
Influences on Attitudes Regarding COVID-19 Vaccination in Germany


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample and Measuring Instruments
2.2. Structural Equation Modeling (SEM) and Three-Level Path Modeling
2.3. Statistical Analysis of Individual Variables
3. Results
3.1. Overall COVID-19 Vaccine Acceptance
3.2. Sociodemographic Characteristics and Acceptance of COVID-19 Vaccination
3.3. Subject Characteristics Related to Life Satisfaction and Own Health Status
3.4. Subject Characteristics Related to Vaccination and COVID-19
3.5. Statistical Modeling
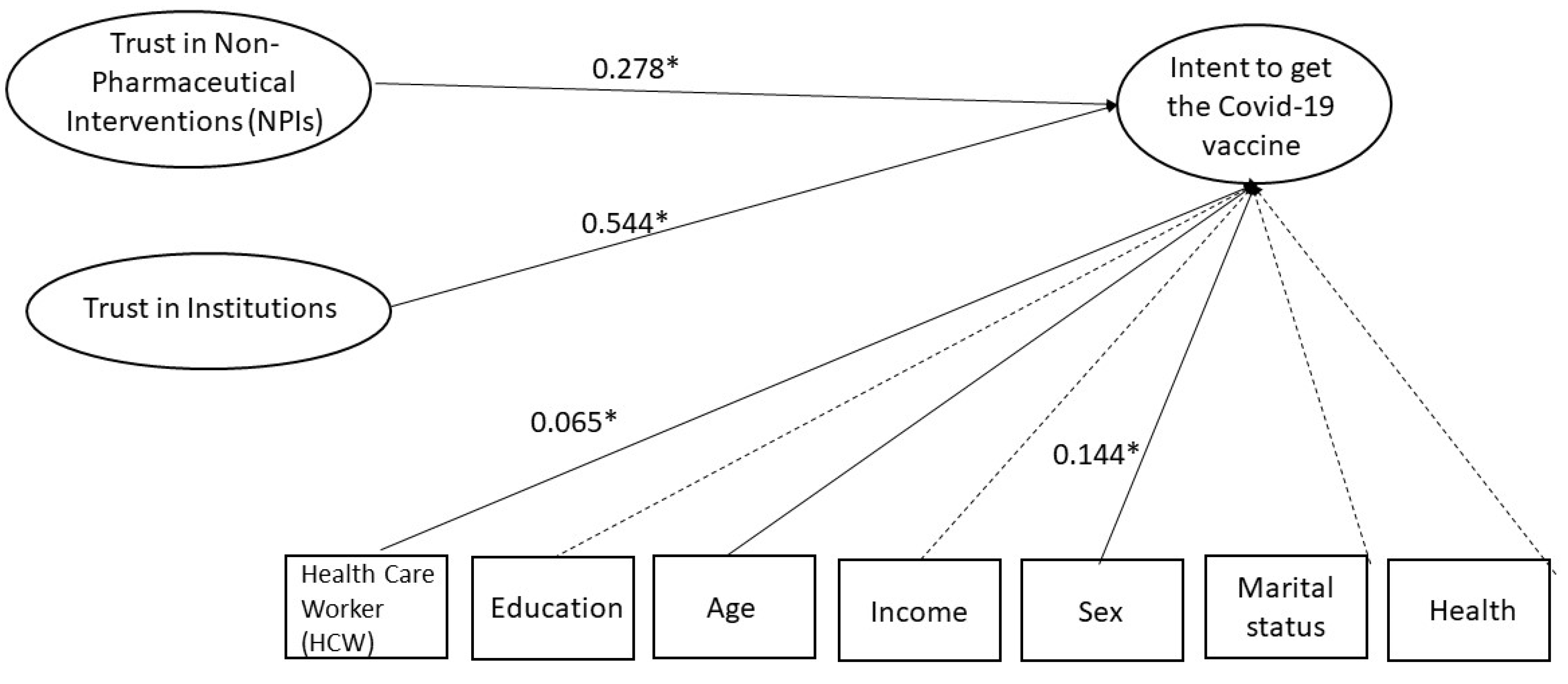
3.5.1. SEM
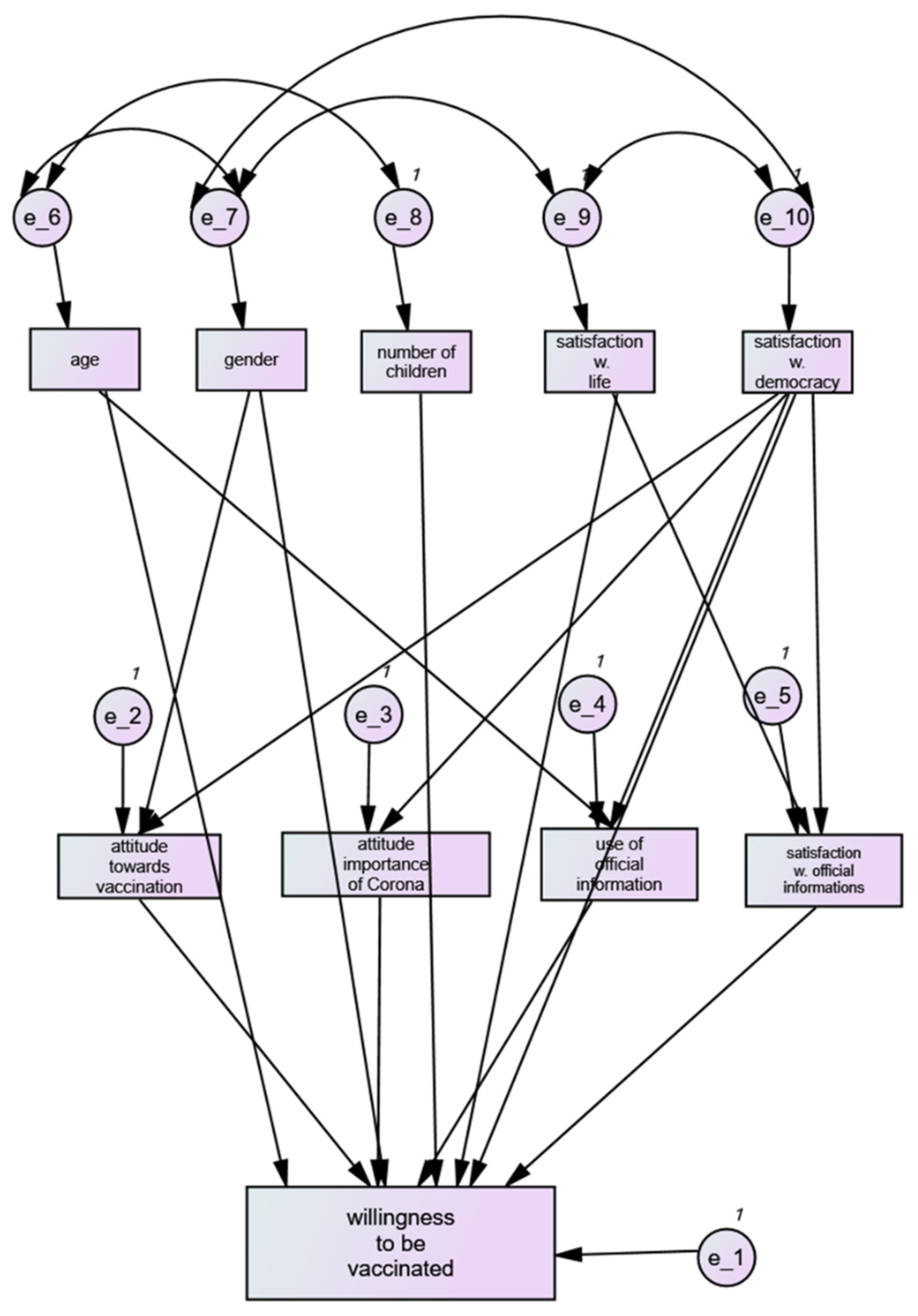
3.5.2. Multivariate Analysis and Path Model
3.6. Results of the Path Model
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fontanet, A.; Cauchemez, S. COVID-19 herd immunity: Where are we? Nat. Rev. Immunol. 2020, 20, 583–584. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kinball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Parliment, E. Vaccine Hesitancy and Drop in Vaccination Rates in Europe. 2018. Available online: https://www.europarl.europa.eu/doceo/document/TA-8-2018-0188_EN.pdf (accessed on 7 March 2022).
- Razai, M.S.; Chaudhry, U.A.; Doerholt, K.; Bauld, L.; Majeed, A. COVID-19 vaccination hesitancy. BMJ 2021, 373, n1138. [Google Scholar] [CrossRef] [PubMed]
- Geoghegan, S.; O’Callaghan, K.P.; Offit, P.A. Vaccine Safety: Myths and Misinformation. Front. Microbiol. 2020, 11, 372. [Google Scholar] [CrossRef] [Green Version]
- Cardona, B. The pitfalls of personalization rhetoric in time of health crisis: COVID-19 pandemic and cracks on neoliberal ideologies. Health Promot. Int. 2021, 36, 714–721. [Google Scholar] [CrossRef] [PubMed]
- Kreps, S.; Prasad, S.; Brownstein, J.S.; Hswen, Y.; Garibaldi, B.T.; Zhang, B.; Kriner, D.L. Factors Associated With US Adults’ Likelihood of Accepting COVID-19 Vaccination. JAMA Netw. Open 2020, 3, e2025594. [Google Scholar] [CrossRef] [PubMed]
- Larson, H.J.; Schulz, W.S.; Tucker, J.D.; Smith, D.M. Measuring vaccine confidence: Introducing a global vaccine confidence index. PLoS Curr. 2015, 7, 13. [Google Scholar] [CrossRef] [PubMed]
- Paul-Ehrlich-Institut. Proof of Vaccination within the Meaning of the Infection Protection Act (IfSG). Available online: https://www.pei.de/EN/newsroom/dossier/coronavirus/coronavirus-content.html?cms_pos=3 (accessed on 23 March 2022).
- University of Erfurt COSMO—COVID-19 Snapshot Monitoring Study. Virusvarianten und Impfen. Available online: https://projekte.uni-erfurt.de/cosmo2020/web/topic/impfung/40-delta-variante/ (accessed on 25 February 2022).
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J.; Schreyogg, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef]
- Detoc, M.; Bruel, S.; Frappe, P.; Tardy, B.; Botelho-Nevers, E.; Gagneux-Brunon, A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine 2020, 38, 7002–7006. [Google Scholar] [CrossRef]
- Verger, P.; Scronias, D.; Dauby, N.; Adedzi, K.A.; Gobert, C.; Bergeat, M.; Gagneur, A.; Dubé, E. Attitudes of healthcare workers towards COVID-19 vaccination: A survey in France and French-speaking parts of Belgium and Canada, 2020. Eurosurveillance 2021, 26, 2002047. [Google Scholar] [CrossRef]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef] [PubMed]
- Ciardi, F.; Menon, V.; Jensen, J.L.; Shariff, M.A.; Pillai, A.; Venugopal, U.; Kasubhsi, M.; Dimitrov, V.; Kanna, B.; Poole, B.D. Knowledge, Attitudes and Perceptions of COVID-19 Vaccination among Healthcare Workers of an Inner-City Hospital in New York. Vaccines 2021, 9, 516. [Google Scholar] [CrossRef] [PubMed]
- Pogue, K.; Jensen, J.L.; Stancil, C.K.; Ferguson, D.G.; Hughes, S.J.; Mello, E.J.; Burgess, R.; Berges, B.K.; Quaye, A.; Poole, B.D. Influences on Attitudes Regarding Potential COVID-19 Vaccination in the United States. Vaccines 2020, 8, 582. [Google Scholar] [CrossRef] [PubMed]
- Yoda, T.; Katsuyama, H. Willingness to Receive COVID-19 Vaccination in Japan. Vaccines 2021, 9, 48. [Google Scholar] [CrossRef]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef]
- Holzmann-Littig, C.; Braunisch, M.C.; Kranke, P.; Popp, M.; Seeber, C.; Fichtner, F.; Litting, B.; Carbajo-Lozoya, J.; Allwang, C.; Frank, T.; et al. COVID-19 Vaccination Acceptance and Hesitancy among Healthcare Workers in Germany. Vaccines 2021, 9, 777. [Google Scholar] [CrossRef] [PubMed]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef] [Green Version]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- ESOMAR. The Role of Data, Research, and Insights Community in Supporting Global Crisis and Post-Crisis Management of COVID-19 Measures. Available online: https://esomar.org/uploads/attachments/cksyl795a02vs04trus9n118r-esomar-management-of-COVID-19-measures.pdf (accessed on 7 March 2022).
- Gadoth, A.; Halbrook, M.; Martin-Blais, R.; Gray, A.; Tobin, N.H.; Ferbas, K.G.; Aldrovandi, G.M.; Rimoin, A.W. Cross-sectional Assessment of COVID-19 Vaccine Acceptance Among Health Care Workers in Los Angeles. Ann. Intern. Med. 2021, 174, 882–885. [Google Scholar] [CrossRef]
- Gagneux-Brunon, A.; Detoc, M.; Bruel, S.; Tardy, B.; Rozaire, O.; Frappe, P.; Botelho-Nevers, E. Intention to get vaccinations against COVID-19 in French healthcare workers during the first pandemic wave: A cross-sectional survey. J. Hosp. Infect. 2021, 108, 168–173. [Google Scholar] [CrossRef]
- Witting, V. Is the Coronavirus Pandemic Undermining German Democracy? Deutsche Welle: Bonn, Germany, 2020. [Google Scholar]
- Gozgor, G. Global Evidence on the Determinants of Public Trust in Governments during the COVID-19. Appl. Res. Qual. Life 2022, 17, 559–578. [Google Scholar] [CrossRef] [PubMed]
- Kantar. Eurobarometer: Resilience and Recovery; Public Opinion One Year into the Pandemic. 2021. Available online: https://www.europarl.europa.eu/at-your-service/files/be-heard/eurobarometer/2021/spring-2021-survey/report.pdf (accessed on 7 March 2022).
- Institute, R.K. Zusammenfassung und Empfehlungen Welle 47. 2021. Available online: https://projekte.uni-erfurt.de/cosmo2020/web/summary/47/ (accessed on 7 March 2022).
- Robert Koch Institute Germany (RKI). COVID-19 Impfquoten-Monitoring in Deutschland (COVIMO)–6; Report. 2021. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Projekte_RKI/COVIMO_Reports/covimo_studie_bericht_6.html;jsessionid=10FF97F90EA7665F2C49F89F9E5A8224.internet071?nn=2444038 (accessed on 7 March 2022).
- Hamel, L.; Lopes, L.; Brodie, M. KFF COVID-19 Vaccine Monitor: What Do We Know About Those Who Want to “Wait and See” Before Getting a COVID-19 Vaccine? 2021. Available online: https://www.kff.org/coronavirus-COVID-19/poll-finding/kff-COVID-19-vaccine-monitor-wait-and-see/ (accessed on 7 March 2022).
- Robert Koch Institute Germany (RKI). Welche Impfquote ist notwendig, um COVID-19 zu kontrollieren? Epidemiol. Bull. 2021, 27, 3–13. [Google Scholar]
- COSMO—COVID-19 Snapshot Monitoring, 7; Booster-Impfung: 18 March 2022. Available online: https://projekte.uni-erfurt.de/cosmo2020/web/topic/impfung/10-impfungen/#booster-impfung (accessed on 7 March 2022).



{kind=link}
{kind=link}
| When a Vaccine for COVID-19 Is Approved and Widely Available to Anyone Who Wants It, Respondent Will: (n = 1092) | Percentage of Sample |
|---|---|
| Get the vaccine immediately | 25.6 |
| Only get the vaccine after consulting with doctor | 25.1 |
| Wait until it has been available for a while to see how it is working for other people | 31.7 |
| Definitely not get the vaccine | 17.6 |
| Total Respondents N = 1092 | N | % | Will Be Vaccinated Right Away (%) | Will Be Vaccinated after Consulting Doctor (%) | Will Wait and See How Others Tolerate Vaccination (%) | Will Not Be Vaccinated at All (%) | |
|---|---|---|---|---|---|---|---|
| Gender (n = 1007) | |||||||
| Male | 434 | 43.1 | 35.0 | 26.5 | 26.3 | 12.1 | p (<0.001) |
| female | 556 | 55.2 | 20.5 | 25.5 | 34.4 | 19.6 | |
| Not male/Not female | 17 | 1.7 | 5.9 | 35.3 | 23.5 | 35.3 | |
| No. children in the family (n = 1092) | |||||||
| Non | 612 | 56.0 | 28.4 | 23.5 | 32.7 | 15.4 | p (<0.001) |
| One child | 232 | 21.2 | 15.9 | 13.2 | 18.3 | 8.6 | |
| Two children | 172 | 15.8 | 23.3 | 29.7 | 34.9 | 12.2 | |
| Three children | 49 | 4.5 | 24.5 | 24.5 | 24.5 | 26.5 | |
| More than three children | 27 | 2.5 | 7.4 | 29.6 | 22.2 | 40.7 | |
| Age group (years) (n = 1092) | |||||||
| 18–25 | 435 | 39.8 | 18.6 | 28.5 | 33.6 | 19.3 | p (<0.001) |
| 26–35 | 273 | 25.0 | 23.8 | 23.8 | 33.3 | 19.0 | |
| 36–45 | 157 | 14.4 | 29.3 | 21.0 | 27.4 | 22.3 | |
| 46–55 | 122 | 11.2 | 34.4 | 23.0 | 33.6 | 9.0 | |
| 56–65 | 66 | 6.0 | 40.9 | 25.8 | 27.3 | 6.1 | |
| 66-77 | 39 | 3.6 | 48.7 | 17.9 | 17.9 | 15.4 | |
| Household income (n = 1078) | |||||||
| EUR < 1250 | 229 | 21.2 | 25.8 | 22.7 | 31.9 | 19.7 | p (<0.058) |
| EUR 1250–1750 | 168 | 15.6 | 19.0 | 31.5 | 33.9 | 15.5 | |
| EUR 1750–2250 | 182 | 16.9 | 19.8 | 28.0 | 30.2 | 22.0 | |
| EUR 2250–3000 | 197 | 18.3 | 25.9 | 25.9 | 31.0 | 17.3 | |
| EUR 3000–4000 | 168 | 15.6 | 39.8 | 25.0 | 33.9 | 11.3 | |
| EUR 4000–5000 | 62 | 5.8 | 32.3 | 16.1 | 30.6 | 21.0 | |
| EUR ≥ 5000 | 72 | 6.7 | 40.3 | 15.3 | 29.2 | 15.3 | |
| Education (n = 1083) | |||||||
| Never completed school | 21 | 1.9 | 23.8 | 28.6 | 28.6 | 19.0 | p (<0.001) |
| Elementary school | 173 | 16.0 | 28.9 | 22.0 | 29.5 | 19.7 | |
| Secondary school | 352 | 32.5 | 23.0 | 26.1 | 31.8 | 19.0 | |
| Technical school diploma | 112 | 10.3 | 22.3 | 24.1 | 38.4 | 15.2 | |
| High-school diploma | 198 | 18.3 | 25.3 | 27.8 | 31.8 | 15.2 | |
| Some college or university of applied sciences degree | 83 | 7.7 | 28.9 | 22.9 | 32.5 | 15.7 | |
| Completed college or university of applied sciences degree | 122 | 11.3 | 31.1 | 26.2 | 29.5 | 13.1 | |
| Doctoral degree | 22 | 2.0 | 22.7 | 13.6 | 27.3 | 36.4 | |
| Marital status n = 1088 | |||||||
| Not married | 386 | 35.5 | 22.0 | 23.3 | 35.2 | 19.4 | p (<0.001) |
| Married | 338 | 31.1 | 36.1 | 24.0 | 27.2 | 12.7 | |
| Living with a partner in a steady relationship | 269 | 24.7 | 19.0 | 27.5 | 34.6 | 19.0 | |
| Widowed | 28 | 2.6 | 14.3 | 42.9 | 25.0 | 17.9 | |
| Divorced | 67 | 6.2 | 25.4 | 23.9 | 23.9 | 26.9 |
| N | % | Will Be Vaccinated Right Away (%) | Will Be Vaccinated after Consulting Doctor (%) | Will Wait and See How Others Tolerate the Vaccine (%) | Will Not Be Vaccinated at All | ||
|---|---|---|---|---|---|---|---|
| Higher risk perception of severe COVID-19 (n = 1073) | |||||||
| Yes | 250 | 23.3 | 36.0 | 30.4 | 25.2 | 8.4 | p(<0.052) |
| No | 700 | 65.2 | 23.6 | 22.6 | 34.3 | 19.6 | |
| Not sure | 123 | 11.5 | 17.1 | 29.3 | 30.1 | 23.6 | |
| Healthcare workers (n = 1068) | |||||||
| Yes | 222 | 20.8 | 22.1 | 31.5 | 32.9 | 13.5 | p (<0.040) |
| No | 846 | 79.2 | 26.8 | 23.6 | 31.3 | 18.2 | |
| Well-being health status (n = 1068) | |||||||
| Very good | 345 | 31.9 | 29.9 | 22.3 | 28.1 | 19.7 | p (<0.002) |
| Good | 450 | 41.6 | 24.7 | 26.0 | 34.7 | 14.7 | |
| Fair | 184 | 17.0 | 22.3 | 26.1 | 38.6 | 13.0 | |
| Poor | 63 | 5.8 | 17.5 | 31.7 | 23.8 | 27.0 | |
| Very poor | 41 | 3.8 | 29.3 | 24.4 | 12.2 | 34.1 | |
| Factor | Odds Ratio 1 | 95% CI | p-Value |
|---|---|---|---|
| Age (years) | 0.98 | 0.97–0.99 | <0.0001 |
| Female gender vs. male gender | 1.65 | 1.30–2.08 | <0.0001 |
| Neither female nor male gender vs. male gender | 1.59 | 0.68–3.74 | 0.29 |
| Number of children | 1.14 | 1.02–1.28 | 0.017 |
| Satisfaction with life (four-point Likert scale) 2 | 1.35 | 1.15–1.59 | 0.0002 |
| Satisfaction with democracy (four-point Likert scale) 2 | 2.63 | 2.28–3.04 | <0.0001 3 |
| Factor | Odds Ratio 1 | 95% CI | p-Value |
|---|---|---|---|
| Less importance of COVID-19 | 1.40 | 1.29–1.51 | <0.0001 |
| No vaccination against influenza | 1.99 | 1.80–2.19 | <0.0001 |
| Satisfaction with information 2 | 1.44 | 1.28–1.62 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fobiwe, J.P.; Martus, P.; Poole, B.D.; Jensen, J.L.; Joos, S. Influences on Attitudes Regarding COVID-19 Vaccination in Germany. Vaccines 2022, 10, 658. https://doi.org/10.3390/vaccines10050658
Fobiwe JP, Martus P, Poole BD, Jensen JL, Joos S. Influences on Attitudes Regarding COVID-19 Vaccination in Germany. Vaccines. 2022; 10(5):658. https://doi.org/10.3390/vaccines10050658
Chicago/Turabian StyleFobiwe, John Paul, Peter Martus, Brian D. Poole, Jamie L. Jensen, and Stefanie Joos. 2022. "Influences on Attitudes Regarding COVID-19 Vaccination in Germany" Vaccines 10, no. 5: 658. https://doi.org/10.3390/vaccines10050658
APA StyleFobiwe, J. P., Martus, P., Poole, B. D., Jensen, J. L., & Joos, S. (2022). Influences on Attitudes Regarding COVID-19 Vaccination in Germany. Vaccines, 10(5), 658. https://doi.org/10.3390/vaccines10050658