
Role of Standardized Plant Extracts in Controlling Alcohol Withdrawal Syndrome—An Experimental Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials and Reagents
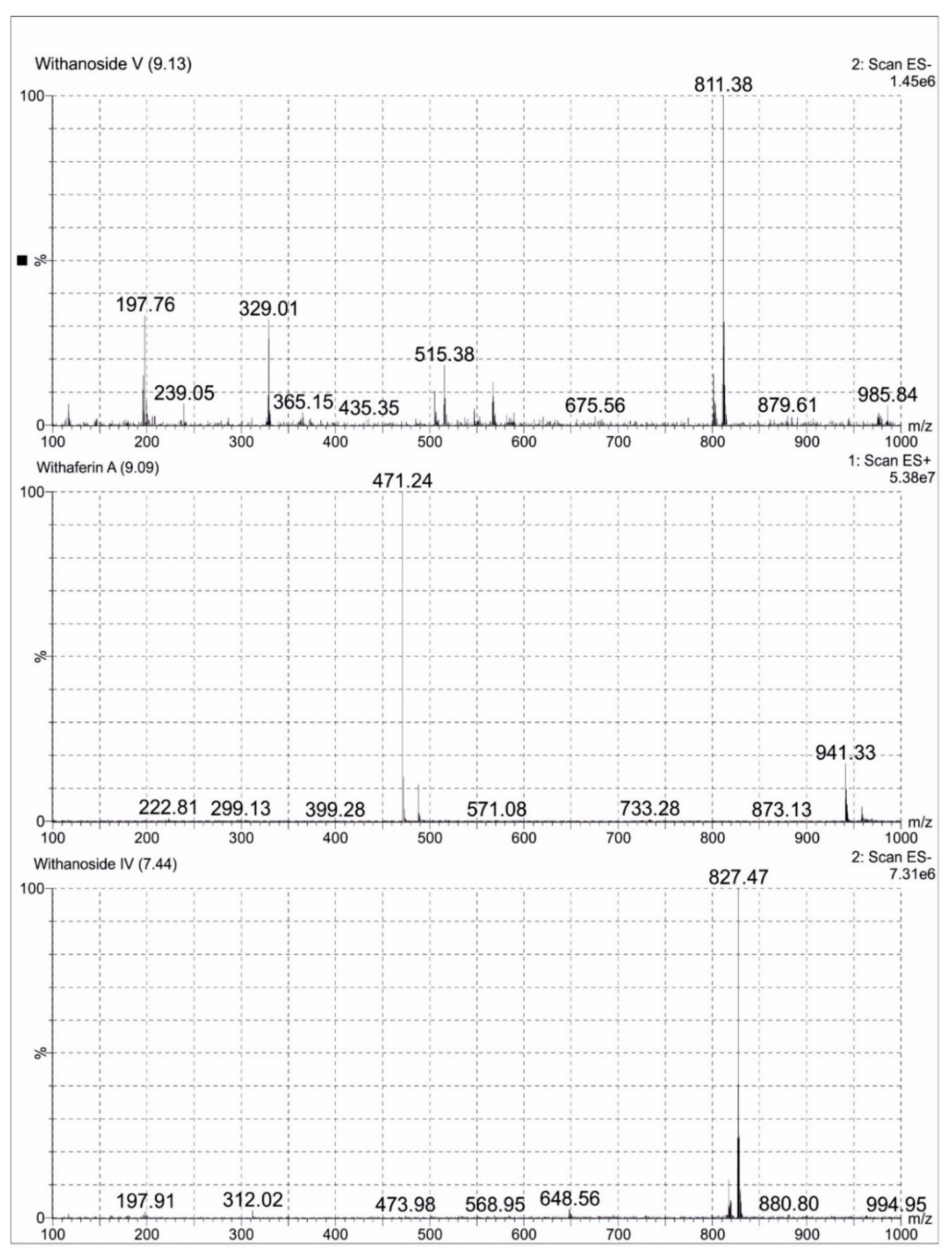
2.2. LCMS Analysis Method of Ashwagandha Extract
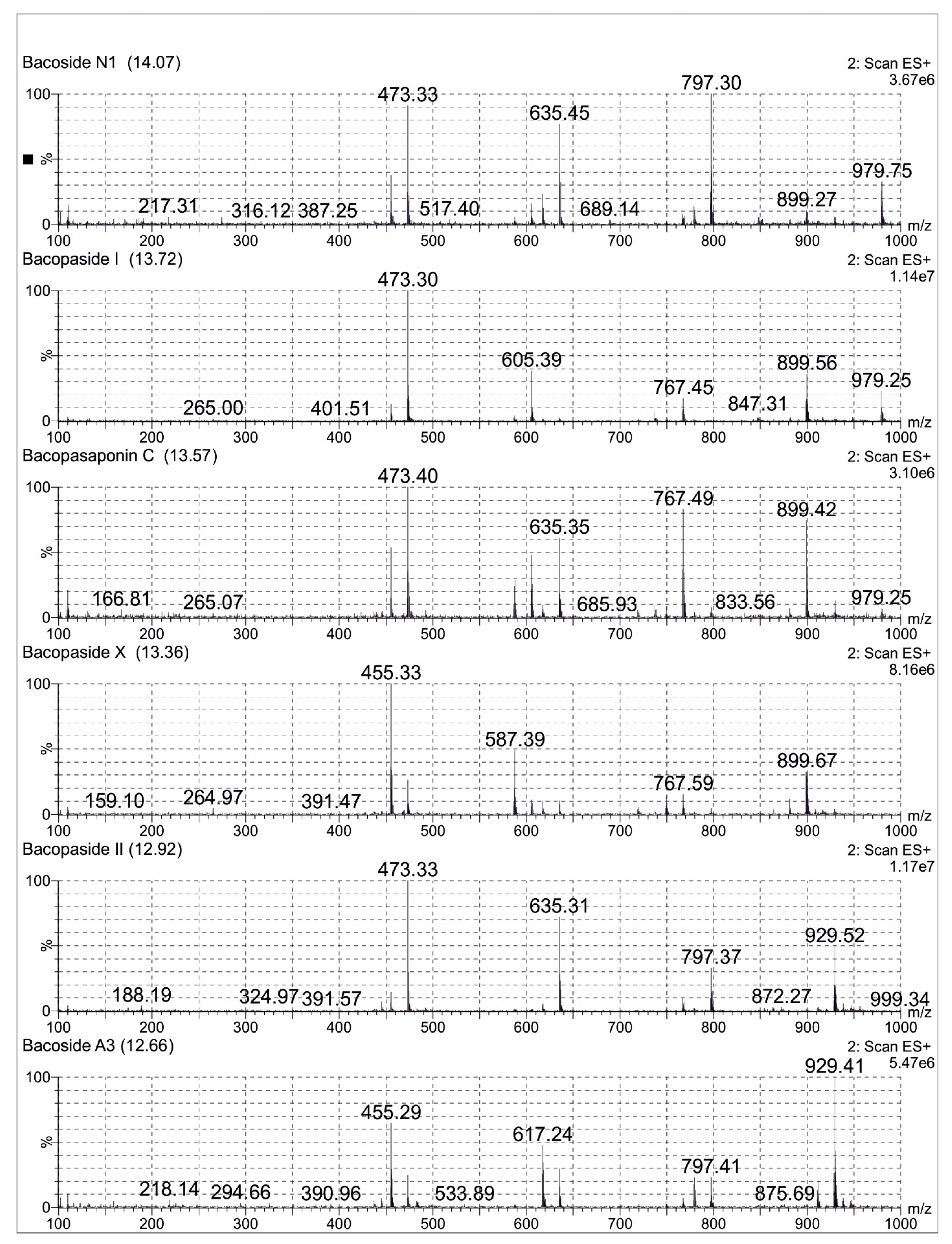
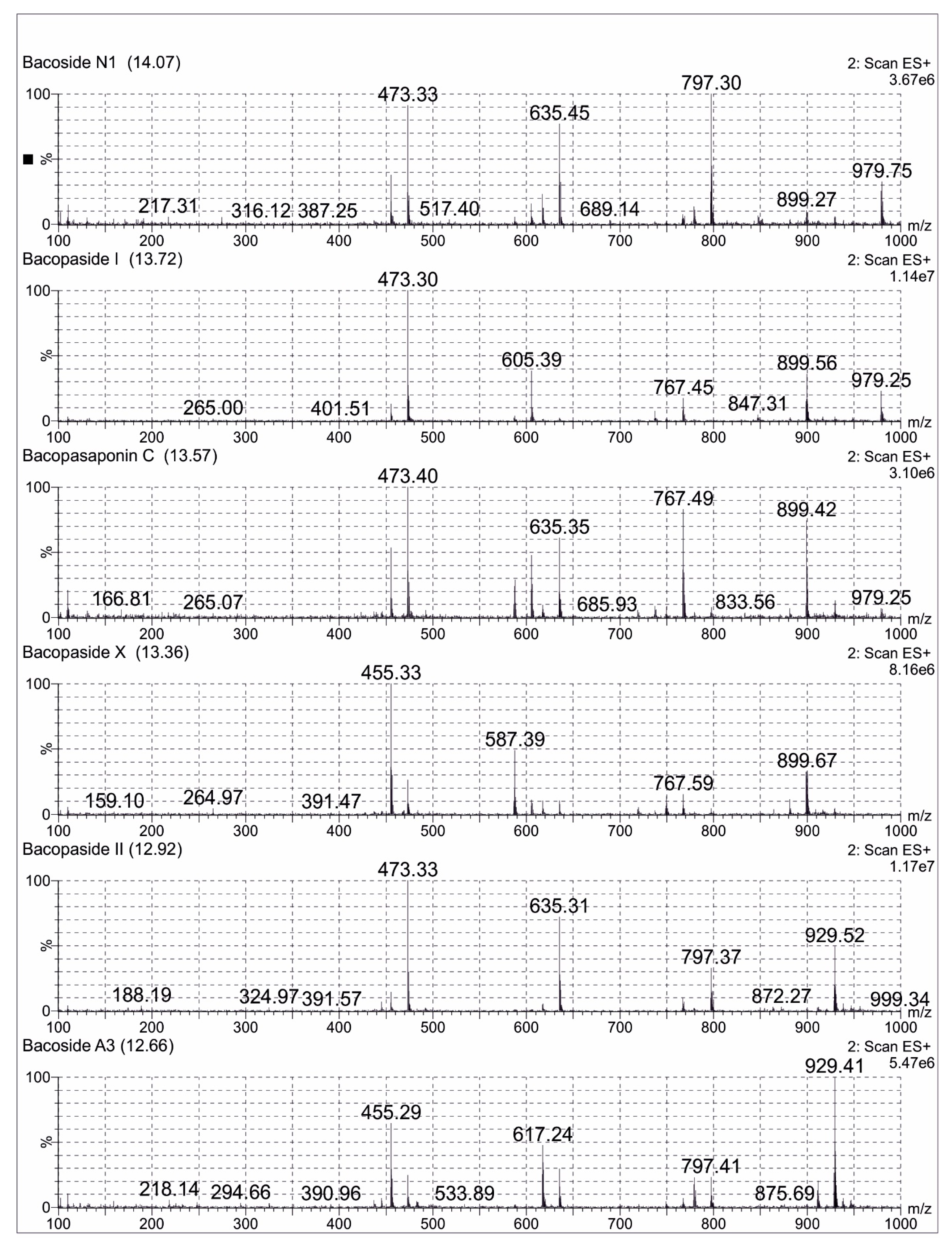
2.3. LCMS Analysis Method of Bacopa Extract
2.4. Animals and Treatment
2.5. Establishment of Alcohol Dependence
2.6. Assessment
2.6.1. Agitation and Stereotyped Behaviour
2.6.2. Elevated Plus Maze
2.6.3. Open Field Test
2.6.4. Pentylenetetrazol Kindling
2.7. Statistical Analysis
3. Results
3.1. Body Weight
3.2. Behavioral Changes during Ethanol Withdrawal
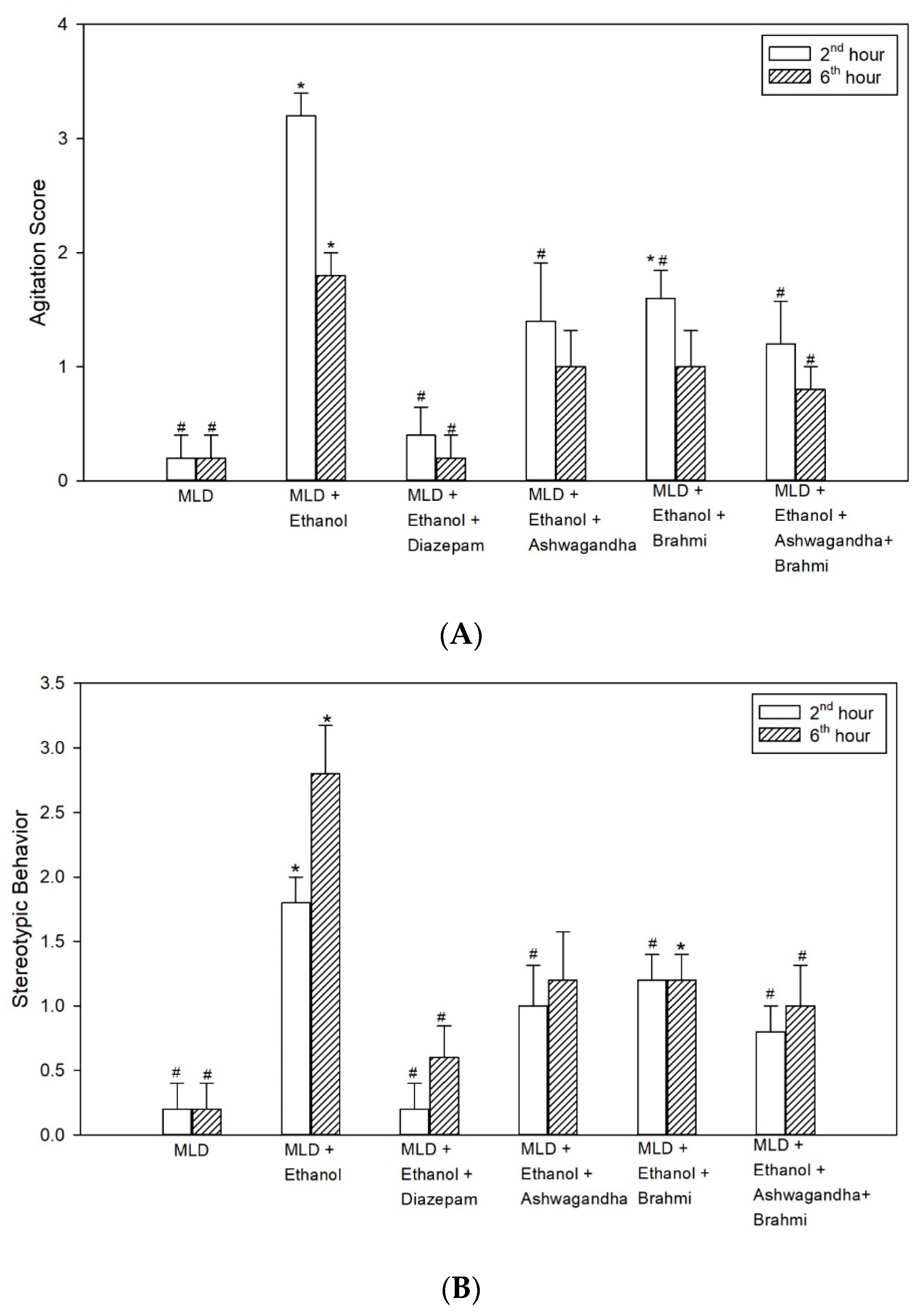
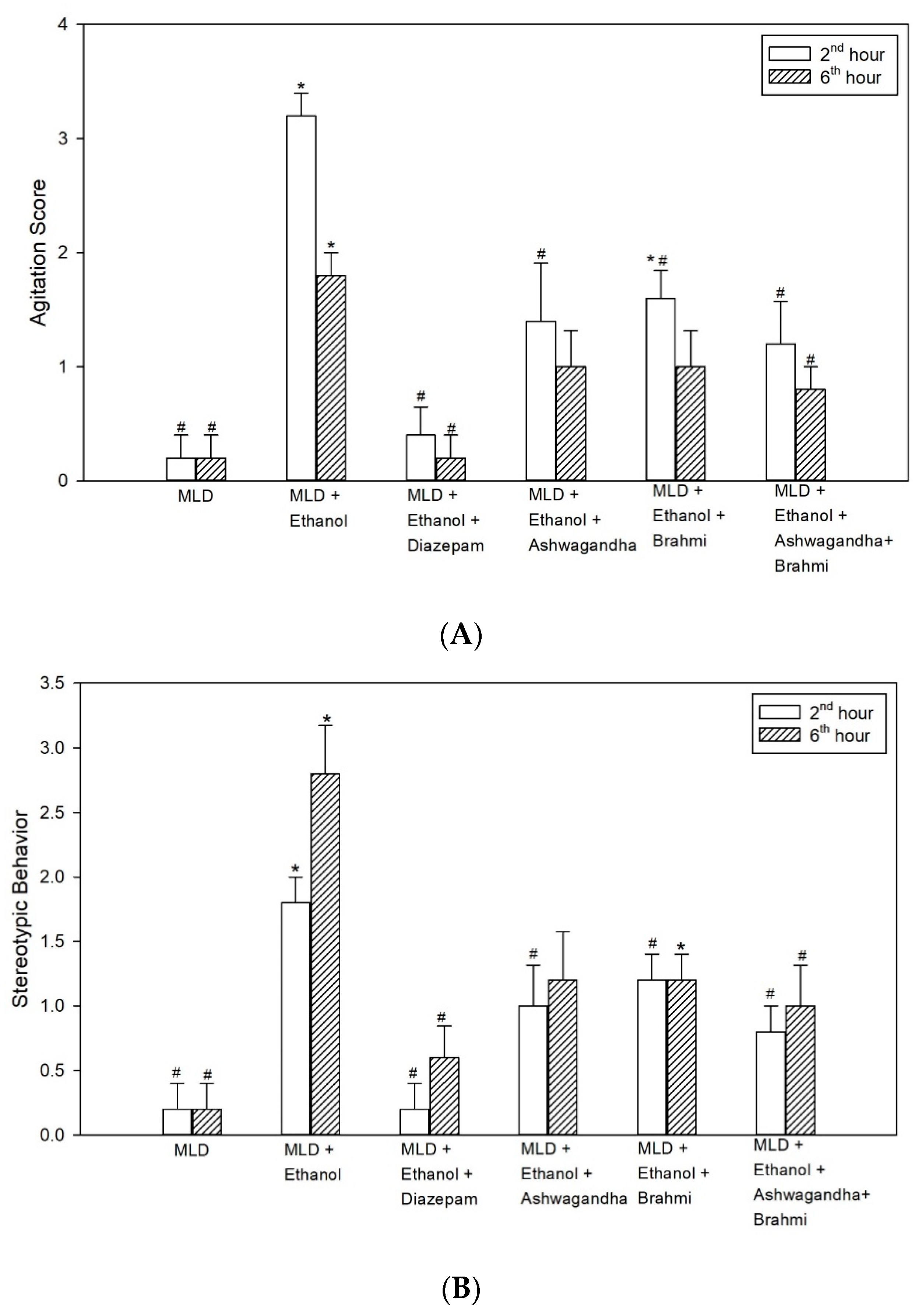
3.2.1. Agitation Score
3.2.2. Stereotypic Behaviour
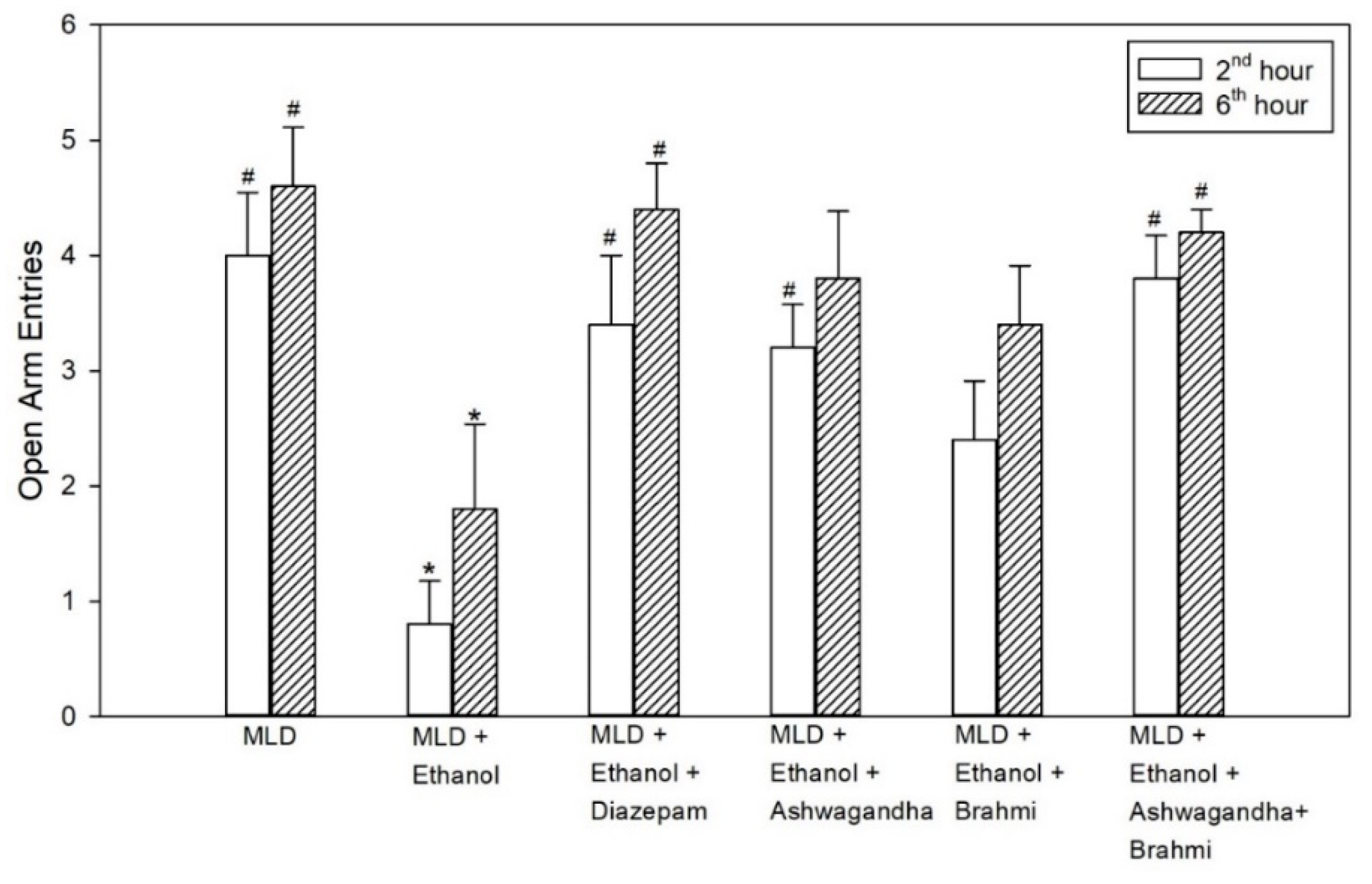
3.3. Elevated Plus Maze (EPZ)
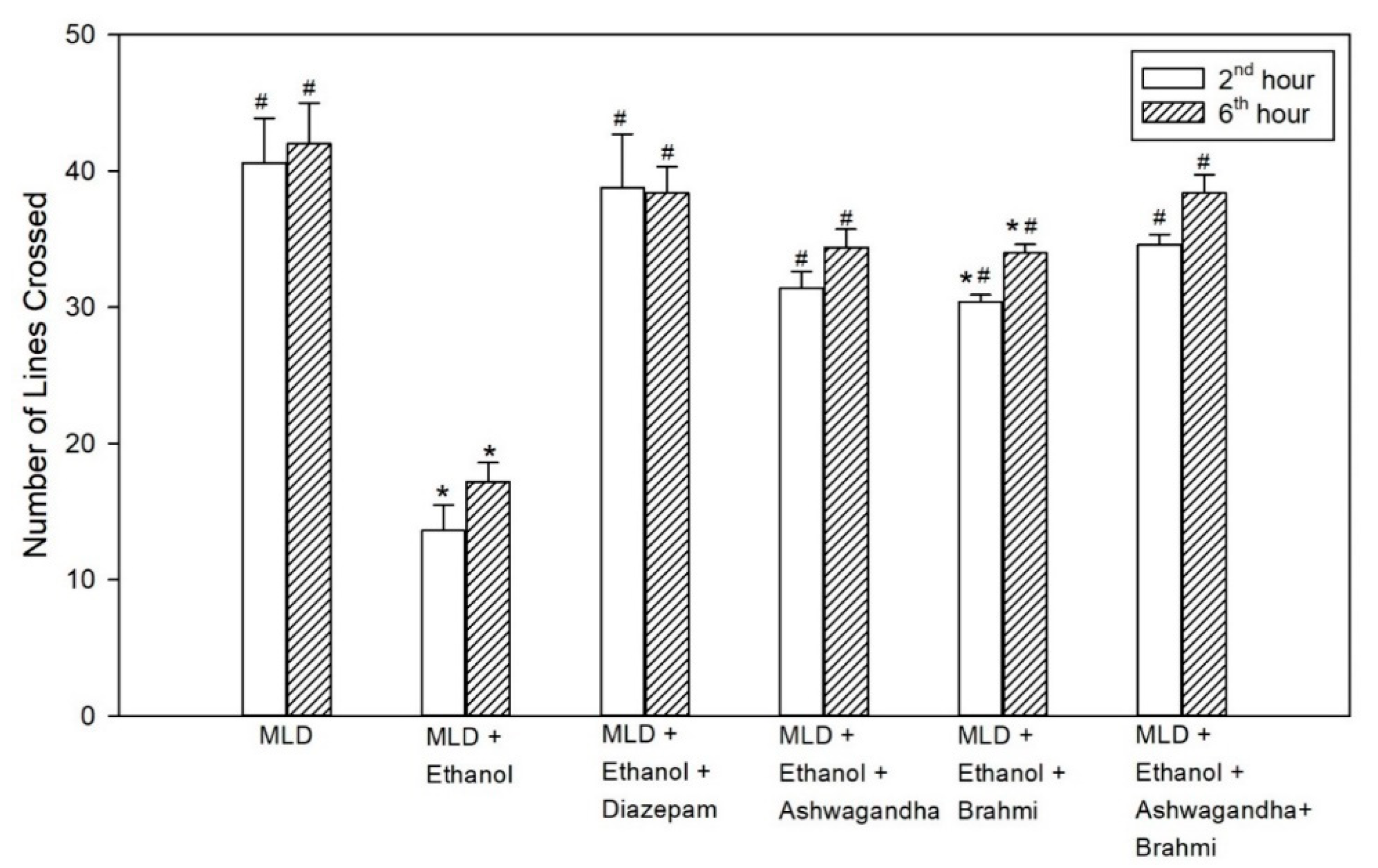
3.4. Open Field Test
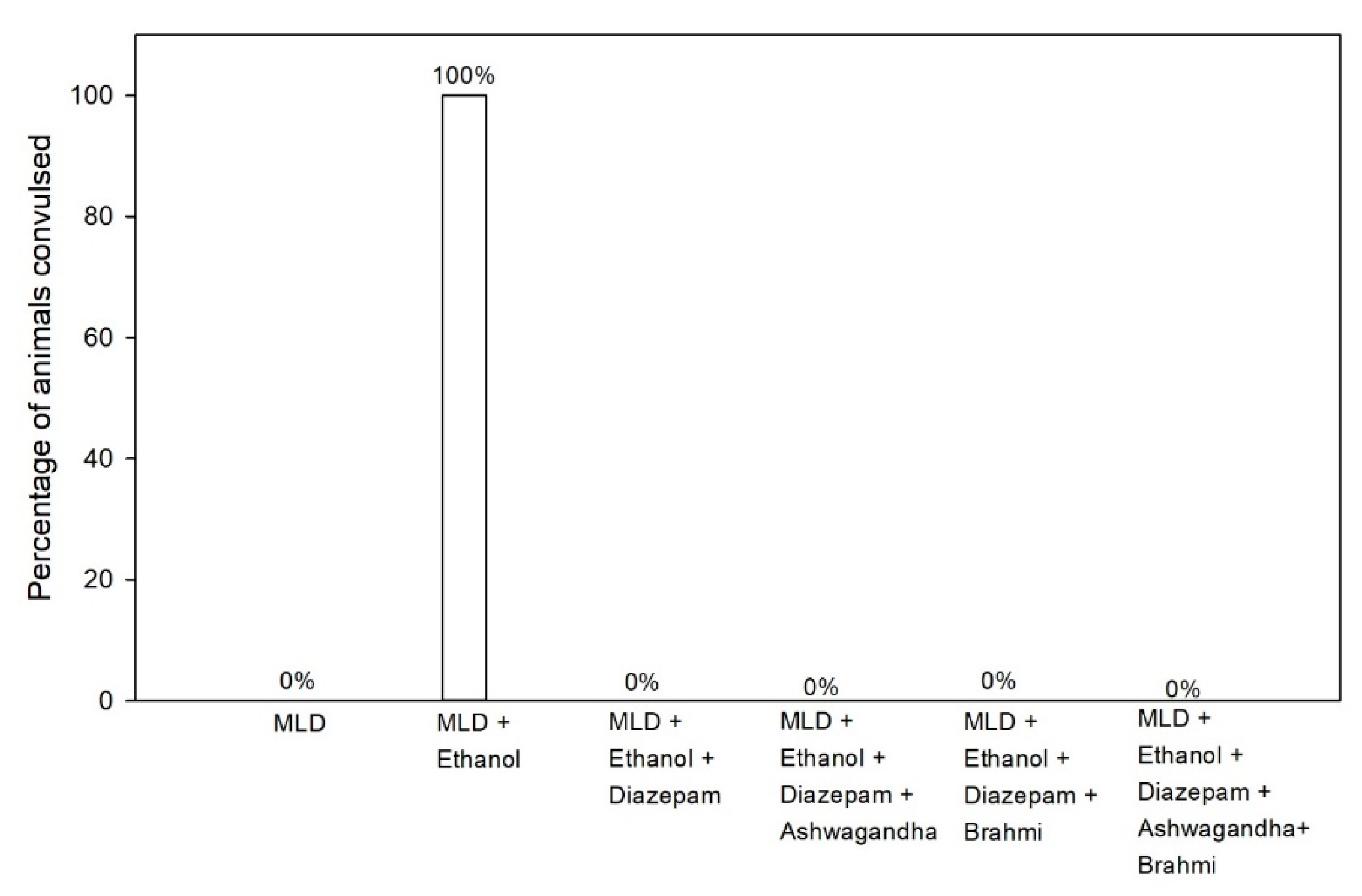
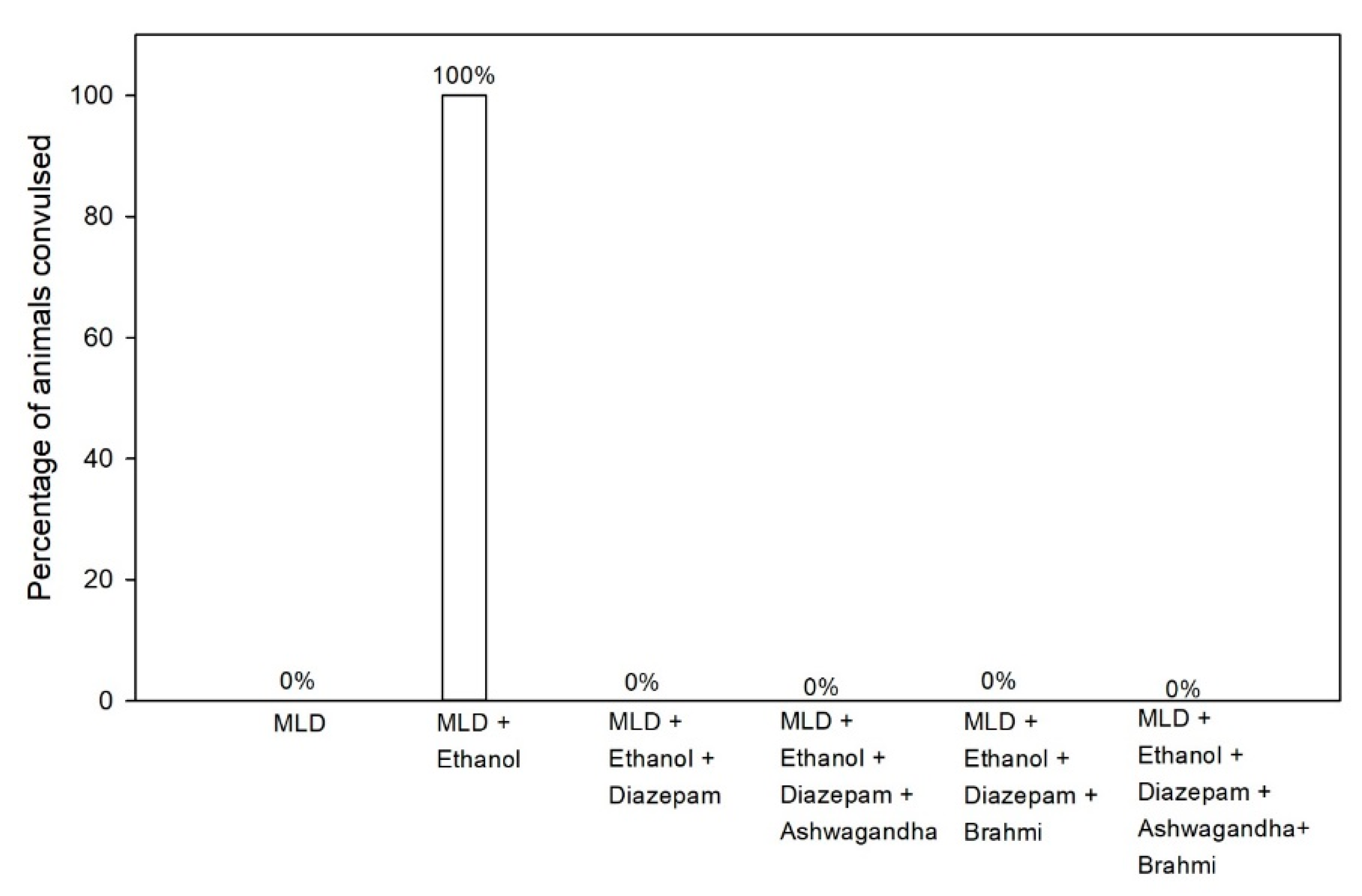
3.5. Pentylenetetrazol (PTZ) Kindling
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Modesto-Lowe, V.; Barron, G.C.; Aronow, B.; Chaplin, M. Gabapentin for alcohol use disorder: A good option, or cause for concern? Cleve Clin. J. Med. 2019, 86, 815. [Google Scholar] [CrossRef] [Green Version]
- Perry, E.C. Inpatient management of acute alcohol withdrawal syndrome. CNS Drugs 2014, 28, 401–410. [Google Scholar] [CrossRef]
- Hughes, J.R. Alcohol withdrawal seizures. Epilepsy Behav. 2009, 15, 92–97. [Google Scholar] [CrossRef]
- Jesse, S.; Bråthen, G.; Ferrara, M.; Keindl, M.; Ben-Menachem, E.; Tanasescu, R.; Brodtkorb, E.; Hillbom, M.; Leone, M.A.; Ludolph, A.C. Alcohol withdrawal syndrome: Mechanisms, manifestations, and management. Acta Neurol. Scand. 2017, 135, 4–16. [Google Scholar] [CrossRef]
- Long, D.; Long, B.; Koyfman, A. The emergency medicine management of severe alcohol withdrawal. Am. J. Emerg. Med. 2017, 35, 1005–1011. [Google Scholar] [CrossRef] [PubMed]
- Airagnes, G.; Ducoutumany, G.; Laffy-Beaufils, B.; Le Faou, A.-L.; Limosin, F. Alcohol withdrawal syndrome management: Is there anything new? Rev. Med. Interne 2019, 40, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Winters, M. Ancient medicine, modern use: Withania somnifera and its potential role in integrative oncology. Altern. Med. Rev. 2006, 11, 269–277. [Google Scholar] [PubMed]
- Schachter, S.C. Botanicals and herbs: A traditional approach to treating epilepsy. Neurotherapeutics 2009, 6, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Gomes, N.G.M.; Campos, M.G.; Órfão, J.M.C.; Ribeiro, C.A.F. Plants with neurobiological activity as potential targets for drug discovery. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2009, 33, 1372–1389. [Google Scholar] [CrossRef] [PubMed]
- Gupta, G.L.; Rana, A.C. Effect of withania somnifera dunal in ethanol-induced anxiolysis and withdrawal anxiety in rats. Indian J. Exp. Biol. 2008, 46, 470–475. [Google Scholar]
- Sreedevi, C.D.; Latha, P.G.; Ancy, P.; Suja, S.R.; Shyamal, S.; Shine, V.J.; Sini, S.; Anuja, G.I.; Rajasekharan, S. Hepatoprotective studies on Sida acuta Burm. J. Ethnopharmacol. 2009, 124, 171–175. [Google Scholar] [CrossRef]
- Bhattacharya, S.K.; Kumar, A.; Ghosal, S. Effects of glycowithanolides from Withania somnifera on an animal model of Alzheimer’s disease and perturbed central cholinergic markers of cognition in rats. Phytother. Res. 1995, 9, 110–113. [Google Scholar] [CrossRef]
- Kuboyama, T.; Tohda, C.; Komatsu, K. Withanoside IV and its active metabolite, sominone, attenuate Aβ (25–35)-induced neurodegeneration. Eur. J. Neurosci. 2006, 23, 1417–1426. [Google Scholar] [CrossRef]
- Kulkarni, S.K.; Dhir, A. Withania somnifera: An Indian ginseng. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2008, 32, 1093–1105. [Google Scholar] [CrossRef] [PubMed]
- Sumathi, T.; Nongbri, A. Hepatoprotective effect of Bacoside-A, a major constituent of Bacopa monniera Linn. Phytomedicine 2008, 15, 901–905. [Google Scholar] [CrossRef] [PubMed]
- Mathew, J.; Balakrishnan, S.; Antony, S.; Abraham, P.M.; Paulose, C.S. Decreased GABA receptor in the cerebral cortex of epileptic rats: Effect of Bacopa monnieri and Bacoside-A. J. Biomed. Sci. 2012, 19, 1–13. [Google Scholar] [CrossRef]
- Vollala, V.R.; Upadhya, S.; Nayak, S. Effect of Bacopa monniera Linn.(brahmi) extract on learning and memory in rats: A behavioral study. J. Vet. Behav. 2010, 5, 69–74. [Google Scholar] [CrossRef]
- Mannan, A.; Abir, A.B.; Rahman, R. Antidepressant-like effects of methanolic extract of Bacopa monniera in mice. BMC Complement. Altern. Med. 2015, 15, 337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gong, M.-F.; Wen, R.-T.; Xu, Y.; Pan, J.-C.; Fei, N.; Zhou, Y.-M.; Xu, J.-P.; Liang, J.-H.; Zhang, H.-T. Attenuation of ethanol abstinence-induced anxiety-and depressive-like behavior by the phosphodiesterase-4 inhibitor rolipram in rodents. Psychopharmacology 2017, 234, 3143–3151. [Google Scholar] [CrossRef]
- Uzbay, I.T.; Kayaalp, S.O. A modified liquid diet of chronic ethanol administration: Validation by ethanol withdrawal syndrome in rats. Pharmacol. Res. 1995, 31, 37–42. [Google Scholar] [CrossRef]
- Girme, A.; Saste, G.; Pawar, S.; Balasubramaniam, A.K.; Musande, K.; Darji, B.; Satti, N.K.; Verma, M.K.; Anand, R.; Singh, R.; et al. Investigating 11 Withanosides and Withanolides by UHPLC–PDA and Mass Fragmentation Studies from Ashwagandha (Withania somnifera). ACS Omega 2020, 5, 27933–27943. [Google Scholar] [CrossRef]
- Nuengchamnong, N.; Sookying, S.; Ingkaninan, K. LC-ESI-QTOF-MS based screening and identification of isomeric jujubogenin and pseudojujubogenin aglycones in Bacopa monnieri extract. J. Pharm. Biomed. Anal. 2016, 129, 121–134. [Google Scholar] [CrossRef]
- Sağlam, E.; Kayir, H.; Çelik, T.; Uzbay, T. Effects of escitalopram on ethanol withdrawal syndrome in rats. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2006, 30, 1027–1032. [Google Scholar] [CrossRef]
- Sağlam, E.; Uzbay, I.T.; Kayir, H.; Çelik, T.; Beyazyürek, M. Effects of venlafaxine on ethanol withdrawal syndrome in rats. Fundam. Clin. Pharmacol. 2004, 18, 693–698. [Google Scholar] [CrossRef]
- Medhi, B.; Prakash, A. Practical Manual of Experimental and Clinical Pharmacology; Jaypee Brothers Medical Publishers: New Delhi, India, 2010; ISBN 8184489536. [Google Scholar]
- Barua, C.C.; Talukdar, A.; Begum, S.A.; Borah, P.; Lahkar, M. Anxiolytic activity of methanol leaf extract of Achyranthes aspera Linn in mice using experimental models of anxiety. Indian J. Pharmacol. 2012, 44, 63. [Google Scholar] [CrossRef] [Green Version]
- Jane, L. How is alcohol withdrawal syndrome best managed in the emergency department? Int. Emerg. Nurs. 2010, 18, 89–98. [Google Scholar] [CrossRef]
- Leggio, L.; Kenna, G.A.; Swift, R.M. New developments for the pharmacological treatment of alcohol withdrawal syndrome. A focus on non-benzodiazepine GABAergic medications. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2008, 32, 1106–1117. [Google Scholar] [CrossRef]
- Liang, J.; Olsen, R.W. Alcohol use disorders and current pharmacological therapies: The role of GABA A receptors. Acta Pharmacol. Sin. 2014, 35, 981–993. [Google Scholar] [CrossRef] [Green Version]
- Maldonado, J.R. Novel algorithms for the prophylaxis and management of alcohol withdrawal syndromes–beyond benzodiazepines. Crit. Care Clin. 2017, 33, 559–599. [Google Scholar] [CrossRef]
- Mannangatti, P.; Naidu, K.N. Indian herbs for the treatment of neurodegenerative disease. In The Benefits of Natural Products for Neurodegenerative Diseases; Springer: Berlin, Germany, 2016; pp. 323–336. [Google Scholar]
- Candelario, M.; Cuellar, E.; Reyes-Ruiz, J.M.; Darabedian, N.; Feimeng, Z.; Miledi, R.; Russo-Neustadt, A.; Limon, A. Direct evidence for GABAergic activity of Withania somnifera on mammalian ionotropic GABAA and GABAρ receptors. J. Ethnopharmacol. 2015, 171, 264–272. [Google Scholar] [CrossRef]
- Kokare, D.M.; Chopde, C.T.; Subhedar, N.K. Participation of α-melanocyte stimulating hormone in ethanol-induced anxiolysis and withdrawal anxiety in rats. Neuropharmacology 2006, 51, 536–545. [Google Scholar] [CrossRef]
- Gatch, M.B.; Wallis, C.J.; Lal, H. Effects of ritanserin on ethanol withdrawal—Induced anxiety in rats. Alcohol 2000, 21, 11–17. [Google Scholar] [CrossRef]
- Ruby, B.; Benson, M.K.; Kumar, E.P.; Sudha, S.; Wilking, J.E. Evaluation of Ashwagandha in alcohol withdrawal syndrome. Asian Pac. J. Trop. Dis. 2012, 2, S856–S860. [Google Scholar] [CrossRef]
- Mishra, A.; Gupta, P.; Kalra, B.S.; Tiwari, Y.K. Efficacy of Ashwagandha and Brahmi Extract on Alcohol Withdrawal Syndrome in Laboratory Rats. Int. J. Pharmacol. 2020, 16, 343–350. [Google Scholar] [CrossRef]
- Kokka, N.; Sapp, D.W.; Taylor, A.M.; Olsen, R.W. The kindling model of alcohol dependence: Similar persistent reduction in seizure threshold to pentylenetetrazol in animals receiving chronic ethanol or chronic pentylenetetrazol. Alcohol. Clin. Exp. Res. 1993, 17, 525–531. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Signs | Scoring | Characteristics Observed |
|---|---|---|
| Agitation | 0 | No irritability or aggressive behaviour |
| 1 | Rats showing mild or moderate irritability | |
| 2 | Very irritable | |
| 3 | handling vocalization and moderately aggressive | |
| 4 | handling vocalization and very aggressive | |
| 5 | spontaneous vocalization and very aggressive | |
| Stereotyped behaviour | 0 | no stereotyped behaviour |
| 1 | rats showing only one stereotyped behaviour | |
| 2 | two stereotyped behaviour | |
| 3 | three stereotyped behaviour | |
| 4 | four stereotyped behaviour | |
| 5 | all stereotyped behaviour |
| Groups | First Entry (Percentage of Rats) | |||
|---|---|---|---|---|
| 2 h | 6 h | |||
| Open Arm | Closed Arm | Open Arm | Closed Arm | |
| MLD | 80% | 20% | 80% | 20% |
| MLD + Ethanol | 0% | 100% | 20% | 80% |
| MLD + Ethanol + Diazepam | 60% | 40% | 80% | 20% |
| MLD + Ethanol + Ashwagandha | 60% | 40% | 60% | 40% |
| MLD + Ethanol + Brahmi | 40% | 60% | 60% | 40% |
| MLD + Ethanol + Ashwagandha + Brahmi | 60% | 40% | 60% | 40% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haque, I.M.; Mishra, A.; Kalra, B.S.; Chawla, S. Role of Standardized Plant Extracts in Controlling Alcohol Withdrawal Syndrome—An Experimental Study. Brain Sci. 2021, 11, 919. https://doi.org/10.3390/brainsci11070919
Haque IM, Mishra A, Kalra BS, Chawla S. Role of Standardized Plant Extracts in Controlling Alcohol Withdrawal Syndrome—An Experimental Study. Brain Sciences. 2021; 11(7):919. https://doi.org/10.3390/brainsci11070919
Chicago/Turabian StyleHaque, Ijasul M., Akhilesh Mishra, Bhupinder Singh Kalra, and Shalini Chawla. 2021. "Role of Standardized Plant Extracts in Controlling Alcohol Withdrawal Syndrome—An Experimental Study" Brain Sciences 11, no. 7: 919. https://doi.org/10.3390/brainsci11070919
APA StyleHaque, I. M., Mishra, A., Kalra, B. S., & Chawla, S. (2021). Role of Standardized Plant Extracts in Controlling Alcohol Withdrawal Syndrome—An Experimental Study. Brain Sciences, 11(7), 919. https://doi.org/10.3390/brainsci11070919