
Tic-Related Obsessive–Compulsive and Eating Disorders in Dandy–Walker Variant: A Case Report and Systematic Reappraisal of Psychiatric Profiles

 ,
, 
 and
and
Abstract
1. Introduction
2. Case Presentation
2.1. Medical History
2.2. Psychiatric Presentation, Diagnosis, and Clinical Course
3. Systematic Review
3.1. Methods
3.2. Results
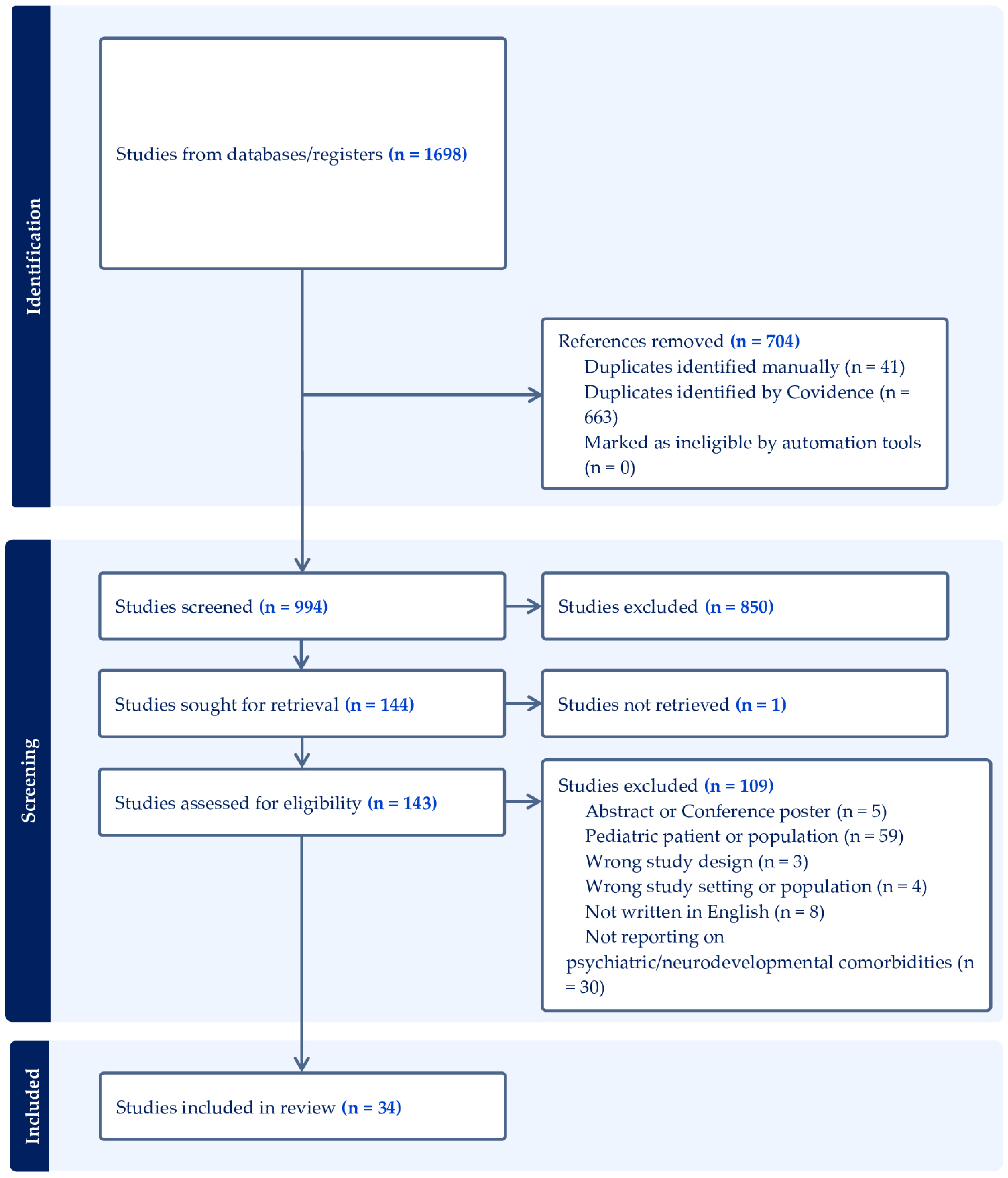
3.2.1. Study Selection

{kind=link}
{kind=link}
| Study ID | Country | Age, Gender | Neuroimaging Description | Neurodevelopmental Comorbidity | Psychiatric Comorbidity | Clinical Setting | Psychotropic Medication at Presentation | Psychotropic Medication at Discharge | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| Aune and Bugge, 2014 [21] | NO | 22, M | DWV (CT, MRI) | Cognitive impairment (WAIS-III, WISC-Revised) Learning disorder (dyslexia) Attention deficit | Schizophrenia (CE, BPRS, MINI) | Inpatient | Risperidone (1 mg/day, oral) | Risperidone (2 mg/day, oral) | Complete remission |
| Bakhla et al., 2010 [22] | IN | 24, M | DWM (CT) | - | Bipolar I disorder (CE) | Inpatient | Lithium (1350 mg/day, oral) Olanzapine (20 mg/day, oral) | Sodium valproate (1500 mg/day, oral) Carbamazepine (400 mg/day, oral) Olanzapine (15 mg/day, oral) | Complete remission |
| Balcioglu et al., 2018 [23] | TR | 36, M | MCM (MRI) | - | Psychosis NOS (CGI, MMSE, PANSS, Rorschach test) | Inpatient Compulsory | - | Risperidone (3 mg/day, oral) Quetiapine (300 mg/day, oral) | Complete remission |
| Batmaz et al., 2017 [24] | TR | 27, M | DWM (MRI) | Psychomotor delay Learning disorder Borderline cognitive functioning (WISC-Revised, WAIS) | Bipolar I disorder (YMRS, CE) | Inpatient Compulsory | Aripiprazole (30 mg/day, oral) Quetiapine (400 mg/day, oral) | Aripiprazole (30 mg/day, oral) Quetiapine (200 mg/day, oral) Sodium valproate (1000 mg/day, oral) Biperiden (4 mg/day, oral) Paliperidone palmitate (100 mg/month, IM) | Complete remission |
| Blaettner et al., 2015 [25] | AT | 19, M | DWV (MRI) | - | Delusional disorder (CE, SCID) | Inpatient | - | Ziprasidone (120 mg/day, oral) Trazodone (150 mg/day, oral) | Complete remission |
| Bout et al., 2021 [26] | MA | 20, M | DWV (MRI) | - | Schizophrenia (PANSS, CDSS) Depression | Inpatient | Risperidone (2 mg/day, oral) | Fluoxetine (20 mg/day, oral) Quetiapine (600 mg/day, oral) | Partial remission |
| Bozkurt Zincir et al., 2014 [27] | TR | 30, F | DWV (MRI) | Borderline cognitive functioning (WAIS-Revised) | Schizophrenia (CE, PANSS) | Inpatient | - | Risperidone (50 mg, depot injection) Risperidone (6 mg/day, oral) Biperiden (4 mg/day, oral) Lorazepam (2.5 mg/day, oral) | Partial remission |
| Buonaguro et al., 2014 [28] | IT | 29, F | DWM (MRI) | - | Psychosis NOS (CE, PANSS, SCID, MMSE, MMPI, BACS, WAIS-R) | Inpatient | Sodium valproate (750 mg/day, oral) Haloperidol (4 mg/day, oral) Biperiden (4 mg/day, oral) | - | - |
| Can et al., 2014 [29] | TR | 32, M | DWV (MRI) | Attention deficit, working memory deficit, learning difficulties (BGVMSS, BVMMS, WMS) | Bipolar I disorder (CE, YMRS, MMPI) | Outpatient | Lithium (dose not given, oral) Sodium valproate (dose not given, oral) Risperidone (dose not given, oral) Biperiden (dose not given, oral) | Sodium valproate (1250 mg/day, oral) Quetiapine (500 mg/day, oral) | Partial remission |
| Dawra et al., 2017 [30] | IN | 18, M | DWV (MRI) | Cognitive impairment | Psychosis NOS (CE) | Inpatient | Sodium phenytoin (100 mg, 3 times/day) Carbamezapine (200 mg, 3 times/day) | Risperidone (2 mg/day, oral); Trihexyphenidyl (2 mg/day, oral) | - |
| El Tahir et al., 2022 [31] | QA | 18, M | DWM (MRI) | Mild intellectual disability (WISC-III) | Intermittent explosive disorder (CE) | - | Topiramate (dose not given, oral) | Sodium valproate (dose not given, oral) Risperidone (dose not given, oral) | Complete remission |
| Ferentinos et al., 2007 [32] | GR | 21, F | MCM (CT, MRI) | Borderline cognitive functioning (ST, WCST, RCF) | Psychosis NOS (CE, PANSS, SOFAS) | Outpatient | Amisulpride (1200 mg/day, oral) | Amisulpride (400 mg/day, oral) Galantamine (8 mg/day, oral) | Complete remission |
| Gama Marques, 2019 [33] | PT | 54, F | DWV (CT) | Moderate intellectual disability | Delusional disorder (CE) | Outpatient | Haloperidol (150 mg/monthly, depot injection) Biperiden (4 mg/day, oral) Venlafaxine (150 mg/day, oral) | Haloperidol (100 mg/monthly, depot injection) Biperiden (4 mg/day, oral) Venlafaxine (150 mg/day, oral) | Complete remission |
| Gan et al., 2012 [34] | CN | Patient 1: 45, M Patient 2: 20, M | Patient 1: MCM (MRI) Patient 2: PFAC (MRI) | Patient 1: Mild intellectual disability (CE) Patient 2: Mild intellectual disability (CE, WAIS-Revised, WMS) | Patient 1: Schizophrenia (CE, BPRS, CGI) Patient 2: Bipolar II disorder (CE, HRSD, BRMRS) | Patient 1: Inpatient Compulsory Patient 2: Inpatient Compulsory | Patient 1: Clozapine (200 mg/day, oral) Patient 2: Duloxetine (90 mg/day, oral) Olanzapine (15 mg/die, oral); Clonazepam (2 mg/day, oral) | Patient 1: (a) First discharge: Clozapine (200 mg/day, oral); (b) Second discharge: Risperidone (7 mg/day, oral) Patient 2: (a) First discharge: Duloxetine (90 mg/day, oral) Olanzapine (15 mg/day, oral) Clonazepam (2 mg/day, oral); (b) Second discharge: Olanzapine (20 mg/day, oral) Sodium valproate (1.2 g/day, oral) Clonazepam (2 mg/day, oral) | Patient 1: Complete remission Patient 2: Complete remission |
| Graf et al., 2013 [35] | DE | 26, M | DWV (MRI) | Psychomotor delay, Language development delay, Learning disorder, Attention-deficit disorder | Intermittent explosive disorder (CE) | Outpatient | - | Quetiapine (dose not given, oral) | - |
| Iancu et al., 1996 [36] | IL | 19, F | DWM (CT, MRI) | - | Psychogenic nonepileptic seizures (CE, EEG) | Inpatient | - | - | Complete remission |
| Isidro-Garcia et al., 2017 [37] | ES | 34, F | DWV (CT, MRI) | - | Schizophrenia (CE, PANSS) | Outpatient | Olanzapine (up to 20 mg/day, oral) Haloperidol (up to 10 mg/day, oral) Paliperidone (up to 12 mg/day, oral) | Clozapine (up to 600 mg/day, oral) Haloperidol (5 mg/day, oral) | Partial remission |
| Kani et al., 2015 [38] | TR | 57, F | MCM (MRI) | Borderline cognitive functioning | Schizophrenia (CE, PANSS) Obsessive–compulsive disorder (CE, Y–BOCS) | Outpatient | Risperidone (4 mg/day, oral) Quetiapine (300 mg/day, oral) Clomipramine (225 mg/day, oral) | Risperidone (4 mg/day, oral) Quetiapine (300 mg/day, oral) Fluvoxamine (300 mg/day, oral) Clonazepam (1 mg/day, oral) | Complete remission |
| Kim et al., 2013 [39] | KR | 33, M | DWV (MRI) | - | Depression (CE, HRSD, BDI) Impulsive behavior (CE) | Inpatient Compulsory | - | Mirtazapine (45 mg/day, oral) Sodium valproate (1500 mg/day, oral) Quetiapine (800 mg/day, oral) | Partial remission |
| Kumar et al., 2011 [40] | IN | 37, F | MCM (MRI) | - | Schizophrenia (CE) | Inpatient | Lorazepam (2 mg three times/day, intramuscular) | - | Relapsing symptoms after discharge |
| Li et al., 2008 [20] | CN | 40, M | DWM (MRI) | - | Bipolar II disorder (CE) | Inpatient | Venlafaxine (dose not given, oral) | Lithium (dose not given, oral) Quetiapine (dose not given, oral) Sertraline (dose not given, oral) | - |
| Mauritz et al., 2014 [41] | NL | 47, F | DWM (-) | - | Posttraumatic Stress Disorder (CE, GAF, DTS, SIDES, DES, PANSS) | Inpatient Outpatient | Quetiapine (600 mg/day, oral) | Quetiapine (600 mg/day, oral) Citalopram (40 mg/day, oral) | Partial remission |
| Ozcan and Ulkevan, 2015 [42] | TR | 34, M | DWV (CT) | - | Bipolar I disorder (CE) | Inpatient | Olanzapine (10 mg/day, oral) | Olanzapine (15 mg/day, oral) Lithium (900 mg/day, oral) Lorazepam (2.5 mg day, oral) | Complete remission |
| Pandurangi et al., 2014 [43] | IN | Patient1: 26, M Patient 2: 20, M | Patient 1: MCM (CT) Patient 2: MCM (MRI) | Patient 1: - Patient 2: - | Patient 1: Bipolar I disorder (CE, YMRS) Patient 2: Schizophrenia (CE, BFCRS) | Patient 1: Outpatient Patient 2: Inpatient | Patient 1: - Patient 2: - | Patient 1: Lithium (800 mg/day) Risperidone (4 mg/day) Patient 2: Risperidone (3 mg/day) | Patient 1: Complete remission; Patient 2: - |
| Papazisis et al., 2007 [44] | GR | 20, M | DWV (CT, MRI) | Mild intellectual disability (WISC-Revised) | Schizophrenia (CE), Obsessive–compulsive disorder (CE, Y–BOCS) | Inpatient | - | Antipsychotic (dose not given, route not given) Antidepressant (dose not given, route not given) | Relapsing symptoms after discharge |
| Porras Segovia et al., 2021 [45] | ES | 32, M | DWV (MRI) | Mild intellectual disability (WAIS-III) | Schizophrenia (CE, PANSS) | Inpatient | - | Olanzapine (10 mg/day, oral) | Partial remission |
| Pradhan et al., 1998 [46] | IN | 33, M | DWM (CT) | Borderline cognitive functioning (LNNB) | Psychosis NOS (CE) | Inpatient | Diphenylhydantoin (300 mg/day, oral) Phenobarbiton (120 mg/day, oral) | Carbamazepine (800 mg/day, oral) | Complete remission |
| Sidana et al., 2013 [47] | IN | 20, M | DWV (CT) | - | Schizophrenia (CE) | - | Olanzapine (10 mg/day, oral) | Aripiprazole (2.5 mg/day, oral) | - |
| Sinha et al., 2017 [48] | IN | 25, M | DWV (MRI) | Motor development delay Borderline cognitive functioning (WAPIS) | Schizophrenia (CE) | Inpatient | Olanzapine (15 mg/day, oral) | Olanzapine (15 mg/day, oral) | Partial remission |
| Trehout et al., 2018 [49] | FR | 24, M | DWM (MRI) | - | Schizophrenia (CE, CAARMS, MINI, PANSS, BPRS) | Inpatient | Olanzapine (5 mg/day, oral) | Clozapine (600 mg/day, oral) Loxapine (dose not given, oral) | Partial remission |
| Turan et al., 2010 [50] | TR | 23, M | MCM (MRI) | - | Bipolar I disorder (CE, YMRS) | Inpatient | Olanzapine (20 mg/day, oral) | Quetiapine (1000 mg/day, oral) Sodium valproate (1500 mg/day, oral) | Complete remission |
| Turner et al., 2001 [51] | UK | 18, F | DWV (CT, MRI) | - | Schizophrenia (CE, WAIS) | Inpatient Compulsory | Fluoxetine (dose not given, oral) | - | Complete remission |
| Williams et al., 2016 [52] | USA | 20, F | DWV (CT, MRI) | Autism spectrum disorder | Schizoaffective disorder (CE) | Inpatient | Haloperidol (7 mg/day, oral) | Olanzapine (20 mg/day, oral) | Relapsing symptoms after discharge |
| Yazici et al., 2022 [53] | TR | 28, F | MCM (MRI) | - | Bipolar I disorder (RCF, MMPI) | Inpatient | Quetiapine (100 mg/day, oral) Haloperidol (10 mg/day, oral) Biperiden (2.5 mg/day, injection) | Quetiapine (100 mg/day, oral) Olanzapine (20 mg/day, oral) Lithium (900 mg/day, oral) | Complete remission |
3.2.2. Characteristics of Studies Included
3.2.3. Neurodevelopmental/Neuropsychological Comorbidities and Psychiatric/Behavioral Phenotypes
3.2.4. Use of Psychopharmacological Medications and Clinical Course
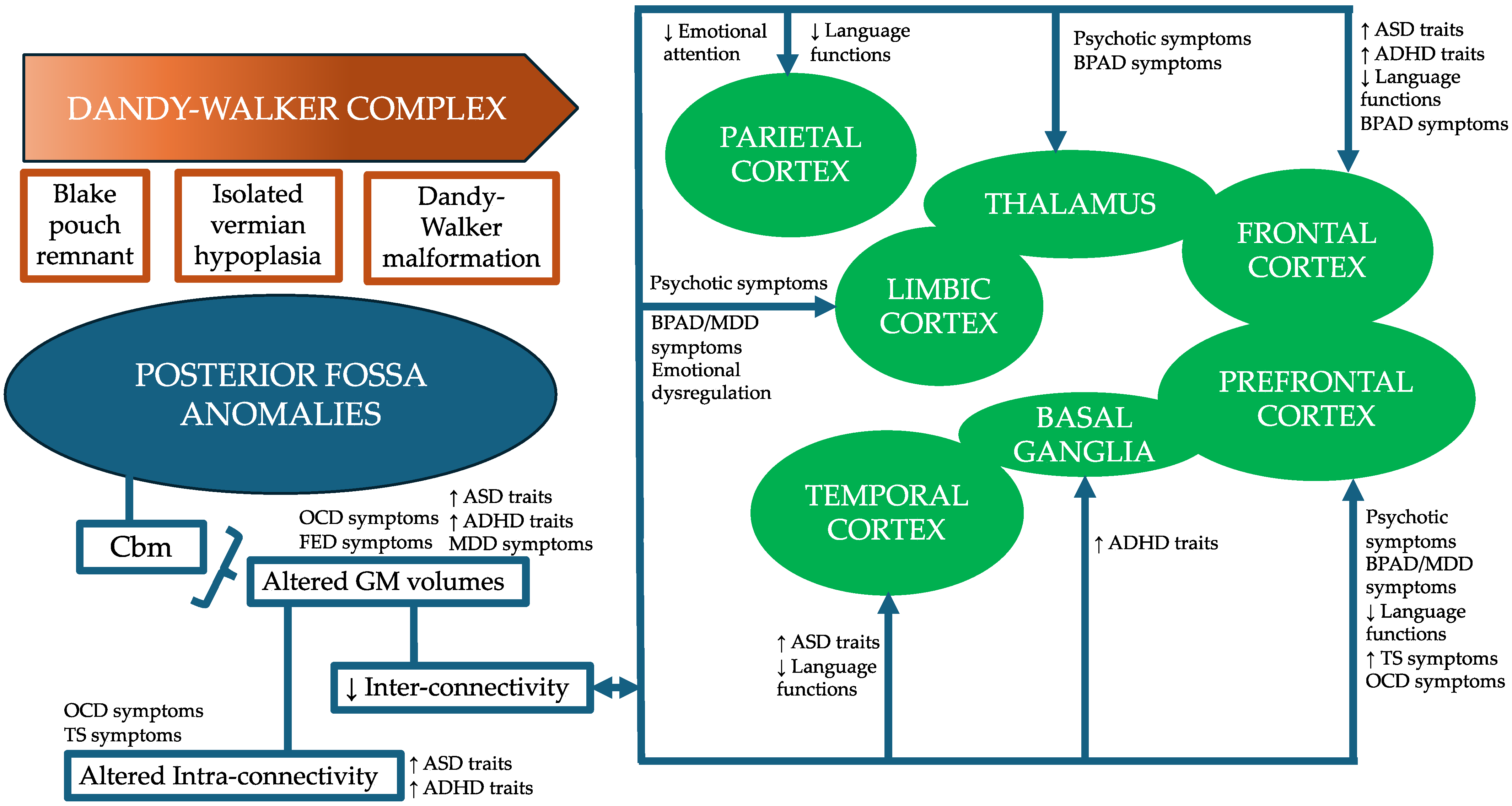
4. Discussion
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barkovich, A.J.; Kjos, B.O.; Norman, D.; Edwards, M.S. Revised classification of posterior fossa cysts and cystlike malformations based on the results of multiplanar MR imaging. Am. J. Neuroradiol. 1989, 10, 977–988. [Google Scholar] [CrossRef]
- Venkatesan, C.; Kline-Fath, B.; Horn, P.S.; Poisson, K.E.; Hopkin, R.; Nagaraj, U.D. Short- and Long-Term Outcomes of Prenatally Diagnosed Dandy-Walker Malformation, Vermian Hypoplasia, and Blake Pouch Cyst. J. Child Neurol. 2021, 36, 1111–1119. [Google Scholar] [CrossRef] [PubMed]
- Nagaraj, U.D.; Kline-Fath, B.M.; Horn, P.S.; Venkatesan, C. Evaluation of Posterior Fossa Biometric Measurements on Fetal MRI in the Evaluation of Dandy-Walker Continuum. AJNR Am. J. Neuroradiol. 2021, 42, 1716–1721. [Google Scholar] [CrossRef]
- Klein, J.L.; Lemmon, M.E.; Northington, F.J.; Boltshauser, E.; Huisman, T.A.; Poretti, A. Clinical and neuroimaging features as diagnostic guides in neonatal neurology diseases with cerebellar involvement. Cerebellum Ataxias 2016, 3, 1. [Google Scholar] [CrossRef] [PubMed]
- Bosemani, T.; Orman, G.; Boltshauser, E.; Tekes, A.; Huisman, T.A.; Poretti, A. Congenital abnormalities of the posterior fossa. Radiographics 2015, 35, 200–220. [Google Scholar] [CrossRef]
- Bokhari, I.; Rehman, L.; Hassan, S.; Hashim, M.S. Dandy-Walker Malformation: A Clinical and Surgical Outcome Analysis. J. Coll. Physicians Surg. Pak. 2015, 25, 431–433. [Google Scholar] [PubMed]
- Olivito, G.; Lupo, M.; Laghi, F.; Clausi, S.; Baiocco, R.; Cercignani, M.; Bozzali, M.; Leggio, M. Lobular patterns of cerebellar resting-state connectivity in adults with Autism Spectrum Disorder. Eur. J. Neurosci. 2018, 47, 729–735. [Google Scholar] [CrossRef] [PubMed]
- D’Mello, A.M.; Crocetti, D.; Mostofsky, S.H.; Stoodley, C.J. Cerebellar gray matter and lobular volumes correlate with core autism symptoms. Neuroimage Clin. 2015, 7, 631–639. [Google Scholar] [CrossRef] [PubMed]
- Ivanov, I.; Murrough, J.W.; Bansal, R.; Hao, X.; Peterson, B.S. Cerebellar morphology and the effects of stimulant medications in youths with attention deficit-hyperactivity disorder. Neuropsychopharmacology 2014, 39, 718–726. [Google Scholar] [CrossRef] [PubMed]
- Verly, M.; Verhoeven, J.; Zink, I.; Mantini, D.; Peeters, R.; Deprez, S.; Emsell, L.; Boets, B.; Noens, I.; Steyaert, J.; et al. Altered functional connectivity of the language network in ASD: Role of classical language areas and cerebellum. Neuroimage Clin. 2014, 4, 374–382. [Google Scholar] [CrossRef]
- Brady, R.O., Jr.; Gonsalvez, I.; Lee, I.; Ongur, D.; Seidman, L.J.; Schmahmann, J.D.; Eack, S.M.; Keshavan, M.S.; Pascual-Leone, A.; Halko, M.A. Cerebellar-Prefrontal Network Connectivity and Negative Symptoms in Schizophrenia. Am. J. Psychiatry 2019, 176, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Stanca, S.; Rossetti, M.; Bongioanni, P. The Cerebellum’s Role in Affective Disorders: The Onset of Its Social Dimension. Metabolites 2023, 13, 1113. [Google Scholar] [CrossRef] [PubMed]
- Ahmadian, N.; van Baarsen, K.; van Zandvoort, M.; Robe, P.A. The Cerebellar Cognitive Affective Syndrome—A Meta-analysis. Cerebellum 2019, 18, 941–950. [Google Scholar] [CrossRef] [PubMed]
- Parums, D.V. Editorial: Review Articles, Systematic Reviews, Meta-Analysis, and the Updated Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 Guidelines. Med. Sci. Monit. 2021, 27, e934475. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.L.; Wang, Y.Y.; Yang, Z.H.; Huang, D.; Weng, H.; Zeng, X.T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 7. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Stone, J.C.; Aromataris, E.; Klugar, M.; Sears, K.; Leonardi-Bee, J.; Barker, T.H. Assessing the risk of bias of quantitative analytical studies: Introducing the vision for critical appraisal within JBI systematic reviews. JBI Evid. Synth. 2023, 21, 467–471. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Barker, T.H.; Moola, S.; Tufanaru, C.; Stern, C.; McArthur, A.; Stephenson, M.; Aromataris, E. Methodological quality of case series studies: An introduction to the JBI critical appraisal tool. JBI Evid. Synth. 2020, 18, 2127–2133. [Google Scholar] [CrossRef] [PubMed]
- Shahsavarinia, K.; Mahmoodpoor, A.; Sadeghi-Ghyassi, F.; Nedayi, A.; Razzaghi, A.; Zehi Saadat, M.; Salehi-Pourmehr, H. Bell’s Palsy and COVID-19 Vaccination: A Systematic Review. Med. J. Islam. Repub. Iran 2022, 36, 85. [Google Scholar] [CrossRef]
- Hashemi, A.; Oroojan, A.A.; Rassouli, M.; Ashrafizadeh, H. Explanation of near-death experiences: A systematic analysis of case reports and qualitative research. Front. Psychol. 2023, 14, 1048929. [Google Scholar] [CrossRef]
- Li, H.; Chen, Q.; Liu, W. Adult asymptomatic case of Dandy-Walker syndrome associated with bipolar disorder. Acta Neuropsychiatr. 2008, 20, 170–171. [Google Scholar] [CrossRef]
- Kvitvik Aune, I.; Bugge, E. Schizophrenia in a young man with dandy-walker variant. Biol. Psychiatry 2014, 75, e9–e10. [Google Scholar] [CrossRef]
- Bakhla, A.K.; Sarkhel, S.; Kumar, R. Bipolar I disorder in a patient with Dandy-Walker malformation. Psychiatry Clin. Neurosci. 2010, 64, 212–213. [Google Scholar] [CrossRef]
- Balcioğlu, Y.H.; Kirlioğlu, S.S.; Berkol, T.D.; Özgen, G. Coincidental mega cisterna magna with psychotic disorder: A possible neuroanatomical liability for a shared psychotic disorder. Anadolu Psikiyatr. Derg. 2018, 19, 106–109. [Google Scholar] [CrossRef]
- Batmaz, M.; Balçik, Z.E.; Özer, Ü.; Hamurişçi Yalçin, B.; Özen, Ş. Dandy-walker malformation presenting with affective symptoms. Noropsikiyatri Ars. 2017, 54, 277–281. [Google Scholar] [CrossRef][Green Version]
- Blaettner, C.; Pfaffenberger, N.M.; Cartes-Zumelzu, F.; Hofer, A. Psychiatric misdiagnoses in Dandy-Walker variant. Neurocase 2015, 21, 499–500. [Google Scholar] [CrossRef] [PubMed]
- Bout, A.; Aarab, C.; Boujraf, S.; Aalouane, R. From cerebellar malformation to suicidal idea: Case report. Clin. Schizophr. Relat. Psychoses 2021, 15. [Google Scholar] [CrossRef]
- Zincir, S.B.; Kivilcim, Y.; Izci, F.; Semiz, U.B. Schizophrenia-Like Psychosis and Dandy-Walker Variant Comorbidity: Case Report. Psychiatry Investig. 2014, 11, 102–104. [Google Scholar] [CrossRef]
- Buonaguro, E.F.; Cimmarosa, S.; De Bartolomeis, A. Dandy-Walker Syndrome with psychotic symptoms: A case report. Riv. Di Psichiatr. 2014, 49, 100–102. [Google Scholar] [CrossRef]
- Can, S.S.; Uǧurlu, G.K.; Çakmak, S. Dandy walker variant and bipolar i disorder with graphomania. Psychiatry Investig. 2014, 11, 336–339. [Google Scholar] [CrossRef][Green Version]
- Dawra, R.D.; Karia, S.; Shah, N.; Desousa, A. Psychosis in a case of Dandy-Walker Syndrome: A case report. J. Clin. Diagn. Res. 2017, 11, VD03–VD04. [Google Scholar] [CrossRef]
- El Tahir, M.; Ahmed, M.; Salman, S.; Elhusein, B. Dandy-Walker malformation and intermittent explosive disorder: A case report. SAGE Open Med. Case Rep. 2022, 10, 5. [Google Scholar] [CrossRef]
- Ferentinos, P.P.; Kontaxakis, V.P.; Havaki-Kontaxaki, B.J.; Paplos, K.G.; Pappa, D.A.; Soldatos, C.R. Refractory psychosis and prominent cognitive deficits in a patient with mega-cisterna magna. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2007, 31, 561–563. [Google Scholar] [CrossRef]
- Gama Marques, J. Twenty years of misdiagnosis of schizophrenia in a patient with Dandy-Walker variant syndrome. Gen. Psychiatry 2019, 32, e100031. [Google Scholar] [CrossRef]
- Gan, Z.; Diao, F.; Han, Z.; Li, K.; Zheng, L.; Guan, N.; Kang, Z.; Wu, X.; Wei, Q.; Cheng, M.; et al. Psychosis and Dandy-Walker complex: Report of four cases. Gen. Hosp. Psychiatry 2012, 34, 102.e7–102.e11. [Google Scholar] [CrossRef]
- Graf, H.; Franke, B.; Abler, B. Cerebellar cognitive affective syndrome in Dandy-Walker variant disorder. J. Neuropsychiatry Clin. Neurosci. 2013, 25, E45–E46. [Google Scholar] [CrossRef]
- Iancu, I.; Kotler, M.; Lauffer, N.; Dannon, P.; Lepkifker, E. Seizures and the Dandy-Walker syndrome: A case of suspected pseudoseizures. Psychother. Psychosom. 1996, 65, 109–111. [Google Scholar] [CrossRef]
- Isidro-García, G.J.; Espina-Barrio, J.A.; Guitián-Domínguez, M. Dandy-Walker variant and refractory psychosis. Actas Esp. De Psiquiatr. 2017, 45, 179–181. [Google Scholar]
- Kani, A.S.; Poyraz, C.A.; İnce, E.; Duran, A. Comorbid schizophrenia and obsessive compulsive disorder associated with mega cisterna magna: A case report. Yeni Symp. 2015, 53, 45–46. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, T.H.; Choi, Y.C.; Chung, S.C.; Moon, S.W. Impulsive behavior and recurrent major depression associated with dandy-walker variant. Psychiatry Investig. 2013, 10, 303–305. [Google Scholar] [CrossRef]
- Kumar, S.; Sur, S.; Singh, A. Mega Cisterna Magna Associated with Recurrent Catatonia: A Case Report. Biol. Psychiatry 2011, 70, E19. [Google Scholar] [CrossRef] [PubMed]
- Mauritz, M.W.; van de Sande, R.; Goossens, P.J.J.; van Achterberg, T.; Draijer, N. Phase-Based Treatment of a Complex Severely Mentally Ill Case Involving Complex Posttraumatic Stress Disorder and Psychosis Related to Dandy Walker Syndrome. J. Trauma Dissociation 2014, 15, 588–606. [Google Scholar] [CrossRef]
- Ulkevan, T. Propolis induced mania with psychotic features: A case report. Klin. Psikofarmakol. Bul. 2015, 25, 207–208. [Google Scholar] [CrossRef]
- Pandurangi, S.; Pandurangi, A.; Matkar, A.; Shetty, N.; Patil, P. Psychiatric manifestations associated with mega cisterna magna. J. Neuropsychiatry Clin. Neurosci. 2014, 26, 169–171. [Google Scholar] [CrossRef]
- Papazisis, G.; Mastrogianni, A.; Karastergiou, A. Early-onset schizophrenia and obsessive-compulsive disorder in a young man with Dandy-Walker variant. Schizophr. Res. 2007, 93, 403–405. [Google Scholar] [CrossRef]
- Porras Segovia, A.; Guerrero-Jiménez, M.; Carrillo de Albornoz Calahorro, C.M.; Gutierrez-Rojas, L. Psychosis and Dandy-Walker syndrome: A case report and review of the literature. Gen. Psychiatry 2021, 34, e100254. [Google Scholar] [CrossRef]
- Pradhan, S.C.; Das, J.; Sinha, V.K. Dandy-walker syndrome with epilepsy and psychosis: An atypical presentation. Indian J. Psychiatry 1998, 40, 189–191. [Google Scholar]
- Sidana, A.; Sarkar, S.; Balasundaram, S.; Praharaj, S.K. Increased sensitivity to atypical antipsychotics in a patient with Dandy-Walker variant with schizophrenia. J. Neuropsychiatry Clin. Neurosci. 2013, 25, E31–E32. [Google Scholar] [CrossRef] [PubMed]
- Sinha, P.; Tarwani, J.; Kumar, P.; Garg, A. Dandy-Walker variant with schizophrenia: Comorbidity or cerebellar cognitive affective syndrome? Indian J. Psychol. Med. 2017, 39, 188–190. [Google Scholar] [CrossRef]
- Trehout, M.; Zhang, N.; Blouet, M.; Borha, A.; Dollfus, S. Dandy-walker malformation-like condition revealed by a refractory schizophrenia: A case report and literature review. Eur. Psychiatry 2018, 48, S397–S398. [Google Scholar]
- Turan, T.; Beşirli, A.; Asdemir, A.; Özsoy, S.; Eşel, E. Manic episode associated with mega cisterna magna. Psychiatry Investig. 2010, 7, 305–307. [Google Scholar] [CrossRef] [PubMed]
- Turner, S.J.; Poole, R.; Nicholson, M.R.; Ghadiali, E.J. Schizophrenia-like psychosis and Dandy–Walker variant. Schizophr. Res. 2001, 48, 365–367. [Google Scholar] [CrossRef]
- Williams, A.J.; Wang, Z.N.; Taylor, S.F. Atypical psychotic symptoms and Dandy-Walker variant. Neurocase 2016, 22, 472–475. [Google Scholar] [CrossRef]
- Yazici, E.; Kose, S.; Gunduz, Y.; Kurt, E.M.; Yazici, A.B. Mega cisterna magna in bipolar mood disorder: A case report. J. Yeungnam Med. Sci. 2022, 39, 58–61. [Google Scholar] [CrossRef]
- Antolini, G.; Colizzi, M. Where Do Neurodevelopmental Disorders Go? Casting the Eye Away from Childhood towards Adulthood. Healthcare 2023, 11, 1015. [Google Scholar] [CrossRef]
- Marquis, S.M.; McGrail, K.; Hayes, M.V. A population-level study of the mental health of siblings of children who have a developmental disability. SSM Popul. Health 2019, 8, 100441. [Google Scholar] [CrossRef]
- Quatrosi, G.; Genovese, D.; Amodio, E.; Tripi, G. The Quality of Life among Siblings of Autistic Individuals: A Scoping Review. J. Clin. Med. 2023, 12, 735. [Google Scholar] [CrossRef]
- Bortoletto, R.; Bassani, L.; Garzitto, M.; Lamberti, M.; Simonati, A.; Darra, F.; Bhattacharyya, S.; Comacchio, C.; Balestrieri, M.; Arcangeli, D.; et al. Risk of psychosis in autism spectrum disorder individuals exposed to psychosocial stressors: A 9-year chart review study. Autism Res. 2023, 16, 2139–2149. [Google Scholar] [CrossRef]
- Rohanachandra, Y.M.; Dahanayake, D.M.; Wijetunge, S. Dandy-Walker Malformation Presenting with Psychological Manifestations. Case Rep. Psychiatry 2016, 2016, 9104306. [Google Scholar] [CrossRef]
- Tang, W.; Shen, T.; Huang, Y.; Zhu, W.; You, S.; Zhu, C.; Zhang, L.; Ma, J.; Wang, Y.; Zhao, J.; et al. Exploring structural and functional alterations in drug-naive obsessive-compulsive disorder patients: An ultrahigh field multimodal MRI study. Asian J. Psychiatry 2023, 81, 103431. [Google Scholar] [CrossRef] [PubMed]
- Tikoo, S.; Suppa, A.; Tommasin, S.; Gianni, C.; Conte, G.; Mirabella, G.; Cardona, F.; Pantano, P. The Cerebellum in Drug-naive Children with Tourette Syndrome and Obsessive-Compulsive Disorder. Cerebellum 2022, 21, 867–878. [Google Scholar] [CrossRef] [PubMed]
- Iyer, P.; Smith, R. Severe feeding difficulties in 3C syndrome. Clin. Dysmorphol. 2005, 14, 101–103. [Google Scholar] [CrossRef]
- Siciliano, L.; Olivito, G.; Leggio, M. The cerebellum gains weight: A systematic review of alterations in cerebellar volume and cerebro-cerebellar functional alterations in individuals with eating disorders. Neurosci. Biobehav. Rev. 2022, 141, 104863. [Google Scholar] [CrossRef]
- Cheng, C.S.; Lin, S.K.; Kuo, C.J. Brexpiprazole for the Treatment of Tics in a Patient with Schizophrenia. Prim. Care Companion CNS Disord. 2023, 25, 48093. [Google Scholar] [CrossRef]
- Albert, U.; Marazziti, D.; Di Salvo, G.; Solia, F.; Rosso, G.; Maina, G. A Systematic Review of Evidence-based Treatment Strategies for Obsessive- compulsive Disorder Resistant to first-line Pharmacotherapy. Curr. Med. Chem. 2018, 25, 5647–5661. [Google Scholar] [CrossRef]
- Conti, D.; Girone, N.; Boscacci, M.; Casati, L.; Cassina, N.; Cerolini, L.; Giacovelli, L.; Vigano, C.; Conde, M.M.; Cremaschi, L.; et al. The use of antipsychotics in obsessive compulsive disorder. Hum. Psychopharmacol. 2024, e2893. [Google Scholar] [CrossRef]
- Sohanpal, S.K.; Deb, S.; Thomas, C.; Soni, R.; Lenotre, L.; Unwin, G. The effectiveness of antidepressant medication in the management of behaviour problems in adults with intellectual disabilities: A systematic review. J. Intellect. Disabil. Res. 2007, 51, 750–765. [Google Scholar] [CrossRef]
- Williams, K.; Brignell, A.; Randall, M.; Silove, N.; Hazell, P. Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorders (ASD). Cochrane Database Syst. Rev. 2013, 8, CD004677. [Google Scholar] [CrossRef]
- Hurwitz, R.; Blackmore, R.; Hazell, P.; Williams, K.; Woolfenden, S. Tricyclic antidepressants for autism spectrum disorders (ASD) in children and adolescents. Cochrane Database Syst. Rev. 2012, 3, CD008372. [Google Scholar] [CrossRef]
- Comacchio, C.; Howard, L.M.; Bonetto, C.; Lo Parrino, R.; Furlato, K.; Semrov, E.; Preti, A.; Mesiano, L.; Neri, G.; De Girolamo, G.; et al. The impact of gender and childhood abuse on age of psychosis onset, psychopathology and needs for care in psychosis patients. Schizophr. Res. 2019, 210, 164–171. [Google Scholar] [CrossRef]
- Comacchio, C.; Antolini, G.; Ruggeri, M.; Colizzi, M. Gender-Oriented Mental Health Prevention: A Reappraisal. Int. J. Environ. Res. Public Health 2022, 19, 1493. [Google Scholar] [CrossRef]
- Zhang, X.; Liang, M.; Qin, W.; Wan, B.; Yu, C.; Ming, D. Gender Differences Are Encoded Differently in the Structure and Function of the Human Brain Revealed by Multimodal MRI. Front. Hum. Neurosci. 2020, 14, 244. [Google Scholar] [CrossRef] [PubMed]
- Odalovic, M.; Gorman, A.; Paul, A.; McCallion, P.; Burke, E.; MacLachlan, M.; McCarron, M.; Henman, M.C.; Moran, M.; O’Connell, J.; et al. Psychotropic medicines’ prevalence, patterns and effects on cognitive and physical function in older adults with intellectual disability in Ireland: Longitudinal cohort study, 2009–2020. BJPsych Open 2024, 10, e39. [Google Scholar] [CrossRef]


| Author/Question | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Quality Appraisal |
|---|---|---|---|---|---|---|---|---|---|
| Aune and Bugge [21] | Y | N | Y | Y | Y | Y | U | Y | Medium |
| Bakhla et al. [22] | Y | N | Y | N | Y | Y | Y | Y | Medium |
| Balcioglu et al. [23] | Y | N | Y | Y | Y | N | N | Y | Medium |
| Batmaz et al. [24] | Y | Y | Y | Y | Y | N | Y | Y | High |
| Blaettner et al. [25] | Y | Y | Y | Y | Y | U | N | Y | Medium |
| Bout et al. [26] | Y | N | Y | Y | Y | Y | N | Y | Medium |
| Bozkurt Zincir et al. [27] | N | N | Y | Y | Y | Y | N | Y | Medium |
| Buonaguro et al. [28] | Y | Y | Y | Y | N | N | N | Y | Medium |
| Can et al. [29] | Y | N | Y | Y | Y | N | Y | Y | Medium |
| Dawra et al. [30] | Y | Y | Y | U | Y | Y | N | Y | Medium |
| El Tahir et al. [31] | Y | Y | Y | Y | N | Y | N | Y | Medium |
| Ferentinos et al. [32] | Y | N | Y | Y | Y | Y | Y | Y | High |
| Gama Marques [33] | Y | Y | Y | Y | Y | Y | N | Y | High |
| Gan et al. [34] | N | Y | Y | Y | Y | Y | N | Y | Medium |
| Graf et al. [35] | N | U | Y | Y | N | Y | N | Y | Medium |
| Iancu et al. [36] | Y | Y | Y | Y | N | Y | NA | Y | Medium |
| Isidro-Garcia et al. [37] | Y | Y | Y | Y | Y | U | N | Y | Medium |
| Kani et al. [38] | Y | Y | Y | Y | Y | Y | N | Y | High |
| Kim et al. [39] | Y | Y | Y | Y | Y | Y | N | Y | High |
| Kumar et al. [40] | Y | Y | Y | Y | Y | Y | N | Y | High |
| Li et al. [20] | N | N | Y | Y | N | N | N | Y | Low |
| Mauritz et al. [41] | Y | Y | Y | Y | Y | N | N | Y | Medium |
| Ozcan and Ulkevan [42] | Y | N | Y | N | Y | Y | N | Y | Medium |
| Pandurangi et al. [43] | Y | Y | Y | Y | Y | N | Y | Y | High |
| Papazisis et al. [44] | N | N | Y | Y | N | Y | N | Y | Medium |
| Porras Segovia et al. [45] | Y | Y | Y | Y | Y | Y | Y | Y | High |
| Pradhan et al. [46] | Y | Y | Y | Y | Y | Y | N | Y | High |
| Sidana et al. [47] | Y | N | Y | N | Y | N | Y | Y | Medium |
| Sinha et al. [48] | Y | Y | Y | Y | Y | Y | N | Y | High |
| Trehout et al. [49] | Y | Y | Y | Y | Y | Y | Y | Y | High |
| Turan et al. [50] | Y | N | Y | Y | Y | Y | Y | Y | High |
| Turner et al. [51] | Y | Y | Y | Y | N | Y | Y | Y | High |
| Williams et al. [52] | Y | Y | Y | U | Y | Y | Y | Y | High |
| Yazici et al. [53] | Y | Y | Y | Y | Y | N | N | Y | Medium |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bortoletto, R.; Candolo, A.; Nicotra, A.; Saetti, L.; Perini, L.; Balestrieri, M.; Colizzi, M.; Comacchio, C. Tic-Related Obsessive–Compulsive and Eating Disorders in Dandy–Walker Variant: A Case Report and Systematic Reappraisal of Psychiatric Profiles. Brain Sci. 2024, 14, 362. https://doi.org/10.3390/brainsci14040362
Bortoletto R, Candolo A, Nicotra A, Saetti L, Perini L, Balestrieri M, Colizzi M, Comacchio C. Tic-Related Obsessive–Compulsive and Eating Disorders in Dandy–Walker Variant: A Case Report and Systematic Reappraisal of Psychiatric Profiles. Brain Sciences. 2024; 14(4):362. https://doi.org/10.3390/brainsci14040362
Chicago/Turabian StyleBortoletto, Riccardo, Anna Candolo, Alessandra Nicotra, Luana Saetti, Laura Perini, Matteo Balestrieri, Marco Colizzi, and Carla Comacchio. 2024. "Tic-Related Obsessive–Compulsive and Eating Disorders in Dandy–Walker Variant: A Case Report and Systematic Reappraisal of Psychiatric Profiles" Brain Sciences 14, no. 4: 362. https://doi.org/10.3390/brainsci14040362
APA StyleBortoletto, R., Candolo, A., Nicotra, A., Saetti, L., Perini, L., Balestrieri, M., Colizzi, M., & Comacchio, C. (2024). Tic-Related Obsessive–Compulsive and Eating Disorders in Dandy–Walker Variant: A Case Report and Systematic Reappraisal of Psychiatric Profiles. Brain Sciences, 14(4), 362. https://doi.org/10.3390/brainsci14040362