
COVID-19 Vaccination in China: Adverse Effects and Its Impact on Health Care Working Decisions on Booster Dose

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Questionnaires
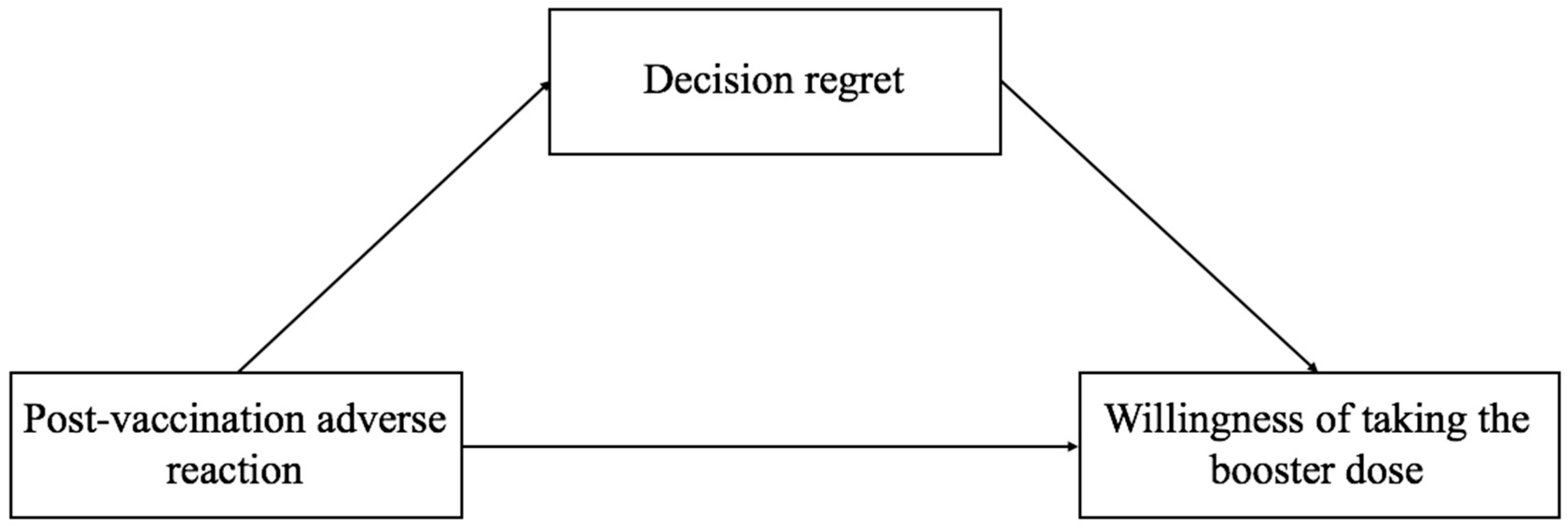
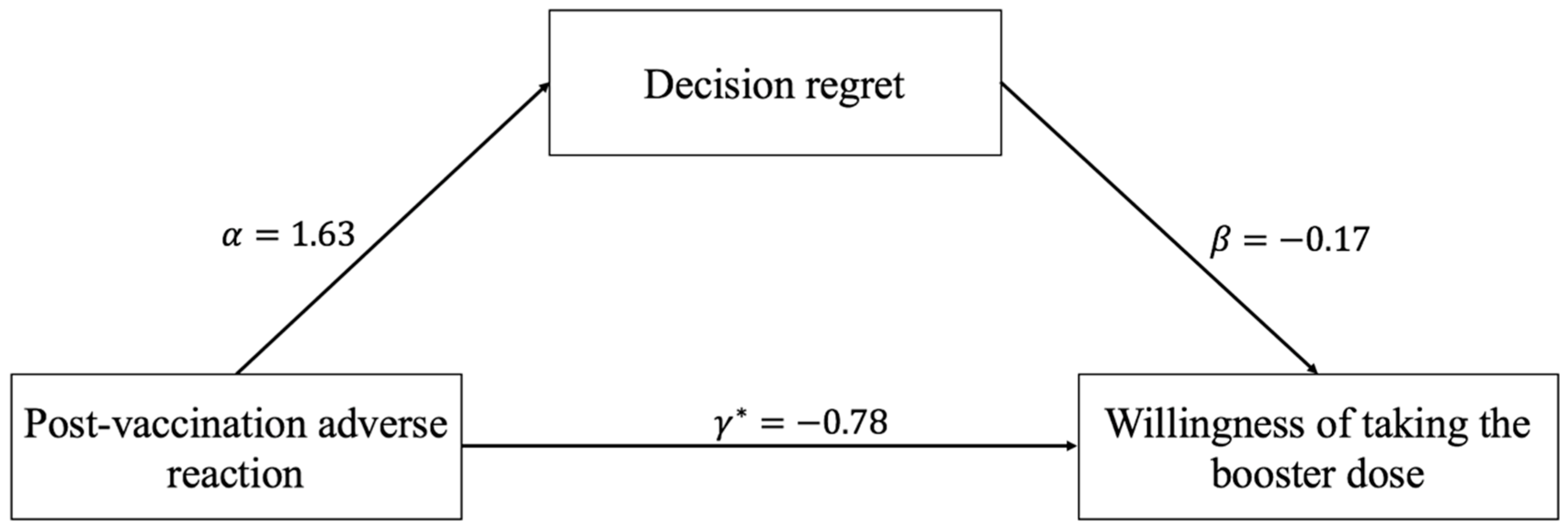
2.3. Mediation Analysis
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Participants
3.2. Correlations between the Main Study Variables
3.3. Testing for the Mediation Model
4. Discussion
4.1. Clinical Implications
4.2. Methodological Consideration
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- Harapan, H.; Itoh, N.; Yufika, A.; Winardi, W.; Keamg, S.; Te, H.; Megawati, D.; Hayati, Z.; Wagner, A.L.; Mudatsir, M. Coronavirus disease 2019 (COVID-19): A literature review. J. Infect. Public Health 2020, 13, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Wiersinga, W.; Rhodes, A.; Cheng, A.; Peacock, S.; Prescott, H. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): A review. J. Am. Med. Assoc. 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Polack, F.; Thomas, S.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Palacios, R.; Patiño, E.; de Oliveira, P.; Conde, M.; Batista, A.; Zeng, G.; Xin, Q.; Kallas, E.G.; Flores, J.; Ockenhouse, C.F.; et al. Double-blind, randomized, placebo-controlled phase III clinical trial to evaluate the efficacy and safety of treating healthcare professionals with the adsorbed COVID-19 (inactivated) vaccine manufactured by Sinovac—PROFISCOV: A structured summary of a study protocol for a randomised controlled trial. Trials 2020, 21, 853. [Google Scholar]
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Levin, E.G.; Rubin, C.; Indenbaum, V.; et al. COVID-19 breakthrough infections in vaccinated health care workers. N. Engl. J. Med. 2021, 385, 1474–1484. [Google Scholar] [CrossRef]
- Naaber, P.; Tserel, L.; Kangro, K.; Sepp, E.; Jürjenson, V.; Adamson, A.; Haljasmägi, L.; Rumm, A.P.; Maruste, R.; Kärner, J.; et al. Dynamics of antibody response to BNT162b2 vaccine after six months: A longitudinal prospective study. Lancet Reg. Health-Eur. 2021, 10, 100208. [Google Scholar] [CrossRef]
- Sabetian, G.; Moghadami, M.; Hashemizadeh Fard Haghighi, L.; Shahriarirad, R.; Fallahi, M.; Asmarian, N.; Moeini, Y.S. COVID-19 infection among healthcare workers: A cross-sectional study in southwest Iran. Virol. J. 2021, 18, 58. [Google Scholar] [CrossRef]
- Zheng, L.; Wang, X.; Zhou, C.; Liu, Q.; Li, S.; Sun, Q.; Wang, M.; Zhou, Q.; Wang, W. Analysis of the infection status of healthcare workers in Wuhan during the COVID-19 outbreak: A cross-sectional study. Clin. Infect. Dis. 2020, 71, 2109–2113. [Google Scholar] [CrossRef]
- Maruyama, A.; Sawa, T.; Teramukai, S.; Katoh, N. Adverse reactions to the first and second doses of Pfizer-BioNTech COVID-19 vaccine among healthcare workers. J. Infect. Chemother. 2022, 28, 934–942. [Google Scholar] [CrossRef] [PubMed]
- Kałucka, S.; Kusideł, E.; Głowacka, A.; Oczoś, P.; Grzegorczyk-Karolak, I. Pre-vaccination stress, post-vaccination adverse reactions, and attitudes towards vaccination after receiving the COVID-19 vaccine among health care workers. Vaccines 2022, 10, 401. [Google Scholar] [CrossRef] [PubMed]
- Becerra Pérez, M.; Menear, M.; Brehaut, J.; Légaré, F. Extent and predictors of decision regret about health care decisions: A systematic review. Med. Decis. Mak. 2016, 36, 777–790. [Google Scholar] [CrossRef] [PubMed]
- Haun, M.; Schakowski, A.; Preibsch, A.; Friederich, H.; Hartmann, M. Assessing decision regret in caregivers of deceased German people with cancer-A psychometric validation of the decision regret scale for caregivers. Health Expect. 2019, 22, 1089–1099. [Google Scholar] [CrossRef] [Green Version]
- Judd, C.; Kenny, D. Process analysis: Estimating mediation in treatment evaluations. Eval. Rev. 1981, 5, 602–619. [Google Scholar] [CrossRef]
- Sobel, M.E. Asymptotic confidence intervals for indirect effects in structural equation models. Sociol. Methodol. 1982, 13, 290–312. [Google Scholar] [CrossRef]
- Baron, R.; Kenny, D. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic and statistical considerations. J. Personal. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- MacKinnon, D.; Fairchild, A.; Fritz, M. Mediation analysis. Annu. Rev. Psychol. 2007, 58, 593–614. [Google Scholar] [CrossRef]
- Preacher, K.; Hayes, A. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef]
- MacKinnon, D.; Lockwood, C.; Hoffman, J.; West, S.; Sheets, V. A comparison of methods to test mediation and other intervening variable effects. Psychol. Methods 2002, 7, 83–104. [Google Scholar] [CrossRef]
- Voysey, M.; Costa Clemens, S.; Madhi, S.; Weckx, L.; Folegatti, P.; Aley, P.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Single-dose administration and the influence of the timing of the booster dose on immunogenicity and efficacy of ChAdOx1 nCoV-19 (AZD1222) vaccine: A pooled analysis of four randomised trials. Lancet 2021, 397, 881–891. [Google Scholar] [CrossRef]
- Ramasamy, M.; Minassian, A.; Ewer, K.; Flaxman, A.; Folegatti, P.; Owens, D.; Voysey, M.; Aley, P.K.; Angus, B.; Babbage, G.; et al. Safety and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): A single-blind, randomised, controlled, phase 2/3 trial. Lancet 2021, 396, 1979–1993. [Google Scholar] [CrossRef]
- Yigit, M.; Ozkaya-Parlakay, A.; Cosgun, Y.; Ince, Y.; Bulut, Y.; Senel, E. Should a third booster dose be scheduled after two doses of CoronaVac? A single-center experience. J. Med. Virol. 2022, 94, 287–290. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M. COVID-19 vaccine hesitancy worldwide: A concise systematic review of vaccine acceptance rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Toro-Ascuy, D.; Cifuentes-Muñoz, N.; Avaria, A.; Pereira-Montecinos, C.; Cruzat, G.; Peralta-Arancibia, K.; Zorondo-Rodríguez, F.; Fuenzalida, L.F. Factors influencing the acceptance of COVID-19 vaccines in a country with a high vaccination rate. Vaccines 2022, 10, 681. [Google Scholar] [CrossRef]
- Koh, S.W.C.; Tan, H.M.; Lee, W.H.; Mathews, J.; Young, D. COVID-19 vaccine booster hesitancy among healthcare workers: A retrospective observational study in Singapore. Vaccines 2022, 10, 464. [Google Scholar] [CrossRef]
- Chu, Y.K.; Chung, P.H.; Pang, F.C. Analysis of the effectiveness of measures on the COVID-19 vaccination rate in Hong Kong. Vaccines 2022, 10, 747. [Google Scholar] [CrossRef]
- Trepanowski, R.; Drążkowski, D. Cross-national comparison of religion as a predictor of COVID-19 vaccination rates. J. Relig. Health 2022, 61, 2198–2211. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Category | Sample | |
|---|---|---|---|
| Number | Percentage (%) | ||
| Post-vaccination adverse reaction | No | 931 | 88.3 |
| Yes | 123 | 11.7 | |
| Age (years) | <30 | 363 | 34.4 |
| 30~39 | 466 | 44.2 | |
| 40~49 | 183 | 17.4 | |
| ≥50 | 42 | 4.0 | |
| Sex | Male | 165 | 15.7 |
| Female | 889 | 84.3 | |
| Education | Senior Secondary and below | 71 | 6.7 |
| Junior college | 162 | 15.4 | |
| Undergraduate | 709 | 67.3 | |
| Graduate | 112 | 10.6 | |
| Occupation | Doctor | 174 | 16.5 |
| Nurse | 670 | 63.6 | |
| Medical Technician | 127 | 12.0 | |
| Others | 83 | 7.9 | |
| Professional titles | Internship | 18 | 1.7 |
| Primary grade | 447 | 42.4 | |
| Medium grade | 359 | 34.1 | |
| Associate professor | 86 | 8.1 | |
| Professor | 47 | 4.5 | |
| Others | 97 | 9.2 | |
| Underlying disease | Yes | 121 | 11.5 |
| No | 933 | 88.5 | |
| Variables | Category | n | % | p-Value | |
|---|---|---|---|---|---|
| Total | 1054 | 87.0 | |||
| Post-vaccination adverse reaction | 22.192 | <0.001 | |||
| No | 931 | 88.8 | |||
| Yes | 123 | 73.2 | |||
| Age(years) | 2.542 | 0.468 | |||
| <30 | 363 | 86.8 | |||
| 30~39 | 466 | 85.8 | |||
| 40~49 | 183 | 89.1 | |||
| ≥50 | 42 | 92.9 | |||
| Sex | 0.241 | 0.624 | |||
| Male | 165 | 88.5 | |||
| Female | 889 | 86.7 | |||
| Education | 3.315 | 0.346 | |||
| Senior Secondary and below | 71 | 87.3 | |||
| Junior college | 162 | 91.4 | |||
| Undergraduate | 709 | 86.2 | |||
| Graduate | 112 | 85.7 | |||
| Occupation | 6.448 | 0.092 | |||
| Doctor | 174 | 83.3 | |||
| Nurse | 670 | 86.6 | |||
| Medical Technician | 127 | 92.3 | |||
| Others | 83 | 89.2 | |||
| Professional titles | 2.316 | 0.678 | |||
| Primary grade and below | 465 | 86.7 | |||
| Medium grade | 359 | 86.1 | |||
| Associate professor | 86 | 88.4 | |||
| Professor | 47 | 93.6 | |||
| Others | 97 | 87.6 | |||
| Underlying disease | 3.787 | 0.052 | |||
| Yes | 121 | 81.0 | |||
| No | 933 | 87.8 | |||
| Variables | Descriptive | 1 | 2 | 3 |
|---|---|---|---|---|
| 1. Post-vaccination adverse reaction (Yes) | 123 (11.7%) | 1.00 | ||
| 2. Decision regret | 8.6 (±3.5) | 0.14 *** | 1.00 | |
| 3. Willingness to take the booster dose (Yes) | 917 (87.0%) | −0.15 *** | −0.22 *** | 1.00 |
| Variable | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|
| OR | 95%CI | B | 95%CI | OR | 95%CI | |
| Independent variable | ||||||
| Post-vaccination adverse reaction (No) | ||||||
| Yes | 0.37 *** | 0.23~0.59 | 1.63 *** | 0.98~2.28 | 0.46 ** | 0.29~0.74 |
| Mediator | ||||||
| Decision regret | 0.84 *** | 0.80~0.89 | ||||
| Controlled variable | ||||||
| Age (<30) | ||||||
| 30~39 | 1.18 | 0.76~1.84 | −0.30 | −0.82~0.21 | 1.14 | 0.72~1.80 |
| 40~49 | 1.54 | 0.83~2.95 | −0.58 | −1.26~0.10 | 1.44 | 0.75~2.82 |
| ≥50 | 2.75 | 0.86~12.46 | −0.20 | −1.36~0.95 | 2.64 | 0.83~11.85 |
| Sex (Male) | ||||||
| Female | 0.75 | 0.37~1.48 | 0.18 | −0.55~0.91 | 0.78 | 0.38~1.55 |
| Education (Senior Secondary and below) | ||||||
| Junior college | 3.10 * | 1.01~9.56 | −1.69 ** | −2.83~−0.55 | 2.53 | 0.79~7.95 |
| Undergraduate | 1.95 | 0.70~5.17 | −1.80 *** | −2.83~−0.78 | 1.55 | 0.54~4.23 |
| Graduate | 2.21 | 0.63~7.64 | −2.21 ** | −3.52~−0.89 | 1.56 | 0.43~5.62 |
| Occupation (Doctor) | ||||||
| Nurse | 1.62 | 0.81~3.08 | −0.54 | −1.35~0.27 | 1.43 | 0.71~2.76 |
| Medical Technician | 3.21 * | 1.34~8.32 | −0.92 * | −1.81~−0.03 | 2.67 * | 1.10~7.02 |
| Others | 2.33 | 0.82~7.21 | 0.28 | −0.85~1.41 | 2.39 | 0.82~7.56 |
| Underlying disease (No) | ||||||
| Yes | 0.56 * | 0.33~0.97 | −0.08 | −0.75~0.59 | 0.54 * | 0.32~0.94 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luo, C.; Chen, H.-X.; Tung, T.-H. COVID-19 Vaccination in China: Adverse Effects and Its Impact on Health Care Working Decisions on Booster Dose. Vaccines 2022, 10, 1229. https://doi.org/10.3390/vaccines10081229
Luo C, Chen H-X, Tung T-H. COVID-19 Vaccination in China: Adverse Effects and Its Impact on Health Care Working Decisions on Booster Dose. Vaccines. 2022; 10(8):1229. https://doi.org/10.3390/vaccines10081229
Chicago/Turabian StyleLuo, Chengwen, Hai-Xiao Chen, and Tao-Hsin Tung. 2022. "COVID-19 Vaccination in China: Adverse Effects and Its Impact on Health Care Working Decisions on Booster Dose" Vaccines 10, no. 8: 1229. https://doi.org/10.3390/vaccines10081229
APA StyleLuo, C., Chen, H.-X., & Tung, T.-H. (2022). COVID-19 Vaccination in China: Adverse Effects and Its Impact on Health Care Working Decisions on Booster Dose. Vaccines, 10(8), 1229. https://doi.org/10.3390/vaccines10081229