Abstract
Substance use disorder (SUD) significantly impacts public health, economics, and legal systems worldwide. Eye Movement Desensitization and Reprocessing (EMDR) was initially developed in the late 1980s as a therapeutic approach for post-traumatic stress disorder (PTSD), using bilateral stimulation to integrate traumatic memories with calming physiological responses. However, the effectiveness of EMDR in treating SUD remains unclear. This study aims to conduct a systematic review and meta-analysis of the impact of EMDR therapy on craving reduction in individuals with SUD. The search was conducted using databases such as PubMed and Web of Science, focusing on studies that measured craving and employed EMDR interventions. Both random and fixed effects models were used to pool effect sizes, utilizing an R software meta-package (R-4.4.1). The study adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The results indicated a significant reduction in cravings among patients undergoing EMDR therapy. Specifically, under the fixed effect model, the standardized mean difference (SMD) was −0.866 with a 95% confidence interval ranging from −1.121 to −0.611 (z = −6.66, p < 0.0001). These findings may demonstrate the significant efficacy of EMDR therapy in decreasing cravings in people with SUD.
1. Introduction
Substance use disorder (SUD) exhibits considerable prevalence that fluctuates based on geographical regions [1]. The effects of SUD on community health, economic conditions, and legal structures are considerable and worsening [2]. SUDs lead to heightened mortality rates, drain economic resources, and challenge legal systems [3]. Approximately 270 million individuals, or about 5.5% of the global population aged 15–64, consumed psychoactive substances in the past year, with an estimated 35 million people suffering from drug use disorders, which include harmful patterns of use or dependency. Annually, drug use is linked to roughly 500,000 deaths, divided between 350,000 men and 150,000 women. In recent times, deaths related to opioid use, primarily synthetic opioids, have altered mortality patterns in several high-income nations [4]. In 2017, drug use was responsible for the loss of over 42 million years of healthy life, accounting for approximately 1.3% of the global disease burden [4]. In México, eight out of ten adolescents, either in detention centers or subject to external corrective measures, reported having used some type of psychoactive substance at some point in their lives, with alcohol, tobacco, and marijuana being the most prevalent [5]. Particularly, there has been a surge in drug-related overdose deaths, which is a trend that has sharply increased over the past decade and intensified during the COVID-19 pandemic [6].
Addiction is described as a progressive cycle consisting of three stages: binge/intoxication, withdrawal/negative affect, and preoccupation/anticipation. This cycle involves changes in the brain’s reward and stress systems [7]. The cycle is driven by two types of reinforcement: positive reinforcement, which encourages substance use through pleasurable effects, and negative reinforcement, which motivates use by reducing or avoiding negative feelings [8,9]. The chronic administration of drugs leads to increased reward thresholds during withdrawal, effectively reducing the perceived reward from drug use. A major challenge in drug addiction is chronic relapse, where individuals repeatedly revert to compulsive drug use long after the acute withdrawal symptoms have subsided. Persistent withdrawal can lead to intense cravings [7,10].
A crucial element of SUD is the development of persistent craving, which is defined as a compelling and intrusive desire or compulsion to use a drug. This craving is primarily driven by memories of the drug’s rewarding effects, which are closely associated with a negative emotional state [7,11,12]. It is suggested that cravings, triggered by cues linked to drug use, progressively intensify during the early stages of abstinence and continue to be elevated over prolonged periods [11]. Research indicates that maladaptive memory associations contribute to the perpetuation of behaviors linked with substance abuse and the experience of cravings. These associations often reinforce negative patterns of behavior, making the cycle of addiction more difficult to break [9,13]. Cravings are often sustained and intensified by vivid sensory imagery stored in memories, where more intense imagery is associated with stronger cravings. Craving is a significant factor in addictive behaviors [11,14], and substantial evidence [15] supports its classification as one of the primary criteria for diagnosing substance use disorders (SUDs) in the most recent edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5).
The presence of craving and deficits in inhibitory control are considered crucial in addiction particularly when individuals encounter specific behavioral triggers [12]. Moreover, findings suggest that alleviating cravings is linked to subsequent reductions in substance use and its associated negative consequences. Consequently, craving is regarded as a potential predictor of relapse and may discourage individuals from attempting to cease their substance use [12,16].
Eye Movement Desensitization and Reprocessing (EMDR) was developed in the late 1980s as a psychological treatment for post-traumatic stress disorder (PTSD) [17], although its clinical applications have been extended considerably over the years. EMDR can mitigate the vividness of these memory images through reprocessing techniques, presenting a viable therapeutic option for addressing such cravings [13]. The Adaptive Information Processing (AIP) model is the prevailing theory used to explain the mechanisms behind Eye Movement Desensitization and Reprocessing (EMDR). This model posits that there is an inherent system within everyone that is physiologically designed to process information toward a state of mental health. It is believed that EMDR leverages bilateral stimulation to facilitate the connection and reintegration of traumatic experiences with relaxing physiological responses [18,19]. Additional theories propose that Eye Movement Desensitization and Reprocessing (EMDR) therapy may enhance interhemispheric interaction, mimic the effects of Rapid Eye Movement (REM) sleep, or fatigue the working memory. These mechanisms are thought to contribute to alterations in the recall of traumatic memories, aiding in their processing and the reduction in trauma-related symptoms [20,21,22,23,24,25,26]. However, the precise mechanisms behind its efficacy remain inconclusive. Recently, Baek et al. reported that EMDR can reduce amygdala activation [27], and De Jongh et al. support that the bilateral stimulation used in EMDR sends inhibitory signals to the amygdala, potentially mitigating emotional responses [28]. Recently, our laboratory presented the first histological report detailing the effects of EMDR. Our findings indicate that visual EMDR stimulation could mitigate hippocampal atrophy during exposure to acute variable stress [29].
Despite its potential, the feasibility of implementing EMDR among individuals with SUD has not been thoroughly researched, and findings regarding its effectiveness are still unclear. Consequently, the utility of EMDR sessions in reducing cravings among this population remains questionable. Therefore, the objective of this study was to assess the research that has integrated EMDR to determine its effectiveness in reducing cravings and to explore the relationship between EMDR therapy and craving reduction in individuals with SUD.
2. Materials and Methods
The meta-analysis was developed based on the PROSPERO (CRD42024531371) on 23 April 2024. The search strategy for each database was developed in accordance with the research question, adhering to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [30] and WorkBooks of Meta-Essentials [31].
2.1. Search Strategy
They were collected from previously published studies that obtained approval from ethical committees. Two independent authors (D.E.M.-F., A.P.G.-P.) searched the Web of Science and PubMed from database inception to 1 February 2024. The search strategy was crafted using a combination of Medical Subject Headings (MeSH) terms and various free-text keywords. Additionally, we enhanced our electronic database searches by reviewing reference lists from pertinent review articles and implemented a forward citation-tracking process for key papers in the field. The primary search was to identify articles that had used EMDR to treat patients with substance use disorder, specifically craving. Therefore, the search key words used were based on terms related to “EMDR” AND “Addiction” OR “Addicted” OR “Substance use” OR “Substance abuse”, OR “Drug” in the title, abstract or index term fields. The detailed search is shown in Table 1.

Table 1.
Comprehensive search strategy for articles on EMDR treatment of craving in patients with substance use disorder.
2.2. Inclusion and Exclusion Criteria
We included all studies that evaluated the effect of EMDR on individual with SUD and assessed craving levels in the meta-analysis. Only studies reporting measurable quantitative outcomes, such as performance measures or tests, were considered. If the abstract lacked sufficient information for inclusion, the full text was reviewed. The analysis was restricted to studies published in English. Exclusions included letters to the editor, clinical cases, commentaries, systematic reviews, qualitative studies, short communications, and meta-analyses. Additionally, if the mean and standard deviation were missing from a graph or table, attempts were made to contact the authors for the necessary data. Any full-text publications that were inaccessible, and for which no response was obtained from the corresponding author after two email attempts, were also excluded; see Table 2.
Table 2.
Summary of studies excluded from the meta-analysis assessing the impact of EMDR therapy on craving in substance use disorder populations.
2.3. Data Extraction
Two authors (D.E.M.-F., A.P.G.-P.) independently screened and identified eligible papers by title, abstract, and full text against prespecified criteria. After the selection process (see Figure 1), relevant data from the selected studies were extracted to an Excel sheet. The researchers independently coded the studies for the variables of interest: first author, year, publication venue, design classification, total sample size, sample size for each group and measure, sample age, primary measure, study location by country, treatment description, number of EMDR sessions, and effect size information. Finally, the effect size calculations were performed by a single researcher in collaboration with the other two researchers who provided input and guidance on decisions when the information presented in the studies was unclear or ambiguous.
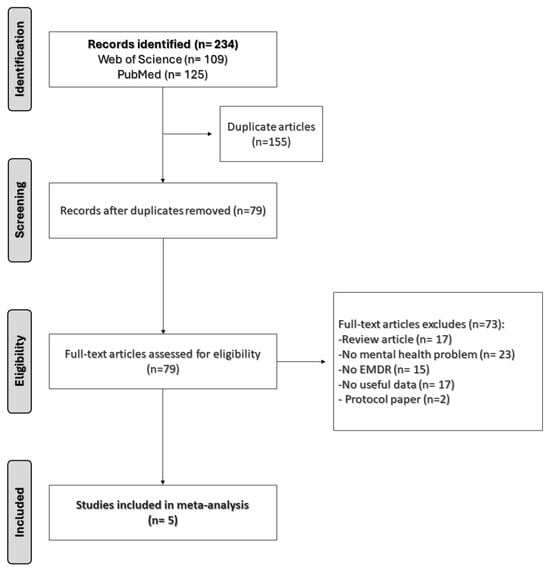
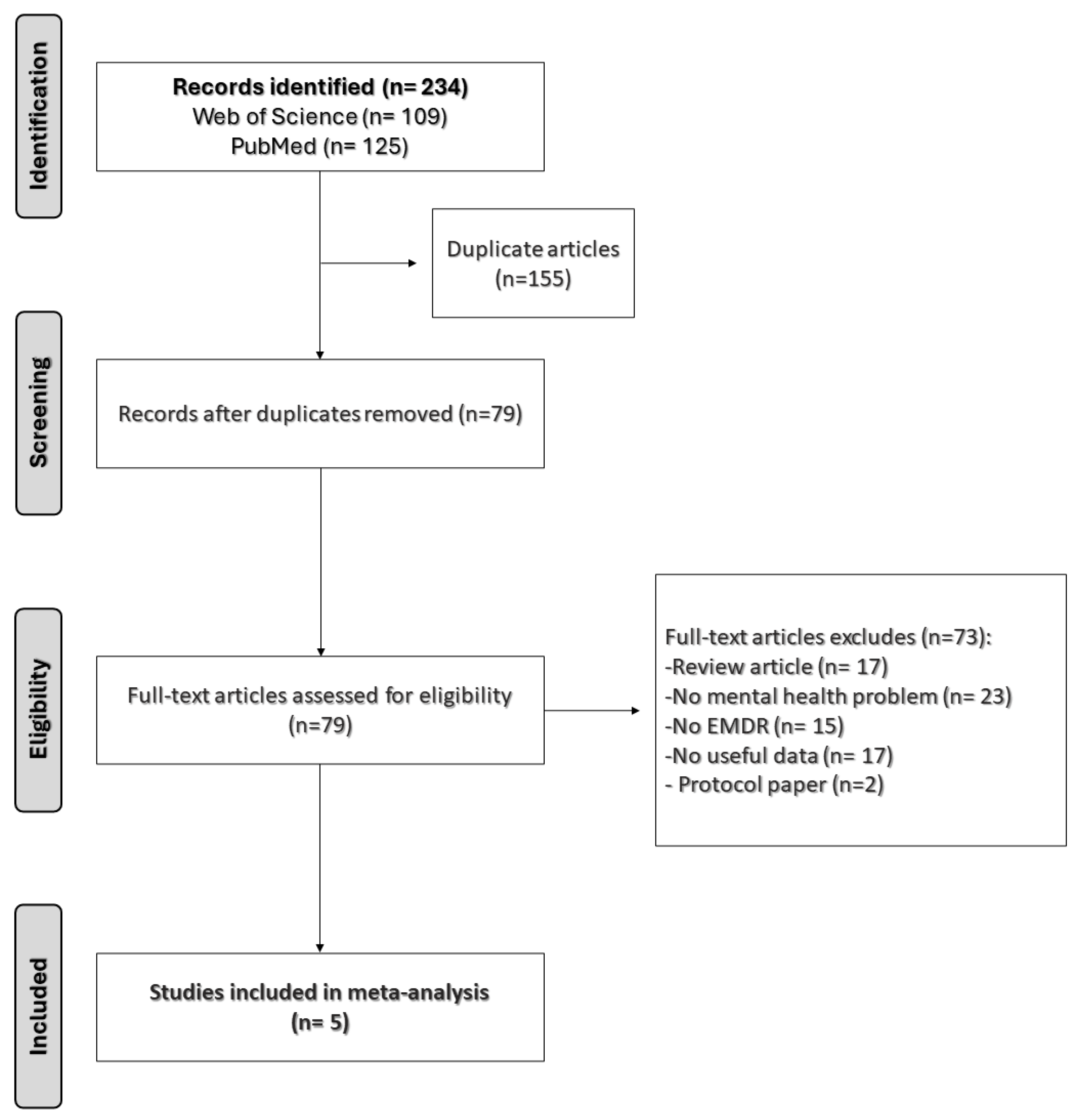
Figure 1.
Flow diagram of study selection process [32,33,34,35].
2.4. Risk of Bias-2
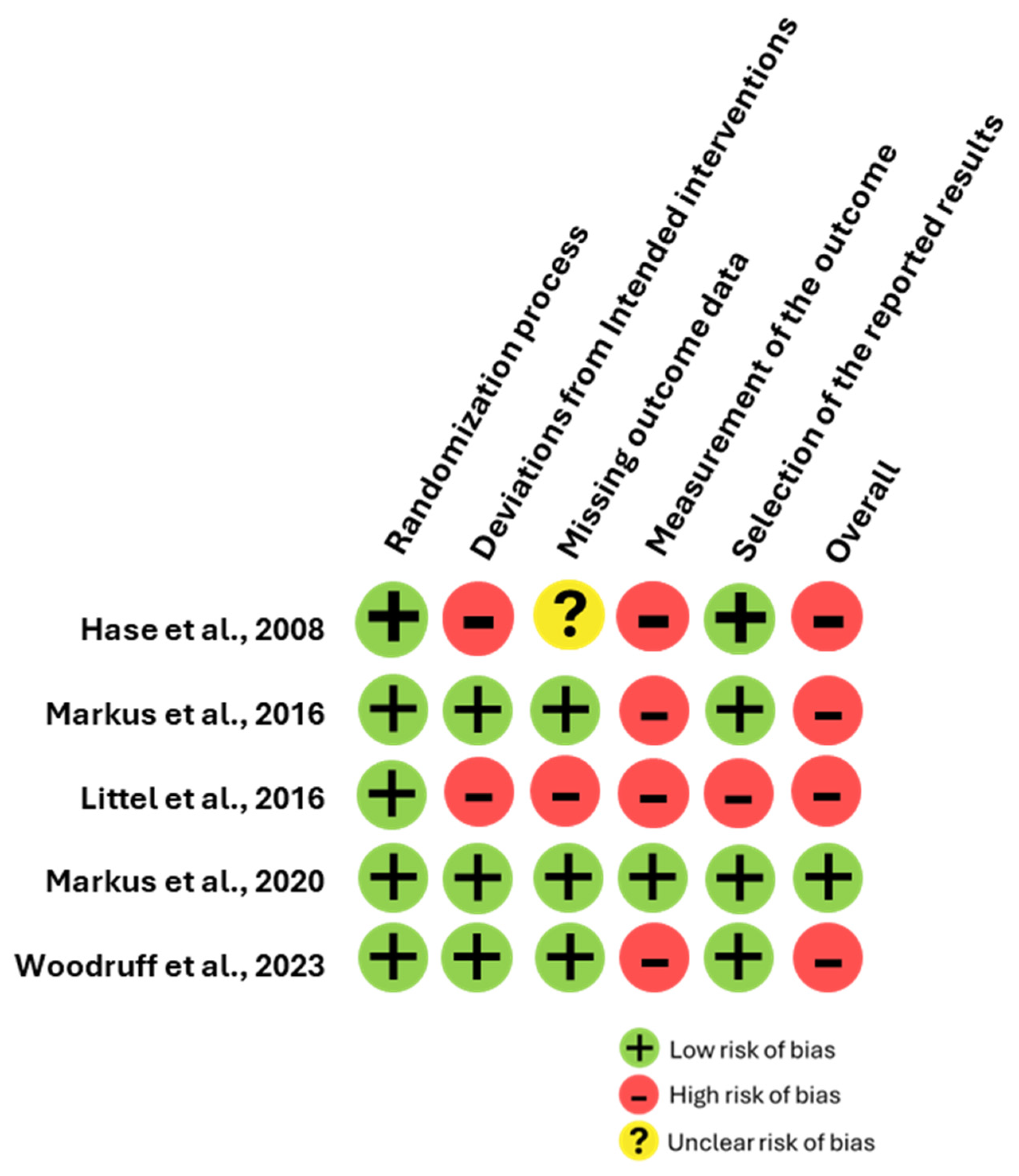
The assessment of risk of bias (RoB-2) was conducted by two independent researchers, I.G.A.-G. and J.G.-E., with a third researcher, D.F.-Q., available for mediation if needed. However, mediation was unnecessary due to consistent agreement among the reviewers. The authors utilized the Cochrane Risk of Bias-2 (RoB-2) tool [36] to evaluate the quality of the research. This tool assesses risk across five distinct domains: (1) randomization process, (2) deviations from the planned intervention, (3) missing outcome data, (4) outcome measurement, and (5) selection of reported results. Each domain is rated on three levels of risk: high, some concerns, and low, which is based on signaling questions within that domain. The overall risk of bias for the study is determined by integrating the evaluations from these domains to form a comprehensive view. A study is typically classified as having a high risk of bias if any domain is rated as high risk or if multiple domains are assessed as having some concerns. Conversely, a study is considered to have a low risk of bias if all domains are rated as low risk. If only a few domains have some concerns, the study is regarded as having some concerns overall.
2.5. Data Analysis
Both random and fixed effects models were used to pool the estimate of the EMDR effects on craving in individuals with SUD. To calculate pooled effect sizes, an R language (version 4.1.2, http://www.Rproject.org, accessed on 1 April 2024) R “meta” package was employed (Supplementary S1: analytic code in R). We calculated the mean difference (MD), and then the pooled SD is calculated to reflect the shared variability between the groups, while the standard error (SE) is obtained by multiplying the pooled SD by the square root of the sum of the inverse of the sample sizes from each group. The standardized mean difference (SMD) is determined by dividing the MD by the pooled SD, and it represents Cohen’s d. Given the tendency of small sample sizes to overestimate the overall effect size, Hedges’ g is applied as an adjustment to provide a more accurate estimation [37]; see Table 3. The I2 statistic was used to measure the degree of heterogeneity caused by variability in the true effect size. The effect sizes of g = 0.20 are small, g = 0.50 as moderate and g = 0.80 as large [28]. Forest plots were created by the meta, metadata, metafor and rmeta function of meta packages, and funnel plots were constructed by the funnel function to estimate the publication bias.
Table 3.
Detailed compilation of extracted data from studies researching EMDR therapy’s efficacy in reducing craving among substance use disorder patients.
3. Results
In this meta-analysis, we evaluated the efficacy of Eye Movement Desensitization and Reprocessing therapy on craving reduction in patients with substance use disorder. The strategy search identified 234 records, and the analysis incorporated findings from five studies, which were uniformly distributed between experimental (134 participants) and control groups (132 participants). The PRISMA diagram in Figure 1 shows the study selection process for this study.
3.1. Study Characteristics
The studies were published between 2008 and 2023 with a sample size ranging from 30 to 109 participants in each study. The samples were aged between 18 and 59 years old with the average age of patients ranging from 23.4 to 47.1. The studies included an active control group with distinct types of psychotherapy including cognitive behavioral therapy (CBT), eye movement (EM), exposure, and finger tapping. The application time for EMDR in all studies varied widely from 24 s to 1.5 h for each session or set, up to twice a week, and the total amount of sessions ranged from two to seven sessions. Craving was assessed in the studies included in this meta-analysis using several validated instruments. Specifically, the Obsessive-Compulsive Drinking Scale (OCDS) was utilized to evaluate obsessive thoughts and compulsive behaviors related to alcohol consumption, offering insights into the cognitive dimensions of craving. The Visual Analog Scale (VAS) was employed, enabling participants to rate the intensity of their craving on a continuum, which facilitated a straightforward quantification of their subjective experiences. Additionally, the Penn Alcohol Craving Scale (PACS) was incorporated to capture various dimensions of alcohol craving, focusing on both its frequency and intensity. Lastly, the Brief Substance Craving Scale (BSCS) was used for its efficiency in measuring overall craving for substances. The characteristics of the selected studies are summarized and presented in Table 4.
Table 4.
Summarized characteristics of the studies.
3.2. Effect of EMDR Therapy on Craving Reduction in Substance Use Disorder
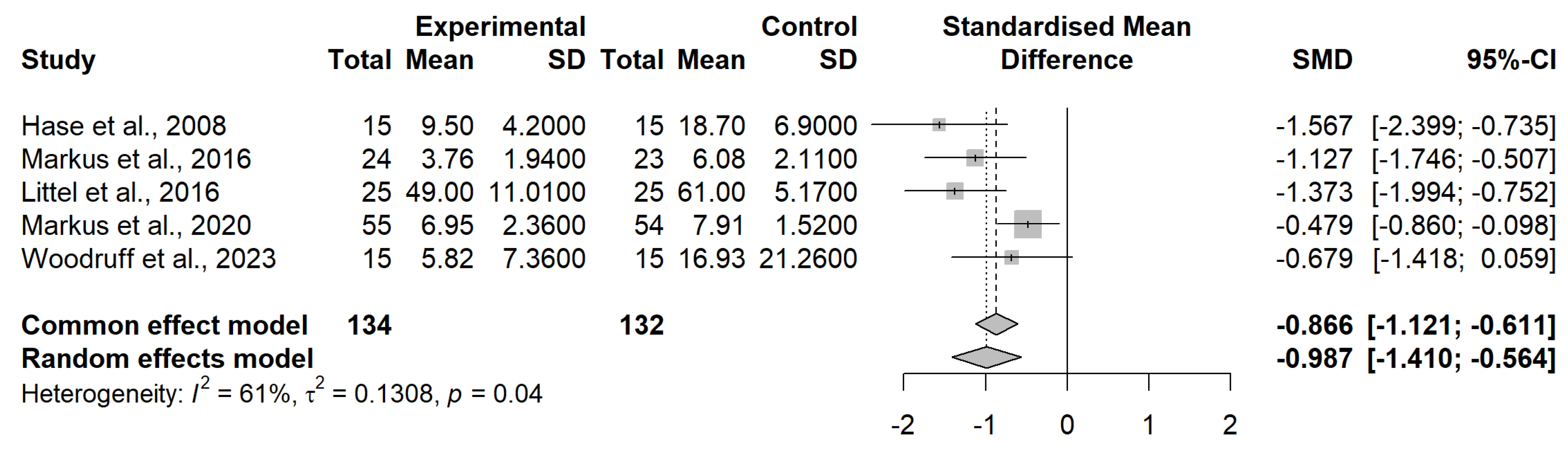
The results revealed a significant reduction in craving among patients receiving EMDR therapy. Specifically, under the common effect model, the SMD was −0.866 with a 95% confidence interval ranging from −1.121 to −0.611 (z = −6.66, p < 0.0001). The random effects model, which accounts for variability among studies, indicated a slightly larger effect size (SMD = −0.987) with a 95% confidence interval from −1.410 to −0.564 (z = −4.57, p < 0.0001).
Regarding the heterogeneity among the included studies, it was found to be moderate to high, I2 of 60.7%, indicating a moderate to high variation in effect sizes. The tau2 value was 0.3616, indicating moderate between-study variance, while the heterogeneity test (Q = 10.17, df = 4, I2 = 60.7%, p = 0.0376) was statistical significantly, suggesting that the observed variability could be attributed to the studies, as shown in Figure 2.
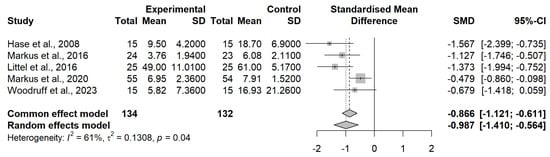
Figure 2.
Forest plot. Negative values indicate less craving symptoms in the EMDR intervention than the control condition.
3.3. Sensitivity Analysis
A sensitivity analysis was conducted sequentially excluding each individual study to evaluate their impact on the combined effect size. The findings indicated that the overall effect size remained relatively stable with individual study effect sizes varying between SMD = −0.7633 and −1.1805. This consistency supports the robustness and dependability of the meta-analysis results.
3.4. Publication Bias
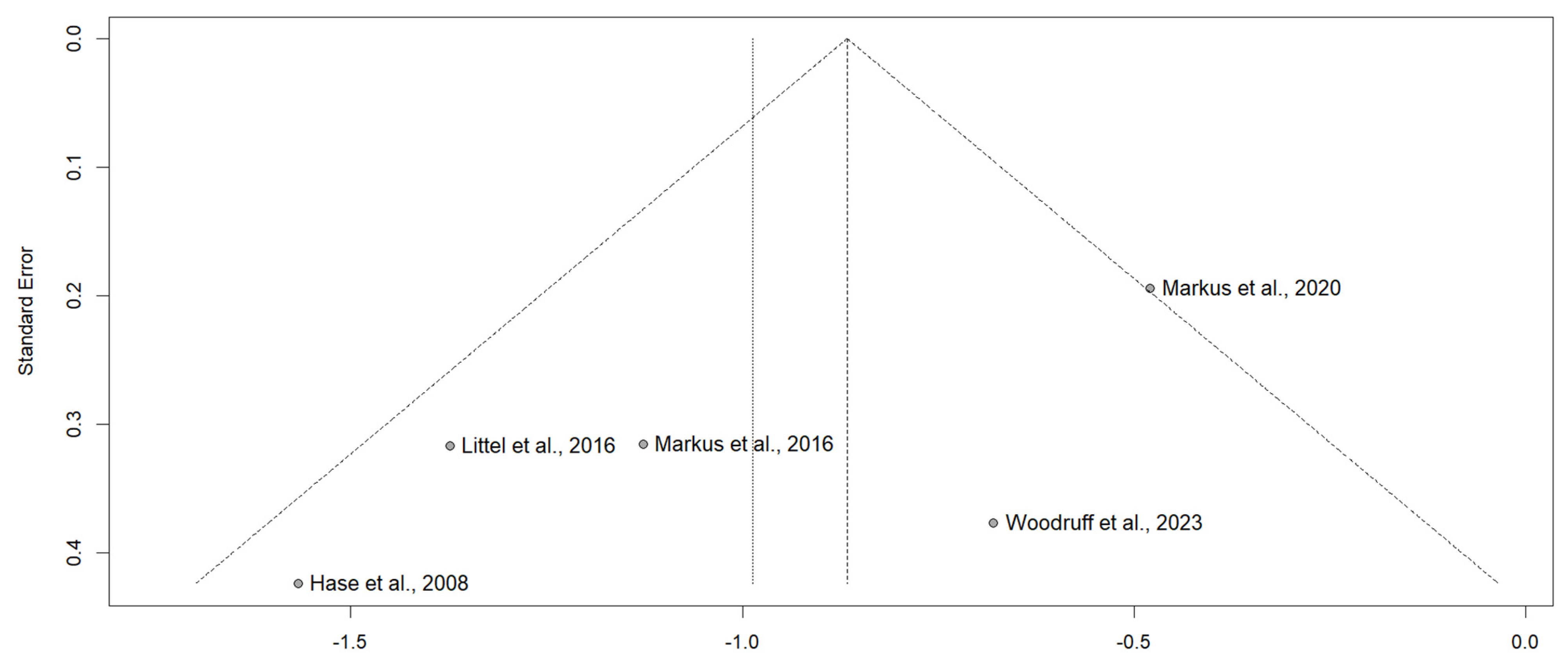
The funnel plot analysis revealed three studies positioned in the lower left quadrant and two studies in the right quadrant, suggesting some degree of symmetry; see Figure 3. However, given the small sample size of only five studies and their moderate heterogeneity, the risk of false positives in the meta-analysis is elevated, which can impact the interpretation of the funnel plot’s symmetry. Furthermore, the Rob-2 assessment indicated that most studies have a high risk of bias, which adds another layer of complexity to the findings; see Figure 4.
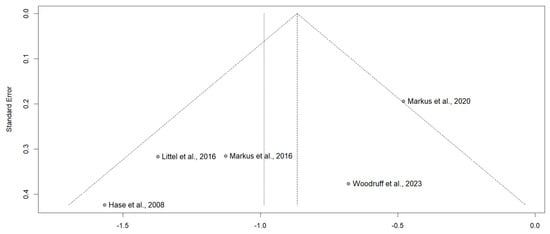
Figure 3.
Funnel plot.
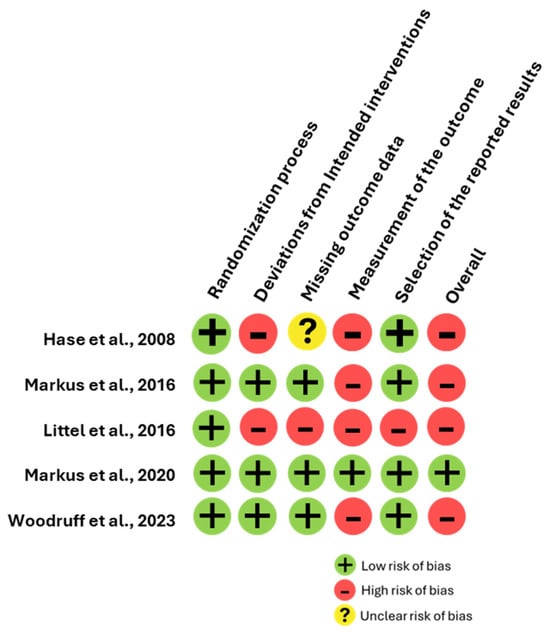
Figure 4.
Cochrane Risk-of-Bias tool for randomized trials version 2 (RoB-2). In this color-coded ranking, green color represents low risk of bias, yellow unclear risk of bias, and red high risk of bias.
4. Discussion
A total of 266 participants were included in this meta-analysis to determine the effectiveness of EMDR on craving reduction in patients with substance use disorder. The results indicate that EMDR therapy significantly reduces craving compared with control conditions. The overall effects size indicates that EMDR therapy had a significant effect on decreasing craving. However, there was a significant moderate heterogeneity among the included studies indicating that the effect of EMDR on craving reduction may vary depending on study-specific factors. Therefore, these results should be interpreted with some caution.
While EMDR appears to be generally effective in reducing cravings, the variability between studies suggests that the magnitude of this effect might differ across different contexts or populations. This level of heterogeneity could stem from differences in study design, participant characteristics, or variations in how cravings were measured across studies. For instance, slight variations in the implementation of EMDR protocols or differences in the severity of substance use disorders among participants could contribute to this variability. Additionally, the number of studies included (n = 5) is relatively small, which can sometimes lead to an overestimation of heterogeneity. The moderate level of heterogeneity does not undermine the overall findings but highlights the need for future studies to explore these differences more thoroughly.
Although the funnel plot did not indicate significant publication bias, it is important to recognize that the absence of visual asymmetry does not entirely eliminate the possibility of such bias. However, publication bias may still exist, particularly if smaller studies with non-significant or negative results are underreported or excluded from publication, potentially distorting the overall evidence. This is why the RoB-2 assessment indicated that most studies have a high risk of bias. Also, in research fields where positive findings are more frequently published, there is a possibility that the perceived impact of EMDR on craving reduction could be overstated. While the funnel plot provides some reassurance, caution should be exercised in interpreting these results. The potential omission of studies with null or negative findings suggests that the true effect size may be smaller than our analysis indicates. Consequently, it is essential for future research to address this issue by ensuring a comprehensive reporting of all study outcomes regardless of their statistical significance.
Furthermore, the beneficial effects of EMDR are primarily linked to bilateral sensory stimulation, which is typically triggered by the therapist’s hand movements that prompt lateral eye movements in patients as they recall distressing memories. This form of bilateral stimulation is thought to enhance information processing and promote an adaptive consolidation of memories. Consequently, it helps diminish emotional distress and promote psychological resilience. This mechanism is believed to underlie the effectiveness of EMDR in alleviating psychological stress and enhancing mental health recovery [38,39,40]. Interestingly, EMDR therapy has been shown to diminish both the vividness and the emotional intensity of positively charged memories [41,42] and even images of potential future events (flash-forwards) [43,44,45], suggesting that EMDR could be effectively used to treat a range of psychopathologies where maladaptive memories and mental imagery are significant factors, such as in cases of substance abuse disorders. The ability of EMDR to modulate the emotional response associated with both negative and positive memories indicates its potential as a versatile therapeutic tool in diverse clinical settings.
In addictive disorders, the act of recalling substance-related memories plays a crucial role in triggering cravings. These cravings are a significant factor in the continuation of substance use and notably increase the risk of relapse. The vividness and emotional intensity of these memories can strongly influence an individual’s ongoing struggle with addiction [46,47]. These memories include both classical and instrumental associations, for example, the links between stress and smoking or smoking and relaxation as well as episodic memories. Episodic memories in this context might involve recalling the first time a substance was used, the consequences of substance use, and experiences related to losing control or relapsing. This comprehensive memory framework plays a pivotal role in how cravings are triggered and managed, impacting the cycle of addiction and recovery efforts [48,49]. Cravings are frequently intensified by sensory imagery, which may involve visualizing the substance, imagining its smell, or anticipating future use. This type of vivid mental imagery can make the craving more acute, effectively reinforcing the desire to use the substance and making it harder for individuals to resist the impulse to relapse [47,50].
Craving reduction can be effectively facilitated through dual-task procedures. Research indicates that when individuals engage in imagery or visuospatial tasks that are unrelated to substance use during moments of intense craving, there is a significant decrease in both the frequency and intensity of these cravings. This method distracts the brain, diverting attention from substance-related thoughts and reducing the overall craving experience [51]. This concurrent cognitive activity serves as an effective coping mechanism to manage the acute effects of cravings and can be seamlessly integrated into clinical practice. To implement this method, individuals experiencing cravings are encouraged to engage in a dual task [52]. This could involve simultaneously performing a cognitive task that requires attention, such as solving a puzzle or engaging in a memory game, while experiencing craving episodes. This distraction helps mitigate the intensity of the cravings by occupying the mind with alternative stimuli, reducing the focus on the desire to use the substance. However, the effectiveness of this approach hinges on the ability of individuals with substance dependencies to recognize the onset of cravings while they are still manageable. Early recognition allows for timely intervention with dual-task activities, preventing cravings from escalating to a level that is more challenging to control [53]. In addition, EMDR treatment has been observed to positively influence emotion regulation. As a result, it facilitates the upregulation of positive and desirable emotions, making them more readily expressed [38].
Research on the full application of EMDR therapy specifically for addiction treatment remains limited. Most studies have primarily concentrated on the use of EMDR to address traumatic memories in individuals who have comorbid PTSD [54,55] and not on memory representations or sensory imagery constituting substance craving and dependence itself [56]. Despite a considerable volume of literature on EMDR and dependency disorders, most of these publications are case studies, proposed protocols for future research, theoretical discussions, or studies that do not specifically focus on substance use disorders. This indicates that while there is growing interest and theoretical backing for using EMDR in the context of dependency, there is a scarcity of rigorous empirical research directly investigating its effectiveness in treating substance use disorders. This lack of focused research underscores the need for well-designed studies to evaluate EMDR’s efficacy specifically in the realm of addiction treatment.
Future research should focus on larger sample sizes and extended follow-up periods to enhance the quality of evidence regarding the long-term benefits of EMDR for individuals with SUD. It is crucial to minimize bias by ensuring rigorous randomization procedures and conducting pretest equivalence checks between groups. Additionally, maintaining robust sample sizes is essential, particularly as follow-up assessments often see reduced participation. Researchers should account for potential attrition by planning for adequate sample sizes and implementing strategies to sustain participant involvement throughout the study. Furthermore, it is important for researchers to thoroughly report potential moderating or confounding variables, including demographic factors (e.g., age, gender, ethnicity) and methodological details (e.g., baseline assessments, measurement reliabilities, specific memory types addressed, treatment duration, EMDR protocols, and any adaptations).
5. Conclusions
These findings suggest that EMDR therapy may have potential benefits in reducing cravings among individuals with substance abuse disorders. However, it is important to acknowledge several limitations in interpreting these results. Variability in study designs and differences in participant demographics could impact the generalizability of our findings. Additionally, the small number of studies included in the analysis limits the strength of our conclusions. These factors highlight the need for further research with larger and more diverse populations to better understand and confirm the effectiveness of EMDR in treating substance abuse disorders.
Supplementary Materials
The following supporting information can be downloaded at https://www.mdpi.com/article/10.3390/brainsci14111110/s1, S1: analytic code in R.
Author Contributions
Design and conceptualization, D.F.-Q., D.E.M.-F. and S.L.; methodology and formal analysis, D.F.-Q., D.E.M.-F., A.P.G.-P., I.G.A.-G. and J.G.-E.; writing (original draft preparation), D.F.-Q. and D.E.M.-F.; writing (review and editing), D.E.M.-F., A.P.G.-P., I.G.A.-G., S.L., J.G.-E. and D.F.-Q.; supervision, D.F.-Q. All authors have read and agreed to the published version of the manuscript.
Funding
Open Access Funding by UDG, Universidad de Guadalajara, Centro Universitario de Ciencias de la Salud, CUCS.
Institutional Review Board Statement
This study was employed in accordance with the guidelines in the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement, and the protocol of the review was registered in the International Prospective Register of Systematic Reviews (PROSPERO) (registration number CRD42024531371). Ethical committee approval for this study was not required.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data extracted from the included studies and the analytic code are available.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Castaldelli-Maia, J.M.; Bhugra, D. Analysis of Global Prevalence of Mental and Substance Use Disorders within Countries: Focus on Sociodemographic Characteristics and Income Levels. Int. Rev. Psychiatry 2022, 34, 6–15. [Google Scholar] [CrossRef] [PubMed]
- Ventura, A.S.; Bagley, S.M. To Improve Substance Use Disorder Prevention, Treatment and Recovery: Engage the Family. J. Addict. Med. 2017, 11, 339–341. [Google Scholar] [CrossRef] [PubMed]
- Franco, S.; Olfson, M.; Wall, M.M.; Wang, S.; Hoertel, N.; Blanco, C. Shared and Specific Associations of Substance Use Disorders on Adverse Outcomes: A National Prospective Study. Drug Alcohol. Depend. 2019, 201, 212–219. [Google Scholar] [CrossRef]
- World Health Organization Public Health Dimension of the World Drug Problem. Available online: https://apps.who.int/gb/ebwha/pdf_files/WHA71/A71_41Rev2-en.pdf (accessed on 2 May 2024).
- INEGI Estadísticas a Propósito Del Día Internacional de La Lucha Contra El Uso Indebido y El Tráfico Ilícito de Drogas. Available online: https://www.inegi.org.mx/contenidos/saladeprensa/aproposito/2023/EAP_DROGAS23.pdf (accessed on 4 March 2023).
- INEGI Salud Mental. Instituto Nacional de Estadística y Geografía. Available online: https://www.inegi.org.mx/temas/salud/#Informacion_general (accessed on 25 July 2023).
- Koob, G.F.; Le Moal, M. Addiction and the Brain Antireward System. Annu. Rev. Psychol. 2008, 59, 29–53. [Google Scholar] [CrossRef]
- Nwonu, C.N.S.; Nwonu, P.C.; Ude, R.A. Neurobiological Underpinnings in Drug Addiction. West. Afr. J. Med. 2022, 39, 874–884. [Google Scholar]
- Volkow, N.D.; Michaelides, M.; Baler, R. The Neuroscience of Drug Reward and Addiction. Physiol. Rev. 2019, 99, 2115–2140. [Google Scholar] [CrossRef]
- Koob, G.F. Addiction Is a Reward Deficit and Stress Surfeit Disorder. Front. Psychiatry 2013, 4, 72. [Google Scholar] [CrossRef]
- Tiffany, S.T.; Wray, J.M. The Clinical Significance of Drug Craving. Ann. N. Y Acad. Sci. 2012, 1248, 1–17. [Google Scholar] [CrossRef]
- Sayette, M.A. The Role of Craving in Substance Use Disorders: Theoretical and Methodological Issues. Annu. Rev. Clin. Psychol. 2016, 12, 407–433. [Google Scholar] [CrossRef]
- *Littel, M.; van den Hout, M.A.; Engelhard, I.M. Desensitizing Addiction: Using Eye Movements to Reduce the Intensity of Substance-Related Mental Imagery and Craving. Front. Psychiatry 2016, 7, 14. [Google Scholar] [CrossRef]
- Levitt, E.E.; Sousa, S.; Costello, M.J.; LaBelle, O.P.; Rush, B.; MacKillop, J. The Clinical Relevance of Impulsivity in Substance Use Disorder Treatment: Examining Within-Treatment Changes and Relationship to Psychiatric Symptoms and Cravings in a Large Inpatient Sample. J. Stud. Alcohol. Drugs 2023, 84, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Vafaie, N.; Kober, H. Association of Drug Cues and Craving With Drug Use and Relapse: A Systematic Review and Meta-Analysis. JAMA Psychiatry 2022, 79, 641–650. [Google Scholar] [CrossRef] [PubMed]
- Bresin, K.; Verona, E. Craving and Substance Use: Examining Psychophysiological and Behavioral Moderators. Int. J. Psychophysiol. 2021, 163, 92–103. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, F. Efficacy of the Eye Movement Desensitization Procedure in the Treatment of Traumatic Memories. J. Trauma. Stress. 1989, 2, 199–223. [Google Scholar] [CrossRef]
- Wilson, D.L.; Silver, S.M.; Covi, W.G.; Foster, S. Eye Movement Desensitization and Reprocessing: Effectiveness and Autonomic Correlates. J. Behav. Ther. Exp. Psychiatry 1996, 27, 219–229. [Google Scholar] [CrossRef]
- Andrade, J.; Kavanagh, D.; Baddeley, A. Eye-Movements and Visual Imagery: A Working Memory Approach to the Treatment of Post-Traumatic Stress Disorder. Br. J. Clin. Psychol. 1997, 36, 209–223. [Google Scholar] [CrossRef]
- Christman, S.D.; Garvey, K.J.; Propper, R.E.; Phaneuf, K.A. Bilateral Eye Movements Enhance the Retrieval of Episodic Memories. Neuropsychology 2003, 17, 221–229. [Google Scholar] [CrossRef]
- Parker, A.; Relph, S.; Dagnall, N. Effects of Bilateral Eye Movements on the Retrieval of Item, Associative, and Contextual Information. Neuropsychology 2008, 22, 136–145. [Google Scholar] [CrossRef]
- Propper, R.E.; Pierce, J.; Geisler, M.W.; Christman, S.D.; Bellorado, N. Effect of Bilateral Eye Movements on Frontal Interhemispheric Gamma EEG Coherence: Implications for EMDR Therapy. J. Nerv. Ment. Dis. 2007, 195, 785–788. [Google Scholar] [CrossRef]
- Stickgold, R. EMDR: A Putative Neurobiological Mechanism of Action. J. Clin. Psychol. 2002, 58, 61–75. [Google Scholar] [CrossRef]
- Gunter, R.W.; Bodner, G.E. How Eye Movements Affect Unpleasant Memories: Support for a Working-Memory Account. Behav. Res. Ther. 2008, 46, 913–931. [Google Scholar] [CrossRef] [PubMed]
- Raboni, M.R.; Alonso, F.F.D.; Tufik, S.; Suchecki, D. Improvement of Mood and Sleep Alterations in Posttraumatic Stress Disorder Patients by Eye Movement Desensitization and Reprocessing. Front. Behav. Neurosci. 2014, 8, 209. [Google Scholar] [CrossRef]
- Smeets, M.A.M.; Dijs, M.W.; Pervan, I.; Engelhard, I.M.; van den Hout, M.A. Time-Course of Eye Movement-Related Decrease in Vividness and Emotionality of Unpleasant Autobiographical Memories. Memory 2012, 20, 346–357. [Google Scholar] [CrossRef]
- Baek, J.; Lee, S.; Cho, T.; Kim, S.-W.; Kim, M.; Yoon, Y.; Kim, K.K.; Byun, J.; Kim, S.J.; Jeong, J.; et al. Neural Circuits Underlying a Psychotherapeutic Regimen for Fear Disorders. Nature 2019, 566, 339–343. [Google Scholar] [CrossRef]
- de Jongh, A.; Amann, B.L.; Hofmann, A.; Farrell, D.; Lee, C.W. The Status of EMDR Therapy in the Treatment of Posttraumatic Stress Disorder 30 Years After Its Introduction. J. EMDR Pract. Res. 2019, 13, 261–269. [Google Scholar] [CrossRef]
- Ruvalcaba-Delgadillo, Y.; Martínez-Fernández, D.E.; Luquin, S.; Moreno-Alcázar, A.; Redolar-Ripoll, D.; Jauregui Huerta, F.; Fernández-Quezada, D. Visual EMDR Stimulation Mitigates Acute Varied Stress Effects on Morphology of Hippocampal Neurons in Male Wistar Rats. Front. Psychiatry 2024, 15, 1396550. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Suurmond, R.; van Rhee, H.; Hak, T. Introduction, Comparison, and Validation of Meta-Essentials: A Free and Simple Tool for Meta-Analysis. Res. Synth. Methods 2017, 8, 537–553. [Google Scholar] [CrossRef]
- Hase, M.; Schallmayer, S.; Sack, M. EMDR Reprocessing of the Addiction Memory: Pretreatment, Posttreatment, and 1-Month Follow-Up. J. EMDR Pract. Res. 2008, 2, 170–179. [Google Scholar] [CrossRef]
- Markus, W.; de Weert-van Oene, G.H.; Becker, E.S.; DeJong, C.A.J. A Multi-Site Randomized Study to Compare the Effects of Eye Movement Desensitization and Reprocessing (EMDR) Added to TAU versus TAU to Reduce Craving and Drinking Behavior in Alcohol Dependent Outpatients: Study Protocol. BMC Psychiatry 2015, 15, 51. [Google Scholar] [CrossRef]
- Markus, W.; Hornsveld, H.K.; Burk, W.J.; de Weert-van Oene, G.H.; Becker, E.S.; DeJong, C.A.J. Addiction-Focused Eye Movement Desensitization and Reprocessing Therapy as an Adjunct to Regular Outpatient Treatment for Alcohol Use Disorder: Results From a Randomized Clinical Trial. Alcohol. Clin. Exp. Res. 2020, 44, 272–283. [Google Scholar] [CrossRef] [PubMed]
- Woodruff, E.; Park, J.; Howard, H.; Gonzalez, M.; Jaber, T. Feasibility and Efficacy of Addiction-Focused Eye Movement Desensitization Reprocessing in Adults with Substance Use Disorder. J. Evid. Based Soc. Work 2023, 21, 282–299. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Hedges, L.V.; Olkin, I. Statistical Methods for Meta-Analysis. Available online: https://www.sciencedirect.com/book/9780080570655/statistical-methods-for-meta-analysis (accessed on 16 April 2024).
- Carletto, S.; Oliva, F.; Barnato, M.; Antonelli, T.; Cardia, A.; Mazzaferro, P.; Raho, C.; Ostacoli, L.; Fernandez, I.; Pagani, M. EMDR as Add-On Treatment for Psychiatric and Traumatic Symptoms in Patients with Substance Use Disorder. Front. Psychol. 2017, 8, 2333. [Google Scholar] [CrossRef]
- Novo Navarro, P.; Landin-Romero, R.; Guardiola-Wanden-Berghe, R.; Moreno-Alcázar, A.; Valiente-Gómez, A.; Lupo, W.; García, F.; Fernández, I.; Pérez, V.; Amann, B.L. 25 Years of Eye Movement Desensitization and Reprocessing (EMDR): The EMDR Therapy Protocol, Hypotheses of Its Mechanism of Action and a Systematic Review of Its Efficacy in the Treatment of Post-Traumatic Stress Disorder. Rev. Psiquiatr. Salud Ment. 2018, 11, 101–114. [Google Scholar] [CrossRef]
- Shapiro, F. The Role of Eye Movement Desensitization and Reprocessing (EMDR) Therapy in Medicine: Addressing the Psychological and Physical Symptoms Stemming from Adverse Life Experiences. Perm. J. 2014, 18, 71–77. [Google Scholar] [CrossRef]
- Hornsveld, H.K.; Houtveen, J.H.; Vroomen, M.; Kapteijn, I.; Aalbers, D.; Hout, M.A. van den Evaluating the Effect of Eye Movements on Positive Memories Such as Those Used in Resource Development and Installation. J. EMDR Pract. Res. 2011, 5, 146–155. [Google Scholar] [CrossRef]
- Engelhard, I.M.; van Uijen, S.L.; van den Hout, M.A. The Impact of Taxing Working Memory on Negative and Positive Memories. Eur. J. Psychotraumatol. 2010, 1, 5623. [Google Scholar] [CrossRef]
- Engelhard, I.M.; van den Hout, M.A.; Janssen, W.C.; van der Beek, J. Eye Movements Reduce Vividness and Emotionality of “Flashforwards”. Behav. Res. Ther. 2010, 48, 442–447. [Google Scholar] [CrossRef]
- Engelhard, I.M.; van den Hout, M.A.; Dek, E.C.P.; Giele, C.L.; van der Wielen, J.-W.; Reijnen, M.J.; van Roij, B. Reducing Vividness and Emotional Intensity of Recurrent “Flashforwards” by Taxing Working Memory: An Analogue Study. J. Anxiety Disord. 2011, 25, 599–603. [Google Scholar] [CrossRef]
- Engelhard, I.M.; van den Hout, M.A.; Smeets, M.A.M. Taxing Working Memory Reduces Vividness and Emotional Intensity of Images about the Queen’s Day Tragedy. J. Behav. Ther. Exp. Psychiatry 2011, 42, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Killen, J.D.; Fortmann, S.P. Craving Is Associated with Smoking Relapse: Findings from Three Prospective Studies. Exp. Clin. Psychopharmacol. 1997, 5, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Goodyear, K. Multisensory Environments to Measure Craving During Functional Magnetic Resonance Imaging. Alcohol Alcohol. 2019, 54, 193–195. [Google Scholar] [CrossRef] [PubMed]
- Müller, C.P. Episodic Memories and Their Relevance for Psychoactive Drug Use and Addiction. Front. Behav. Neurosci. 2013, 7, 34. [Google Scholar] [CrossRef] [PubMed]
- Goodman, J.; Packard, M.G. Memory Systems and the Addicted Brain. Front. Psychiatry 2016, 7, 24. [Google Scholar] [CrossRef]
- Andrade, J.; May, J.; Kavanagh, D. Sensory Imagery in Craving: From Cognitive Psychology to New Treatments for Addiction. J. Exp. Psychopathol. 2012, 3, 127–145. [Google Scholar] [CrossRef]
- Kemps, E.; Tiggemann, M. A Role for Mental Imagery in the Experience and Reduction of Food Cravings. Front. Psychiatry 2015, 5, 193. [Google Scholar] [CrossRef]
- Garavan, H.; Hester, R. The Role of Cognitive Control in Cocaine Dependence. Neuropsychol. Rev. 2007, 17, 337–345. [Google Scholar] [CrossRef]
- Schwabe, L.; Nader, K.; Pruessner, J.C. Reconsolidation of Human Memory: Brain Mechanisms and Clinical Relevance. Biol. Psychiatry 2014, 76, 274–280. [Google Scholar] [CrossRef]
- Calancie, O.G.; Khalid-Khan, S.; Booij, L.; Munoz, D.P. Eye Movement Desensitization and Reprocessing as a Treatment for PTSD: Current Neurobiological Theories and a New Hypothesis. Ann. N. Y. Acad. Sci. 2018, 1426, 127–145. [Google Scholar] [CrossRef]
- Scelles, C.; Bulnes, L.C. EMDR as Treatment Option for Conditions Other Than PTSD: A Systematic Review. Front. Psychol. 2021, 12, 644369. [Google Scholar] [CrossRef]
- Zweben, J.; Yeary, J. EMDR in the Treatment of Addiction. J. Chem. Depend. Treat. 2006, 8, 115–127. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).