
Developing a Digital Solution for Remote Assessment in Multiple Sclerosis: From Concept to Software as a Medical Device

 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Concept, Proof of Concept, and Assessment of Unmet Needs
3. Desirability: Challenges in Developing a Digital Solution That PLwMS and HCPs Need and Use
4. Regulatory Standards: Data Security, Verification and Validation
5. Taking an Adaptive Approach
6. Future Horizons
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Filippi, M.; Bar-Or, A.; Piehl, F.; Preziosa, P.; Solari, A.; Vukusic, S.; Rocca, M.A. Multiple sclerosis. Nat. Rev. Dis. Primers 2018, 4, 43. [Google Scholar] [CrossRef]
- Lorscheider, J.; Buzzard, K.; Jokubaitis, V.; Spelman, T.; Havrdova, E.; Horakova, D.; Trojano, M.; Izquierdo, G.; Girard, M.; Duquette, P. Defining secondary progressive multiple sclerosis. Brain 2016, 139, 2395–2405. [Google Scholar] [CrossRef] [Green Version]
- Allen-Philbey, K.; Middleton, R.; Tuite-Dalton, K.; Baker, E.; Stennett, A.; Albor, C.; Schmierer, K. Can we improve the monitoring of people with multiple sclerosis using simple tools, data sharing, and patient engagement? Front. Neurol. 2020, 11, 464. [Google Scholar] [CrossRef] [PubMed]
- Lublin, F.D.; Reingold, S.C.; Cohen, J.A.; Cutter, G.R.; Sørensen, P.S.; Thompson, A.J.; Wolinsky, J.S.; Balcer, L.J.; Banwell, B.; Barkhof, F. Defining the clinical course of multiple sclerosis: The 2013 revisions. Neurology 2014, 83, 278–286. [Google Scholar] [CrossRef] [Green Version]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444. [Google Scholar] [CrossRef] [Green Version]
- Amato, M.P.; Portaccio, E.; Goretti, B.; Zipoli, V.; Hakiki, B.; Giannini, M.; Pastò, L.; Razzolini, L. Cognitive impairment in early stages of multiple sclerosis. Neurol. Sci. 2010, 31, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Inojosa, H.; Proschmann, U.; Akgün, K.; Ziemssen, T. Should we use clinical tools to identify disease progression? Front. Neurol. 2021, 11, 1890. [Google Scholar] [CrossRef] [PubMed]
- Manouchehrinia, A.; Zhu, F.; Piani-Meier, D.; Lange, M.; Silva, D.G.; Carruthers, R.; Glaser, A.; Kingwell, E.; Tremlett, H.; Hillert, J. Predicting risk of secondary progression in multiple sclerosis: A nomogram. Mult. Scler. 2019, 25, 1102–1112. [Google Scholar] [CrossRef]
- Inan, O.; Tenaerts, P.; Prindiville, S.; Reynolds, H.; Dizon, D.; Cooper-Arnold, K.; Turakhia, M.; Pletcher, M.; Preston, K.; Krumholz, H. Digitizing clinical trials. Jpn. Digit. Med. 2020, 3, 1–7. [Google Scholar] [CrossRef]
- Haase, R.; Schultheiss, T.; Kempcke, R.; Thomas, K.; Ziemssen, T. Modern communication technology skills of patients with multiple sclerosis. Mult. Scler. 2013, 19, 1240. [Google Scholar] [CrossRef]
- Center, P.R. Cell Phone and Smartphone Ownership Demographics. Available online: www.pewinternet.org/data-trend/mobile/cell-phone-and-smartphone-ownership-demographics/ (accessed on 15 June 2021).
- Prasad, S.; Ramachandran, R.; Jennings, C. Development of Smartphone Technology to Monitor Disease Progression in Multiple Sclerosis (P01. 144). Neurology 2012, 78. [Google Scholar] [CrossRef]
- Bove, R.; White, C.C.; Giovannoni, G.; Glanz, B.; Golubchikov, V.; Hujol, J.; Jennings, C.; Langdon, D.; Lee, M.; Legedza, A. Evaluating more naturalistic outcome measures: A 1-year smartphone study in multiple sclerosis. Neurol. Neuroimmun. Neuroinflamm. 2015, 2, e162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boukhvalova, A.K.; Kowalczyk, E.; Harris, T.; Kosa, P.; Wichman, A.; Sandford, M.A.; Memon, A.; Bielekova, B. Identifying and quantifying neurological disability via smartphone. Front. Neurol. 2018, 9, 740. [Google Scholar] [CrossRef] [PubMed]
- Feys, P.; Giovannoni, G.; Dijsselbloem, N.; Centonze, D.; Eelen, P.; Lykke Andersen, S. The importance of a multi-disciplinary perspective and patient activation programmes in MS management. Mult. Scler. 2016, 22, 34–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marziniak, M.; Brichetto, G.; Feys, P.; Meyding-Lamadé, U.; Vernon, K.; Meuth, S.G. The use of digital and remote communication technologies as a tool for multiple sclerosis management: Narrative review. JMIR Rehabil. Assist. Technol. 2018, 5, e7805. [Google Scholar] [CrossRef] [PubMed]
- Cancela, J.; Charlafti, I.; Colloud, S.; Wu, C. Digital health in the era of personalized healthcare: Opportunities and challenges for bringing research and patient care to a new level. Digit. Health 2021, 7–31. [Google Scholar] [CrossRef]
- Scholz, M.; Haase, R.; Schriefer, D.; Voigt, I.; Ziemssen, T. Electronic health interventions in the case of multiple sclerosis: From theory to practice. Brain Sci. 2021, 11, 180. [Google Scholar] [CrossRef]
- Lavorgna, L.; Russo, A.; De Stefano, M.; Lanzillo, R.; Esposito, S.; Moshtari, F.; Rullani, F.; Piscopo, K.; Buonanno, D.; Morra, V.B. Health-related coping and social interaction in people with multiple sclerosis supported by a social network: Pilot study with a new methodological approach. Interact. J. Med. Res. 2017, 6, e7402. [Google Scholar] [CrossRef] [Green Version]
- Allam, A.; Kostova, Z.; Nakamoto, K.; Schulz, P.J. The effect of social support features and gamification on a Web-based intervention for rheumatoid arthritis patients: Randomized controlled trial. J. Med. Internet Res. 2015, 17, e3510. [Google Scholar] [CrossRef]
- Fernandez-Luque, L.; Elahi, N.; Grajales, F., 3rd. An analysis of personal medical information disclosed in YouTube videos created by patients with multiple sclerosis. Stud. Health Technol. Inform. 2009, 150, 292–296. [Google Scholar]
- Biogen. Aby App—By above MS. Available online: https://www.abovems.com/en_us/home/ms-support-events/aby-app.html (accessed on 22 July 2021).
- Settle, J.R.; Maloni, H.W.; Bedra, M.; Finkelstein, J.; Zhan, M.; Wallin, M.T. Monitoring medication adherence in multiple sclerosis using a novel web-based tool: A pilot study. J. Telemed. Telecare 2016, 22, 225–233. [Google Scholar] [CrossRef]
- De Angelis, M.; Lavorgna, L.; Carotenuto, A.; Petruzzo, M.; Lanzillo, R.; Brescia Morra, V.; Moccia, M. Digital Technology in Clinical Trials for Multiple Sclerosis: Systematic Review. J. Clin. Med. 2021, 10, 2328. [Google Scholar] [CrossRef] [PubMed]
- International Medical Device Regulators Forum. Available online: http://www.imdrf.org/docs/imdrf/final/technical/imdrf-tech-140918-samd-framework-risk-categorization-141013.pdf (accessed on 12 July 2021).
- Midaglia, L.; Mulero, P.; Montalban, X.; Graves, J.; Hauser, S.L.; Julian, L.; Baker, M.; Schadrack, J.; Gossens, C.; Scotland, A. Adherence and satisfaction of smartphone-and smartwatch-based remote active testing and passive monitoring in people with multiple sclerosis: Nonrandomized interventional feasibility study. J. Med. Internet Res. 2019, 21, e14863. [Google Scholar] [CrossRef] [Green Version]
- Montalban, X.; Graves, J.; Midaglia, L.; Mulero, P.; Julian, L.; Baker, M.; Schadrack, J.; Gossens, C.; Ganzetti, M.; Scotland, A. A smartphone sensor-based digital outcome assessment of multiple sclerosis. Mult. Scler. 2021, 13524585211028561. [Google Scholar] [CrossRef] [PubMed]
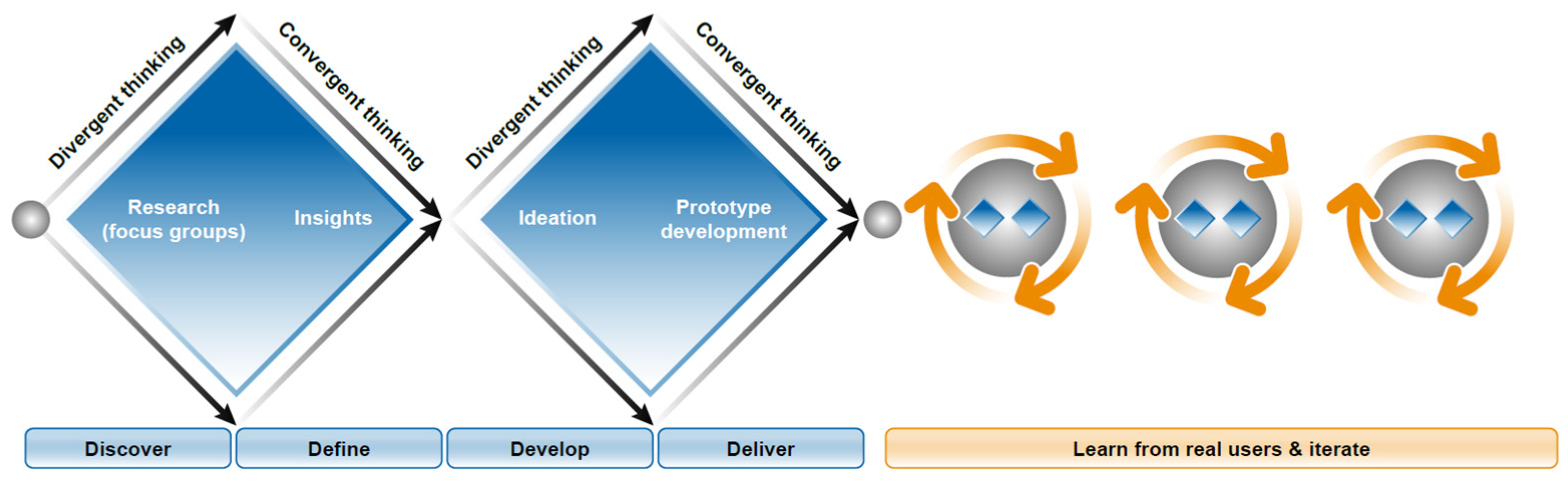
- British Design Council. What Is the Framework for Innovation? Design Council’s Evolved Double Diamond. Available online: https://www.designcouncil.org.uk/news-opinion/what-framework-innovation-design-councils-evolved-double-diamond (accessed on 12 July 2021).
- Heesen, C.; Böhm, J.; Reich, C.; Kasper, J.; Goebel, M.; Gold, S. Patient perception of bodily functions in multiple sclerosis: Gait and visual function are the most valuable. Mult. Scler. 2008, 14, 988–991. [Google Scholar] [CrossRef] [PubMed]
- Bethoux, F.; Bennett, S. Evaluating walking in patients with multiple sclerosis: Which assessment tools are useful in clinical practice? Int. J. MS Care 2011, 13, 4–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubuisson, N.; Baker, D.; Thomson, A.; Marta, M.; Gnanapavan, S.; Turner, B.; Giovannoni, G.; Schmierer, K. Disease modification in advanced MS: Focus on upper limb function. Mult. Scler. 2017, 23, 1956–1957. [Google Scholar] [CrossRef]
- Ortiz-Rubio, A.; Cabrera-Martos, I.; Rodríguez-Torres, J.; Fajardo-Contreras, W.; Díaz-Pelegrina, A.; Valenza, M.C. Effects of a home-based upper limb training program in patients with multiple sclerosis: A randomized controlled trial. Arch. Phys. Med. Rehabilit. 2016, 97, 2027–2033. [Google Scholar] [CrossRef]
- Kister, I.; Bacon, T.E.; Chamot, E.; Salter, A.R.; Cutter, G.R.; Kalina, J.T.; Herbert, J. Natural history of multiple sclerosis symptoms. Int. J. MS Care 2013, 15, 146–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, S.L.; Genova, H.M.; DeLuca, J.; Chiaravalloti, N.D. Information processing speed in multiple sclerosis: Past, present, and future. Mult. Scler. 2017, 23, 772–789. [Google Scholar] [CrossRef]
- Oreja-Guevara, C.; Ayuso Blanco, T.; Brieva Ruiz, L.; Hernández Pérez, M.Á.; Meca-Lallana, V.; Ramió-Torrentà, L. Cognitive dysfunctions and assessments in multiple sclerosis. Front. Neurol. 2019, 10, 581. [Google Scholar] [CrossRef]
- Patti, F.; Amato, M.; Trojano, M.; Bastianello, S.; Tola, M.; Goretti, B.; Caniatti, L.; Di Monte, E.; Ferrazza, P.; Brescia Morra, V. Cognitive impairment and its relation with disease measures in mildly disabled patients with relapsing—Remitting multiple sclerosis: Baseline results from the Cognitive Impairment in Multiple Sclerosis (COGIMUS) study. Mult. Scler. 2009, 15, 779–788. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, V.; Jaric, S. Hand function in multiple sclerosis: Force coordination in manipulation tasks. Clin. Neurophysiol. 2008, 119, 2274–2281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ulwick, T. What Is Jobs-to-be-Done? Available online: https://jobs-to-be-done.com/what-is-jobs-to-be-done-fea59c8e39eb (accessed on 12 July 2021).
- Pratap, A.; Neto, E.C.; Snyder, P.; Stepnowsky, C.; Elhadad, N.; Grant, D.; Mohebbi, M.H.; Mooney, S.; Suver, C.; Wilbanks, J. Indicators of retention in remote digital health studies: A cross-study evaluation of 100,000 participants. Jpn. Digit. Med. 2020, 3, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Burrus, O.; Gupta, C.; Ortiz, A.; Zulkiewicz, B.; Furberg, R.; Uhrig, J.; Harshbarger, C.; Lewis, M.A. Principles for developing innovative HIV digital health interventions: The case of Positive Health Check. Med. Care 2018, 56, 756–760. [Google Scholar] [CrossRef]
- Pagoto, S.; Bennett, G.G. How behavioral science can advance digital health. Transl. Behav. Med. 2013, 3, 271–276. [Google Scholar] [CrossRef] [Green Version]
- Klonoff, D.C. Behavioral theory: The missing ingredient for digital health tools to change behavior and increase adherence. J. Diabetes Sci. Technol. 2019, 13, 276–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duhigg, C. The Power of Habit: Why We Do What We Do and How to Change; Random House: New York, NY, USA, 2013; pp. 1–371. [Google Scholar]
- Fogg, B.J. Tiny Habits: The Small Changes That Change Everything; Eamon Dolan Books: Boston, MA, USA, 2019. [Google Scholar] [CrossRef]
- Fogg, B.J. A behavior model for persuasive design. In Proceedings of the 4th International Conference on Persuasive Technology, Claremont, CA, USA, 26–29 April 2009; pp. 1–7. [Google Scholar] [CrossRef]
- Cugelman, B. Gamification: What it is and why it matters to digital health behavior change developers. JMIR Serious Games 2013, 1, e3139. [Google Scholar] [CrossRef]
- Mathews, S.C.; McShea, M.J.; Hanley, C.L.; Ravitz, A.; Labrique, A.B.; Cohen, A.B. Digital health: A path to validation. Jpn. Digit. Med. 2019, 2, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Food and Drug Administration. Software as a Medical Device (SAMD). Clinical Evaluation-Guidance for Industry and Food and Drug Administration Staff. Retrieved June; 2017; Volume 29, p. 2020. Available online: https://www.fda.gov/files/medical%20devices/published/Software-as-a-Medical-Device-%28SAMD%29--Clinical-Evaluation---Guidance-for-Industry-and-Food-and-Drug-Administration-Staff.pdf (accessed on 15 September 2021).
- Article 2 of Regulation (EU) 2017/745-MDR. Off. J. Eur. Union 2017, L 117/1–L 117/175. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=OJ%3AL%3A2017%3A117%3ATOC (accessed on 15 September 2021).
- FDA. FDA Digital Devices: Digital Health Center of Excellence Services. Available online: https://www.fda.gov/medical-devices/digital-health-center-excellence/digital-health-center-excellence-services (accessed on 12 July 2021).
- Bennett, K.; Bennett, A.J.; Griffiths, K.M. Security considerations for e-mental health interventions. J. Med. Internet Res. 2010, 12, e61. [Google Scholar] [CrossRef] [PubMed]
- Commission, E. Green Paper on Mobile Health (“mHealth”). 2014, pp. 1–20. Available online: https://digital-strategy.ec.europa.eu/en/library/green-paper-mobile-health-mhealth (accessed on 12 July 2021).
- Recruitment, B.C.P. Leveraging Mobile Health Technology for Patient Recruitment. 2012, pp. 1–16. Available online: https://docplayer.net/10235751-Leveraging-mobile-health-technology-for-patient-recruitment-an-emerging-opportunity.html (accessed on 12 July 2021).
- Leclerc, O.; Smith, J. How New Biomolecular Platforms and Digital Technologies Are Changing R&D. Available online: https://www.mckinsey.com/industries/pharmaceuticals-and-medical-products/our-insights/how-new-biomolecular-platforms-and-digital-technologies-are-changing-r-and-d (accessed on 12 July 2021).
- Izmailova, E.S.; Wagner, J.A.; Ammour, N.; Amondikar, N.; Bell-Vlasov, A.; Berman, S.; Bloomfield, D.; Brady, L.S.; Cai, X.; Calle, R.A. Remote digital monitoring for medical product development. Clin. Transl. Sci. 2021, 14, 94–101. [Google Scholar] [CrossRef]
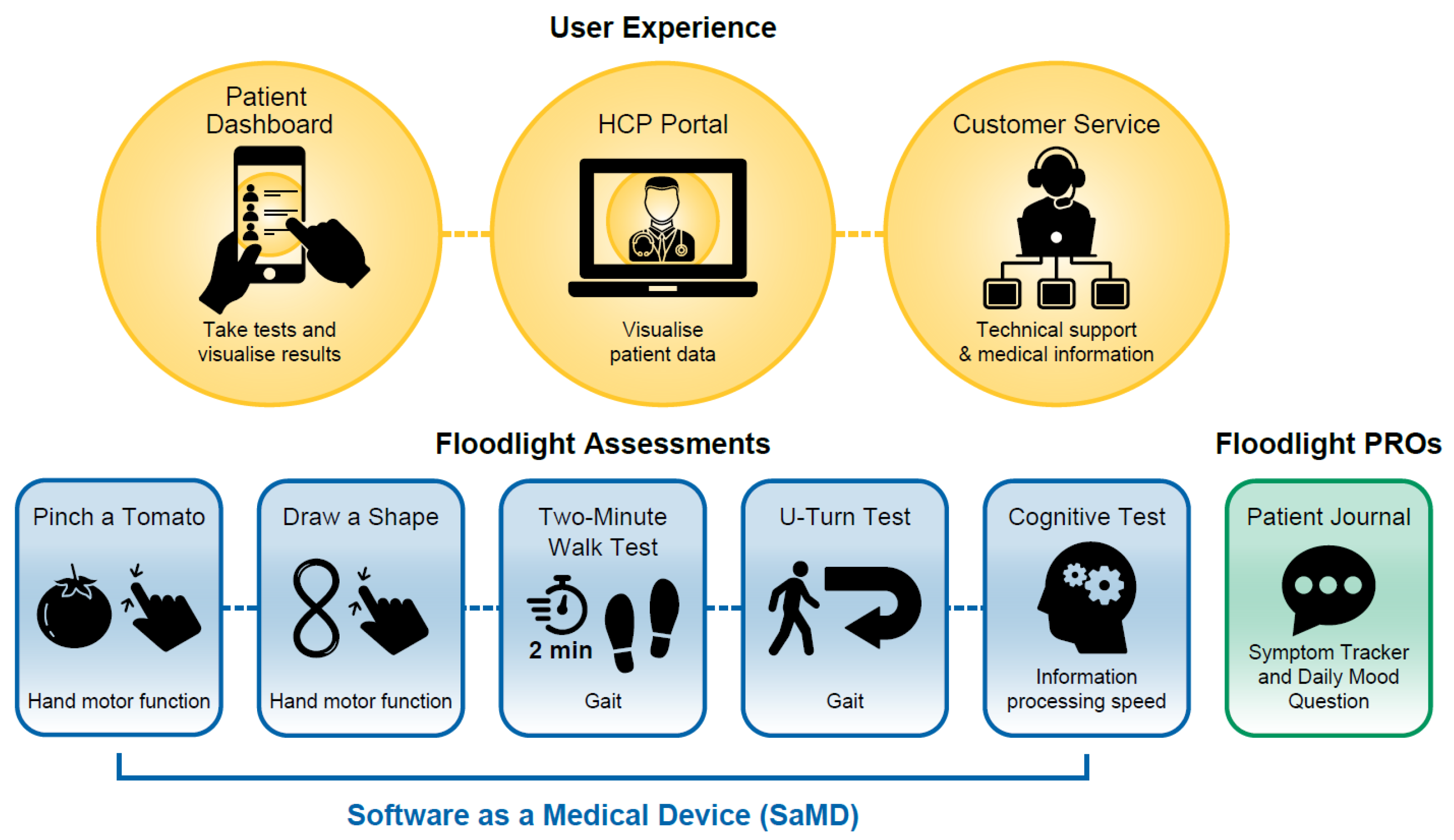
- Cheng, W.-Y.; Bourke, A.K.; Lipsmeier, F.; Bernasconi, C.; Belachew, S.; Gossens, C.; Graves, J.S.; Montalban, X.; Lindemann, M. U-turn speed is a valid and reliable smartphone-based measure of multiple sclerosis-related gait and balance impairment. Gait Posture 2021, 84, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Creagh, A.; Simillion, C.; Scotland, A.; Lipsmeier, F.; Bernasconi, C.; Belachew, S.; van Beek, J.; Baker, M.; Gossens, C.; Lindemann, M. Smartphone-based remote assessment of upper extremity function for multiple sclerosis using the Draw a Shape Test. Physiol. Meas. 2020, 41, 054002. [Google Scholar] [CrossRef]
- Creagh, A.P.; Simillion, C.; Bourke, A.K.; Scotland, A.; Lipsmeier, F.; Bernasconi, C.; van Beek, J.; Baker, M.; Gossens, C.; Lindemann, M. Smartphone-and smartwatch-based remote characterisation of ambulation in multiple sclerosis during the two-minute walk test. IEEE J. Biomed. Health Inform. 2020, 25, 838–849. [Google Scholar] [CrossRef]
- Bourke, A.K.; Scotland, A.; Lipsmeier, F.; Gossens, C.; Lindemann, M. Gait characteristics harvested during a smartphone-based self-administered 2-minute walk test in people with multiple sclerosis: Test-retest reliability and minimum detectable change. Sensors 2020, 20, 5906. [Google Scholar] [CrossRef]
- Bernat, J.L. Ethical and quality pitfalls in electronic health records. Neurology 2013, 80, 1057–1061. [Google Scholar] [CrossRef]
- Romero, M.R.; Staub, A. Specialty Task Force: A Strategic Component to Electronic Health Record (EHR) Optimization. Stud. Health Technol. Inform. 2016, 225, 1051–1052. [Google Scholar]
- D’Souza, M.; Papadopoulou, A.; Girardey, C.; Kappos, L. Standardization and digitization of clinical data in multiple sclerosis. Nat. Rev. Neurol. 2021, 17, 119–125. [Google Scholar] [CrossRef]
- Organisation, W.H. Digital Implementation Investment Guide (DIIG): Integrating Digital Interventions into Health Programmes. 2020, pp. 1–182. Available online: https://www.who.int/publications/i/item/9789240010567 (accessed on 12 July 2021).
- Breuer, R.; Zurkiya, D.N.; Samorezov, J.; Patangay, A.; Zerbi, C.; Company, F.M. Omnichannel Engagement in Medtech: The Time Is Now. Available online: https://www.mckinsey.com/industries/pharmaceuticals-and-medical-products/our-insights/omnichannel-engagement-in-medtech-the-time-is-now (accessed on 12 July 2021).
- Iacob, N.; Simonelli, F. Towards a European Health Data Ecosystem. Eur. J. Risk Regul. 2020, 11, 884–893. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van der Walt, A.; Butzkueven, H.; Shin, R.K.; Midaglia, L.; Capezzuto, L.; Lindemann, M.; Davies, G.; Butler, L.M.; Costantino, C.; Montalban, X. Developing a Digital Solution for Remote Assessment in Multiple Sclerosis: From Concept to Software as a Medical Device. Brain Sci. 2021, 11, 1247. https://doi.org/10.3390/brainsci11091247
van der Walt A, Butzkueven H, Shin RK, Midaglia L, Capezzuto L, Lindemann M, Davies G, Butler LM, Costantino C, Montalban X. Developing a Digital Solution for Remote Assessment in Multiple Sclerosis: From Concept to Software as a Medical Device. Brain Sciences. 2021; 11(9):1247. https://doi.org/10.3390/brainsci11091247
Chicago/Turabian Stylevan der Walt, Anneke, Helmut Butzkueven, Robert K. Shin, Luciana Midaglia, Luca Capezzuto, Michael Lindemann, Geraint Davies, Lesley M. Butler, Cristina Costantino, and Xavier Montalban. 2021. "Developing a Digital Solution for Remote Assessment in Multiple Sclerosis: From Concept to Software as a Medical Device" Brain Sciences 11, no. 9: 1247. https://doi.org/10.3390/brainsci11091247
APA Stylevan der Walt, A., Butzkueven, H., Shin, R. K., Midaglia, L., Capezzuto, L., Lindemann, M., Davies, G., Butler, L. M., Costantino, C., & Montalban, X. (2021). Developing a Digital Solution for Remote Assessment in Multiple Sclerosis: From Concept to Software as a Medical Device. Brain Sciences, 11(9), 1247. https://doi.org/10.3390/brainsci11091247