The high costs of aggression: Public expenditures resulting from conduct disorder. J. Public Health 2005, 95, 1767–1772. [Google Scholar] [CrossRef]
- Nock, M.K.; Kazdin, A.E.; Hiripi, E.; Kessler, R.C. Prevalence, subtypes, and correlates of DSM-IV conduct disorder in the National Comorbidity Survey Replication. Psychol. Med. 2006, 36, 699–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Werner, K.B.; Few, L.R.; Bucholz, K.K. Epidemiology, comorbidity, and behavioral genetics of antisocial personality disorder and psychopathy. Psychiat. Ann. 2015, 45, 195–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livesley, W.J.; Larstone, R. Handbook of Personality Disorders: Theory, Research, and Treatment; Guilford Press: New York, NY, USA, 2018. [Google Scholar]
- Wallace, G.L.; Shaw, P.; Lee, N.R.; Clasen, L.S.; Raznahan, A.; Lenroot, R.K.; Martin, A.; Giedd, J.N. Distinct cortical correlates of autistic versus antisocial traits in a longitudinal sample of typically developing youth. J. Neurosci. 2012, 32, 4856–4860. [Google Scholar] [CrossRef] [PubMed]
- Morgado, A.M.; da Luz Vale-Dias, M. The antisocial phenomenon in adolescence: What is literature telling us? Aggress. Violent Behav. 2013, 18, 436–443. [Google Scholar] [CrossRef]
- Moffitt, T.E. Male antisocial behaviour in adolescence and beyond. Nat. Hum. Behav. 2018, 2, 177–186. [Google Scholar] [CrossRef]
- Nasaescu, E.; Zych, I.; Ortega-Ruiz, R.; Farrington, D.P.; Llorent, V.J. Longitudinal patterns of antisocial behaviors in early adolescence: A latent class and latent transition analysis. Eur. J. Psychol. Appl. Leg. Context 2020, 12, 85–92. [Google Scholar] [CrossRef]
- Johnson, J.G.; Cohen, P.; Chen, H.; Kasen, S.; Brook, J.S. Parenting behaviors associated with risk for offspring personality disorder during adulthood. Arch. Gen. Psychiatry 2006, 63, 579–587. [Google Scholar] [CrossRef]
- Harris-McKoy, D.; Cui, M. Parental control, adolescent delinquency, and young adult criminal behavior. J. Child Fam. Stud. 2013, 22, 836–843. [Google Scholar] [CrossRef]
- Johnson, W.L.; Giordano, P.C.; Longmore, M.A.; Manning, W.D. Parents, identities, and trajectories of antisocial behavior from adolescence to young adulthood. J. Dev. Life Course Criminol. 2016, 2, 442–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blonigen, D.M.; Littlefield, A.K.; Hicks, B.M.; Sher, K.J. Course of Antisocial Behavior during Emerging Adulthood: Developmental Differences in Personality. J. Res. Pers. 2010, 44, 729–733. [Google Scholar] [CrossRef] [Green Version]
- Arnett, J.J. Emerging adulthood. A theory of development from the late teens through the twenties. Am. Psychol. 2000, 55, 469–480. [Google Scholar] [CrossRef]
- Polek, E.; Jones, P.B.; Fearon, P.; Brodbeck, J.; Moutoussis, M.; Dolan, R.; Fonagy, P.; Bullmore, E.T.; Goodyer, I.M. Personality dimensions emerging during adolescence and young adulthood are underpinned by a single latent trait indexing impairment in social functioning. BMC Psychiatry 2018, 26, 18–23. [Google Scholar] [CrossRef] [Green Version]
- Hyde, L.W.; Waller, R.; Shaw, D.S.; Murray, L.; Forbes, E.E. Deflections from adolescent trajectories of antisocial behavior: Contextual and neural moderators of antisocial behavior stability into emerging adulthood. J. Child Psychol. Psychiatry 2018, 59, 1073–1082. [Google Scholar] [CrossRef] [PubMed]
- Moffitt, T.E. Adolescence-limited and life-course-persistent antisocial behavior: A developmental taxonomy. Psychol. Rev. 1993, 100, 674–701. [Google Scholar] [CrossRef] [PubMed]
- Diamantopoulou, S.; Verhulst, F.C.; van der Ende, J. Testing developmental pathways to antisocial personality problems. J. Abnorm. Child Psychol. 2010, 38, 91–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikolajewski, A.J.; Bobadilla, L.; Taylor, J. Antisocial Personality Disorder. In Encyclopedia of Adolescence; Levesque, R.J.R., Ed.; Springer: New York, NY, USA, 2016; pp. 1–13. [Google Scholar]
- Kazemian, L. Desistence from crime: Theoretical, empirical, methodological, and policy considerations. J. Contemp. Crim. Justice 2007, 23, 5–27. [Google Scholar] [CrossRef]
- Wood, D.; Crapnell, T.; Lau, L.; Bennett, A.; Lotstein, D.; Ferris, M.; Kuo, A. Emerging adulthood as a critical stage in the life course. In Handbook of Life Course Health Development; Halfon, N., Forrest, C.B., Lerner, R.M., Faustman, E.M., Eds.; Springer: Cham, Switzerland, 2018; pp. 123–143. [Google Scholar]
- Frick, P.J.; Viding, E. Antisocial behavior from a developmental psychopathology perspective. Dev. Psychopathol. 2009, 21, 1111–1131. [Google Scholar] [CrossRef]
- Rhule-Louie, D.M.; McMahon, R.J. Problem behavior and romantic relationships: Assortative mating, behavior contagion, and desistance. Clin. Child Fam. Psychol. Rev. 2007, 10, 53–100. [Google Scholar] [CrossRef]
- Monahan, K.C.; Steinberg, L.; Cauffman, E. Age differences in the impact of employment on antisocial behavior. Child Dev. 2013, 84, 791–801. [Google Scholar] [CrossRef] [PubMed]
- Burt, S.A.; Donnellan, M.B.; Humbad, M.N.; Hicks, B.M.; McGue, M.; Iacono, W.G. Does marriage inhibit antisocial behavior? An examination of selection vs causation via a longitudinal twin design. Arch. Gen. Psychiatry 2010, 67, 1309–1315. [Google Scholar] [CrossRef] [PubMed]
- Arnett, J.J. The Oxford Handbook of Emerging Adulthood; Oxford University Press: New York, NY, USA, 2016. [Google Scholar]
- Fingerman, K.L.; Yahirun, J.J. Emerging adulthood in the context of family. In The Oxford Handbook of Emerging Adulthood; Arnett, J.J., Ed.; Oxford University Press: New York, NY, USA, 2016; pp. 163–176. [Google Scholar]
- Lee, C.Y.S.; Goldstein, S.E. Loneliness, stress, and social support in young adulthood: Does the source of support matter? J. Youth Adolesc. 2016, 45, 568–580. [Google Scholar] [CrossRef] [PubMed]
- Parra, Á.; Sánchez-Queija, I.; García-Mendoza, M.D.C.; Coimbra, S.; Egídio Oliveira, J.; Díez, M. Perceived parenting styles and adjustment during emerging adulthood: A cross-national perspective. Int. J. Environ. Res. Public Health 2019, 16, 2757. [Google Scholar] [CrossRef] [Green Version]
- Hassan, T.; Alam, M.M.; Wahab, A.; Hawlader, M.D. Prevalence and associated factors of internet addiction among young adults in Bangladesh. J. Egypt Public Health Assoc. 2020, 95, 3. [Google Scholar] [CrossRef]
- Hoskins, D.H. Consequences of parenting on adolescent outcomes. Societie 2014, 4, 506–531. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Fuentes, M.D.C.; Molero Jurado, M.D.M.; Barragán Martín, A.B.; Gázquez Linares, J.J. Family functioning, emotional intelligence, and values: Analysis of the relationship with aggressive behavior in adolescents. Int. J. Environ. Res. Public Health 2019, 16, 478. [Google Scholar] [CrossRef] [Green Version]
- Hawi, N.S.; Samaha, M. Relationships among smartphone addiction, anxiety, and family relations. Behav. Inf. Technol. 2017, 36, 1046–1052. [Google Scholar] [CrossRef]
- Pereira-Morales, A.J.; Adan, A.; Camargo, A.; Forero, D.A. Substance use and suicide risk in a sample of young Colombian adults: An exploration of psychosocial factors. Am. J. Addict. 2017, 26, 388–394. [Google Scholar] [CrossRef]
- Marzilli, E.; Cerniglia, L.; Ballarotto, G.; Cimino, S. Internet Addiction among Young Adult University Students: The Complex Interplay between Family Functioning, Impulsivity, Depression, and Anxiety. Int. J. Environ. Res. Public Health 2020, 17, 8231. [Google Scholar] [CrossRef]
- Ju, C.; Wu, R.; Zhang, B.; You, X.; Luo, Y. Parenting style, coping efficacy, and risk-taking behavior in Chinese young adults. J. Pacific. Rim. Psychol. 2020, 14, E3. [Google Scholar] [CrossRef] [Green Version]
- Marzilli, E.; Ballarotto, G.; Cimino, S.; Cerniglia, L. Motor vehicle collisions in adolescence: The role of family support. [Incidenti stradali in adolescenza: Il ruolo del supporto genitoriale]. Rass. Psicol. 2018, 34, 17–28. [Google Scholar]
- Asano, R.; Yoshizawa, H.; Yoshida, T.; Harada, C.; Tamai, R.; Yoshida, T. Effects of parental parenting attitudes on adolescents’ socialization via adolescents’ perceived parenting. Jpn. J. Psychol. 2016, 87, 284–293. [Google Scholar] [CrossRef] [Green Version]
- Pinquart, M. Associations of parenting dimensions and styles with externalizing problems of children and adolescents: An updated meta-analysis. Dev. Psychol. 2017, 53, 873–932. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-García, D.; González-Castro, P.; Núñez, J.C.; Rodríguez, C.; Cerezo, R. Impact of family and friends on antisocial adolescent behavior: The mediating role of impulsivity and empathy. Front. Psychol. 2019, 10, 2071. [Google Scholar] [CrossRef] [PubMed]
- Inguglia, C.; Costa, S.; Ingoglia, S.; Cuzzocrea, F.; Liga, F. The role of parental control and coping strategies on adolescents’ problem behaviors. Curr. Psychol. 2020, 1–14. [Google Scholar] [CrossRef]
- Lee, J.Y.; Brook, J.S.; Finch, S.J.; Brook, D.W. An adverse family environment during adolescence predicts marijuana use and antisocial personality disorder in adulthood. J. Child Fam. Stud. 2016, 25, 661–668. [Google Scholar] [CrossRef] [Green Version]
- Shen, J.J.; Cheah, C.S.L.; Yu, J. Asian American and European American emerging adults’ perceived parenting styles and self-regulation ability. Asian Am. J. Psychol. 2018, 9, 140–148. [Google Scholar] [CrossRef]
- Fossati, A.; Barratt, E.S.; Carretta, I.; Leonardi, B.; Grazioli, F.; Maffei, C. Predicting borderline and antisocial personality disorder features in nonclinical subjects using measures of impulsivity and aggressiveness. Psychiatry Res. 2004, 125, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Fossati, A.; Barratt, E.S.; Borroni, S.; Villa, D.; Grazioli, F.; Maffei, C. Impulsivity, aggressiveness, and DSM-IV personality disorders. Psychiatry Res. 2007, 149, 157–167. [Google Scholar] [CrossRef]
- Jones, S.E.; Miller, J.D.; Lynam, D.R. Personality, antisocial behavior, and aggression: A meta-analytic review. J. Crim. Justice 2011, 39, 329–337. [Google Scholar] [CrossRef]
- Maneiro, L.; Gómez-Fraguela, J.A.; Cutrín, O.; Romero, E. Impulsivity traits as correlates of antisocial behaviour in adolescents. Pers. Individ. Dif. 2017, 104, 417–422. [Google Scholar] [CrossRef]
- Schmits, E.; Glowacz, F. Delinquency and drug use among adolescents and emerging adults: The role of aggression, impulsivity, empathy, and cognitive distortions. J. Subst. Use 2019, 24, 162–169. [Google Scholar] [CrossRef]
- Van Langen, M.A.; Wissink, I.B.; Van Vugt, E.S.; Van der Stouwe, T.; Stams, G.J.J.M. The relation between empathy and offending: A meta-analysis. Aggress. Violent Behav. 2014, 19, 179–189. [Google Scholar] [CrossRef]
- Velotti, P.; Garofalo, C.; Dimaggio, G.; Fonagy, P. Mindfulness, alexithymia, and empathy moderate relations between trait aggression and antisocial personality disorder traits. Mindfulness 2019, 10, 1082–1090. [Google Scholar] [CrossRef]
- Garofalo, C.; Velotti, P.; Callea, A.; Popolo, R.; Salvatore, G.; Cavallo, F.; Dimaggio, G. Emotion dysregulation, impulsivity and personality disorder traits: A community sample study. Psychiatry Res. 2018, 266, 186–192. [Google Scholar] [CrossRef]
- Rhee, S.H.; Woodward, K.; Corley, R.P.; du Pont, A.; Friedman, N.P.; Hewitt, J.K.; Hink, L.K.; Robinson, J.; Zahn-Waxler, C. The association between toddlerhood empathy deficits and antisocial personality disorder symptoms and psychopathy in adulthood. Dev. Psychopathol. 2021, 33, 173–183. [Google Scholar] [CrossRef]
- Moeller, F.G.; Barratt, E.S.; Dougherty, D.M.; Schmitz, J.M.; Swann, A.C. Psychiatric aspects of impulsivity. Am. J. Psychiatry 2001, 158, 1783–1793. [Google Scholar] [CrossRef] [PubMed]
- Massey, S.H.; Newmark, R.L.; Wakschlag, L.S. Explicating the role of empathic processes in substance use disorders: A conceptual framework and research agenda. Drug Alcohol. Rev. 2018, 37, 316–332. [Google Scholar] [CrossRef] [PubMed]
- Fossati, A.; Gratz, K.L.; Maffei, C.; Borroni, S. Emotion dysregulation and impulsivity additively predict borderline personality disorder features in Italian nonclinical adolescents. Pers. Ment. Health 2013, 7, 320–333. [Google Scholar] [CrossRef] [PubMed]
- Komarovskaya, I.; Loper, A.B.; Warren, J. The role of impulsivity in antisocial and violent behavior and personality disorders among incarcerated women. Crim. Justice Behav. 2007, 34, 1499–1515. [Google Scholar] [CrossRef] [Green Version]
- Umut, G.; Evren, C.; Alniak, I.; Karabulut, V.; Cetin, T.; Agachanli, R.; Evren, B. Relationship between impulsivity and antisocial personality disorder, severity of psychopathology and novelty seeking in a sample of inpatients with heroin use disorder. Heroin Addict. Relat. Clin. Probl. 2017, 19, 65–72. [Google Scholar]
- Urben, S.; Habersaat, S.; Suter, M.; Pihet, S.; De Ridder, J.; Stéphan, P. Gender differences in at risk versus offender adolescents: A dimensional approach of antisocial behavior. Psychiatr. Q 2016, 87, 619–631. [Google Scholar] [CrossRef]
- Martin, S.; Zabala, C.; Del-Monte, J.; Graziani, P.; Aizpurua, E.; Barry, T.J.; Ricarte, J. Examining the relationships between impulsivity, aggression, and recidivism for prisoners with antisocial personality disorder. Aggress. Violent Behav. 2019, 49, 101314. [Google Scholar] [CrossRef]
- Grant, J.E.; Chamberlain, S.R. Obsessive compulsive personality traits: Understanding the chain of pathogenesis from health to disease. J. Psychiatr. Res. 2019, 116, 69–73. [Google Scholar] [CrossRef]
- Ryan, S.R.; Friedman, C.K.; Liang, Y.; Lake, S.L.; Mathias, C.W.; Charles, N.E.; Acheson, A.; Dougherty, D.M. Family Functioning as a Mediator of Relations between Family History of Substance Use Disorder and Impulsivity. Addict. Disord. Their. Treat. 2016, 15, 17–24. [Google Scholar] [CrossRef] [Green Version]
- Khan, S.; Kamal, A. Adaptive family functioning and borderline personality disorder: Mediating role of impulsivity. J. Pak. Med. Assoc. 2020, 70, 86–89. [Google Scholar] [CrossRef]
- Boele, S.; Van der Graaff, J.; De Wied, M.; Van der Valk, I.E.; Crocetti, E.; Branje, S. Linking parent–child and peer relationship quality to empathy in adolescence: A multilevel meta-analysis. J. Youth Adolesc. 2019, 48, 1033–1055. [Google Scholar] [CrossRef] [Green Version]
- Asghari Sharabiani, A.; Basharpoor, S. The mediating role of empathy in the relationship between family functioning and bullying in students. J. Fam. Psychol. 2019, 5, 15–26. [Google Scholar]
- Achenbach, T.M.; Rescorla, L.A. Manual for the ASEBA Adult Forms & Profiles; Research Center for Children, Youth & Families: Burlington, VT, USA, 2003. [Google Scholar]
- Paquette Boots, D.; Wareham, J. An exploration of DSM-oriented scales in the prediction of criminal offending among urban American youths. Crim. Justice Behav. 2009, 36, 840–860. [Google Scholar] [CrossRef]
- Epstein, N.B.; Baldwin, L.M.; Bishop, D.S. The McMaster family assessment device. J. Marital Fam. Ther. 1983, 9, 171–180. [Google Scholar] [CrossRef]
- Grandi, S.; Fabbri, S.; Scortichini, S.; Bolzani, R. Validazione italiana del Family Assessment Device (FAD). Riv. Psichiatr. 2007, 42, 114–122. [Google Scholar] [CrossRef]
- Patton, J.H.; Stanford, M.S.; Barratt, E.S. Factor structure of the Barratt impulsiveness scale. J. Clin. Psychol. 1995, 51, 768–774. [Google Scholar] [CrossRef]
- Fossati, A.; Di Ceglie, A.; Acquarini, E.; Barratt, E.S. Psychometric properties of an Italian version of the Barratt Impulsiveness Scale-11 (BIS-11) in nonclinical subjects. J. Clin. Psychol. 2001, 57, 815–828. [Google Scholar] [CrossRef]
- Davis, M.H. A multidimensional approach to individual differences in empathy. JSAS Cat. Sel. Doc. Psychol. 1980, 10, 85. [Google Scholar]
- Davis, M.H. Measuring individual differences in empathy: Evidence for a multidimensional approach. J. Pers. Soc. Psychol. 1983, 44, 113–126. [Google Scholar] [CrossRef]
- Albiero, P.; Ingoglia, S.; Lo Coco, A. Contributo all’adattamento italiano dell’Interpersonal Reactivity Index. TPM Test. Psychom. Method Appl. Psychol. 2006, 13, 107–125. [Google Scholar]
- Pulos, S.; Elison, J.; Lennon, R. Hierarchical structure of the Interpersonal Reactivity Index. Soc. Behav. Personal. 2004, 32, 355–360. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; Guilford Publications: New York, NY, USA, 2017. [Google Scholar]
- Marsden, J.; Glazebrook, C.; Tully, R.; Völlm, B. Do adult males with antisocial personality disorder (with and without co-morbid psychopathy) have deficits in emotion processing and empathy? A systematic review. Aggress. Violent Behav. 2019, 48, 197–217. [Google Scholar] [CrossRef]
- Azevedo, J.; Vieira-Coelho, M.; Castelo-Branco, M.; Coelho, R.; Figueiredo-Braga, M. Impulsive and premeditated aggression in male offenders with antisocial personality disorder. PLoS ONE 2020, 15, e0229876. [Google Scholar] [CrossRef] [PubMed]
- Luberto, C.M.; Shinday, N.; Song, R.; Philpotts, L.L.; Park, E.R.; Fricchione, G.L.; Yeh, G.Y. A systematic review and meta-analysis of the effects of meditation on empathy, compassion, and prosocial behaviors. Mindfulness 2018, 9, 708–724. [Google Scholar] [CrossRef] [PubMed]
- Mayer, S.V.; Jusyte, A.; Klimecki-Lenz, O.M.; Schönenberg, M. Empathy and altruistic behavior in antisocial violent offenders with psychopathic traits. Psychiatry Res. 2018, 269, 625–632. [Google Scholar] [CrossRef] [Green Version]
- Pfabigan, D.M.; Seidel, E.M.; Wucherer, A.M.; Keckeis, K.; Derntl, B.; Lamm, C. Affective empathy differs in male violent offenders with high-and low-trait psychopathy. J. Pers. Disord. 2015, 29, 42–61. [Google Scholar] [CrossRef] [PubMed]
- Sezen-Balcikanli, G.; Sezen, M. The relationship between empathy and antisocial-prosocial behaviours in youth field hockey players. Int. J. Learn. Chang. 2019, 11, 57–65. [Google Scholar] [CrossRef]
- Seidel, E.M.; Pfabigan, D.M.; Keckeis, K.; Wucherer, A.M.; Jahn, T.; Lamm, C.; Derntl, B. Empathic competencies in violent offenders. Psychiatry Res. 2013, 210, 1168–1175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verona, E.; Bresin, K.; Patrick, C.J. Revisiting psychopathy in women: Cleckley/Hare conceptions and affective response. J. Abnorm. Psychol. 2013, 122, 1088–1093. [Google Scholar] [CrossRef]
- Decety, J.; Chen, C.; Harenski, C.; Kiehl, K.A. An fMRI study of affective perspective taking in individuals with psychopathy: Imagining another in pain does not evoke empathy. Front. Hum. Neurosci. 2013, 7, 489. [Google Scholar] [CrossRef] [Green Version]
- Marsh, A.A.; Finger, E.C.; Fowler, K.A.; Adalio, C.J.; Jurkowitz, I.T.; Schechter, J.C.; Pine, D.S.; Decety, J.; Blair, R.J. Empathic responsiveness in amygdala and anterior cingulate cortex in youths with psychopathic traits. J. Child. Psychol. Psychiatry 2013, 54, 900–910. [Google Scholar] [CrossRef]
- Li, D.; Zhang, W.; Wang, Y. Parental behavioral control, psychological control and chinese adolescents’ peer victimization: The mediating role of self-control. J. Child Fam. Stud. 2015, 24, 628–637. [Google Scholar] [CrossRef]
- Chamberlain, S.R.; Tiego, J.; Fontenelle, L.F.; Hook, R.; Parkes, L.; Segrave, R.; Hauser, T.U.; Dolan, R.J.; Goodyer, I.M.; Bullmore, E.; et al. Fractionation of impulsive and compulsive trans-diagnostic phenotypes and their longitudinal associations. Aust. N. Z. J. Psychiatry 2019, 53, 896–907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedman, N.P.; Rhee, S.H.; Ross, J.M.; Corley, R.P.; Hewitt, J.K. Genetic and environmental relations of executive functions to antisocial personality disorder symptoms and psychopathy. Int. J. Psychophysiol. 2018, 18, 30331–30333. [Google Scholar] [CrossRef] [PubMed]
- Schorr, M.T.; Tietbohl-Santos, B.; de Oliveira, L.M.; Terra, L.; de Borba Telles, L.E.; Hauck, S. Association between different types of childhood trauma and parental bonding with antisocial traits in adulthood: A systematic review. Child Abuse Negl. 2020, 107, 104621. [Google Scholar] [CrossRef]
- Moreno-García, I.; Meneres-Sancho, S.; Camacho-Vara de Rey, C.; Servera, M. A randomized controlled trial to examine the posttreatment efficacy of neurofeedback, behavior therapy, and pharmacology on ADHD measures. J. Atten. Disord. 2019, 23, 374–383. [Google Scholar] [CrossRef] [PubMed]
- van Dongen, J.D. The empathic brain of psychopaths: From social science to neuroscience in empathy. Front. Psychol. 2020, 11, 695. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Age in years, M (SD) | 22.16 (2.18) | |
| Gender, n (%) | ||
| Male | 166 (47.4) | |
| Female | 184 (52.6) | |
| Romantic relationship status, n (%) | ||
| Single | 133 (38) | |
| Partnered | 137 (39.1) | |
| Cohabitant | 62 (17.7) | |
| Married | 18 (5.1) | |
| Living status, n (%) | ||
| Living with family members | 245 (60) | |
| Not living with family members | 105 (30) | |
| Level of education, n (%) | ||
| Less than high school | 30 (8.6) | |
| High school | 155 (44.3) | |
| More than high school | 165 (47.1) | |
| Employment status, n (%) | ||
| Unemployed | 57 (16.3) | |
| Unemployed student | 107 (30.6) | |
| Employed student | 30 (8.6) | |
| Part-time employment | 87 (24.9) | |
| Full-time employment | 69 (19.7) |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1.ASR_Antis | 1 | |||||||||||||
| 2. FAD_PS | −0.05 | 1 | ||||||||||||
| 3.FAD_Com | −0.05 | 0.46 ** | 1 | |||||||||||
| 4.FAD_Rol | −0.34 ** | 0.30 ** | −0.09 | 1 | ||||||||||
| 5.FAD_AI | −0.49 ** | 0.31 ** | −0.20 ** | 0.53 ** | 1 | |||||||||
| 6.FAD_AR | −0.36 ** | 0.08 | −0.08 | 0.38 * | 0.42 ** | 1 | ||||||||
| 7.FAD_ BC | −0.63 ** | 0.06 | 0.12 * | 0.34 * | 0.53 ** | 0.41 ** | 1 | |||||||
| 8.IRI_PT | −0.49 ** | −0.04 | 0.04 | 0.13 * | 0.27 ** | 0.14 ** | 0.37 ** | 1 | ||||||
| 9.IRI_FS | −0.23 ** | 0.04 | 0.11 * | 0.02 | 0.10 * | 0.08 | 0.26 ** | 0.36 ** | 1 | |||||
| 10.IRI_PD | 0.06 | 0.15 ** | 0.04 | −0.16 ** | −0.15 ** | −0.15 ** | −0.10 | 0.01 | 0.31 ** | 1 | ||||
| 11.IRI_EC | −0.53 ** | −0.04 | −0.02 | 0.15 ** | 0.28 ** | 0.16 ** | 0.34 ** | 0.59 ** | 0.44 ** | 0.10 | 1 | |||
| 12.BIS_Att | 0.43 ** | 0.01 | −0.01 | −0.19 ** | −0.23 ** | −0.20 ** | −0.26 ** | −0.28 ** | −0.04 | 0.10 | −0.28 ** | 1 | ||
| 13.BIS_Mot | 0.59 ** | −0.01 | 0.01 | −0.23 ** | −0.39 ** | −0.26 ** | −0.43 ** | −0.41 ** | −0.12 * | 0.01 | −0.40 ** | 0.56 ** | 1 | |
| 14.BIS_NP | 0.44 ** | 0.04 | −0.02 | −0.17 ** | −0.24 ** | −0.15 ** | −0.31 ** | −0.43 ** | −0.24 ** | 0.03 | −0.36 ** | 0.43 ** | 0.56 ** | 1 |
| M | 6.63 | 14.28 | 19.22 | 24.94 | 19.32 | 15.56 | 24.38 | 18.82 | 16.42 | 12.24 | 19.36 | 16.26 | 20.14 | 24.26 |
| DS | 6.62 | 3.01 | 2.79 | 3.39 | 3.52 | 2.70 | 3.36 | 4.46 | 4.56 | 4.42 | 4.29 | 3.33 | 4.51 | 4.29 |
| Adjusted Coefficients | |||||
|---|---|---|---|---|---|
| B (SE) | t | p | |||
| Covariates | |||||
| Gender a | 0.05 (0.45) | 0.18 | 0.90 | ||
| Age | 0.12 (0.10) | 1.19 | 0.23 | ||
| Relationship status b | |||||
| Partnered | −1.36 (0.52) | −2.61 | 0.009 ** | ||
| Cohabit | −1.29 (1.00) | −1.28 | 0.20 | ||
| Married | −0.75 (1.30) | −0.57 | 0.56 | ||
| Living setup c | −0.28 (0.96) | −0.29 | 0.71 | ||
| Level of education d | |||||
| High school | −0.29 (0.81) | −0.36 | 0.71 | ||
| More than high school | −0.89 (0.86) | −1.04 | 0.29 | ||
| Occupation e | |||||
| Unemployed student | −1.34 (0.69) | −1.94 | 0.06 | ||
| Employed student | −1.15 (0.96) | −1.19 | 0.23 | ||
| Employed part time | −1.83 (0.83) | −2.20 | 0.03 * | ||
| Employed full time | −2.74 (0.90) | −3.02 | 0.003 ** | ||
| Predictors | |||||
| FAD | Roles | −0.07 (0.07) | −1.03 | 0.30 | |
| Affective Involvement | −0.11 (0.08) | −1.34 | 0.18 | ||
| Affective Responsiveness | −0.14 (0.09) | −1.51 | 0.13 | ||
| Behavioral Control | −0.54 (0.08) | −6.27 | 0.000 *** | ||
| IRI | Perspective Taking | −0.11 (0.06) | −1.77 | 0.08 | |
| Fantasy | 0.06 (0.05) | 1.27 | 0.20 | ||
| Empathic Concern | −0.34 (0.06) | −5.07 | 0.000 *** | ||
| BIS-11 | Attentional Impulsivity | 0.14 (0.08) | 1.79 | 0.07 | |
| Motor Impulsivity | 0.26 (0.07) | 3.73 | 0.000 *** | ||
| Non-planning Impulsivity | 0.06 (0.06) | 1.02 | 0.30 | ||
| Adjusted R2 | 0.64 | ||||
| Indirect Effect | Effect (BootSE) | LLCI | ULCI |
|---|---|---|---|
| Total | −0.37 (0.05) | −0.49 | −0.27 |
| Behavioral Control→Empathic Concern→Antisocial Personality Problems | −0.15 (0.03) | −0.23 | −0.09 |
| Behavioral Control→Motor Impulsivity→Antisocial Personality Problems | −0.22 (0.04) | −0.31 | −0.14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marzilli, E.; Cerniglia, L.; Cimino, S. Antisocial Personality Problems in Emerging Adulthood: The Role of Family Functioning, Impulsivity, and Empathy. Brain Sci. 2021, 11, 687. https://doi.org/10.3390/brainsci11060687
Marzilli E, Cerniglia L, Cimino S. Antisocial Personality Problems in Emerging Adulthood: The Role of Family Functioning, Impulsivity, and Empathy. Brain Sciences. 2021; 11(6):687. https://doi.org/10.3390/brainsci11060687
Chicago/Turabian StyleMarzilli, Eleonora, Luca Cerniglia, and Silvia Cimino. 2021. "Antisocial Personality Problems in Emerging Adulthood: The Role of Family Functioning, Impulsivity, and Empathy" Brain Sciences 11, no. 6: 687. https://doi.org/10.3390/brainsci11060687
APA StyleMarzilli, E., Cerniglia, L., & Cimino, S. (2021). Antisocial Personality Problems in Emerging Adulthood: The Role of Family Functioning, Impulsivity, and Empathy. Brain Sciences, 11(6), 687. https://doi.org/10.3390/brainsci11060687