
Heart Rate Variability Analyses in Parkinson’s Disease: A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Eligibility Criteria
2.2. Data Extraction
2.3. Statistical Analyses
3. Results
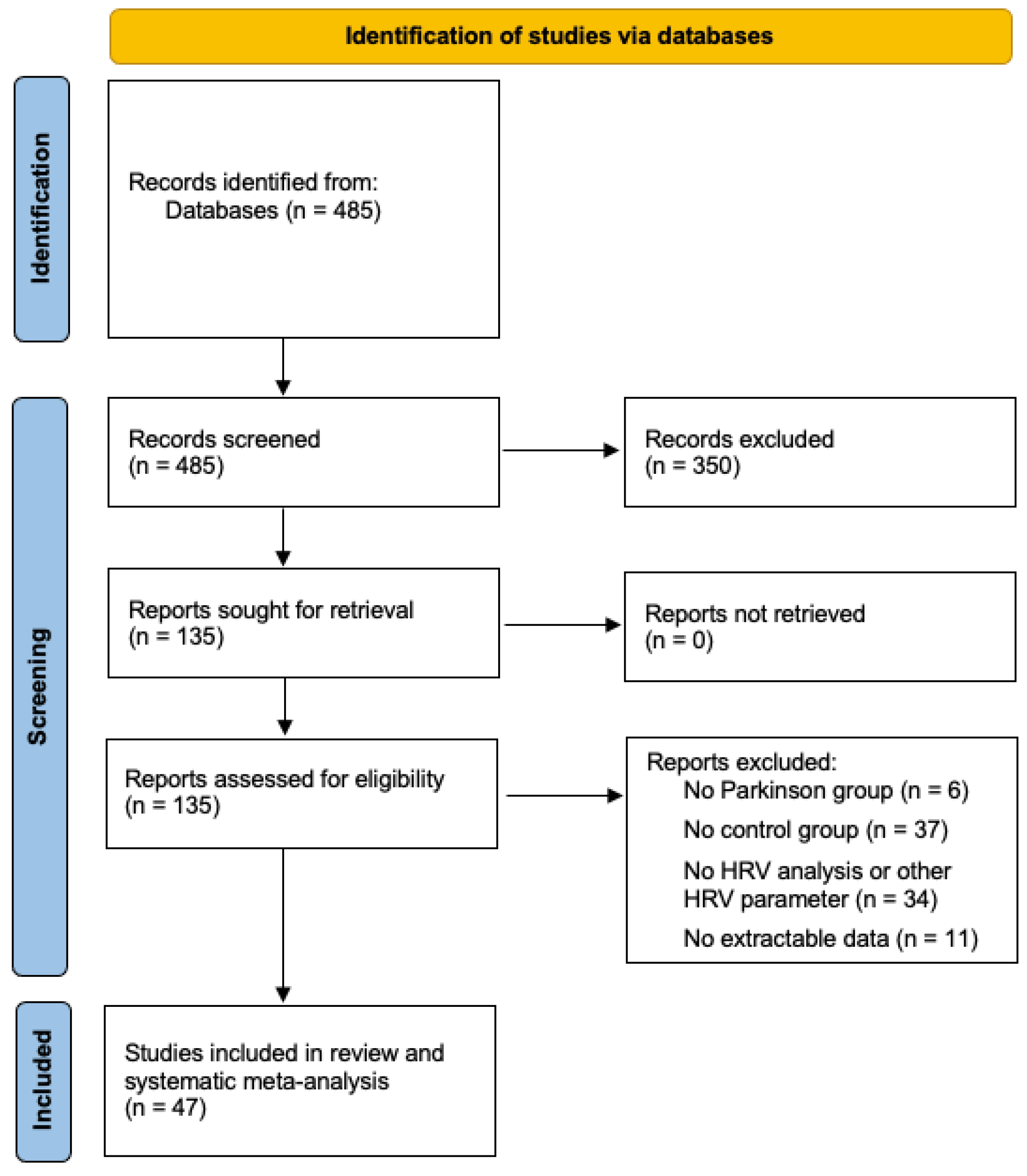
3.1. Selection and Study Population
3.2. Study Characteristics
3.3. Random-Effects Meta-Analyses
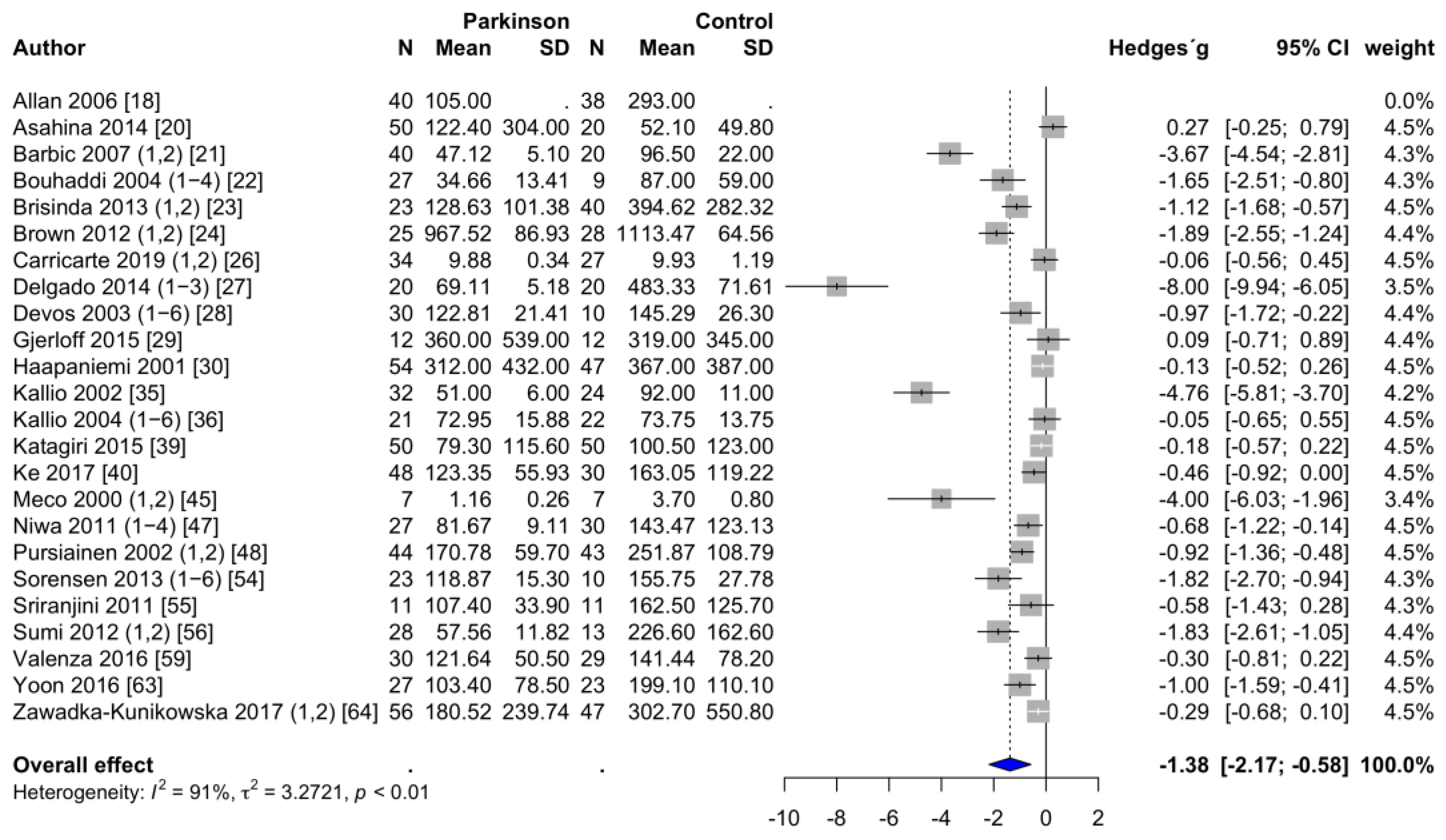
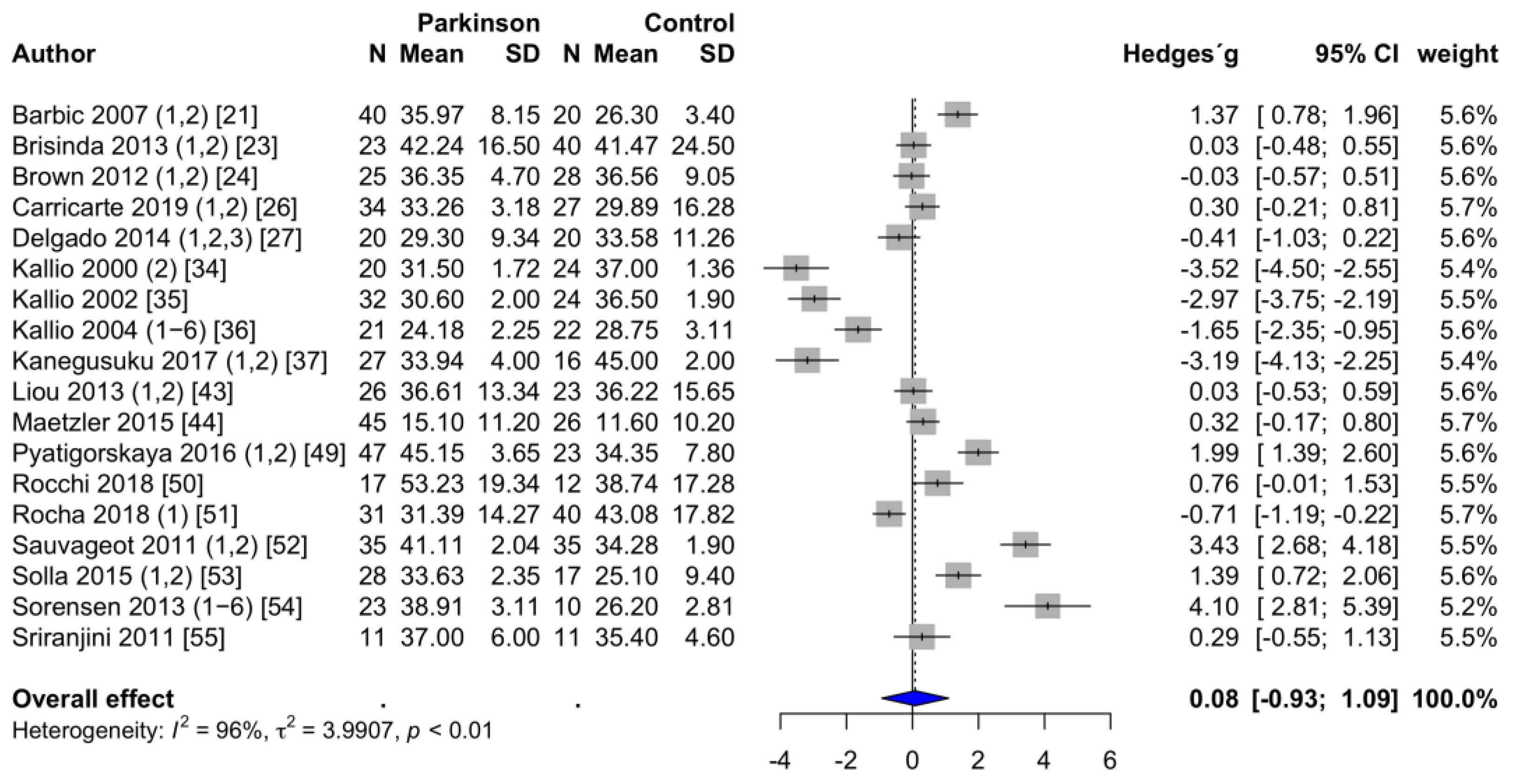
3.3.1. Frequency-Domain Parameters of HRV
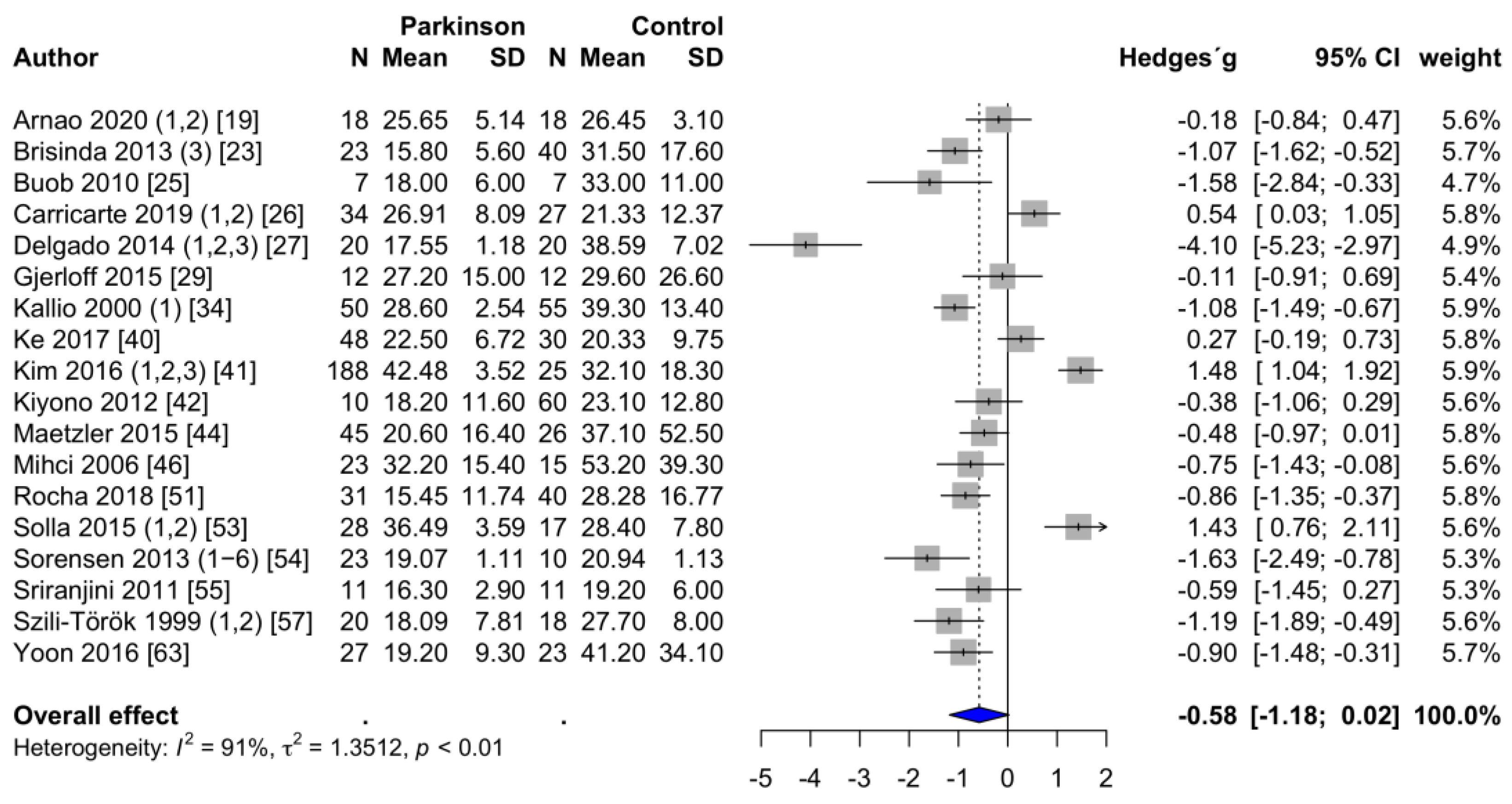
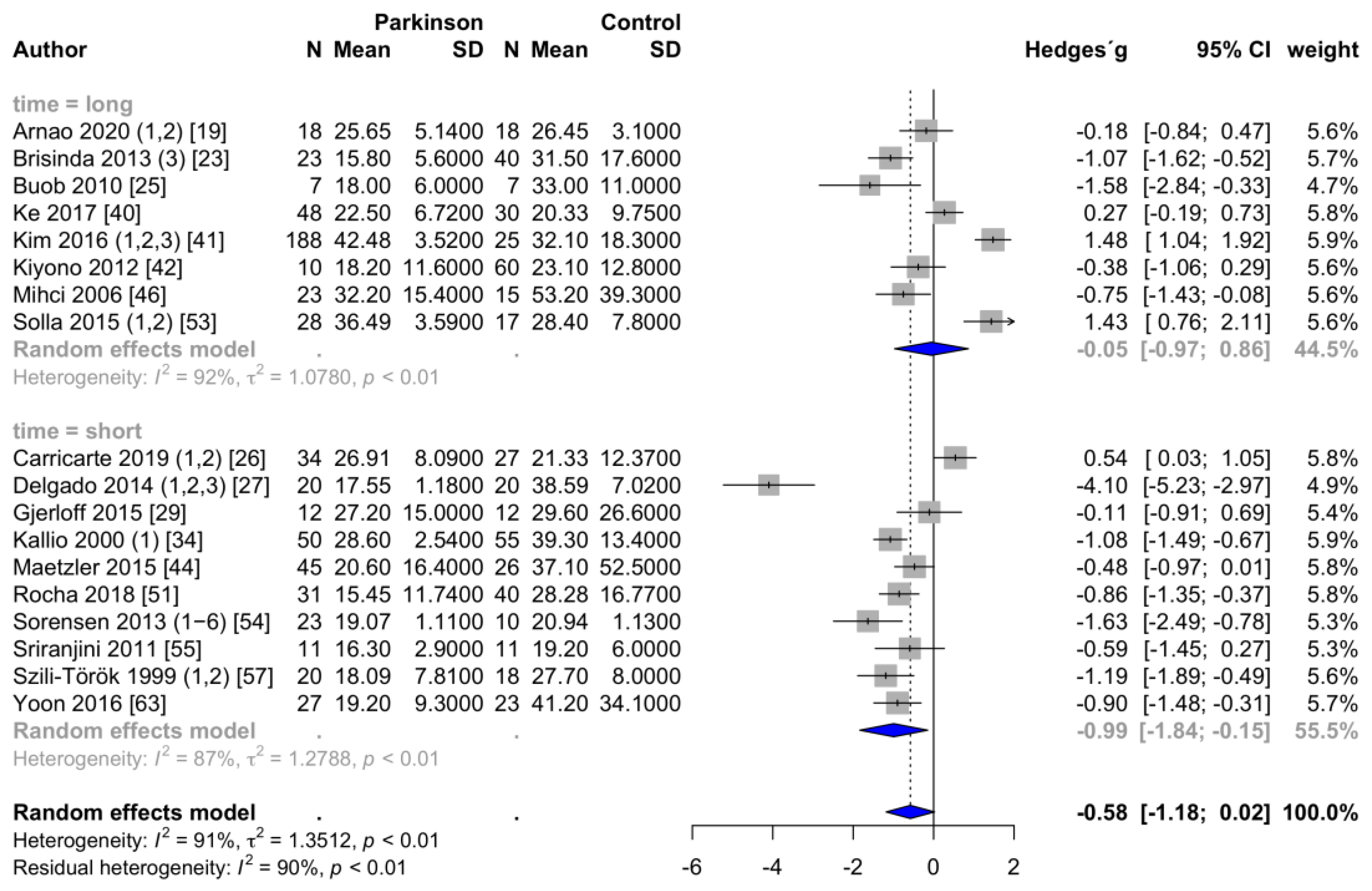
3.3.2. Time-Domain Parameters of HRV
3.4. Between-Study Heterogeneity
3.5. Subgroup Analyses
3.6. Meta-Regression
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Group | HRV Analysis | Measurement | N | Age (y) | N | Age (y) | Disease | Hoehn/Yahr |
|---|---|---|---|---|---|---|---|---|---|
| Parameter | Duration | (PD) | (PD) | (HC) | (HC) | Duration (y) | Stage | ||
| Allan (2006) [18] | PD patients with dementia | HFms2 | short | 40 | 72 | 38 | 76 | 5.0 | na |
| Arnao (2020), 1 [19] | ambulatory setting, daytime | RMSSD, pNN50 | long | 18 | 56 | 18 | 56 | 5.0 | na |
| Arnao (2020), 2 [19] | ambulatory setting, nighttime | RMSSD, pNN50 | long | 18 | 56 | 18 | 56 | 5.0 | na |
| Asahina (2014) [20] | PD patients, early untreated | HFms2 | short | 50 | 64 | 20 | 64 | 1.8 | 1.6 |
| Barbic (2007), 1 [21] | PD patients without orthostatic hypotension | HFms2, HFnu | short | 19 | 66 | 20 | 64 | 7.5 | 2.7 |
| Barbic (2007), 2 [21] | PD patients with orthostatic hypotension | HFms2, HFnu | short | 21 | 69 | 20 | 64 | 10.5 | 2.8 |
| Bouhaddi (2004), 1 [22] | involvement of L-dopa therapy, newly diagnosed without L-dopa | HFms2 | short | 9 | 61 | 9 | 63 | 1.2 | 1.0 |
| Bouhaddi (2004), 2 [22] | involvement of L-dopa therapy, newly diagnosed with L-dopa | HFms2 | short | 9 | 61 | 9 | 63 | 1.2 | 1.0 |
| Bouhaddi (2004), 3 [22] | involvement of L-dopa therapy, long-term treated without L-dopa | HFms2 | short | 18 | 69 | 9 | 63 | 6.0 | 2.0 |
| Bouhaddi (2004), 4 [22] | involvement of L-dopa therapy, long-term treated with L-dopa | HFms2 | short | 18 | 69 | 9 | 63 | 6.0 | 2.0 |
| Brisinda (2013), 1 [23] | PD patients, frequency analysis, during sleep | HFms2, HFnu | short | 23 | 63 | 40 | na | na | 2.0 |
| Brisinda (2013), 2 [23] | PD patients, frequency analysis, daily activity | HFms2, HFnu | short | 23 | 63 | 40 | na | na | 2.0 |
| Brisinda (2013), 3 [23] | PD patients, time-domain analysis | RMSSD, pNN50 | long | 23 | 63 | 40 | na | na | 2.0 |
| Brown (2012), 1 [24] | resting condition, compared to older healthy controls | HFms2, HFnu | short | 25 | na | 28 | na | na | na |
| Brown (2012), 2 [24] | deep breathing, compared to older healthy controls | HFms2, HFnu | short | 25 | na | 28 | na | na | na |
| Buob (2010) [25] | early stages of PD | RMSSD | long | 7 | 50 | 7 | 50 | 4.0 | na |
| Carricarte (2019), 1 [26] | PD patients, LRRK2-associated | HFms2, HFnu, RMSSD | short | 14 | 63 | 27 | 59 | 10.8 | na |
| Carricarte (2019), 2 [26] | PD patients, idiopathic | HFms2, HFnu, RMSSD | short | 20 | 64 | 27 | 59 | 6.3 | na |
| Delgado (2014), 1 [27] | Mexican PD patients, supine resting | HFms2, HFnu, RMSSD, pNN50 | short | 20 | 61 | 20 | 38 | 3.7 | na |
| Delgado (2014), 2 [27] | Mexican PD patients, active standing | HFms2, HFnu, RMSSD, pNN50 | short | 20 | 61 | 20 | 38 | 3.7 | na |
| Delgado (2014), 3 [27] | Mexican PD patients, controlled breathing | HFms2, HFnu, RMSSD, pNN50 | short | 20 | 61 | 20 | 38 | 3.7 | na |
| Devos (2003), 1 [28] | untreated PD patients, disease duration less than 2 years, daytime | HFms2 | long | 10 | 60 | 10 | 61 | 1.5 | na |
| Devos (2003), 2 [28] | untreated PD patients, disease duration less than 2 years, nighttime | HFms2, pNN50 | long | 10 | 60 | 10 | 61 | 1.5 | na |
| Devos (2003), 3 [28] | treated PD patients, disease duration more than 2 years, daytime | HFms2 | long | 10 | 63 | 10 | 61 | 8.0 | na |
| Devos (2003), 4 [28] | treated PD patients, disease duration more than 2 years, nighttime | HFms2, pNN50 | long | 10 | 63 | 10 | 61 | 8.0 | na |
| Devos (2003), 5 [28] | treated PD patients, advanced PD with motor complications, daytime | HFms2 | long | 10 | 62 | 10 | 61 | 8.6 | na |
| Devos (2003), 6 [28] | treated PD patients, advanced PD with motor complications, nighttime | HFms2, pNN50 | long | 10 | 62 | 10 | 61 | 8.6 | na |
| Gjerloff (2015) [29] | association with Donepezil positron emission tomography | HFms2, RMSSD | short | 12 | 64 | 12 | 62 | 5.3 | 2.2 |
| Haapaniemi (2001) [30] | ambulatory setting, 24 h | HFms2 | long | 54 | 61 | 47 | 60 | 1.7 | 1.5 # |
| Harnod (2014) [31] | association with motor symptom duration | HF (ln) * | short | 32 | 62 | 32 | na | 9.8 | 2.7 |
| Jain (2011) [32] | association with pupil measures | HF (*10−1s2/Hz) * | short | 17 | 65 | 18 | 60 | na | 1.7 |
| Jaipurkar (2018), 1 [33] | PD patients, supine resting | HFms2 * | short | 31 | 61 | 31 | 60 | 3.6 | na |
| Jaipurkar (2018), 2 [33] | PD patients, head-up tilt table test | HFms2 * | short | 31 | 61 | 31 | 60 | 3.6 | na |
| Kallio (2000), 1 [34] | PD patients, untreated | RMSSD | short | 50 | 60 | 55 | 56 | 2.2 | 1.7 |
| Kallio (2000), 2 [34] | PD patients, untreated, fast Fourier transform analysis | HFnu, pNN50 | short | 20 | na | 24 | na | na | na |
| Kallio (2002) [35] | PD patients, untreated, fast Fourier transform analysis | HFms2, HFnu | short | 32 | 58 | 24 | 54 | na | na |
| Kallio (2004), 1 [36] | association with nocturnal sleep patterns, awake | HFms2, HFnu | long | 21 | 58 | 22 | 56 | 1.8 | 1.5 |
| Kallio (2004), 2 [36] | association with nocturnal sleep patterns, REM | HFms2, HFnu | long | 21 | 58 | 22 | 56 | 1.8 | 1.5 |
| Kallio (2004), 3 [36] | association with nocturnal sleep patterns, sleep stage 1 | HFms2, HFnu | long | 21 | 58 | 22 | 56 | 1.8 | 1.5 |
| Kallio (2004), 4 [36] | association with nocturnal sleep patterns, sleep stage 2 | HFms2, HFnu | long | 21 | 58 | 22 | 56 | 1.8 | 1.5 |
| Kallio (2004), 5 [36] | association with nocturnal sleep patterns, sleep stage 3 | HFms2, HFnu | long | 21 | 58 | 22 | 56 | 1.8 | 1.5 |
| Kallio (2004), 6 [36] | association with nocturnal sleep patterns, sleep stage 4 | HFms2, HFnu | long | 21 | 58 | 22 | 56 | 1.8 | 1.5 |
| Kanegusuku (2017), 1 [37] | effect of progressive resistance training, PD training group | HFnu | short | 15 | 67 | 16 | 68 | 8.5 | 2.5 |
| Kanegusuku (2017), 2 [37] | effect of progressive resistance training, PD control group | HFnu | short | 12 | 63 | 16 | 68 | 9.0 | 2.4 |
| Kang (2012) [38] | association with olfactory dysfunction | HFms2 * | short | 15 | 66 | 18 | 60 | na | 1.7 |
| Katagiri (2015) [39] | association with myocardial scintigraphy | HFms2 | short | 50 | 66 | 50 | 67 | na | na |
| Ke (2017) [40] | association with sympathetic skin response | HFms2, RMSSD, pNN50 | long | 48 | 69 | 30 | 63 | 5.4 | na |
| Kim (2016), 1 [41] | PD patients, mild stage | RMSSD, pNN50 | long | 106 | 66 | 25 | 67 | 2.2 | 1.1 |
| Kim (2016), 2 [41] | PD patients, moderate stage | RMSSD, pNN50 | long | 51 | 72 | 25 | 67 | 4.5 | 2.2 |
| Kim (2016), 3 [41] | PD patients, severe stage | RMSSD, pNN50 | long | 31 | 71 | 25 | 67 | 5.8 | 3.2 |
| Kiyono (2012) [42] | ambulatory setting, daytime | HF (ln) *, RMSSD | long | 10 | 69 | 60 | 69 | 10.7 | 3.6 |
| Liou (2013), 1 [43] | association with electroencephalography, quiet breathing | HFnu | short | 26 | 67 | 23 | 65 | 2.6 | 1.3 |
| Liou (2013), 2 [43] | association with electroencephalography, deep breathing | HFnu | short | 26 | 67 | 23 | 65 | 2.6 | 1.3 |
| Maetzler (2015) [44] | association with sympathetic skin response, metronomic breathing | HFnu, RMSSD, pNN50 | short | 45 | 66 | 26 | 65 | 3.8 | 2.1 |
| Meco (2000), 1 [45] | effect of treatment with Tolcapone (before treatment), daytime | HFms2 | long | 7 | 70 | 7 | na | 14.1 | 2.1 |
| Meco (2000), 2 [45] | effect of treatment with Tolcapone (before treatment), nighttime | HFms2 | long | 7 | 70 | 7 | na | 14.1 | 2.1 |
| Mihci (2006) [46] | ambulatory setting, 24 h | RMSSD, pNN50 | long | 23 | 66 | 15 | 67 | 5.5 | 2.5 # |
| Niwa (2011), 1 [47] | PD patients, early stage, daytime | HFms2 | long | 9 | 71 | 30 | 69 | 4.8 | na |
| Niwa (2011), 2 [47] | PD patients, early stage, nighttime | HFms2 | long | 9 | 71 | 30 | 69 | 4.8 | na |
| Niwa (2011), 3 [47] | PD patients, advanced stage, daytime | HFms2 | long | 18 | 69 | 30 | 69 | 7.1 | na |
| Niwa (2011), 4 [47] | PD patients, advanced stage, nighttime | HFms2 | long | 18 | 69 | 30 | 69 | 7.1 | na |
| Pursiainen (2002), 1 [48] | PD patients, untreated, daytime | HFms2 | long | 44 | 63 | 43 | 60 | 1.7 | 1.8 |
| Pursiainen (2002), 2 [48] | PD patients, untreated, nighttime | HFms2 | long | 44 | 63 | 43 | 60 | 1.7 | 1.8 |
| Pyatigorskaya (2016), 1 [49] | association with magnetic resonance imaging, slow wave sleep | HFnu | long | 47 | 62 | 23 | 60 | na | 2.0 |
| Pyatigorskaya (2016), 2 [49] | association with magnetic resonance imaging, REM sleep | HFnu | long | 47 | 62 | 23 | 60 | na | 2.0 |
| Rocchi (2018) [50] | comparison to second control group (REM sleep behavior disorder) | HFnu | short | 17 | 68 | 12 | 69 | 2.3 | na |
| Rocha (2018) [51] | effect of game therapy training (before training) | HFnu, RMSSD | short | 31 | 78 | 40 | 72 | 8.0 | 2.0 |
| Sauvageot (2011), 1 [52] | association with nocturnal sleep patterns, Non REM | HFnu, pNN50 | long | 35 | 66 | 35 | 65 | 6.6 | 2.4 |
| Sauvageot (2011), 2 [52] | association with nocturnal sleep patterns, REM | HFnu, pNN50 | long | 35 | 66 | 35 | 65 | 6.6 | 2.4 |
| Solla (2015), 1 [53] | PD patients, tremor dominant subtype | HFnu, RMSSD, pNN50 | long | 17 | 63 | 17 | 65 | 6.0 | 2.1 |
| Solla (2015), 2 [53] | PD patients, akinetic-rigid subtype | HFnu, RMSSD, pNN50 | long | 11 | 66 | 17 | 65 | 7.9 | 2.7 |
| Sorensen (2013), 1 [54] | association with rapid-eye movement sleep behavior, awake | HFms2, HFnu, RMSSD, pNN50 | short | 10 | 63 | 10 | 59 | na | 1.4 |
| Sorensen (2013), 2 [54] | association without rapid-eye movement sleep behavior, awake | HFms2, HFnu, RMSSD, pNN50 | short | 13 | 61 | 10 | 59 | na | 0.9 |
| Sorensen (2013), 3 [54] | association with rapid-eye movement sleep behavior, Non REM | HFms2, HFnu, RMSSD, pNN50 | short | 10 | 63 | 10 | 59 | na | 1.4 |
| Sorensen (2013), 4 [54] | association without rapid-eye movement sleep behavior, Non REM | HFms2, HFnu, RMSSD, pNN50 | short | 13 | 61 | 10 | 59 | na | 0.9 |
| Sorensen (2013), 5 [54] | association with rapid-eye movement sleep behavior, REM | HFms2, HFnu, RMSSD, pNN50 | short | 10 | 63 | 10 | 59 | na | 1.4 |
| Sorensen (2013), 6 [54] | association without rapid-eye movement sleep behavior, REM | HFms2, HFnu, RMSSD, pNN50 | short | 13 | 61 | 10 | 59 | na | 0.9 |
| Sriranjini (2011) [55] | effect of a single dose L-dopa (before intake) | HFms2, HFnu, RMSSD, pNN50 | short | 11 | 57 | 11 | 55 | 4.1 | 2.1 |
| Sumi (2012), 1 [56] | effect of deep brain stimulation (before stimulation), off medication | HFms2 | short | 28 | 62 | 13 | 58 | 22.0 | 3.9 |
| Sumi (2012), 2 [56] | effect of deep brain stimulation (before stimulation), on medication | HFms2 | short | 28 | 62 | 13 | 58 | 22.0 | 2.4 |
| Szili-Török (1999), 1 [57] | association with baroreflex sensitivity, normal | HF (ms/Hz) *, RMSSD, pNN50 | short | 12 | 64 | 18 | 65 | na | 2.0 |
| Szili-Török (1999), 2 [57] | association with baroreflex sensitivity, impaired | HF (ms/Hz) *, RMSSD, pNN50 | short | 8 | 67 | 18 | 65 | na | 2.1 |
| Trachani (2012) [58] | effect of deep brain stimulation (before stimulation) | HFms2 *, HFnu * | short | 24 | 62 | 24 | na | 12.8 | 3.1 |
| Valenza (2016) [59] | computational assessment of heartbeat dynamics | HFms2 | short | 30 | 67 | 29 | 61 | na | na |
| Visanji (2017), 1 [60] | PD patients, LRRK2-associated | HF (log) *, RMSSD * | short | 20 | 64 | 32 | 59 | 11.5 | na |
| Visanji (2017), 2 [60] | PD patients, idiopathic | HF (log) *, RMSSD * | short | 26 | 64 | 32 | 59 | 6.2 | na |
| Walter (2018) [61] | association with vagus nerve atrophy | RMSSD * | short | 20 | 73 | 20 | 70 | 10.1 | na |
| Weise (2015) [62] | association with auricular branch of vagus nerve stimulation | HF (ln) * | short | 50 | 64 | 50 | 64 | 6.4 | 2.3 |
| Yoon (2016) [63] | PD patients, tremor dominant subtype, drug naiv | HFms2, RMSSD | short | 27 | 64 | 23 | 63 | 1.6 | na |
| Zawadka-Kunikowska (2017), 1 [64] | association with peripheral vascular resistance, vasodilation reaction | HFms2 | short | 15 | 67 | 47 | 66 | 9.0 | 2.9 |
| Zawadka-Kunikowska (2017), 2 [64] | association with peripheral vascular resistance, vasoconstriction reaction | HFms2 | short | 41 | 69 | 47 | 66 | 6.0 | 2.0 |
References
- Antony, P.M.; Diederich, N.J.; Kruger, R.; Balling, R. The hallmarks of Parkinson’s disease. FEBS J. 2013, 280, 5981–5993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Titova, N.; Qamar, M.A.; Chaudhuri, K.R. The Nonmotor Features of Parkinson’s Disease. Int. Rev. Neurobiol. 2017, 132, 33–54. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Zhao, E.J.; Zhang, W.; Lu, Y.; Liu, R.; Huang, X.; Ciesielski-Jones, A.J.; Justice, M.A.; Cousins, D.S.; Peddada, S. Meta-analyses on prevalence of selected Parkinson’s nonmotor symptoms before and after diagnosis. Transl. Neurodegener. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Hawkes, C.H.; Del Tredici, K.; Braak, H. Parkinson’s disease: A dual-hit hypothesis. Neuropathol. Appl. Neurobiol. 2007, 33, 599–614. [Google Scholar] [CrossRef] [PubMed]
- Schwiertz, A.; Spiegel, J.; Dillmann, U.; Grundmann, D.; Burmann, J.; Fassbender, K.; Schafer, K.H.; Unger, M.M. Fecal markers of intestinal inflammation and intestinal permeability are elevated in Parkinson’s disease. Parkinsonism Relat. Disord. 2018, 50, 104–107. [Google Scholar] [CrossRef]
- Forsyth, C.B.; Shannon, K.M.; Kordower, J.H.; Voigt, R.M.; Shaikh, M.; Jaglin, J.A.; Estes, J.D.; Dodiya, H.B.; Keshavarzian, A. Increased intestinal permeability correlates with sigmoid mucosa alpha-synuclein staining and endotoxin exposure markers in early Parkinson’s disease. PLoS ONE 2011, 6, e28032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braak, H.; Rub, U.; Gai, W.P.; Del Tredici, K. Idiopathic Parkinson’s disease: Possible routes by which vulnerable neuronal types may be subject to neuroinvasion by an unknown pathogen. J. Neural Transm. 2003, 110, 517–536. [Google Scholar] [CrossRef] [PubMed]
- Ask, T.F.; Lugo, R.G.; Sutterlin, S. The Neuro-Immuno-Senescence Integrative Model (NISIM) on the Negative Association Between Parasympathetic Activity and Cellular Senescence. Front. Neurosci. 2018, 12, 726. [Google Scholar] [CrossRef] [Green Version]
- Goldstein, D.S. Dysautonomia in Parkinson disease. Compr. Physiol. 2014, 4, 805–826. [Google Scholar] [CrossRef] [Green Version]
- Zis, P.; Erro, R.; Walton, C.C.; Sauerbier, A.; Chaudhuri, K.R. The range and nature of non-motor symptoms in drug-naive Parkinson’s disease patients: A state-of-the-art systematic review. NPJ Parkinsons Dis. 2015, 1, 15013. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Task Force of the European Society of Cardiology; The North American Society of Pacing and Electrophysiology. Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation 1996, 93, 1043–1065. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karemaker, J.M. Counterpoint: Respiratory sinus arrhythmia is due to the baroreflex mechanism. J. Appl. Physiol. (1985) 2009, 106, 1742–1743; discussion 1744. [Google Scholar] [CrossRef]
- Da Costa, B.R.; Cevallos, M.; Altman, D.G.; Rutjes, A.W.; Egger, M. Uses and misuses of the STROBE statement: Bibliographic study. BMJ Open 2011, 1, e000048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrer, M.; Cuijpers, P.; Furukawa, T.A.; Ebert, D. Doing Meta-Analysis in R: A Hands-on Guide. Available online: https://bookdown.org/MathiasHarrer/Doing_Meta_Analysis_in_R/ (accessed on 31 January 2021).
- Allan, L.M.; Ballard, C.G.; Allen, J.; Murray, A.; Davidson, A.W.; McKeith, I.G.; Kenny, R.A. Autonomic dysfunction in dementia. J. Neurol. Neurosurg. Psychiatry 2007, 78, 671–677. [Google Scholar] [CrossRef]
- Arnao, V.; Cinturino, A.; Mastrilli, S.; Butta, C.; Maida, C.; Tuttolomondo, A.; Aridon, P.; D’Amelio, M. Impaired circadian heart rate variability in Parkinson’s disease: A time-domain analysis in ambulatory setting. BMC Neurol. 2020, 20, 152. [Google Scholar] [CrossRef]
- Asahina, M.; Mathias, C.J.; Katagiri, A.; Low, D.A.; Vichayanrat, E.; Fujinuma, Y.; Yamanaka, Y.; Kuwabara, S. Sudomotor and cardiovascular dysfunction in patients with early untreated Parkinson’s disease. J. Parkinsons Dis. 2014, 4, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Barbic, F.; Perego, F.; Canesi, M.; Gianni, M.; Biagiotti, S.; Costantino, G.; Pezzoli, G.; Porta, A.; Malliani, A.; Furlan, R. Early abnormalities of vascular and cardiac autonomic control in Parkinson’s disease without orthostatic hypotension. Hypertension 2007, 49, 120–126. [Google Scholar] [CrossRef]
- Bouhaddi, M.; Vuillier, F.; Fortrat, J.O.; Cappelle, S.; Henriet, M.T.; Rumbach, L.; Regnard, J. Impaired cardiovascular autonomic control in newly and long-term-treated patients with Parkinson’s disease: Involvement of L-dopa therapy. Auton. Neurosci. 2004, 116, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Brisinda, D.; Sorbo, A.R.; Di Giacopo, R.; Venuti, A.; Bentivoglio, A.R.; Fenici, R. Cardiovascular autonomic nervous system evaluation in Parkinson disease and multiple system atrophy. J. Neurol. Sci. 2014, 336, 197–202. [Google Scholar] [CrossRef]
- Brown, R.; Duma, S.; Piguet, O.; Broe, G.A.; Macefield, V.G. Cardiovascular variability in Parkinson’s disease and extrapyramidal motor slowing. Clin. Auton. Res. 2012, 22, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Buob, A.; Winter, H.; Kindermann, M.; Becker, G.; Moller, J.C.; Oertel, W.H.; Bohm, M. Parasympathetic but not sympathetic cardiac dysfunction at early stages of Parkinson’s disease. Clin. Res. Cardiol. 2010, 99, 701–706. [Google Scholar] [CrossRef]
- Carricarte Naranjo, C.; Marras, C.; Visanji, N.P.; Cornforth, D.J.; Sanchez-Rodriguez, L.; Schule, B.; Goldman, S.M.; Estevez, M.; Stein, P.K.; Lang, A.E.; et al. Increased markers of cardiac vagal activity in leucine-rich repeat kinase 2-associated Parkinson’s disease. Clin. Auton. Res. 2019, 29, 603–614. [Google Scholar] [CrossRef]
- Delgado, G.; Estanol, B.; Rodriguez-Violante, M.; Martinez-Memije, R.; Infante-Vazquez, O.; Bertado-Ramirez, N. Cardiovascular variability in Mexican patients with Parkinson’s disease. Arq. Neuropsiquiatr. 2014, 72, 762–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devos, D.; Kroumova, M.; Bordet, R.; Vodougnon, H.; Guieu, J.D.; Libersa, C.; Destee, A. Heart rate variability and Parkinson’s disease severity. J. Neural. Transm. 2003, 110, 997–1011. [Google Scholar] [CrossRef]
- Gjerloff, T.; Fedorova, T.; Knudsen, K.; Munk, O.L.; Nahimi, A.; Jacobsen, S.; Danielsen, E.H.; Terkelsen, A.J.; Hansen, J.; Pavese, N.; et al. Imaging acetylcholinesterase density in peripheral organs in Parkinson’s disease with 11C-donepezil PET. Brain 2015, 138, 653–663. [Google Scholar] [CrossRef] [Green Version]
- Haapaniemi, T.H.; Pursiainen, V.; Korpelainen, J.T.; Huikuri, H.V.; Sotaniemi, K.A.; Myllyla, V.V. Ambulatory ECG and analysis of heart rate variability in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2001, 70, 305–310. [Google Scholar] [CrossRef] [Green Version]
- Harnod, D.; Wen, S.H.; Chen, S.Y.; Harnod, T. The association of heart rate variability with parkinsonian motor symptom duration. Yonsei Med. J. 2014, 55, 1297–1302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, S.; Siegle, G.J.; Gu, C.; Moore, C.G.; Ivanco, L.S.; Jennings, J.R.; Steinhauer, S.R.; Studenski, S.; Greenamyre, J.T. Autonomic insufficiency in pupillary and cardiovascular systems in Parkinson’s disease. Parkinsonism Relat. Disord. 2011, 17, 119–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaipurkar, R.; Mohan, L.; Tomar, R. Autonomic cardiovascular regulation in Parkinson’s disease by head-up tilt tes-A cross-sectional study. Natl. J. Physiol. Pharm. Pharmacol. 2018, 8, 1287–1292. [Google Scholar] [CrossRef] [Green Version]
- Kallio, M.; Haapaniemi, T.; Turkka, J.; Suominen, K.; Tolonen, U.; Sotaniemi, K.; Heikkila, V.P.; Myllyla, V. Heart rate variability in patients with untreated Parkinson’s disease. Eur. J. Neurol. 2000, 7, 667–672. [Google Scholar] [CrossRef]
- Kallio, M.; Suominen, K.; Bianchi, A.M.; Makikallio, T.; Haapaniemi, T.; Astafiev, S.; Sotaniemi, K.A.; Myllya, V.V.; Tolonen, U. Comparison of heart rate variability analysis methods in patients with Parkinson’s disease. Med. Biol. Eng. Comput. 2002, 40, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Kallio, M.; Suominen, K.; Haapaniemi, T.; Sotaniemi, K.; Myllyla, V.V.; Astafiev, S.; Tolonen, U. Nocturnal cardiac autonomic regulation in Parkinson’s disease. Clin. Auton. Res. 2004, 14, 119–124. [Google Scholar] [CrossRef]
- Kanegusuku, H.; Silva-Batista, C.; Pecanha, T.; Nieuwboer, A.; Silva, N.D., Jr.; Costa, L.A.; de Mello, M.T.; Piemonte, M.E.; Ugrinowitsch, C.; Forjaz, C.L. Effects of Progressive Resistance Training on Cardiovascular Autonomic Regulation in Patients With Parkinson Disease: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2017, 98, 2134–2141. [Google Scholar] [CrossRef]
- Kang, P.; Kloke, J.; Jain, S. Olfactory dysfunction and parasympathetic dysautonomia in Parkinson’s disease. Clin. Auton. Res. 2012, 22, 161–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katagiri, A.; Asahina, M.; Araki, N.; Poudel, A.; Fujinuma, Y.; Yamanaka, Y.; Kuwabara, S. Myocardial (123)I-MIBG Uptake and Cardiovascular Autonomic Function in Parkinson’s Disease. Parkinsons Dis. 2015, 2015, 805351. [Google Scholar] [CrossRef] [Green Version]
- Ke, J.Q.; Shao, S.M.; Zheng, Y.Y.; Fu, F.W.; Zheng, G.Q.; Liu, C.F. Sympathetic skin response and heart rate variability in predicting autonomic disorders in patients with Parkinson disease. Medicine 2017, 96, e6523. [Google Scholar] [CrossRef]
- Kim, J.S.; Lee, S.H.; Oh, Y.S.; Park, J.W.; An, J.Y.; Park, S.K.; Han, S.R.; Lee, K.S. Cardiovascular Autonomic Dysfunction in Mild and Advanced Parkinson’s Disease. J. Mov. Disord. 2016, 9, 97–103. [Google Scholar] [CrossRef] [Green Version]
- Kiyono, K.; Hayano, J.; Kwak, S.; Watanabe, E.; Yamamoto, Y. Non-gaussianity of low frequency heart rate variability and sympathetic activation: Lack of increases in multiple system atrophy and Parkinson disease. Front. Physiol. 2012, 3, 34. [Google Scholar] [CrossRef] [Green Version]
- Liou, L.M.; Ruge, D.; Chang, Y.P.; Wu, M.N.; Hsu, C.Y.; Lin, C.W.; Tsai, C.L.; Lai, C.L. Functional connectivity between lateral premotor-parietal circuits and the cardiac autonomic system in Parkinson’s disease. J. Neurol. Sci. 2013, 326, 48–52. [Google Scholar] [CrossRef]
- Maetzler, W.; Karam, M.; Berger, M.F.; Heger, T.; Maetzler, C.; Ruediger, H.; Bronzova, J.; Lobo, P.P.; Ferreira, J.J.; Ziemssen, T.; et al. Time- and frequency-domain parameters of heart rate variability and sympathetic skin response in Parkinson’s disease. J. Neura.l Transm. 2015, 122, 419–425. [Google Scholar] [CrossRef]
- Meco, G.; Vanacore, N.; Locuratolo, N.; Bonifati, V.V.; Vella, C.; Giovani, A.; Tubani, L.; Baratta, L.; Mastrocola, C. Heart rate variability in Parkinson’s disease patients treated with tolcapone. Parkinsonism Relat. Disord. 2000, 6, 223–227. [Google Scholar] [CrossRef]
- Mihci, E.; Kardelen, F.; Dora, B.; Balkan, S. Orthostatic heart rate variability analysis in idiopathic Parkinson’s disease. Acta Neurol. Scand. 2006, 113, 288–293. [Google Scholar] [CrossRef]
- Niwa, F.; Kuriyama, N.; Nakagawa, M.; Imanishi, J. Circadian rhythm of rest activity and autonomic nervous system activity at different stages in Parkinson’s disease. Auton. Neurosci. 2011, 165, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Pursiainen, V.; Haapaniemi, T.H.; Korpelainen, J.T.; Huikuri, H.V.; Sotaniemi, K.A.; Myllyla, V.V. Circadian heart rate variability in Parkinson’s disease. J. Neurol. 2002, 249, 1535–1540. [Google Scholar] [CrossRef] [PubMed]
- Pyatigorskaya, N.; Mongin, M.; Valabregue, R.; Yahia-Cherif, L.; Ewenczyk, C.; Poupon, C.; Debellemaniere, E.; Vidailhet, M.; Arnulf, I.; Lehericy, S. Medulla oblongata damage and cardiac autonomic dysfunction in Parkinson disease. Neurology 2016, 87, 2540–2545. [Google Scholar] [CrossRef]
- Rocchi, C.; Placidi, F.; Liguori, C.; Del Bianco, C.; Lauretti, B.; Diomedi, M.; Pisani, A.; Mercuri, N.B.; Izzi, F. Daytime autonomic activity in idiopathic rapid eye movement sleep behavior disorder: A preliminary study. Sleep Med. 2018, 52, 163–167. [Google Scholar] [CrossRef]
- Rocha, R.S.B.; De Oliveira Rocha, L.S.; Pena, E.S.M.; Caldas, L.C.P.; Moreno, M.A. Analysis of autonomic modulation of heart rate in patients with Parkinson’s disease and elderly individuals submitted to game therapy training. Geriatr. Gerontol. Int. 2018, 18, 20–25. [Google Scholar] [CrossRef]
- Sauvageot, N.; Vaillant, M.; Diederich, N.J. Reduced sympathetically driven heart rate variability during sleep in Parkinson’s disease: A case-control polysomnography-based study. Mov. Disord. 2011, 26, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Solla, P.; Cadeddu, C.; Cannas, A.; Deidda, M.; Mura, N.; Mercuro, G.; Marrosu, F. Heart rate variability shows different cardiovascular modulation in Parkinson’s disease patients with tremor dominant subtype compared to those with akinetic rigid dominant subtype. J. Neural. Transm. 2015, 122, 1441–1446. [Google Scholar] [CrossRef]
- Sorensen, G.L.; Mehlsen, J.; Jennum, P. Reduced sympathetic activity in idiopathic rapid-eye-movement sleep behavior disorder and Parkinson’s disease. Auton. Neurosci. 2013, 179, 138–141. [Google Scholar] [CrossRef] [PubMed]
- Sriranjini, S.J.; Ganesan, M.; Datta, K.; Pal, P.K.; Sathyaprabha, T.N. Effect of a single dose of standard levodopa on cardiac autonomic function in Parkinson’s disease. Neurol. India 2011, 59, 659–663. [Google Scholar] [CrossRef] [PubMed]
- Sumi, K.; Katayama, Y.; Otaka, T.; Obuchi, T.; Kano, T.; Kobayashi, K.; Oshima, H.; Fukaya, C.; Yamamoto, T.; Ogawa, Y.; et al. Effect of subthalamic nucleus deep brain stimulation on the autonomic nervous system in Parkinson’s disease patients assessed by spectral analyses of R-R interval variability and blood pressure variability. Stereotact. Funct. Neurosurg. 2012, 90, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Szili-Török, T.; Rudas, L.; Dibó, G.; Paprika, D.; Kardos, A. Abnormal cardiovascular autonomic regulation in Parkinson´s disease. J. Clin. Basic Cardiol. 1999, 2, 245–247. [Google Scholar]
- Trachani, E.; Constantoyannis, C.; Sakellaropoulos, G.C.; Stavrinou, M.L.; Nikiforidis, G.; Chroni, E. Heart rate variability in Parkinson’s disease unaffected by deep brain stimulation. Acta Neurol. Scand. 2012, 126, 56–61. [Google Scholar] [CrossRef]
- Valenza, G.; Orsolini, S.; Diciotti, S.; Citi, L.; Scilingo, E.P.; Guerrisi, M.; Danti, S.; Lucetti, C.; Tessa, C.; Barbieri, R.; et al. Assessment of spontaneus cardiovascular oscillations in Parkinson´s disease. Biomed. Signal Process. Control 2016, 26, 80–89. [Google Scholar] [CrossRef] [Green Version]
- Visanji, N.P.; Bhudhikanok, G.S.; Mestre, T.A.; Ghate, T.; Udupa, K.; AlDakheel, A.; Connolly, B.S.; Gasca-Salas, C.; Kern, D.S.; Jain, J.; et al. Heart rate variability in leucine-rich repeat kinase 2-associated Parkinson’s disease. Mov. Disord. 2017, 32, 610–614. [Google Scholar] [CrossRef]
- Walter, U.; Tsiberidou, P.; Kersten, M.; Storch, A.; Lohle, M. Atrophy of the Vagus Nerve in Parkinson’s Disease Revealed by High-Resolution Ultrasonography. Front. Neurol. 2018, 9, 805. [Google Scholar] [CrossRef] [Green Version]
- Weise, D.; Adamidis, M.; Pizzolato, F.; Rumpf, J.J.; Fricke, C.; Classen, J. Assessment of brainstem function with auricular branch of vagus nerve stimulation in Parkinson’s disease. PLoS ONE 2015, 10, e0120786. [Google Scholar] [CrossRef]
- Yoon, J.H.; Kim, M.S.; Lee, S.M.; Kim, H.J.; Hong, J.M. Heart rate variability to differentiate essential tremor from early-stage tremor-dominant Parkinson’s disease. J. Neurol. Sci. 2016, 368, 55–58. [Google Scholar] [CrossRef] [PubMed]
- Zawadka-Kunikowska, M.; Slomko, J.; Tafil-Klawe, M.; Klawe, J.J.; Cudnoch-Jedrzejewska, A.; Newton, J.L.; Zalewski, P. Role of peripheral vascular resistance as an indicator of cardiovascular abnormalities in patients with Parkinson’s disease. Clin. Exp. Pharmacol. Physiol. 2017, 44, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Braak, H.; Ghebremedhin, E.; Rub, U.; Bratzke, H.; Del Tredici, K. Stages in the development of Parkinson’s disease-related pathology. Cell Tissue Res. 2004, 318, 121–134. [Google Scholar] [CrossRef] [PubMed]
- Goetz, C.G.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stebbins, G.T.; Stern, M.B.; Tilley, B.C.; Dodel, R.; Dubois, B.; et al. Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Process, format, and clinimetric testing plan. Mov. Disord. 2007, 22, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Nunan, D.; Sandercock, G.R.; Brodie, D.A. A quantitative systematic review of normal values for short-term heart rate variability in healthy adults. Pacing Clin. Electrophysiol. 2010, 33, 1407–1417. [Google Scholar] [CrossRef] [PubMed]
- Geovanini, G.R.; Vasques, E.R.; de Oliveira Alvim, R.; Mill, J.G.; Andreao, R.V.; Vasques, B.K.; Pereira, A.C.; Krieger, J.E. Age and Sex Differences in Heart Rate Variability and Vagal Specific Patterns-Baependi Heart Study. Glob. Heart 2020, 15, 71. [Google Scholar] [CrossRef] [PubMed]
- Sammito, S.; Bockelmann, I. Reference values for time- and frequency-domain heart rate variability measures. Heart Rhythm 2016, 13, 1309–1316. [Google Scholar] [CrossRef]
- Abhishekh, H.A.; Nisarga, P.; Kisan, R.; Meghana, A.; Chandran, S.; Trichur, R.; Sathyaprabha, T.N. Influence of age and gender on autonomic regulation of heart. J. Clin. Monit. Comput. 2013, 27, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Koenig, J.; Thayer, J.F. Sex differences in healthy human heart rate variability: A meta-analysis. Neurosci. Biobehav. Rev. 2016, 64, 288–310. [Google Scholar] [CrossRef] [PubMed]
- Hayano, J.; Yuda, E. Pitfalls of assessment of autonomic function by heart rate variability. J. Physiol. Anthropol. 2019, 38, 3. [Google Scholar] [CrossRef] [Green Version]
- Chelban, V.; Vichayanrat, E.; Schottlaende, L.; Iodice, V.; Houlden, H. Autonomic dysfunction in genetic forms of synucleinopathies. Mov. Disord. 2018, 33, 359–371. [Google Scholar] [CrossRef] [PubMed]
- Yasuma, F.; Hayano, J. Respiratory sinus arrhythmia: Why does the heartbeat synchronize with respiratory rhythm? Chest 2004, 125, 683–690. [Google Scholar] [CrossRef]

| Characteristics | PD Patients (n = 1566) | Controls (n = 1206) |
|---|---|---|
| Gender (male, %) | 60.8 | 55.3 |
| Age (years) | 65.0 ± 0.6 | 62.6 ± 1.0 |
| Disease duration (years) | 5.8 ± 0.5 | - |
| Hoehn and Yahr stage | 2.2 ± 0.1 | - |
| UPDRS | 32.3 ± 3.6 | - |
| UPDRSIII | 21.4 ± 2.2 | - |
| (A) Raw Analyses | PD Patients | Controls | SMD | ci.lb | ci.ub | p value | I2 (%) | Tau2 | k |
| HF (ms2) | 145.2 ± 41.1 | 219.4 ± 48.8 | −1.38 | −2.17 | −0.58 | 0.002 | 91 | 3.27 | 23 |
| HF (nu) | 34.7 ± 1.8 | 33.2 ± 1.9 | 0.08 | −0.93 | 1.09 | 0.867 | 96 | 3.99 | 18 |
| RMSSD (ms) | 23.4 ± 1.9 | 28.9 ± 1.8 | −0.58 | −1.18 | 0.02 | 0.059 | 92 | 1.35 | 18 |
| pNN50 (%) | 4.7 ± 1.1 | 6.8 ± 1.3 | −0.46 | −1.54 | 0.63 | 0.378 | 96 | 3.39 | 14 |
| (B) Heterogeneity Analyses | PD Patients | Controls | SMD | ci.lb | ci.ub | p value | I2 (%) | Tau2 | k |
| HF (ms2) | 107.7 ± 11.0 | 183.0 ± 22.0 | −0.79 | −1.13 | −0.45 | <0.001 | 67 | 0.28 | 14 |
| HF (nu) | 34.5 ± 3.3 | 33.8 ± 3.2 | 0.04 | −0.29 | 0.36 | 0.810 | 53 | 0.12 | 9 |
| RMSSD (ms) | 21.7 ± 1.2 | 24.7 ± 1.1 | −0.65 | −0.97 | −0.32 | 0.001 | 66 | 0.18 | 12 |
| pNN50 (%) | 3.5 ± 0.5 | 5.5 ± 0.8 | −0.59 | −1.06 | −0.12 | 0.020 | 64 | 0.28 | 9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heimrich, K.G.; Lehmann, T.; Schlattmann, P.; Prell, T. Heart Rate Variability Analyses in Parkinson’s Disease: A Systematic Review and Meta-Analysis. Brain Sci. 2021, 11, 959. https://doi.org/10.3390/brainsci11080959
Heimrich KG, Lehmann T, Schlattmann P, Prell T. Heart Rate Variability Analyses in Parkinson’s Disease: A Systematic Review and Meta-Analysis. Brain Sciences. 2021; 11(8):959. https://doi.org/10.3390/brainsci11080959
Chicago/Turabian StyleHeimrich, Konstantin G., Thomas Lehmann, Peter Schlattmann, and Tino Prell. 2021. "Heart Rate Variability Analyses in Parkinson’s Disease: A Systematic Review and Meta-Analysis" Brain Sciences 11, no. 8: 959. https://doi.org/10.3390/brainsci11080959
APA StyleHeimrich, K. G., Lehmann, T., Schlattmann, P., & Prell, T. (2021). Heart Rate Variability Analyses in Parkinson’s Disease: A Systematic Review and Meta-Analysis. Brain Sciences, 11(8), 959. https://doi.org/10.3390/brainsci11080959