
Clinical and Immunologic Efficacy of the Recombinant Adenovirus Type-5-Vectored (CanSino Bio) Vaccine in University Professors during the COVID-19 Delta Wave

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
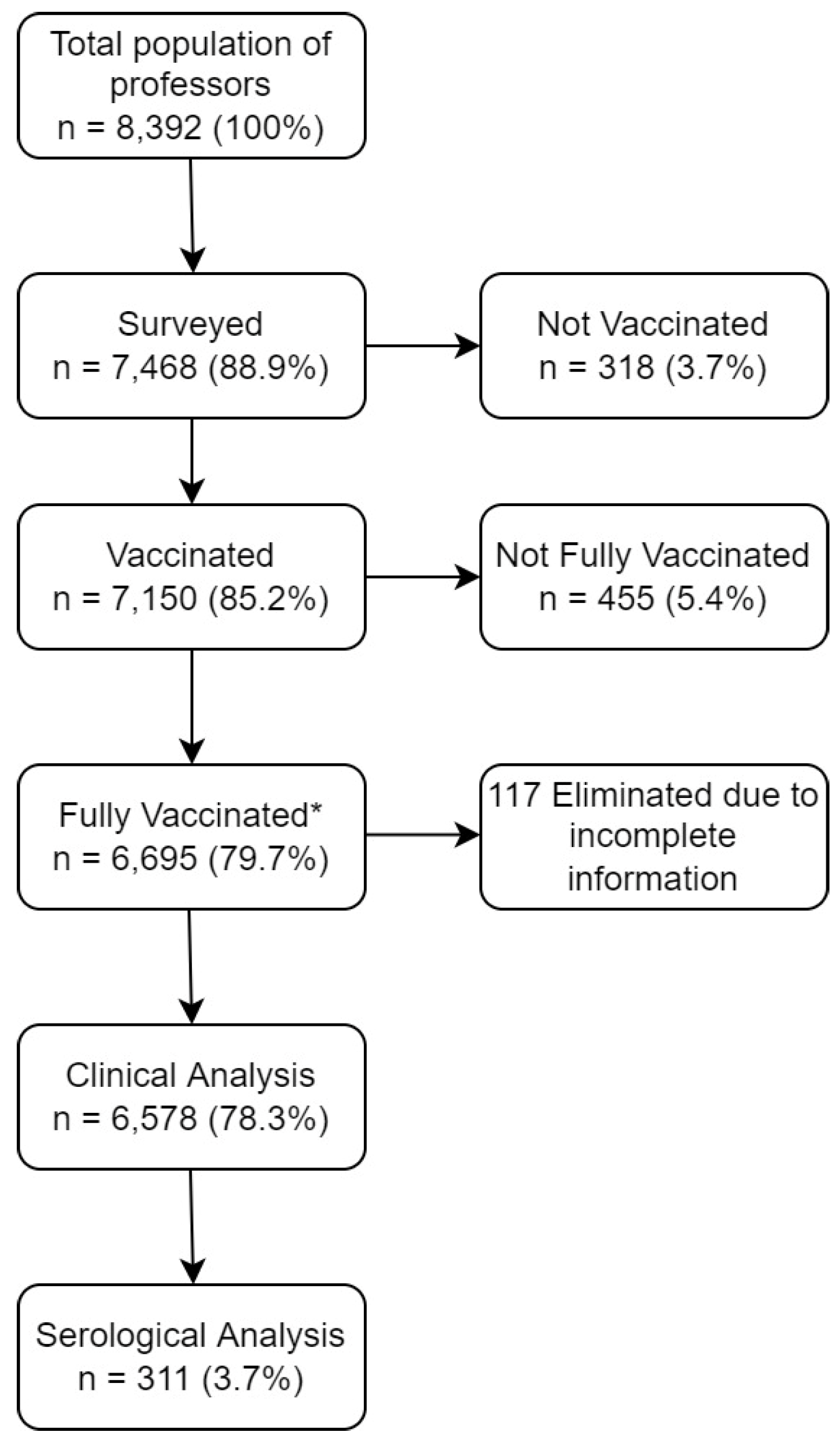
2.2. Study Design and Participants
2.3. Blood Sampling and Antibody Measurement
2.4. Definitions
2.5. Statistical Analysis
3. Results
3.1. Clinical and Epidemiologic Data
3.2. Serologic Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hannah Ritchie, E.M.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Ortiz-Ospina, E.; Hasell, J.; Macdonald, B.; Beltekian, D.; Roser, M. Coronavirus Pandemic (COVID-19). Available online: https://ourworldindata.org/coronavirus (accessed on 23 October 2021).
- Javier Silva, L.A.; Rosario Pacahuala, E.A. Governments and vaccination against COVID-19. Vacunas 2021, 22, 125–126. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. COVID-19 Vaccine Tracker and Landscape. Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines (accessed on 25 October 2021).
- Pan American Health Organization. Coronavirus Disease. (In Spanish). Available online: https://www.paho.org/es/documentos/actualizacion-epidemiologica-enfermedad-porcoronavirus-covid-19-9-febrero-2021 (accessed on 23 October 2021).
- Chase Harrison, L.H.; Zissis, C. Tracking the path towards vaccination in Latinamerica. (In Spanish). Available online: https://www.as-coa.org/articles/cronologia-rastreando-el-camino-hacia-la-vacunacion-en-america-latina (accessed on 25 October 2021).
- Sáenz-Guzmán, C. Vaccination in teachers will be from April 20 to May 28: Health Secretary of Mexico. (In Spanish). Available online: https://www.capital21.cdmx.gob.mx/noticias/?p=18421 (accessed on 25 October 2021).
- Federal Commission for the Protection against Sanitary Risk. Authorized COVID-19 vaccines. (In Spanish). Available online: https://www.gob.mx/cofepris/acciones-y-programas/vacunas-covid-19-autorizadas (accessed on 11 November 2021).
- Government of Mexico. National Policy of Vaccine administration against SARS-CoV-2 to prevent COVID-19 in Mexico. (In Spanish). Available online: http://vacunacovid.gob.mx/wordpress/wp-content/uploads/2021/09/2021.09.28-PNVx_COVID-1.pdf. (accessed on 28 September 2021).
- Zhu, F.C.; Li, Y.H.; Guan, X.H.; Hou, L.H.; Wang, W.J.; Li, J.X.; Wu, S.P.; Wang, B.S.; Wang, Z.; Wang, L.; et al. Safety, tolerability, and immunogenicity of a recombinant adenovirus type-5 vectored COVID-19 vaccine: A dose-escalation, open-label, non-randomised, first-in-human trial. Lancet 2020, 395, 1845–1854. [Google Scholar] [CrossRef]
- Kaur, S.P.; Gupta, V. COVID-19 Vaccine: A comprehensive status report. Virus Res. 2020, 288, 198114. [Google Scholar] [CrossRef] [PubMed]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cardenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against COVID-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef] [PubMed]
- Logunov, D.Y.; Dolzhikova, I.V.; Shcheblyakov, D.V.; Tukhvatulin, A.I.; Zubkova, O.V.; Dzharullaeva, A.S.; Kovyrshina, A.V.; Lubenets, N.L.; Grousova, D.M.; Erokhova, A.S.; et al. Safety and efficacy of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine: An interim analysis of a randomised controlled phase 3 trial in Russia. Lancet 2021, 397, 671–681. [Google Scholar] [CrossRef]
- Zhang, Y.; Zeng, G.; Pan, H.; Li, C.; Hu, Y.; Chu, K.; Han, W.; Chen, Z.; Tang, R.; Yin, W.; et al. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine in healthy adults aged 18-59 years: A randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. Lancet Infect. Dis. 2021, 21, 181–192. [Google Scholar] [CrossRef]
- Zhu, F.C.; Guan, X.H.; Li, Y.H.; Huang, J.Y.; Jiang, T.; Hou, L.H.; Li, J.X.; Yang, B.F.; Wang, L.; Wang, W.J.; et al. Immunogenicity and safety of a recombinant adenovirus type-5-vectored COVID-19 vaccine in healthy adults aged 18 years or older: A randomised, double-blind, placebo-controlled, phase 2 trial. Lancet 2020, 396, 479–488. [Google Scholar] [CrossRef]
- Zhu, F.; Jin, P.; Zhu, T.; Wang, W.; Ye, H.; Pan, H.; Hou, L.; Li, J.; Wang, X.; Wu, S.; et al. Safety and immunogenicity of a recombinant adenovirus type-5-vectored COVID-19 vaccine with a homologous prime-boost regimen in healthy participants aged 6 years and above: A randomised, double-blind, placebo-controlled, phase 2b trial. Clin. Infect. Dis. 2021, ciab845. [Google Scholar] [CrossRef] [PubMed]
- Assadiasl, S.; Fatahi, Y.; Zavvar, M.; Nicknam, M.H. COVID-19: Significance of antibodies. Human Antibodies 2020, 28, 287–297. [Google Scholar] [CrossRef] [PubMed]
- Earle, K.A.; Ambrosino, D.M.; Fiore-Gartland, A.; Goldblatt, D.; Gilbert, P.B.; Siber, G.R.; Dull, P.; Plotkin, S.A. Evidence for antibody as a protective correlate for COVID-19 vaccines. Vaccine 2021, 39, 4423–4428. [Google Scholar] [CrossRef] [PubMed]
- Guzman-Martinez, O.; Guardado, K.; de Guevara, E.L.; Navarro, S.; Hernandez, C.; Zenteno-Cuevas, R.; Montero, H. IgG Antibodies Generation and Side Effects Caused by Ad5-nCoV Vaccine (CanSino Biologics) and BNT162b2 Vaccine (Pfizer/BioNTech) among Mexican Population. Vaccines 2021, 9, 999. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Bello, J.; Morales-Nunez, J.J.; Machado-Sulbaran, A.C.; Diaz-Perez, S.A.; Torres-Hernandez, P.C.; Balcazar-Felix, P.; Gutierrez-Brito, J.A.; Lomeli-Nieto, J.A.; Munoz-Valle, J.F. Neutralizing Antibodies against SARS-CoV-2, Anti-Ad5 Antibodies, and Reactogenicity in Response to Ad5-nCoV (CanSino Biologics) Vaccine in Individuals with and without Prior SARS-CoV-2. Vaccines 2021, 9, 1047. [Google Scholar] [CrossRef] [PubMed]
- Government of Mexico. COVID-19 Daily Technical Report in Mexico. (In Spanish). Available online: https://www.gob.mx/cms/uploads/attachment/file/661859/Comunicado_Tecnico_Diario_COVID-19_2021.08.12.pdf (accessed on 2 September 2021).
- Consorcio Mexicano de Vigilancia Genómica (CoViGen-Mex). Genomic surveillance program of SARS-CoV-2. Report from 16 June 2021. (In Spanish). Available online: http://mexcov2.ibt.unam.mx:8080/COVID-TRACKER/open/reports/16%20de%20Junio%20del%202021.pdf (accessed on 7 November 2021).
- Consorcio Mexicano de Vigilancia Genómica (CoViGen-Mex). Genomic surveillance program of SARS-CoV-2. Report from 28 July 2021. (In Spanish). Available online: http://mexcov2.ibt.unam.mx:8080/COVID-TRACKER/open/reports/28%20de%20Julio%202021.pdf (accessed on 7 November 2021).
- Consorcio Mexicano de Vigilancia Genómica (CoViGen-Mex). Genomic surveillance program of SARS-CoV-2. Report from 25 August 2021. (In Spanish). Available online: http://mexcov2.ibt.unam.mx:8080/COVID-TRACKER/open/reports/25%20de%20Agosto%20del%202021.pdf (accessed on 7 November 2021).
- Consorcio Mexicano de Vigilancia Genómica (CoViGen-Mex). Genomic surveillance program of SARS-CoV-2. Report from 20 October 2021. (In Spanish). Available online: http://mexcov2.ibt.unam.mx:8080/COVID-TRACKER/open/reports/Lote27_20Octubre2021_IBT_ReporteTotal.pdf (accessed on 7 November 2021).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Falsey, A.R.; Sobieszczyk, M.E.; Hirsch, I.; Sproule, S.; Robb, M.L.; Corey, L.; Neuzil, K.M.; Hahn, W.; Hunt, J.; Mulligan, M.J.; et al. Phase 3 Safety and Efficacy of AZD1222 (ChAdOx1 nCoV-19) COVID-19 Vaccine. N. Engl. J. Med. 2021, 385, 2348–2360. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| After Vaccination | CanSino n = 5360 n (%) | Pfizer/ BioNTech n = 619 n (%) | AstraZeneca/ Oxford n = 466 n (%) | Sputnik V n = 5 n (%) | Janssen/J&J n = 58 n (%) | CoronoVac n = 97 n (%) | Moderna n = 90 n (%) | p-Value * |
|---|---|---|---|---|---|---|---|---|
| Primary breakthrough symptomatic infection | ||||||||
| Total | 224 (4.17) | 14 (2.26) | 10 (2.14) | 0 (0.00) | 2 (3.44) | 1 (1.03) | 2 (2.22) | <0.001 |
| Outpatient | 216 (4.02) | 14 (2.26) | 10 (2.14) | 0 (0.00) | 2 (3.44) | 1 (1.03) | 2 (2.22) | <0.001 |
| Hospitalization | 8 (0.14) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0.21 |
| Supplemental oxygen | 7 (0.13) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0.20 |
| Mechanical ventilation | 1 (0.02) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0.57 |
| Death | 1 (0.02) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0.57 |
| Breakthrough symptomatic reinfection from previously infected participants | ||||||||
| Total | 15 (0.27) | 1 (0.16) | 2 (0.42) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0.64 |
| Outpatient | 14 (0.26) | 1 (0.16) | 2 (0.42) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0.07 |
| Hospitalization | 1 (0.01) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0.57 |
| Supplemental oxygen | 1 (0.01) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0.57 |
| Mechanical ventilation | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | NA |
| Death | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guzmán-López, S.; Darwich-Salazar, A.; Bocanegra-Ibarias, P.; Salas-Treviño, D.; Flores-Treviño, S.; Pérez-Alba, E.; Nuzzolo-Shihadeh, L.M.; Pérez-Rodríguez, E.; Camacho-Ortiz, A. Clinical and Immunologic Efficacy of the Recombinant Adenovirus Type-5-Vectored (CanSino Bio) Vaccine in University Professors during the COVID-19 Delta Wave. Vaccines 2022, 10, 656. https://doi.org/10.3390/vaccines10050656
Guzmán-López S, Darwich-Salazar A, Bocanegra-Ibarias P, Salas-Treviño D, Flores-Treviño S, Pérez-Alba E, Nuzzolo-Shihadeh LM, Pérez-Rodríguez E, Camacho-Ortiz A. Clinical and Immunologic Efficacy of the Recombinant Adenovirus Type-5-Vectored (CanSino Bio) Vaccine in University Professors during the COVID-19 Delta Wave. Vaccines. 2022; 10(5):656. https://doi.org/10.3390/vaccines10050656
Chicago/Turabian StyleGuzmán-López, Santos, Armine Darwich-Salazar, Paola Bocanegra-Ibarias, Daniel Salas-Treviño, Samantha Flores-Treviño, Eduardo Pérez-Alba, Laura M. Nuzzolo-Shihadeh, Edelmiro Pérez-Rodríguez, and Adrián Camacho-Ortiz. 2022. "Clinical and Immunologic Efficacy of the Recombinant Adenovirus Type-5-Vectored (CanSino Bio) Vaccine in University Professors during the COVID-19 Delta Wave" Vaccines 10, no. 5: 656. https://doi.org/10.3390/vaccines10050656