
Frequency and Nuisance Level of Adverse Events in Individuals Receiving Homologous and Heterologous COVID-19 Booster Vaccine

 ,
,  ,
,  ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
- Types, number, and frequency of different adverse events (local and systemic) following the administration of each dose of COVID-19 vaccine;
- Duration of adverse events after administration of each dose of COVID-19 vaccine;
- Level of the nuisance of adverse events (if present) following administration of each dose of COVID-19 vaccine (measured with a 10-point Likert-type scale, where 1—low level of nuisance, 10—very high level of a nuisance);
- Demographical factors differentiating the frequency of adverse events and their nuisance level after the administration of the homologous and heterologous booster;
- Frequency and types of pharmaceuticals self-administered by participants to counteract the adverse events;
- Willingness to receive the potential future doses of the COVID-19 if recommended by the health authorities.
2.2. Statistical Analysis
3. Results
3.1. Demographic Characteristics
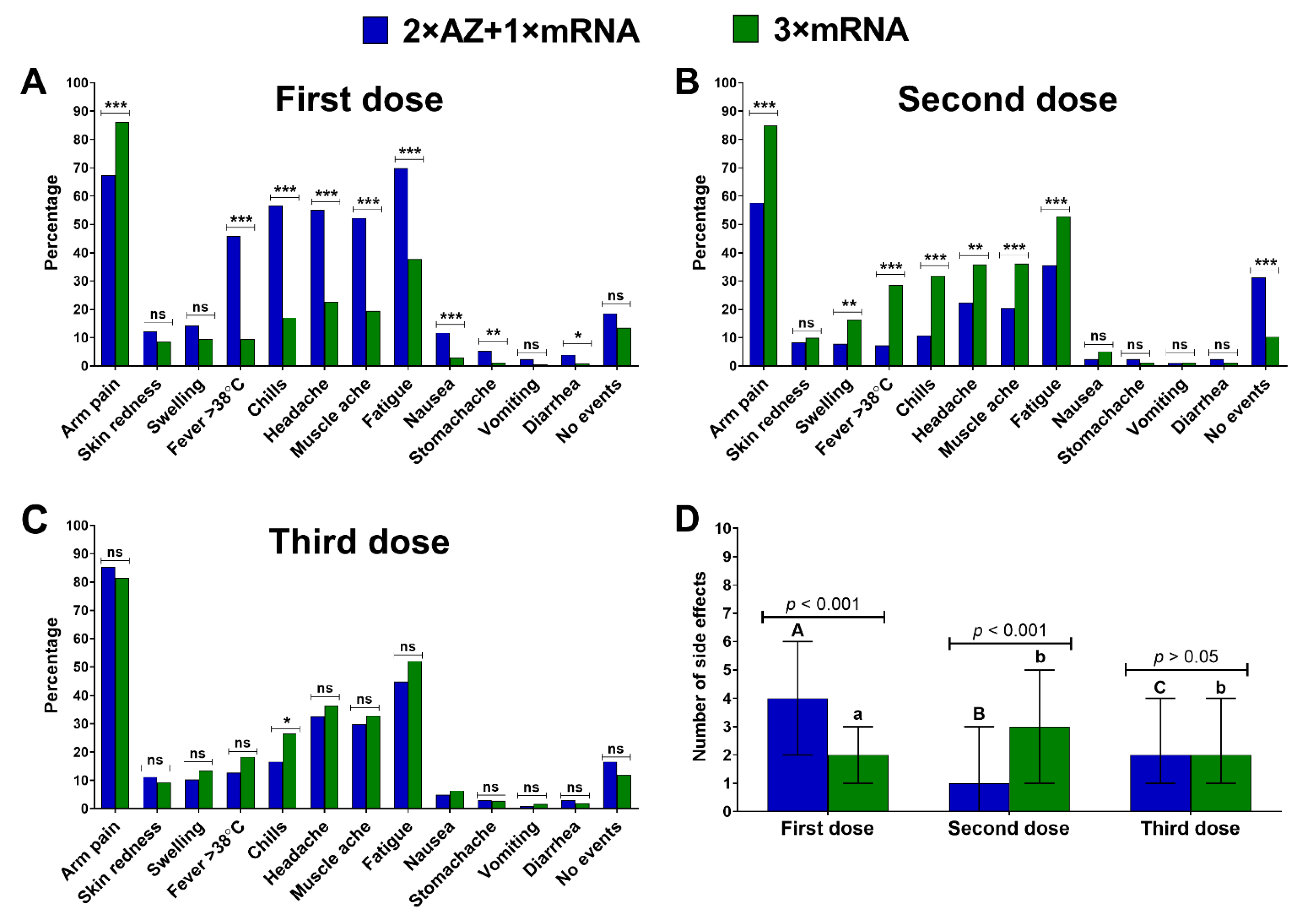
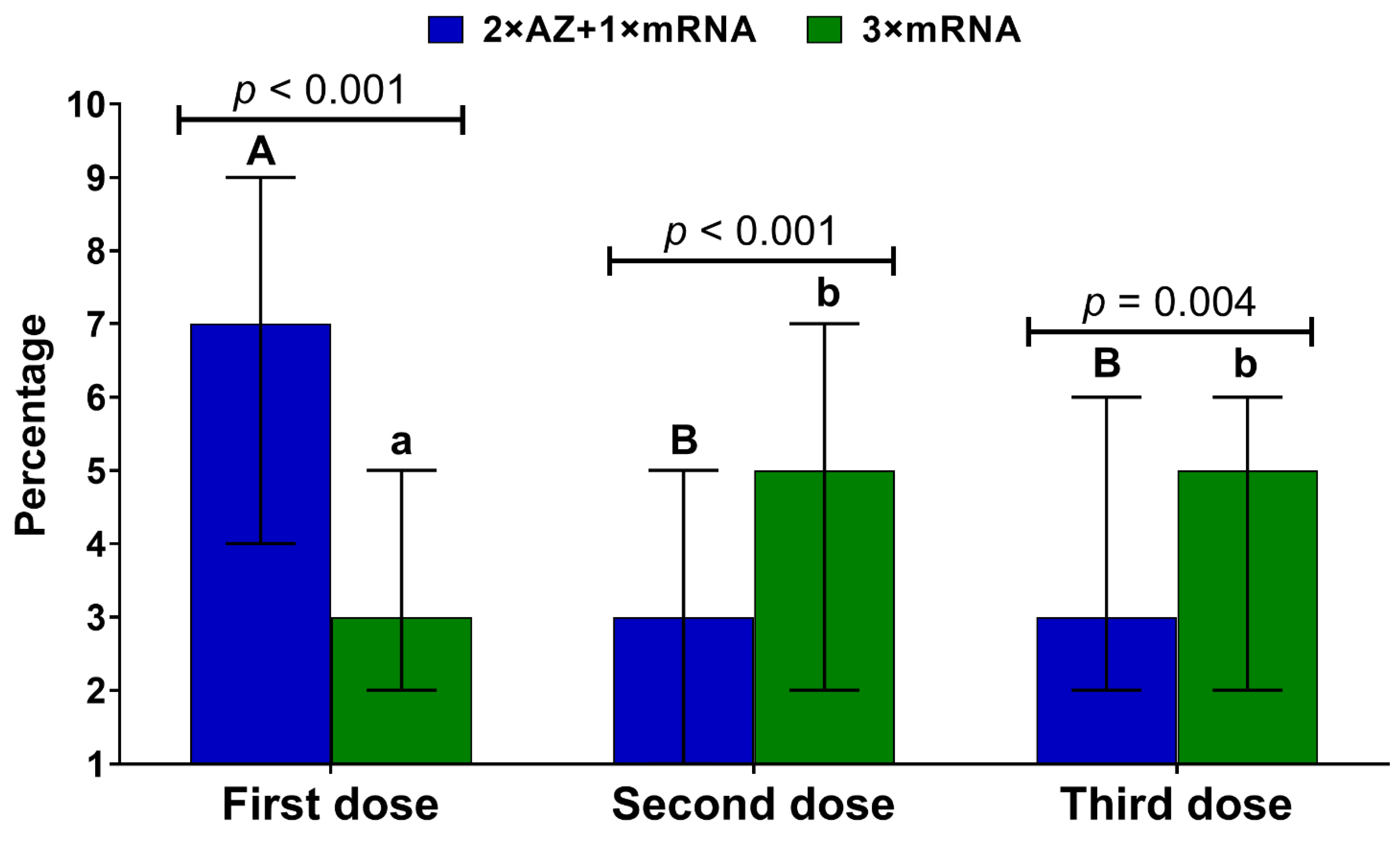
3.2. Occurrence of Vaccine Adverse Events
3.3. Level of Nuisance of Vaccine Adverse Events
3.4. Pharmaceuticals Used to Counteract Vaccine Adverse Events
3.5. Willingness to Receive Future COVID-19 Vaccine Doses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rzymski, P.; Camargo, C.A.; Fal, A.; Flisiak, R.; Gwenzi, W.; Kelishadi, R.; Leemans, A.; Nieto, J.J.; Ozen, A.; Perc, M.; et al. COVID-19 Vaccine Boosters: The Good, the Bad, and the Ugly. Vaccines 2021, 9, 1299. [Google Scholar] [CrossRef] [PubMed]
- Krause, P.R.; Fleming, T.R.; Peto, R.; Longini, I.M.; Figueroa, J.P.; Sterne, J.A.C.; Cravioto, A.; Rees, H.; Higgins, J.P.T.; Boutron, I.; et al. Considerations in Boosting COVID-19 Vaccine Immune Responses. Lancet 2021, 398, 1377–1380. [Google Scholar] [CrossRef]
- Sikora, D.; Rzymski, P. COVID-19 Vaccination and Rates of Infections, Hospitalizations, ICU Admissions, and Deaths in the European Economic Area during Autumn 2021 Wave of SARS-CoV-2. Vaccines 2022, 10, 437. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Beltran, W.F.; St Denis, K.J.; Hoelzemer, A.; Lam, E.C.; Nitido, A.D.; Sheehan, M.L.; Berrios, C.; Ofoman, O.; Chang, C.C.; Hauser, B.M.; et al. MRNA-Based COVID-19 Vaccine Boosters Induce Neutralizing Immunity against SARS-CoV-2 Omicron Variant. Cell 2022, 185, 457–466.e4. [Google Scholar] [CrossRef]
- Johnson, A.G.; Amin, A.B.; Ali, A.R.; Hoots, B.; Cadwell, B.L.; Arora, S.; Avoundjian, T.; Awofeso, A.O.; Barnes, J.; Bayoumi, N.S.; et al. COVID-19 Incidence and Death Rates among Unvaccinated and Fully Vaccinated Adults with and without Booster Doses during Periods of Delta and Omicron Variant Emergence—25 U.S. Jurisdictions, April 4–December 25, 2021. Morb. Mortal. Wkly. Rep. 2022, 71, 132–138. [Google Scholar] [CrossRef]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Sachdeva, R.; Gower, C.; Ramsay, M.; Bernal, J.L. Effectiveness of COVID-19 Booster Vaccines against COVID-19 Related Symptoms, Hospitalisation and Death in England. Nat. Med. 2022, 28, 831–837. [Google Scholar] [CrossRef]
- Rzymski, P.; Pazgan-Simon, M.; Kamerys, J.; Moniuszko-Malinowska, A.; Sikorska, K.; Wernik, J.; Zarębska-Michaluk, D.; Supronowicz, Ł.; Sobala-Szczygieł, B.; Skrzat-Klapaczyńska, A.; et al. Severe Breakthrough COVID-19 Cases during Six Months of Delta Variant (B.1.617.2) Domination in Poland. Vaccines 2022, 10, 557. [Google Scholar] [CrossRef]
- Mohamed, K.; Rzymski, P.; Islam, M.S.; Makuku, R.; Mushtaq, A.; Khan, A.; Ivanovska, M.; Makka, S.A.; Hashem, F.; Marquez, L.; et al. COVID-19 Vaccinations: The Unknowns, Challenges, and Hopes. J. Med. Virol. 2022, 94, 1336–1349. [Google Scholar] [CrossRef]
- WHO COVID-19 Vaccines. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/COVID-19-vaccines (accessed on 3 May 2022).
- Agenda, Policy & Strategy Interim Recommendations for Heterologous COVID-19 Vaccine Schedules. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-vaccines-SAGE-recommendation-heterologous-schedules (accessed on 1 April 2022).
- COVID-19 Vaccine Tracker. Available online: https://vaccinetracker.ecdc.europa.eu/public/extensions/COVID-19/vaccine-tracker.html (accessed on 31 January 2022).
- EMA COVID-19 Vaccine Janssen: EMA Recommendation on Booster Dose. Available online: https://www.ema.europa.eu/en/news/COVID-19-vaccine-janssen-ema-recommendation-booster-dose (accessed on 4 April 2022).
- Atmar, R.L.; Lyke, K.E.; Deming, M.E.; Jackson, L.A.; Branche, A.R.; El Sahly, H.M.; Rostad, C.A.; Martin, J.M.; Johnston, C.; Rupp, R.E.; et al. Homologous and Heterologous COVID-19 Booster Vaccinations. N. Engl. J. Med. 2022, 386, 1046–1057. [Google Scholar] [CrossRef]
- Costa Clemens, S.A.; Weckx, L.; Clemens, R.; Almeida Mendes, A.V.; Ramos Souza, A.; Silveira, M.B.V.; da Guarda, S.N.F.; de Nobrega, M.M.; de Moraes Pinto, M.I.; Gonzalez, I.G.S.; et al. Heterologous versus Homologous COVID-19 Booster Vaccination in Previous Recipients of Two Doses of CoronaVac COVID-19 Vaccine in Brazil (RHH-001): A Phase 4, Non-Inferiority, Single Blind, Randomised Study. Lancet 2022, 399, 521–529. [Google Scholar] [CrossRef]
- Mayr, F.B.; Talisa, V.B.; Shaikh, O.; Yende, S.; Butt, A.A. Effectiveness of Homologous or Heterologous COVID-19 Boosters in Veterans. N. Engl. J. Med. 2022, 386, 1375–1377. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.T.; Quach, T.H.T.; Tran, T.M.; Phuoc, H.N.; Nguyen, H.T.; Vo, T.K.; Van Vo, G. Reactogenicity and Immunogenicity of Heterologous Prime-Boost Immunization with COVID-19 Vaccine. Biomed. Pharmacother. 2022, 147, 112650. [Google Scholar] [CrossRef] [PubMed]
- Munro, A.P.S.; Janani, L.; Cornelius, V.; Aley, P.K.; Babbage, G.; Baxter, D.; Bula, M.; Cathie, K.; Chatterjee, K.; Dodd, K.; et al. Safety and Immunogenicity of Seven COVID-19 Vaccines as a Third Dose (Booster) Following Two Doses of ChAdOx1 NCov-19 or BNT162b2 in the UK (COV-BOOST): A Blinded, Multicentre, Randomised, Controlled, Phase 2 Trial. Lancet 2021, 398, 2258–2276. [Google Scholar] [CrossRef]
- Normark, J.; Vikström, L.; Gwon, Y.-D.; Persson, I.-L.; Edin, A.; Björsell, T.; Dernstedt, A.; Christ, W.; Tevell, S.; Evander, M.; et al. Heterologous ChAdOx1 NCoV-19 and MRNA-1273 Vaccination. N. Engl. J. Med. 2021, 385, 1049–1051. [Google Scholar] [CrossRef] [PubMed]
- Shaw, R.H.; Stuart, A.; Greenland, M.; Liu, X.; Nguyen Van-Tam, J.S.; Snape, M.D. Com-COV Study Group Heterologous Prime-Boost COVID-19 Vaccination: Initial Reactogenicity Data. Lancet 2021, 397, 2043–2046. [Google Scholar] [CrossRef]
- Powell, A.A.; Power, L.; Westrop, S.; McOwat, K.; Campbell, H.; Simmons, R.; Ramsay, M.E.; Brown, K.; Ladhani, S.N.; Amirthalingam, G. Real-World Data Shows Increased Reactogenicity in Adults after Heterologous Compared to Homologous Prime-Boost COVID-19 Vaccination, March-June 2021, England. Eurosurveillance 2021, 26, 2100634. [Google Scholar] [CrossRef]
- Grochowska, M.; Ratajczak, A.; Zdunek, G.; Adamiec, A.; Waszkiewicz, P.; Feleszko, W. A Comparison of the Level of Acceptance and Hesitancy towards the Influenza Vaccine and the Forthcoming COVID-19 Vaccine in the Medical Community. Vaccines 2021, 9, 475. [Google Scholar] [CrossRef]
- Rzymski, P.; Poniedziałek, B.; Fal, A. Willingness to Receive the Booster COVID-19 Vaccine Dose in Poland. Vaccines 2021, 9, 1286. [Google Scholar] [CrossRef]
- Rzymski, P.; Falfushynska, H.; Fal, A. Vaccination of Ukrainian Refugees: Need for Urgent Action. Clin. Infect. Dis. 2022. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 MRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the MRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Folegatti, P.M.; Ewer, K.J.; Aley, P.K.; Angus, B.; Becker, S.; Belij-Rammerstorfer, S.; Bellamy, D.; Bibi, S.; Bittaye, M.; Clutterbuck, E.A.; et al. Safety and Immunogenicity of the ChAdOx1 NCoV-19 Vaccine against SARS-CoV-2: A Preliminary Report of a Phase 1/2, Single-Blind, Randomised Controlled Trial. Lancet 2020, 396, 467–478. [Google Scholar] [CrossRef]
- Kremer, E.J. Pros and Cons of Adenovirus-Based SARS-CoV-2 Vaccines. Mol. Ther. 2020, 28, 2303–2304. [Google Scholar] [CrossRef] [PubMed]
- Falsey, A.R.; Sobieszczyk, M.E.; Hirsch, I.; Sproule, S.; Robb, M.L.; Corey, L.; Neuzil, K.M.; Hahn, W.; Hunt, J.; Mulligan, M.J.; et al. Phase 3 Safety and Efficacy of AZD1222 (ChAdOx1 NCoV-19) COVID-19 Vaccine. N. Engl. J. Med. 2021, 385, 2348–2360. [Google Scholar] [CrossRef]
- Stuart, A.S.V.; Shaw, R.H.; Liu, X.; Greenland, M.; Aley, P.K.; Andrews, N.J.; Cameron, J.C.; Charlton, S.; Clutterbuck, E.A.; Collins, A.M.; et al. Immunogenicity, Safety, and Reactogenicity of Heterologous COVID-19 Primary Vaccination Incorporating MRNA, Viral-Vector, and Protein-Adjuvant Vaccines in the UK (Com-COV2): A Single-Blind, Randomised, Phase 2, Non-Inferiority Trial. Lancet 2022, 399, 36–49. [Google Scholar] [CrossRef]
- Doedée, A.M.C.M.; Boland, G.J.; Pennings, J.L.A.; de Klerk, A.; Berbers, G.A.M.; van der Klis, F.R.M.; de Melker, H.E.; van Loveren, H.; Janssen, R. Effects of Prophylactic and Therapeutic Paracetamol Treatment during Vaccination on Hepatitis B Antibody Levels in Adults: Two Open-Label, Randomized Controlled Trials. PLoS ONE 2014, 9, e98175. [Google Scholar] [CrossRef] [Green Version]
- Coronavirus (COVID-19) Vaccines Side Effects and Safety. Available online: https://www.nhs.uk/conditions/coronavirus-COVID-19/coronavirus-vaccination/safety-and-side-effects/ (accessed on 4 April 2022).
- Bancos, S.; Bernard, M.P.; Topham, D.J.; Phipps, R.P. Ibuprofen and Other Widely Used Non-Steroidal Anti-Inflammatory Drugs Inhibit Antibody Production in Human Cells. Cell. Immunol. 2009, 258, 18–28. [Google Scholar] [CrossRef] [Green Version]
- Kazama, I.; Senzaki, M. Does Immunosuppressive Property of Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) Reduce COVID-19 Vaccine-Induced Systemic Side Effects? Drug Discov. Ther. 2021, 15, 278–280. [Google Scholar] [CrossRef]
- Haas, J.W.; Bender, F.L.; Ballou, S.; Kelley, J.M.; Wilhelm, M.; Miller, F.G.; Rief, W.; Kaptchuk, T.J. Frequency of Adverse Events in the Placebo Arms of COVID-19 Vaccine Trials: A Systematic Review and Meta-Analysis. JAMA Netw. Open 2022, 5, e2143955. [Google Scholar] [CrossRef]
- Amanzio, M.; Corazzini, L.L.; Vase, L.; Benedetti, F. A Systematic Review of Adverse Events in Placebo Groups of Anti-Migraine Clinical Trials. Pain 2009, 146, 261–269. [Google Scholar] [CrossRef]
- Ballou, S.; Iturrino, J.; Rangan, V.; Cheng, V.; Kelley, J.M.; Lembo, A.; Kaptchuk, T.J.; Nee, J. Improving Medication Tolerance: A Pilot Study in Disorders of Gut-Brain Interaction Treated with Tricyclic Antidepressants. J. Clin. Gastroenterol. 2021, 56, 452–456. [Google Scholar] [CrossRef] [PubMed]
- Rief, W. Fear of Adverse Effects and COVID-19 Vaccine Hesitancy: Recommendations of the Treatment Expectation Expert Group. JAMA Health Forum 2021, 2, e210804. [Google Scholar] [CrossRef]
- Schmid, P.; Rauber, D.; Betsch, C.; Lidolt, G.; Denker, M.-L. Barriers of Influenza Vaccination Intention and Behavior—A Systematic Review of Influenza Vaccine Hesitancy, 2005–2016. PLoS ONE 2017, 12, e0170550. [Google Scholar] [CrossRef]
- Rapport, F.; Hibbert, P.; Baysari, M.; Long, J.C.; Seah, R.; Zheng, W.Y.; Jones, C.; Preece, K.; Braithwaite, J. What Do Patients Really Want? An in-Depth Examination of Patient Experience in Four Australian Hospitals. BMC Health Serv. Res. 2019, 19, 38. [Google Scholar] [CrossRef] [Green Version]
- Biasio, L.R.; Corsello, G.; Costantino, C.; Fara, G.M.; Giammanco, G.; Signorelli, C.; Vecchio, D.; Vitale, F. Communication about Vaccination: A Shared Responsibility. Hum. Vaccines Immunother. 2016, 12, 2984–2987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, M.B.; Bor, A.; Jørgensen, F.; Lindholt, M.F. Transparent Communication about Negative Features of COVID-19 Vaccines Decreases Acceptance but Increases Trust. Proc. Natl. Acad. Sci. USA 2021, 118, e2024597118. [Google Scholar] [CrossRef]
- Rzymski, P.; Borkowski, L.; Drąg, M.; Flisiak, R.; Jemielity, J.; Krajewski, J.; Mastalerz-Migas, A.; Matyja, A.; Pyrć, K.; Simon, K.; et al. The Strategies to Support the COVID-19 Vaccination with Evidence-Based Communication and Tackling Misinformation. Vaccines 2021, 9, 109. [Google Scholar] [CrossRef]
- Stańczak-Mrozek, K.I.; Sobczak, A.; Lipiński, L.; Sienkiewicz, E.; Makarewicz, D.; Topór-Mądry, R.; Pinkas, J.; Sierpiński, R.A. The Potential Benefits of the Influenza Vaccination on COVID-19 Mortality Rate-A Retrospective Analysis of Patients in Poland. Vaccines 2021, 10, 5. [Google Scholar] [CrossRef]
- Taghioff, S.M.; Slavin, B.R.; Holton, T.; Singh, D. Examining the Potential Benefits of the Influenza Vaccine against SARS-CoV-2: A Retrospective Cohort Analysis of 74,754 Patients. PLoS ONE 2021, 16, e0255541. [Google Scholar] [CrossRef]
- Benn, C.S.; Netea, M.G.; Selin, L.K.; Aaby, P. A Small Jab—A Big Effect: Nonspecific Immunomodulation by Vaccines. Trends Immunol. 2013, 34, 431–439. [Google Scholar] [CrossRef]
- Netea, M.G.; Domínguez-Andrés, J.; Barreiro, L.B.; Chavakis, T.; Divangahi, M.; Fuchs, E.; Joosten, L.A.B.; van der Meer, J.W.M.; Mhlanga, M.M.; Mulder, W.J.M.; et al. Defining Trained Immunity and Its Role in Health and Disease. Nat. Rev. Immunol. 2020, 20, 375–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kovačić, D.; Gajić, A.A.; Latinović, D.; Softić, A. Hypothetical Immunological and Immunogenetic Model of Heterogenous Effects of BCG Vaccination in SARS-CoV-2 Infections: BCG-Induced Trained and Heterologous Immunity. J. Med. Sci. 2021, 90, e551. [Google Scholar] [CrossRef]
- Rubin, R. COVID-19 Vaccine Makers Plan for Annual Boosters, but It’s Not Clear They’ll Be Needed. JAMA 2021, 326, 2247–2249. [Google Scholar] [CrossRef] [PubMed]
- Zarębska-Michaluk, D.; Rzymski, P.; Moniuszko-Malinowska, A.; Brzdęk, M.; Martonik, D.; Rorat, M.; Wielgat, J.; Kłos, K.; Musierowicz, W.; Wasilewski, P.; et al. Does Hospitalization Change the Perception of COVID-19 Vaccines among Unvaccinated Patients? Vaccines 2022, 10, 476. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, H.; Mathieu, E.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Ortiz-Ospina, E.; Hasell, J.; Macdonald, B.; Beltekian, D.; Roser, M. Coronavirus Pandemic (COVID-19). Our World in Data. 2020. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 1 April 2022).



{kind=link}
{kind=link}
| Parameter | All (n = 457) | 2 × AZ + 1 × mRNA (n = 205) | 3 × mRNA (n = 252) | p-Value |
|---|---|---|---|---|
| Gender | 65.6 (300)/ | 66.3 (136)/ | 65.1 (164)/ | >0.05 |
| Women/men, % (n) | 34.4 (157) | 33.7 (69) | 34.9 (88) | |
| Age (years), mean ± SD | 35.8 ± 14.9 | 44.6 ± 12.4 | 28.7 ± 12.8 | <0.001 |
| (min–max) | (19–75) | (20–69) | (19–75) | |
| ≥50 years, % (n) | 22.5 (103) | 34.1 (70) | 13.1 (33) | <0.001 |
| BMI (kg/m2), mean ± SD | 24 ± 4.5 | 23 ± 4.3 | 24.8 ± 4.5 | <0.001 |
| (min–max) | (16.5–46.3) | (16.5–44.2) | (17.5–46.3) | |
| Underweight, % (n) | 6.6 (30) | 9.3 (19) | 4.4 (11) | 0.036 |
| Normal weight, % (n) | 58.4 (267) | 65.4 (134) | 52.8 (133) | 0.007 |
| Overweight, % (n) | 25.4 (116) | 19 (39) | 30.5 (77) | 0.005 |
| Obese, % (n) | 9.6 (44) | 6.3 (13) | 12.3 (31) | 0.032 |
| Influenza vaccination status | ||||
| Unvaccinated, % (n) | 57.5 (263) | 67.3 (138) | 49.6 (125) | <0.001 |
| Vaccinated for the first time in 2021 | 17.5 (80) | 10.3 (21) | 23.4 (59) | <0.001 |
| Vaccinated annually at least twice | 25 (114) | 22.4 (46) | 27 (68) | <0.001 |
| Parameter | Number of Side Effects after 3rd Dose | |
|---|---|---|
| 2 × AZ + 1 × mRNA | 3 × mRNA | |
| Number of side effects after 1st dose | 0.37 (***) | 0.37 (***) |
| Number of side effects after 2nd dose | 0.41 (***) | 0.55 (***) |
| Parameter | Vaccine Dose | Level of Nuisance after 3rd Dose | |
|---|---|---|---|
| 2 × AZ + 1 × mRNA | 3 × mRNA | ||
| Number of side effects | 1st dose | 0.37 (ns) | 0.18 (**) |
| 2nd dose | 0.07 (ns) | 0.41 (***) | |
| Level of nuisance of side effects | 1st dose | 0.22 (**) | 0.13 (ns) |
| 2nd dose | 0.32 (***) | 0.52 (***) | |
| Pharmaceutical | Vaccine Scheme | First Dose | p-Value | Second Dose | p-Value | Third Dose | p-Value |
|---|---|---|---|---|---|---|---|
| None, despite side effects | 2 × AZ + 1 × mRNA | 23.2 | 0.003 | 47.0 | >0.05 | 41.2 | >0.05 |
| 3 × mRNA | 53.2 | 38.0 | 40.7 | ||||
| Paracetamol | 2 × AZ + 1 × mRNA | 57.3 | <0.001 | 37.0 | <0.001 | 40.5 | >0.05 |
| 3 × mRNA | 32.9 | 42.7 | 38.1 | ||||
| Ibuprofen | 2 × AZ + 1 × mRNA | 11.9 | >0.05 | 10.0 | 13.7 | >0.05 | |
| 3 × mRNA | 10.8 | 16.2 | 18.0 | ||||
| Metamizole | 2 × AZ + 1 × mRNA | 4.9 | >0.05 | 3.0 | >0.05 | 2.3 | >0.05 |
| 3 × mRNA | 2.5 | 3.1 | 1.5 | ||||
| Acetylsalicylic acid | 2 × AZ + 1 × mRNA | 2.7 | >0.05 | 3.0 | >0.05 | 2.3 | >0.05 |
| 3 × mRNA | 0.6 | 0.0 | 1.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rzymski, P.; Sikora, D.; Zeyland, J.; Poniedziałek, B.; Kiedik, D.; Falfushynska, H.; Fal, A. Frequency and Nuisance Level of Adverse Events in Individuals Receiving Homologous and Heterologous COVID-19 Booster Vaccine. Vaccines 2022, 10, 754. https://doi.org/10.3390/vaccines10050754
Rzymski P, Sikora D, Zeyland J, Poniedziałek B, Kiedik D, Falfushynska H, Fal A. Frequency and Nuisance Level of Adverse Events in Individuals Receiving Homologous and Heterologous COVID-19 Booster Vaccine. Vaccines. 2022; 10(5):754. https://doi.org/10.3390/vaccines10050754
Chicago/Turabian StyleRzymski, Piotr, Dominika Sikora, Joanna Zeyland, Barbara Poniedziałek, Dorota Kiedik, Halina Falfushynska, and Andrzej Fal. 2022. "Frequency and Nuisance Level of Adverse Events in Individuals Receiving Homologous and Heterologous COVID-19 Booster Vaccine" Vaccines 10, no. 5: 754. https://doi.org/10.3390/vaccines10050754
APA StyleRzymski, P., Sikora, D., Zeyland, J., Poniedziałek, B., Kiedik, D., Falfushynska, H., & Fal, A. (2022). Frequency and Nuisance Level of Adverse Events in Individuals Receiving Homologous and Heterologous COVID-19 Booster Vaccine. Vaccines, 10(5), 754. https://doi.org/10.3390/vaccines10050754