
Intensity of Humoral Immune Responses, Adverse Reactions, and Post-Vaccination Morbidity after Adenovirus Vector-Based and mRNA Anti-COVID-19 Vaccines

 ,
,  ,
,  , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Laboratory Tests
2.3. Statistical Analysis
3. Results
3.1. Adverse Reactions after Vaccination
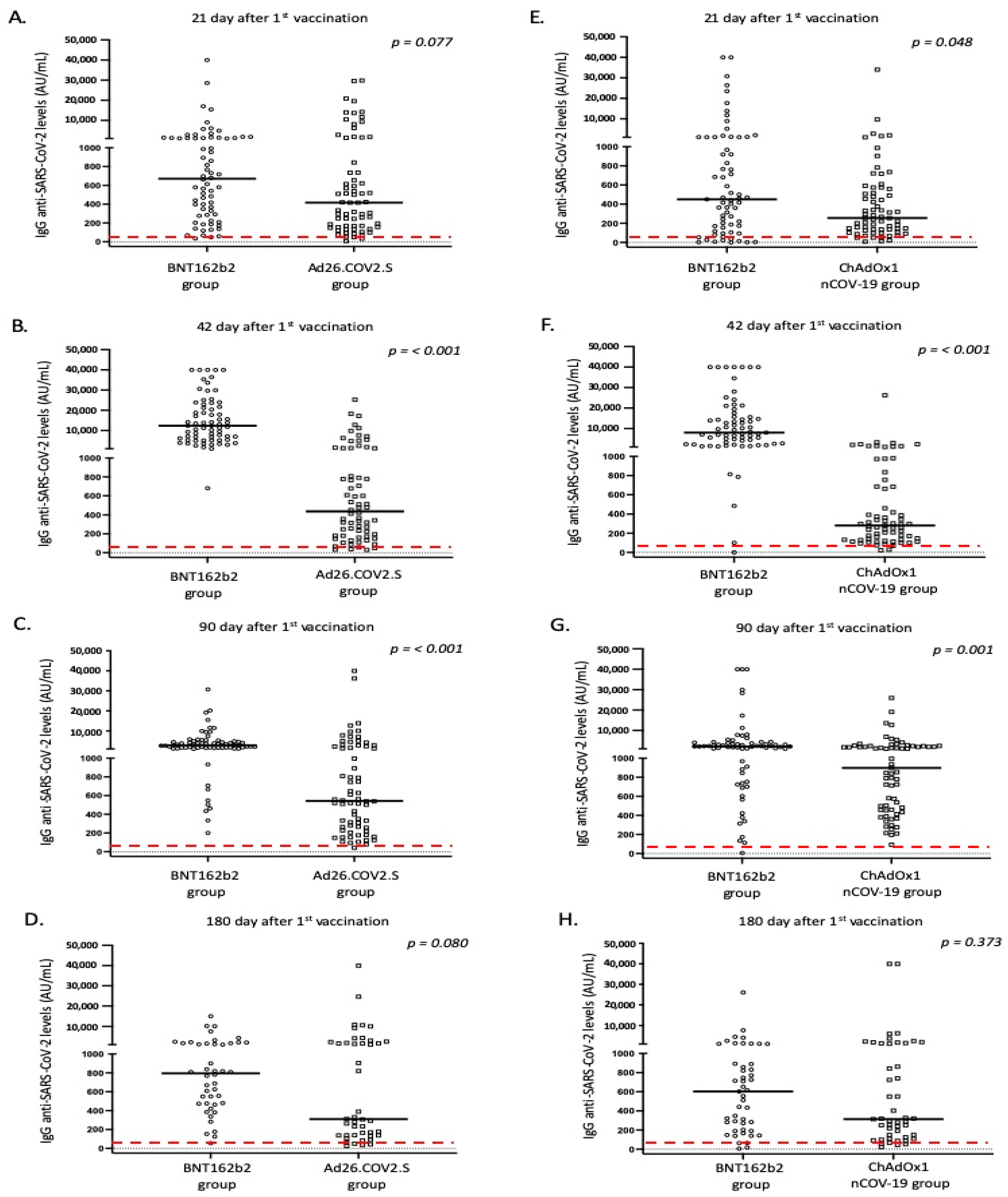
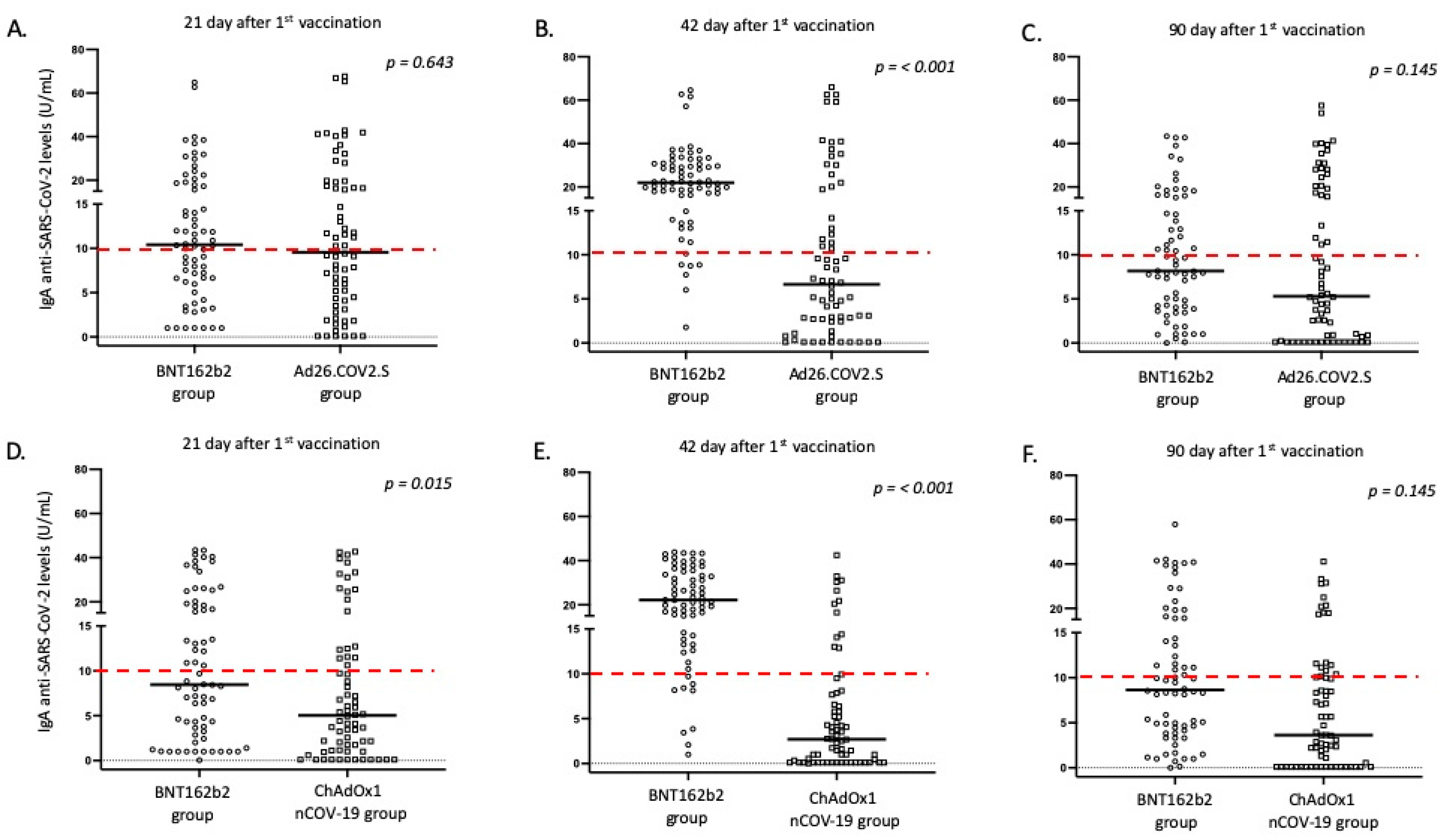
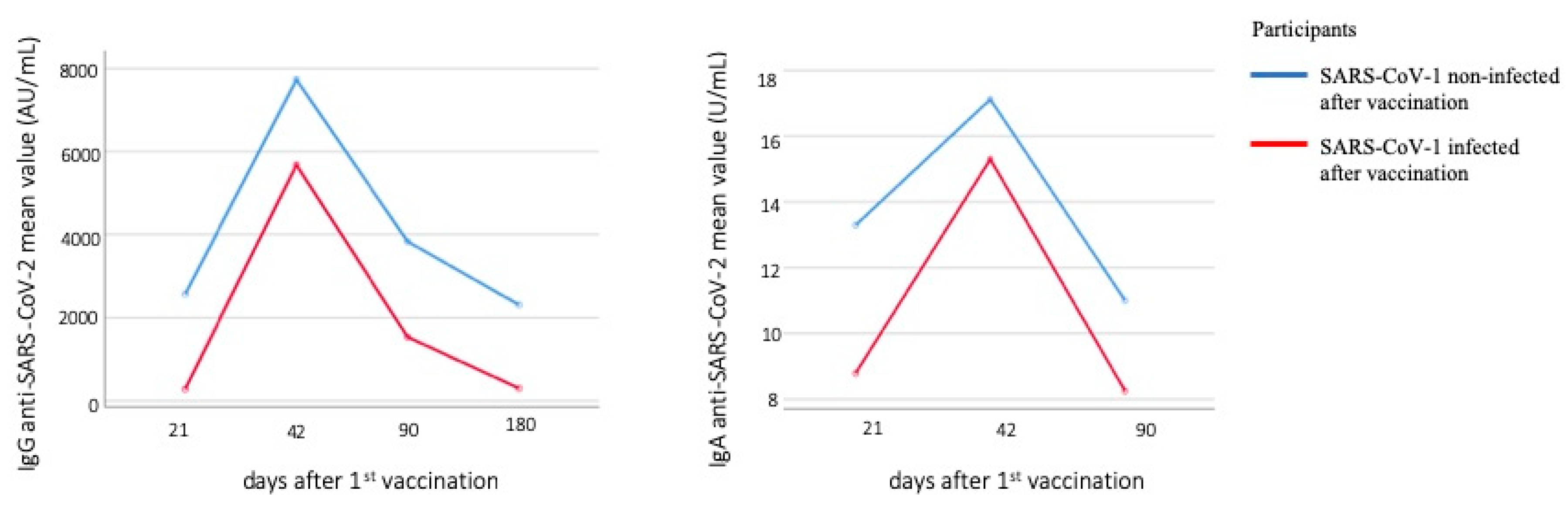
3.2. Intensity and Dynamics of IgG and IgA Responses after Vaccination
3.3. Correlation of IgG Responses with Demographic and Clinical Parameters of Vaccinated Individuals
3.4. Correlation of IgA Responses with Demographic and Clinical Parameters of Vaccinated Individuals
3.5. Correlation of Antibody Titers and COVID-19 after Vaccination
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Novel Coronavirus (2019-nCoV) Situation Report-11. Available online: https://apps.who.int/iris/bitstream/handle/10665/330776/nCoVsitrep31Jan2020-eng.pdf (accessed on 11 June 2022).
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization declares global emergency: A review of the 2019 Novel Coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the Coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Forni, G.; Mantovani, A. COVID-19 Vaccines: Where we stand and challenges ahead. Cell Death Differ. 2021, 28, 626–639. [Google Scholar] [CrossRef] [PubMed]
- Mascellino, M.T.; Di Timoteo, F.; De Angelis, M.; Oliva, A. Overview of the main anti-SARS-CoV-2 vaccines: Mechanism of action, efficacy and safety. Infect. Drug Resist. 2021, 14, 3459–3476. [Google Scholar] [CrossRef] [PubMed]
- Krammer, F. SARS-CoV-2 vaccines in development. Nature 2020, 586, 516–527. [Google Scholar] [CrossRef] [PubMed]
- WHO Issues Its First Emergency Use Validation for a COVID-19 Vaccine and Emphasizes Need for Equitable Global Access. Available online: https://www.who.int/news/item/31-12-2020-who-issues-its-first-emergency-use-validation-for-a-covid-19-vaccine-and-emphasizes-need-for-equitable-global-access (accessed on 9 June 2022).
- Lamb, Y.N. BNT162b2 mRNA COVID-19 vaccine: First approval. Drugs 2021, 81, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Yang, H.; Ji, W.; Wu, W.; Chen, S.; Zhang, W.; Duan, G. Virology, epidemiology, pathogenesis, and control of COVID-19. Viruses 2020, 12, 372. [Google Scholar] [CrossRef] [Green Version]
- Walls, A.C.; Park, Y.-J.; Tortorici, M.A.; Wall, A.; McGuire, A.T.; Veesler, D. Structure, function, and antigenicity of the SARS-CoV-2 spike glycoprotein. Cell 2020, 181, 281–292.e6. [Google Scholar] [CrossRef]
- Wu, J.; Liang, B.; Chen, C.; Wang, H.; Fang, Y.; Shen, S.; Yang, X.; Wang, B.; Chen, L.; Chen, Q.; et al. SARS-CoV-2 infection induces sustained humoral immune responses in convalescent patients following symptomatic COVID-19. Nat. Commun. 2021, 12, 1813. [Google Scholar] [CrossRef]
- Martinez-Flores, D.; Zepeda-Cervades, J.; Cruz-Resendiz, A.; Aguirre-Sampieri, S.; Sampieri, A.; Vaca, L. SARS-CoV-2 vaccines based on the Spike glycoprotein and implications of the new viral variants. Front. Immunol. 2021, 12, 701501. [Google Scholar] [CrossRef]
- Mistry, P.; Barmania, F.; Mellet, J.; Peta, K.; Strydom, A.; Viljoen, I.M.; James, W.; Gordon, S.; Petter, M.S. SARS-CoV-2 variants, vaccines, and host immunity. Front. Immunol. 2022, 12, 809244. [Google Scholar] [CrossRef] [PubMed]
- Duan, L.; Zheng, Q.; Zhang, H.; Niu, Y.; Lou, Y.; Wang, H. The SARS-CoV-2 spike glycoprotein biosynthesis, structure, function, and antigenicity: Implications for the design of spike-based vaccine immunogens. Front. Immunol. 2020, 11, 576622. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency—Comirnaty. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/comirnaty (accessed on 29 June 2022).
- European Medicines Agency—Comirnaty: Annex I—Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/comirnaty-epar-product-information_en.pdf (accessed on 11 June 2022).
- European Medicines Agency—Vaxzervia: Annex I—Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/vaxzevria-previously-covid-19-vaccine-astrazeneca-epar-product-information_en.pdf (accessed on 11 June 2022).
- European Medicines Agency—JCOVDEN: Annex I—Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/jcovden-previously-covid-19-vaccine-janssen-epar-product-information_en.pdf (accessed on 11 June 2022).
- Xie, J.; Feng, S.; Li, X.; Gea-Mallorquí, E.; Prats-Uribe, A.; Prieto-Alhambra, D. Comparative effectiveness of the BNT162b2 and ChAdOx1 vaccines against COVID-19 in people over 50. Nat. Commun. 2022, 13, 1519. [Google Scholar] [CrossRef] [PubMed]
- Naranbhai, V.; Garcia-Beltran, W.F.; Chang, C.C.; Berrios Mairena, C.; Thierauf, J.C.; Kirkpatrick, G.; Onozato, M.L.; Cheng, J.; St Denis, K.J.; Lam, E.C.; et al. Comparative immunogenicity and effectiveness of MRNA-1273, BNT162b2, and Ad26.COV2.S COVID-19 vaccines. J. Infect. Dis. 2021, 225, 1141–1150. [Google Scholar] [CrossRef] [PubMed]
- Speletas, M.; Kyritsi, M.A.; Vontas, A.; Theodoridou, A.; Chrysanthidis, T.; Hatzianastasiou, S.; Petinaki, E.; Hadjichristodoulou, C. Evaluation of two chemiluminescent and three ELISA immunoassays for the detection of SARS-CoV-2 IgG antibodies: Implications for disease diagnosis and patients’ management. Front. Immunol. 2020, 11, 609242. [Google Scholar] [CrossRef] [PubMed]
- Speletas, M.; Voulgaridi, I.; Sarrou, S.; Dadouli, A.; Mouchtouri, V.A.; Nikoulis, D.J.; Tsakona, M.; Kyritsi, M.A.; Peristeri, A.-M.; Avakian, I.; et al. Intensity and dynamics of anti-SARS-CoV-2 immune responses after BNT162b2 MRNA vaccination: Implications for public health vaccination strategies. Vaccines 2022, 10, 316. [Google Scholar] [CrossRef] [PubMed]
- Kaneko, N.; Kuo, H.H.; Boucau, J.; Farmer, J.R.; Allard-Chamard, H.; Mahajan, V.S.; Piechocka-Trocha, A.; Lefteri, K.; Osborn, M.; Bals, J.; et al. Loss of Bcl-6-Expressing T Follicular Helper Cells and Germinal Centers in COVID-19. Cell 2020, 183, 143–175.e13. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Ramasamy, M.N.; Minassian, A.M.; Ewer, K.J.; Flaxman, A.L.; Folegatti, P.M.; Owens, D.R.; Voysey, M.; Aley, P.K.; Angus, B.; Babbage, G.; et al. Safety and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): A single-blind, randomized, Controlled, Phase 2/3 Trial. Lancet 2020, 396, 1979–1993. [Google Scholar] [CrossRef]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and efficacy of single-dose Ad26.COV2.S vaccine against COVID-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef]
- Mathioudakis, A.G.; Ghrew, M.; Ustianowski, A.; Ahmad, S.; Borrow, R.; Papavasileiou, L.P.; Petrakis, D.; Bakerly, N.D. Self-reported real-world safety and reactogenicity of COVID-19 vaccines: A vaccine recipient survey. Life 2021, 11, 249. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Khillan, R.; Mishra, Y.; Khurana, S. The safety profile of COVID-19 vaccinations in the United States. Am. J. Infect. Control 2022, 50, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Mateus, J.; Coelho, C.H.; Dan, J.M.; Moderbacher, C.R.; Gálvez, R.I.; Cortes, F.H.; Grifoni, A.; Tarke, A.; Chang, J.; et al. Humoral and cellular immune memory to four COVID-19 vaccines. Cell 2022, 185, 2434–2451. [Google Scholar] [CrossRef] [PubMed]
- Szczepanek, J.; Skorupa, M.; Goroncy, A.; Jarkiewicz-Tretyn, J.; Wypych, A.; Sandomierz, D.; Jarkiewicz-Tretyn, A.; Dejewska, J.; Ciechanowska, K.; Pałgan, K.; et al. Anti-SARS-CoV-2 IgG against the S protein: A comparison of BNT162b2, mRNA-1273, ChAdOx1 nCoV-2019 and Ad26.COV2.S vaccines. Vaccines 2022, 10, 99. [Google Scholar] [CrossRef]
- Wisnewski, A.V.; Campillo Luna, J.; Redlich, C.A. Human IgG and IgA Responses to COVID-19 mRNA vaccines. PLoS ONE 2021, 16, e0249499. [Google Scholar] [CrossRef]
- Zurac, S.; Nichita, L.; Mateescu, B.; Mogodici, C.; Bastian, A.; Popp, C.; Cioplea, M.; Socoliuc, C.; Constantin, C.; Neagu, M. COVID-19 vaccination and IgG and IgA antibody dynamics in healthcare workers. Mol. Med. Rep. 2021, 24, 578. [Google Scholar] [CrossRef] [PubMed]
- Romero-Pinedo, S.; Quesada, M.; Horndler, L.; Álvarez-Fernández, S.; Olmo, A.; Abia, D.; Alarcón, B.; Delgado, P. Vaccine type-, age- and past infection-dependence of the humoral response to SARS-CoV-2 spike S protein. Front. Immunol. 2022, 13, 809285. [Google Scholar] [CrossRef]
- Kang, Y.M.; Minn, D.; Lim, J.; Lee, K.-D.; Jo, D.H.; Choe, K.-W.; Kim, M.J.; Kim, J.M.; Kim, K.N. Comparison of antibody response elicited by ChAdOx1 and BNT162b2 COVID-19 vaccine. J. Korean Med. Sci. 2021, 36, e311. [Google Scholar] [CrossRef]
- Pellini, R.; Venuti, A.; Pimpinelli, F.; Abril, E.; Blandino, G.; Campo, F.; Conti, L.; De Virgilio, A.; De Marco, F.; Di Domenico, E.G.; et al. Initial observations on age, gender, BMI and hypertension in antibody responses to SARS-CoV-2 BNT162b2 vaccine. EClinicalMedicine 2021, 36, 100928. [Google Scholar] [CrossRef]
- Notarte, K.I.; Ver, A.T.; Velasco, J.V.; Pastrana, A.; Catahay, J.A.; Salvagno, G.L.; Yap, E.P.H.; Martinez-Sobrido, L.; Torrelles, J.B.; Lippi, G.; et al. Effects of age, sex, serostatus, and underlying comorbidities on humoral response post-SARS-CoV-2 Pfizer-BioNTech mRNA vaccination: A systematic review. Crit. Rev. Clin. Lab. Sci. 2022, 28, 1–18. [Google Scholar] [CrossRef]
- Fiolet, T.; Kherabi, Y.; MacDonald, C.-J.; Ghosn, J.; Peiffer-Smadja, N. Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: A narrative review. Clin. Microbiol. Infect. 2022, 28, 202–221. [Google Scholar] [CrossRef] [PubMed]
- Cohn, B.A.; Cirillo, P.M.; Murphy, C.C.; Krigbaum, N.Y.; Wallace, A.W. SARS-CoV-2 vaccine protection and deaths among US veterans during 2021. Science 2022, 375, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Rzymski, P.; Perek, B.; Flisiak, R. Thrombotic thrombocytopenia after COVID-19 vaccination: In search of the underlying mechanism. Vaccines 2021, 9, 559. [Google Scholar] [CrossRef] [PubMed]
- Long, B.; Bridwell, R.; Gottlieb, M. Thrombosis with thrombocytopenia syndrome associated with COVID-19 vaccines. Am. J. Emerg. Med. 2021, 49, 58–61. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| BNT162b2 | ChAdOx1 nCoV-19 | Ad26.COV2.S | |
|---|---|---|---|
| 135 (n, %) | 67 (n, %) | 68 (n, %) | |
| Gender (male/female) | 81/54 | 39/28 | 42/26 |
| Age (years; median, range) | 49.0 (27–84) | 64.0 (33–84) | 46.5 (20–74) |
| Hypertension | 29, 21.5 | 30, 44.8 | 6, 8.8 |
| Diabetes mellitus | 11, 8.2 | 11, 16.4 | 1, 1.5 |
| Dyslipidemia | 23, 17.0 | 20, 29.9 | 2, 2.9 |
| Chronic heart disease ^ | 9, 6.7 | 6, 9.0 | 3, 4.4 |
| Chronic respiratory disease * | 5, 3.7 | 1, 1.5 | 1, 1.5 |
| Stroke and transient ischemic attacks | 7, 5.2 | 1, 1.5 | 0, 0.0 |
| Thrombotic attacks | 0, 0.0 | 0, 0.0 | 2, 2.9 |
| Chronic liver disease # | 2, 1.5 | 1, 1.5 | 0, 0.0 |
| Chronic kidney disease ^^ | 1, 0.7 | 0, 0.0 | 0, 0.0 |
| Thyroid disease ** | 10, 7.4 | 6, 9.0 | 5, 7.4 |
| Autoimmune/autoinflammatory disease § | 7, 5.2 | 2, 3.0 | 0, 0.0 |
| Cancer ## | 2, 1.5 | 1, 1.5 | 1, 1.5 |
| Insomnia or psychiatric diseases *** | 25, 18.5 | 1, 1.5 | 2, 2.9 |
| Others ^^^ | 20, 14.8 | 10, 14.9 | 3, 4.4 |
| Previous COVID-19 disease | 20, 14.8 | 2, 3.0 | 13, 19.1 |
| BNT162b2 (No. 68) | Ad26.COV2.S (No. 68) | p1 ^ | p2 ^ | ||
|---|---|---|---|---|---|
| 1st Dosage (n, %) | 2nd Dosage (n, %) | 1st Dosage (n, %) | |||
| Sex (M/F) | 42/26 | 42/26 | |||
| Age (years; median, range) | 45.0, 27–74 | 46.5, 20–74 | |||
| Local pain | 22, 34.9 | 15, 23.8 | 12, 17.6 | 0.029 | 0.397 |
| Fever | 1, 1.5 | 9, 13.2 | 20, 29.4 | <0.001 | 0.035 |
| Myalgias | 3, 4.8 | 13, 20.6 | 4, 5.9 | 1.000 | 0.018 |
| Fatigue | 4, 6.4 | 15, 23.8 | 14, 20.6 | 0.022 | 0.679 |
| Headache | 6, 9.5 | 2, 3.2 | 7, 10.3 | 1.000 | 0.167 |
| Flu-like symptoms | 0, 0.0 | 1, 1.6 | 0, 0.0 | 1.000 | 0.481 |
| Others * | 4, 6.4 | 7, 11.1 | 8, 11.8 | 0.369 | 1.000 |
| BNT162b2 (No. 67) | ChAdOx1 nCoV-19 (No. 67) | p1 ^ | p2 ^ | |||
| 1st Dosage (n, %) | 2nd Dosage (n, %) | 1st Dosage (n, %) | 2nd Dosage (n, %) | |||
| Sex (M/F) | 39/28 | 39/27 | 39/28 | 39/27 | ||
| Age (years; median, range) | 64.0 (33–84) | 64.0 (33–84) | ||||
| Local pain | 10, 24.4 | 8, 20.0 | 21, 31.3 | 11, 16.7 | 0.514 | 0.795 |
| Fever | 1, 1.5 | 3, 4.6 | 18, 26.9 | 3, 4.6 | <0.001 | 1.000 |
| Myalgias | 0, 0.0 | 2, 5.0 | 8, 11.9 | 2, 3.0 | 0.023 | 0.632 |
| Fatigue | 4, 9.8 | 7, 17.5 | 15, 22.4 | 6, 9.1 | 0.121 | 0.231 |
| Headache | 3, 7.3 | 3, 7.5 | 7, 10.5 | 1, 1.5 | 0.739 | 0.149 |
| Flu-like symptoms | 0, 0.0 | 0, 0.0 | 1, 1.5 | 0, 0.0 | 1.000 | 1.000 |
| Others * | 1, 2.4 | 0, 0.0 | 8, 11.9 | 7, 10.6 | 0.149 | 0.043 |
| BNT162b2 (No. 67) | ChAdOx1 nCoV-19H (No. 67) | p1 * | BNT162b2 (No. 68) | Ad26.COV2.S (No. 68) | p2 * | BNT162b2 Total | Adenovirus Vector-Based Total | p3 * | |
|---|---|---|---|---|---|---|---|---|---|
| Sex (male/female) | 39/28 | 39/28 | 42/26 | 42/26 | 81/54 | 81/54 | |||
| Age (median, range) | 64.0, 33.0–84.0 | 64.0, 33.0–84.0 | 45.0, 27.0–74.0 | 46.5, 20.0–74.0 | 49.0, 27.0–84.0 | 49.0, 20.0–84.0 | |||
| Day 21 | |||||||||
| IgG (median, range) (AU/mL) | 450.5, 0.0–40,000.0 | 255.4, 7.8–33,994.22 | 0.048 | 670.8, 35.9–40,000.0 | 416.2, 7.1–29,806.1 | 0.077 | 541.8, 0.0–40,000.0 | 308.2, 7.1–33,994.2 | <0.001 |
| IgG positivity (n, %) | 58, 86.6 | 63, 94.0 | 67, 98.5 | 64, 94.1 | 125, 92.6 | 128, 94.8 | |||
| IgA median, range (U/mL) | 8.5, 0.0–43.5 | 5.0, 0.1–42.7 | 0.015 | 10.4, 1.0–64.9 | 9.6, 0.1–67.6 | 0.643 | 10.3, 14.2, 0.0–64.9 | 7.2, 0.1–67.6 | 0.023 |
| IgA positivity (n, %) | 31, 46.3 | 19, 28.4 | 37, 54.4 | 33, 48.5 | 68, 50.4 | 52, 38.5 | |||
| Day 42 | |||||||||
| IgG (median, range) (AU/mL) | 8015.3, 0.2–40,000.0 | 281.0, 22.4–26,246.5 | <0.001 | 12,369.4, 680.8–40,000.0 | 436.5, 29.6–25,236.4 | <0.001 | 10,576.2, 0.2–40,000.0 | 326.9, 22.4–26,246.5 | <0.001 |
| IgG positivity (n, %) | 66, 98.5 | 65, 97.0 | 68, 100.0 | 66, 97.1 | 134, 99.3 | 131, 97.0 | |||
| IgA median, range (U/mL) | 22.2, 1.0–43.9 | 2.7, 0.0–42.5 | <0.001 | 22.0, 1.8–64.6 | 6.7, 0.1–66.0 | <0.001 | 22.2, 1.0–64.6 | 4.2, 0.0–66.0 | <0.001 |
| IgA positivity (n, %) | 59, 88.10 | 11, 16.4 | 62, 91.2 | 24, 35.3 | 121, 89.6 | 35, 25.9 | |||
| Day 90 | |||||||||
| IgG (median, range) (AU/mL) | 2181.9, 5.4–40,000.0 | 898.1, 91.8–25,934.9 | 0.001 | 2822.2, 200.5–30,759.0 | 543.6, 43.2–40,000.0 | <0.001 | 2345.4, 5.4–40,000.0 | 745.3, 1 43.2–40,000.0 | <0.001 |
| IgG positivity (n, %) | 66, 98.5 | 67, 100.0 | 68, 100.0 | 67, 98.5 | 134. 99.3 | 134, 99.3 | |||
| IgA median, range (U/mL) | 8.8, 0.0–57.9 | 3.6, 0.1–41.1 | 0.145 | 8.2, 0.0–43.4 | 5.3, 0.0–57.5 | 0.145 | 8.6, 1 0.0–57.9 | 4.7, 0.1–57.5 | <0.001 |
| IgA positivity (n, %) | 29, 43.3 | 17, 25.4 | 29, 42.6 | 26, 38.2 | 58, 43.0 | 43, 31.9 | |||
| Day 180 | (n: 47) | (n: 44) | (n: 91) | ||||||
| IgG (median, range) (AU/mL) | 602.5, 5.0–26,031.9 | 314.2, 23.3–40,000.0 | 0.373 | 795.1, 55.2–14,969.0 | 309.8, 25.2–40,000.0 | 0.080 | 686.7, 5.0–26,031.9 | 312.4, 23.3–40,000.0 | 0.057 |
| IgG positivity (n, %) | 45, 95.7 | 45, 95.7 | 44, 100.0 | 40, 90.9 | 89, 97.8 | 85, 93.0 | |||
| Dependent Variable | Parameter | p1 | Coefficient | p2 * | Coefficient |
|---|---|---|---|---|---|
| Anti-S IgG levels on day 21 | Age | 0.611 | 12.2 (−34.9, 59.3) | 0.079 | −9.4 (−20.0, 1.1) |
| Vaccine type (adenovirus vector-based vs. mRNA) | 0.484 | −381.5 (−1452.6, 689.7) | 0.002 | −381.3 (−618.9, −143.8) | |
| Comorbidity (no vs. ≥1) | 0.472 | 495.9 (−859.9, 1851.7) | 0.098 | −248.1 (−542.6, 46.4) | |
| COVID-19 history before vaccination | <0.001 | 15,364.8 (13,768.0, 16,961.6) | Excluded | ||
| Anti-S IgG levels on day 42 | Age | 0.441 | −31.65 (−112.38, 49.10) | 0.009 | −97.89 (−171.36, −24.41) |
| Vaccine type (adenovirus vector-based vs. mRNA) | <0.001 | −12,041 (−13,875.5, −10,206.4) | <0.001 | −10,707.98 (−12,356.9, 9059.0) | |
| Comorbidity (no vs. ≥1) | 0.358 | −1082.2 (−3396.3, 1232.0) | 0.077 | −1835.1 (−3872.8, 202.6) | |
| COVID-19 history before vaccination | <0.001 | 12,559.8 (9832.2, 15,287.5) | Excluded | ||
| COVID-19 history after vaccination | 0.002 | 17,143.2 (−6431.5, 27,855.0) | |||
| Anti-S IgG levels on day 90 | Age | 0.103 | 48.12 (−9.78, 106.02) | 0.268 | −18.6 (−51.49, 14.38) |
| Vaccine type (adenovirus vector-based vs. mRNA) | 0.001 | −2320.6 (−3635.8, −1005.3) | 0.002 | −1149.5 (−1888.9, −410.1) | |
| Comorbidity (no vs. ≥1) | 0.590 | 453.6 (−1202.7, 2110.0) | 0.665 | 200.2 (−709.8, 1110.3) | |
| COVID-19 history before vaccination | <0.001 | 8871.6 (6923.1, 10,820.1) | Excluded | ||
| COVID-19 history after vaccination | <0.001 | 16,889.1 (12,695.6, 21,082.6) | |||
| Anti-S IgG levels on day 180 | Age | 0.522 | 20.54 (−42.71, 83.79) | 0.077 | −14.18 (−29.92, 1.55) |
| Vaccine type (adenovirus vector-based vs. mRNA) | 0.542 | −435.8 (−1844.6, 973.0) | 0.204 | −222.8 (−567.8, 122.1) | |
| Comorbidity (no vs. ≥1) | 0.564 | 504.7 (−1219.2, 2228.6) | 0.840 | −43.4 (−466.9, 380.2) | |
| COVID-19 history before vaccination | 0.003 | 3419.2 (1162.7, 5675.7) | Excluded | ||
| COVID-19 history after vaccination | <0.001 | 14,638.1 (11,790.0, 17,486.3) | |||
| Dependent Variable | Parameter | p1 | Coefficient | p2 * | Coefficient |
|---|---|---|---|---|---|
| Anti-S IgA levels on day 21 | Age | 0.146 | −0.08 (−0.19, 0.03) | 0.301 | −0.05 (−0.16, 0.05) |
| Vaccine type (adenovirus vector-based vs. mRNA) | 0.551 | −0.7 (−3.2, 1.7) | 0.093 | −2.0 (−4.3, 0.3) | |
| Comorbidity (no vs. ≥1) | 0.560 | −0.9 (−4.0, 2.2) | 0.245 | −1.7 (−4.6, 1.2) | |
| COVID-19 history before vaccination | <0.001 | 27.8 (24.1, 31.3) | Excluded | ||
| Anti-S IgA levels on day 42 | Age | 0.186 | −0.08 (−0.19, 0.04) | 0.651 | −0.03 (−0.14, 0.09) |
| Vaccine type (adenovirus vector-based vs. mRNA) | <0.001 | −14.2 (−16.8, −11.6) | <0.001 | −16.1 (−18.6, −13.6) | |
| Comorbidity (no vs. ≥1) | 0.520 | −1.1 (−4.4, 2.2) | 0.301 | −1.6 (−4.7, 1.5) | |
| COVID-19 history before vaccination | <0.001 | 22.4 (18.5, 26.2) | Excluded | ||
| COVID-19 history after vaccination | 0.001 | 26.3 (10.9, 41.6) | |||
| Anti-S IgA levels on day 90 | Age | 0.661 | 0.02 (−0.08, 0.12) | 0.765 | 0.01 (−0.08, 0.11) |
| Vaccine type (adenovirus vector-based vs. mRNA) | 0.009 | −2.9 (−5.2, −0.8) | 0.002 | −3.2 (−5.2, −1.2) | |
| Comorbidity (no vs. ≥1) | 0.680 | −0.6 (−3.3, 2.2) | 0.280 | −1.4 (−3.9, 1.1) | |
| COVID-19 history before vaccination | <0.001 | 22.5 (19.2, 25.7) | Excluded | ||
| COVID-19 history after vaccination | <0.001 | 21.4 (13.8, 28.9) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Voulgaridi, I.; Sarrou, S.; Dadouli, A.; Peristeri, A.-M.; Nasika, A.; Onoufriadis, I.; Kyritsi, M.A.; Anagnostopoulos, L.; Theodoridou, A.; Avakian, I.; et al. Intensity of Humoral Immune Responses, Adverse Reactions, and Post-Vaccination Morbidity after Adenovirus Vector-Based and mRNA Anti-COVID-19 Vaccines. Vaccines 2022, 10, 1268. https://doi.org/10.3390/vaccines10081268
Voulgaridi I, Sarrou S, Dadouli A, Peristeri A-M, Nasika A, Onoufriadis I, Kyritsi MA, Anagnostopoulos L, Theodoridou A, Avakian I, et al. Intensity of Humoral Immune Responses, Adverse Reactions, and Post-Vaccination Morbidity after Adenovirus Vector-Based and mRNA Anti-COVID-19 Vaccines. Vaccines. 2022; 10(8):1268. https://doi.org/10.3390/vaccines10081268
Chicago/Turabian StyleVoulgaridi, Ioanna, Styliani Sarrou, Aikaterini Dadouli, Athanasia-Marina Peristeri, Asimina Nasika, Ilias Onoufriadis, Maria A. Kyritsi, Lemonia Anagnostopoulos, Aikaterini Theodoridou, Ioanna Avakian, and et al. 2022. "Intensity of Humoral Immune Responses, Adverse Reactions, and Post-Vaccination Morbidity after Adenovirus Vector-Based and mRNA Anti-COVID-19 Vaccines" Vaccines 10, no. 8: 1268. https://doi.org/10.3390/vaccines10081268