
Prevalence and Correlates of the Concurrence of Autism Spectrum Disorder and Obsessive Compulsive Disorder in Children and Adolescents: A Systematic Review and Meta-Analysis

 , , , ,
, , , ,
Abstract
1. Introduction
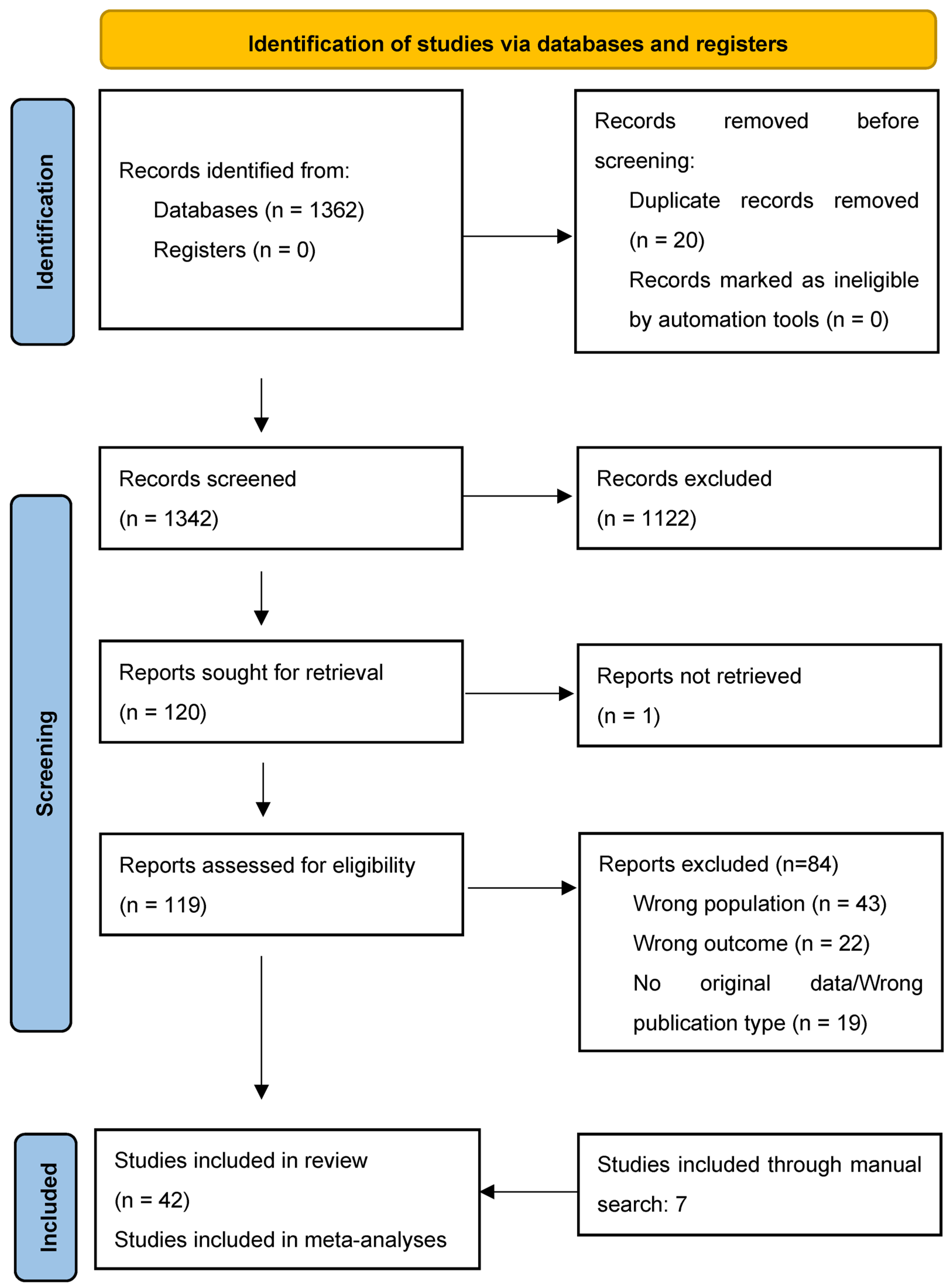
2. Methods
2.1. Search Strategy and Selection Criteria
2.2. Data Extraction
2.3. Risk of Bias (Quality) Assessment
2.4. Strategy for Data Synthesis and Statistics

{kind=link}
{kind=link}
{kind=link}
| Author (Year) | City (Country) | NOS Score | Sample Size | ASD Diagnostic Criteria | Setting | Sample Type | Mean IQ ± SD | Mean Age ± SD (Range) | Females (%) | Ethnicity (%) | Key Findings |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Amr (2012) * [29] | Multiple (Jordan, Egypt, and Saudi Arabia) | 6 | 60 | DSM-IV-TR | Clinical | AS, PDD-NOS | 61.3 ± 21.6 | 8.4 ± 1.8 (6–11 years) | 38.3 | N.a. | Of individuals with ASD, 55.0% met criteria for OCD (DSM-IV-TR). OCD was the most prevalent comorbid disorder among the ASD sample. |
| Gurkan (2009) * [30] | Ankara (Turkey) | 5 | 40 | DSM-IV-TR | Clinical | ASD (N = 18), AS (N = 11), PDD-NOS (N = 11) | 88.5 ± 18.9 | 10.8 ± 3.6 (6–18 years) | 10.0 | N.a. | Of the individuals with ASD, 15.8% met criteria for OCD (DSM-IV-TR). |
| Leyfer (2006) * [31] | Boston, Salt Lake City (USA) | 8 | 109 | DSM-IV-TR | Community | ASD with some spoken language | 81.5 ± 24.5 | 9.2 ± 2.7 (5–17 years) | 5.7 | N.a. | Of the individuals with ASD, 37.2% met criteria for OCD (DSM-IV-TR). The most common type of compulsion was a ritual involving other individuals having to perform a certain way (e.g., greeting and separation rituals, question-asking rituals). |
| Margari (2019) * [32] | Bari (Italy) | 7 | 159 | DSM-5 | Clinical | High functioning ASD | 106.5 ± 16.9 | 10.3 ± 4.3 (N.a.) | 37.1 | N.a. | Of the individuals with ASD, 5.0% of male individuals and 0.0% of female individuals met criteria for OCD (DSM-5). |
| Mazefsky (2012) * [33] | Pittsburgh (USA) | 6 | 35 | DSM-IV | Community/Clinical | High functioning ASD | 105.0 ± 17.0 | 12.1 ± 2.0 (10–17 years) | 20.0 | Caucasian (88.6) | When a structured psychiatric interview carefully took ASD-related impairment into account using the autism comorbidity interview, only 2.9% of the individuals with ASD met criteria for OCD (DSM-IV-TR) |
| Sturm (2004) * [34] | Stockholm (Sweden) | 6 | 101 | DSM-IV | Clinical | AS (N = 91), PDD-NOS (N = 9), high functioning ASD (N = 1) | N.a. | 9.8 ± N.a. (5–12 years) | 29.7 | N.a. | Of the individuals with ASD, 6.9% met criteria for OCD (DSM-IV). Also, 48.5% children had symptoms of obsessive compulsive disorder, and, in 24.8%, these symptoms were severe. |
| Fucà (2023) * [35] | Rome (Italy) | 6 | 472 | DSM-5 | Clinical | ASD with IQ > 70 | 90.6 ± 19.3 | 7.2 ± 3.4 (3–18 years) | 17.5 | N.a. | Of the individuals with ASD, 0.6% met criteria for OCD (DSM-5). Adolescents exhibited greater prevalence of OCD and anxiety disorders than preschoolers. |
| Gjevik (2011) * [36] | Oslo (Norway) | 7 | 71 | DSM-IV | Community | AS (N = 12), PDD-NOS (N = 12), ASD (N = 47) | 65.2 ± 29.6 | 11.8 ± 3.3 (6–18 years) | 18.3 | N.a. | Of the individuals with ASD, 9.9% met criteria for OCD (DSM-IV criteria). OCD was more common in older children. Children with OCD had worries about contamination, checking, and hand washing. |
| Joshi (2010) * [37] | Boston (USA) | 8 | 217 | DSM-III-R | Clinical | ASD/PDD-NOS | N.a. | 9.7 ± 3.6 (3–17.9 years) | 13.4 | N.a. | Of the individuals with ASD, 24.4% met criteria for OCD (DSM-III-R). |
| Romero (2016) * [38] | Málaga (Spain) | 6 | 123 | DSM-IV-TR/DSM-5 | Community | ASD (N = 57), PDD-NOS (N = 66) | N.a. | 10.6 ± 3.0 (5–15.9 years) | 18.0 | N.a. | Of the individuals with ASD, 40.7% met criteria for OCD (DSM-5). Patients fulfilling criteria for DSM-5 criteria for ASD had higher prevalences of OCD. |
| Van der Plas (2016) * [17] | Toronto (Canada) | 7 | 99 | DSM-IV | Community | ASD | N.a. | 11.0 ± 2.3 (6–17.9 years) | 12.1 | Caucasian (29.3) | Of the individuals with ASD, 6.2% met criteria for OCD (DSM-IV). Among those that did not meet criteria, ASD youth exhibited more OCD traits than individuals without ASD. |
| Caamaño (2013) * [39] | Madrid (Spain) | 7 | 25 | DSM-IV-TR | Clinical | ASD without intellectual disability | 97.9 ± 27.6 | 12.8 ± 2.9 (7–17.9 years) | 4.0 | Caucasian (92.0) | Of the individuals with ASD, 12.5% met criteria for OCD (DSM-IV-TR). ASD youth exhibited more OCD traits than individuals without ASD, even in the absence of a concurrent disorder. |
| Muris (1998) * [40] | South-Limburg (The Netherlands) | 7 | 44 | DSM-III-R | Clinical | ASD (N = 15), PDD-NOS (N = 29) | 79.5 ± 14.0 | 9.7 ± 4.8 (2–17.9 years) | N.a. | N.a. | Of the individuals with ASD, 11.4% met criteria for OCD (DSM-III-TR). An additional 61.3% of the sample also exhibited rituals, but most parents or guardians did not know whether these rituals caused distress. |
| Simonoff (2008) * [41] | Multiple (UK) | 8 | 112 | ICD-10 | Community | ASD (N = 62), PDD (N = 50) | 72.7 ± 21.6 | 11.5 ± N.a. (10–14.9 years) | 12.5 | White (95.0) | Of the individuals with ASD, 8.2% met criteria for OCD (DSM-IV). The authors suggested their rates were lower than other studies because they required a purposeful quality to obsessional thoughts and compulsions in order to meet criteria. |
| de Bruin (2006) * [42] | Rotterdam (The Netherlands) | 8 | 94 | DSM-IV | Clinical | PDD-NOS | 91.2 ± 17.4 | 8.5 ± 1.9 (6–12.9 years) | 11.7 | N.a. | Of the individuals with ASD, 6.4% met criteria for OCD (DSM-IV). |
| Green (2000) * [43] | Manchester (UK) | 5 | 20 | ICD-10 | Clinical | AS | 92.2 ± 17.7 | 13.8 ± N.a. (11–19 years) | 0.0 | N.a. | Of the individuals with ASD, 25.0% met criteria for OCD (ICD-10). The authors noted the difficulty in distinguishing between obsessive compulsive symptoms and the bizarre preoccupations characteristic of the core autistic disorder. |
| Mattila (2010) * [44] | Multiple (Finland) | 7 | 50 | DSM-IV | Community/Clinical | AS | >75 | 12.7 ± 1.5 (9.8–16.3 years) | 24.0 | N.a. | Of the individuals with ASD, 22.0% met criteria for OCD (DSM-IV). |
| Mukaddes (2010) * [45] | Istanbul (Turkey) | 7 | 60 | DSM-IV | Clinical | AS (N = 30), HF-ASD (N = 30) | 98.5 ± N.a. | 10.7 ± N.a. (6–15.9 years) | 0.0 | N.a. | Of the individuals with ASD, 37.2% met criteria for OCD (DSM-IV). No significant differences were found between AS and HF-ASD in the prevalence of this co-occurrence. |
| Witwer (2010) * [46] | Ohio (USA) | 6 | 61 | DSM-IV | Clinical | AS (N = 16), ASD (N = 17), PDD-NOS (N = 26) | 68.4 ± 23.3 | 11.2 ± 3.8 (6–17.9 years) | 82.0 | Caucasian (77.0) | Of the individuals with ASD, 4.9% met criteria for OCD (DSM-IV). However, an additional 42.6% reported significant OCD symptoms without meeting criteria. OCD symptom endorsement was not impacted by IQ. The authors noted the difficulty in distinguishing OCD symptoms from ASD-related repetitive behaviours. |
| Wozniak (1997) * [47] | Massachusetts (USA) | 6 | 52 | DSM-III-R | Clinical | PDD | N.a. | 9.8 ± 3.8 (Range N.a.) | 24.0 | N.a. | Of the individuals with ASD, 16.0% met criteria for OCD (DSM-III-R). |
| King (2009) [48] | Multiple (USA) | 8 | 149 | DSM-IV-TR | Clinical | ASD or AS with >8 score for compulsive behaviours on CY-BOCS | N.a. | 9.1 ± 3.2 (5–17 years) | 16.8 | Caucasian (72.5), Black (11.4), other (16.1) | Citalopram was not superior to placebo (p = 0.81) in the treatment of compulsive behaviour in children and adolescents with ASD. |
| Iniesta-Sepúlveda (2017) [49] | Multiple (USA) | 5 | 9 | DSM-IV-TR | Clinical | Primary OCD + high functioning ASD | N.a. | 14.0 ± 2.0 (11–17 years) | 11.1 | Caucasian (89.0), Hispanic (11.0) | Intensive (3–6 h/day, 24–80 sessions) CBT with ASD-specific modifications was effective for 78% of participants, and large treatment effects (d = 1.35–2.58) were obtained in OCD symptom severity. |
| Mandell (2008) [50] | Pennsylvania (USA) | 6 | 760 | DSM | Community | ASD, AS, PDD-NOS | N.a. | 9.3 ± 4.3 (5–21 years) | 16.0 | White (83.0), African American (8.9) | Concurrent OCD was a significant risk factor for psychiatric hospitalization among children with ASD (OR 2.35; p < 0.01). |
| Author (Year) | City (Country) | NOS Score | Sample Size | OCD Diagnostic Criteria | Setting | OCD Severity | Mean Age ± SD (Range) | Females (%) | Ethnicity (%) | Key Findings |
|---|---|---|---|---|---|---|---|---|---|---|
| Rintala (2017) * [51] | Multiple (Finland) | 8 | 3372 | ICD-9; ICD-10 | Clinical | N.a. | 15.2 ± 4.1 (3–25 years) | 53.2 | N.a. | Of individuals with OCD, 13.4% of male individuals and 3.4% of female individuals met criteria for an ASD disorder (ICD-9 299X; ICD-10 F84). Females were significantly less likely to present this co-occurrence (OR 0.22; p < 0.01). |
| Schachar (2022) * [52] | Ontario (Canada) | 6 | 171 | DSM-5 | Clinical/Community | TOCS 65.4 ± 9.2 | 12.7 ± 2.6 (7–17.9 years) | 40.4 | N.a. | Of individuals with OCD, 8.8% of male and 4.3% of female individuals with OCD met criteria for an ASD disorder (DSM-5, ADI-R, ADOS-2). Antipsychotic use was more common among OCD cases with ASD. |
| Griffiths (2017-A) * [53] | Southport (Australia) | 7 | 80 | DSM-IV | Community | CY-BOCS 25.7 ± 4.6 | 12.3 ± 2.7 (7–17.9 years) | 55.0 | White (90.0), Black (2.5), Native Asian (2.5) | Of the individuals with OCD, 5.0% met criteria for an ASD disorder. An additional 27.5% of the sample showed moderate ASD traits. ASD traits were associated with greater functional impairment above OCD severity. Family accommodation mediated the relationship between ASD traits and functional impairment. |
| Farrell (2012) * [54] | Southport (Australia) | 6 | 43 | DSM-IV | Clinical | CY-BOCS 21.4 ± 6.6 | 11.1 ± 2.5 (7–17.9 years) | 30.2 | N.a. | Of the individuals with OCD in the sample, 34.9% met criteria for a PDD disorder. This did not significantly influence treatment response to a group CBT intervention at post-treatment but was associated with poorer treatment response at a 6-month follow-up. |
| Arildskov (2015) * [55] | Multiple (Denmark, Norway, and Sweden) | 7 | 257 | DSM-IV-TR | Clinical | CY-BOCS 24.7 ± 5.1 | 12.8 ± 2.8 (7–17.9 years) | 51.4 | N.a. | Of the individuals with OCD, 9.7% met criteria for an ASD disorder, with a male preponderance with a sex ratio of 2.6:1. Autism-specific social and communication difficulties were not related to OCD severity, while restricted repetitive behaviour was positively related to OCD severity. |
| Ivarsson (2007) * [56] | Gothenburg (Sweden) | 8 | 109 | DSM-IV | Clinical | N.a. | N.a. | 55.0 | N.a. | While only 8.3% of the individuals with OCD met criteria for an ASD disorder, autistic traits were common among the sample. OCD symptom scores were highest in cases with concurrent ASD. |
| Martin (2020) * [57] | London (UK) | 8 | 1345 | ICD-10 | Clinical | N.a. | 14.0 ± 2.6 (4–17.9 years) | 52.2 | White (66.2), Black (6.2), Asian (4.9) | Of the individuals with OCD, 24.9% met criteria for an ASD disorder. Youth with OCD + ASD had lower psychosocial functioning compared to those with either OCD or ASD, and showed significant improvements in functioning after service utilization, but their gains were smaller than those with OCD. |
| Jaspers-Fayers (2017) * [58] | Vancouver (Canada) | 6 | 136 | DSM-IV | Clinical | CY-BOCS 21.2 ± 8.0 | 13.1 ± 2.7 (6–19 years) | 46.0 | White (71.0), Asian (18.0), other (11.0) | Of the individuals with OCD, 6.0% met criteria for a PDD. |
| Adam (2019) * [59] | Cologne (Germany) | 7 | 181 | ICD-10 | Clinical | N.a. | 13.2 ± 3.0 (6–18 years) | 49.7 | N.a. | Of the individuals with OCD, 5.0% met criteria for a PDD. |
| Sevilla-Carmeno (2019) * [60] | Stockholm (Sweden) | 7 | 193 | ICD-10/DSM-5 | Clinical | CY-BOCS 22.6 ± 4.4 | 13.6 ± 2.4 (6–17 years) | 55.4 | N.a. | Of the individuals with OCD, 19.7% met criteria for ASD. |
| Peris (2017) * [61] | Los Angeles (USA) | 6 | 322 | DSM-IV-TR | Clinical | CY-BOCS 25.2 ± 4.8 | 12.3 ± 2.8 (7–17 years) | 47.0 | White (72.0), Hispanic (10.0) | Of the individuals with OCD, 3.0% met criteria for ASD. |
| Griffiths (2017-B) [62] | Southport (Australia) | 7 | 50 | DSM-IV | Community | CY-BOCS 23.3 ± 6.6 | 12.0 ± 2.5 (7–17 years) | 12.0 | N.a. | Concurrent OCD and ASD was associated with significantly higher functional impairment (t = 2.91; p < 0.01), and more concurrent disorders overall (X2 = 2.51; p = 0.02) than OCD without concurrent ASD. Families of individuals with concurrent OCD and ASD engaged in more accommodating behaviours (t = 3.41; p < 0.01). Youth with both disorders had poorer treatment response (t = 7.67; p < 0.01) at a six month follow-up. |
| Lewin (2011) [63] | Multiple (USA) | 7 | 70 | DSM-IV | Clinical | CY-BOCS 26.2 ± 7.2 | 9.9 ± 1.8 (7–13 years) | 20.0 | Caucasian (74.0), Hispanic (4.0), other (22.0) | Individuals with OCD and concurrent ASD did not differ from patients with OCD for total severity scores, obsessions, or compulsions scores. ADHD symptoms, social phobia, and separation anxiety disorder were more common among youth with ASD + OCD. Youth with ASD + OCD were significantly less likely to endorse sexual obsessions, checking, or washing or repeating compulsions. |
| Murray (2015) [64] | London (UK) | 8 | 44 | ICD-10 | Clinical | CY-BOCS 29.4 ± 5.0 | 15.0 ± 3.8 (7–13 years) | 40.9 | N.a. | Individuals with OCD and concurrent ASD (N = 22), compared to age-matched OCD youth without ASD (N = 22) showed lower rates of response (38.3% vs. 48.2%) and remission (9.0% vs. 46.0%) to CBT. |
| Wickberg (2022) [65] | Stockholm (Sweden) | 6 | 22 | DSM-5 | Clinical | CY-BOCS 21.7 ± 3.7 | 13.9 ± 1.6 (7–17 years) | 33.3 | N.a. | Internet-delivered CBT was deemed acceptable and was associated with clinically significant improvement in CY-BOCS scores with a large within-group effect-size (d = 1.33). However, in-person CBT produced significantly larger effects (d = 2.69) among the same population. |
| Jassi (2021) [66] | London (UK) | 7 | 34 | ICD-11 | Clinical | CY-BOCS 27.7 ± 4.2 | 15.2 ± 1.7 (7–17 years) | 32.4 | N.a. | An autism-adapted CBT manual for adolescents with ASD was found to present significant rates of response (52.9%) and remission (35.3%) that maintained at a 3-month follow-up in a small, naturalistic study. |
| Jassi (2023) [67] | London (UK) | 9 | 619 | ICD-11 | Clinical | CY-BOCS 27.7 ± 4.9 | 14.6 ± 2.2 (6–18 years) | 46.8 | N.a. | Young individuals with OCD + ASD (N = 172) were more likely to endorse poorer insight into their OCD (t = −2.56; p < 0.01), have greater functional impairment (CGAS score t = 4.10; p < 0.01), greater levels of concurrent psychopathology (SDQ total difficulties score t = −6.27; p < 0.01), higher levels of family accommodation (t = −4.32; p < 0.01), and were more likely to be on medication (X2 = 22.6; p < 0.01), compared to OCD youth without concurrent ASD (N = 447). Whilst both groups benefitted from CBT ± medication, the OCD–ASD group had significantly poorer treatment responses (OR = 0.34; p < 0.01). |
| Højgaard (2023) [68] | Multiple (Denmark, Norway, and Sweden) | 7 | 257 | DSM-IV | Community | CY-BOCS 24.7 ± 5.1 | 12.8 ± 2.8 (7–17 years) | 51.4 | N.a. | Of the individuals with OCD, 9.70% presented clinically significant autistic traits (as measured with ASSQ, cut-off 17). Comorbid ADHD (OR 7.06) and tic disorders (OR 7.11), subclinical internalizing and externalizing symptoms according to CBCL (OR from 1.18 to 1.58), low insight (OR 1.79), and ordering/arranging OCD symptoms (OR N.a., p < 0.01) were found to be significantly associated with autistic traits. Individuals with OCD with or without autistic traits did not differ on CBT treatment outcomes. |
| Vause (2015) [69] | Ontario (Canada) | 7 | 14 | DSM-5 | Clinical | CY-BOCS compulsions 14.6 ± 1.6 | 9.7 ± 1.5 (8–12 years) | 35.7 | N.a. | In a preliminary RCT, a combination of traditional CBT and function-based behavioural assessment significantly decreased OCD-like behaviours at post-treatment and a 5-month follow-up (F = 6.98; p = 0.02). |
| Mack (2010) [70] | London (UK) | 6 | 24 | ICD-10 | Clinical | CY-BOCS 24.0 ± 6.8 | 14.3 ± 1.7 (12–18 years) | 16.7 | N.a. | Individuals with OCD only did not present statistically significant differences from individuals with co-occurrent OCD and ASD. However, individuals meeting criteria for both diagnoses reported more peer relationship problems. |
3. Results
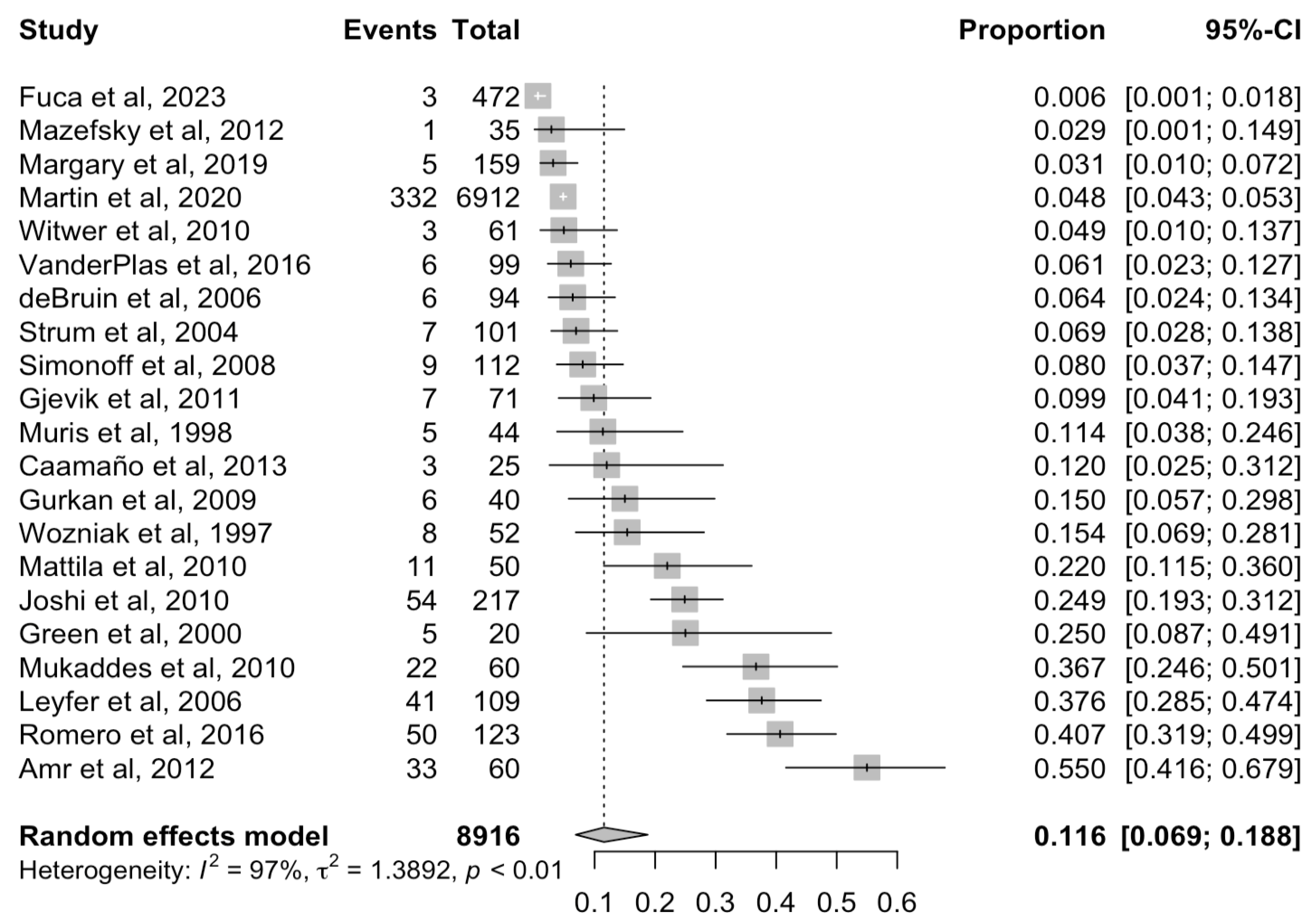
3.1. Prevalence of Obsessive Compulsive Disorder among Children and Adolescents with Autism Spectrum Disorder
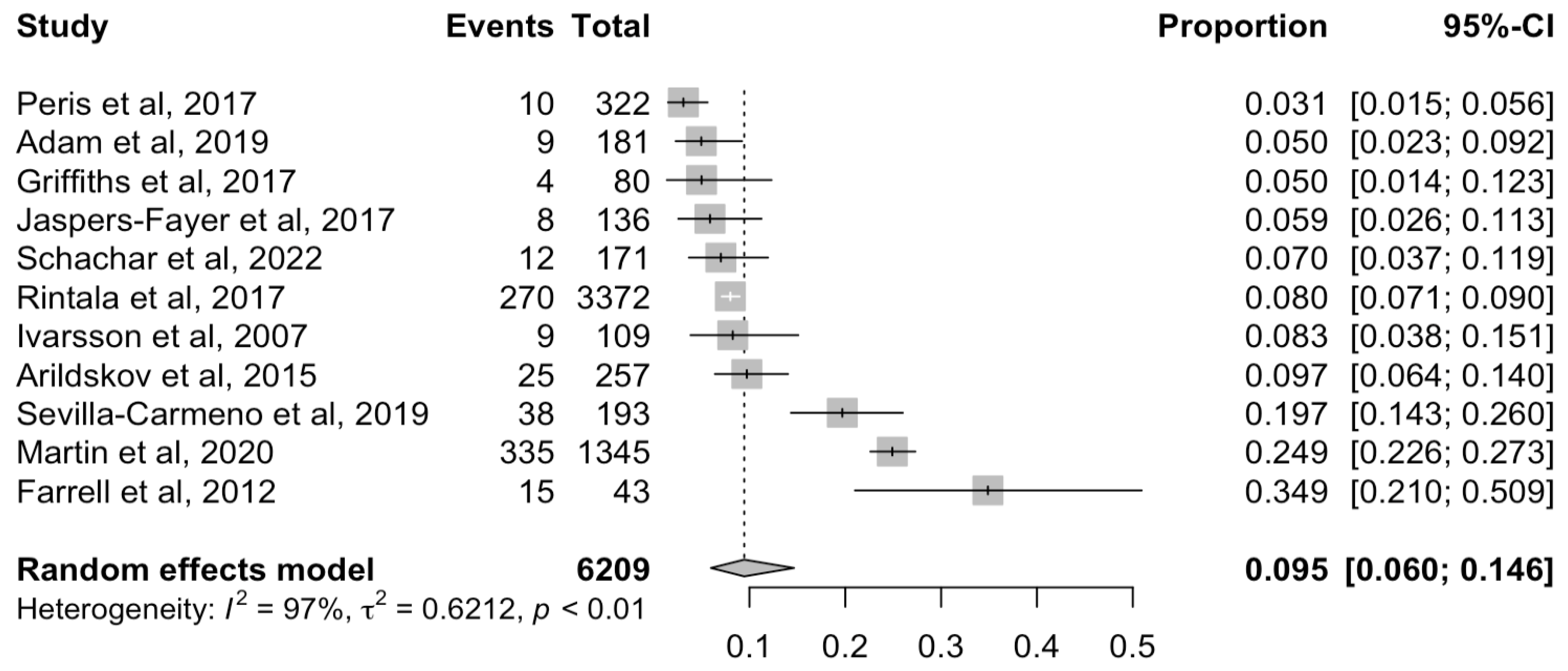
3.2. Prevalence of Autism Spectrum Disorder among Children and Adolescents with Obsessive Compulsive Disorder
3.3. Sociodemographic Factors
3.4. Psychopathological Features
3.5. Prognostic Factors
3.6. Therapeutic Factors
3.7. Quality of the Included Studies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statements
Conflicts of Interest
References
- Anonymous. Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association Publishing: Washington, DC, USA, 2022. [Google Scholar]
- Rydzewska, E.; Dunn, K.; Cooper, S. Umbrella systematic review of systematic reviews and meta-analyses on comorbid physical conditions in people with autism spectrum disorder. Br. J. Psychiatry 2021, 218, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Lai, M.; Kassee, C.; Besney, R.; Bonato, S.; Hull, L.; Mandy, W.; Szatmari, P.; Ameis, S.H. Prevalence of co-occurring mental health diagnoses in the autism population: A systematic review and meta-analysis. Lancet Psychiatry 2019, 6, 819–829. [Google Scholar] [CrossRef] [PubMed]
- Mutluer, T.; Aslan Genç, H.; Özcan Morey, A.; Yapici Eser, H.; Ertinmaz, B.; Can, M.; Munir, K. Population-Based Psychiatric Comorbidity in Children and Adolescents With Autism Spectrum Disorder: A Meta-Analysis. Front. Psychiatry 2022, 13, 856208. [Google Scholar] [CrossRef] [PubMed]
- Hossain, M.M.; Khan, N.; Sultana, A.; Ma, P.; McKyer, E.; Ahmed, H.U.; Purohit, N. Prevalence of comorbid psychiatric disorders among people with autism spectrum disorder: An umbrella review of systematic reviews and meta-analyses. Psychiatry Res. 2020, 287, 112922. [Google Scholar] [CrossRef] [PubMed]
- Stein, D.J.; Costa, D.L.C.; Lochner, C.; Miguel, E.C.; Reddy, Y.C.J.; Shavitt, R.G.; van den Heuvel, O.A.; Simpson, H.B. Obsessive–compulsive disorder. Nat. Rev. Dis. Primers 2019, 5, 52. [Google Scholar] [CrossRef] [PubMed]
- Sharma, E.; Sharma, L.P.; Balachander, S.; Lin, B.; Manohar, H.; Khanna, P.; Lu, C.; Garg, K.; Thomas, T.L.; Au, A.C.L.; et al. Comorbidities in Obsessive-Compulsive Disorder Across the Lifespan: A Systematic Review and Meta-Analysis. Front. Psychiatry 2021, 12, 703701. [Google Scholar] [CrossRef] [PubMed]
- Paula-Pérez, I. Diagnóstico diferencial entre el trastorno obsesivo compulsivo y los patrones de comportamiento, actividades e intereses restringidos y repetitivos en los trastornos del espectro autista. Rev. Psiquiatr. Salud Ment. 2013, 6, 178–186. [Google Scholar] [CrossRef] [PubMed]
- Paula-Pérez, I. Differential diagnosis between obsessive compulsive disorder and restrictive and repetitive behavioural patterns, activities and interests in autism spectrum disorders. Rev. Psiquiatr. Salud Ment. 2013, 6, 178–186. [Google Scholar] [CrossRef]
- Jiujias, M.; Kelley, E.; Hall, L. Restricted, Repetitive Behaviors in Autism Spectrum Disorder and Obsessive–Compulsive Disorder: A Comparative Review. Child Psychiatry Hum. Dev. 2017, 48, 944–959. [Google Scholar] [CrossRef] [PubMed]
- Militerni, R.; Bravaccio, C.; Falco, C.; Fico, C.; Palermo, M.T. Repetitive behaviors in autistic disorder. Eur. Child Adolesc. Psychiatry 2002, 11, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Veale, D.; Roberts, A. Obsessive-compulsive disorder. BMJ 2014, 348, g2183. [Google Scholar] [CrossRef]
- Postorino, V.; Kerns, C.M.; Vivanti, G.; Bradshaw, J.; Siracusano, M.; Mazzone, L. Anxiety Disorders and Obsessive-Compulsive Disorder in Individuals with Autism Spectrum Disorder. Curr. Psychiatry Rep. 2017, 19, 92. [Google Scholar] [CrossRef] [PubMed]
- Weston, L.; Hodgekins, J.; Langdon, P.E. Effectiveness of cognitive behavioural therapy with people who have autistic spectrum disorders: A systematic review and meta-analysis. Clin. Psychol. Rev. 2016, 49, 41–54. [Google Scholar] [CrossRef] [PubMed]
- Pazuniak, M.; Pekrul, S.R. Obsessive–Compulsive Disorder in Autism Spectrum Disorder Across the Lifespan. Child Adolesc. Psychiatr. Clin. N. Am. 2020, 29, 419–432. [Google Scholar] [CrossRef]
- Kerns, C.M.; Kendall, P.C. The Presentation and Classification of Anxiety in Autism Spectrum Disorder. Clin. Psychol. 2012, 19, 323–347. [Google Scholar] [CrossRef]
- Van der Plas, E.; Dupuis, A.; Arnold, P.; Crosbie, J.; Schachar, R. Association of Autism Spectrum Disorder with Obsessive-Compulsive and Attention-Deficit/Hyperactivity Traits and Response Inhibition in a Community Sample. J. Autism Dev. Disord. 2016, 46, 3115–3125. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269, W64. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.G.; Simera, I.; Hoey, J.; Moher, D.; Schulz, K. EQUATOR: Reporting guidelines for health research. Lancet 2008, 371, 1149–1150. [Google Scholar] [CrossRef] [PubMed]
- Anonymous. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV-TR; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Anonymous. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- World Health Organization. International Classification of Diseases, Eleventh Revision (ICD-11). 2021. Available online: https://icd.who.int/browse11 (accessed on 1 February 2024).
- Anonymous. The ICD-10 Classification of Mental and Behavioural Disorders; WHO: Geneva, Switzerland, 1993. [Google Scholar]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Non-Randomized Studies in Meta-Analyses. 2012. Available online: http://wwwohrica/programs/clinical_epidemiology/oxfordasp2021 (accessed on 23 January 2024).
- Ioannidis, J.P.A.; Patsopoulos, N.A.; Evangelou, E. Uncertainty in heterogeneity estimates in meta-analyses. BMJ 2007, 335, 914–916. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- R Foundation for Statistical Computing. R: A Language and Environment for Statistical Computing. version 1.4.1106. 2021. Available online: https://www.R-project.org (accessed on 12 December 2023).
- Amr, M.; Raddad, D.; El-Mehesh, F.; Bakr, A.; Sallam, K.; Amin, T. Comorbid psychiatric disorders in Arab children with Autism spectrum disorders. Res. Autism Spectr. Disord. 2012, 6, 240–248. [Google Scholar] [CrossRef]
- Gürkan, K.; Akçakin, M.; Kiliç, B.; Bilgiç, A. Psychiatric Comorbidity and Drug Treatments in High Functioning Children and Adolescents with Pervasive Developmental Disorders. Neurol. Psychiatry Brain Res. 2008, 15, 143–150. [Google Scholar]
- Leyfer, O.T.; Folstein, S.E.; Bacalman, S.; Davis, N.O.; Dinh, E.; Morgan, J.; Tager-Flusberg, H.; Lainhart, J.E. Comorbid Psychiatric Disorders in Children with Autism: Interview Development and Rates of Disorders. J. Autism Dev. Disord. 2006, 36, 849–861. [Google Scholar] [CrossRef] [PubMed]
- Margari, L.; Palumbi, R.; Peschechera, A.; Craig, F.; de Giambattista, C.; Ventura, P.; Margari, F. Sex-Gender Comparisons in Comorbidities of Children and Adolescents With High-Functioning Autism Spectrum Disorder. Front. Psychiatry 2019, 10, 159. [Google Scholar] [CrossRef] [PubMed]
- Mazefsky, C.A.; Oswald, D.P.; Day, T.N.; Eack, S.M.; Minshew, N.J.; Lainhart, J.E. ASD, a Psychiatric Disorder, or Both? Psychiatric Diagnoses in Adolescents with High-Functioning ASD. J. Clin. Child Adolesc. Psychol. 2012, 41, 516–523. [Google Scholar] [CrossRef] [PubMed]
- Sturm, H.; Fernell, E.; Gillberg, C. Autism spectrum disorders in children with normal intellectual levels: Associated impairments and subgroups. Dev. Med. Child Neurol. 2004, 46, 444–447. [Google Scholar] [CrossRef]
- Fucà, E.; Guerrera, S.; Valeri, G.; Casula, L.; Novello, R.L.; Menghini, D.; Vicari, S. Psychiatric Comorbidities in Children and Adolescents with High-Functioning Autism Spectrum Disorder: A Study on Prevalence, Distribution and Clinical Features in an Italian Sample. J. Clin. Med. 2023, 12, 677. [Google Scholar] [CrossRef] [PubMed]
- Gjevik, E.; Eldevik, S.; Fjæran-Granum, T.; Sponheim, E. Kiddie-SADS Reveals High Rates of DSM-IV Disorders in Children and Adolescents with Autism Spectrum Disorders. J. Autism Dev. Disord. 2011, 41, 761–769. [Google Scholar] [CrossRef] [PubMed]
- Joshi, G.; Petty, C.; Wozniak, J.; Henin, A.; Fried, R.; Galdo, M.; Kotarski, M.; Walls, S.; Biederman, J. The Heavy Burden of Psychiatric Comorbidity in Youth with Autism Spectrum Disorders: A Large Comparative Study of a Psychiatrically Referred Population. J. Autism Dev. Disord. 2010, 40, 1361–1370. [Google Scholar] [CrossRef] [PubMed]
- Romero, M.; Aguilar, J.M.; Del-Rey-Mejías, Á.; Mayoral, F.; Rapado, M.; Peciña, M.; Barbancho, M.Á.; Ruiz-Veguilla, M.; Lara, J.P. Psychiatric comorbidities in autism spectrum disorder: A comparative study between DSM-IV-TR and DSM-5 diagnosis. Int. J. Clin. Health Psychol. 2016, 16, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Caamaño, M.; Boada, L.; Merchán-Naranjo, J.; Moreno, C.; Llorente, C.; Moreno, D.; Arango, C.; Parellada, M. Psychopathology in Children and Adolescents with ASD Without Mental Retardation. J. Autism Dev. Disord. 2013, 43, 2442–2449. [Google Scholar] [CrossRef]
- Muris, P.; Steerneman, P.; Merckelbach, H.; Holdrinet, I.; Meesters, C. Comorbid Anxiety Symptoms in Children with Pervasive Developmental Disorders. J. Anxiety Disord. 1998, 12, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Simonoff, E.; Pickles, A.; Charman, T.; Chandler, S.; Loucas, T.; Baird, G. Psychiatric Disorders in Children With Autism Spectrum Disorders: Prevalence, Comorbidity, and Associated Factors in a Population-Derived Sample. J. Am. Acad. Child Adolesc. Psychiatry 2008, 47, 921–929. [Google Scholar] [CrossRef] [PubMed]
- De Bruin, E.I.; Ferdinand, R.F.; Meester, S.; de Nijs, P.F.A.; Verheij, F. High Rates of Psychiatric Co-Morbidity in PDD-NOS. J. Autism Dev. Disord. 2007, 37, 877–886. [Google Scholar] [CrossRef] [PubMed]
- Green, J.; Gilchrist, A.; Burton, D.; Cox, A. Social and psychiatric functioning in adolescents with Asperger syndrome compared with conduct disorder. J. Autism Dev. Disord. 2000, 30, 279–293. [Google Scholar] [CrossRef] [PubMed]
- Mattila, M.; Hurtig, T.; Haapsamo, H.; Jussila, K.; Kuusikko-Gauffin, S.; Kielinen, M.; Linna, S.; Ebeling, H.; Bloigu, R.; Joskitt, L.; et al. Comorbid Psychiatric Disorders Associated with Asperger Syndrome/High-functioning Autism: A Community- and Clinic-based Study. J. Autism Dev. Disord. 2010, 40, 1080–1093. [Google Scholar] [CrossRef]
- Mukaddes, N.M.; Hergüner, S.; Tanidir, C. Psychiatric disorders in individuals with high-functioning autism and Asperger’s disorder: Similarities and differences. World J. Biol. Psychiatry 2010, 11, 964–971. [Google Scholar] [CrossRef]
- Witwer, A.N.; Lecavalier, L. Validity of Comorbid Psychiatric Disorders in Youngsters with Autism Spectrum Disorders. J. Dev. Phys. Disabil. 2010, 22, 367–380. [Google Scholar] [CrossRef]
- Wozniak, J.; Biederman, J.; Faraone, S.V.; Frazier, J.; Kim, J.; Millstein, R.; Gershon, J.; Thornell, A.; Cha, K.; Snyder, J.B. Mania in Children With Pervasive Developmental Disorder Revisited. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 1552–1559. [Google Scholar] [CrossRef]
- King, B.H.; Hollander, E.; Sikich, L.; McCracken, J.T.; Scahill, L.; Bregman, J.D.; Donnelly, C.L.; Anagnostou, E.; Dukes, K.; Sullivan, L.; et al. Lack of Efficacy of Citalopram in Children With Autism Spectrum Disorders and High Levels of Repetitive Behavior: Citalopram Ineffective in Children With Autism. Arch. Gen. Psychiatry 2009, 66, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Iniesta-Sepúlveda, M.; Nadeau, J.M.; Ramos, A.; Kay, B.; Riemann, B.C.; Storch, E.A. An Initial Case Series of Intensive Cognitive–Behavioral Therapy for Obsessive–Compulsive Disorder in Adolescents with Autism Spectrum Disorder. Child Psychiatry Hum. Dev. 2018, 49, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Mandell, D.S. Psychiatric Hospitalization Among Children with Autism Spectrum Disorders. J. Autism Dev. Disord. 2008, 38, 1059–1065. [Google Scholar] [CrossRef] [PubMed]
- Rintala, H.; Chudal, R.; Leppämäki, S.; Leivonen, S.; Hinkka-Yli-Salomäki, S.; Sourander, A. Register-based study of the incidence, comorbidities and demographics of obsessive-compulsive disorder in specialist healthcare. BMC Psychiatry 2017, 17, 64. [Google Scholar] [CrossRef]
- Schachar, R.J.; Dupuis, A.; Anagnostou, E.; Georgiades, S.; Soreni, N.; Arnold, P.D.; Burton, C.L.; Crosbie, J. Obsessive-compulsive disorder in children and youth: Neurocognitive function in clinic and community samples. J. Child Psychol. Psychiatry 2022, 63, 881–889. [Google Scholar] [CrossRef]
- Griffiths, D.L.; Farrell, L.J.; Waters, A.M.; White, S.W. ASD Traits Among Youth with Obsessive–Compulsive Disorder. Child Psychiatry Hum. Dev. 2017, 48, 911–921. [Google Scholar] [CrossRef] [PubMed]
- Farrell, L.; Waters, A.; Milliner, E.; Ollendick, T. Comorbidity and treatment response in pediatric obsessive-compulsive disorder: A pilot study of group cognitive-behavioral treatment. Psychiatry Res. 2012, 199, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Arildskov, T.W.; Højgaard, D.R.M.A.; Skarphedinsson, G.; Thomsen, P.H.; Ivarsson, T.; Weidle, B.; Melin, K.H.; Hybel, K.A. Subclinical autism spectrum symptoms in pediatric obsessive–compulsive disorder. Eur. Child Adolesc. Psychiatry 2016, 25, 711–723. [Google Scholar] [CrossRef]
- Ivarsson, T.; Melin, K. Autism spectrum traits in children and adolescents with obsessive-compulsive disorder (OCD). J. Anxiety Disord. 2008, 22, 969–978. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.F.; Jassi, A.; Cullen, A.E.; Broadbent, M.; Downs, J.; Krebs, G. Co-occurring obsessive–compulsive disorder and autism spectrum disorder in young people: Prevalence, clinical characteristics and outcomes. Eur. Child Adolesc. Psychiatry 2020, 29, 1603–1611. [Google Scholar] [CrossRef] [PubMed]
- Jaspers-Fayer, F.; Han, S.H.J.; Chan, E.; McKenney, K.; Simpson, A.; Boyle, A.; Ellwyn, R.; Stewart, S.E. Prevalence of Acute-Onset Subtypes in Pediatric Obsessive-Compulsive Disorder. J. Child Adolesc. Psychopharmacol. 2017, 27, 332–341. [Google Scholar] [CrossRef] [PubMed]
- Adam, J.; Goletz, H.; Mattausch, S.; Plück, J.; Döpfner, M. Psychometric evaluation of a parent-rating and self-rating inventory for pediatric obsessive-compulsive disorder: German OCD Inventory for Children and Adolescents (OCD-CA). Child Adolesc. Psychiatry Ment. Health 2019, 13, 25. [Google Scholar] [CrossRef] [PubMed]
- Sevilla-Cermeño, L.; Isomura, K.; Larsson, H.; Åkerstedt, T.; Vilaplana-Pérez, A.; Lahera, G.; Mataix-Cols, D.; Fernández de la Cruz, L. Insomnia in obsessive-compulsive disorder: A Swedish population-based cohort study. J. Affect. Disord. 2020, 266, 413–416. [Google Scholar] [CrossRef] [PubMed]
- Peris, T.S.; Rozenman, M.; Bergman, R.L.; Chang, S.; O’Neill, J.; Piacentini, J. Developmental and clinical predictors of comorbidity for youth with obsessive compulsive disorder. J. Psychiatr. Res. 2017, 93, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, D.L.; Farrell, L.J.; Waters, A.M.; White, S.W. Clinical correlates of obsessive compulsive disorder and comorbid autism spectrum disorder in youth. J. Obs. Compuls. Relat. Disord. 2017, 14, 90–98. [Google Scholar] [CrossRef]
- Lewin, A.B.; Wood, J.J.; Gunderson, S.; Murphy, T.K.; Storch, E.A. Phenomenology of Comorbid Autism Spectrum and Obsessive-Compulsive Disorders Among Children. J. Dev. Phys. Disabil. 2011, 23, 543–553. [Google Scholar] [CrossRef]
- Murray, K.; Jassi, A.; Mataix-Cols, D.; Barrow, F.; Krebs, G. Outcomes of cognitive behaviour therapy for obsessive–compulsive disorder in young people with and without autism spectrum disorders: A case controlled study. Psychiatry Res. 2015, 228, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Wickberg, F.; Lenhard, F.; Aspvall, K.; Serlachius, E.; Andrén, P.; Johansson, F.; Silverberg-Mörse, M.; Mataix-Cols, D. Feasibility of internet-delivered cognitive-behavior therapy for obsessive-compulsive disorder in youth with autism spectrum disorder: A clinical benchmark study. Internet Interv. 2022, 28, 100520. [Google Scholar] [CrossRef] [PubMed]
- Jassi, A.; Fernández de la Cruz, L.; Russell, A.; Krebs, G. An Evaluation of a New Autism-Adapted Cognitive Behaviour Therapy Manual for Adolescents with Obsessive–Compulsive Disorder. Child Psychiatry Hum. Dev. 2021, 52, 916–927. [Google Scholar] [CrossRef] [PubMed]
- Jassi, A.D.; Vidal-Ribas, P.; Krebs, G.; Mataix-Cols, D.; Monzani, B. Examining clinical correlates, treatment outcomes and mediators in young people with comorbid obsessive–compulsive disorder and autism spectrum disorder. Eur. Child Adolesc. Psychiatry 2023, 32, 1201–1210. [Google Scholar] [CrossRef] [PubMed]
- Højgaard, D.R.M.A.; Arildskov, T.W.; Skarphedinsson, G.; Hybel, K.A.; Ivarsson, T.; Weidle, B.; Melin, K.; Torp, N.C.; Thomsen, P.H. Do Autistic Traits Predict Outcome of Cognitive Behavioral Therapy in Pediatric Obsessive-Compulsive Disorder? Res. Child Adolesc. Psychopathol. 2023, 51, 1083–1095. [Google Scholar] [CrossRef] [PubMed]
- Vause, T.; Neil, N.; Jaksic, H.; Jackiewicz, G.; Feldman, M. Preliminary Randomized Trial of Function-Based Cognitive-Behavioral Therapy to Treat Obsessive Compulsive Behavior in Children With Autism Spectrum Disorder. Focus Autism Other Dev. Disabil. 2017, 32, 218–228. [Google Scholar] [CrossRef]
- Mack, H.; Fullana, M.A.; Russell, A.J.; Mataix-Cols, D.; Nakatani, E.; Heyman, I. Obsessions and Compulsions in Children with Asperger’s Syndrome or High-Functioning Autism: A Case-Control Study. Aust. N. Z. J. Psychiatry 2010, 44, 1082–1088. [Google Scholar] [CrossRef] [PubMed]
- PRISMA. PRISMA Flow Diagram. Available online: http://prisma-statement.org/prismastatement/flowdiagram.aspx (accessed on 12 September 2021).
- Berkson, J. Limitations of the Application of Fourfold Table Analysis to Hospital Data. Leuk. Res. 2014, 43, 511–515. [Google Scholar] [CrossRef] [PubMed]
- Geller, D.A. Obsessive-Compulsive and Spectrum Disorders in Children and Adolescents. Psychiatr. Clin. N. Am. 2006, 29, 353–370. [Google Scholar] [CrossRef] [PubMed]
- Zeidan, J.; Fombonne, E.; Scorah, J.; Ibrahim, A.; Durkin, M.S.; Saxena, S.; Yusuf, A.; Shih, A.; Elsabbagh, M. Global prevalence of autism: A systematic review update. Autism Res. 2022, 15, 778–790. [Google Scholar] [CrossRef] [PubMed]
- Yeh, T.; Chen, M.; Bai, Y.; Tsai, S.; Hsu, J.; Huang, K.; Su, T.; Chen, T.; Liang, C. Longitudinal follow-up of subsequent psychiatric comorbidities among children and adolescents with autism spectrum disorder. J. Affect. Disord. 2023, 331, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Rosen, T.E.; Mazefsky, C.A.; Vasa, R.A.; Lerner, M.D. Co-occurring psychiatric conditions in autism spectrum disorder. Int. Rev. Psychiatry 2018, 30, 40–61. [Google Scholar] [CrossRef] [PubMed]
- Ozyurt, G.; Besiroglu, L. Autism Spectrum Symptoms in Children and Adolescents with Obsessive Compulsive Disorder and Their Mothers. Noro Psikiyatr. Arsivi 2018, 55, 40–48. [Google Scholar] [CrossRef]
- Hollander, E.; King, A.; Delaney, K.; Smith, C.J.; Silverman, J.M. Obsessive–compulsive behaviors in parents of multiplex autism families. Psychiatry Res. 2003, 117, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Samuels, J.F.; Wang, Y.; Cao, H.; Ritter, M.; Nestadt, P.S.; Krasnow, J.; Greenberg, B.D.; Fyer, A.J.; McCracken, J.T.; et al. Polygenic risk score and heritability estimates reveals a genetic relationship between ASD and OCD. Eur. Neuropsychopharmacol. 2017, 27, 657–666. [Google Scholar] [CrossRef] [PubMed]
- Strom, N.I.; Grove, J.; Meier, S.M.; Bækvad-Hansen, M.; Becker Nissen, J.; Damm Als, T.; Halvorsen, M.; Nordentoft, M.; Mortensen, P.B.; Hougaard, D.M.; et al. Polygenic Heterogeneity Across Obsessive-Compulsive Disorder Subgroups Defined by a Comorbid Diagnosis. Front. Genet. 2021, 12, 711624. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Cao, H.; Kural, K.C.; Fang, Q.; Zhang, F. Integrative analysis of shared genetic pathogenesis by autism spectrum disorder and obsessive-compulsive disorder. Biosci. Rep. 2019, 39, BSR20191942. [Google Scholar] [CrossRef] [PubMed]
- Jacob, S.; Landeros-Weisenberger, A.; Leckman, J.F. Autism spectrum and obsessive-compulsive disorders: OC behaviors, phenotypes and genetics. Autism Res. 2009, 2, 293–311. [Google Scholar] [CrossRef] [PubMed]
- Talantseva, O.I.; Romanova, R.S.; Shurdova, E.M.; Dolgorukova, T.A.; Sologub, P.S.; Titova, O.S.; Kleeva, D.F.; Grigorenko, E.L. The global prevalence of autism spectrum disorder: A three-level meta-analysis. Front. Psychiatry 2023, 14, 1071181. [Google Scholar] [CrossRef] [PubMed]
- Fawcett, E.J.; Power, H.; Fawcett, J.M. Women Are at Greater Risk of OCD Than Men. Br. J. Psychol. 2020, 81, 19r13085. [Google Scholar] [CrossRef] [PubMed]
- Ruscio, A.M.; Stein, D.J.; Chiu, W.T.; Kessler, R.C. The epidemiology of obsessive-compulsive disorder in the National Comorbidity Survey Replication. Mol. Psychiatry 2010, 15, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Scahill, L.; Mcdougle, C.J.; Williams, S.K.; Dimitropoulos, A.; Aman, M.G.; Mccracken, J.T.; Tierney, E.; Arnold, L.E.; Cronin, P.; Grados, M.; et al. Children’s Yale-Brown Obsessive Compulsive Scale Modified for Pervasive Developmental Disorders. J. Am. Acad. Child Adolesc. Psychiatry 2006, 45, 1114–1123. [Google Scholar] [CrossRef]
- Uljarevic, M.; Hamilton, A. Recognition of Emotions in Autism: A Formal Meta-Analysis. J. Autism Dev. Disord. 2013, 43, 1517–1526. [Google Scholar] [CrossRef]
- Demetriou, E.A.; DeMayo, M.M.; Guastella, A.J. Executive Function in Autism Spectrum Disorder: History, Theoretical Models, Empirical Findings, and Potential as an Endophenotype. Front. Psychiatry 2019, 10, 753. [Google Scholar] [CrossRef] [PubMed]
- Salazar de Pablo, G.; Pascual-Sánchez, A.; Panchal, U.; Clark, B.; Krebs, G. Efficacy of remotely-delivered cognitive behavioural therapy for obsessive-compulsive disorder: An updated meta-analysis of randomised controlled trials. J. Affect. Disord. 2023, 322, 289–299. [Google Scholar] [CrossRef] [PubMed]
- Öst, L.; Riise, E.N.; Wergeland, G.J.; Hansen, B.; Kvale, G. Cognitive behavioral and pharmacological treatments of OCD in children: A systematic review and meta-analysis. J. Anxiety Disord. 2016, 43, 58–69. [Google Scholar] [CrossRef] [PubMed]
- Salazar de Pablo, G.; Pastor Jordá, C.; Vaquerizo-Serrano, J.; Moreno, C.; Cabras, A.; Arango, C.; Hernández, P.; Veenstra-VanderWeele, J.; Simonoff, E.; Fusar-Poli, P.; et al. Systematic Review and Meta-analysis: Efficacy of Pharmacological Interventions for Irritability and Emotional Dysregulation in Autism Spectrum Disorder and Predictors of Response. J. Am. Acad. Child Adolesc. Psychiatry 2023, 62, 151–168. [Google Scholar] [CrossRef]
- Thamby, A.; Jaisoorya, T. Antipsychotic augmentation in the treatment of obsessive-compulsive disorder. Indian J. Psychiatry 2019, 61, 51–57. [Google Scholar] [CrossRef]
- Siafis, S.; Çıray, O.; Wu, H.; Schneider-Thoma, J.; Bighelli, I.; Krause, M.; Rodolico, A.; Ceraso, A.; Deste, G.; Huhn, M.; et al. Pharmacological and dietary-supplement treatments for autism spectrum disorder: A systematic review and network meta-analysis. Mol. Autism 2022, 13, 10. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aymerich, C.; Pacho, M.; Catalan, A.; Yousaf, N.; Pérez-Rodríguez, V.; Hollocks, M.J.; Parellada, M.; Krebs, G.; Clark, B.; Salazar de Pablo, G. Prevalence and Correlates of the Concurrence of Autism Spectrum Disorder and Obsessive Compulsive Disorder in Children and Adolescents: A Systematic Review and Meta-Analysis. Brain Sci. 2024, 14, 379. https://doi.org/10.3390/brainsci14040379
Aymerich C, Pacho M, Catalan A, Yousaf N, Pérez-Rodríguez V, Hollocks MJ, Parellada M, Krebs G, Clark B, Salazar de Pablo G. Prevalence and Correlates of the Concurrence of Autism Spectrum Disorder and Obsessive Compulsive Disorder in Children and Adolescents: A Systematic Review and Meta-Analysis. Brain Sciences. 2024; 14(4):379. https://doi.org/10.3390/brainsci14040379
Chicago/Turabian StyleAymerich, Claudia, Malein Pacho, Ana Catalan, Noorulain Yousaf, Violeta Pérez-Rodríguez, Matthew J. Hollocks, Mara Parellada, Georgina Krebs, Bruce Clark, and Gonzalo Salazar de Pablo. 2024. "Prevalence and Correlates of the Concurrence of Autism Spectrum Disorder and Obsessive Compulsive Disorder in Children and Adolescents: A Systematic Review and Meta-Analysis" Brain Sciences 14, no. 4: 379. https://doi.org/10.3390/brainsci14040379
APA StyleAymerich, C., Pacho, M., Catalan, A., Yousaf, N., Pérez-Rodríguez, V., Hollocks, M. J., Parellada, M., Krebs, G., Clark, B., & Salazar de Pablo, G. (2024). Prevalence and Correlates of the Concurrence of Autism Spectrum Disorder and Obsessive Compulsive Disorder in Children and Adolescents: A Systematic Review and Meta-Analysis. Brain Sciences, 14(4), 379. https://doi.org/10.3390/brainsci14040379