
Significant Increase in Antibody Titers after the 3rd Booster Dose of the Pfizer–BioNTech mRNA COVID-19 Vaccine in Healthcare Workers in Greece




Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Haas, E.J.; Angulo, F.J.; McLaughlin, J.M.; Anis, E.; Singer, S.R.; Khan, F.; Brooks, N.; Smaja, M.; Mircus, G.; Pan, K.; et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: An observational study using national surveillance data. Lancet 2021, 397, 1819–1829. [Google Scholar] [CrossRef]
- Pritchard, E.; Matthews, P.C.; Stoesser, N.; Eyre, D.W.; Gethings, O.; Vihta, K.D.; Jones, J.; House, T.; VanSteenHouse, H.; Bell, I.; et al. Impact of vaccination on new SARS-CoV-2 infections in the United Kingdom. Nat. Med. 2021, 27, 1370–1378. [Google Scholar] [CrossRef] [PubMed]
- Singanayagam, A.; Hakki, S.; Dunning, J.; Madon, K.J.; Crone, M.A.; Koycheva, A.; Derqui-Fernandez, N.; Barnett, J.L.; Whitfield, M.G.; Varro, R.; et al. Community transmission and viral load kinetics of the SARS-CoV-2 delta (B.1.617.2) variant in vaccinated and unvaccinated individuals in the UK: A prospective, longitudinal, cohort study. Lancet Infect. Dis. 2022, 22, 183–195. [Google Scholar] [CrossRef]
- Tartof, S.Y.; Slezak, J.M.; Fischer, H.; Hong, V.; Ackerson, B.K.; Ranasinghe, O.N.; Frankland, T.B.; Ogun, O.A.; Zamparo, J.M.; Gray, S.; et al. Effectiveness of mRNA BNT162b2 COVID-19 vaccine up to 6 months in a large integrated health system in the USA: A retrospective cohort study. Lancet 2021, 398, 1407–1416. [Google Scholar] [CrossRef]
- Chemaitelly, H.; Tang, P.; Hasan, M.R.; AlMukdad, S.; Yassine, H.M.; Benslimane, F.M.; Al Khatib, H.A.; Coyle, P.; Ayoub, H.H.; Al Kanaani, Z.; et al. Waning of BNT162b2 Vaccine Protection against SARS-CoV-2 Infection in Qatar. N. Engl. J. Med. 2021, 385, e83. [Google Scholar] [CrossRef] [PubMed]
- Doria-Rose, N.; Suthar, M.S.; Makowski, M.; O’Connell, S.; McDermott, A.B.; Flach, B.; Ledgerwood, J.E.; Mascola, J.R.; Graham, B.S.; Lin, B.C.; et al. Antibody Persistence through 6 Months after the Second Dose of mRNA-1273 Vaccine for Covid-19. N. Engl. J. Med. 2021, 384, 2259–2261. [Google Scholar] [CrossRef]
- Ducloux, D.; Colladant, M.; Chabannes, M.; Yannaraki, M.; Courivaud, C. Humoral response after 3 doses of the BNT162b2 mRNA COVID-19 vaccine in patients on hemodialysis. Kidney Int. 2021, 100, 702–704. [Google Scholar] [CrossRef]
- Wu, K.; Choi, A.; Koch, M.; Ma, L.; Hill, A.; Nunna, N.; Huang, W.; Oestreicher, J.; Colpitts, T.; Bennett, H.; et al. Preliminary Analysis of Safety and Immunogenicity of a SARS-CoV-2 Variant Vaccine Booster. medRxiv 2021. [Google Scholar] [CrossRef]
- Kontopoulou, K.; Ainatzoglou, A.; Ifantidou, A.; Nakas, C.T.; Gkounti, G.; Adamopoulos, V.; Papadopoulos, N.; Papazisis, G. Immunogenicity after the first dose of the BNT162b2 mRNA Covid-19 vaccine: Real-world evidence from Greek healthcare workers. J. Med. Microbiol. 2021, 70, 001387. [Google Scholar] [CrossRef]
- Kontopoulou, K.; Ainatzoglou, A.; Nakas, C.T.; Ifantidou, A.; Goudi, G.; Antoniadou, E.; Adamopoulos, V.; Papadopoulos, N.; Papazisis, G. Second dose of the BNT162b2 mRNA vaccine: Value of timely administration but questionable necessity among the seropositive. Vaccine 2021, 39, 5078–5081. [Google Scholar] [CrossRef]
- Kontopoulou, K.; Nakas, C.; Ntenti, C.; Katsioulis, C.; Goulas, A.; Papazisis, G. Antibody Titers 3-Months Post-Vaccination with the Pfizer/Biontech Vaccine in Greece. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3899094 (accessed on 4 August 2021).
- Kontopoulou, K.; Nakas, C.; Ainatzoglou, A.; Goudi, G.; Katsioulis, C.; Papazisis, G. Evolution of Antibody Titers Up to 6 Months Post-Immunization with the BNT162b2 Pfizer/BioNTech Vaccine in Greece. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3922311 (accessed on 12 September 2021).
- SARS-CoV-2 Immunoassay. Abbott Core Laboratory (Internet). 2021. Available online: https://www.corelaboratory.abbott/int/en/offerings/segments/infectious-disease/sars-cov-2- (accessed on 21 February 2021).
- Butch, A.W. Dilution protocols for detection of hook effects/prozone phenomenon. Clin. Chem. 2000, 46, 1719–1721. [Google Scholar] [CrossRef] [Green Version]
- AllplexTM. 2019-nCoV-2 Master Assay (Cat. No. RV10284X). Available online: https://www.fda.gov/media/137178/download (accessed on 20 January 2021).
- Terpos, E.; Karalis, V.; Sklirou, A.D.; Apostolakou, F.; Ntanasis-Stathopoulos, I.; Bagratuni, T.; Iconomidou, V.A.; Malandrakis, P.; Korompoki, E.; Papassotiriou, I.; et al. Third dose of the BNT162b2 vaccine results in very high levels of neutralizing antibodies against SARS-CoV-2: Results of a prospective study in 150 health professionals in Greece. Am. J. Hematol. 2022, 97, E147–E150. [Google Scholar] [CrossRef] [PubMed]
- Terpos, E.; Trougakos, I.P.; Apostolakou, F.; Charitaki, I.; Sklirou, A.D.; Mavrianou, N.; Papanagnou, E.D.; Liacos, C.I.; Gumeni, S.; Rentziou, G.; et al. Age-dependent and gender-dependent antibody responses against SARS-CoV-2 in health workers and octogenarians after vaccination with the BNT162b2 mRNA vaccine. Am. J. Hematol. 2021, 96, E257–E259. [Google Scholar] [CrossRef] [PubMed]
- Falsey, A.R.; Frenck, R.W., Jr.; Walsh, E.E.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Bailey, R.; Swanson, K.A.; Xu, X.; et al. SARS-CoV-2 Neutralization with BNT162b2 Vaccine Dose 3. N. Engl. J. Med. 2021, 385, 1627–1629. [Google Scholar] [CrossRef]
- Lau, C.S.; Phua, S.K.; Liang, Y.L.; Oh, M.L.; Aw, T.C. SARS-CoV-2 Spike and Neutralizing Antibody Kinetics 90 Days after Three Doses of BNT162b2 mRNA COVID-19 Vaccine in Singapore. Vaccines 2022, 10, 331. [Google Scholar] [CrossRef]
- Barda, N.; Dagan, N.; Cohen, C.; Hernán, M.A.; Lipsitch, M.; Kohane, I.S.; Reis, B.Y.; Balicer, R.D. Effectiveness of a third dose of the BNT162b2 mRNA COVID-19 vaccine for preventing severe outcomes in Israel: An observational study. Lancet 2021, 398, 2093–2100. [Google Scholar] [CrossRef]
- Saciuk, Y.; Kertes, J.; Stein, N.S.; Zohar, A.E. Effectiveness of a Third Dose of BNT162b2 mRNA Vaccine. J. Infect. Dis. 2022, 225, 30–33. [Google Scholar] [CrossRef]
- Ai, J.; Zhang, H.; Zhang, Y.; Lin, K.; Zhang, Y.; Wu, J.; Wan, Y.; Huang, Y.; Song, J.; Fu, Z.; et al. Omicron variant showed lower neutralizing sensitivity than other SARS-CoV-2 variants to immune sera elicited by vaccines after boost. Emerg. Microbes Infect. 2022, 11, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Beltran, W.F.; Denis, K.J.; Hoelzemer, A.; Lam, E.C.; Nitido, A.D.; Sheehan, M.L.; Berrios, C.; Ofoman, O.; Chang, C.C.; Hauser, B.M.; et al. mRNA-based COVID-19 vaccine boosters induce neutralizing immunity against SARS-CoV-2 Omicron variant. Cell 2022, 185, 457–466.e4. [Google Scholar] [CrossRef]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R.; et al. Protection of BNT162b2 Vaccine Booster against Covid-19 in Israel. N. Engl. J. Med. 2021, 385, 1393–1400. [Google Scholar] [CrossRef]
- Patalon, T.; Gazit, S.; Pitzer, V.E.; Prunas, O.; Warren, J.L.; Weinberger, D.M. Short term reduction in the odds of testing positive for SARS-CoV-2; A comparison between two doses and three doses of the BNT162b2 vaccine. medRxiv 2021. [Google Scholar] [CrossRef]
- Thompson, M.G.; Natarajan, K.; Irving, S.A.; Rowley, E.A.; Griggs, E.P.; Gaglani, M.; Klein, N.P.; Grannis, S.J.; DeSilva, M.B.; Stenehjem, E.; et al. Effectiveness of a Third Dose of mRNA Vaccines Against COVID-19–Associated Emergency Department and Urgent Care Encounters and Hospitalizations Among Adults During Periods of Delta and Omicron Variant Predominance—VISION Network, 10 States, August 2021–January 2022. MMWR Morb. Mortal. Wkly. Rep. 2021, 71, 1291–1293. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| N | 9 Months GMC (95% CI) | 9 Months Relative to 6 Months GMC Fold Change (95% CI) | 3rd Dose GMC (95% CI) | 3rd Dose Relative to 6 Months GMC Fold Change | 3rd Dose Relative to 9 Months GMC Fold Change | ||
|---|---|---|---|---|---|---|---|
| 129 | 437.47 (383.34, 499.24) | 0.489 (0.447, 0.535) | 20,231.52 (18,062.02, 22,661.60) | 22.84 (19.77, 26.39) | 46.30 (41.09, 52.17) | ||
| SEX | Male | 50 | 464.14 (367.45, 586.26) | 0.452 (0.365, 0.558) | 20,429.62 (17,014.89, 24,529.66) | 20.16 (14.63, 27.79) | 44.02 (35.81, 54.10) |
| Female | 79 | 421.39 (358.81, 494.88) | 0.508 (0.464, 0.556) | 20,107.13 (17,344.50, 23,309.79) | 24.24 (20.80, 28.26) | 47.81 (41.23, 55.43) | |
| p-value | 0.429 | 0.893 | |||||
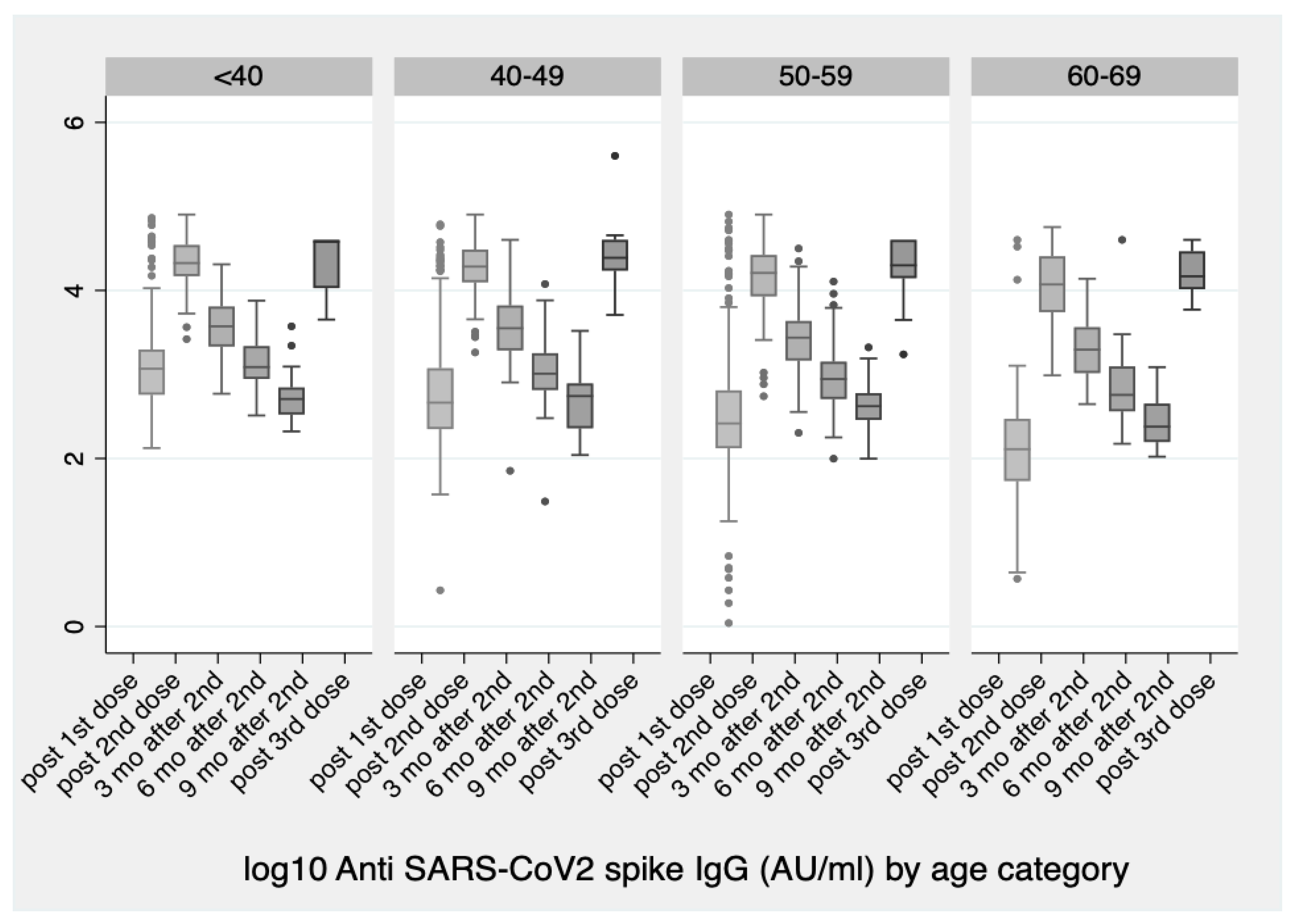
| AGE | <40 | 19 | 567.45 (395.85, 813.45) | 0.452 (0.386, 0.529) | 22,145.50 (15,643.38, 31,350.21) | 23.46 (16.47, 33.42) | 39.03 (26.28, 57.95) |
| 40– | 38 | 537.71 (407.08, 710.26) | 0.458 (0.395, 0.531) | 22,948.09 (18,909.49, 27,849.23) | 19.59 (14.87, 25.81) | 42.84 (33.26, 55.19) | |
| 50– | 53 | 413.07 (346.50, 492.44) | 0.563 (0.476, 0.665) | 19,131.27 (15,858.29, 23,079.75) | 24.83 (19.81, 31.12) | 46.31 (39.12, 54.83) | |
| 60– | 19 | 261.98 (190.83, 359.66) | 0.420 (0.328, 0.539) | 16791.01 (12,599.75, 22,376.47) | 26.20 (16.95, 40.49) | 64.09 (51.40, 79.91) | |
| p-value | 0.002 | 0.294 | |||||
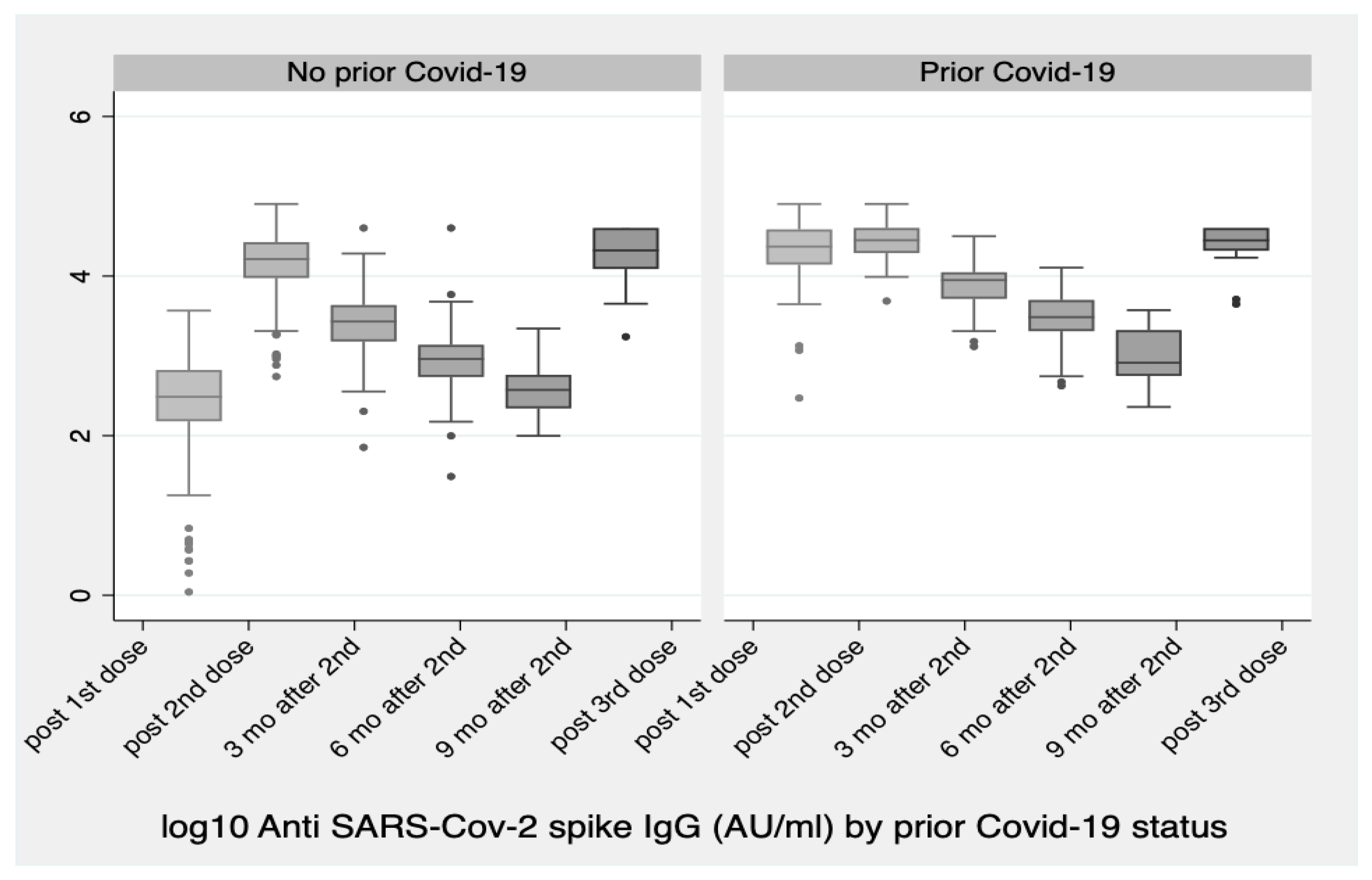
| prior COVID status | NO | 110 | 380.49 (335.82, 431.10) | 0.503 (0.457, 0.554) | 19556.40 (17,304.41, 22,101.46) | 26.22 (23.22, 29.62) | 51.47 (46.14, 57.41) |
| YES | 19 | 981.29 (668.44, 1440.58) | 0.415 (0.314, 0.548) | 24624.25 (17,959.36, 33,762.55) | 10.25 (5.75, 18.26) | 25.09 (16.09, 39.13) | |
| p-value | <0.001 | 0.155 |
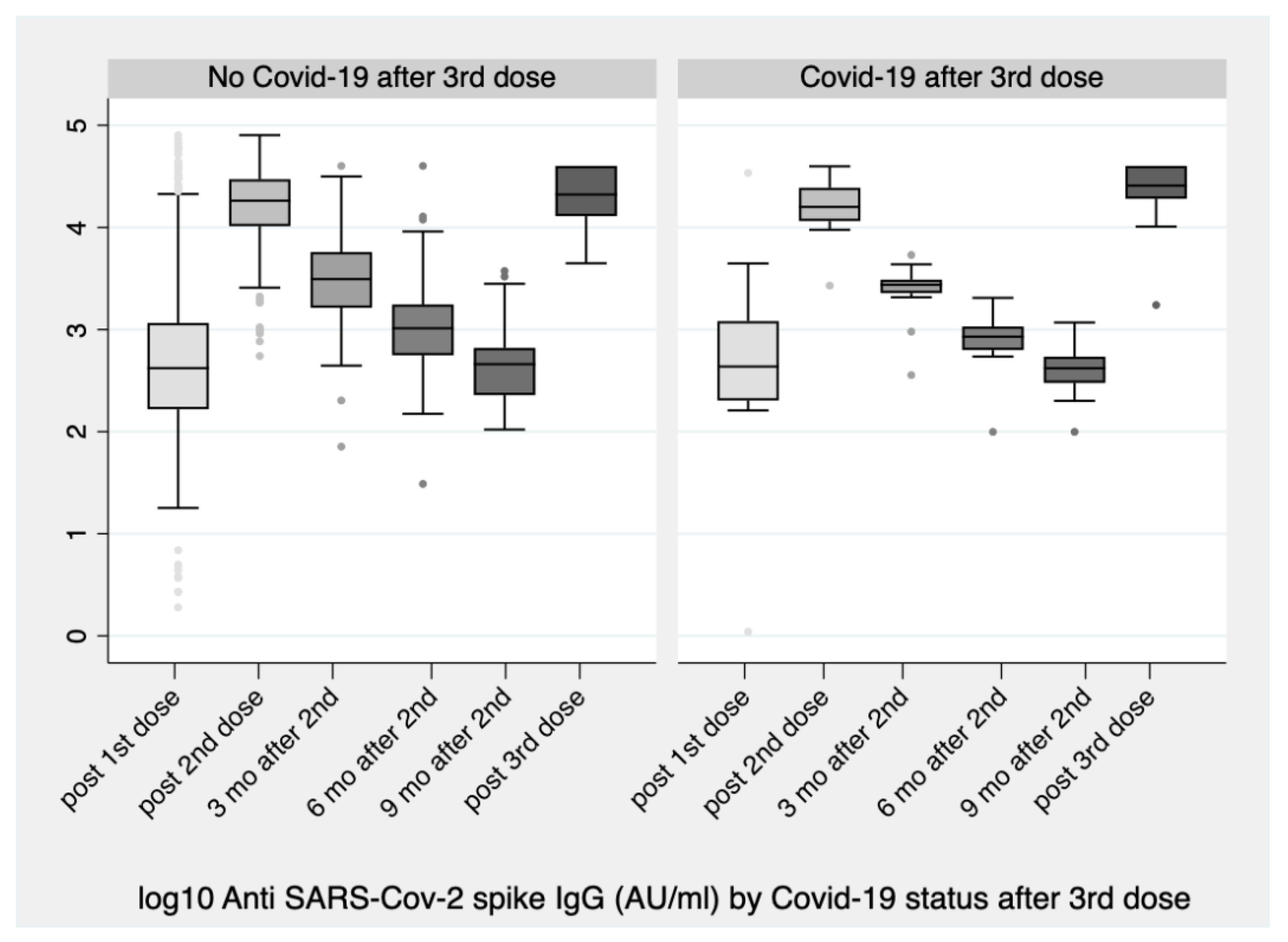
| COVID after 3rd Dose | N | After 1st Dose | After 2nd Dose | 3 mo after 2nd | 6 mo after 2nd | 9 mo after 2nd | After 3rd Dose | |
|---|---|---|---|---|---|---|---|---|
| GMC | N | 111 | 460.57 (318.73, 665.53) | 15,585.5 (13,349.04, 18,196.66) | 2945.32 (2467.74, 3515.33) | 890.06 (740.40, 1069.96) | 445.85 (384.56, 516.90) | 19871.33 (17,655.59, 22,365.14) |
| Y | 18 | 464.96 (168.03, 1286.57) | 16,433.37 (11,997.75, 22,508.85) | 2408.92 (1722.07, 3369.72) | 783.01 (549.53, 1115.67) | 389.15 (294.80, 513.70) | 22,601.53 (15,275.04, 33,442.08) | |
| p-value | 0.985 | 0.793 | 0.382 | 0.573 | 0.482 | 0.439 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kontopoulou, K.; Nakas, C.T.; Papazisis, G. Significant Increase in Antibody Titers after the 3rd Booster Dose of the Pfizer–BioNTech mRNA COVID-19 Vaccine in Healthcare Workers in Greece. Vaccines 2022, 10, 876. https://doi.org/10.3390/vaccines10060876
Kontopoulou K, Nakas CT, Papazisis G. Significant Increase in Antibody Titers after the 3rd Booster Dose of the Pfizer–BioNTech mRNA COVID-19 Vaccine in Healthcare Workers in Greece. Vaccines. 2022; 10(6):876. https://doi.org/10.3390/vaccines10060876
Chicago/Turabian StyleKontopoulou, Konstantina, Christos T. Nakas, and Georgios Papazisis. 2022. "Significant Increase in Antibody Titers after the 3rd Booster Dose of the Pfizer–BioNTech mRNA COVID-19 Vaccine in Healthcare Workers in Greece" Vaccines 10, no. 6: 876. https://doi.org/10.3390/vaccines10060876
APA StyleKontopoulou, K., Nakas, C. T., & Papazisis, G. (2022). Significant Increase in Antibody Titers after the 3rd Booster Dose of the Pfizer–BioNTech mRNA COVID-19 Vaccine in Healthcare Workers in Greece. Vaccines, 10(6), 876. https://doi.org/10.3390/vaccines10060876